preliminary experience with pure antiestrogens...
TRANSCRIPT

Vol. 7, 4369s-4375s, December 2001 (Suppl.) Clinical Cancer Research 4369s
Preliminary Experience with Pure Antiestrogens 1
Anthony Howell z CRC Department of Medical Oncology, University of Manchester, Christie Hospital, Manchester M20 4BX, United Kingdom
Abstract Endocrine therapy plays an important role in the man-
agement of all stages of breast cancer, and the development of effective endocrine therapies has focused on modifying the response of hormone-sensitive tumors to estrogen. The most widely used agents are the nonsteroidal antiestrogens or selective estrogen receptor (ER) modulators, the class to which tamoxifen, the standard in terms of antiestrogen ther- apy, belongs. Tamoxifen is effective in both adjuvant and first-line settings and is now used as prophylactic therapy in high-risk individuals. However, the partial agonist activity of tamoxifen on the uterus, coupled with "tumor flare" and the development of tamoxifen resistance, has limited its therapeutic utility. Attempts to eliminate the partial agonist activity of tamoxifen and increase its potency have led to the development of fulvestrant (Faslodex), the first in a new class of pure antiestrogens, the ER down-regulators. Fulves- trant has a high affinity for the ER compared with tamox- ifen but has none of the agonist activities of tamoxifen. This new agent is showing promising clinical activity in the treat- ment of advanced breast cancer after tamoxifen therapy. Fulvestrant's lack of ER agonist activity may provide a longer duration of response compared with tamoxifen, as it did in a preclinical setting. Fulvestrant has demonstrated that it is at least as effective as the third-generation aro- matase inhibitor anastrozole in patients whose disease has relapsed or recurred on prior endocrine therapy and is currently being evaluated in Phase III trials v e r s u s tamox- ifen for the first-line therapy of advanced breast cancer. Future clinical studies will evaluate fulvestrant in adjuvant and neoadjuvant settings, together with its optimal sequenc- ing in relation to tamoxifen and other endocrine therapies.
Introduction Antiestrogen therapy, and tamoxifen in particular, has im-
proved the treatment of all stages of breast cancer over the last 3 decades (1). The term "antiestrogen" encompasses all agents that antagonize the physiological effects of the female hormone estrogen or 1713-estradiol. Tamoxifen (Nolvadex), a nonsteroi- dal, triphenylethylene-based antiestrogen (Fig. 1) with tissue-
1 Presented at the First International Conference on Recent Advances and Future Directions in Endocrine Therapy for Breast Cancer, June 21-23, 2001, Cambridge, MA. 2 To whom requests for reprints should be addressed, at CRC Depart- ment of Medical Oncology, University of Manchester, Christie Hospital, Wilmslow Road, Withington, Manchester M20 4BX, United Kingdom. Phone: 44-(0)161-446-8037; Fax: 44-(0)161-446-3299; E-mail: mafia. parker@ christie-tr.nwest.nhs.uk.
specific estrogenic (agonist) and antiestrogenic (antagonist) ac- tivity, has been the antiestrogen of choice in the clinic for over 25 years. The biological effects of tamoxifen are mediated primarily by inhibiting the actions of estrogen mediated through its binding to the ER. 3 The antiestrogenic activity of tamoxifen in the breast has established it as the standard for the treatment of all stages of breast cancer. Tamoxifen given for different durations in an adjuvant setting has been associated with an up to 47% reduction in the risk of contralateral breast cancer (2) and a 45% reduction in invasive cancer in patients with ductal carcinoma in situ (3). Furthermore, the prospective evaluation of tamoxifen for the prevention of cancer in high-risk women in the National Surgical Adjuvant Breast and Bowel Project P1 breast cancer prevention study (4) showed tamoxifen to reduce the relative risk of invasive cancer by 49% in all age groups. Although these observations have not been confirmed in two European studies, tamoxifen has been approved by the Food and Drug Administration for breast cancer prevention in high-risk individuals (5).
Long-term tamoxifen treatment is associated with at least two other clinical benefits normally associated with endogenous systemic estrogen. These are the maintenance of bone density (6, 7) and the lowering of circulating low-density lipoprotein cholesterol (8) with a beneficial effect on cardiovascular disease (5, 9), both issues of importance to perimenopausal and postm- enopausal women. However, tamoxifen is also associated with a slight increase in the risk of endometrial cancer (4, 9, 10) and as yet unsubstantiated concerns over second malignancies (11). These observations are of particular concern when tamoxifen is used in an adjuvant setting because patients may be receiving therapy for up to 5 years. Tamoxifen is also associated with a tumor-stimulatory effect, sometimes seen as a transient flare at the start of treatment (12), and perhaps most importantly with the acquisition of "tamoxifen resistance," in which tamoxifen no longer inhibits tumor growth and, in some cases, actually pro- motes it (13). Antiestrogen therapy is also associated with an increased incidence of thromboembolic phenomena, including deep-vein thrombosis, pulmonary embolism, and possibly cere- brovascular events (14, 15). The most common serious adverse event with tamoxifen is thromboembolism (4). However, de- spite these negative aspects of tamoxifen therapy, the benefits for the treatment and prevention of breast cancer are considered to substantially outweigh the risks.
Furthermore, the success of tamoxifen in the treatment of breast cancer has proved invaluable in the search for and devel- opment of new antiestrogens that selectively retain the favorable estrogenic and antiestrogenic properties of tamoxifen. In fact, it is the standard against which all new endocrine therapies, in-
3 The abbreviations used are: ER, estrogen receptor; SERM, selective estrogen receptor modulator; ERD, ER down-regulator; PgR, progester- one receptor; ERE, estrogen response element; ROW, Rest of the World.
Research. on June 11, 2018. © 2001 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
4370s Fulvestrant (Faslodex) in Breast Cancer Therapy
Tamoxifen Toremifene
~ N M ~ ~NMe=
Cl
Raloxifene Fulvestrant
o
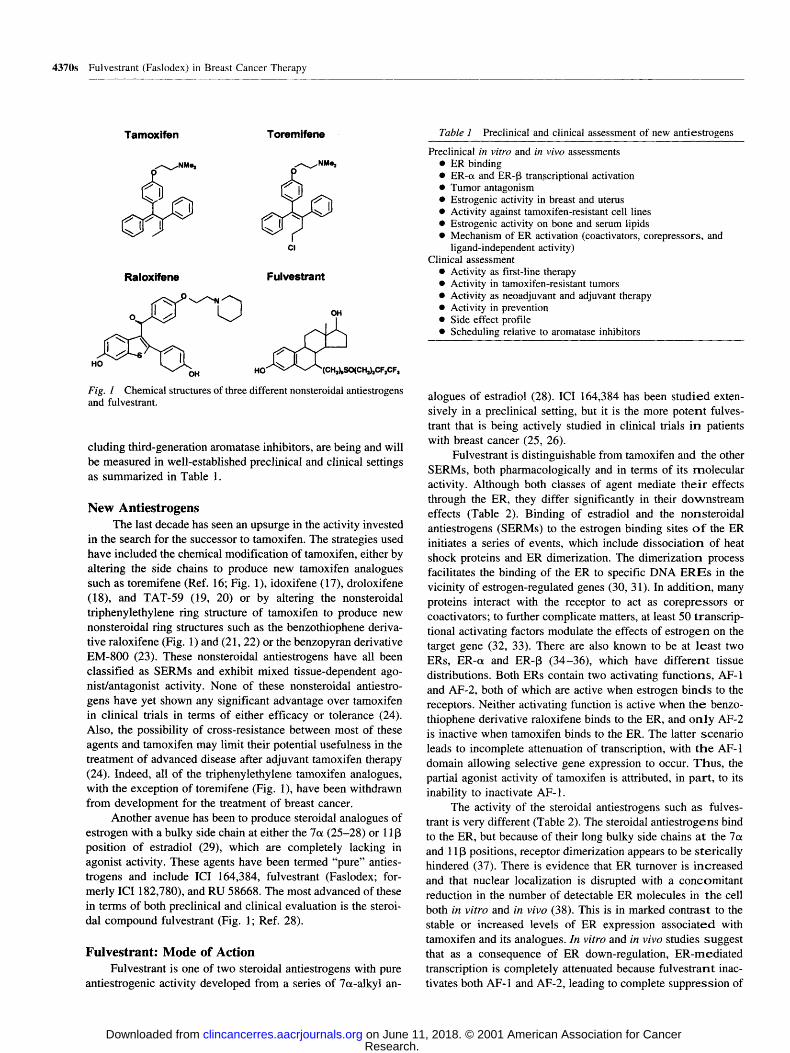
Fig. 1 Chemical structures of three different nonsteroidal antiestrogens and fulvestrant.
cluding third-generation aromatase inhibitors, are being and will be measured in well-established preclinical and clinical settings as summarized in Table 1.
New Antiestrogens The last decade has seen an upsurge in the activity invested
in the search for the successor to tamoxifen. The strategies used have included the chemical modification of tamoxifen, either by altering the side chains to produce new tamoxifen analogues such as toremifene (Ref. 16; Fig. 1), idoxifene (17), droloxifene (18), and TAT-59 (19, 20) or by altering the nonsteroidal triphenylethylene ring structure of tamoxifen to produce new nonsteroidal ring structures such as the benzothiophene deriva- tive raloxifene (Fig. 1) and (21, 22) or the benzopyran derivative EM-800 (23). These nonsteroidal antiestrogens have all been classified as SERMs and exhibit mixed tissue-dependent ago- nist/antagonist activity. None of these nonsteroidal antiestro- gens have yet shown any significant advantage over tamoxifen in clinical trials in terms of either efficacy or tolerance (24). Also, the possibility of cross-resistance between most of these agents and tamoxifen may limit their potential usefulness in the treatment of advanced disease after adjuvant tamoxifen therapy (24). Indeed, all of the triphenylethylene tamoxifen analogues, with the exception of toremifene (Fig. 1), have been withdrawn from development for the treatment of breast cancer.
Another avenue has been to produce steroidal analogues of estrogen with a bulky side chain at either the 7~ (25-28) or 11 [3 position of estradiol (29), which are completely lacking in agonist activity. These agents have been termed "pure" anties- trogens and include ICI 164,384, fulvestrant (Faslodex; for- merly ICI 182,780), and RU 58668. The most advanced of these in terms of both preclinical and clinical evaluation is the steroi- dal compound fulvestrant (Fig. 1; Ref. 28).
Fulvestrant: Mode of Action Fulvestrant is one of two steroidal antiestrogens with pure
antiestrogenic activity developed from a series of 7~-alkyl an-
Table 1 Preclinical and clinical assessment of new antiestrogens
Preclinical in vitro and in vivo assessments �9 ER binding �9 ER-a and ER-13 transcriptional activation �9 Tumor antagonism �9 Estrogenic activity in breast and uterus �9 Activity against tamoxifen-resistant cell lines �9 Estrogenic activity on bone and serum lipids �9 Mechanism of ER activation (coactivators, corepressors, and
ligand-independent activity) Clinical assessment
�9 Activity as first-line therapy �9 Activity in tamoxifen-resistant tumors �9 Activity as neoadjuvant and adjuvant therapy �9 Activity in prevention �9 Side effect profile �9 Scheduling relative to aromatase inhibitors
alogues of estradiol (28). ICI 164,384 has been studied exten- sively in a preclinical setting, but it is the more potent fulves- trant that is being actively studied in clinical trials in patients with breast cancer (25, 26).
Fulvestrant is distinguishable from tamoxifen and the other SERMs, both pharmacologically and in terms of its molecular activity. Although both classes of agent mediate thei r effects through the ER, they differ significantly in their downstream effects (Table 2). Binding of estradiol and the nonsteroidal antiestrogens (SERMs) to the estrogen binding sites o f the ER initiates a series of events, which include dissociation of heat shock proteins and ER dimerization. The dimerization process facilitates the binding of the ER to specific DNA E R E s in the vicinity of estrogen-regulated genes (30, 31). In addition, many proteins interact with the receptor to act as corepressors or coactivators; to further complicate matters, at least 50 transcrip- tional activating factors modulate the effects of estrogen on the target gene (32, 33). There are also known to be at least two ERs, ER-oL and ER-[3 (34-36), which have different tissue distributions. Both ERs contain two activating functions, AF-1 and AF-2, both of which are active when estrogen b inds to the receptors. Neither activating function is active when the benzo- thiophene derivative raloxifene binds to the ER, and o n l y AF-2 is inactive when tamoxifen binds to the ER. The latter scenario leads to incomplete attenuation of transcription, with t h e AF-1 domain allowing selective gene expression to occur. Thus, the partial agonist activity of tamoxifen is attributed, in part , to its inability to inactivate AF-1.
The activity of the steroidal antiestrogens such as fulves- trant is very different (Table 2). The steroidal antiestrogens bind to the ER, but because of their long bulky side chains at the 7o~ and 11 [3 positions, receptor dimerization appears to be sterically hindered (37). There is evidence that ER turnover is increased and that nuclear localization is disrupted with a concomitant reduction in the number of detectable ER molecules in the cell both in vitro and in vivo (38). This is in marked contrast to the stable or increased levels of ER expression associated with tamoxifen and its analogues. In vitro and in vivo studies suggest that as a consequence of ER down-regulation, ER-rnediated transcription is completely attenuated because fulvestrant inac- tivates both AF-1 and AF-2, leading to complete suppression of
Research. on June 11, 2018. © 2001 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Clinical Cancer Research 4371s
Table 2 Modes of action of estradiol, tamoxifen, and fulvestrant after binding to the ER
1. The natural ligand E binds to the ER with high affinity and dissociates HSP90
2. The E-ER complex homodimerizes and localizes preferentially in the cell nucleus
3. E-ER homodimer binds to the ERE in the promoter region of estrogen-sensitive genes
4. Activation of transcription by ER involves two transcription activation functions, AF-1 and AF-2, of the ER and transcriptional coactivators to stimulate the activity of RNA polymerase II (RNA POL II)
T (SERMs) 1. T binds to ER with low affinity compared with E and
dissociates HSP90. 2. T-ER complex homodimerizes and translocates to the cell
nucleus. AF-1 but not AF-2 is active. 3. T-ER dimer binds DNA sequence to ERE in promoter region of
estrogen-sensitive genes 4. Transcription of E-responsive gene(s) is attenuated because AF-
2 is inactive and the T-ER complex attenuates coactivator binding; partial agonist activity results because AF-1 in T-ER complex remains active.
F (ERD) 1. F binds to ER with high affinity and dissociates HSP90 2. Rapid degradation of ER triggered by binding 3. Reduced rate of dimerization and nuclear localization of F-ER
complex 4. Reduced binding of F-ER to ERE 5. No transcription of E-responsive genes; because AF-1 and AF-2
are inactive, no coactivators are recruited
'~ E, estradiol; HSP, heat shock protein; T, tamoxifen; F, fulves- trant.
the expression of estrogen-dependent genes. Thus, not only is fulvestrant described as a pure antiestrogen, it is also now described as an ERD.
Preclinical Studies The preclinical characteristics of fulvestrant, which define
this compound as a "pure" antiestrogen devoid of estrogen-like activity, have been reviewed extensively (28, 39, 40) and pro- vided the first evidence that fulvestrant may offer a potential therapeutic advantage over tamoxifen. These characteristics in- clude an affinity for the ER approximately 100 times that of tamoxifen, the specific absence of estrogen-like activity on the uterus both in vitro and in vivo, and the capacity to completely block the stimulatory activities of both estrogens and antiestro- gens with partial agonist activity, such as tamoxifen. For exam- ple, in the rat uterus, in contrast to estradiol and tamoxifen, fulvestrant did not induce genes such as calbindin D, insulin-like growth factor I, vascular endothelial growth factor, and c-los and, when administered before estradiol or tamoxifen, it com- pletely blocked the induction of these genes by these agents (24). Moreover, fulvestrant has been shown not to block the
[3H]estradiol uptake of in the brain, suggesting that fulvestrant does not cross the blood-brain barrier (41) and therefore in humans may not cause the hot flushes associated with the nonsteroidal antiestrogens. The preclinical animal data on the effects of fulvestrant on bone density are conflicting, with reports of reduced cancellous bone volume in one study (42) and
no effect on overall density in another (43), and are being investigated further. The absence of estrogenic activity has important consequences for the development of resistance, which is a major concern during tamoxifen therapy. In vitro
studies have demonstrated that tamoxifen-resistant cell lines remain sensitive to growth inhibition by fulvestrant (44-46), whereas cells resistant to fulvestrant exhibit early cross-resis- tance to tamoxifen (47). Also, tamoxifen-resistant tumors re- main sensitive to fulvestrant in vivo (48). Preclinical studies in nude mice have shown fulvestrant to suppress the growth of established MCF-7 xenografts for twice as long as tamoxifen and to delay the onset of tumor growth for longer than tamox- ifen (48). Taken collectively, these data suggest that fulvestrant is a more effective estrogen antagonist than tamoxifen and is able to produce a longer response in the animal model. More- over, other animal studies have confirmed the complete absence of uterine-stimulating activity and shown fulvestrant to block the uterotrophic action of tamoxifen (27). In ovariectomized, estrogen-treated monkeys, the extent of involution of the endo- metrium was similar in animals treated with fulvestrant and in animals in which estrogen treatment was withdrawn (39). Over- all, these data indicate that the mode of action and the preclinical effects of fulvestrant are distinct from those of tamoxifen and the newer SERMs and support the concept that fulvestrant represents a novel type of antiestrogen with clinical potential and possibly important implications for the endocrine manage- ment of breast cancer in terms of the sequencing of steroidal and nonsteroidal antiestrogen therapies.
Clinical Studies The data regarding the clinical potential of fulvestrant in
patients with breast cancer are also encouraging. Administration of a short-acting, propylene glycol-based formulation of fulves- trant at doses of 6 or 18 mg daily by i.m. injection for 1 week to postmenopausal breast cancer patients before surgery resulted in a reduction in proliferation, as measured by Ki67 labeling index, and a reduction or absence of expression of ER and PgRs in ER-positive tumors (26). Treatment with fulvestrant also resulted in a clinically significant reduction in the expression of the estrogen-regulated gene pS2, but this was unrelated to tumor ER status. Similar experiments with tamoxifen had produced no change in ER expression, slightly increased PgR expression, and a reduction in the Ki67 labeling index after a median 21 days of treatment.
Although fulvestrant reduced ER expression to almost un- detectable levels, no other changes suggestive of an endocrine- insensitive phenotype were observed (24). This, coupled with the absence of changes in Ki67 in ER-negative tumors treated with fulvestrant, suggests that the effect is the result of antag- onism of estrogen at the ER level. This antiestrogenic effect has been confirmed in a study of premenopausal patients scheduled for hysterectomy for benign gynecological disease who were randomized to receive either 7 consecutive daily doses of the short-acting formulation of fulvestrant or observation before surgery. No increase in endometrial thickness was observed in the fulvestrant-treated patients (49), and there was also signifi- cantly lower ER expression in the myometrium of the treated group (50).
Research. on June 11, 2018. © 2001 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
4372s Fulvestrant (Faslodex) in Breast Cancer Therapy
100
9o
7O
5O
I ~ 3O
# 2O
10
M e d i a n D u r a t i o n o f R e s p o n s e
F u l v e s t r a n t 26 m o n t h s Aceta te
: �9 ........... . . . . . . . . . . . . . ~ : ~ : : : : : ::::: : :
�9 ~ p o . 0 4
�9 - , - MA (n =3S)
..... Fu lves tmnt (n = 13)
0 6 12 18 24 30 36
Months
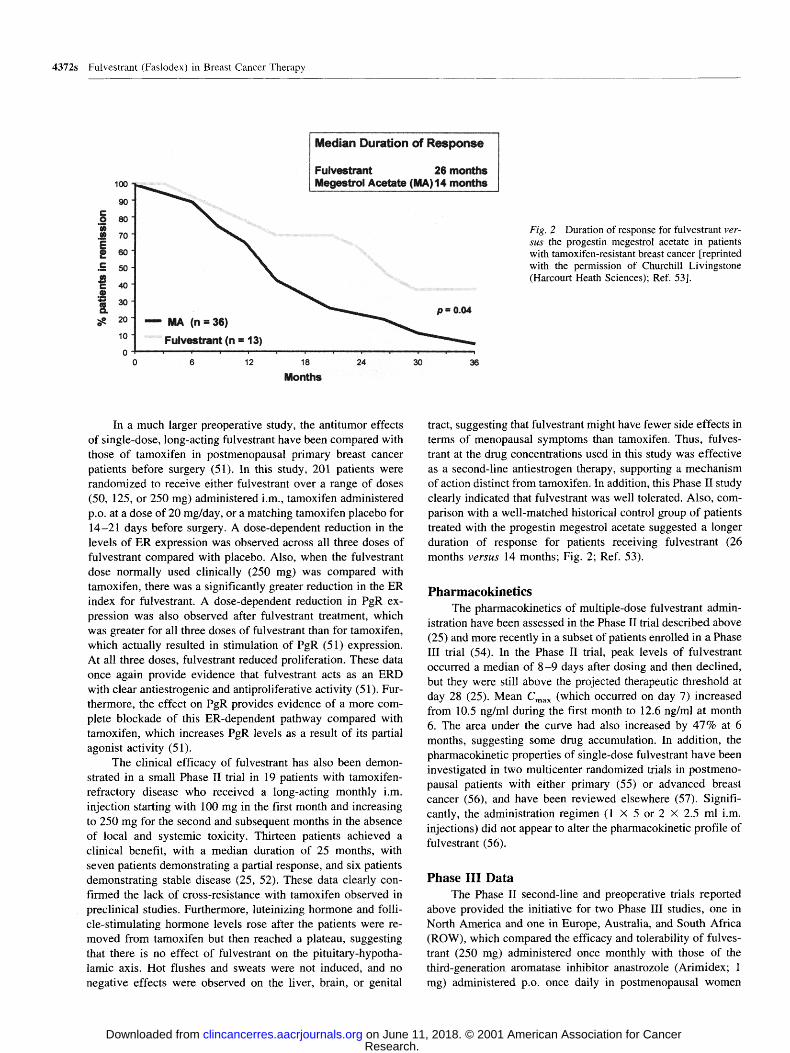
Fig. 2 Duration of response for fulvestrant ver-
sus the progestin megestrol acetate in patients with tamoxifen-resistant breast cancer [reprinted with the permission of Churchill Livingstone (Harcourt Heath Sciences); Ref. 53].
In a much larger preoperative study, the antitumor effects of single-dose, long-acting fulvestrant have been compared with those of tamoxifen in postmenopausal primary breast cancer patients before surgery (51). In this study, 201 patients were randomized to receive either fulvestrant over a range of doses (50, 125, or 250 mg) administered i.m., tamoxifen administered p.o. at a dose of 20 mg/day, or a matching tamoxifen placebo for 14-21 days before surgery. A dose-dependent reduction in the levels of ER expression was observed across all three doses of fulvestrant compared with placebo. Also, when the fulvestrant dose normally used clinically (250 mg) was compared with tamoxifen, there was a significantly greater reduction in the ER index for fulvestrant. A dose-dependent reduction in PgR ex- pression was also observed after fulvestrant treatment, which was greater for all three doses of fulvestrant than for tamoxifen, which actually resulted in stimulation of PgR (51) expression. At all three doses, fulvestrant reduced proliferation. These data once again provide evidence that fulvestrant acts as an ERD with clear antiestrogenic and antiproliferative activity (51). Fur- thermore, the effect on PgR provides evidence of a more com- plete blockade of this ER-dependent pathway compared with tamoxifen, which increases PgR levels as a result of its partial agonist activity (51).
The clinical efficacy of fulvestrant has also been demon- strated in a small Phase II trial in 19 patients with tamoxifen- refractory disease who received a long-acting monthly i.m. injection starting with 100 mg in the first month and increasing to 250 mg for the second and subsequent months in the absence of local and systemic toxicity. Thirteen patients achieved a clinical benefit, with a median duration of 25 months, with seven patients demonstrating a partial response, and six patients demonstrating stable disease (25, 52). These data clearly con- firmed the lack of cross-resistance with tamoxifen observed in preclinical studies. Furthermore, luteinizing hormone and folli- cle-stimulating hormone levels rose after the patients were re- moved from tamoxifen but then reached a plateau, suggesting that there is no effect of fulvestrant on the pituitary-hypotha- lamic axis. Hot flushes and sweats were not induced, and no negative effects were observed on the liver, brain, or genital
tract, suggesting that fulvestrant might have fewer side effects in terms of menopausal symptoms than tamoxifen. Thus, fulves- trant at the drug concentrations used in this study was effective as a second-line antiestrogen therapy, supporting a mechanism of action distinct from tamoxifen. In addition, this Phase II study clearly indicated that fulvestrant was well tolerated. Also, com- parison with a well-matched historical control group of patients treated with the progestin megestrol acetate suggested a longer duration of response for patients receiving fulvestrant (26 months v e r s u s 14 months; Fig. 2; Ref. 53).
Pharmacokinetics The pharmacokinetics of multiple-dose fulvestrant admin-
istration have been assessed in the Phase II trial described above (25) and more recently in a subset of patients enrolled in a Phase III trial (54). In the Phase II trial, peak levels of fulvestrant occurred a median of 8 -9 days after dosing and then declined, but they were still above the projected therapeutic threshold at day 28 (25). Mean Cma x (which occurred on day 7) increased from 10.5 ng/ml during the first month to 12.6 ng/ml at month 6. The area under the curve had also increased by 47% at 6 months, suggesting some drug accumulation. In addition, the pharmacokinetic properties of single-dose fulvestrant have been investigated in two multicenter randomized trials in postmeno- pausal patients with either primary (55) or advanced breast cancer (56), and have been reviewed elsewhere (57). Signifi- cantly, the administration regimen (1 • 5 or 2 • 2.5 ml i.m. injections) did not appear to alter the pharmacokinetic profile of fulvestrant (56).
Phase III Data The Phase II second-line and preoperative trials reported
above provided the initiative for two Phase III studies, one in North America and one in Europe, Australia, and South Africa (ROW), which compared the efficacy and tolerability of fulves- trant (250 mg) administered once monthly with those of the third-generation aromatase inhibitor anastrozole (Arimidex; 1 mg) administered p.o. once daily in postmenopausal women
Research. on June 11, 2018. © 2001 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Clinical Cancer Research 4373s
whose disease had progressed on or after prior endocrine ther- apy (58, 59). The vast majority (>96%) of patients across both trials had received prior tamoxifen therapy. The North American trial was a double-blind trial and recruited patients from 83 centers in the United States and Canada, whereas the second trial was an open-label study conducted principally in Europe and recruited patients from 82 centers. Altogether, 400 and 451 patients were analyzed for efficacy in the North American and ROW trials, respectively. The primary end point in both trials was time to disease progression, with secondary end points across both trials that included objective response, duration of response, time to death, tolerability, quality of life, and phar- macokinetics.
The median time to disease progression was numerically longer with fulvestrant compared with anastrozole for both the North American (5.4 v e r s u s 3.4 months) and ROW (5.5 v e r s u s
5.1 months) trials but was not statistically significant in either trial. The objective response rates were not significantly differ- ent in either trial (17.5% for both arms in the North American trial and 20.7% v e r s u s 15.7% for fulvestrant and anastrozole, respectively, in the ROW trial). In those patients who re- sponded, median duration of response to fulvestrant and anas- trozole was 19.3 and 10.5 months, respectively, in the North American trial and 14.3 and 14.0 months, respectively, in the ROW trial. The clinical benefit rates (defined as complete and partial responses and disease stabilization lasting -> 24 weeks) for fulvestrant v e r s u s anastrozole were 42.2% v e r s u s 36.1% for the North American trial and 44.6% v e r s u s 45.0% for the ROW trial. In both trials, the most frequently reported adverse events were gastrointestinal disturbances ( e . g . , nausea, vomiting, con- stipation, and diarrhea): 53.4% and 39.7% of patients suffered from at least one gastrointestinal disturbance in the North Amer- ican and ROW trials, respectively. Overall, the incidence of adverse events was similar for the recipients of anastrozole and fulvestrant in both trials. The withdrawal rates in the fulvestrant and anastrozole groups were low in both trials, with 2.5% v e r s u s
2.6% of patients withdrawing due to an adverse event in the North American trial and 3.2% v e r s u s 2.2% of patients with- drawing due to an adverse event in the ROW trial (58, 59). Thus, in both studies, fulvestrant was at least as effective as the aromatase inhibitor anastrozole, with a longer duration of re- sponse in the North American trial, confirming fulvestrant as an effective treatment in postmenopausal patients with advanced breast cancer recurring or progressing even after tamoxifen therapy. Fulvestrant was also well tolerated and is the first antiestrogen reported to be at least as effective as a new gener- ation aromatase inhibitor. This is of particular significance in light of the fact that two trials comparing anastrozole with tamoxifen in the first-line treatment of breast cancer have shown anastrozole to be superior to tamoxifen both in terms of time to progression and in terms of a lower incidence of thromboem- bolic events and vaginal bleeding (60, 61).
Conclusion Fulvestrant is clearly the first in a new class of antiestro-
gen. This novel steroidal ERD is currently being investigated in Phase III trials. Its mode of action (Table 2) and clinical efficacy and side effect profile (Table 3) are distinct from those of
Table 3 Summary of clinical efficacy and side effect profiles of fulvestrant and tamoxifen
Clinical activity Tamoxifen Fulvestrant
Prevention + ND a Neoadjuvant + + Adjuvant + Ongoing Advanced + + Tamoxifen resistance 0 + Agonist activity on uterus + - Bone density + ? Lipids ~ = Blood-brain barrier + NT
a ND, not determined; ~, a favorable change; =, no change; NT, not tested.
tamoxifen, and preliminary data from two Phase III studies show it to be as effective as the third-generation aromatase inhibitor anastrozole as a second-line endocrine therapy in post- menopausal patients who have failed on prior tamoxifen therapy (58, 59).
It is well recognized that patients whose disease progresses after responding to tamoxifen can achieve further responses with third-generation steroidal (exemestane) and nonsteroidal (anastrozole and letrozole) aromatase inhibitors, and these are currently being investigated as a first-line therapy in metastatic adjuvant and neoadjuvant settings. Fulvestrant is also being investigated in these clinical settings. Thus, fulvestrant not only provides an alternative to tamoxifen, it also offers the opportu- nity of a further response, at least equivalent to that of anastro- zole, in patients who have failed on tamoxifen and has potential as a subsequent therapy after tamoxifen in an adjuvant setting. The results of the ongoing Phase III clinical trials are eagerly awaited, particularly those comparing fulvestrant with tamox- ifen as a first-line therapy in advanced disease and the adjuvant studies.
Open Discussion Dr. Per Lonning: You mentioned that the 125-rag dose
was abandoned early in the trial because of very low response. Now, we have something like 100 patients with evaluable re- sponses to that dose. Now, if you look at general pharmacoki- netics about when you give a drug to a population, 95% confi- dence intervals for the area under the curve is a ratio of 1:4 for a drug with predictable pharmacokinetics. That tells you that if you double the dose for a drug, a large number of the patients will get similar drug levels with the two doses. So it 's really a concern to me that the response rate to the 125-mg dose was that low, and I think we really need to see the data, because between fulvestrant and Arimidex, there could be a benefit in favor of fulvestrant. It may be by chance.
Dr. Kent Osborne: In the American study there are some responses to the lower dose. There are pharrnacokinetic studies with those doses of fulvestrant. I don't think the confidence intervals are as broad as you might have predicted. You ' re not having to worry about bioavailability, which is so different in lots of patients, with an i.m. injection. I 've asked the pharma- cokinetics researcher what would happen if you double the dose
Research. on June 11, 2018. © 2001 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

4374s Fulvestrant (Faslodex) in Breast Cancer Therapy
even further to 500 mg, which is the dose I favor. He said the
serum levels would double in the majority of patients.
Dr. Lonn ing : The 1:4 ratio with the confidence intervals in general relates to drugs that are completely absorbed. If you
have drugs with more unpredictable absorption like megestrol
acetate, you get a 1:10 ratio. I 've never seen a drug with a smaller confidence interval than 1:4.
Dr. A n t h o n y Howell : We published the pharmacokinetics,
and they ' re in that Br i t i sh J o u r n a l o f C a n c e r paper (Br. J. Cancer, 74: 300-308, 1996). It did show relatively small con-
f idence intervals, and there was also accumulation with time.
With the first injection you achieved what were thought to be
therapeutic biologically effective levels at that time, or else these studies would never have gone on at all.
Dr . Osborne : Having granted that, though, I think this dose issue is a real issue, primarily because of that 125-mg dose.
The fact that there were very few responses tells me that we ' re
pretty close to the ineffective dose, and we may not be at the
optimal dose, particularly in premenopausal women in whom there is competing estrogen to bind the receptor. So I think it 's
a very important issue and deserves more study. Dr. Kathleen Pritehard: We can give them a couple of
injections at 2-week intervals for the first month. Dr. Osborne : I 'm just hoping that the insurance companies
don ' t read the fine print, because that's what I 'm going to do in my a d hoc s tudy-g ive them a double dose at first to get the level up there.
Dr. Howel l : That was the argument with tamoxifen, obvi- ously, to give a loading dose of 40 mg qds.
Dr. Alan Wake l ing : Tell us about that tamoxifen study with the loading dose.
Dr. Osborne : It worked, but there you ' re dealing with a drug that has partial agonist activity, and that strategy may counteract that early tickle, as Craig Jordan calls it. I ' m not sure what that means in a molecular sense, but he says when you tickle the receptor initially that you may get this agonist effect that can lead to tumor growth.
Dr. Howel l : We don ' t have hard data on whether the loading dose strategy prevented any flares, but we don ' t see very many flares anyway.
Dr. P r i t e h a r d : If you ' re taking this drug into the adjuvant setting, you might make the argument that it doesn ' t matter, because you ' re going to get a level of what you need in a few months anyway. Or you could make the argument that it 's that initial time period that matters the most and this is a crucial issue, just as it probably is in metastatic disease.
References 1. Cole, M. P., Jones, C. T. A., and Todd, I. D. H. A new anti- oestrogenic agent in late breast cancer. An early clinical appraisal of ICI 164,474. Br. J. Cancer, 25: 270-275, 1996. 2. Tamoxifen for early breast cancer: an overview of the randomised trials. Early Breast Cancer Trialists' Collaborative Group. Lancet, 351: 1451-1467, 1998. 3. Wolmark, N., Colangelo, L., and Wieand, S. National Surgical Adjuvant Breast and Bowel Project trials in colon cancer. Semin. Oncol., 28: 9-13, 2001. 4. Fisher, B., Costantino, J. P., Wickerham, D. L., et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant
Breast and Bowel Project P-1 Study. J. Natl. Cancer Inst. (Bethesda), 90: 1371-1388, 1998. 5. Chlebowski, R. T., Collyar, D. E., Somerfield, M. R., et al. American Society of Clinical Oncology technology assessment on breast cancer risk reduction strategies: tamoxifen and raloxifene. J. Clin. Oncol., 17: 1939-1955, 1999.
6. Love, R. R., Mazess, R. B., Barden, H. S., et al. Effects of tamoxifen on bone mineral density in postmenopausal women with breast cancer. N. Engl. J. Med., 326: 852-856, 1992. 7. Bilmoria, M. M., Jordan, V. C., and Morrow, M. Additional benefits of tamoxifen for postmenopausal patients. In: V. C. Jordan (ed.), Ta- moxifen: A Guide for Clinicians and Patients, pp. 75-89. Huntington, NY: PRR Inc., 1996.
8. Love, R. R., Newcomb, P. A., Wiebe, D. A., et al. Effects of tamoxifen therapy on lipid and lipoprotein levels in postmenopausal patients with node-negative breast cancer. J. Natl. Cancer Inst. (Bethes- da), 82: 1327-1332, 1990.
9. Love, R. R., Wiebe, D. A., Newcomb, P. A., et al. Effects of tamoxifen on cardiovascular risk factors in postmenopausal women. Ann. Intern. Med., 115: 860-864, 1991.
10. Fisher, B., Costantino, J. P., Redmond, C. K., et al. Endometrial cancer in tamoxifen-treated breast cancer patients: findings from the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-14. J. Natl. Cancer Inst. (Bethesda), 86: 527-37, 1994. 11. Jordan, V. C., and Morrow, M. Should clinicians be concerned about the carcinogenic potential of tamoxifen? Eur. J. Cancer, 11: 1714-1721, 1994.
12. Plotkin, D., Lechner, J. J., Jung, W. E., et al. Tamoxifen flare in advanced breast cancer. J. Am. Med. Assoc., 240: 2644-2646, 1978.
13. Howell, A., Dodwell, D. J., Anderson, H., et al. Response after withdrawal of tamoxifen. Ann. Oncol., 3: 611-617, 1992.
14. Hendrick, A., and Subramanian, V. P. Tamoxifen and thromboem- bolism. J. Am. Med. Assoc., 243: 514-515, 1980.
15. Lipton, A., Harvey, H. A., and Hamilton, R. W. Venous thrombosis as a side effect of tamoxifen treatment. Cancer Treat. Rep., 68: 887- 889, 1984. 16. Kangas, L., Nieminen, A. L., Blanco, G., et al. A new triphenyl- ethylene compound, Fc-l157a. II. Antitumor effects. Cancer Che- mother. Pharmacol., 17: 109-113, 1986.
17. Chander, S. K., McCague, R., Luqmani, Y., et al. Pyrrolidino-4- iodotamoxifen and 4-iodotamoxifen, new analogues of the antiestrogen tamoxifen for the treatment of breast cancer. Cancer Res., 5 1 : 5 8 5 1 - 5858, 1991. 18. Loser, R., Seibel, K., and Eppenberger, U. No loss of estrogenic or anti-estrogenic activity after demethylation of droloxifene (3-OH- tamoxifen). Int. J. Cancer, 36: 701-703, 1985.
19. Toko, T., Sugimoto, Y., Matsuo, K., et al. TAT-59, a new triph- enylethylene derivative with antitumor activity against hormone-depen- dent tumors. Eur. J. Cancer, 26: 397-404, 1990.
20. Toko, T., Shibata, J., Nukatsuka, M., et al. Antiestrogenic activity of DP-TAT-59, an active metabolite of TAT-59 against human breast cancer. Cancer Chemother. Pharmacol., 39: 390-398, 1997.
21. Palkowitz, A. D., Glasebrook, A. L., Thrasher, K. J., et al. Discov- ery and synthesis of [6-hydroxy-3-[4-[2-(1-piperidinyl)ethoxy]phe- noxy]-2-(4-hydroxyphenyl)]benzo[b]thiophene: a novel, highly potent, selective estrogen receptor modulator. J. Med. Chem., 40: 1407-1416, 1997. 22. Clemens, J. A., Bennett, D. R., Black, L. J., et al. Effects of a new antiestrogen, keoxifene (LY156758), on growth of carcinogen-induced mammary tumors and on LH and prolactin levels. Life Sci., 32: 2869- 2875, 1983. 23. Gauthier, S., Caron, B., Cloutier, J., et al. (S)-(+)-4-[7-(2,2- Dimethyl- 1-oxopropoxy)-4-methyl-2- [4- [2-(1-piperidinyl)-ethoxy]phe- nyl]-2H-l-benzopyran-3-yl]-phenyl 2,2-dimethylpropanoate (EM-800): a highly potent, specific, and orally active nonsteroidal antiestrogen. J. Med. Chem., 4 0 : 2 1 1 7 - 2 1 2 2 , 1997.
Research. on June 11, 2018. © 2001 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Clinical Cancer Research 4375s
24. Howell, A., Osborne, C. K., Morris, C., et al. ICI 182,780 (Faslo- alex): development of a novel "pure" antiestrogen. Cancer (Phila.), 89: 817-825, 2000.
25. Howell, A., DeFriend, D. J., Robertson, J. F., et al. Pharmacoki- netics, pharmacological and anti-tumour effects of the specific anti- oestrogen ICI 182780 in women with advanced breast cancer. Br. J. Cancer, 74: 300-308, 1996.
26. DeFriend, D. J., Howell, A., Nicholson, R. I., et al. Investigation of a new pure antiestrogen (ICI 182780) in women with primary breast cancer. Cancer Res., 54: 408-414, 1994.
27. Wakeling, A. E., Dukes, M., and Bowler, J. A potent specific pure antiestrogen with clinical potential. Cancer Res., 51: 3867-3873, 1991.
28. Wakeling, A. E., and Bowler, J. ICI 182,780, a new antioestrogen with clinical potential. J. Steroid Biochem. Mol. Biol., 43: 173-177, 1992. 29. Van de Velde, P., Nique, F., Planchon, P., et al. RU 58668: further in vitro and in vivo pharmacological data related to its antitumoral activity. J. Steroid Biochem. Mol. Biol., 59: 449-457, 1996.
30. McGregor, J. I., and Jordan, V. C. Basic guide to the mechanisms of antioestrogen action. Pharmacol. Rev., 50: 151-196, 1998.
31. Beato, M., Chalepakis, G., Schauer, M., et al. DNA regulatory elements for steroid hormones. J. Steroid Biochem., 32: 737-747, 1989.
32. Webb, P., Nguyen, P., Shinsako, J., et al. Estrogen receptor acti- vation function 1 works by binding to p160 coactivator proteins. Mol. Endocrinol., 12: 1605-1618, 1998.
33. Johnston, S. R., Lu, B., Scott, G. K., et al. Increased activator protein-1 DNA binding and c-jun NH2-terminal kinase activity in hu- man breast tumors with acquired tamoxifen resistance. Clin. Cancer Res., 5: 251-256, 1999.
34. Kuiper, G. G., and Gustafsson, J. A. The novel estrogen receptor-J3 subtype: potential role in the cell- and promoter-specific actions of estrogens and anti-estrogens. FEBS Lett., 410: 87-90, 1997.
35. Katzenellenbogen, B. S., and Korach, K. S. A new actor in the estrogen receptor drama-enter ER-[3. Endocrinology, 138: 861-862, 1997. 36. Mosselman, S., Polman, J., and Dijkema, R. ER [3: identification and characterization of a novel human estrogen receptor. FEBS Lett., 392: 49-53, 1996.
37. Parker, M. G. Action of "pure" antiestrogens in inhibiting estrogen receptor action. Breast Cancer Res. Treat., 26: 131-137, 1993.
38. Pink, J. J., and Jordan, V. C. Models of estrogen receptor regulation by estrogens and antiestrogens in breast cancer cell lines. Cancer Res., 56: 2321-2330, 1996.
39. Dukes, M., Miller, D., Wakeling, A. E., et al. Antiuterotrophic effects of a pure antioestrogen, ICI 182,780: magnetic resonance imag- ing of the uterus in ovariectomized monkeys. J. Endocrinol., 135: 239-247, 1992. 40. Dukes, M., Waterton, J. C., and Wakeling, A. E. Antiuterotrophic effects of the pure antioestrogen ICI 182,780 in adult female monkeys (Macaca nemestrina): quantitative magnetic resonance imaging. J. En- docrinol., 138: 203-210, 1993.
41. Wade, G. N., Blaustein, J. D., and Gray, J. M., et al. ICI 182,780: a pure antiestrogen that affects behaviors and energy balance in rats without acting in the brain. Am. J. Physiol., 265: R1392-R1398, t993.
42. Gallagher, A., Chambers, T. J., and Tobias, J. H. The estrogen antagonist ICI 182,780 reduces cancellous bone volume in female rats. Endocrinology, 133: 2787-2791, 1993.
43. Wakeling, A. E. The future of pure antioestrogens in clinical breast cancer. Breast Cancer Res. Treat., 25: 1-9, 1993.
44. Coopman, P., Garcia, M., Brunner, N., et aL Anti-proliferative and anti-estrogenic effects of ICI 164,384 and ICI 182,780 in 4-OH-tamox- ifen-resistant human breast-cancer cells. Int. J. Cancer, 56: 295-300, 1994. 45. Brunner, N., Frandsen, T. L., Holst-Hansen, C., et al. MCF7/LCC2: a 4-hydroxytamoxifen-resistant human breast cancer variant that retains
sensitivity to the steroidal antiestrogen ICI 182,780. Cancer Res., 53: 3229-3232, 1993.
46. Hu, X. F., Veroni, M., De Luise, M., et al. Circumvention of tamoxifen resistance by the pure anti-estrogen ICI 182,780. Int. J. Cancer, 55: 873-876, 1993.
47. Brunner, N., Boysen, B., Jirus, S., et al. MCF7/LCC9: an anties- trogen-resistant MCF-7 variant in which acquired resistance to the steroidal antiestrogen ICI 182,780 confers an early cross-resistance to the nonsteroidal antiestrogen tamoxifen. Cancer Res., 57: 3486-3493, 1997. 48. Osborne, C. K., Coronado-Heinsohn, E. B., Hilsenbeck, S. G., et al. Comparison of the effects of a pure steroidal antiestrogen with those of tamoxifen in a model of human breast cancer. J. Natl. Cancer Inst. (Bethesda), 87: 746-750, 1995.
49. Thomas, E. J., Walton, P. L., Thomas, N. M., et al. The effects of ICI 182,780, a pure anti-oestrogen, on the hypothalamic-pituitary- gonadal axis and on endometrial proliferation in pre-menopausal women. Hum. Reprod., 9: 1991-1996, 1994.
50. Dowsett, M., Howell, R., Salter, J., et al. Effects of the pure anti-oestrogen ICI 182780 on oestrogen receptors, progesterone recep- tors and Ki67 antigen in human endometrium in vivo. Hum. Reprod., 10: 262-267, 1995.
51. Robertson, J. F. R., Nicholson, R., Anderson, E., et al. The anti- tumour effects of single-dose long-acting Faslodex (ICI 182,780) com- pared with tamoxifen in postmenopausal primary breast cancer patients treated before surgery. Breast Cancer Res. Treat., 59: 99, 2000.
52. Howell, A., DeFriend, D., Robertson, J., et al. Response to a specific antioestrogen (ICI 182780) in tamoxifen-resistant breast cancer. Lancet, 345: 29-30, 1995.
53. Robertson, J. F. R., Howell, A., De Friend, D. J., et al. Duration of remission to ICI 182,780 compared to megestrol acetate in tamoxifen resistant breast cancer. Breast Cancer Res. Treat., 6: 186-189, 1997.
54. Robertson, J., and Harrison, M. ICI 182,780 (Faslodex) (FAS) 250 mg monthly intramuscular (i.m.) injection shows consistent PK during long-term dosing in postmenopausal women with advanced breast can- cer (ABC). Proc. Am. Assoc. Cancer Res., 42: 856, 2001.
55. Robertson, J., Nicholson, R., Gee, J. M., et aL The pharmacokinet- ics of single dose Faslodex TM (ICI 182,780) in postmenopausal primary breast cancer: relationship with estrogen receptor down regulation. Proc. Am. Soc. Clin. Oncol., 19: 94a, 2000.
56. Robertson, J. F. R. A comparison of single-dose pharmacokinetics of Faslodex (fulvestrant) 250 mg when given as either one • 5 ml intramuscular injection or two • 2.5 ml injections in postmenopausal women with advanced breast cancer. Breast Cancer Res. Treat., 64: 53, 2000. 57. Curran, M., and Wiseman, L. Fulvestrant. Drugs, in press, 2001.
58. Howell, A., Robertson, J. F. R., Quaresma-Albano, J., et al. Com- parison of efficacy and tolerabiltiy of fulvestrant (Faslodex TM) with anastrazole (Arimidex TM) in post-menopausal women with advanced breast cancer (ABC): preliminary results. Breast Cancer Res. Treat., 64: 27, 2000.
59. Osborne, C. K., Pippen, J., Jones, S. E., et al. Faslodex (ICI 182,780) shows longer duration of response compared with Arimidex (anastrozole) in postmenopausal (PM) women with advanced breast cancer (ABC). Preliminary results of a Phase III North American trial. Breast Cancer Res. Treat., 65: 261, 2001.
60. Nabholtz, J. M., Buzdar, A., Pollak, M., et al. Anastrozole is superior to tamoxifen as first-line therapy for advanced breast cancer in postmenopausal women: results of a North American multicenter ran- domized trial. Arimidex Study Group. J. Clin. Oncol., 18: 3758-3767, 2000. 61. Bonneterre, J., Thurlimann, B., Robertson, J. F., et al. Anastrozole versus tamoxifen as first-line therapy for advanced breast cancer in 668 postmenopausal women: results of the Tamoxifen or Arimidex Ran- domized Group Efficacy and Tolerability study. J. Clin. Oncol., 18: 3748-3757, 2000.
Research. on June 11, 2018. © 2001 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
2001;7:4369s-4375s. Clin Cancer Res Anthony Howell Preliminary Experience with Pure Antiestrogens
Updated version
http://clincancerres.aacrjournals.org/content/7/12/4369s
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/7/12/4369sTo request permission to re-use all or part of this article, use this link
Research. on June 11, 2018. © 2001 American Association for Cancerclincancerres.aacrjournals.org Downloaded from