prenatal aneuploidy screening using cell free dna · prenatal aneuploidy screening using cell free...
TRANSCRIPT

10/15/2015
1
Prenatal Aneuploidy Screening Using cell Free DNA
Mary E. Norton MDProfessor, Obstetrics,
Gynecology and Reproductive Sciences
University of California, San Francisco
What Does the Evidence Tell Us? Oct 2015
Disclosures
o Research support from Natera and Ariosa
o No lucrative personal financial contracts
020406080
100120
Detection rate of prenatal screening for Down syndrome has improved over time
Det
ectio
n R
ate
(%)
The questions being debated:
o Is cfDNA screening the best option for low risk patients?
o Is cfDNA screening the best choice for primaryscreening for any or all patients?

10/15/2015
2
Professional Society Opinions: ACOG; ACMG; International Society of Prenatal Diagnosis;
National Society of Genetic CounselorsCommon themes (2012):There are recognized benefits, but…o Not diagnostic
• Needs confirmationo Only detects common trisomieso Requires comprehensive genetic counselingo Should only be used in validated groups (eg high risk)o Need a low risk study before introducing into general
population screening
Rumsfeld on current status of NIPT?“There are known knowns. There are things we know, we know. We also know there are known unknowns. That is to say, we know there are some things we do not know. But there are also unknown unknowns. The ones we don’t know we don’t know.”
-Donald Rumsfeld, 2002
Cell free fetal DNA
o Short segments of fetal DNA (<200 base pairs) circulate in maternal plasma
o Origin is primarily placenta
Maternal DNA
Fetal DNA
Cell free DNA results from apoptosis

10/15/2015
3
Analysis of cell free DNA
Zhong, X, Holzgreve, W, Glob. libr. women's med 2009
Trisomy 21 Non-Trisomy 21
DR: 99.2% (98.5 - 99.6)FPR: 0.09% (0.05 - 0.13)
Trisomy 21 performance cfDNA testing: meta-analysis (Gil et al, Ultrasound Obstet Gynecol, 2015)
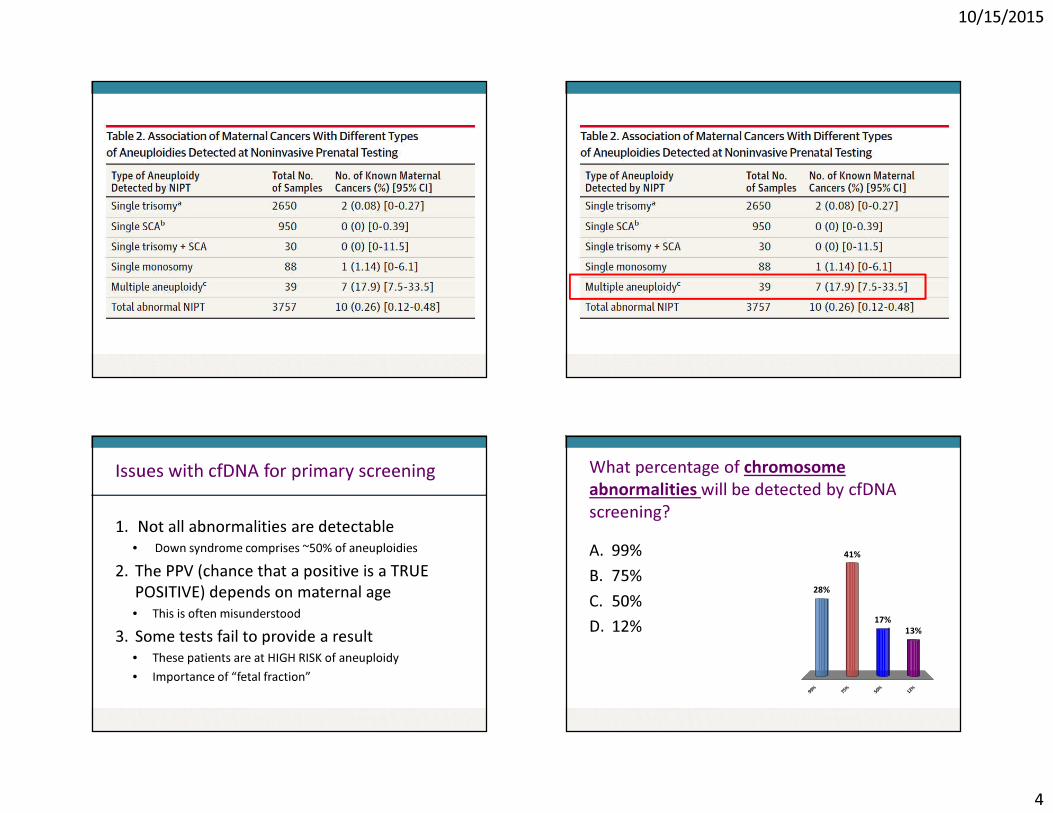
Cell free DNA: Biologic ChallengesFalse positives:o Unrecognized or vanishing twino Placental mosaicismo Maternal genetic variation o Maternal malignancyFalse negatives:o Low level of fetal DNA o Placental mosaicismo Maternal genetic variation Failed results: o Increased BMIo Low level of fetal DNAo Fetal aneuploidy
False positive cfDNA results and cancer
10/15/2015
4
Issues with cfDNA for primary screening
1. Not all abnormalities are detectable• Down syndrome comprises ~50% of aneuploidies
2. The PPV (chance that a positive is a TRUE POSITIVE) depends on maternal age• This is often misunderstood
3. Some tests fail to provide a result• These patients are at HIGH RISK of aneuploidy• Importance of “fetal fraction”
What percentage of chromosome abnormalities will be detected by cfDNAscreening?A. 99%B. 75%C. 50%D. 12%
9 9 % 7 5 % 5 0 % 1 2 %
28%
13%17%
41%

10/15/2015
5
Spectrum of Genetic Disease
Structural Malformations
Autosomal recessiveAutosomal dominant
X-linked
Chromosomal/karyotype
CNV (microarray)
Spectrum of Genetic Disease
Structural Malformations
Autosomal recessiveAutosomal dominant
X-linked
Chromosomal/karyotype
CNV (microarray)
Aneuploidies Present in HIGH RISK Women
Tri 21: 53.2%Sex chromosomal: 8.2%
Tri 13: 4.6%
Tri 18: 17.0%
Other*16.9%
Norton et al, SMFM, 2014
*Not detected by cfDNA
Aneuploidies Present in LOW RISK Women
Tri 21: 49.2%
Sex chromosomal: 9.9%
Tri 13: 5.5%
Tri 18:12.9%
Other*20.8%
Norton et al, SMFM, 2015
*Not detected by cfDNA

10/15/2015
6
Rate of abnormalities by maternal age cfDNA Detection Raten=452,901 patients screened in California
Total Cases with Aneuploidy (n=2575)
cfDNADetectable
Not Detected No Result
N=69+560(24.5%)
N=1841(71.4%)
N=105(4.1%)
Not Detectable(False negative+Non-detectable)
In low-risk patients, this is a very accurate test for a rare event.

10/15/2015
7
NIPT and diagnostic testing with chromosomal microarray (CMA)
Microarray detects an abnormality in 1.7% of cases (about 1/60)AND:
NIPT detects T13,18, 21 – about 1/500 pregnanciesTHEN:
� If NIPT is the routine screening test, it will detect about 12% of diagnosable chromosomal abnormalities
NIPT and diagnostic testing with chromosomal microarray (CMA)
Microarray detects an abnormality in 1.7% of cases (about 1/60)AND:
NIPT detects T13,18, 21 – about 1/500 pregnanciesTHEN:
� If NIPT is the routine screening test, it will detect about 12% of diagnosable chromosomal abnormalities
NIPT and diagnostic testing with chromosomal microarray (CMA)
Microarray detects an abnormality in 1.7% of cases (about 1/60)AND:
NIPT detects T13,18, 21 – about 1/500 pregnanciesTHEN:
� If NIPT is the routine screening test, it will detect about 12% of diagnosable chromosomal abnormalities
Your 25 yo patient has cfDNA screening and the result is positive for trisomy 13. What is the chance that the fetus actually has trisomy 13?A. >99%B. 75%C. 50%D. <10%
> 9 9%
7 5%
5 0%
< 1 0%
34%
28%
17%21%

10/15/2015
8
o N=1914 women undergoing standard screeningo Mean maternal age = 29.6 yrso Primary outcome = false positive rates for T18 and T21
cfDNA vs Standard Screening
Bianchi et al, NEJM, 2014
FPR PPVcfDNA 0.3% 45.5% p<.001Standard 3.6% 4.2%
o Only 8 aneuploidy cases in the cohort (5: T21, 2: T18, and 1: T13)
o All were detected
o 15,841 women had cfDNA and first trimester screening
o Mean maternal age = 30.7 yrs
“NEXT” study: 15,841 average risk women
Cell free DNA
screening
First trimester screening
Detection rate 38/38 (100%)
30/38 (79%) P=0.008
False positive rate
0.06% 5.4% P<0.0001
Positive predictivevalue
81% 3.4% P<0.0001
Norton et al, NEJM, 2015

10/15/2015
9
Wang et al, Genetics in Medicine, 2014
Aneuploidy No. of positives No (%)confirmed
T21 41 38/41 (93%)T18 25 16/25 (64%)T13 16 7/16 (44%)45X 16 6/16 (38%)
Total 98 67 (67%)
o 6.2% had termination without karyotype confirmation
o Disconcerting if only 67% are true positives

10/15/2015
10
Consequences of false positive results
N=100,000 1% false positives
1000 abnormal results6.2% TAB w/o confirmation
62 TAB
42 TP 21 FP
21 TAB of normal fetuses
NIPT
67% PPV
Consequences of false positive results
N=100,0005% false positives
5000 abnormal results
0.2% loss rate (amnio)
10 losses of normal fetuses
N=100,000 1% false positives
1000 abnormal results6.2% TAB w/o confirmation
62 TAB
42 TP 21 FP
21 TAB of normal fetuses
NIPT Serum Screening
67% PPV
If your patient has a positive result:www.perinatalquality.org

10/15/2015
11
The poorly understood PPV Your patient has cfDNA screening, and the lab calls to tell you the test failed to provide a result. What are possible reasons for this?
A. Maternal obesityB. The fetus has a chromosome
abnormalityC. The blood was drawn too earlyD. All of the above
M at e r n
a l ob e s
i t y
T h e f e t
u s ha s a
c h ro m
o . . .T h e
b l oo d
w a s d r a
w n t . .
A l l o f t
h e a b o
v e
16%
71%
12%1%

10/15/2015
12
Published Trials of NIPT: failure ratesTrial Failure rate
Chiu et al (2011) 11/764 (1.4%)Ehrich et al. (2011) 18/467 (3.8%)Palomaki et al. (2011) 13/1696 (0.8%)Bianchi et al. (2012) 30/532 (3.0%)Norton et al (2012) 148/3228 (4.6%)Zimmermann et al (2012) 21/166 (12.6%)Pergament et al (2014) 85/1051 (8%)Norton et al (2015) 488/16,329 (3.0%)
All 729/23,182 (3.1%)
Fetal fraction of DNA and test failure
3-5% of samples do not provide a result
• Low fraction fetal DNA, failed sequencing, high variability in counts
• Some association with gestational age (<10 wks) • Low fetal fraction associated with maternal BMI
- 20% at >250 lbs- 50% at >350 lbs
� Low fetal fraction is associated with aneuploidy�Repeating test will provide a result in SOME cases
Obesity in US Adults Pergament et al, 2014
o N=1051 samples were analyzed
o N=85/1051 (8%) samples failed to obtain a result
o 20/85 (22%) were aneuploid
�“No call” cases represent a very high risk group
Obstet Gynecol 2014

10/15/2015
13
No ResultsN = 102(2.3%)
Total Pregnancies SampledN = 4446
Redraw Declined N=39
High Risk N = 157(3.5%)
RedrawnN = 63
Low RiskN = 4187(94.2%)
Low RiskN=32 (50.8%)
High Risk N=5 (7.9%)
No ResultN=26(41.3%)
NO FINAL RESULTN = 65 (1.5%)
Kaiser cfDNA Experience: No Results Cases
No ResultsN = 102(2.3%)
Total Pregnancies SampledN = 4446
Redraw Declined N=39
High Risk N = 157(3.5%)
RedrawnN = 63
Low RiskN = 4187(94.2%)
Low RiskN=32 (50.8%)
High Risk N=5 (7.9%)
No ResultN=26(41.3%)
NO FINAL RESULTN = 65 (1.5%)
Kaiser cfDNA Experience: No Results Cases
No ResultsN = 102(2.3%)
Total Pregnancies SampledN = 4446
Redraw Declined N=39
High Risk N = 157(3.5%)
RedrawnN = 63
Low RiskN = 4187(94.2%)
Low RiskN=32 (50.8%)
High Risk N=5 (7.9%)
No ResultN=26(41.3%)
NO FINAL RESULTN = 65 (1.5%)
Kaiser cfDNA Experience: No Results Cases
KPNC 10/29/12 – 6/30/14Total pregnancies sampled = 4446
Abnormal chromosomes 9/65 (14%)
Normal chromosomes13/65 (20%)
Chromosomes not done43/65 (66%)
Kaiser cfDNA: No Results
NO FINAL RESULTN = 65 (1.5%)

10/15/2015
14
Failed cfDNA screens indicate increased risk for aneuploidy
Failed tests increase aneuploidy risk:
Author OR for aneuploidyo Norton et al, NEJM 2015: 6.2o Pergament et al, Obstet Gynecol 2014: 2.5o Turocy et al, SMFM 2015: 5.7
The questions being debated:
o Is cfDNA screening the best option for low risk patients?
o Is cfDNA screening the best choice for primaryscreening for any or all patients?
NIPT is more precise for T13, 18, 21
cfDNA Current NT + serum screen
NIPT is more precise for T13, 18, 21
cfDNA Current NT + serum screen
Other abnormalities

10/15/2015
15
cfDNA vs Sequential Screening:Detection and False Positive Rates
Cohort Detection Rate
False Positive Rate
Sequential screening
81.6% 4.5%
cfDNA if “no results” cases = high risk
77.1% 3.7%
cfDNA if “no results” have no follow up
70.7% 0.7%
cfDNA and Ultrasound Abnormalities
Normal U/S Abnormal U/ST13, 18, 21 25 (4.9%) 88 (23.4%)Other chromosomalabnormalities
13 (2.5%) 29 (7.7%)
Total detectable cfDNA
25/38 (66%) 88/117 (75%)
Benachi et al, Obstet Gynecol, 2015
NIPT: Expanded panelsLaboratories have added other trisomies and microdeletionso Trisomies 16 and 22o Microdeletion syndromes
• 22q (diGeorge)• 5p (cri-du-chat)• 1p36• 15q (Prader Willi)• 4p (Wolf-Hirshhorn)
NIPT: Expanded panels
o Trisomies 16 and 22• Rarely seen in viable pregnancies except as mosaics• Common causes of confined placental mosaicism
- Much more common in CVS samples than amniocentesis• Even complete trisomy in the placenta often
associated with a normal fetus• With both, confined placental mosaicism can be
associated with IUGR, so false positive cases should be followed for fetal growth (eg ultrasound at 30-32 wks)

10/15/2015
16
Microdeletion syndromes are rareSyndrome Frequency Features22q11.2 (DiGeorge)
1/4,000 Varies: cardiac, palatal, immune, intellectual disability
1q36 1/10,000 Severe intellectual disability (ID), +/- obvious structural anomalies
Angelman 1/20,000 Severe ID, seizures, speech delay
Prader-Willi 1/30,000 Obesity, ID, behavioral problems
Cri-du-chat 1/50,000 Microcephaly, ID, +/- CHDWolf-Hirshhorn 1/50,000 ID, seizures, +/- CL/CP
Testing for Rare Disorders
N=100,000
2 Wolf-Hirschhorn 99,998 not WHS
2 TP; 0 FN 800 FP; 99,198 TN
OAPR = 1/400
Population Risk = 1/50,000(Wolf-Hirschhorn, 4p-: Assume 99% sensitivity and 99.2% specificity)
ACOG/SMFM September 2015o Conventional screening is most appropriate
first line screen for most patientso Ethically any patient may choose cfDNA
screening, but should be counseled regarding limitations and benefits
o Diagnostic testing is required to confirm abnormal results before irreversible decisions
o Testing for microdeletions and in twins should not be performed
10/15/2015
17
Important counseling points
o NIPT is NOT diagnostico Extremely high sensitivity and specificity for
Down syndrome o Somewhat lower for trisomy 13, 18 and sex
chromosomeso Approximately 20-30% of chromosome
abnormalities identified with invasive testing are NOT detectable with NIPT
All patients deserve equal access
o ACOG indicates that testing should no longer be stratified by maternal age
o We’ve spent the past decade trying to abolish “advanced maternal age” and the 35 yo cutoff
o It is unethical to withhold this test
All patients deserve equal access
o ACOG indicates that testing should no longer be stratified by maternal age
o We’ve spent the past decade trying to abolish “advanced maternal age” and the 35 yo cutoff
o It is unethical to withhold this test�There is a difference between withholding
something for an individual patient, and recommending it for all patients as policy
All patients should have access to all test options…(the Jim Carrey approach)

10/15/2015
18
Ethics, access and counselingo While it is not ethical to withhold tests from one
groupo It is necessary to provide fair and balanced
counseling regarding the pros and cons of ALL test options• cfDNA is very good for the common aneuploidies, but
doesn’t detect other serious chromosome abnormalities
• In low risk patients, a positive result is more likely to be a false positive
• In patients at low risk for the common aneuploidies, other screening options provide broader coverage at lower cost
Appropriate counselingo While it is not ethical to withhold tests from one
groupo It is necessary to provide fair and balanced
counseling regarding the pros and cons of ALL test options• cfDNA is very good for the common aneuploidies, but
doesn’t detect other serious chromosome abnormalities
• In low risk patients, a positive result is more likely to be a false positive
• In patients at low risk for the common aneuploidies, other screening options provide broader coverage at lower cost
Appropriate counselingo While it is not ethical to withhold tests from one
groupo It is necessary to provide fair and balanced
counseling regarding the pros and cons of ALL test options• cfDNA is very good for the common aneuploidies, but
doesn’t detect other serious chromosome abnormalities
• In low risk patients, a positive result is more likely to be a false positive
• In patients at low risk for the common aneuploidies, other screening options provide broader coverage at lower cost
Appropriate counselingo While it is not ethical to withhold tests from one
groupo It is necessary to provide fair and balanced
counseling regarding the pros and cons of ALL test options• cfDNA is very good for the common aneuploidies, but
doesn’t detect other serious chromosome abnormalities
• In low risk patients, a positive result is more likely to be a false positive
• In patients at low risk for the common aneuploidies, other screening options provide broader coverage for more conditions

10/15/2015
19
Thank You!