preventing and managing pressure injuries · preventing and managing pressure injuries. ... alissa...
TRANSCRIPT

Implementation of NSQHS - Standard 8:
Preventing and Managing Pressure Injuries
Tracy Nowicki & Cherie FranksClinical Nurse Consultant-
QuEST & Nursing Director Clinical Effectiveness
The Prince Charles Hospital
Acknowledgements TPCH Tissue Viability Committee members

Location and Services
Image courtesy of health.qld.gov.au
•Cardiac and thoracic medicine and surgery •Emergency medicine – adults and children •General medical and general surgical services •Orthopaedic joint surgery (elective) •Acute geriatrics and rehabilitative medicine •Children’s inpatient services •Comprehensive and integrated mental health service •Palliative care Image courtesy of baulderstone.com.au
1

Accreditation May 2013•
First Public Hospital in QLD to be assessed against all 10
of
the National Standards•
All Standards met
10 Met with Merits•
Medication-
1
•
Blood and blood products-
2•
Falls-
4
•
Pressure Injury-
3
Image Courtesy of TPCH Newsletter
2

• Implementing Standard 8 -Governance

Patient
4

Patient
Occupational Therapy
Physiotherapy
Nursing Services /
Community
Medicine / Surgery
Executive / Management /
Quality
Dieticians
Pharmacy
QuEST
Podiatry
Wound Management
Services
Patient
5
• Map out your evidence against the standards – and do this early
• Identify the evidence you have already
• What are you doing well?
• Where do you need to focus?
• Where are you gaps?
• What you need to do, by when and by whom?
6

TPCH Pressure Injury Prevalence Studies
260 261246
265
335366
349372
408 413
8762 55
3775 66
3054 51
30
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Am
ount
0
50
100
150
200
250
300
350
400
450
Prevalence 16.15% 14.18% 13.82% 7.27% 13.73% 12.02% 5.15% 10.75% 9.30% 6.00%
Hospital Acquired 13.73% 6.90% 11.79% 4.15% 10.45% 7.92% 4.20% 7.26% 7.40% 4.00%
PI on admission 2.41% 7.28% 2.03% 3.11% 3.48% 4.64% 1.40% 3.76% 2.00% 2.00%
Incident report 10.34% 17.74% 18.18% 35% 22% 44% 70% 67% 68% 83%
How many pt surveyed 260 261 246 265 335 366 349 372 408 413
Howmany PI 87 62 55 37 75 66 30 54 51 30
2002 2003 2005 2006 2008 2009 2010 Mar‐11 Nov‐11 2012
Percentage
7

8

9
Skin Inspection: It’s Important to Us!
• Measure problem• Audit• Improve• Educate• Make it sustainable• Reward• Evaluate
10
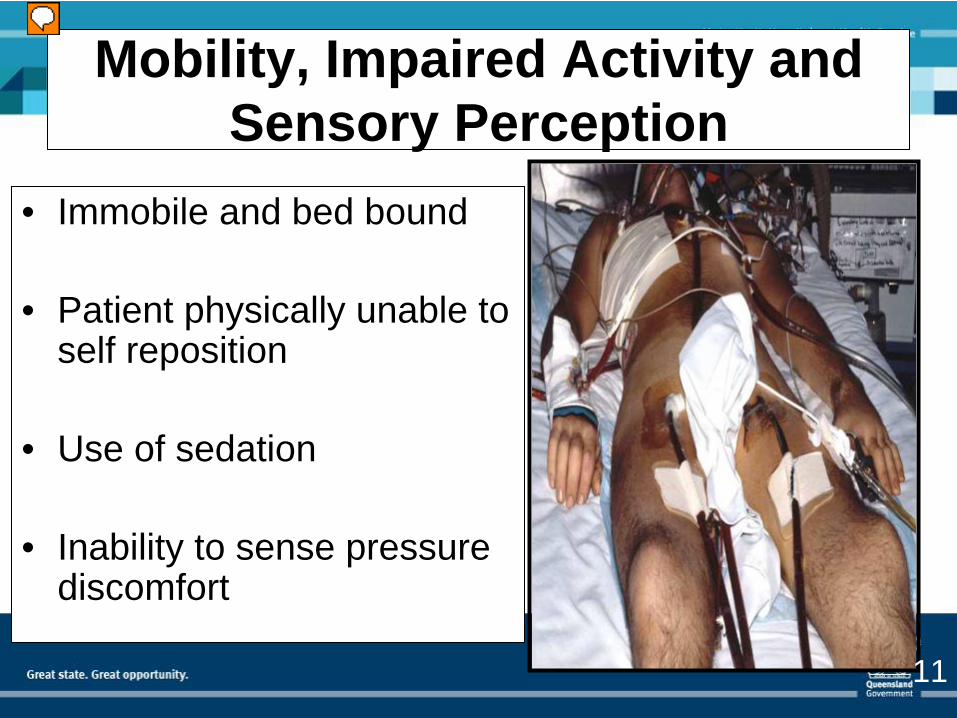
Mobility, Impaired Activity and Sensory Perception
• Immobile and bed bound
• Patient physically unable to self reposition
• Use of sedation
• Inability to sense pressure discomfort
11

12

Prevention: It’s Important to Us!
• Risk Screening: Waterlow & Glamorgan• Updated to now include new terminology • Time• Procedure expects risk assessment within 8
hours• Compliance: 84% (State: 77%)• Pre & post knowledge tests• Updated Management Plan• Procedure
13

• Increase in MST completion from 58 to 95% (n=304)• 2009 – moving MST to top increased completion 14%
State Leaders in Screening
14

Adjunct Devices for the Heels Prevention is important to us!
15

Prevention is important to us!
16
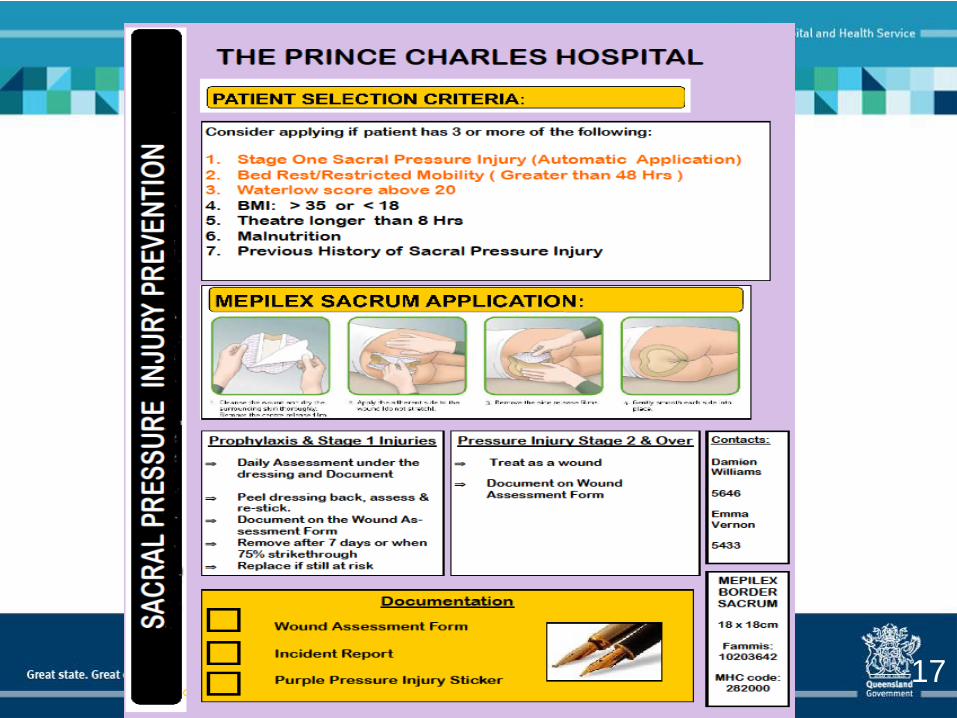
17

Standardisation of Skin Care
18

Simplifying Education & Measure
19

The Prince Charles Hospital Pressure Injury Prevention Action Plans 2010/2011
Programme: Nursing Director: Mary Wheeldon
Issue Action By Whom By When Outcomes
20

Treatment: It’s Important to Us
21
Incident Report Evaluation It’s Important to Us! Immediate response
22

Pressure Injury Prevention: Current Research
• Systematic review of interventions to reduce pressure injury in immobile critically ill patients.
Alissa Anderson, Paul Fulbrook
• Validity and reliability of four pressure injury risk assessment scales for use in intensive care.
Paul Fulbrook, Alissa Anderson
• Predictive validity of a new pressure injury risk assessment tool for critically ill patients.
Alissa Anderson, Paul Fulbrook
• Metro North survey of nurses’ knowledge of skin integrity and its management. Petra Lawrence, Paul Fulbrook, Sandra Miles, Cherie Franks & Debra Cutler
• Prevalence of pressure injury: a ten year analysis.Sandra Miles, Paul Fulbrook, Tracy Nowicki, Cherie Franks, Debra Cutler
23

Consumer Engagement: It’s Important to Us!
24

Anita Rush, ClinicalEquipment Specialist - Berkshire Equipment
Right Equipment………But Watch Out!
25

Lessons Learnt
• Cyclic process- Continuous quality improvement cycle• Keep all evidence: measure, measure, measure • Utilise resources wisely- use one tool and adapt• Identify key/ high use areas and focus energy/ time on these • Continue with gap analysis and action plans for each service line
and utilise unit champions• Develop relationships across all disciplines- its not just the Doctors
and Nurses!• Be passionate- its not about ticking as many boxes as possible• Strong leadership and Executive buy-in• Start planning early
26

Where to from here?
• Consumer engagement• Keeping action plans ACTIVE• Evaluate time on Waterlow• Skin Failure • Documentation• New Staging System• Heel Pressure Injuries• Continue to engage all disciplines• Research• Shear, pressure, moisture• Staff knowledge surveys• Mucosal, head, heel PIs
Keep the Wind in Your Sails!
27

Pressure Injury Prevention & Management is Important to ALL of
us
28

Cherie FranksNursing Director Clinical [email protected]
Tracy NowickiClinical Nurse [email protected]
29