prenatal cell free dna screening - kusm-w wesley ob/gyn ob.pdf · prenatal cell free dna screening...
TRANSCRIPT

S H O B A N A K U B E N D R A N , M B B S , M S , C G C
G E N E T I C C O U N S E L O R
A S S T . P R O F E S S O R
D E P T O F P E D I A T R I C S
K U S M W I C H I T A
M A R C H 3 0 , 2 0 1 6
Prenatal Cell Free DNA Screening

Nothing to Disclose!
Not affiliated with any genetic testing laboratory

Acknowledgement
Slides from
NSGC
ACOG
SMFM
Images of technology from laboratory websites

Objectives
Compare cfDNA screening technologies versus conventional screening
Performance and limitations of cfDNA for Common aneuploidy
Microdeletion syndrome
Whole genome
Pre and post test counseling for cfDNA
Educational resources for providers and patients

Terminology
Prenatal cell-free DNA (cfDNA) Screening
Non-invasive Prenatal Screening (NIPS)
Non-invasive Prenatal Testing (NIPT)
FISH – fluorescent insitu hybridization
SNP – single nucleotide polymorphism
Sequencing – reading nucleotide sequence

Where does cell free fetal DNA originate from
1. 2. 3.
18%14%
68%1. Fetus
2. Trophoblast
3. Mesenchyme

In the past 6 months which is your preferred method of prenatal aneuploidy screening for low risk
1. 2. 3. 4.
95%
0%0%5%
1. Quad screen
2. Integrated screen
3. Other analyte screen
4. Cell free fetal DNA

In the past 6 months which is your preferred method of prenatal aneuploidy screening for high risk
1. 2. 3. 4.
6%
67%
0%
28%
1. Quad screen
2. Integrated screen
3. Other analyte screen
4. Cell free fetal DNA

When you order NIPT have you included screening for microdeletion syndromes?
1. 2. 3.
18%
47%
35%
1. Yes
2. No
3. I have not ordered NIPT

I am knowledgeable about microdeletion conditions on the NIPT panel and can explain the pros and cons of screening for those conditions to a patient
1. 2. 3.
0%
13%
87%1. Yes
2. No
3. Somewhat knowledgeable

27 year old has fetal DNA test and it detects T21. The test is 99% sensitive and specific. She is 16 weeks GA and no apparent anomalies on ultrasound. The chance for her to have a
child with Down syndrome is
1. 2. 3. 4.
12%
47%
29%
12%
1. 25%
2. 50%
3. 75%
4. 99%


How is cfDNA screening different than conventional screening?
Uses a DNA-based technology
Can be performed anytime after 9-10 weeks gestation
Differences in conditions screened for
Has higher sensitivity/specificity
Implications of failed screening
Results reporting

Fetal DNA – originates from trophoblast cells of placenta

Opstal et alFalse Negative NIPT Results: Risk Figures for Chromosomes 13, 18 and 21 Based on Chorionic Villi Results in 5967 Cases and Literature Review

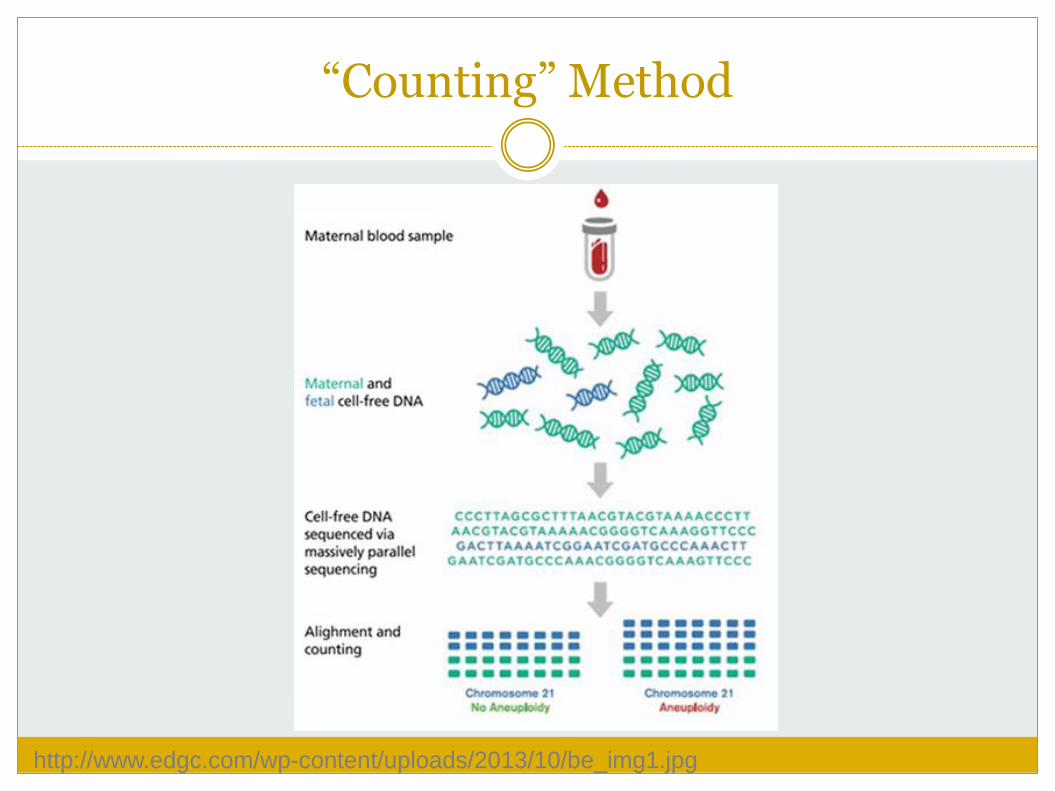
Circulating cell free DNA (cfDNA)
Originates from cells of the trophoblast (placenta)
Once in maternal serum, cells lyse and the chromosomes degrade into small DNA fragments
3-13% of total cell free DNA in maternal serum
Reliably detected >9-10 weeks gestation
Clears from maternal system after birth
Diagrams by Ariosa Diagnostics- http://www.ariosadx.com
http://www.edgc.com/wp-content/uploads/2013/10/be_img1.jpg
“Counting” Method

Genotyping Method
Natera/Panorama/Quest

NIPT Methods and Laboratories
Counting Genotyping
Shotgun MPSS Targeted MPSS SNP
Sequenom (MaterniT21) Ariosa (Harmony) Labcorp (Informaseq)
Natera (Panorama)
Illumina (Verifi) Progenity

Smith et al 2013 Noninvasive screening tools for Down syndrome: a review

Smith et al 2013 Noninvasive screening tools for Down syndrome: a review
Performance Comparison
All tests have a high sensitivity and specificity for trisomy 18 and 21 regardless of which molecular technique is used

NIPT Methods and Laboratories
Counting Genotyping
Shotgun MPSS Targeted MPSS SNP
Sequenom (MaterniT21) (multifetal gestation, egg donor, IVF). Fetal fraction reported
Illumina platform: Ariosa (Harmony); Labcorp (Informaseq) (twin)
Natera (Panorama) (cannot use for multifetal gestations, donor egg). Detects triploidy, vanishing twin
Illumina platform:(Verifi) Progenity (twin) Fetal fraction not reported

Comparison of prenatal screening and diagnostic test options
Test Detection rate for DS
(%)
Detection rate for all
aneuploidies (%)
Screen positive rate (%)
First trimester screen 80 69 5
Sequential/Integrated screen
93 82 5
Cell-free DNA screen 99 72 1-9
(includes no call/test failures)
Chorionic Villus Sampling
>99 >99 1 (includes mosaicism)
Amniocentesis >99 >99 0.2 (includes mosaicism)
SMFM. Prenatal aneuploidy screening with cfDNA. Am J Obstet Gynecol 2015.

Screening for Fetal Aneuploidy
No one screening test is superior to other screening tests in all test characteristics
A discussion of the risks, benefits, and alternatives of various
methods of prenatal screening and diagnostic testing should occur with all patients.
Parallel or simultaneous testing with multiple screening methodologies for aneuploidy is not cost-effective and should not be performed.
Patients may decline all screening or diagnostic testing for
aneuploidy.
How is cfDNA screening different than conventional screening?
Uses a DNA-based technology
Can be performed anytime after 9-10 weeks gestation
Differences in conditions screened for Microdeletions
Whole genome
Has higher sensitivity/specificity particularly for T21
Implications of failed screening
Results reporting

What can cfDNA screen for?
All labs Trisomy 21 (Down syndrome)
Trisomy 18 (Edwards syndrome)
Trisomy 13 (Patau syndrome)

What can cfDNA screen for?
X & Y chromosome variation in singleton pregnancies
Monosomy X (Turner syndrome)
XXY (Klinefelter syndrome)
XXX
XYY

What can cfDNA screen for?
Some labs offer screening for: Triploidy
Trisomy 16
Trisomy 22
Trisomy 9
Specific microdeletion syndromes
22q, 1p36, 4p, 5p, 8q, 11q, 15q

Microdeletion Conditions
Syndrome Incidence Features
22q11.2 1 in 2000 Mild to moderate ID, heart defect, hypocalcemia, immune problems,
Prader Willi 1 in 10,000 Mild to severe ID, behavior problems, hypotonia, obesity
Angelman syndrome 1 in 12,000 Severe ID, no speech, seizures
Cri du chat 1 in 20,000 Moderate to severe ID, behavior problems
1p36 1 in 5000 Severe ID, hearing loss, seizures,
2015 ACOG/SMFM Committee Opinion: Cell-free DNA screening for fetal aneuploidy
Rare conditions Low Positive Predictive Value
Routine cfDNA screening for microdeletion syndromes should not be performed.
cfDNA screening is not recommended for women with multiple gestations.
How is cfDNA screening different than conventional screening?
Uses a DNA-based technology
Can be performed anytime after 9-10 weeks gestation
Differences in conditions screened for Microdeletions
Whole genome
Has higher sensitivity/specificity particularly for T21
Implications of failed screening
Results reporting

How accurate is cfDNA screening?
Gil et al., Ultrasound in Obstetrics & Gynecology 2015; 45: 249-266 * Data from high risk pregnancies. In many studies, cases with mosaicism, complex karyotypes and maternal samples with low fetal fraction were excluded.
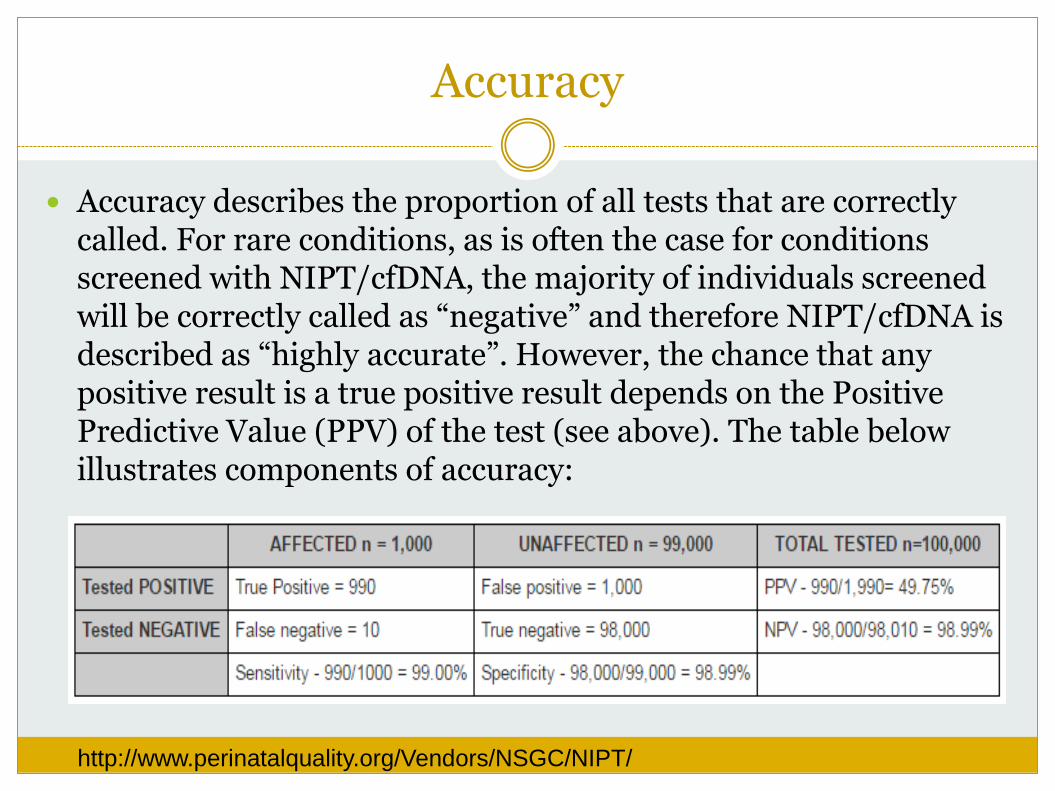
Accuracy
Accuracy describes the proportion of all tests that are correctly called. For rare conditions, as is often the case for conditions screened with NIPT/cfDNA, the majority of individuals screened will be correctly called as “negative” and therefore NIPT/cfDNA is described as “highly accurate”. However, the chance that any positive result is a true positive result depends on the Positive Predictive Value (PPV) of the test (see above). The table below illustrates components of accuracy:
http://www.perinatalquality.org/Vendors/NSGC/NIPT/


Sensitivity and Specificity
Sensitivity refers to the detection rate - the proportion of all individuals with a condition who are correctly identified as “positive” by a screening test. If 1,000 tested individuals have a given condition and 990 of them
test “positive“ for that condition, the test’s sensitivity is 99%. Sensitivity = Detection Rate = 990/1,000 = 99%
Specificity refers to the proportion of all individuals without a condition who are correctly identified as “negative” by a screening test. If 99,000 out of 100,000 unaffected individuals do not have a
condition and 98,000 test “negative”, the test’s specificity is 99%. Specificity = 98,000/99,000 = 99%
http://www.perinatalquality.org/Vendors/NSGC/NIPT/

PPV and NPV
The Positive Predictive Value (PPV) represents the proportion of positive test results that are truly positive. It answers the question: “If my test is positive, what is the chance my baby is affected?” For example, a PPV of 50% indicates that half of the cases in a given population
who have a positive test result are predicted to actually be affected with the condition. Although test sensitivity and specificity are expected to remain the same across a broad population, the PPV of a test varies based on the prevalence of the condition in a given population. The rarer the condition in a given population, the lower the PPV when sensitivity and specificity remain unchanged.
The Negative Predictive Value (NPV) represents the proportion of
negative test results that are truly negative. It answers the question: “If my test is negative, what is the chance that my baby is unaffected?” For example, if the NPV is 99% in a given population, then approximately 99%
of individuals who have a negative test result in that population would be expected to have an unaffected pregnancy. In this example, 1% of women receiving a negative result will have an affected pregnancy (false negative result).

False Positive and False Negative
The False Positive Rate (FPR) reflects the percentage of unaffected cases which test positive. If 1,000 of 99,000 unaffected individuals have a positive test result, the false positive rate is 1,000/99,000 = .01 or 1%.
The False Negative Rate (FNR) reflects the percentage of affected cases which test negative. If 100 of 1,000 affected individuals have a negative test result, the false negative rate in is 100/1,000 = .01 or 1%.
http://www.perinatalquality.org/Vendors/NSGC/NIPT/

Positive and Negative Predictive Value (PPV and NPV)
PPV: the likelihood that a positive test is a true positive
NPV: the likelihood that a negative test is a true negative
Depends on:
the prevalence of the condition
a priori risk age, family history, maternal serum screen results, ultrasound findings, etc.
As the prevalence of disease decreases, so will the PPV

Noninvasive prenatal testing in the general obstetric population: clinical performance and counseling considerations in over 85 000 cases
Prenatal Diagnosis Volume 36, Issue 3, pages 237-243, 27 JAN 2016 DOI: 10.1002/pd.4766 http://onlinelibrary.wiley.com/doi/10.1002/pd.4766/full#pd4766-fig-0003

Positive Predictive Value of cfDNA screening
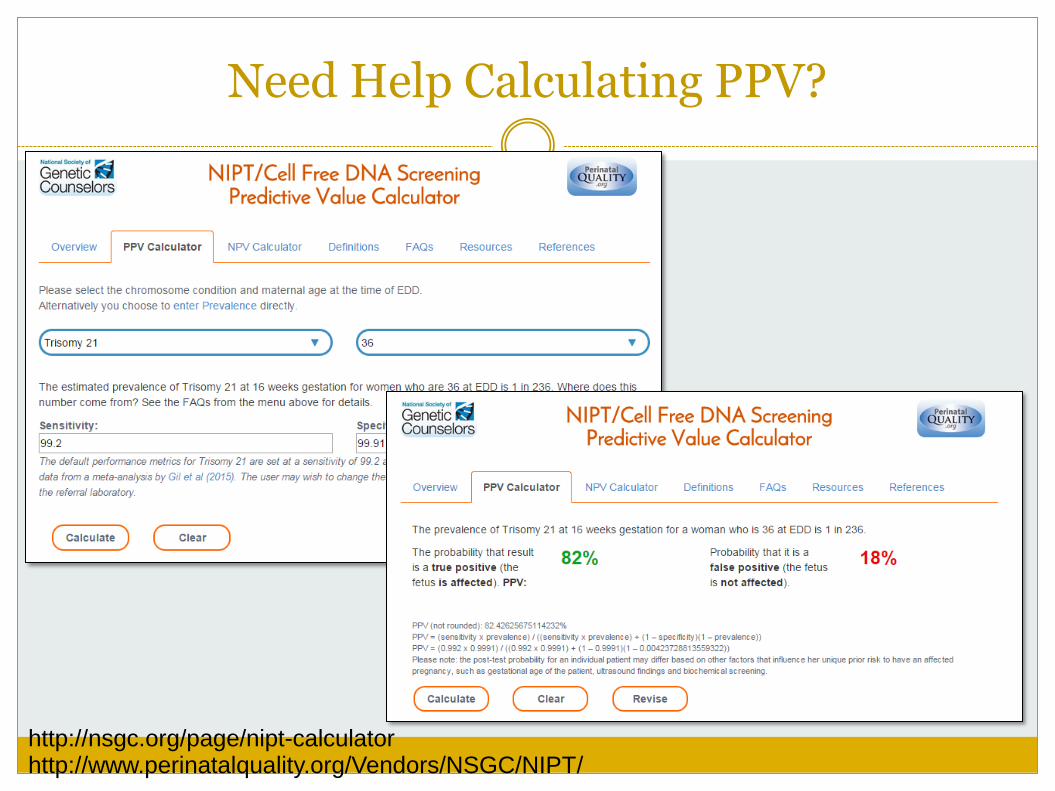
Need Help Calculating PPV?
http://nsgc.org/page/nipt-calculator http://www.perinatalquality.org/Vendors/NSGC/NIPT/

Calculate PPV
https://www.perinatalquality.org/Vendors/NSGC/NIPT/

How is cfDNA screening different than conventional screening?
Uses a DNA-based technology
Can be performed anytime after 9-10 weeks gestation
Differences in conditions screened for Microdeletions
Whole genome
Has higher sensitivity/specificity particularly for T21
Implications of failed screening
Results reporting

“No call” results (screening failure)
Not reported, indeterminate, or uninterpretable results Occurs in 1-8% of patients 50-60% of repeat screens will provide a result Repeat screening may delay diagnosis of aneuploidy
Can be due to: Low fetal fraction Maternal conditions Aneuploidy
Call the performing laboratory for more information

Fetal fraction (the amount of cfDNA coming from the pregnancy)
Lower earlier in gestation
Lower in obese women
Lower in placentas with certain aneuploidies Particularly trisomy 18 and triploidy
Can lead to false negatives

2015 ACOG/SMFM Committee Opinion: Cell-free DNA screening for fetal aneuploidy
Women with a “no call” test result should receive further genetic counseling and be offered comprehensive ultrasound evaluation and diagnostic testing because of an increased risk of aneuploidy.
Patients should be counseled that a negative cfDNA test result does not ensure an unaffected pregnancy.

How is cfDNA screening different than conventional screening?
Uses a DNA-based technology
Can be performed anytime after 9-10 weeks gestation
Differences in conditions screened for
Has higher sensitivity/specificity
Implications of failed screening
Results reporting

Results reporting
Normal
Negative
Low risk (may give specific probability)
No aneuploidy detected

Results reporting

Results reporting
“No call”
No results available
Inconclusive
Unable to interpret

How is cfDNA screening similar to conventional screening?
1. Still a screening test Just as “non-invasive” as other screening tests
Diagnostic testing and genetic counseling is recommended after a positive cfDNA screen
The decision to terminate the pregnancy should not be made based on cfDNA results alone
6% of women with an abnormal NIPT result elected to terminate pregnancy without diagnostic testing

Case Example #1
35yo G2P1 woman with cfDNA test at 10 weeks showing increased risk for trisomy 13
Ultrasound at 12 weeks shows no abnormalities
Patient elects CVS

Case Example #1
Aneuploidy FISH: Mosaic for trisomy 13
Final karyotype: 46, XX
Confined placental mosaicism (CPM) Occurs in ~1% of CVS
Aneuploid --------------------Euploid---------------------
Placenta Fetus
Nondisjunction
Placenta Fetus

How is cfDNA screening similar to conventional screening?
1. Still a screening test
2. False positives and false negatives occur Residual risk for aneuploidy exists after negative result

2015 ACOG/SMFM Committee Opinion: Cell-free DNA screening for fetal aneuploidy
Conventional screening methods remain the most appropriate choice for first-line screening for most women in the general obstetric population due to Limitations of cfDNA screening performance
Limited data on cost-effectiveness in low-risk obstetric population

How is cfDNA screening similar to conventional screening?
Still a screening test
False positives and false negatives occur
Does not screen for all chromosome abnormalities, genetic conditions or birth defects
What doesn’t cfDNA screen for?
All known chromosome abnormalities 50-75% of aneuploidy in high risk population is Down syndrome, trisomy
18, or trisomy 13
Cannot differentiate between non-disjunction trisomy, translocation, mosaic
2% of pregnancies with an abnormal traditional screen and a normal cfDNA screen are found to have a chromosomal abnormality
All genetic conditions Single gene disorders, such as cystic fibrosis or achondroplasia, cannot be
identified
Family history should be evaluated to determine if patient should be offered other testing options for a particular disorder
What doesn’t cfDNA screen for?
Birth defects Such as neural tube defects, congenital heart defects, etc. cannot be
identified
Ultrasound and MSAFP-only should still be considered
If a fetal structural anomaly is identified on ultrasound examination, diagnostic testing should be offered rather than cfDNA screening

Case Example #2
Positive quad for trisomy 18 @ 17 weeks Low uE3
Low risk cfDNA result
Multiple congenital anomalies noted @ 20 week ultrasound

Case Example #2
Patient undergoes amniocentesis 46,XY
Normal chromosome microarray
Amniotic fluid sent for additional testing confirms diagnosis of Smith-Lemli-Opitz Syndrome (SLOS)
Take home message: cfDNA cannot screen for everything-
If a fetal structural anomaly is identified on ultrasound, diagnostic testing should be offered rather than cell-free
DNA screening 2015 ACOG/SMFM Committee Opinion: Cell-free DNA screening for fetal aneuploidy

Discordant NIPT Case
20 year old – NIPT – trisomy 13. 18 week ultrasound - no anomalies on fetus
20 week amnio – Turner syndrome
Coarctation aorta detected at birth
31 year old – NIPT – triple X 20 week amnio – fetus is normal female
31 year old karyotype – triple X!
2 cases of screen positive for 22q11 deletion One confirmed
Second negative

How do you implement cfDNA screening into your practice?

How do you implement cfDNA screening into your practice?
Pre-screen counseling for all patients is imperative
Can be challenging due to Time constraints
Rapid advances
Patients’ focus on fetal sex

Counseling patients
Talk to your patients: If their pregnancy was affected with a genetic disorder or
chromosome abnormality, would they want to know?
What would the information mean to them?

Counseling patients
Review reasons why patients would choose to accept screening Preparation
Termination
Review reasons why patients would decline screening Would not terminate
Would cause unwanted stress or worry

Counseling patients
“I don’t want any testing
that may cause a miscarriage”
Most women fall
somewhere in the middle
“I would terminate a pregnancy
with any major problem”
Fear of Miscarriage Fear of Abnormality

Informed consent
Patients need to know: They can decline all screening or diagnostic testing
for aneuploidy
cfDNA is a screening test and diagnostic testing is recommended for confirmation of positive results
Accuracy of cfDNA screening
What conditions are (and are not) being screened for
The possibility of a “no call” result

Post-test counseling
Normal results: Should be disclosed by a medical professional designated to
review this information
“Low risk”, not “no risk” for conditions on the panel
Still have option to have diagnostic testing
Still be offered MSAFP screening or ultrasound evaluation

Post-test counseling
Abnormal results or “No Call” results NOT diagnostic
Comprehensive ultrasound and diagnostic testing should be offered
Refer to a genetic counselor or MFM specialist
Dar P, Curnow KJ, Gross SJ, Hall MP, Stosic M, Demko Z, et al. Clinical experience and follow-up with large scale single-nucleotide polymorphism-based noninvasive prenatal aneuploidy testing. Am J Obstet Gynecol 2014;

Agarwal et al 2014 Commercial Landscape of noninvasive prenatal testing in the United States


I found this presentation
1 2 3
33% 33%33%
1. Informative and will enable me to order NIPT appropriately
2. Need more information
3. Too much information

Resources Fact sheets SMFM: https://www.smfm.org/publications/189-prenatal-aneuploidy-screening-using-
cell-free-dna NSGC:
Provider fact sheets: http://nsgc.org/page/non-invasive-prenatal-testing-healthcare-providers http://nsgc.org/page/abnormal-non-invasive-prenatal-testing-results
Patient fact sheet: http://nsgc.org/d/do/4584
Perinatal Quality Foundation/National Society of Genetic Counselors Online Predictive Value Calculator: http://nsgc.org/page/nipt-calculator
Lettercase: Prenatal Screening and Testing for Chromosome Conditions: http://www.lettercase.org/prenataltesting/
Genetics Support Foundation Patient video: https://www.geneticsupportfoundation.org/genetics-and-you/pregnancy-
and-genetics/noninvasive-prenatal-testing-the-real-deal-and-what-you-need-to-know
Society for Maternal-Fetal Medicine (SMFM) Consult Series #36: Prenatal aneuploidy screening using cell-free DNA: http://www.ajog.org/article/S0002-9378(15)00324-5/pdf
ACOG & SMFM Joint Committee Opinion: Noninvasive Prenatal Testing for Fetal Aneuploidy: http://www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Genetics/Cell-free-DNA-Screening-for-Fetal-Aneuploidy
ACOG: More Information: For Committee Opinion #640—Cell-free DNA (cfDNA) Screening for Fetal Aneuploidy: www.acog.org/More-Info/cfDNA

Acknowledgements
NSGC
Cori Feist
Shannon Wieloch
Katie Stoll
ACOG
Joseph Biggio
Britt Rink
SMFM
Mary Norton
Sean Blackwell


References
Lo et al (2010), Maternal plasma DNA sequencing reveals the genome wide genetic and mutational profile of the fetus. Science and Translational Medicine. 2, 61.
Nicolaides et al (2012), Noninvasive prenatal testing for fetal trisomies in a routinely screened first-trimester population. American Journal of Obstetrics and Gynecology. 207, 374.
Wang et al (2013), Gestational age and maternal weight effects on fetal cell-free DNA in maternal plasma. Prenatal Diagnosis. 33, 661-666.
Vora and O’Brien (2014), Noninvasive prenatal testing for microdeletion syndromes and expanded trisomies. Obstetrics and Gynecology, 123, 1097- 1099.
Wang et al (2014), Maternal mosaicism is a significant contributor to discordant sex chromosomal aneuploidies associated with noninvasive prenatal testing. Clinical Chemistry, 60, 251-259.
Gil et al (2015), Analysis of cell free DNA in maternal blood in screening for fetal aneuploidies: an updated meta-analysis. Ultrasound in Obstetrics and Gynecology. 45; 249-266.
Norton et al (2015), Cell-free DNA analysis for noninvasive examination of trisomy. New England Journal of Medicine.
SMFM Publications Committee (2015), Prenatal aneuploidy screening using cell-free DNA. American Journal of Obstetrics & Gynecology
ACOG Committee on Genetics & SMFM, Joint Committee Opinion #640 (2015): Cell-free DNA Screening for Fetal Aneuploidy. Published ahead of print.
Questions?