preventie(2.0(– wat(zijn(de( mogelijkheden? · preventie(2.0(– wat(zijn(de(mogelijkheden?...
TRANSCRIPT
Preventie 2.0 – Wat zijn de mogelijkheden?Sebastian Köhler, Ph.D.
NeuroepidemiologieAlzheimer Centrum Limburg
School for Mental Health and NeuroscienceMaastricht University
Themamiddag Deltaplan DementieAmersfoort 15-‐12-‐2016
Articles
790 www.thelancet.com/neurology Vol 13 August 2014
See Online for appendix
marginally higher than the 1·39 used previously.11 For depression, two recent meta-analyses provided somewhat lower estimates than the 1·90 used previously.12 In one meta-analysis13 the estimated combined RR was 1·66 (95% CI 1·29–2·24) based on data from four prospective cohort studies, whereas in the other14 it was 1·65 (1·42–1·92) based on data from 23 studies. The latter estimate was used because it was based on a more
comprehensive analysis. The appendix provides further details of revised estimates. The prevalence of each of the seven risk factors worldwide and in the USA, UK, and Europe were taken from various population-derived sources using the same age ranges as Barnes and Yaff e.8 Panel 1 describes the defi nitions used for each of the risk factors. The appendix lists sources for the RRs and prevalence rates used.
Statistical analysisAssuming there is a causal relation between a risk factor and a disease, the PAR is the proportion of cases of a disease in the population attributable to the risk factor. The PAR for each risk factor was calculated using Levin’s formula:16
where P is the population prevalence of the risk factor.This formula is intended for unadjusted estimates, but
since the RRs were obtained from multiple sources, other methods were not available. The combined estimate of the PAR used by Barnes and Yaff e8 assumed independence of risk factors:
PARcombined = 1 – Π 1 – PAR
The assumption of independence of risk factors is almost certainly biased, but was necessary because of an absence of other methods. To account for non - independence of the risk factors, a novel modi-fi cation of the formula was used, which involved weighting the PAR for each risk factor:
PARAdjustedCombined = 1 – Π 1 – (w × PAR)
where the weight w was computed using the estimate of 1 minus the proportion of the variance shared with the other risk factors (ie, communality).
The communality for each risk factor was estimated using data for adults aged 16 years and older from the Health Survey for England 2006,17 in which all seven risk factors were measured. The presence of each risk factor, ignoring the age ranges, was used to calculate the RRs. The communality was calculated via principal components analysis of the inter-risk-factor tetrachoric correlation matrix. Specifi cally, it was calculated as the square of the loadings on the fi rst two principal components since both had eigenvalues greater than one—the Kaiser criterion for selecting the number of components to extract.18 Together, the two principal components explained 50% of the total variance between the risk factors, which suggests substantial overlap. The communalities for each risk factor and self-reported risk factor prevalence from the Health Survey for England 2006 are given in table 1.
The total number of Alzheimer’s disease cases attributable to each risk factor was estimated by
PAR =P × (RR – 1)
1 + P × (RR – 1)
Prevalence* PAR (95% CI) Number of attributable cases in 2010 (95% CI)†
Worldwide
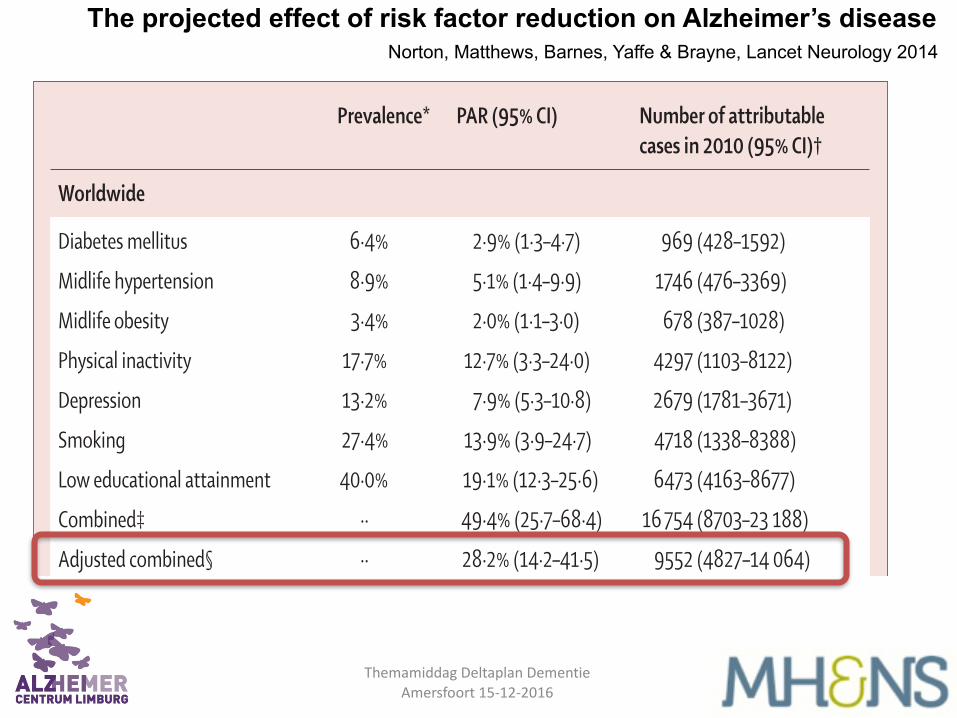
Diabetes mellitus 6·4% 2·9% (1·3–4·7) 969 (428–1592)
Midlife hypertension 8·9% 5·1% (1·4–9·9) 1746 (476–3369)
Midlife obesity 3·4% 2·0% (1·1–3·0) 678 (387–1028)
Physical inactivity 17·7% 12·7% (3·3–24·0) 4297 (1103–8122)
Depression 13·2% 7·9% (5·3–10·8) 2679 (1781–3671)
Smoking 27·4% 13·9% (3·9–24·7) 4718 (1338–8388)
Low educational attainment 40·0% 19·1% (12·3–25·6) 6473 (4163–8677)
Combined‡ ·· 49·4% (25·7–68·4) 16 754 (8703–23 188)
Adjusted combined§ ·· 28·2% (14·2–41·5) 9552 (4827–14 064)
USA
Diabetes mellitus 10·3% 4·5% (2·0–7·3) 240 (107–389)
Midlife hypertension 14·3% 8·0% (2·2–15·1) 425 (119–798)
Midlife obesity 13·1% 7·3% (4·3–10·8) 386 (226–570)
Physical inactivity 32·5% 21·0% (5·8–36·6) 1115 (308–1942)
Depression 19·2% 11·1% (7·5–15·0) 588 (395–796)
Smoking 20·6% 10·8% (3·0–19·8) 574 (159–1050)
Low educational attainment 13·3% 7·3% (4·4–10·3) 386 (236–544)
Combined‡ ·· 52·7% (25·9–72·8) 2796 (1374–3858)
Adjusted combined§ ·· 30·6% (14·5–45·3) 1622 (771–2401)
Europe
Diabetes mellitus 6·9% 3·1% (1·4–5·0) 222 (98–364)
Midlife hypertension 12·0% 6·8% (1·9–13·0) 492 (136–934)
Midlife obesity 7·2% 4·1% (2·4–6·2) 299 (172–448)
Physical inactivity 31·0% 20·3% (5·6–35·6) 1461 (401–2564)
Depression 18·5% 10·7% (7·2–14·5) 774 (520–1049)
Smoking 26·6% 13·6% (3·8–24·2) 978 (277–1745)
Low educational attainment 26·6% 13·6% (8·5–18·6) 978 (614–1342)
Combined‡ ·· 54·0% (27·2–73·7) 3891 (1959–5311)
Adjusted combined§ ·· 31·4% (15·3–46·0) 3033 (1472–4332)
UK
Diabetes mellitus 4·9% 1·9% (0·8–3·1) 14 (6–23)
Midlife hypertension 12·4% 7·0% (1·9–13·3) 53 (15–101)
Midlife obesity 11·8% 6·6% (3·9–9·8) 50 (29–74)
Physical inactivity 34·0% 21·8% (6·1–37·7) 166 (46–287)
Depression 13·9% 8·3% (5·5–11·3) 63 (42–86)
Smoking 20·0% 10·6% (2·9–19·4) 80 (22–147)
Low educational attainment 23·6% 12·2% (7·6–16·9) 93 (58–128)
Combined‡ ·· 52·0% (25·6–71·9) 395 (194–547)
Adjusted combined§ ·· 30·0% (14·3–44·4) 228 (109–338)
PAR=population-attributable risk. *Sources detailed in the appendix. †In thousands. ‡Assuming independence of the risk factors. §Adjusting for non-independence of the risk factors.
Table 2: Estimates for population-attributable risk and the number of attributable cases in 2010
Norton, Matthews, Barnes, Yaffe & Brayne, Lancet Neurology 2014The projected effect of risk factor reduction on Alzheimer’s disease
Themamiddag Deltaplan DementieAmersfoort 15-‐12-‐2016
Preventie: de on-mogelijkheden
• Leeftijd
• Geslacht
• Schoolopleiding
• Genetica
• Structurele hersenschade
Themamiddag Deltaplan DementieAmersfoort 15-‐12-‐2016
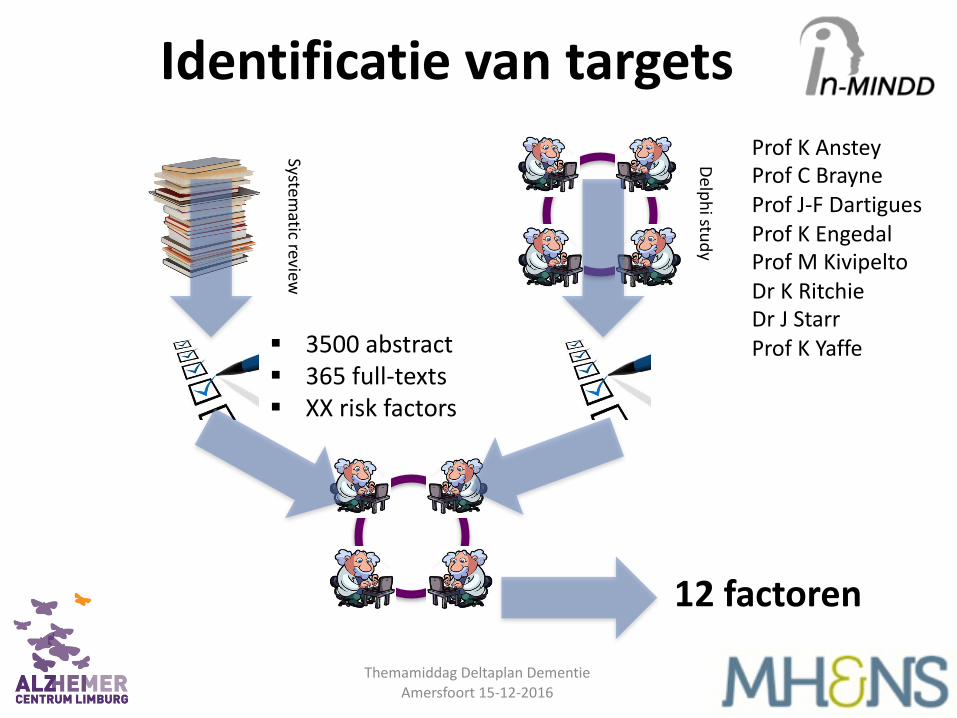
§ 3500 abstract§ 365 full-‐texts§ XX risk factors
12 factorenSystem
atic review
Delphi study
Prof K AnsteyProf C BrayneProf J-‐F DartiguesProf K EngedalProf M KivipeltoDr K RitchieDr J StarrProf K Yaffe
Themamiddag Deltaplan DementieAmersfoort 15-‐12-‐2016
Identificatie van targets
Themamiddag Deltaplan DementieAmersfoort 15-‐12-‐2016
Modificeerbare risicofactoren
Deckers et al., Int J Ger Psychiatry 2015
928 www.thelancet.com/neurology Vol 14 September 2015
Review
Forette et al (1998)21* Syst-Eur studyTzourio et al (2003)22† PROGRESS studyShumaker et al (2004)23 WHIMS study, oestrogen groupShumaker et al (2003)24 WHIMS study, oestrogen + progesterone groupViswanathan et al (2009)25 VISP study
Ball et al (2002)26 ACTIVE study
Thal et al (2005)27 Rofecoxib protocol 078
Petersen et al (2005)28‡ ADCS Donepezil and Vitamin E trial
Feldman et al (2007)29 InDDEx study
Oken et al (2006)30
Salloway et al (2004)31 Donepezil 401 study
Ford et al (2010)32
DeKosky et al (2008)33 GEM study
Tierney et al (2009)34
Lykestos et al (2007)35 ADAPT study
Peters et al (2008)36 HYVET-COG study
Winblad et al (2008)37 GAL-INT-11/18 studies
Vellas et al (2012)38 GuidAge study
McMahon et al (2006)39
Doody et al (2009)40
Launer et al (2011)41 ACCORD-MIND study
Eussen et al (2006)42
Muscari et al (2010)43§
Lautenschlager et al (2008)44 FABS study
Smith et al (2010)45 VITACOG study
van de Rest et al (2008)46
Yurko-Mauro et al (2010)47 MIDAS study
Dangour et al (2010)48 OPAL study
Smith et al (2009)49 IMPACT study
Klusmann et al (2010)50¶ BBF study
Kwok et al (2012)51
Mastroiacovo et al (2015)52 CoCoA study-cognitively healthy
Desideri et al (2012)53 CoCoA study-mild cognitive impairment
Lui-Ambrose et al (2010)54 Brain Power study
Ihle-Hanson et al (2014)55
Vidovich et al (2015)56 PACE study
Anderson-Hanley et al (2012)57 Cybercycle study
Hajjar et al (2012)58 AVEC study
Barnes et al (2013)59 MAX study
Lee et al (2014)60||
Diamond et al (2015)61
Ngandu et al (2015)62 FINGER study
Wolinsky et al (2013)63 Iowa Healthy and Active Minds study
Kwok et al (2013)64
Suzuki et al (2013)65§
Gomez-Isla et al (2008)66** TRIMCI study
Peters et al (2012)67**
Makizako et al (2012)68**
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 Positive Negative
Type of primary endpoint and end result
Study timeline
D
D
D
D
D
D
D
D
D
D
D
D
(D)
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
C
B
B
B
B
n=2418
n=6105
n=2947
n=4532
n=150
n=2832
n=1457
n=769
n=1018
n=135
n=270
n=299
n=3069
n=142
n=2528
n=3336
n=2048
n=2854
n=276
n=821
n=2977
n=195
n=120
n=170
n=271
n=302
n=485
n=867
n=487
n=259
n=429
n=90
n=90
n=155
n=195
n=160
n=79
n=53
n=126
n=460
n=90
n=1200
n=681
n=200
n=100
n=257n=232
n=50
DCB
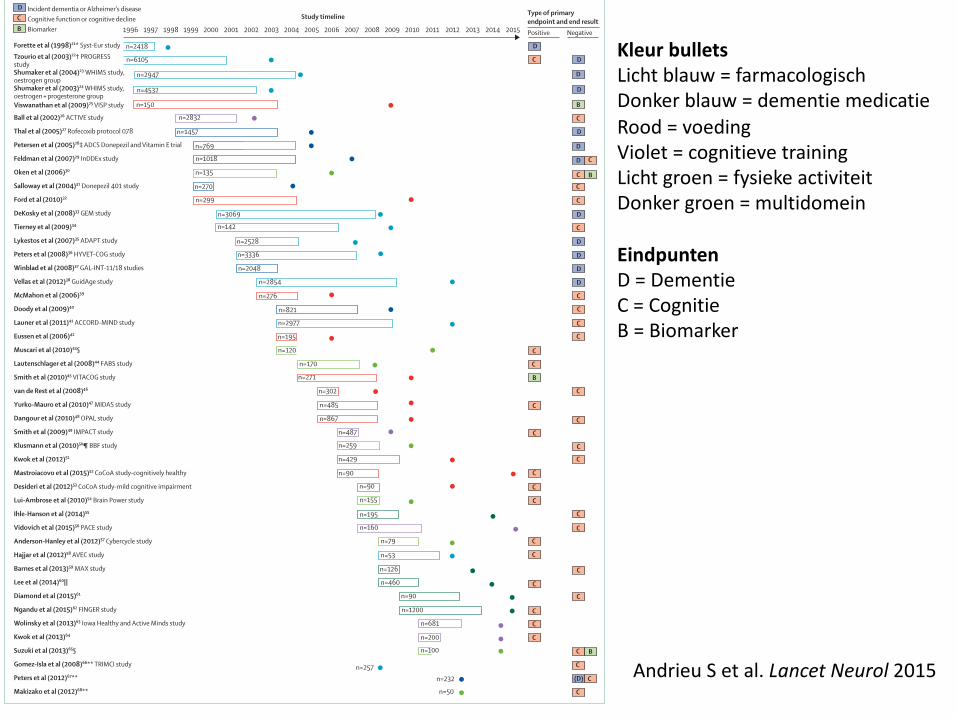
Incident dementia or Alzheimer’s diseaseCognitive function or cognitive declineBiomarker
Kleur bulletsLicht blauw = farmacologischDonker blauw = dementie medicatieRood = voedingViolet = cognitieve trainingLicht groen = fysieke activiteitDonker groen = multidomein
EindpuntenD = DementieC = CognitieB = Biomarker
Andrieu S et al. Lancet Neurol 2015
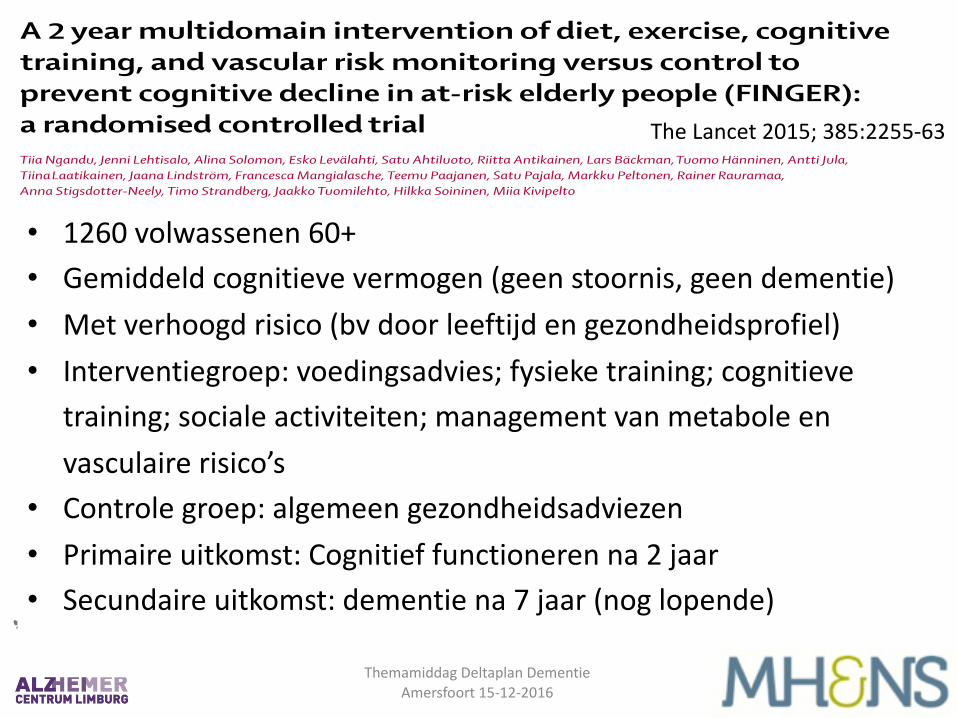
• 1260 volwassenen 60+• Gemiddeld cognitieve vermogen (geen stoornis, geen dementie)• Met verhoogd risico (bv door leeftijd en gezondheidsprofiel)• Interventiegroep: voedingsadvies; fysieke training; cognitieve
training; sociale activiteiten; management van metabole en vasculaire risico’s
• Controle groep: algemeen gezondheidsadviezen• Primaire uitkomst: Cognitief functioneren na 2 jaar• Secundaire uitkomst: dementie na 7 jaar (nog lopende)
Articles
www.thelancet.com Vol 385 June 6, 2015 2255
A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trialTiia Ngandu, Jenni Lehtisalo, Alina Solomon, Esko Levälahti, Satu Ahtiluoto, Riitta Antikainen, Lars Bäckman, Tuomo Hänninen, Antti Jula, Tiina Laatikainen, Jaana Lindström, Francesca Mangialasche, Teemu Paajanen, Satu Pajala, Markku Peltonen, Rainer Rauramaa, Anna Stigsdotter-Neely, Timo Strandberg, Jaakko Tuomilehto, Hilkka Soininen, Miia Kivipelto
SummaryBackground Modifi able vascular and lifestyle-related risk factors have been associated with dementia risk in observational studies. In the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER), a proof-of-concept randomised controlled trial, we aimed to assess a multidomain approach to prevent cognitive decline in at-risk elderly people from the general population.
Methods In a double-blind randomised controlled trial we enrolled individuals aged 60–77 years recruited from previous national surveys. Inclusion criteria were CAIDE (Cardiovascular Risk Factors, Aging and Dementia) Dementia Risk Score of at least 6 points and cognition at mean level or slightly lower than expected for age. We randomly assigned participants in a 1:1 ratio to a 2 year multidomain intervention (diet, exercise, cognitive training, vascular risk monitoring), or a control group (general health advice). Computer-generated allocation was done in blocks of four (two individuals randomly allocated to each group) at each site. Group allocation was not actively disclosed to participants and outcome assessors were masked to group allocation. The primary outcome was change in cognition as measured through comprehensive neuropsychological test battery (NTB) Z score. Analysis was by modifi ed intention to treat (all participants with at least one post-baseline observation). This trial is registered at ClinicalTrials.gov, number NCT01041989.
Findings Between Sept 7, 2009, and Nov 24, 2011, we screened 2654 individuals and randomly assigned 1260 to the intervention group (n=631) or control group (n=629). 591 (94%) participants in the intervention group and 599 (95%) in the control group had at least one post-baseline assessment and were included in the modifi ed intention-to-treat analysis. Estimated mean change in NTB total Z score at 2 years was 0·20 (SE 0·02, SD 0·51) in the intervention group and 0·16 (0·01, 0·51) in the control group. Between-group diff erence in the change of NTB total score per year was 0·022 (95% CI 0·002–0·042, p=0·030). 153 (12%) individuals dropped out overall. Adverse events occurred in 46 (7%) participants in the intervention group compared with six (1%) participants in the control group; the most common adverse event was musculoskeletal pain (32 [5%] individuals for intervention vs no individuals for control).
Interpretation Findings from this large, long-term, randomised controlled trial suggest that a multidomain intervention could improve or maintain cognitive functioning in at-risk elderly people from the general population.
Funding Academy of Finland, La Carita Foundation, Alzheimer Association, Alzheimer’s Research and Prevention Foundation, Juho Vainio Foundation, Novo Nordisk Foundation, Finnish Social Insurance Institution, Ministry of Education and Culture, Salama bint Hamdan Al Nahyan Foundation, Axa Research Fund, EVO funding for University Hospitals of Kuopio, Oulu, and Turku and for Seinäjoki Central Hospital and Oulu City Hospital, Swedish Research Council, Swedish Research Council for Health, Working Life and Welfare, and af Jochnick Foundation.
IntroductionLate-life cognitive impairment and dementia have become serious human, social, and economic burdens.1 WHO1 and the G8 Dementia Summit (2013)2 emphasised prevention as a key element to counteract the dementia epidemic. Findings from observational studies have linked several vascular and lifestyle-related risk factors with increased risk of late-life cognitive impairment and Alzheimer’s disease, the most common cause of dementia.3 A third of Alzheimer’s disease cases worldwide are estimated to be
attributable to seven modifi able factors (low education, midlife hypertension, midlife obesity, diabetes, physical inactivity, smoking, and depression), providing prevention opportunities.3 However, randomised controlled trials are desperately needed to confi rm these associations and investigate strategies to maintain cognitive functioning and prevent cognitive impairment.4,5
Previous single-domain prevention trials for cognitive impairment and dementia have yielded mainly negative results.4 Some positive associations with cognition were
Lancet 2015; 385: 2255–63
Published OnlineMarch 12, 2015http://dx.doi.org/10.1016/S0140-6736(15)60461-5
Chronic Disease Prevention Unit (T Ngandu PhD, J Lehtisalo MSc, E Levälahti MSc, S Ahtiluoto MD, Prof A Jula PhD, Prof T Laatikainen PhD, J Lindström PhD, Prof M Peltonen PhD, Prof J Tuomilehto PhD, Prof M Kivipelto PhD) and Welfare and Health Promotion Unit (S Pajala PhD), National Institute for Health and Welfare, Helsinki, Finland; Karolinska Institutet Center for Alzheimer Research, Stockholm, Sweden (T Ngandu, A Solomon PhD, Prof M Kivipelto); Institute of Clinical Medicine/Neurology (A Solomon, Prof H Soininen PhD, Prof M Kivipelto) and Institute of Public Health and Clinical Nutrition (Prof T Laatikainen), University of Eastern Finland, Kuopio, Finland; Aging Research Center, Karolinska Institutet-Stockholm University, Stockholm, Sweden (A Solomon, Prof L Bäckman PhD, F Mangialasche PhD, Prof M Kivipelto); Institute of Health Sciences/Geriatrics, University of Oulu and Oulu University Hospital, Oulu, Finland (Prof R Antikainen PhD, Prof T Strandberg PhD); Medical Research Center Oulu, Oulu University Hospital, Oulu, Finland (Prof R Antikainen); Oulu City Hospital, Oulu, Finland (Prof R Antikainen); Department of Neurology (T Hänninen PhD, Prof H Soininen) and Department of Clinical Physiology and Nuclear Medicine
The Lancet 2015; 385:2255-‐63
Themamiddag Deltaplan DementieAmersfoort 15-‐12-‐2016
Articles
2260 www.thelancet.com Vol 385 June 6, 2015
data in the study. The report was approved for submission by all authors. The corresponding author had fi nal responsibility for the decision to submit for publication.
ResultsBetween Sept 7, 2009, and Nov 24, 2011, 2654 individuals were screened and 1260 were randomly assigned to the intensive intervention group (n=631) or control group (n=629; fi gure 1). 1168 (93%) participants completed the 12 month assessments, and 1105 (88%) participants
completed the 24 month assessments. 16 individuals who withdrew from the study came to the fi nal cognitive evaluation. The intervention was completed in February, 2014. The mITT analyses included 1190 participants (94% of all enrolled participants). Dropout rates were similar in the intervention (87 [14%] participants) and control (66 [11%] participants) groups (p=0·07). The main reasons for dropout were health-related (56 [37%] participants), lack of time or motivation (22 [14%]), and diffi culties in arranging participation (18 [12%]). Ten individuals died during the study.
Baseline characteristics have previously been described in detail.15 The intervention and control groups were similar at baseline (table 1; baseline characteristics for intention-to-treat population are provided in the appendix). The mean age of the population was 69·3 years (SD 4·7), education 10·0 years (SD 3·4), and mini mental state examination score 26·8 points (SD 2·0). Mean cognitive performance was less than 0·5 SD below the average level for the cognitively normal Finnish pop ulation.15 Several vascular and lifestyle risk factors were present.
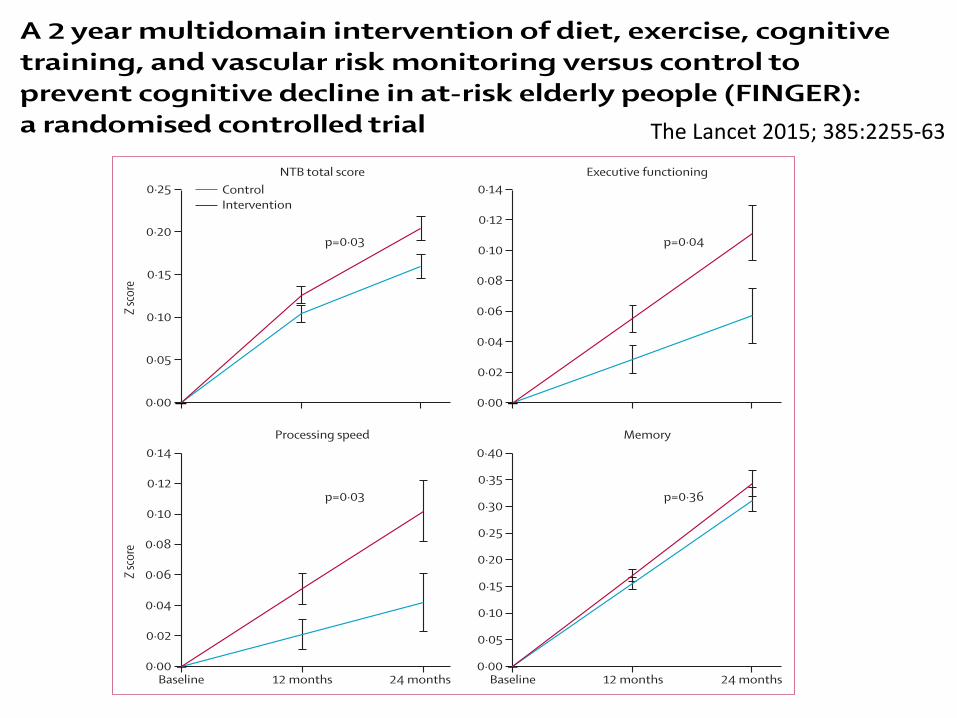
We noted a signifi cant benefi cial eff ect of the intervention for the primary outcome (fi gure 2, appendix). Estimated mean change in NTB total Z score at 2 years was 0·20 (SE 0·01, SD 0·51) in the intervention group and 0·16 (0·01, 0·51) in the control group. The mean diff erence between groups (group × time interaction) in change of NTB total score per year was 0·022 (95%CI 0·002–0·042, p=0·030). Improvement in NTB total score after 24 months was 25% higher in the intervention group than in the control group. The results remained unchanged in sensi tivity analyses, including intention-to-treat analyses (appendix).
We also noted a signifi cant intervention eff ect for the secondary cognitive outcomes of executive functioning (p=0·039) and processing speed (p=0·029; fi gure 2, appendix). Improvement in executive functioning was 83% higher, and in processing speed 150% higher, in the intervention group than in the control group. The intervention was not associated with signifi cant change in the prespecifi ed memory domain.
Post-hoc abbreviated memory score analyses showed a signifi cant between-group diff erence (p=0·036; appendix). NTB total score fell in 307 (28%) participants between the assessments at baseline and 24 months. Risk of cognitive decline was increased in the control group compared with intervention group for NTB total score (odds ratio 1·31, 95% CI 1·01–1·71), executive functioning, and processing speed (table 2).
We also noted signifi cant intervention eff ects after 2 years for other secondary outcomes such as BMI, dietary habits, and physical activity (appendix).
Self-reported adherence (any vs no participation) to intervention domains was high: nutrition, 579 (100%) participants; physical exercise, 523 (90%) participants;
See Online for appendix
Figure 2: Change in cognitive performance during the 2 year interventionFigure shows estimated mean change in cognitive performance from baseline until 12 and 24 months (higher scores suggest better performance) in the modifi ed intention-to-treat population. Error bars are SEs. Mixed-model repeated-measures analyses were used to assess between-group diff erences (group × time interaction) in changes from baseline to 24 months based on data from all participants with at least one post-baseline measurement. NTB=neuropsychiatric test battery.
Baseline 12 months 24 months0·00
0·02
0·04
0·06
0·10
0·14
0·12
0·08
0·00
0·02
0·04
0·06
0·10
0·14
0·12
0·08
Z sco
re
Baseline 12 months 24 months0·00
0·05
0·10
0·20
0·30
0·40
0·35
0·25
0·15
0·00
0·05
0·10
0·15
0·20
0·25
Z sco
re
ControlIntervention
NTB total score Executive functioning
Processing speed Memory
p=0·03 p=0·04
p=0·03 p=0·36
Odds ratio (95% CI) p value
Intervention (n=554) Control (n=565)
Overall cognitive decline
NTB total score 1 (reference) 1·31 (1·01–1·71) 0·04
Cognitive decline per domain
NTB memory score 1 (reference) 1·23 (0·95–1·60) 0·12
NTB executive functioning score 1 (reference) 1·29 (1·02–1·64) 0·04
NTB processing speed score 1 (reference) 1·35 (1·06–1·71) 0·01
In post-hoc analyses, we defi ned cognitive decline as decrease in NTB total score (overall decline) and NTB domain scores (decline per domain) between the assessments at baseline and at 24 months. Logistic regression analyses were used to assess risk of cognitive decline in the control group compared with the intervention group. Analyses are based on all participants with data available at both baseline and 24 months. NTB=neuropsychological test battery.
Table 2: Risk of cognitive decline from baseline to 24 months
Articles
www.thelancet.com Vol 385 June 6, 2015 2255
A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trialTiia Ngandu, Jenni Lehtisalo, Alina Solomon, Esko Levälahti, Satu Ahtiluoto, Riitta Antikainen, Lars Bäckman, Tuomo Hänninen, Antti Jula, Tiina Laatikainen, Jaana Lindström, Francesca Mangialasche, Teemu Paajanen, Satu Pajala, Markku Peltonen, Rainer Rauramaa, Anna Stigsdotter-Neely, Timo Strandberg, Jaakko Tuomilehto, Hilkka Soininen, Miia Kivipelto
SummaryBackground Modifi able vascular and lifestyle-related risk factors have been associated with dementia risk in observational studies. In the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER), a proof-of-concept randomised controlled trial, we aimed to assess a multidomain approach to prevent cognitive decline in at-risk elderly people from the general population.
Methods In a double-blind randomised controlled trial we enrolled individuals aged 60–77 years recruited from previous national surveys. Inclusion criteria were CAIDE (Cardiovascular Risk Factors, Aging and Dementia) Dementia Risk Score of at least 6 points and cognition at mean level or slightly lower than expected for age. We randomly assigned participants in a 1:1 ratio to a 2 year multidomain intervention (diet, exercise, cognitive training, vascular risk monitoring), or a control group (general health advice). Computer-generated allocation was done in blocks of four (two individuals randomly allocated to each group) at each site. Group allocation was not actively disclosed to participants and outcome assessors were masked to group allocation. The primary outcome was change in cognition as measured through comprehensive neuropsychological test battery (NTB) Z score. Analysis was by modifi ed intention to treat (all participants with at least one post-baseline observation). This trial is registered at ClinicalTrials.gov, number NCT01041989.
Findings Between Sept 7, 2009, and Nov 24, 2011, we screened 2654 individuals and randomly assigned 1260 to the intervention group (n=631) or control group (n=629). 591 (94%) participants in the intervention group and 599 (95%) in the control group had at least one post-baseline assessment and were included in the modifi ed intention-to-treat analysis. Estimated mean change in NTB total Z score at 2 years was 0·20 (SE 0·02, SD 0·51) in the intervention group and 0·16 (0·01, 0·51) in the control group. Between-group diff erence in the change of NTB total score per year was 0·022 (95% CI 0·002–0·042, p=0·030). 153 (12%) individuals dropped out overall. Adverse events occurred in 46 (7%) participants in the intervention group compared with six (1%) participants in the control group; the most common adverse event was musculoskeletal pain (32 [5%] individuals for intervention vs no individuals for control).
Interpretation Findings from this large, long-term, randomised controlled trial suggest that a multidomain intervention could improve or maintain cognitive functioning in at-risk elderly people from the general population.
Funding Academy of Finland, La Carita Foundation, Alzheimer Association, Alzheimer’s Research and Prevention Foundation, Juho Vainio Foundation, Novo Nordisk Foundation, Finnish Social Insurance Institution, Ministry of Education and Culture, Salama bint Hamdan Al Nahyan Foundation, Axa Research Fund, EVO funding for University Hospitals of Kuopio, Oulu, and Turku and for Seinäjoki Central Hospital and Oulu City Hospital, Swedish Research Council, Swedish Research Council for Health, Working Life and Welfare, and af Jochnick Foundation.
IntroductionLate-life cognitive impairment and dementia have become serious human, social, and economic burdens.1 WHO1 and the G8 Dementia Summit (2013)2 emphasised prevention as a key element to counteract the dementia epidemic. Findings from observational studies have linked several vascular and lifestyle-related risk factors with increased risk of late-life cognitive impairment and Alzheimer’s disease, the most common cause of dementia.3 A third of Alzheimer’s disease cases worldwide are estimated to be
attributable to seven modifi able factors (low education, midlife hypertension, midlife obesity, diabetes, physical inactivity, smoking, and depression), providing prevention opportunities.3 However, randomised controlled trials are desperately needed to confi rm these associations and investigate strategies to maintain cognitive functioning and prevent cognitive impairment.4,5
Previous single-domain prevention trials for cognitive impairment and dementia have yielded mainly negative results.4 Some positive associations with cognition were
Lancet 2015; 385: 2255–63
Published OnlineMarch 12, 2015http://dx.doi.org/10.1016/S0140-6736(15)60461-5
Chronic Disease Prevention Unit (T Ngandu PhD, J Lehtisalo MSc, E Levälahti MSc, S Ahtiluoto MD, Prof A Jula PhD, Prof T Laatikainen PhD, J Lindström PhD, Prof M Peltonen PhD, Prof J Tuomilehto PhD, Prof M Kivipelto PhD) and Welfare and Health Promotion Unit (S Pajala PhD), National Institute for Health and Welfare, Helsinki, Finland; Karolinska Institutet Center for Alzheimer Research, Stockholm, Sweden (T Ngandu, A Solomon PhD, Prof M Kivipelto); Institute of Clinical Medicine/Neurology (A Solomon, Prof H Soininen PhD, Prof M Kivipelto) and Institute of Public Health and Clinical Nutrition (Prof T Laatikainen), University of Eastern Finland, Kuopio, Finland; Aging Research Center, Karolinska Institutet-Stockholm University, Stockholm, Sweden (A Solomon, Prof L Bäckman PhD, F Mangialasche PhD, Prof M Kivipelto); Institute of Health Sciences/Geriatrics, University of Oulu and Oulu University Hospital, Oulu, Finland (Prof R Antikainen PhD, Prof T Strandberg PhD); Medical Research Center Oulu, Oulu University Hospital, Oulu, Finland (Prof R Antikainen); Oulu City Hospital, Oulu, Finland (Prof R Antikainen); Department of Neurology (T Hänninen PhD, Prof H Soininen) and Department of Clinical Physiology and Nuclear Medicine
The Lancet 2015; 385:2255-‐63
Themamiddag Deltaplan DementieAmersfoort 15-‐12-‐2016
The Lancet 2016; 388:797-‐805
• 3526 ouderen 70 t/m 78 jaar (gem 74.5)• Gerecruteerd via 118 huisartspraktijken• Interventiegroep: 6 jaar, 3x per jaar gezonheidscheck (door
verpleegkundige), individueel leefstijladvies, starten zorg zonodig• Controle groep: standaard zorg door huisarts• Primaire uitkomst: Incidente dementie na mediaan 6.7 jaar
Themamiddag Deltaplan DementieAmersfoort 15-‐12-‐2016
The Lancet 2016; 388:797-‐805
Articles
802 www.thelancet.com Vol 388 August 20, 2016
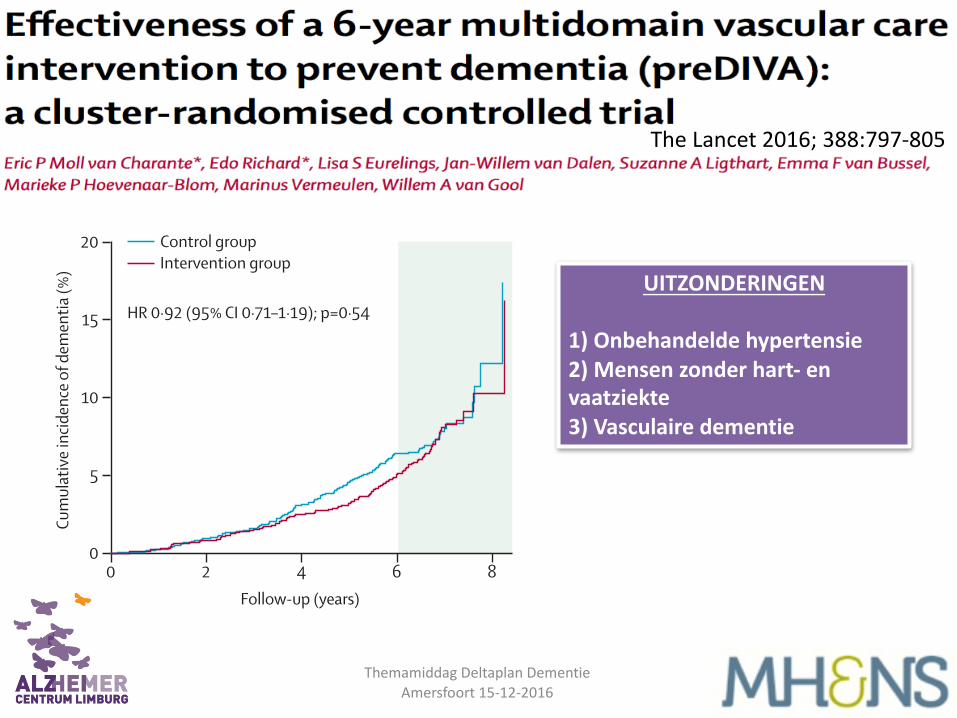
In participants with untreated hypertension who were adherent to the intervention, dementia occurred in 22 (4%) of 512 in the intervention group compared with 35 (7%) of 471 in the control group (HR 0∙54, 95% CI 0∙32–0∙92; p=0∙02; appendix). In participants with a history free from cardiovascular disease who were adherent to the intervention, dementia occurred in 45 (5%) of participants in the intervention group and in 69 (7%) of 934 participants in the control group (HR 0·64, 95% CI 0·44–0·94; p=0·02; appendix).
Disability did not diff er between groups, with ALDS scores at 6 years of 85∙7 in both study groups (adjusted mean diff erence –0∙02, 95% CI –0∙38 to 0∙42; p=0∙93;
table 3). 309 (16%) of 1885 participants died in the intervention group, compared with 269 (16%) of 1634 participants in the control group (HR 0∙98, 95% CI 0∙80–1∙18; p=0∙81; table 2). Cardiovascular disease events occurred in 273 (19%) of 1469 participants in the intervention group and 228 (17%) of 1307 participants in the control group (HR 1∙06, 95% CI 0∙86–1∙31; p=0∙57; table 2).
Cognition and the number of depressive symptoms did not diff er between both groups (table 3). Systolic blood pressure decreased more in the intervention group than in the control group (adjusted mean diff erence –2∙06 mm Hg, 95% CI –3∙21 to –0∙90; p=0∙0005). BMI, total cholesterol, and LDL cholesterol decreased in both groups, but diff erences were not signifi cant (appendix).
Antihypertensive medication was started in 329 (58%) of 568 participants in the intervention group and 231 (48%) of 479 in the control group, irrespective of baseline blood pressure (odds ratio [OR] 1∙48, 95% CI 1∙16–1∙89; p=0∙002). In participants with hypertension who were not using antihypertensive drugs at baseline, these proportions were 295 (67%) of 439 in the intervention group compared with 203 (56%) of 364 in the control group (OR 1∙62, 95% CI 1∙22–2∙17; p=0∙001). These medication changes were associated with substantial eff ects on blood pressure in both the intervention and control groups (appendix). Changes in other medication and lifestyle variables are given in the appendix.
There was no excess mortality in either group. The median number of hospital admissions per 1000 participants per year was 117 in the intervention group and 108 in the control group (adjusted mean diff erence –3, 95% CI –24 to 18; p=0∙78). There were no signifi cant diff erences between groups in frequencies of serious adverse events for hypotension, syncope, electrolyte abnormalities, injurious falls, or acute kidney injury or failure (appendix).
DiscussionIn this randomised controlled trial, we recorded no eff ect of 6∙7 years of nurse-led intensive vascular care on incident all-cause dementia. We also observed no eff ect on mortality, cardiovascular disease, or disability, despite a greater improvement in systolic blood pressure in the intervention group compared with the control group.
There are several possible explanations for this fi nding. First, the contrast between study groups in cardiovascular risk reduction was relatively small. As a result of the pragmatic nature of the study, the intensity of the vascular care that was delivered might have been insuffi cient to induce relevant eff ects on lifestyle change. Moreover, in primary care settings already providing high standards of cardiovascular risk management, it might be diffi cult to improve overall effi cacy, especially for secondary cardiovascular prevention. This theory is supported by subgroup analyses showing the strongest eff ects of the intervention in participants with
Figure 2: Kaplan-Meier plot of cumulative incidence of dementiaTo allow participants recruited early into the trial to continue follow-up until the 6-year assessment of the last participant was completed, the study was extended for participants randomised early (ie, in 2006–07). The hazard ratio (HR) refers to an analysis including all participants, up to 8 years of follow-up. The period beyond the planned 6-year follow-up, concerning few participants, is shaded.
Number at riskControl group
Intervention group
0
16011853
2
15401785
4
14371674
6
11301290
8
2832
Follow-up (years)
HR 0·92 (95% CI 0·71–1·19); p=0·54
0
5
10
15
20
Cum
ulat
ive i
ncid
ence
of d
emen
tia (%
)
Control groupIntervention group
Intervention Control Hazard ratio (95% CI) p value
All-cause dementia 121/1853 (7%) 112/1601 (7%) 0·92 (0·71–1·19) 0·54
Alzheimer’s disease* 99/1831 (5%) 81/1570 (5%) 1·05 (0·78–1·41) 0·74
Non-Alzheimer’s dementia*† 11/1743 (1%) 23/1512 (2%) 0·37 (0·18–0·76) 0·007
Unspecifi ed types of dementia* 11/1743 (1%) 8/1497 (1%) 1·24 (0·46–3·41) 0·67
Cardiovascular events‡ 273/1469 (19%) 228/1307 (17%) 1·06 (0·86–1·31) 0·57
Myocardial infarction 68/1503 (5%) 57/1339 (4%) 1·03 (0·71–1·49) 0·87
Stroke including TIA 120/1503 (8%) 102/1341 (8%) 1·05 (0·80–1·38) 0·74
Other§ 103/1495 (7%) 83/1333 (6%) 1·08 (0·78–1·50) 0·65
Death 309/1885 (16%) 269/1634 (16%) 0·98 (0·80–1·18) 0·81
Cardiovascular death¶ 63/1639 (4%) 60/1425 (4%) 0·91 (0·63–1·32) 0·63
Other¶ 126/1702 (7%) 125/1490 (8%) 0·87 (0·68–1·12) 0·28
Data are n (%), unless otherwise indicated. Further details are given in the appendix. TIA=transient ischaemic attack. *Participants with a dementia subtype other than the one being analysed were left out of the denominator. †Non-Alzheimer’s dementia includes vascular dementia (seven in the intervention group vs 12 in the control group); Lewy body dementia (two vs six); Parkinson’s dementia (two vs two); frontotemporal dementia (none vs one); primary progressive aphasia (none vs one); and other (none vs one). ‡Including fatal and non-fatal myocardial infarction and stroke, and angina pectoris, TIA, and peripheral arterial disease. §Angina pectoris and peripheral arterial disease. ¶The cause of death was unknown for 120 participants in the intervention group and 84 in the control group; therefore, numbers of cardiovascular and other causes of death do not add up to the total number of deaths.
Table 2: Clinical outcomes
UITZONDERINGEN
1) Onbehandelde hypertensie2) Mensen zonder hart-‐ envaatziekte3) Vasculaire dementie
Attitudes to dementia Findings from the 2015 British Social Attitudes survey
Attitudes to dementia Findings from the 2015 British Social Attitudes survey
British Social Attitudes | Attitudes to dementia
NatCen Social Research 2
Summary This paper presents findings on attitudes to dementia in Britain. While the majority of people have known someone with dementia and knowledge of the symptoms of dementia is high, there are clear gaps in public knowledge of the risk factors. There is also evidence of stigmatising attitudes towards people living with dementia.
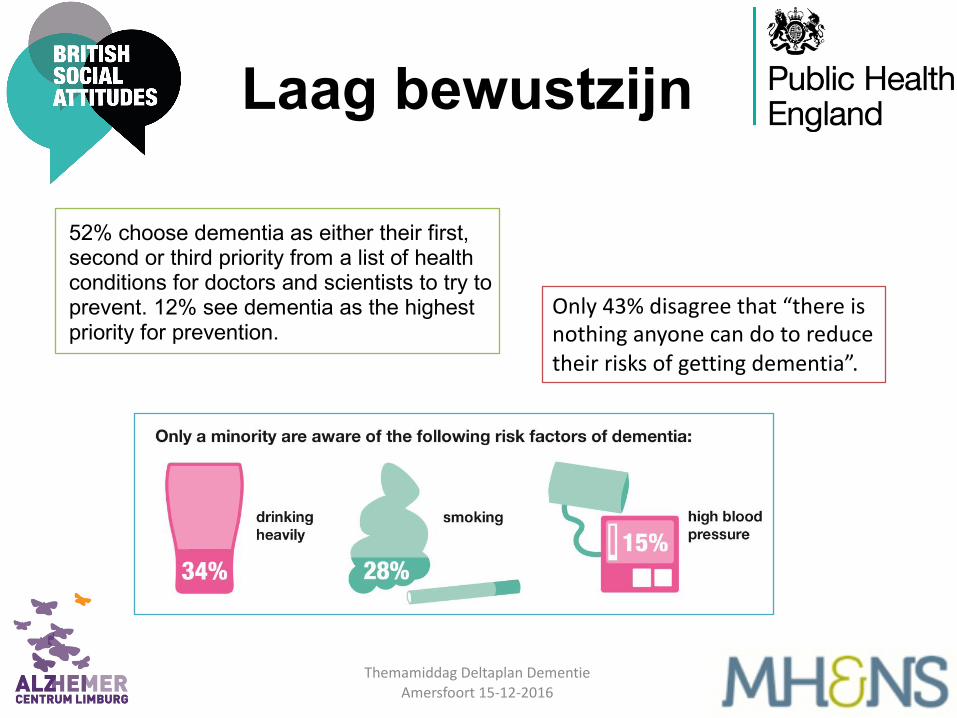
52% choose dementia as either their first, second or third priority from a list of health conditions for doctors and scientists to try to prevent. 12% see dementia as the highest priority for prevention.
Public knowledge of risk factors for dementia is considerably lower than knowledge of symptoms of dementia. 21% fail to identify any of seven risk factors correctly, while 43% identify just one or two risk factors.
Around half of people agree that “people with dementia can enjoy life to the full” (52%) and disagree that “I would find it hard to talk to someone with dementia” (57%). A substantial majority hold relatively negative views about caring for someone with dementia. Only 39% agree that “caring for someone with dementia is often very rewarding” and as many as 71% agree that “caring for someone with dementia often means that your own health suffers”.
British Social Attitudes | Attitudes to dementia
NatCen Social Research 2
Summary This paper presents findings on attitudes to dementia in Britain. While the majority of people have known someone with dementia and knowledge of the symptoms of dementia is high, there are clear gaps in public knowledge of the risk factors. There is also evidence of stigmatising attitudes towards people living with dementia.
52% choose dementia as either their first, second or third priority from a list of health conditions for doctors and scientists to try to prevent. 12% see dementia as the highest priority for prevention.
Public knowledge of risk factors for dementia is considerably lower than knowledge of symptoms of dementia. 21% fail to identify any of seven risk factors correctly, while 43% identify just one or two risk factors.
Around half of people agree that “people with dementia can enjoy life to the full” (52%) and disagree that “I would find it hard to talk to someone with dementia” (57%). A substantial majority hold relatively negative views about caring for someone with dementia. Only 39% agree that “caring for someone with dementia is often very rewarding” and as many as 71% agree that “caring for someone with dementia often means that your own health suffers”.
Laag bewustzijn
Only 43% disagree that “there is nothing anyone can do to reduce their risks of getting dementia”.
Themamiddag Deltaplan DementieAmersfoort 15-‐12-‐2016
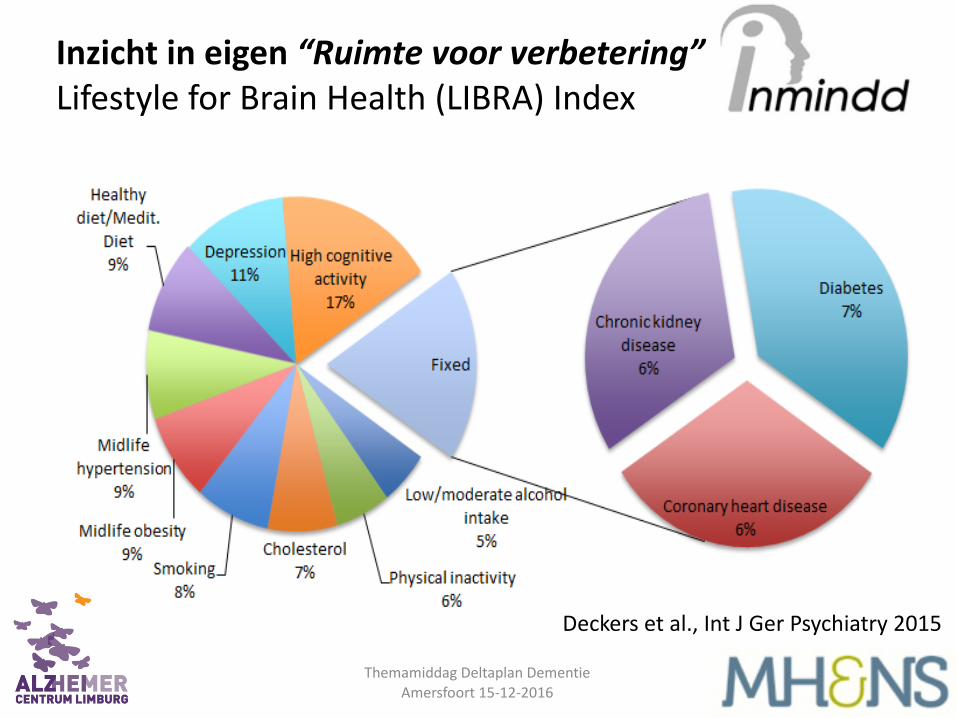
Deckers et al., Int J Ger Psychiatry 2015
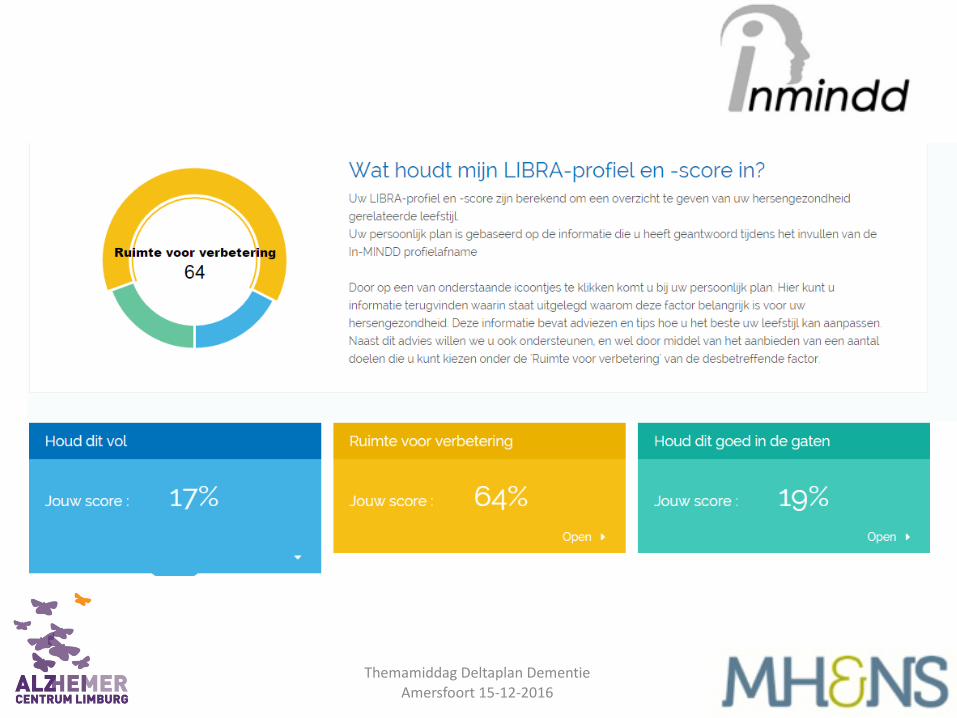
Inzicht in eigen “Ruimte voor verbetering”Lifestyle for Brain Health (LIBRA) Index
Themamiddag Deltaplan DementieAmersfoort 15-‐12-‐2016

Van observatie naar implementatie
Doetinchem Cohort Studie
Themamiddag Deltaplan DementieAmersfoort 15-‐12-‐2016
In-‐MINDD haalbaarheids studie• Randomized controlled trial•• Huisartsenpraktijken• 451 deelnemers 40 t/m 60 jaar• Minimaal één LIBRA risicofactor volgens HA• Interventiegroep: inzicht persoonlijk LIBRA-‐profiel,
gesprek met HA, toegang tot online ondersteuningspagina met informatie en leefstijladviezen
• Controle groep: algemeen gezondheidsadvies• Primaire uitkomst: reductie LIBRA score na 6 maanden
Themamiddag Deltaplan DementieAmersfoort 15-‐12-‐2016
www.inmindd.eu
Themamiddag Deltaplan DementieAmersfoort 15-‐12-‐2016


Implementatie project:MijnBreincoach• Een bewustwordingscampagne om hersengezondheidop de agenda te zetten in Limburg
• Om mensen daadwerkelijk te helpen in het dagelijks leven bij de uitvoer van een persoonlijk preventief actieplan gericht op reductie van het risico op dementie
• Met behulp van de applicatie Mijn Breincoach• Samen met de GGDs in Limburg
18Themamiddag Deltaplan Dementie
Amersfoort 15-‐12-‐2016
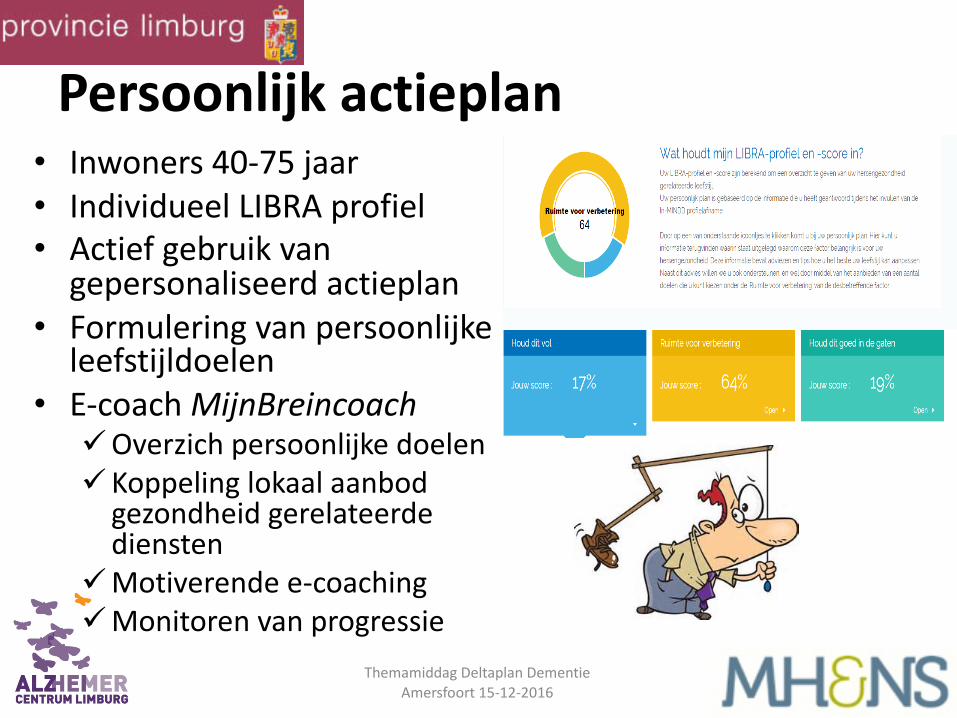
Persoonlijk actieplan• Inwoners 40-‐75 jaar• Individueel LIBRA profiel• Actief gebruik van gepersonaliseerd actieplan
• Formulering van persoonlijke leefstijldoelen
• E-‐coach MijnBreincoachüOverzich persoonlijke doelenüKoppeling lokaal aanbod gezondheid gerelateerde diensten
üMotiverende e-‐coachingüMonitoren van progressie
19Themamiddag Deltaplan Dementie
Amersfoort 15-‐12-‐2016
Ø Preventie heeft al per ongeluk plaatsgevonden!ØMogelijk meer winst te halen door gerichte actiesØWat goed is voor het hart is goed voor het breinØ Bewustzijn nu nog laag in bevolkingØMeest effectief
ü Indien vroeg begin (bv middelbare leeftijd)ü Als er individueel ruimte voor verbetering isü Door meerdere factoren te behandelenü Indien targets relevant en haalbaar zijn voor
de persoonü Indien mensen actief gecoached worden in
behalen van eigen leefstijl doelen (b.v. in persona, eHealth)Themamiddag Deltaplan Dementie
Amersfoort 15-‐12-‐2016
Take home messages
