prevalence of cervical spinal injury in trauma · social, and economic...
TRANSCRIPT
Neurosurg. Focus / Volume 25 / November 2008
Neurosurg Focus 25 (5):E10, 2008
1
Quadriplegia due to spinal cord injury is a dev-astating consequence of trauma to the cervical spine, involving numerous functional, psycho-
social, and economic ramifications.7,12,13,24,25,27–29,45,
49,61 Identification of unstable CSI is therefore an essential aspect of the trauma evaluation in preventing subsequent neurological damage.6,22,71,72,75,76 This task is especially difficult in patients who are not clinically evaluable (un-evaluable group) because of intoxication or concomitant head injury, and has led to the use of advanced imaging techniques such as CT and MR imaging for radiologi-cal clearance.1,2,15,20,58,83,90,91 Continued advances in imag-ing quality and sensitivity now raise questions about the practice of clearing even alert, low-risk patients by clini-cal criteria alone,30 and have precluded the establishment of any consensus regarding the appropriate indications for the use of imaging studies.58,65,67,85,90
Although a lower threshold for the use of advanced imaging would hypothetically result in the detection and possible prevention of a greater number of CSIs, these benefits must be weighed against the associated risks and considerable costs of performing such studies and the additional treatments initiated due to false-positive results.18,19,41,77 Indeed, complications have been reported
in 6–71% of critically ill patients during and after trans-port.94 Accurate knowledge of the prevalence of CSI in trauma patients is therefore essential for assessing the need for immobilization and/or further imaging. Scat-tered studies of CSI in clinical series composed of all trauma patients report CSI prevalences ranging from 1 to 14%.59,87 However, unevaluable patients require a higher index of suspicion than the general trauma popu-lation,5,46,51,64,80,96 with one patient series estimating that a GCS score ≤ 8 incurs an almost 6-fold increase in the risk of CSI.50 Numerous patient series have examined the sensitivities of various imaging modalities in the detec-tion of CSI, and as such represent a large volume of data from which to calculate overall prevalence. However, considerable variation exists in rates of radiographic evi-dence of CSI, with 1 study reporting CT or MR imaging findings in 40% of obtunded patients.90 By systematically pooling data from relevant clinical series, more general-izable estimates of CSI prevalence in all trauma patients, alert patients, and unevaluable patients with trauma can be determined, along with the proportion of patients whose unstable injuries confer a risk of quadriplegia.
MethodsWe performed English-language searches of Med-
line and PubMed for articles published between 1985
Prevalence of cervical spinal injury in trauma
Andrew H. Milby, b.S.,1 CASey H. HAlpern, M.d.,1 wenSHeng guo, pH.d.,2 And SHerMAn C. Stein, M.d.11Department of Neurosurgery, Hospital of the University of Pennsylvania; and 2Center for Clinical Epidemi-ology and Biostatistics, University of Pennsylvania, School of Medicine, Philadelphia, Pennsylvania
Object. Diagnosis of cervical spinal injury (CSI) is an essential aspect of the trauma evaluation. This task is especially difficult in patients who are not clinically able to be evaluated (unevaluable) because of distracting pain-ful injuries, intoxication, or concomitant head injury. For this population, the appropriate use of advanced imaging techniques for cervical spinal clearance remains undetermined. This study was undertaken to estimate the prevalence of unstable CSI, particularly among patients in whom clinical evaluation is impossible or unreliable.
Methods. Estimates of the prevalence of CSI in populations consisting of all trauma patients, alert patients only, and clinically unevaluable patients only were determined by variance-weighted pooling of data from 65 publications (281,864 patients) that met criteria for review.
Results. The overall prevalence of CSI among all trauma patients was 3.7%. The prevalence of CSI in alert pa-tients was 2.8%, whereas unevaluable patients were at increased risk of CSI with a prevalence of 7.7% (p = 0.007). Overall, 41.9% of all CSI cases were considered to exhibit instability.
Conclusions. Trauma patients who are clinically unevaluable have a higher prevalence of CSI than alert patients. Knowledge of the prevalence and risk of such injuries may help establish an evidence-based approach to the detection and management of clinically occult CSI. (DOI: 10.3171/FOC.2008.25.11.E10)
Key wordS • cervical spine injury • prevalence • trauma
1
Abbreviations used in this paper: CSI = cervical spine injury; GCS = Glasgow Coma Scale.
Unauthenticated | Downloaded 06/26/20 04:01 AM UTC

A. H. Milby et al.
2 Neurosurg. Focus / Volume 25 / November 2008
Tabl
e 1:
Pre
vale
nce
of C
SI in
all
trau
ma
patie
nts
Auth
or &
Yea
rSe
tting
Cas
e Ac
crua
l Met
hod
Patie
nt P
opul
atio
nN
o. o
f Pa
tient
sIn
jury
Inci
denc
e
Bani
t et a
l., 2
000
sing
le U
S Le
vel I
trau
ma
cent
erre
trosp
ectiv
e ev
alua
tion
of c
linic
al a
lgor
ithm
all t
raum
a ad
mis
sion
s44
600.
036
Bayl
ess
& R
ay, 1
989
sing
le U
S Le
vel I
trau
ma
cent
erre
trosp
ectiv
e ob
serv
atio
nal
blun
t hea
d tra
uma
adm
issi
ons
176
0.01
7Bo
rock
et a
l., 1
991
sing
le U
S Le
vel I
trau
ma
cent
erre
trosp
ectiv
e ev
alua
tion
of c
linic
al a
lgor
ithm
blun
t tra
uma
adm
issi
ons
179
0.08
4C
ox e
t al.,
200
1si
ngle
US
Leve
l I tr
aum
a ce
nter
pros
pect
ive
eval
uatio
n of
clin
ical
alg
orith
mal
l tra
uma
adm
issi
ons
910.
044
Dem
etria
des
et a
l., 2
000
sing
le U
S Le
vel I
trau
ma
cent
erre
trosp
ectiv
e ob
serv
atio
nal
blun
t tra
uma
adm
issi
ons
14,7
550.
020
Edw
ards
et a
l., 2
001
sing
le N
ethe
rland
s Le
vel I
trau
ma
cent
erpr
ospe
ctiv
e ev
alua
tion
of c
linic
al a
lgor
ithm
high
-ene
rgy
traum
a ad
mis
sion
s17
570.
022
Gal
e et
al.,
200
5si
ngle
US
Leve
l I tr
aum
a ce
nter
retro
spec
tive
eval
uatio
n of
clin
ical
alg
orith
mbl
unt t
raum
a ad
mis
sion
s40
00.
048
Gro
ssm
an e
t al.,
199
910
6 U
S Le
vel I
–III
traum
a ce
nter
sre
trosp
ectiv
e su
rvey
all t
raum
a ad
mis
sion
s11
1,21
90.
043
Han
son
et a
l., 2
000
sing
le U
S Le
vel I
trau
ma
cent
erre
trosp
ectiv
e ev
alua
tion
of c
linic
al a
lgor
ithm
all t
raum
a ad
mis
sion
s42
850.
020
Har
ris e
t al.,
200
0si
ngle
US
Leve
l I tr
aum
a ce
nter
pros
pect
ive
eval
uatio
n of
clin
ical
alg
orith
mtra
uma
patie
nts
with
non
spin
al in
jurie
s14
50.
021
Insk
o et
al.,
200
2si
ngle
US
Leve
l I tr
aum
a ce
nter
retro
spec
tive
obse
rvat
iona
ltra
uma
patie
nts
unde
rgoi
ng fl
exio
n-ex
tens
ion
radi
ogra
phy
106
0.08
5
Krei
pke
et a
l., 1
989
sing
le U
S Le
vel I
trau
ma
cent
erpr
ospe
ctiv
e ob
serv
atio
nal
all t
raum
a ad
mis
sion
s86
00.
028
Lee
et a
l., 2
001
sing
le U
S Le
vel I
trau
ma
cent
erre
trosp
ectiv
e ob
serv
atio
nal
traum
a pa
tient
s un
derg
oing
bot
h ra
diog
raph
y an
d C
T60
40.
050
Mat
hen
et a
l., 2
007
sing
le U
S Le
vel I
trau
ma
cent
erpr
ospe
ctiv
e ob
serv
atio
nal
patie
nts
with
nec
k pa
in, n
euro
logi
cal d
efic
it, o
r in
toxi
catio
n66
70.
090
McC
ullo
ch e
t al.,
200
5si
ngle
US
Leve
l I tr
aum
a ce
nter
pros
pect
ive
obse
rvat
iona
ltra
uma
patie
nts
unde
rgoi
ng b
oth
radi
ogra
phy
and
CT
407
0.14
3
Mac
Don
ald
et a
l., 1
990
sing
le C
anad
ian
Leve
l I tr
aum
a ce
nter
retro
spec
tive
obse
rvat
iona
lm
otor
veh
icle
cra
sh tr
aum
a ad
mis
sion
s77
50.
119
Mow
er e
t al.,
200
121
US
univ
ersi
ty a
nd c
omm
unity
hos
pita
lspr
ospe
ctiv
e ob
serv
atio
nal
blun
t tra
uma
adm
issi
ons
34,0
690.
024
Nei
feld
et a
l., 1
988
four
US
traum
a ce
nter
sre
trosp
ectiv
e ev
alua
tion
of c
linic
al a
lgor
ithm
blun
t hea
d or
nec
k tra
uma
adm
issi
ons
886
0.03
0N
guye
n &
Cla
rk, 2
005
sing
le U
S Le
vel I
trau
ma
cent
erpr
ospe
ctiv
e ob
serv
atio
nal
patie
nts
with
nec
k pa
in, n
euro
logi
cal d
efic
it, o
r in
toxi
catio
n21
90.
014
Pras
ad e
t al.,
199
9si
ngle
Can
adia
n Le
vel I
trau
ma
cent
erre
trosp
ectiv
e ob
serv
atio
nal
“mul
titra
uma”
adm
issi
ons
6500
0.07
2Pt
ak e
t al.,
200
1si
ngle
US
Leve
l I tr
aum
a ce
nter
retro
spec
tive
obse
rvat
iona
lal
l tra
uma
adm
issi
ons
unde
rgoi
ng C
T67
60.
089
Rob
erge
et a
l., 1
988
sing
le U
S Le
vel I
trau
ma
cent
erpr
ospe
ctiv
e ev
alua
tion
of c
linic
al a
lgor
ithm
blun
t tra
uma
adm
issi
ons
467
0.01
7R
ober
ge &
Wea
rs, 1
992
sing
le U
S Le
vel I
trau
ma
cent
erpr
ospe
ctiv
e ev
alua
tion
of c
linic
al a
lgor
ithm
blun
t tra
uma
adm
issi
ons
480
0.03
5R
oss
et a
l., 1
992
sing
le U
S Le
vel I
trau
ma
cent
erpr
ospe
ctiv
e ob
serv
atio
nal
blun
t tra
uma
adm
issi
ons
410
0.03
2Sa
nche
z et
al.,
200
5si
ngle
US
Leve
l II t
raum
a ce
nter
pros
pect
ive
obse
rvat
iona
lal
l tra
uma
adm
issi
ons
2603
0.03
8Sh
arm
a et
al.,
200
7si
ngle
US
univ
ersi
ty h
ospi
tal e
mer
genc
y de
partm
ent
pros
pect
ive
obse
rvat
iona
lal
l tra
uma
adm
issi
ons
9903
0.01
3
Spite
ri et
al.,
200
6si
ngle
UK
traum
a ce
nter
retro
spec
tive
eval
uatio
n of
clin
ical
alg
orith
mtra
uma
adm
issi
ons
unde
rgoi
ng c
ervi
cal C
T43
40.
081
Willi
ams
et a
l., 1
992
sing
le U
S Le
vel I
trau
ma
cent
erre
trosp
ectiv
e ob
serv
atio
nal
all t
raum
a ad
mis
sion
s50
210.
045
Yana
r et a
l., 2
007
Trau
ma
regi
stry
, US
coun
typr
ospe
ctiv
e ob
serv
atio
nal
adul
t ped
estri
ans
inju
red
by v
ehic
les
6766
0.02
6
Unauthenticated | Downloaded 06/26/20 04:01 AM UTC

Neurosurg. Focus / Volume 25 / November 2008
Prevalence of cervical spine injury in trauma
3
and January 2008. The search used various combinations of the key words “spinal injuries,” “cervical vertebrae,” “instability,” “trauma,” “clearance,” “neck,” “diagnosis,” “epidemiology,” “prevalence,” and “incidence.” We re-fined the search by eliminating laboratory studies, case reports, editorials, or reviews without newly reported data, and case series with duplicated or overlapping data. These findings were supplemented by using the “Find Similar” and “Find Citing Articles” features of Medline and “Related Articles” feature of PubMed, as well as the bibliographies of selected articles. Articles were analyzed and compared with reference to the setting, study organi-zation, definitions of clinical criteria, and data collection methods. Studies restricted to children < 15 years of age were excluded. If a study reported prevalence rates from pediatric cases separately from those in an adult popula-tion, these data were also excluded from the analysis.
Studies meeting our criteria for inclusion were or-ganized into 3 categories: those composed of all trauma patients, alert patients, and unevaluable patients with trauma. Those studies reporting rates of instability upon detection of CSI were also placed into a fourth catego-ry, which overlapped in part with the previously listed categories. The “all trauma” category contained series in which patients were not further classified by clinical evaluability on presentation. These series were composed of patients with either unrestricted blunt and penetrating trauma or blunt trauma alone, whereas those composed solely of patients with penetrating trauma were excluded. Patients were deemed alert if they had reliable clinical ex-amination findings, consisting minimally of being able to respond to questions regarding neck pain and cooperate with neck movement instructions. Patients were consid-ered unevaluable if impaired consciousness, inebriation, confusion, endotracheal intubation, or distracting injuries rendered the clinical examination of the cervical spine unreliable. An unstable injury was defined as any frac-ture, dislocation, or purely ligamentous injury necessitat-ing external stabilization and/or operative fixation. Data concerning unstable injuries were pooled from all series reporting their prevalence without subclassification on the basis of clinical evaluability.
Mean prevalence values for each group were ob-tained using variance-weighted pooling. A mixed-effects logistic regression model was used, using SAS PROC NLMIXED (SAS, Inc.). Data within each study were considered a cluster and a hierarchical model was used to calculate the average prevalence rate. The binary nature of the outcome allowed the use of summary statistics as a proxy for the entire data set. The effect across studies was assumed to vary as a normal distribution. The overall prevalence rate was calculated as the population-average estimate, together with its 95% confidence intervals. Mean prevalence values for alert and unevaluable patients were compared, using a likelihood ratio test for pooled data.60 We considered differences with a probability value < 0.05 to be statistically significant.
ResultsSixty-five studies with a total of 281,864 subjects Ta
ble
2: P
reva
lenc
e of
CSI
in a
lert
trau
ma
patie
nts
Auth
or &
Yea
rSe
tting
Cas
e Ac
crua
l Met
hod
Patie
nt P
opul
atio
nN
o. o
f Pa
tient
s
Inju
ryIn
ci-
denc
e
Barb
a et
al.,
200
1si
ngle
US
Leve
l I tr
aum
a ce
nter
retro
spec
tive
eval
uatio
n of
clin
ical
alg
orith
mtra
uma
adm
issi
ons
unde
rgoi
ng c
ervi
cal C
T32
40.
046
Erso
y et
al.,
199
5si
ngle
Tur
kish
uni
vers
ity h
ospi
tal e
mer
-ge
ncy
depa
rtmen
tre
trosp
ectiv
e ob
serv
atio
nal
cons
ciou
s an
d or
ient
ed b
lunt
trau
ma
adm
issi
ons
303
0.04
3
Gon
zale
z et
al.,
199
9si
ngle
US
Leve
l I tr
aum
a ce
nter
pros
pect
ive
obse
rvat
iona
law
ake
and
aler
t blu
nt tr
aum
a ad
mis
sion
s21
760.
015
McN
amar
a et
al.,
198
8si
ngle
US
Leve
l II t
raum
a ce
nter
pros
pect
ive
obse
rvat
iona
lpa
tient
s w
ith n
eck
pain
follo
win
g tra
umat
ic in
jury
351
0.02
0M
cNam
ara
et a
l., 1
990
sing
le U
S Le
vel I
I tra
uma
cent
erre
trosp
ectiv
e ob
serv
atio
nal
aler
t, no
nint
oxic
ated
blu
nt tr
aum
a ad
mis
sion
s28
60.
017
Rot
h et
al.,
199
4si
ngle
US
milit
ary
med
ical
cen
ter
pros
pect
ive
coho
rtal
ert,
noni
ntox
icat
ed b
lunt
trau
ma
adm
issi
ons
286
0.01
7St
iell
et a
l., 2
001
10 C
anad
ian
traum
a ce
nter
spr
ospe
ctiv
e ev
alua
tion
of c
linic
al a
lgor
ithm
patie
nts
with
acu
te b
lunt
trau
ma
to h
ead
or n
eck
8924
0.01
7St
iell
et a
l., 2
003
9 C
anad
ian
terti
ary
care
hos
pita
lspr
ospe
ctiv
e ev
alua
tion
of c
linic
al a
lgor
ithm
patie
nts
with
acu
te b
lunt
trau
ma
to h
ead
or n
eck
8283
0.02
6Za
bel e
t al.,
199
7si
ngle
US
Leve
l I tr
aum
a ce
nter
retro
spec
tive
obse
rvat
iona
lal
ert t
raum
a ad
mis
sion
s35
30.
025
Unauthenticated | Downloaded 06/26/20 04:01 AM UTC

A. H. Milby et al.
4 Neurosurg. Focus / Volume 25 / November 2008
Tabl
e 3:
Pre
vale
nce
of C
SI in
clin
ical
ly u
neva
luab
le tr
aum
a pa
tient
s*
Auth
or &
Yea
rSe
tting
Cas
e Ac
crua
l Met
hod
Patie
nt P
opul
atio
nN
o. o
f Pa
tient
sIn
jury
Inci
denc
e
Bolin
ger e
t al.,
200
4si
ngle
US
Leve
l I tr
aum
a ce
nter
pros
pect
ive
eval
uatio
n of
clin
ical
alg
orith
mpa
tient
s w
ith T
BI a
nd G
CS
scor
es <
844
600.
036
Broo
ks &
Wille
tt, 2
001
sing
le U
K tra
uma
cent
erre
trosp
ectiv
e ob
serv
atio
nal
unco
nsci
ous
traum
a pa
tient
s17
60.
017
Chi
u et
al.,
200
1si
ngle
US
Leve
l I tr
aum
a ce
nter
retro
spec
tive
obse
rvat
iona
lpa
tient
s w
ith G
CS
scor
es <
15
on a
dmis
sion
179
0.08
4D
'Alis
e et
al.,
199
92
US
Leve
l I tr
aum
a ce
nter
sre
trosp
ectiv
e ob
serv
atio
nal
intu
bate
d fo
r hea
d or
sev
ere
mul
tisys
tem
inju
ries
910.
044
Dav
is e
t al.,
200
1si
ngle
US
Leve
l I tr
aum
a ce
nter
pros
pect
ive
eval
uatio
n of
clin
ical
alg
orith
mhe
ad-in
jure
d IC
U a
dmis
sion
s14
,755
0.02
0D
iaz
et a
l., 2
003
sing
le U
S Le
vel I
trau
ma
cent
erpr
ospe
ctiv
e ob
serv
atio
nal
alte
red
men
tal s
tatu
s or
dis
tract
ing
inju
ries
1757
0.02
2Fr
eedm
an e
t al.,
200
5si
ngle
Aus
tralia
n tra
uma
cent
erre
trosp
ectiv
e ob
serv
atio
nal
unco
nsci
ous
traum
a pa
tient
s ad
mitt
ed to
ICU
400
0.04
8G
eck
et a
l., 2
001
sing
le U
S Le
vel I
trau
ma
cent
erre
trosp
ectiv
e ob
serv
atio
nal
patie
nts
with
hig
h-en
ergy
mec
hani
sms
of in
jury
111,
219
0.04
3G
riffe
n et
al.,
200
3si
ngle
US
Leve
l I tr
aum
a ce
nter
retro
spec
tive
obse
rvat
iona
lal
tere
d m
enta
l sta
tus
or n
euro
logi
cal d
efic
it42
850.
020
Grif
fiths
et a
l., 2
002
sing
le U
S Le
vel I
trau
ma
cent
erre
trosp
ectiv
e ob
serv
atio
nal
unco
nsci
ous
or s
emic
onsc
ious
trau
ma
patie
nts
145
0.02
1H
ogan
et a
l., 2
005
sing
le U
S Le
vel I
trau
ma
cent
erre
trosp
ectiv
e ob
serv
atio
nal
obtu
nded
trau
ma
patie
nts
106
0.08
5H
olly
et a
l., 2
002
2 U
S Le
vel I
trau
ma
cent
ers
retro
spec
tive
obse
rvat
iona
lhe
ad in
jury
with
GC
S sc
ores
3-1
2, o
r GC
S sc
ore
>12
with
C
T ab
norm
ality
860
0.02
8
Jelly
et a
l., 2
000
sing
le U
K tra
uma
cent
erpr
ospe
ctiv
e ob
serv
atio
nal
patie
nts
intu
bate
d fo
r pol
ytra
uma
604
0.05
0Ki
hicz
ak e
t al.,
200
1si
ngle
US
Leve
l I tr
aum
a ce
nter
retro
spec
tive
obse
rvat
iona
lun
eval
uabl
e pa
tient
s un
derg
oing
MR
imag
ing
afte
r neg
a-tiv
e C
T66
70.
090
Pada
yach
ee e
t al.,
200
6si
ngle
UK
traum
a ce
nter
pros
pect
ive
obse
rvat
iona
lun
cons
ciou
s w
ith T
BI in
ICU
407
0.14
3Pi
att e
t al.,
200
6al
l Pen
nsyl
vani
a tra
uma
cent
ers
retro
spec
tive
obse
rvat
iona
lTB
I w/ G
CS
scor
es <
877
50.
119
Sche
narts
et a
l., 2
001
sing
le U
S Le
vel I
trau
ma
cent
erpr
ospe
ctiv
e ev
alua
tion
of c
linic
al a
lgor
ithm
alte
red
men
tal s
tatu
s af
ter b
lunt
trau
mat
ic in
jury
34,0
690.
024
Sees
et a
l., 1
998
sing
le U
S m
ilitar
y m
edic
al c
ente
rre
trosp
ectiv
e ob
serv
atio
nal
unre
spon
sive
or o
btun
ded
with
GC
S sc
ores
≤ 1
088
60.
030
Stas
sen
et a
l., 2
006
sing
le U
S Le
vel I
trau
ma
cent
erre
trosp
ectiv
e ev
alua
tion
of c
linic
al a
lgor
ithm
obtu
nded
blu
nt tr
aum
a pa
tient
s21
90.
014
Wid
der e
t al.,
200
4si
ngle
Can
adia
n Le
vel I
trau
ma
cent
erpr
ospe
ctiv
e ob
serv
atio
nal
obtu
nded
blu
nt tr
aum
a pa
tient
s65
000.
072
* IC
U =
inte
nsiv
e ca
re u
nit;
TBI =
trau
mat
ic b
rain
inju
ry.
Unauthenticated | Downloaded 06/26/20 04:01 AM UTC
Neurosurg. Focus / Volume 25 / November 2008
Prevalence of cervical spine injury in trauma
5
Tabl
e 4:
Pre
vale
nce
of u
nsta
ble
CSI
s in
all
trau
ma
patie
nts
Auth
or &
Yea
rSe
tting
Cas
e Ac
crua
l Met
hod
Patie
nt P
opul
atio
nN
o. o
f Pa
tient
sIn
jury
Inci
denc
e
Bani
t et a
l., 2
000
sing
le U
S Le
vel I
trau
ma
cent
erre
trosp
ectiv
e ev
alua
tion
of c
linic
al
algo
rithm
all t
raum
a ad
mis
sion
s15
10.
291
Bern
e et
al.,
199
9si
ngle
US
Leve
l I tr
aum
a ce
nter
pros
pect
ive
obse
rvat
iona
lbl
unt t
raum
a w
ith in
toxi
catio
n or
par
alyt
ics
200.
400
Chi
u et
al.,
200
1si
ngle
US
Leve
l I tr
aum
a ce
nter
retro
spec
tive
obse
rvat
iona
lpa
tient
s w
ith G
CS
scor
es <
15
on a
dmis
sion
471
0.55
6D
avis
et a
l., 1
993
6 U
S tra
uma
cent
ers
retro
spec
tive
obse
rvat
iona
lal
l tra
uma
adm
issi
ons
740
0.18
1D
emet
riade
s et
al.,
200
0si
ngle
US
Leve
l I tr
aum
a ce
nter
retro
spec
tive
obse
rvat
iona
lbl
unt t
raum
a ad
mis
sion
s29
20.
219
Free
dman
et a
l., 2
005
sing
le A
ustra
lian
traum
a ce
nter
retro
spec
tive
obse
rvat
iona
lun
cons
ciou
s tra
uma
patie
nts
adm
itted
to IC
U7
0.71
4G
eck
et a
l., 2
001
sing
le U
S Le
vel I
trau
ma
cent
erre
trosp
ectiv
e ob
serv
atio
nal
patie
nts
with
hig
h-en
ergy
mec
hani
sms
of in
jury
30.
333
Ger
relts
et a
l., 1
991
sing
le U
S Le
vel I
trau
ma
cent
erre
trosp
ectiv
e ob
serv
atio
nal
blun
t tra
uma
adm
issi
ons
500.
400
Gol
dber
g et
al.,
200
121
US
univ
ersi
ty a
nd c
omm
unity
ho
spita
lsre
trosp
ectiv
e ob
serv
atio
nal
blun
t tra
uma
adm
issi
ons
818
0.70
7
Grif
fiths
et a
l., 2
002
sing
le U
S Le
vel I
trau
ma
cent
erre
trosp
ectiv
e ob
serv
atio
nal
unco
nsci
ous
or s
emic
onsc
ious
trau
ma
patie
nts
21.
000
Har
ris e
t al.,
200
0si
ngle
US
Leve
l I tr
aum
a ce
nter
pros
pect
ive
eval
uatio
n of
clin
ical
alg
o-rit
hmtra
uma
patie
nts
with
non
spin
al in
jurie
s3
1.00
0
Hol
ly e
t al.,
200
22
US
Leve
l I tr
aum
a ce
nter
sre
trosp
ectiv
e ob
serv
atio
nal
head
inju
ry w
ith G
CS
scor
es 3
–12,
or G
CS
scor
es >
12
with
CT
abno
rmal
ity24
0.58
3
Mac
Don
ald
et a
l., 1
990
sing
le C
anad
ian
Leve
l I tr
aum
a ce
nter
retro
spec
tive
obse
rvat
iona
lm
otor
veh
icle
acc
iden
t tra
uma
adm
issi
ons
920.
174
Mat
hen
et a
l., 2
007
sing
le U
S Le
vel I
trau
ma
cent
erpr
ospe
ctiv
e ob
serv
atio
nal
patie
nts
with
nec
k pa
in, n
euro
logi
cal d
efic
it, o
r int
oxic
a-tio
n60
0.25
0
Rei
d et
al.,
198
7si
ngle
Can
adia
n Le
vel I
trau
ma
cent
erre
trosp
ectiv
e ob
serv
atio
nal
coho
rt of
pat
ient
s w
ith k
now
n C
SIs
253
0.34
8
Ros
s et
al.,
199
2si
ngle
US
Leve
l I tr
aum
a ce
nter
pros
pect
ive
obse
rvat
iona
lbl
unt t
raum
a ad
mis
sion
s43
0.30
2Sc
hena
rts e
t al.,
200
1si
ngle
US
Leve
l I tr
aum
a ce
nter
pros
pect
ive
eval
uatio
n of
clin
ical
alg
o-rit
hmal
tere
d m
enta
l sta
tus
afte
r blu
nt tr
aum
atic
inju
ry70
0.17
1
Slik
er e
t al.,
200
5m
ultip
le L
evel
I tra
uma
cent
ers
retro
spec
tive
liter
atur
e re
view
obtu
nded
blu
nt tr
aum
a pa
tient
s16
50.
612
Spite
ri et
al.,
200
6si
ngle
UK
traum
a ce
nter
retro
spec
tive
eval
uatio
n of
clin
ical
al
gorit
hmtra
uma
adm
issi
ons
unde
rgoi
ng c
ervi
cal C
T95
0.91
6
Wid
der e
t al.,
200
4si
ngle
Can
adia
n Le
vel I
trau
ma
cent
erpr
ospe
ctiv
e ob
serv
atio
nal
obtu
nded
blu
nt tr
aum
a pa
tient
s18
0.00
0
Yana
r et a
l., 2
007
2 U
S Le
vel I
trau
ma
cent
ers
retro
spec
tive
obse
rvat
iona
lpe
dest
rians
inju
red
by a
utom
obile
s17
80.
242
Unauthenticated | Downloaded 06/26/20 04:01 AM UTC
A. H. Milby et al.
6 Neurosurg. Focus / Volume 25 / November 2008
were selected with information on the prevalence of CSI or the proportion of instability in CSI.3,4,8–11,14,16,17,21,23,26,31–
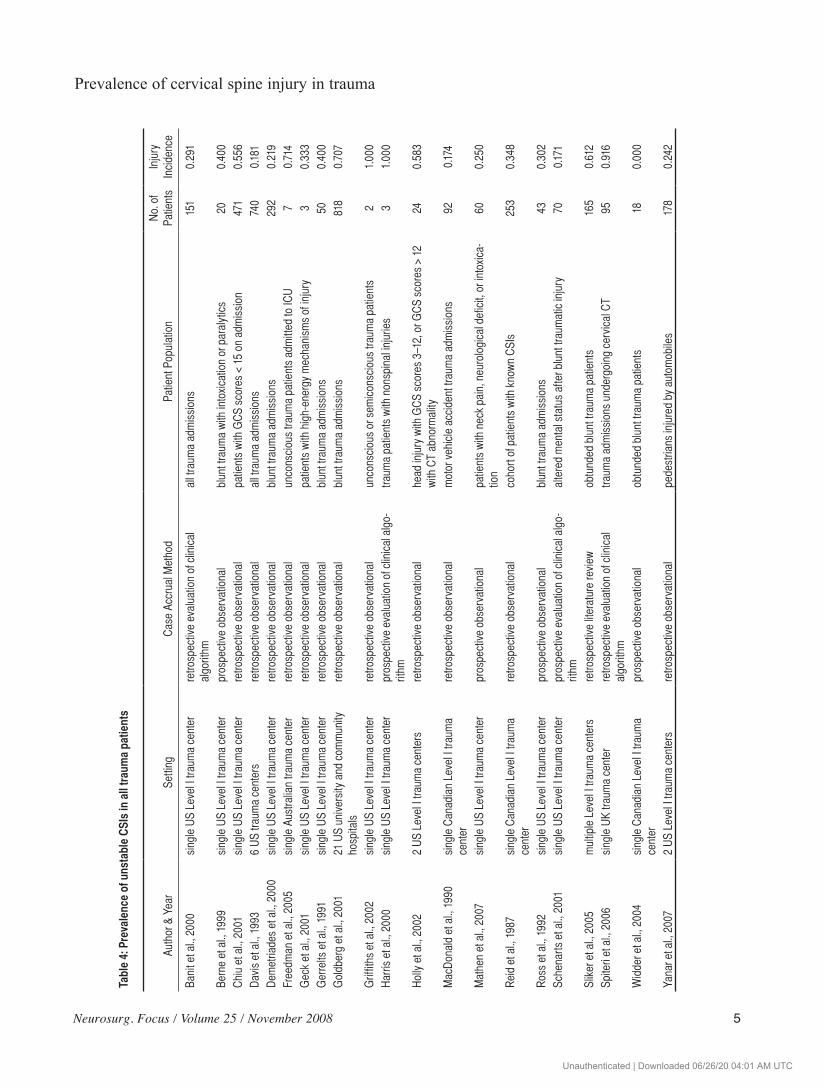
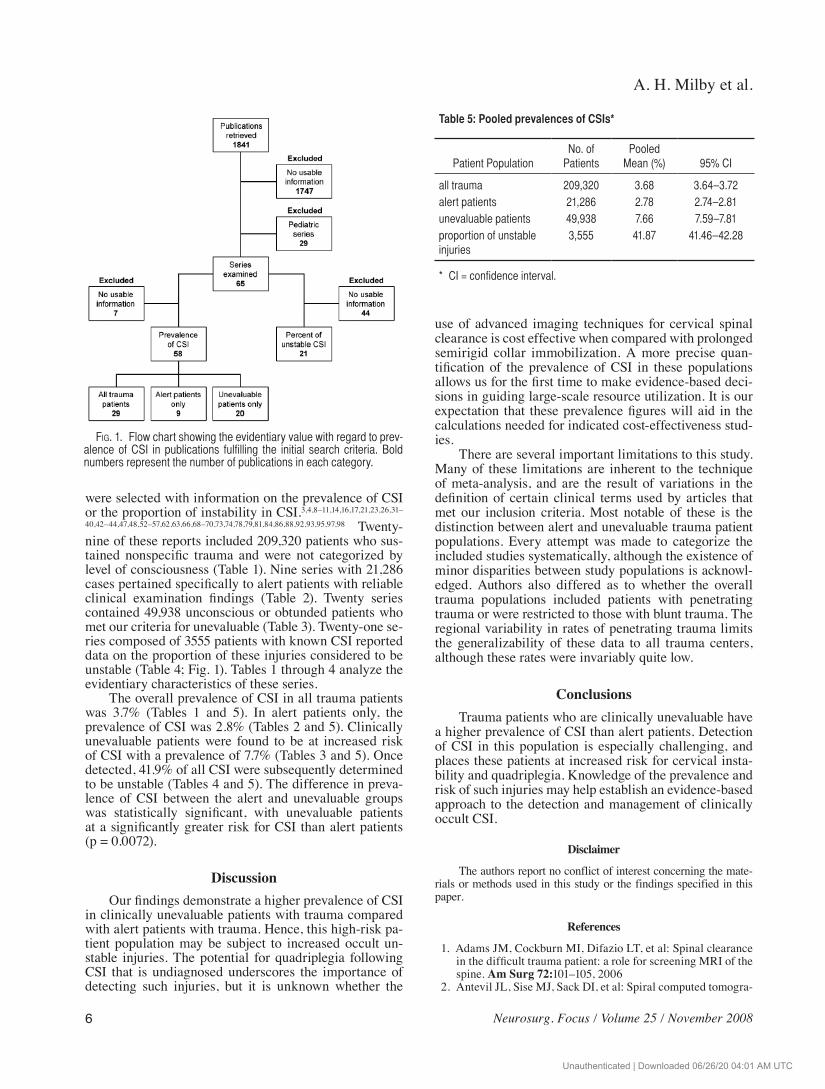
40,42–44,47,48,52–57,62,63,66,68–70,73,74,78,79,81,84,86,88,92,93,95,97,98 Twenty-nine of these reports included 209,320 patients who sus-tained nonspecific trauma and were not categorized by level of consciousness (Table 1). Nine series with 21,286 cases pertained specifically to alert patients with reliable clinical examination findings (Table 2). Twenty series contained 49,938 unconscious or obtunded patients who met our criteria for unevaluable (Table 3). Twenty-one se-ries composed of 3555 patients with known CSI reported data on the proportion of these injuries considered to be unstable (Table 4; Fig. 1). Tables 1 through 4 analyze the evidentiary characteristics of these series.
The overall prevalence of CSI in all trauma patients was 3.7% (Tables 1 and 5). In alert patients only, the prevalence of CSI was 2.8% (Tables 2 and 5). Clinically unevaluable patients were found to be at increased risk of CSI with a prevalence of 7.7% (Tables 3 and 5). Once detected, 41.9% of all CSI were subsequently determined to be unstable (Tables 4 and 5). The difference in preva-lence of CSI between the alert and unevaluable groups was statistically significant, with unevaluable patients at a significantly greater risk for CSI than alert patients (p = 0.0072).
DiscussionOur findings demonstrate a higher prevalence of CSI
in clinically unevaluable patients with trauma compared with alert patients with trauma. Hence, this high-risk pa-tient population may be subject to increased occult un-stable injuries. The potential for quadriplegia following CSI that is undiagnosed underscores the importance of detecting such injuries, but it is unknown whether the
use of advanced imaging techniques for cervical spinal clearance is cost effective when compared with prolonged semirigid collar immobilization. A more precise quan-tification of the prevalence of CSI in these populations allows us for the first time to make evidence-based deci-sions in guiding large-scale resource utilization. It is our expectation that these prevalence figures will aid in the calculations needed for indicated cost-effectiveness stud-ies.
There are several important limitations to this study. Many of these limitations are inherent to the technique of meta-analysis, and are the result of variations in the definition of certain clinical terms used by articles that met our inclusion criteria. Most notable of these is the distinction between alert and unevaluable trauma patient populations. Every attempt was made to categorize the included studies systematically, although the existence of minor disparities between study populations is acknowl-edged. Authors also differed as to whether the overall trauma populations included patients with penetrating trauma or were restricted to those with blunt trauma. The regional variability in rates of penetrating trauma limits the generalizability of these data to all trauma centers, although these rates were invariably quite low.
ConclusionsTrauma patients who are clinically unevaluable have
a higher prevalence of CSI than alert patients. Detection of CSI in this population is especially challenging, and places these patients at increased risk for cervical insta-bility and quadriplegia. Knowledge of the prevalence and risk of such injuries may help establish an evidence-based approach to the detection and management of clinically occult CSI.
Disclaimer
The authors report no conflict of interest concerning the mate-rials or methods used in this study or the findings specified in this paper.
References
1. Adams JM, Cockburn MI, Difazio LT, et al: Spinal clearance in the difficult trauma patient: a role for screening MRI of the spine. Am Surg 72:101–105, 2006
2. Antevil JL, Sise MJ, Sack DI, et al: Spiral computed tomogra-
Fig. 1. Flow chart showing the evidentiary value with regard to prev-alence of CSI in publications fulfilling the initial search criteria. Bold numbers represent the number of publications in each category.
Table 5: Pooled prevalences of CSIs*
Patient PopulationNo. of
PatientsPooled
Mean (%) 95% CI
all trauma 209,320 3.68 3.64–3.72alert patients 21,286 2.78 2.74–2.81unevaluable patients 49,938 7.66 7.59–7.81proportion of unstable injuries
3,555 41.87 41.46–42.28
* CI = confidence interval.
Unauthenticated | Downloaded 06/26/20 04:01 AM UTC

Neurosurg. Focus / Volume 25 / November 2008
Prevalence of cervical spine injury in trauma
7
phy for the initial evaluation of spine trauma: a new standard of care? J Trauma 61:382–387, 2006
3. Banit DM, Grau G, Fisher JR: Evaluation of the acute cervi-cal spine: a management algorithm. J Trauma 49:450–456, 2000
4. Barba CA, Taggert J, Morgan AS, et al: A new cervical spine clearance protocol using computed tomography. J Trauma 51:652–657, 2001
5. Bayless P, Ray VG: Incidence of cervical spine injuries in as-sociation with blunt head trauma. Am J Emerg Med 7:139–142, 1989
6. Bellabarba C, Mirza SK, West GA, et al: Diagnosis and treat-ment of craniocervical dislocation in a series of 17 consecu-tive survivors during an 8-year period. J Neurosurg Spine 4:429–440, 2006
7. Berkowitz M: Assessing the socioeconomic impact of im-proved treatment of head and spinal cord injuries. J Emerg Med 11 (Suppl 1):63–67, 1993
8. Berne JD, Velmahos GC, El-Tawil Q, et al: Value of complete cervical helical computed tomographic scanning in identify-ing cervical spine injury in the unevaluable blunt trauma pa-tient with multiple injuries: a prospective study. J Trauma 47:896–893, 1999
9. Bolinger B, Shartz M, Marion D: Bedside fluoroscopic flex-ion and extension cervical spine radiographs for clearance of the cervical spine in comatose trauma patients. J Trauma 56:132–136, 2004
10. Borock EC, Gabram SG, Jacobs LM, et al: A prospective analysis of a two-year experience using computed tomog-raphy as an adjunct for cervical spine clearance. J Trauma 31:1001–1006, 1991
11. Brooks RA, Willett KM: Evaluation of the Oxford protocol for total spinal clearance in the unconscious trauma patient. J Trauma 50:862–867, 2001
12. Burney RE, Maio RF, Maynard F, et al: Incidence, character-istics, and outcome of spinal cord injury at trauma centers in North America. Arch Surg 128:596–599, 1993
13. Cardenas DD, Hoffman JM, Kirshblum S, et al: Etiology and incidence of rehospitalization after traumatic spinal cord inju-ry: a multicenter analysis. Arch Phys Med Rehabil 85:1757–1763, 2004
14. Chiu WC, Haan JM, Cushing BM, et al: Ligamentous inju-ries of the cervical spine in unreliable blunt trauma patients: incidence, evaluation, and outcome. J Trauma 50:457–464, 2001
15. Como JJ, Thompson MA, Anderson JS, et al: Is magnetic resonance imaging essential in clearing the cervical spine in obtunded patients with blunt trauma? J Trauma 63:544–549, 2007
16. Cox MW, McCarthy M, Lemmon G, et al: Cervical spine in-stability: clearance using dynamic fluoroscopy. Curr Surg 58:96–100, 2001
17. D’Alise MD, Benzel EC, Hart BL: Magnetic resonance imag-ing evaluation of the cervical spine in the comatose or ob-tunded trauma patient. J Neurosurg 91:54–59, 1999
18. Daffner RH: Controversies in cervical spine imaging in trau-ma patients. Emerg Radiol 11:2–8, 2004
19. Daffner RH: Controversies in cervical spine imaging in trau-ma patients. Semin Musculoskelet Radiol 9:105–115, 2005
20. Daffner RH, Sciulli RL, Rodriguez A, et al: Imaging for eval-uation of suspected cervical spine trauma: a 2-year analysis. Injury 37:652–658, 2006
21. Davis JW, Kaups KL, Cunningham MA, et al: Routine evalu-ation of the cervical spine in head-injured patients with dy-namic fluoroscopy: a reappraisal. J Trauma 50:1044–1047, 2001
22. Davis JW, Phreaner DL, Hoyt DB, et al: The etiology of missed cervical spine injuries. J Trauma 34:342–346, 1993
23. Demetriades D, Charalambides K, Chahwan S, et al: Nonskel-
etal cervical spine injuries: epidemiology and diagnostic pit-falls. J Trauma 48:724–727, 2000
24. DeVivo MJ: Causes and costs of spinal cord injury in the Unit-ed States. Spinal Cord 35:809–813, 1997
25. DeVivo MJ, Rutt RD, Black KJ, et al: Trends in spinal cord injury demographics and treatment outcomes between 1973 and 1986. Arch Phys Med Rehabil 73:424–430, 1992
26. Diaz JJ Jr, Gillman C, Morris JA Jr, et al: Are five-view plain films of the cervical spine unreliable? A prospective evalu-ation in blunt trauma patients with altered mental status. J Trauma 55:658–654, 2003
27. Dryden DM, Saunders LD, Jacobs P, et al: Direct health care costs after traumatic spinal cord injury. J Trauma 59:443–449, 2005
28. Dryden DM, Saunders LD, Rowe BH, et al: Depression fol-lowing traumatic spinal cord injury. Neuroepidemiology 25:55–61, 2005
29. Dryden DM, Saunders LD, Rowe BH, et al: Utilization of health services following spinal cord injury: a 6-year follow-up study. Spinal Cord 42:513–525, 2004
30. Duane TM, Dechert T, Wolfe LG, et al: Clinical examina-tion and its reliability in identifying cervical spine fractures. J Trauma 62:1405–1410, 2007
31. Edwards MJ, Frankema SP, Kruit MC, et al: Routine cervical spine radiography for trauma victims: does everybody need it? J Trauma 50:529–534, 2001
32. Ersoy G, Karcioglu O, Enginbas Y, et al: Are cervical spine x-rays mandatory in all blunt trauma patients? Eur J Emerg Med 2:191–195, 1995
33. Freedman I, van Gelderen D, Cooper DJ, et al: Cervical spine assessment in the unconscious trauma patient: a major trauma service’s experience with passive flexion-extension radiogra-phy. J Trauma 58:1183–1188, 2005
34. Gale SC, Gracias VH, Reilly PM, et al: The inefficiency of plain radiography to evaluate the cervical spine after blunt trauma. J Trauma 59:1121–1125, 2005
35. Geck MJ, Yoo S, Wang JC: Assessment of cervical ligamen-tous injury in trauma patients using MRI. J Spinal Disord 14:371–377, 2001
36. Gerrelts BD, Petersen EU, Mabry J, et al: Delayed diagnosis of cervical spine injuries. J Trauma 31:1622–1626, 1991
37. Goldberg W, Mueller C, Panacek E, et al: Distribution and patterns of blunt traumatic cervical spine injury. Ann Emerg Med 38:17–21, 2001
38. Gonzalez RP, Fried PO, Bukhalo M, et al: Role of clinical examination in screening for blunt cervical spine injury. J Am Coll Surg 189:152–157, 1999
39. Griffen MM, Frykberg ER, Kerwin AJ, et al: Radiographic clearance of blunt cervical spine injury: plain radiograph or computed tomography scan? J Trauma 55:222–227, 2003
40. Griffiths HJ, Wagner J, Anglen J, et al: The use of forced flex-ion/extension views in the obtunded trauma patient. Skeletal Radiol 31:587–591, 2002
41. Grogan EL, Morris JA Jr, Dittus RS, et al: Cervical spine eval-uation in urban trauma centers: lowering institutional costs and complications through helical CT scan. J Am Coll Surg 200:160–165, 2005
42. Grossman MD, Reilly PM, Gillett T, et al: National survey of the incidence of cervical spine injury and approach to cervical spine clearance in U.S. trauma centers. J Trauma 47:684–690, 1999
43. Hanson JA, Blackmore CC, Mann FA, et al: Cervical spine in-jury: a clinical decision rule to identify high-risk patients for helical CT screening. AJR Am J Roentgenol 174:713–717, 2000
44. Harris MB, Kronlage SC, Carboni PA, et al: Evaluation of the cervical spine in the polytrauma patient. Spine 25:2884–2892, 2000
45. Harvey LA, Batty J, Jones R, et al: Hand function of C6 and
Unauthenticated | Downloaded 06/26/20 04:01 AM UTC
A. H. Milby et al.
8 Neurosurg. Focus / Volume 25 / November 2008
C7 tetraplegics 1 - 16 years following injury. Spinal Cord 39:37–43, 2001
46. Hills MW, Deane SA: Head injury and facial injury: is there an increased risk of cervical spine injury? J Trauma 34:549–544, 1993
47. Hoffman JR, Mower WR, Wolfson AB, et al: Validity of a set of clinical criteria to rule out injury to the cervical spine in pa-tients with blunt trauma. National Emergency X-Radiography Utilization Study Group. N Engl J Med 343:94–99, 2000
48. Hogan GJ, Mirvis SE, Shanmuganathan K, et al: Exclusion of unstable cervical spine injury in obtunded patients with blunt trauma: is MR imaging needed when multi-detector row CT findings are normal? Radiology 237:106–113, 2005
49. Hollingworth W, Relyea-Chew A, Comstock BA, et al: The risk of bankruptcy before and after brain or spinal cord injury: a glimpse of the iceberg’s tip. Med Care 45:702–711, 2007
50. Holly LT, Kelly DF, Counelis GJ, et al: Cervical spine trauma associated with moderate and severe head injury: incidence, risk factors, and injury characteristics. J Neurosurg 96:285–291, 2002
51. Iida H, Tachibana S, Kitahara T, et al: Association of head trauma with cervical spine injury, spinal cord injury, or both. J Trauma 46:450–452, 1999
52. Insko EK, Gracias VH, Gupta R, et al: Utility of flexion and extension radiographs of the cervical spine in the acute evalu-ation of blunt trauma. J Trauma 53:426–429, 2002
53. Jelly LM, Evans DR, Easty MJ, et al: Radiography versus spi-ral CT in the evaluation of cervicothoracic junction injuries in polytrauma patients who have undergone intubation. Radio-graphics 20:S251-252, 2000
54. Kihiczak D, Novelline RA, Lawrason JN, et al: Should an MR scan be performed routinely after a normal clearance CT scan in the trauma patient? Experience with 59 cases. Emerg Ra-diol 8:276–278, 2001
55. Kreipke DL, Gillespie KR, McCarthy MC, et al: Reliability of indications for cervical spine films in trauma patients. J Trauma 29:1438–1439, 1989
56. Lee HJ, Sharma V, Shah K, et al: The role of spiral CT vs plain films in acute cervical spine trauma: a comparative study. Emerg Radiol 8:311–314, 2001
57. MacDonald RL, Schwartz ML, Mirich D, et al: Diagnosis of cervical spine injury in motor vehicle crash victims: how many x-rays are enough? J Trauma 30:392–397, 1990
58. Mathen R, Inaba K, Munera F, et al: Prospective evaluation of multislice computed tomography versus plain radiograph-ic cervical spine clearance in trauma patients. J Trauma 62:1427–1431, 2007
59. McCulloch PT, France J, Jones DL, et al: Helical computed tomography alone compared with plain radiographs with ad-junct computed tomography to evaluate the cervical spine after high-energy trauma. J Bone Joint Surg Am 87:2388–2394, 2005
60. McGee S: Simplifying likelihood ratios. J Gen Intern Med 17:646–649, 2002
61. McKinley W, Santos K, Meade M, et al: Incidence and out-comes of spinal cord injury clinical syndromes. J Spinal Cord Med 30:215–224, 2007
62. McNamara RM, Heine E, Esposito B: Cervical spine injury and radiography in alert, high-risk patients. J Emerg Med 8:177–182, 1990
63. McNamara RM, O’Brien MC, Davidheiser S: Post-traumatic neck pain: a prospective and follow-up study. Ann Emerg Med 17:906–911, 1988
64. Michael DB, Guyot DR, Darmody WR: Coincidence of head and cervical spine injury. J Neurotrauma 6:177–189, 1989
65. Molina DK, Nichols JJ, Dimaio VJ: The sensitivity of com-puted tomography (CT) scans in detecting trauma: are CT scans reliable enough for courtroom testimony? J Trauma 63:625–629, 2007
66. Mower WR, Hoffman JR, Pollack CV Jr, et al: Use of plain radiography to screen for cervical spine injuries. Ann Emerg Med 38:1–7, 2001
67. Muchow RD, Resnick DK, Abdel MP, et al: Magnetic reso-nance imaging (MRI) in the clearance of the cervical spine in blunt trauma: a meta-analysis. J Trauma 64:179–189, 2008
68. Neifeld GL, Keene JG, Hevesy G, et al: Cervical injury in head trauma. J Emerg Med 6:203–207, 1988
69. Nguyen GK, Clark R: Adequacy of plain radiography in the diagnosis of cervical spine injuries. Emerg Radiol 11:158–161, 2005
70. Padayachee L, Cooper DJ, Irons S, et al: Cervical spine clear-ance in unconscious traumatic brain injury patients: dynamic flexion-extension fluoroscopy versus computed tomography with three-dimensional reconstruction. J Trauma 60:341–345, 2006
71. Piatt JH Jr: Detected and overlooked cervical spine injury in comatose victims of trauma: report from the Pennsylva-nia Trauma Outcomes Study. J Neurosurg Spine 5:210–216, 2006
72. Poonnoose PM, Ravichandran G, McClelland MR: Missed and mismanaged injuries of the spinal cord. J Trauma 53:314–320, 2002
73. Prasad VS, Schwartz A, Bhutani R, et al: Characteristics of injuries to the cervical spine and spinal cord in polytrauma patient population: experience from a regional trauma unit. Spinal Cord 37:560–568, 1999
74. Ptak T, Kihiczak D, Lawrason JN, et al: Screening for cervi-cal spine trauma with helical CT: experience with 676 cases. Emerg Radiol 8:315–319, 2001
75. Ravichandran G, Silver JR: Missed injuries of the spinal cord. Br Med J (Clin Res Ed) 284:953–956, 1982
76. Reid DC, Henderson R, Saboe L, et al: Etiology and clini-cal course of missed spine fractures. J Trauma 27:980–986, 1987
77. Richards PJ, Summerfield R, George J, et al: Major trauma & cervical clearance radiation doses & cancer induction. Injury 39:347–356, 2008
78. Roberge RJ, Wears RC: Evaluation of neck discomfort, neck tenderness, and neurologic deficits as indicators for radiog-raphy in blunt trauma victims. J Emerg Med 10:539–544, 1992
79. Roberge RJ, Wears RC, Kelly M, et al: Selective application of cervical spine radiography in alert victims of blunt trauma: a prospective study. J Trauma 28:784–788, 1988
80. Ross SE, O’Malley KF, DeLong WG, et al: Clinical predictors of unstable cervical spinal injury in multiply injured patients. Injury 23:317–319, 1992
81. Roth BJ, Martin RR, Foley K, et al: Roentgenographic evalu-ation of the cervical spine. A selective approach. Arch Surg 129:643–645, 1994
82. Sanchez B, Waxman K, Jones T, et al: Cervical spine clear-ance in blunt trauma: evaluation of a computed tomography-based protocol. J Trauma 59:179–183, 2005
83. Sarani B, Waring S, Sonnad S, et al: Magnetic resonance im-aging is a useful adjunct in the evaluation of the cervical spine of injured patients. J Trauma 63:637–640, 2007
84. Schenarts PJ, Diaz J, Kaiser C, et al: Prospective comparison of admission computed tomographic scan and plain films of the upper cervical spine in trauma patients with altered men-tal status. J Trauma 51:663–669, 2001
85. Schuster R, Waxman K, Sanchez B, et al: Magnetic resonance imaging is not needed to clear cervical spines in blunt trauma patients with normal computed tomographic results and no motor deficits. Arch Surg 140:762–766, 2005
86. Sees DW, Rodriguez Cruz LR, Flaherty SF, et al: The use of bedside fluoroscopy to evaluate the cervical spine in obtunded trauma patients. J Trauma 45:768–771, 1998
87. Sharma OP, Oswanski MF, Yazdi JS, et al: Assessment for
Unauthenticated | Downloaded 06/26/20 04:01 AM UTC

Neurosurg. Focus / Volume 25 / November 2008
Prevalence of cervical spine injury in trauma
9
additional spinal trauma in patients with cervical spine injury. Am Surg 73:70–74, 2007
88. Sliker CW, Mirvis SE, Shanmuganathan K: Assessing cervi-cal spine stability in obtunded blunt trauma patients: review of medical literature. Radiology 234:733–739, 2005
89. Spiteri V, Kotnis R, Singh P, et al: Cervical dynamic screening in spinal clearance: now redundant. J Trauma 61:1171–1177, 2006
90. Stassen NA, Williams VA, Gestring ML, et al: Magnetic resonance imaging in combination with helical computed tomography provides a safe and efficient method of cervical spine clearance in the obtunded trauma patient. J Trauma 60:171–177, 2006
91. Stelfox HT, Velmahos GC, Gettings E, et al: Computed to-mography for early and safe discontinuation of cervical spine immobilization in obtunded multiply injured patients. J Trauma 63:630–636, 2007
92. Stiell IG, Clement CM, McKnight RD, et al: The Canadian C-spine rule versus the NEXUS low-risk criteria in patients with trauma. N Engl J Med 349:2510–2518, 2003
93. Stiell IG, Wells GA, Vandemheen KL, et al: The Canadian C-spine rule for radiography in alert and stable trauma patients. JAMA 286:1841–1848, 2001
94. Waydhas C: Intrahospital transport of critically ill patients. Crit Care 3:R83–R89, 1999
95. Widder S, Doig C, Burrowes P, et al: Prospective evaluation of computed tomographic scanning for the spinal clearance of obtunded trauma patients: preliminary results. J Trauma 56:1179–1184, 2004
96. Williams J, Jehle D, Cottington E, et al: Head, facial, and clavicular trauma as a predictor of cervical-spine injury. Ann Emerg Med 21:719–722, 1992
97. Yanar H, Demetriades D, Hadjizacharia P, et al: Pedestrians injured by automobiles: risk factors for cervical spine injuries. J Am Coll Surg 205:794–799, 2007
98. Zabel DD, Tinkoff G, Wittenborn W, et al: Adequacy and ef-ficacy of lateral cervical spine radiography in alert, high-risk blunt trauma patient. J Trauma 43:952–958, 1997
Manuscript submitted July 14, 2008.Accepted July 29, 2008.Address correspondence to: Sherman C. Stein, M.D., Hospital
of the University of Pennsylvania, Department of Neurosurgery, 3 Silverstein, 3400 Spruce Street, Philadelphia, Pennsylvania 19104. email: [email protected].
Unauthenticated | Downloaded 06/26/20 04:01 AM UTC