primary melanoma of the esophagus, a diagnostic challenge · primary melanoma of the esophagus is a...
TRANSCRIPT

Asian Journal of Surgery (2015) 38, 236e238
Available online at www.sciencedirect.com
journal homepage: www.e-asianjournalsurgery.com
CASE REPORT
Primary melanoma of the esophagus,a diagnostic challenge
Yirong Sim a,*, Jonathan Shunming Teo a, Jabed Iqbal b,Weng Hoong Chan a
aDepartment of General Surgery, Singapore General Hospital, SingaporebDepartment of Pathology, Singapore General Hospital, Singapore
Received 3 April 2012; received in revised form 31 July 2012; accepted 31 October 2012Available online 19 February 2013
KEYWORDSesophageal Cancer;esophagealMelanoma;
melanoma
* Corresponding author. DepartmSingapore General Hospital, OutramSingapore.
E-mail address: yirong.sim@mohh.
1015-9584/$36 Copyright ª 2012, Asiahttp://dx.doi.org/10.1016/j.asjsur.20
Summary Primary melanoma of the esophagus is a rare condition. Its diagnosis can be chal-lenging, as its presentation is similar to that of other esophageal malignancies, especially whenmelanin is not evidently expressed in the melanoma. We report a case of esophageal mela-noma in a 59-year-old Chinese male, whose histological diagnosis was confirmed from the eso-phagectomy specimen.Copyright ª 2012, Asian Surgical Association. Published by Elsevier Taiwan LLC. All rightsreserved.
1. Introduction
First described by Baur in 1906,1 primary malignantmelanoma of the esophagus occurs very rarely, with anincidence of 3.6 in 1 billion, and it contributes to 0.1e0.2%of all esophageal neoplasms.2 From 2000 to 2011, of the134 cases of esophagectomies performed in our institutionfor esophageal carcinoma, only one had esophagealmelanoma; we herein present a case report of thispatient.
ent of General Surgery,Road, Singapore 169608,
com.sg (Y. Sim).
n Surgical Association. Published12.11.001
2. Case report
This is a case report of a 59-year-old Chinese male whopresented with a 2-week history of progressive dysphagiawithout regurgitation and any other constitutional symp-toms, and with no known medical history.
An esophagogastroduodenoscopy was performed, whichrevealed a nonpigmented polypoidal mass 25 cm from theincisor (Fig. 1), antral gastritis, and duodenitis. A biopsy ofthe polypoidal mass revealed a poorly differentiated inva-sive squamous cell carcinoma. Computed tomography(Fig. 2) confirmed a large (4.3 � 2.1 cm2), homogenouslyenhancing lobulated mass in the esophagus at the level ofthe aortic arch, extending just distal to the carina, withenlarged right upper paratracheal lymph nodes
by Elsevier Taiwan LLC. All rights reserved.
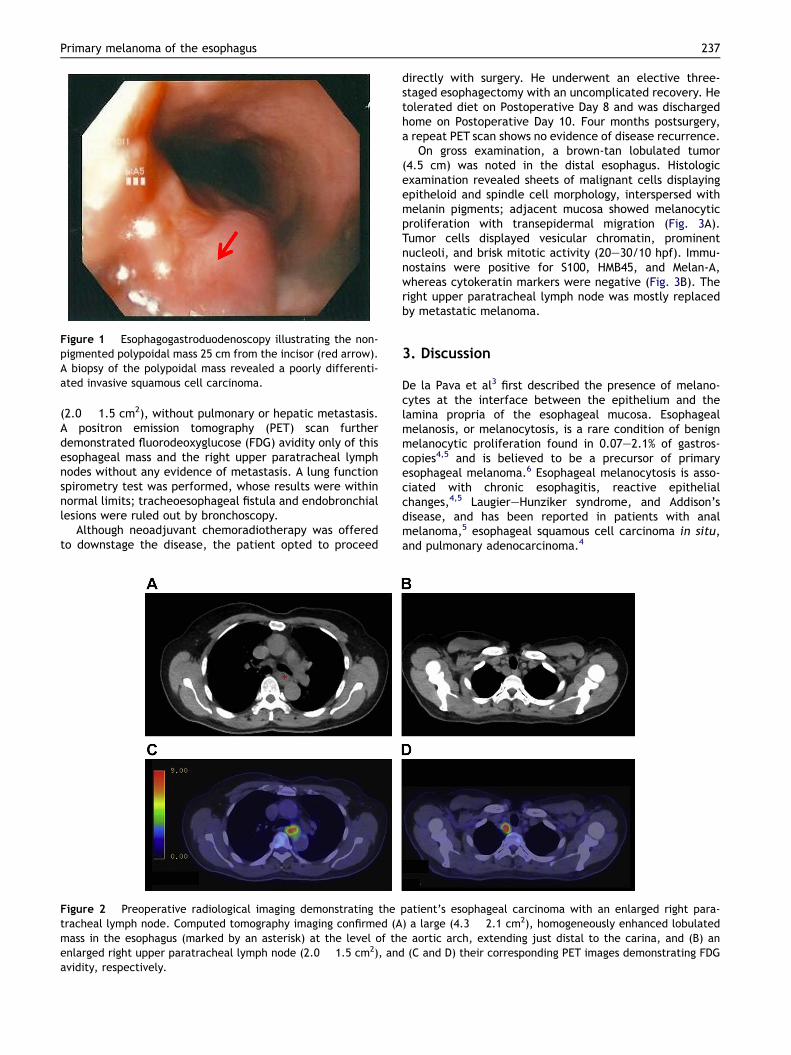
Figure 1 Esophagogastroduodenoscopy illustrating the non-pigmented polypoidal mass 25 cm from the incisor (red arrow).A biopsy of the polypoidal mass revealed a poorly differenti-ated invasive squamous cell carcinoma.
Primary melanoma of the esophagus 237
(2.0 � 1.5 cm2), without pulmonary or hepatic metastasis.A positron emission tomography (PET) scan furtherdemonstrated fluorodeoxyglucose (FDG) avidity only of thisesophageal mass and the right upper paratracheal lymphnodes without any evidence of metastasis. A lung functionspirometry test was performed, whose results were withinnormal limits; tracheoesophageal fistula and endobronchiallesions were ruled out by bronchoscopy.
Although neoadjuvant chemoradiotherapy was offeredto downstage the disease, the patient opted to proceed
Figure 2 Preoperative radiological imaging demonstrating thetracheal lymph node. Computed tomography imaging confirmed (Amass in the esophagus (marked by an asterisk) at the level of thenlarged right upper paratracheal lymph node (2.0 � 1.5 cm2), andavidity, respectively.
directly with surgery. He underwent an elective three-staged esophagectomy with an uncomplicated recovery. Hetolerated diet on Postoperative Day 8 and was dischargedhome on Postoperative Day 10. Four months postsurgery,a repeat PET scan shows no evidence of disease recurrence.
On gross examination, a brown-tan lobulated tumor(4.5 cm) was noted in the distal esophagus. Histologicexamination revealed sheets of malignant cells displayingepitheloid and spindle cell morphology, interspersed withmelanin pigments; adjacent mucosa showed melanocyticproliferation with transepidermal migration (Fig. 3A).Tumor cells displayed vesicular chromatin, prominentnucleoli, and brisk mitotic activity (20e30/10 hpf). Immu-nostains were positive for S100, HMB45, and Melan-A,whereas cytokeratin markers were negative (Fig. 3B). Theright upper paratracheal lymph node was mostly replacedby metastatic melanoma.
3. Discussion
De la Pava et al3 first described the presence of melano-cytes at the interface between the epithelium and thelamina propria of the esophageal mucosa. Esophagealmelanosis, or melanocytosis, is a rare condition of benignmelanocytic proliferation found in 0.07e2.1% of gastros-copies4,5 and is believed to be a precursor of primaryesophageal melanoma.6 Esophageal melanocytosis is asso-ciated with chronic esophagitis, reactive epithelialchanges,4,5 LaugiereHunziker syndrome, and Addison’sdisease, and has been reported in patients with analmelanoma,5 esophageal squamous cell carcinoma in situ,and pulmonary adenocarcinoma.4
patient’s esophageal carcinoma with an enlarged right para-) a large (4.3 � 2.1 cm2), homogeneously enhanced lobulatede aortic arch, extending just distal to the carina, and (B) an(C and D) their corresponding PET images demonstrating FDG

Figure 3 Histopathological images of the esophageal tumor: (A) diffuse sheets of spindle and epitheloid melanocytic cells withbrisk mitoses and marked nuclear pleomorphism (400�) and (B) diffuse and strong HMB45 staining of melanoma cells.
238 Y. Sim et al.
Clinically, primary esophageal melanoma presents simi-larly to other esophageal malignancies. Endoscopically, itoften presents as a solitary polypoidal mass in the middle ordistal third of the esophagus, which may be pigmented ornonpigmented, although multiple lesions have been re-ported in 12% of cases.7 The challenge in clinching a histo-logical diagnosis arises when the biopsy specimen lacksmelanin granules,6 misguiding the diagnosis as epithelialcarcinomas, although the latter typically present in theproximal third of the esophagus. Likewise, the malignantcells in our patient displayed a diversemorphology,making itdifficult to be identified from the initial biopsy and requiringan en bloc resection to clinch the histological diagnosis.
Immunohistochemical staining of biopsy specimens withmelanocytic-specific markers such as HMB45 antibodiescan increase the accuracy of a pretreatment diagnosis;however, one may question the efficacy of such a routinescreening stain, given the rarity of primary esophagealmelanomas. On presentation, metastatic disease ispresent in approximately 50% of patients (31% hepatic, 29%mediastinal, 18% pulmonary, and 13% cerebral),7 witha mean survival rate of less than 5% at 5 years, a mediansurvival rate of 10 months, and a disease-related mortalityof 85%.2
The primary treatment is surgical excision with discre-tionary lymphadenectomy for operable melanomas, withtotal or near-total esophagectomy offering the best survivaloutcome (5 years vs. 9 months for local resection).2 There isa role for immunomodulatory therapy in patients withmetastatic disease and for palliative external beam radio-therapy in those with unresectable esophageal mela-nomas.8 Newer treatment modalities, such as intraluminalbrachytherapy and laser photoablation,9,10 have showngreat promise, but not without its potential toxicities, suchas esophagitis, ulcerations, strictures.
4. Conclusion
Primary melanoma of the esophagus is a rare condition thatmay pose diagnostic difficulty, especially if it is non-pigmented and lacks melanin granules in a biopsy
specimen. We propose that an esophageal melanoma beconsidered as a differential diagnosis if the tumor is poly-poidal. On diagnosis, one should rule out a primary mela-noma peripherally, lest the management strategy bealtered for a metastatic melanoma. Total or near-totalesophagectomy offers the best survival outcome, andnewer adjuvant therapies such as brachytherapy and pho-toablation show promising potential.
References
1. Garfinkle JM, Cahan WG. Primary melanocarcinoma of theesophagus. First histologically proven case. Cancer. 1952;5:921e926.
2. Sabanathan S, Eng J, Pradhan GN. Primary malignant mela-noma of the esophagus. Am J Gastroenterol. 1989;84:1475e1481.
3. De la Pava S, Nigogosyan G, Pickren JW, Cabrera A. Melanosisof the esophagus. Cancer. 1963;16:48e50.
4. Walter A, van Rees BP, Heijnen BH, van Lanschot JJ,Offerhaus GJ. Atypical melanocytic proliferation associatedwith squamous cell carcinoma in situ of the esophagus.Virchows Arch A Pathol Anat Histopathol. 2000;437:203e207.
5. Horowitz M, Nobrega MM. Primary anal melanoma associatedwith melanosis of the upper gastrointestinal tract. Endoscopy.1998;30:485e487.
6. Chang F, Deere H. Esophageal melanocytosis morphologicfeatures and review of the literature. Arch Pathol Lab Med.2006;130:552e557.
7. Chalkiadakis G, Wihlm JJM, Morand G, Weill-Bousson M,Witz JP. Primary malignant melanoma of the esophagus. AnnThorac Surg. 1985;39:472e475.
8. Fogarty GB, Tartaglia CJ, Peters LJ. Primary melanoma of theoesophagus well palliated by radiotherapy. Br J Radiol. 2004;77:1050e1052.
9. Tessa M, Rotta P, Ragona R, et al. Concomitant chemotherapyand external radiotherapy plus brachytherapy for locallyadvanced esophageal cancer: results of a retrospective multi-center study. Tumori. 2005;91:406e414.
10. Wayman J, Irving M, Russell N, Nicoll J, Raimes SA. Intraluminalradiotherapy and Nd:YAG laser photoablation for primarymalignant melanoma of the esophagus. Gastrointest Endosc.2004;59:927e929.