principles of infection prevention and control · how do we implement the principles? •framework...
TRANSCRIPT

Principles of Infection Prevention and
Control
Liz Van Horne
Manager, Core Competencies
Senior Infection Prevention & Control Professional
OAHPP
Outbreak Management Workshop
September 15, 2010

Objectives
• To describe the principles of infection prevention and
control for:
– Routine Practices
– Additional Precautions
– Rationale for use

How do we implement the principles?
• Framework for all infection prevention and control
programs is built around consistent use of
– Routine Practices and
– Additional Precautions
• Implementation will vary depending on the health care
setting
• Principles remain the same

Principles and Rationale of Routine
Practices• All patients are potentially infectious, therefore:
– Same principles of practice should be used
• ALL the time
• With ALL patients
– ALL contact with blood, body fluid, secretions,
excretions, mucous membranes, non-intact skin or
soiled items could potentially transmit infectious
organisms
Routine Practices prevent transmission of organisms from:
Resident/Patient to
resident/patient
Resident/Patient to staff
Staff to resident/patient
Staff to staff

Elements of Routine Practices
• Risk assessment
• Environmental controls
• Administrative controls
• Sufficient and accessible barrier equipment, i.e. PPE

Risk Assessment
• Dynamic process based on continuing changes in
information as care progresses, thus must be done before
each interaction with a client/patient/resident (PIDAC)

Assessing Risk
• Risk of transmission involves factors related to:
– Client/patient/resident infection status
– Client/patient/resident characteristics
– Type of care activities being performed
– Resources available for control
– Health care provider immune status

Risk Assessment
Do I need protection because of a risk of exposure to blood,
secretions/excretions or body fluids?
Do I need protection because of the patient’s symptoms?
What are the organizational requirements for a patient with an
identified infection?

Will hands be exposed to
blood/body fluid or contaminated
items?
If yes,Wear gloves and perform
hand hygiene
Will face be exposed to
splash, spray, cough or
sneeze?
If yes,Wear facial protection
Will clothing or skin be exposed
to splashes?If yes, Wear a gown

Hand Hygiene –
• Elements of a hand hygiene program for all health care SETTINGS
– Multifaceted and multidisciplinary
– Point of care hand hygiene products
– Education on where, when, and how to clean hands
– Skin integrity
• Elements for health care FACILITIES
– Management support
– Environmental and system supports
– Observational audits and feedback

Alcohol-Based Hand Rub (ABHR)
• Preferred method of cleaning hands
– Can be performed without leaving the resident/patient
– Use when hands are not visibly soiled
• 70-90% alcohol
• Non-alcohol products are not to be used

Personal Protective Equipment
• PPE used alone or in combination to prevent exposure of health care
provider
• Selection based on the risk assessment
• PPE should be put on just prior to the interaction and removed
immediately after the interaction is done
• Staff must have quick, easy access to sufficient supplies of PPE
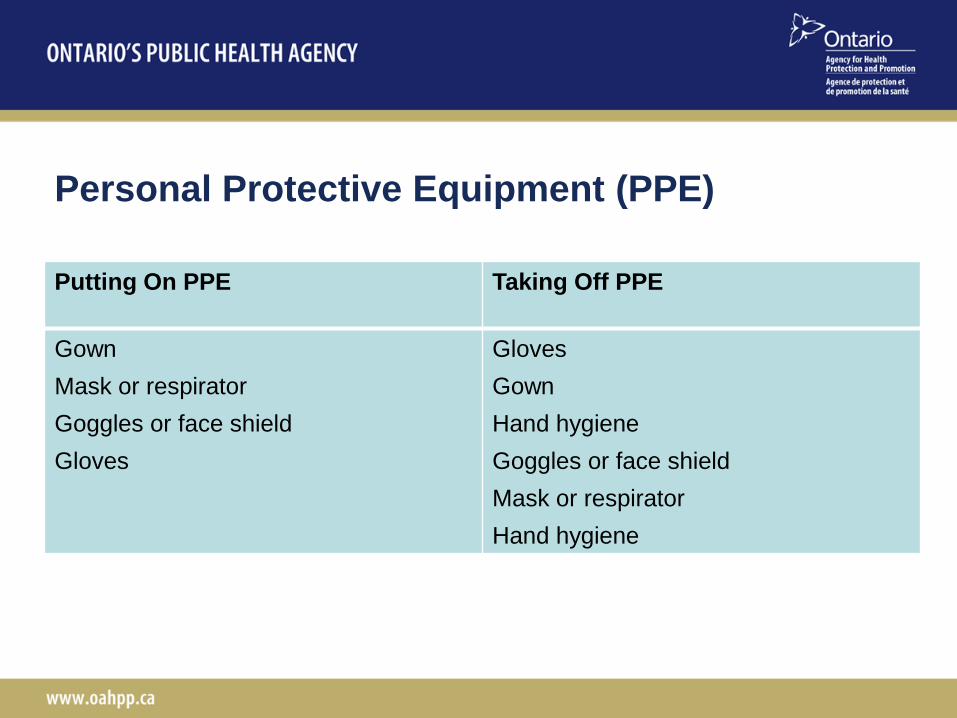
Personal Protective Equipment (PPE)
Putting On PPE Taking Off PPE
Gown
Mask or respirator
Goggles or face shield
Gloves
Gloves
Gown
Hand hygiene
Goggles or face shield
Mask or respirator
Hand hygiene

Gloves
• Medical grade gloves must be used for contact with mucous membranes,
non-intact skin, blood and body fluids
• Gloves are NOT required for routine health care activities that are limited
to intact skin
– Eg. taking blood pressure, bathing, dressing
• Compliance with hand hygiene

Appropriate Glove Use
• Task specific and single-use for the task
• Size must be correct
• Clean hands before putting on gloves
• Remove gloves immediately after the activity
• Clean hands after removing gloves
• Change gloves when moving from contaminated body site to a clean body
site on the same patient
• Do not wash or re-use gloves
• Gloves must be changed in between patients or when moving from a dirty
to clean procedure on the same patient

Types of Gloves
• Good quality vinyl gloves are suitable for most tasks
• Latex/synthetic gloves (nitrile or neoprene) are prefereable for clinical
procedures where manual dexterity or prolonged contact are expected
• Powdered latex gloves have been associated with latex allergy
• Gloves that fit snugly around the wrist are preferred for use with gowns

Gowns
• Only wear when providing care for patients
• Put on immediately before task
• Removed immediately after task

Masks and Respirators
• Masks
– To protect the mucous membranes of the health care provider when
anticipated splashes of blood or body fluids are anticipated
– Used in operating theatres and for performing aseptic procedures
– Place on coughing patient to limit dissemination of respiratory
secretions
• Respirators
– To prevent inhalation of small particles that may contain infectious
agents transmitted via airborne route
– Must be fit-tested
– Used for aerosol-generating procedures
• Sputum induction, diagnostic bronchoscopy

Eye Protection
• Used to protect the mucous membranes when splashing is anticipated
– Safety glasses
– Safety goggles
– Face shields
– Visors attached to masks
(does not include prescription eye glasses)
• Disposable or reusable
– Central processing area or assigned staff member to clean reusable
eye protection between uses is recommended

Environmental Controls
• Accommodation and Placement
• Environment and equipment cleaning
• Dishware and eating utensils
• Linen and waste
– Laundry
– Waste management
– Handling of sharps

Accommodation and Placement
• Single rooms with dedicated bathroom and sink are
preferred for all patients
• Decision making considerations for placement:
– Is patient soiling environment due to poor hygiene or incontinence?
– Does patient have an infection that might be transmitted to others?
– What is the condition of others in the unit?
– Does the patient have an indwelling device or non-intact skin?
– What is the susceptibility level of the patient or potential roommates?
– Can they follow directions on hygiene?

Environment and Equipment Cleaning
• Cleaning and disinfection of non-critical equipment
between patients
• High-level disinfection of semi-critical and sterilization of
critical medical equipment
• Daily and terminal cleaning of rooms
• Cleaning requirements for rooms with C. difficile or VRE
positive patients

Dishes, Linen and Waste
• Dishware and utensils do not need special processing
– Regular dishwashing processes are effective
• Laundry – soiled with blood/body fluids -- handle
ROUTINELY
– Bag/contain at the site of collection
– Use leak-proof bags/containers if contaminated with blood/body
substances
• Waste
– Protective apparel (gloves, footwear)
– Sharps disposal

Administrative Controls
• Policies and procedures
• Education
• Healthy workplace policies
• Respiratory etiquette
• Immunization
• Monitoring of compliance and feedback
• Staffing

Additional Precautions

Principles and Rationale of Additional
Precautions
• Additional Precautions are used in addition to Routine
Practices when a patient has a certain microorganism
– Includes suspect cases eg. diarrhea with no identified
cause
– Includes colonization eg. MRSA
• Application of Additional Precautions may differ depending
on the health setting and the needs – eg. long term care
and community

Elements of Additional Precautions
• Specialized accommodation and signage
• Barrier equipment
• Dedicated equipment
• Additional cleaning
• Limited transport procedures
• Communication

Additional Precautions
• Interventions used in ADDITION to Routine Practices
• Protect staff and patients from transmission of known or suspected
infectious agents
• Based on mode of transmission:
– Contact
– Droplet
– Airborne
• May be combined for some agents
– e.g. Droplet + Contact

What does this mean to Public Health?
Remember...
• Infection prevention and control involves applying principles to the
situation
• There are few ‘black and white’ rules – only a variety of gray shades

Questions?