vaccine administration: preventing serious shoulder injuries
TRANSCRIPT

J o u r n a l o f t h e A m e r i c a n P h a r m a c i s t s A s s o c i a t i o njapha.org102 JAPhA | 53:2 | MAr/APr 2013
Vaccine Update
Erroneous administration of intramuscular vaccines, particu-larly above the deltoid muscle, can result in serious shoulder injuries and diminished vaccine efficacy.1 With few studies published ad-dressing injection technique before 2002, inconsistencies arose regard-ing optimal vaccine administration, thus causing variations in current practice.2 We will examine cases of serious shoulder injuries as a result of incorrect technique and provide a step-by-step guide to the proper administration of intramuscular in-jections.
In 2006, Bodor and Montalvo3 reported two cases of vaccine-re-lated shoulder dysfunction. One patient received the 23-valent pneu-mococcal vaccine and the other an influenza vaccine. Both patients re-ported receiving injections high into the deltoid muscle, within 1 to 2 cm of the acromion. Both patients no-ticed severe shoulder pain and loss of range of motion within 2 days and increasing pain during a period of 2 to 5 months. One patient was diag-nosed with subacromial bursitis that later progressed to adhesive capsuli-tis or frozen shoulder; the other was diagnosed with bicipital tendonitis, subacromial bursitis, and a mild C6 sensory radiculopathy. The authors recommended that guidelines spec-ify avoiding vaccine injections in the upper third of the deltoid muscle. They recommended that health pro-fessionals consider vaccine-related shoulder dysfunction in patients presenting with shoulder pain and weakness following a vaccine injec-tion.
Atanasoff et al.4 reported a series of 13 cases submitted to the Vaccine Injury Compensation Program be-tween 2006 and 2010, in which pa-tients experienced shoulder injury related to vaccine administration. Of the cases, 62% received influenza
vaccine and the remainder received tetanus–diphtheria toxoids, Td–acellular pertussis, or human papil-lomavirus vaccine. The proposed mechanism of injury was that vac-cine, an antigenic substance, injected into synovial tissue resulted in an immune-mediated inflammatory re-sponse. Of patients, 46% stated that the vaccine was injected “too high” into the deltoid muscle. Magnetic resonance images revealed fluid col-lections in the deep deltoid or over-lying the rotator cuff tendons, bur-sitis, fluid buildup within the bursa, or rotator cuff tears. About one-third of patients (31%) required surgery, with one-half of those requiring a
Vaccine administration: preventing serious shoulder injuriesStephan Foster and McLisa V. davis
second surgical intervention. Many patients (69%) had residual symp-toms, and 31% experienced full re-covery. The authors proposed seat-ing both the injector and the patient to reduce the probability of injecting high into the deltoid muscle.
Injecting into the thickest, most central portion of the deltoid muscle is important in preventing these se-vere shoulder injuries. The injection must be administered into the mus-cle at a 90-degree angle to the skin. Health professionals need to remain knowledgeable about the anatomy of the shoulder (Figure 1) to avoid injecting too high. Further, review-ing current recommendations for in-tramuscular injections helps ensure that proper technique is used.
Recommendations for intra-muscular vaccine administration are as follows5–7:
Humerus
Deltoid muscle
Acromion Clavicle
Articular capsule
Subacromial bursa Supraspinatus muscle
and tendon
Synovial membrane
Figure 1. Cross-section of the shoulder joint
Send your immunization questions to the JAPhA Contributing Editors who coor-dinate the Vaccine Update column:
❚ Mary S. Hayney, PharmD, BCPS, Associate Professor of Pharmacy, School of Pharmacy, University of Wisconsin, Madison ([email protected])
❚ John D. Grabenstein, PhD, Director of Scientific Affairs, Merck Vaccine Division ([email protected])
This article is supported by a Cooperative Agreement provided by the Centers for Disease Control and Prevention (CDC) entitled “Pharmacists: Connecting, Communicating and Collaborating for Improved Community Health” (1U66 IP000114). The opinions expressed in this article do not represent the viewpoints of the CDC.
J o u r n a l o f t h e A m e r i c a n P h a r m a c i s t s A s s o c i a t i o n japha.org MAr/APr 2013 | 53:2 | JAPhA 103
Vaccine Update
Wash and dry hands thoroughly with bactericidal soap and water or use bactericidal hand sanitizer to pre-vent contamination of syringe or vac-cine. Gloves are optional. ❚ Verify the correct vaccine. Ex-
amine the vaccine solution for cloudiness or sedimentation and check the expiration date. Discard the solution and never administer to the patient if any of these changes are found or the vaccine is expired.
❚ Using aseptic technique, load dose into the syringe. Pick an ap-propriate needle size. Use a 1-in needle for most adult patients. For male patients weighing more than 118 kg or female patients more than 90 kg, use a 1.5-in needle. For adults weighing less than 60 kg, use a 0.625-in needle. (General rule: Women have more subcutaneous fat than men.8,9)
❚ Organize vaccine-filled syringe, alcohol swab, cotton ball, ban-dage, and biohazard sharps con-tainer near the patient.
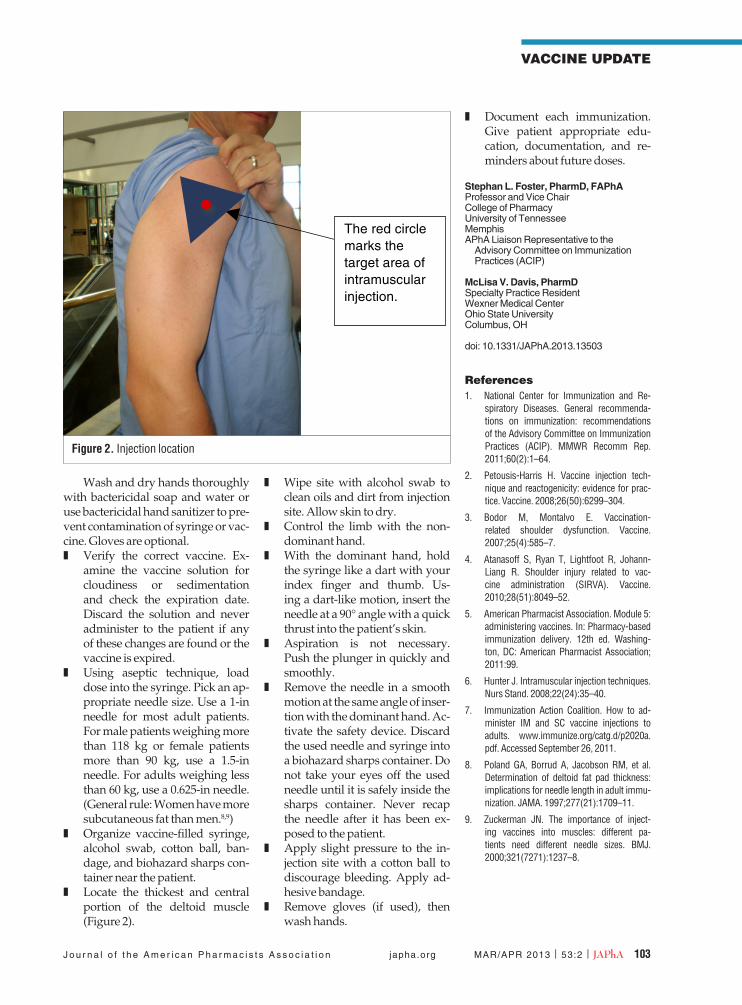
❚ Locate the thickest and central portion of the deltoid muscle (Figure 2).
❚ Wipe site with alcohol swab to clean oils and dirt from injection site. Allow skin to dry.
❚ Control the limb with the non-dominant hand.
❚ With the dominant hand, hold the syringe like a dart with your index finger and thumb. Us-ing a dart-like motion, insert the needle at a 90° angle with a quick thrust into the patient’s skin.
❚ Aspiration is not necessary. Push the plunger in quickly and smoothly.
❚ Remove the needle in a smooth motion at the same angle of inser-tion with the dominant hand. Ac-tivate the safety device. Discard the used needle and syringe into a biohazard sharps container. Do not take your eyes off the used needle until it is safely inside the sharps container. Never recap the needle after it has been ex-posed to the patient.
❚ Apply slight pressure to the in-jection site with a cotton ball to discourage bleeding. Apply ad-hesive bandage.
❚ Remove gloves (if used), then wash hands.
❚ Document each immunization. Give patient appropriate edu-cation, documentation, and re-minders about future doses.
Stephan L. Foster, PharmD, FAPhAProfessor and Vice ChairCollege of PharmacyUniversity of TennesseeMemphisAPhA Liaison representative to the Advisory Committee on Immunization Practices (ACIP)
McLisa V. Davis, PharmDSpecialty Practice residentWexner Medical CenterOhio State UniversityColumbus, OH
doi: 10.1331/JAPhA.2013.13503
References1. National Center for Immunization and Re-
spiratory Diseases. General recommenda-tions on immunization: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2011;60(2):1–64.
2. Petousis-Harris H. Vaccine injection tech-nique and reactogenicity: evidence for prac-tice. Vaccine. 2008;26(50):6299–304.
3. Bodor M, Montalvo E. Vaccination-related shoulder dysfunction. Vaccine. 2007;25(4):585–7.
4. Atanasoff S, Ryan T, Lightfoot R, Johann-Liang R. Shoulder injury related to vac-cine administration (SIRVA). Vaccine. 2010;28(51):8049–52.
5. American Pharmacist Association. Module 5: administering vaccines. In: Pharmacy-based immunization delivery. 12th ed. Washing-ton, DC: American Pharmacist Association; 2011:99.
6. Hunter J. Intramuscular injection techniques. Nurs Stand. 2008;22(24):35–40.
7. Immunization Action Coalition. How to ad-minister IM and SC vaccine injections to adults. www.immunize.org/catg.d/p2020a.pdf. Accessed September 26, 2011.
8. Poland GA, Borrud A, Jacobson RM, et al. Determination of deltoid fat pad thickness: implications for needle length in adult immu-nization. JAMA. 1997;277(21):1709–11.
9. Zuckerman JN. The importance of inject-ing vaccines into muscles: different pa-tients need different needle sizes. BMJ. 2000;321(7271):1237–8.
Figure 2. Injection location
The red circle marks the target area of intramuscular injection.