presentación de powerpoint - academia.cat · a phase ii is planned in first line mpc with. ......
TRANSCRIPT

Quimioteràpia per l'adenocarcinoma de pàncrees. Com són de bons els resultats?
Que ̀ esperem en un futur pròxim?
Carles Pericay(Oncologia. Hospital Parc Taulí)

Projecting Cancer Deaths to 2030
Rahib et al, Cancer Res 2014
Lung

1ª línia al càncer de pàncrees

Treating advanced pancreatic cancer: the story so far
• Pre-1997: 5-fluorouracil monotherapy
• 1997: GEM monotherapy shown to improve survival,1 becomes standard of care for advanced PC
• 2000s: Various GEM-based combinations fail to demonstrate clinically significant survival benefit
• 2007: Erlotinib/GEM shows significant survival benefit vs GEM,2 approved in Europe
• 2011: FOLFIRINOX shows significantly improved survival and response ratesvs GEM,3 but is associated with greater toxicity
• 2013: MPACT Trial of nab-P + Gem as a backbone therapy of metastaticPancreatic Cancer
1. Burris HA, et al. J Clin Oncol. 1997;15:2403‒2413; 2. Moore MJ, et al. J Clin Oncol. 2007;25:1960‒1966; 3. Conroy T, et al. N Engl J Med. 2011;364:1817‒1825.GEM, gemcitabine; FOLFIRINOX, oxaliplatin, irinotecan, fluorouracil, leucovorin; PC, pancreatic cancer
The FOLFIRINOX regimen has not been approved by the EMA for treatment of pancreatic cancer.

Chemotherapy for advanced disease
Gemcitabine 5FU
CBR 23.8% 4.8%
Median TTF 9 weeks 4 weeks
Median survival
5.6 months 4.4 months
PR and SD for >8/52
44.4% 19%
1 year survival 18% 2%
Burris et al JCO 1997



* Adjusted for PS, pain and disease extent at randomization
HR = 0.81*95% CI (0.67, 0.97)P = 0.025
Gemcitabine + ErlotinibMedian = 6.37 months1 Year Survival = 24%
Gemcitabine + PlaceboMedian = 5.91 months1 Year Survival = 17%
Perc
enta
ge
0
20
40
60
80
100
Time (Months)0 6 12 18 24
Moore JCO 2007
Locally advanced/metastatic pancreatic cancerNCIC CTG PA.3 – Overall Survival
HR = 0.81*95% CI (0.67, 0.97)P=0.025
Gemcitabine + ErlotinibMedian = 6.37 months1 Year survival = 24%
Gemcitabine + PlaceboMedian = 5.91 months1 Year survival = 17%

Study Design
1:1, stratified by KPS, region, liver metastasis
Planned N = 842
• Stage IV• No prior treatment
for metastatic disease
• KPS ≥70 • Measurable disease• Total bilirubin ≤ULN
nab-Paclitaxel 125 mg/m2 IV qw 3/4 weeks
+Gemcitabine
1000 mg/m2 IV qw 3/4 weeks
Gemcitabine1000 mg/m2 IV qw for 7/8 weeks
then qw 3/4 weeks
Von Hoff et al., ASCO GI 2013
§ Primary Endpoint: – OS
§ Secondary Endpoints:– PFS and ORR by
Independent Review (RECIST)
§ Safety and Tolerability– by NCI CTCAE v3.0
• With 608 events, 90% power to detect OS HR = 0.769 (2–sided α = 0.049)
• 1 interim analysis for futility• Treat until progression• CT scans every 8 weeks

Prodige 4 - ACCORD 11 trial design
Stratification :
n centern performance status: 0 versus 1n location of the tumor: head versus other location of the primary
Metastaticpancreaticcancer
RANDOMIZE
Folfirinox
Gemcitabine6 months of
chemotherapyrecommended
CT scans: obtained
every 2 months
for both arms:
342ptsECOG PS 0-1





2ª línia al càncer de pàncrees

2002-2003165pt: 23 pt/23pt 1ªlínea: Gemcitabina – SLP 4,57 m(BSC) vs 4,75m(OFF)2ªlínea: OFF- 4,82m vs BSC- 2,30m (p=0,008)
BSC versus OFF: folinic acid 200 mg/m2 followed by 5-fluorouracil 2 g/m2 (24 h) on d1, d8, d15, d22 and oxaliplatin 85 mg/m2 on days 8 and 22 every 43 days + BSC

Rama A: 5FULV2 + Cisplatino 50mg/m2 /2 semanas (102 pt)Rama B: Gemcitabina 1000mg/m2/semana/7 semanas /8 (100 pt)
SLP: 3,4 m vs 3,5 m
SG: 6,7 m vs 8,03 m

2ª linea (61%): Rama A: 68%Rama B: 55%
2ª linea por progresión: SLP1: 2,6m vs 3,6mSLP2: ITT. 5,03m vs 5,8m
QT 2ª: 6,03 m vs 8,8 m

CONKO 003
FF OFF
PFS from start 2nd line Rx 9 weeks 13 weeks (log rank p =0.012)
OS from start 2nd line Rx 13 weeks 26 weeks (log rank p=0.014)
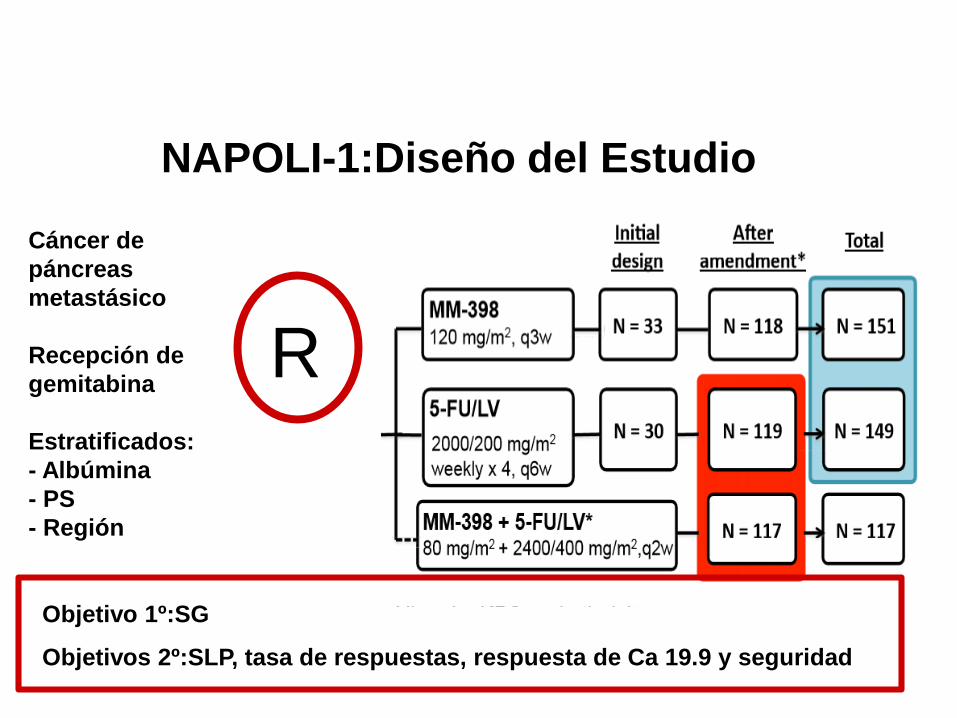
NAPOLI-1:Diseño del EstudioCáncer de páncreas metastásico
Recepción de gemitabina
Estratificados:- Albúmina- PS- Región
Objetivo 1º:SG
Objetivos 2º:SLP, tasa de respuestas, respuesta de Ca 19.9 y seguridad
R

NAPOLI-1:Resultados: SG

NAPOLI-1:Objetivos secundarios
Variable MM-398+ 5FU/Lv(n:117)
5Fu/LV(n:119)
SLP mediana,meses( IC 95%)
3,1(2,7-4,2)
1,5(1,4-1,8)
Tasa de respuestas ,%(IC 95%)
16(9,6-22,9)
1(0-2,5)
Reducción Ca 19.9, respuesta/evaluables
36(27/76)
12(8/69)

Efectos Secundarios

Biologia al càncer de pàncrees
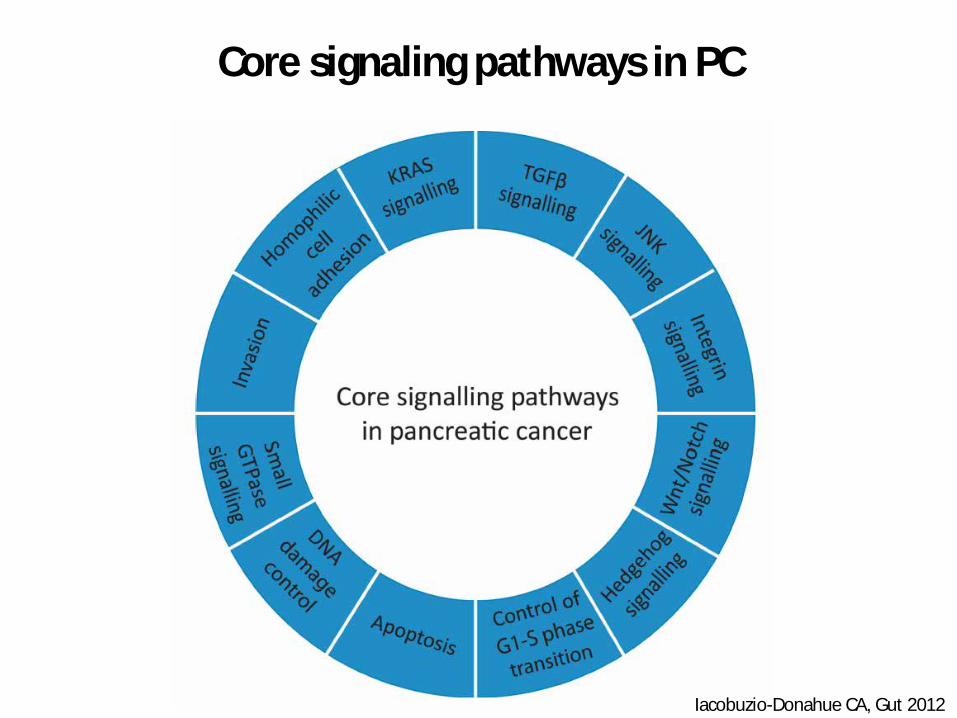
Core signaling pathways in PC
Iacobuzio-Donahue CA, Gut 2012
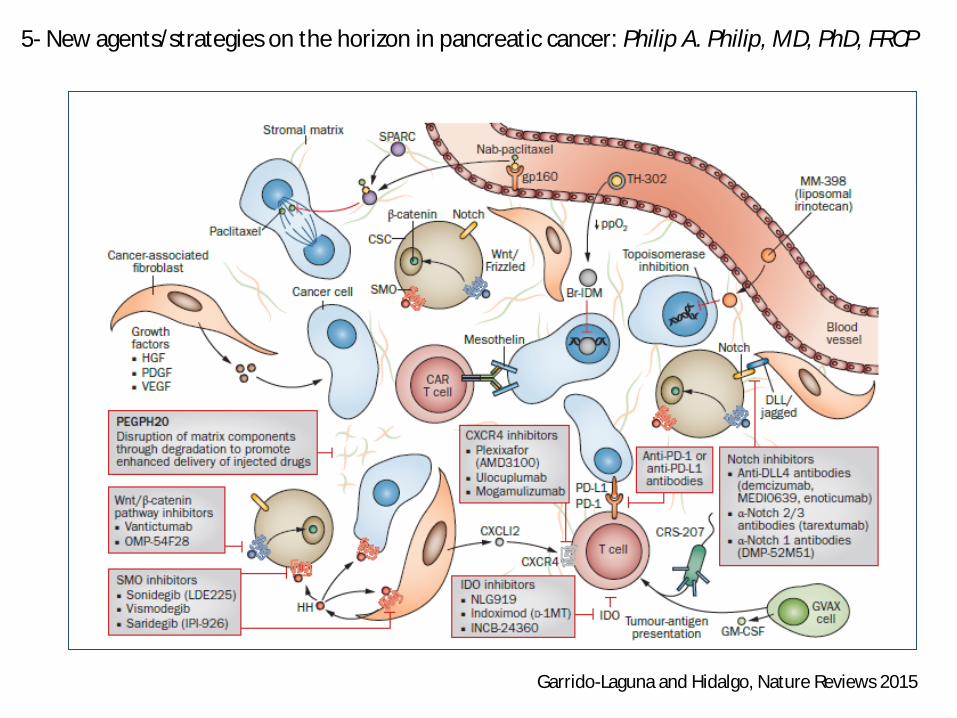
Garrido-Laguna and Hidalgo, Nature Reviews 2015
5- New agents/strategies on the horizon in pancreatic cancer: Philip A. Philip, MD, PhD, FRCP



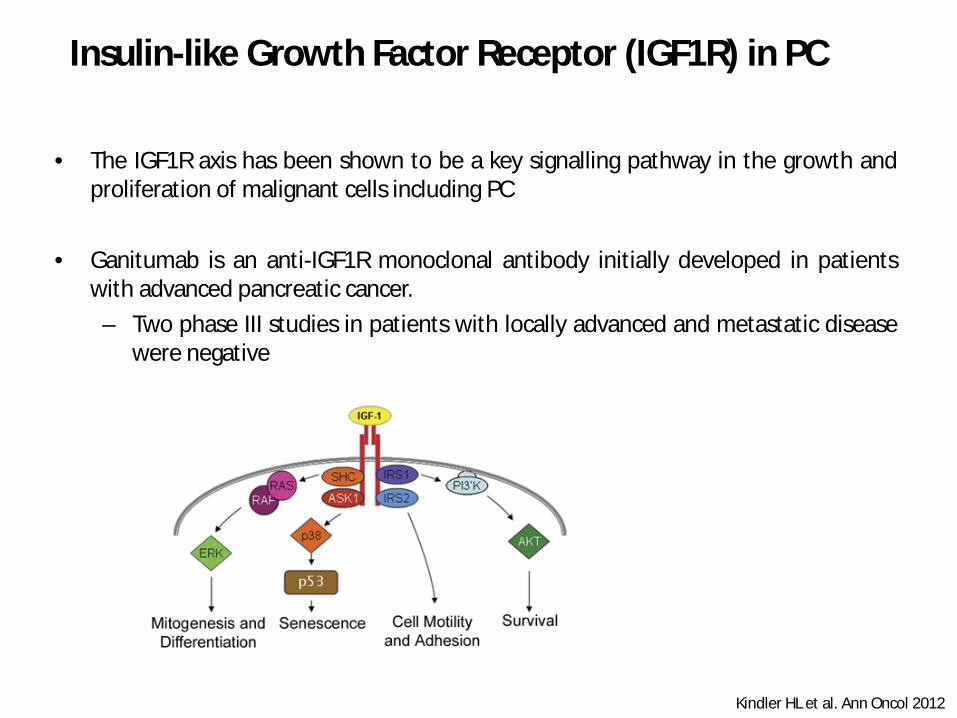
• The IGF1R axis has been shown to be a key signalling pathway in the growth andproliferation of malignant cells including PC
• Ganitumab is an anti-IGF1R monoclonal antibody initially developed in patientswith advanced pancreatic cancer.– Two phase III studies in patients with locally advanced and metastatic disease
were negative
Insulin-like Growth Factor Receptor (IGF1R) in PC
Kindler HL et al. Ann Oncol 2012

IGFR-1R inhibitors have more activity in patients with elevated free IGF-1 serum levels
MM-141 is an IGF-1R and ErbB3 directed antibody.A phase II is planned in first line mPC with positive serum levels of free IGF-1 withMM-141+ Gem+ nab-paclitaxel vs Gem+nab-paclitaxel.

Stroma and PC
Hidalgo and N Engl J Med 2010
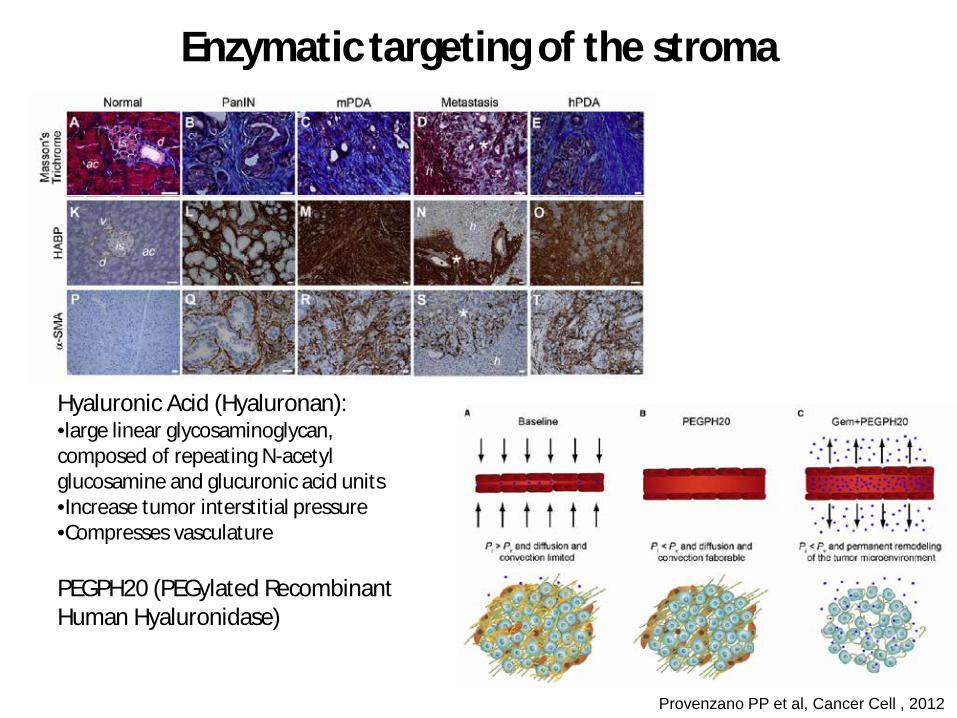
Enzymatic targeting of the stroma
Provenzano PP et al, Cancer Cell , 2012
Hyaluronic Acid (Hyaluronan):•large linear glycosaminoglycan, composed of repeating N-acetyl glucosamine and glucuronic acid units•Increase tumor interstitial pressure•Compresses vasculature
PEGPH20 (PEGylated Recombinant Human Hyaluronidase)

Hingorani, ASCO GI 2015
Phase 1b Study: Increased PFS and OS in High HA Patients treated with PEGPH20 + Gemcitabine

Hingorani, ASCO 2015
PFS in HA-High Patients
Hingorani, ASCO 2015
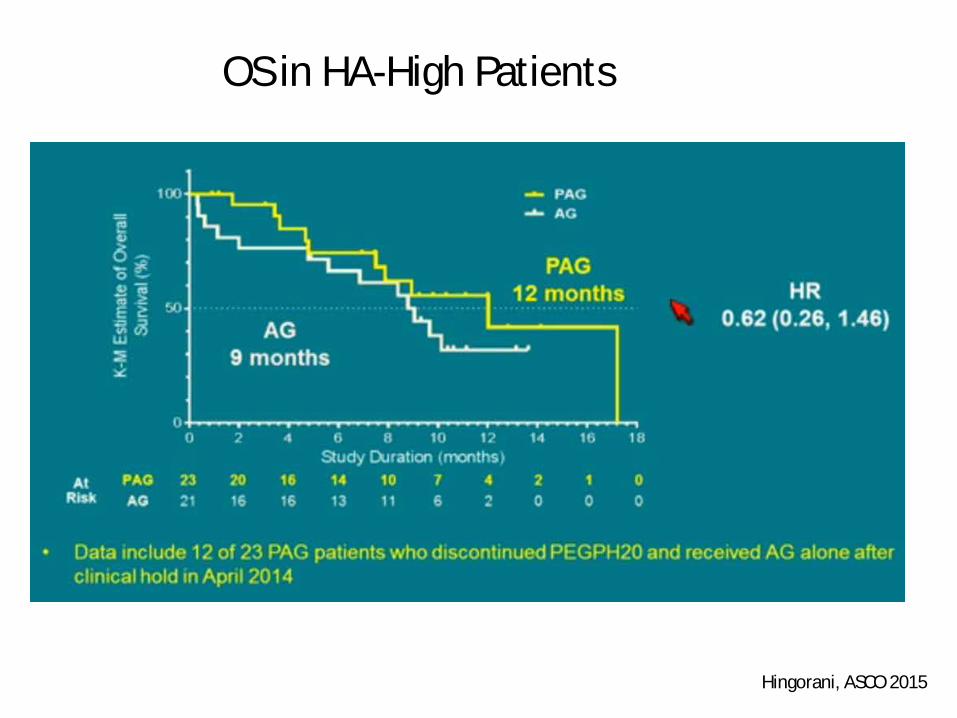
OS in HA-High Patients

Hingorani, ASCO 2015
ORR and DoR in HA-HIGH Patients (Blinded Central review

Yabuuchi S et al. Cancer Lett 2013
Targeting the Notch pathway
Notch Pathway•Receptors:
- Notch-1, -2, -3 & -4•Ligands:
– DLL-1, -3 & -4– JAG-1 & -2
• Mediates intercellular signaling in stem-cell self-renewal, proliferation and differentiation• Activation of Notch-2 & -3 has been implicated in several tumor types including PC
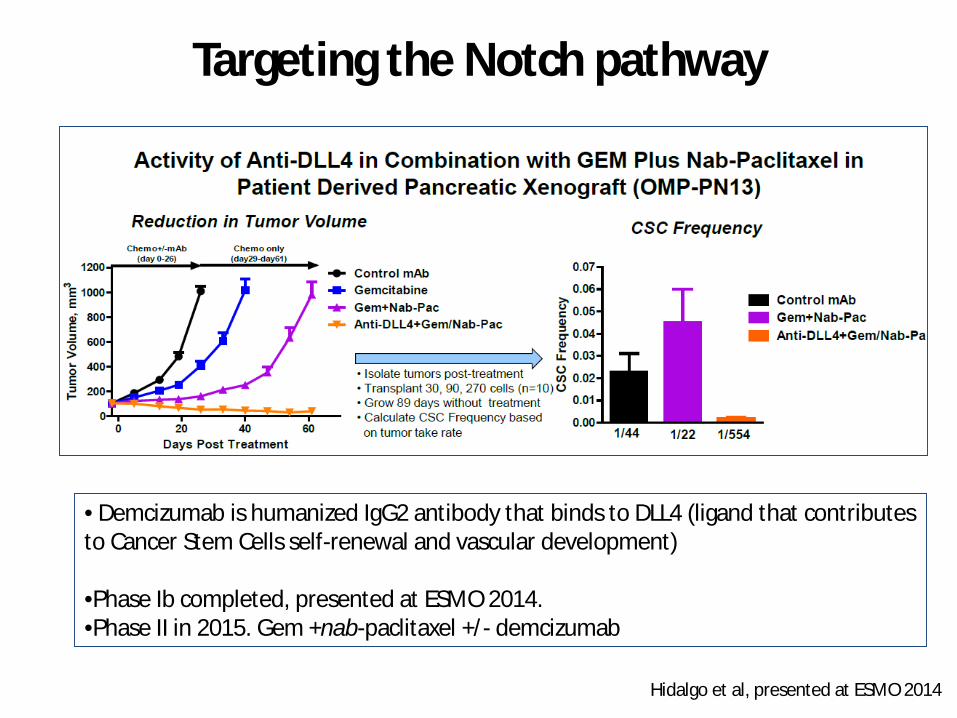
Targeting the Notch pathway
• Demcizumab is humanized IgG2 antibody that binds to DLL4 (ligand that contributes to Cancer Stem Cells self-renewal and vascular development)
•Phase Ib completed, presented at ESMO 2014. •Phase II in 2015. Gem +nab-paclitaxel +/- demcizumab
Hidalgo et al, presented at ESMO 2014

Targeting the Notch pathway
Hidalgo et al, presented at ESMO 2014PR 41%, SD 45%, Clinical benefit rate 86%

Targeting the Notch pathway
Trial MOA Development Phase
Status Line of Therapy
Tarextumab(OMP-59R5) ± Abraxane + Gem
Anti-Notch 2,3 Pathway Inhibitor
Phase Ib/II Currently Recruiting
1st line advanced panc
Demcizumab Abraxane + Gem
Cancer Stem cell target DLL-4 mAb
Phase I/II Phase I completedPhase II in 2015
1st line advanced panc
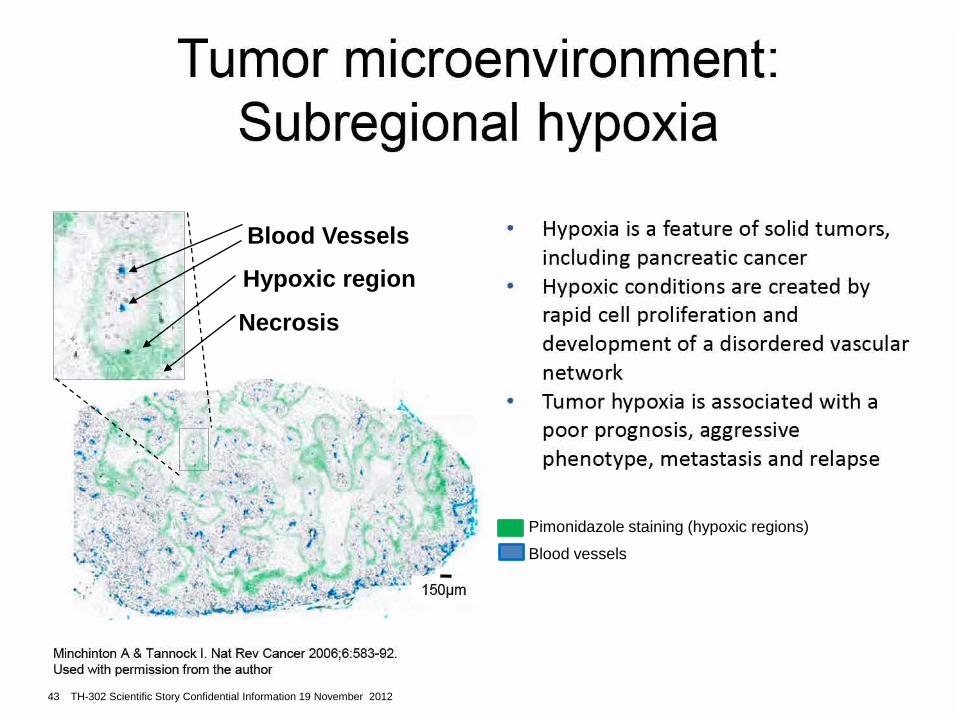
Tumor microenvironment: Subregional hypoxia
• Hypoxia is a feature of solid tumors, including pancreatic cancer
• Hypoxic conditions are created by rapid cell proliferation and development of a disordered vascular network
• Tumor hypoxia is associated with a poor prognosis, aggressive phenotype, metastasis and relapse
Minchinton A & Tannock I. Nat Rev Cancer 2006;6:583-92.Used with permission from the author
150µm
Blood Vessels
Hypoxic region
Necrosis
Pimonidazole staining (hypoxic regions)Blood vessels
43 TH-302 Scientific Story Confidential Information 19 November 2012

Chemotherapy targets oxygenated tumor component
Vessels
Doxorubicin
Hypoxia
Minchinton AI, Tannock IF. Nat Rev Cancer. 2006 Aug;6(8):583-92.Used with permission from the author
• Hypoxia leads to a more aggressive, invasive, metastatic phenotype, and is associated with treatment failure as conventional anti-cancer therapies struggle to penetrate hypoxic areas
44 TH-302 Scientific Story Confidential Information 19 November 2012

Evofosfamide (TH-302) in combination with gemcitabine in previously untreated patients with metastatic or locally advanced unresectable pancreatic ductal adenocarcinoma: primary analysis of the randomized, double-blind phase III MAESTRO study

Randomized, double-blind phase III MAESTRO trial: design

Overall survival

Progression-free survival

ALGORITMO
PACIENTE BUEN ECOGTUMOR CUERPO-COLA
NO PROBLEMAS BILIARES-STENT
PACIENTE BUEN-INTERMEDIO ECOGTUMOR CUERPO-COLA
TUMOR CABEZA SIN PROBLEMAS BILIARES
FOLFIRINOXNAB-PACLITAXEL + GEMCITABINA1ª LINEA
2ª LINEA GEM MonoterapiaGEM CAPE/CISPL
Nab-Paclitaxel
GEM MonoterapiaGEM+CAPE
FOLFOX/FOLFIRINOXMM-398+FUFA
Gemcitabina+ Erlotinib

