pregnancy, epilepsy, and women s issues.15
TRANSCRIPT

Pregnancy, Epilepsy,and Women’s Issues
Page B. Pennell, MD
ABSTRACTPurpose of Review: Optimal treatment of women with epilepsy includes consider-ation of the complex interactions of sex steroid hormones with epilepsy andantiepileptic drugs, and of the potential risks of any antiepileptic drug prescribedduring a pregnancy.Recent Findings: Clinical studies in women with epilepsy have provided a betterfoundation of knowledge about the complex relationships between cycling sex steroidhormones, seizure frequency, antiepileptic drugs, contraception, and neuroendocrineabnormalities. Pregnancy registries and observational studies have provided key datathat allow for a better estimation of risks to the developing fetus.Summary: Understanding these key factors should enable informed treatmentrecommendations that can reduce adverse health effects in women with epilepsy andimprove both seizure control and maternal and fetal outcomes.
Continuum (Minneap Minn) 2013;19(3):697–714.
INTRODUCTIONCare for women with epilepsy presentsseveral specific challenges towardantiepileptic drug (AED) selection andprescription in light of drug risks duringany potential pregnancy, planned orunplanned, and the complex interac-tions between the AEDs and female sexsteroid hormones.
TRIDIRECTIONAL INTERACTIONSBETWEEN EPILEPSY,ANTIEPILEPSY DRUGS, ANDSEX STEROID HORMONESMultidirectional interactions exist be-tween epilepsy and seizures, female sexsteroid hormones, and AEDs (Figure 7-1).Female sex steroid hormones and theirmetabolites act as direct neurosteroids,modulating brain excitability via bothshort-latency neuronal membrane-mediated effects and long-latency geno-mic effects.1 Animal studies have consis-tently suggested that estrogen promotesneuroexcitatory properties. Progester-
one instead promotes neuroinhibitoryproperties, primarily through its me-tabolite allopregnanolone. Therefore,changes in endogenous and exoge-nous female sex steroid hormones levelscan influence seizure control directly.Changes in estradiol levels can also in-crease the clearance of some AEDs, andpotentially worsen seizure control indi-rectly through lowering of AED serumconcentrations. Additionally, both AEDsand epilepsy itself can adversely affectfunction of the hypothalamic-pituitary-ovarian axis (Figure 7-21).
CATAMENIAL EPILEPSYThe term ‘‘catamenial epilepsy’’ de-notes that seizure frequency increasesduring certain phases of the menstrualcycle. A catamenial pattern can occurwith any seizure type or epilepsy syn-drome, but it has been most commonlyreported and studied in focal epilepsies.
The average menstrual cycle is 28days, with day 1 being the first day of
Address correspondence toDr Page B. Pennell,Department of Neurology,Brigham and Women’sHospital, 75 Francis St,Boston, MA 02115,[email protected].
Relationship Disclosure:Dr Pennell reportsno disclosure.
Unlabeled Use ofProducts/InvestigationalUse Disclosure:Dr Pennell discusses theunlabeled use of progesteronelozenges for the treatment ofcatamenial epilepsy.
* 2013, American Academyof Neurology.
697Continuum (Minneap Minn) 2013;19(3):697–714 www.ContinuumJournal.com
Review Article
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

menses and ovulation occurring onday 14 (also designated as day -14 toadjust for cycle lengths other than 28days). The menstrual cycle has twomajor phases: the follicular phase (days1 through 14) and the luteal phase(days -14 to -1). Figure 7-31 displaysthe fluctuating levels of estradiol andprogesterone in normal menstrual cy-cling, as well as in anovulatory men-
strual cycling with an inadequate lutealphase. Catamenial seizures most com-monly worsen when levels of estrogenare relatively higher than progesteroneor when levels are rapidly changing.
Criteria for Catamenial EpilepsyFor women with epilepsy, prevalenceestimates for catamenial epilepsy varybetween 12.5% and 75%, but using themost accepted definition of a consistentdoubling of seizure frequency during atleast one of the three specific portionsof the menstrual cycle (Figure 7-31),approximately one-third of womenwithfocal epilepsy may be classified as hav-ing catamenial seizures.2
Treatment OptionsMost reported treatments for catamenialepilepsy have been in women with a C1pattern. A C1 catamenial pattern isassociated with exacerbation of seizuresin the perimenstrual phase (day -3 to day
KEY POINT
h Criteria forcatamenialepilepsy havebecome more consistentand formalized.
FIGURE 7-1 Multidirectional interactions of epilepsy andseizures, female sex steroid hormones and fertility,and antiepileptic drugs and concentrations.
FIGURE 7-2 Hypothalamic-pituitary-ovarian axis.
GnRH = gonadotropin-releasing hormone;FSH = follicle-stimulating hormone;LH = luteinizing hormone.
Adapted from Harden CL, Pennell PB, Lancet Neurol.1
B 2013, with permission from Elsevier.www.sciencedirect.com/science/article/pii/S1474442212702399.
698 www.ContinuumJournal.com June 2013
Pregnancy and Epilepsy
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

+3 of next cycle). Case reports or smallseries suggest that acetazolamide orclobazam given during the menstrualphase of seizure worsening may behelpful.1 Medroxyprogesterone acetate,a synthetic progestin-only contraceptiveagent, can also reduce seizure frequency3
but may be associated with side effectsof weight gain, bone density loss, anddelayed return of fertility.
The only double-blind, placebo-controlled, randomized trial for cat-amenial epilepsy involved adjunctiveprogesterone lozenges during menstrual
FIGURE 7-3 Patterns of catamenial epilepsy. Day 1 is the first day of menstrual flow and dayj14 is the day of ovulation. A, Normal cycle with normal ovulation. C1 patternis associated with exacerbation of seizures in the perimenstrual phase (day j3
to day +3 of next cycle), and C2 pattern is associated with exacerbation of seizures in theperiovulatory phase (day +10 to day j13). B, Inadequate luteal phase cycle with anovulation.The C3 pattern is associated with exacerbations during the entire inadequate luteal phase(day +10 to day +3 of the next cycle).
C = catamenial seizure pattern; F = follicular phase; O = periovulatory phase;L = luteal phase; M = perimenstrual phase.
Reprinted from Harden CL, Pennell PB, Lancet Neurol.1 B 2013, with permission from Elsevier. www.sciencedirect.com/science/article/pii/S1474442212702399.
699Continuum (Minneap Minn) 2013;19(3):697–714 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

days 14 to 28. Although the primaryoutcomes were not significant, benefitwas demonstrated for a subgroup ofwomen who had a threefold or greaterseizure frequency increase during theC1 phase (days -3 to +3).4
PERIMENOPAUSE ANDMENOPAUSEWomen with epilepsy may be at riskfor early onset of menopause. In onestudy, 14% of women with epilepsy hadpremature ovarian failure comparedwith 4% of healthy control women, andthe age of menopause and seizure fre-quency have beennegatively correlated.5,6
Small studies suggest that womenwith epilepsy may experience increasedseizures during the perimenopausaltransition and decreased seizures aftermenopause is complete, especially ifthey had a catamenial pattern duringearlier reproductive years.7 During peri-menopause, estrogen levels can risesteadily, remain stable, or become er-ratic with surges until menopause iscomplete, while cyclic luteal phase pro-gesterone elevation gradually decreasesduring anovulatory cycles.
Hormone replacement therapyshould be used with caution in womenwith epilepsy. Seizure frequency dose-dependently increased during a 3-month controlled trial of a combinationest rogen-medroxyprogesteronehormone-replacement therapy regimen.8
REPRODUCTIVE FUNCTIONIncreased rates of polycystic ovariansyndrome, decreased libido, infertility,and early menopause have been de-scribed in women with epilepsy. Theeffects of epilepsy, seizures, underlyingbrain abnormalities, and interictal epi-leptiform discharges are difficult todistinguish from AED effects on femalesex steroid hormones. Hypothalamichypogonadism has been described inboth women and men with epilepsy.
Gonadotropin-releasing hormone(GnRH) is produced by a small num-ber of cells located in the preopticarea of the hypothalamus and controlsovarian activity via pulsatile secretionand stimulation of pituitary hormonerelease (follicle-stimulating hormone[FSH] and luteinizing hormone [LH]).This GnRH cell population can beinjured by seizures in a rodent model.1
Human studies demonstrated that tem-poral lobe epilepsy lateralization maybe associated with different patterns ofreproductive dysfunction. In an inves-tigation of unilateral temporal lobeepilepsy, left temporal lobe dischargeswere associated with polycystic ovarysyndrome, and right-sided dischargeswith hypothalamic hypogonadism.9
Polycystic ovarian syndrome is amajor cause of infertility and appearsmore frequently in women with epi-lepsy. Criteria for diagnosis include thepresence of hyperandrogenism andovarian dysfunction (oligo-anovulation,polycystic ovaries, or both).10 Polycysticovarian syndrome has been morefrequently reported in association withgenetic (idiopathic) generalized than fo-cal epilepsy syndromes, although morewomen with generalized epilepsy re-ceived valproate treatment. In onestudy, many metabolic abnormalitiesof polycystic ovarian syndrome werereduced by discontinuing valproate.11 Arandomized prospective study of womenwith epilepsy reported that polycysticovarian syndrome features developedmore frequently during valproate thanlamotrigine treatment, especially inwomen with epilepsy who began treat-ment before 26 years of age.12
Effects of Antiepileptic Drugson Reproductive HormonesIn general, hepatic enzyme-inducingAEDs directly alter female sex steroidhormone levels (Table 7-1) and induceproduction of sex hormoneYbinding
KEY POINT
h For patients having athreefold or greaterincrease in seizurefrequency in a C1pattern, cyclicprogesterone lozengesare an adjunctivetreatment option.
700 www.ContinuumJournal.com June 2013
Pregnancy and Epilepsy
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

globulin, thereby reducing both en-dogenous biologically active (free)reproductive hormone serum levelsand exogenous contraceptive hormonelevels, as discussed further below.1 AEDeffects on circulating sex steroid hor-mone levels can also affect sexualfunction. In a study of sexual functionand hormones in women with epilepsy,women receiving enzyme-inducingAEDs had statistically higher sexual
dysfunction and lower sexual arousalcompared to controls.13 Questionsabout sexual function should be partof the routine evaluation in the out-patient clinic. Sexual dysfunction inwomen with epilepsy has multifactorialcauses, but AED type is one contribut-ing and potentially modifiable factor,and available evidence suggests thatnonYenzyme-inducing AEDs showmore favorable profiles.13
Fertility and Childbirth RatesWhile birth rates encompass psycho-social factors such as choosing whetherto bear children, infertility refers to acouple not using contraceptive methodsfor 1 year and not conceiving. The KeralaRegistry of Epilepsy and Pregnancyreported a 38% infertility rate amongyounger women with epilepsy activelytrying to conceive after marriage, withhigher infertility rates in those receiv-ing AED polytherapy.14 Other studiesof women with epilepsy have beeninconsistent but suggest decreased fertil-ity rates. Another study also reported thatthe reduced rate of childbirth holds inmarried women with epilepsy (69% ofexpected number of live-born chil-dren).15 A population-based Finnishcohort study of newly diagnosedwomen with epilepsy reported slightlylower childbirth rates than in a refer-ence cohort,16 whereas a comparableIcelandic study suggested no differ-ence in childbearing rates in womenwith epilepsy.17
Several biological reasons couldcause decreased fertility in women withepilepsy, including central dysregu-lation of the hypothalamic-pituitary-ovarian axis, premature ovarian failure,polycystic ovarian syndrome, and ef-fects of enzyme-inducing AEDs.1 Inaddition to these factors, geographicand cultural differences are likely sub-stantial factors that influence self-directed decisions. The ‘‘Ideal World’’
TABLE 7-1 Antiepileptic Drugs:Degree of Inductionof Metabolism
of Sex Steroid Hormones(Endogenous Sex SteroidHormones and ExogenousHormonal Contraceptives)
b Strong Inducersa
Phenobarbital
Phenytoin
Carbamazepine
Primidone
Oxcarbazepine
Clobazam
b Weak Inducersa
Topiramate
Lamotrigine
Felbamate
Rufinamide
b Noninducers
Ethosuximide
Valproate
Gabapentin
Clonazepam
Tiagabine
Levetiracetam
Zonisamide
Pregabalin
Vigabatrin
Lacosamide
Ezogabineb
a Avoid concomitant use with thelowest-dose oral contraceptive pills.
b United States Adopted Name; known inrest of world as retigabine.
701Continuum (Minneap Minn) 2013;19(3):697–714 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

survey of Epilepsy Action UK womenfound that 33% of women with epi-lepsy were considering not havingchildren because of their epilepsy.18
CONTRACEPTIONEffective contraception in women withepilepsy is essential to allow for pre-conception planning and to implementthe measures known to improve preg-nancy outcomes. However, concomitantuse of AEDs and hormonal contracep-tives is complicated because of bidirec-tional pharmacokinetic interactions,pharmacodynamic consequences, andpotential effects on seizure control.
Enzyme-inducing AEDs lead to rapidclearance of female sex steroid hor-mones and may allow ovulation inwomen taking oral contraceptives orother hormonal forms of birth control(eg, vaginal ring, patch). Table 7-1categorizes the different AEDs accord-ing to the degree of female sex steroidhormones induction. These data arederived primarily from pharmacoki-netic interaction studies between theAED and oral contraceptive formulations.Other authors have recommended high-dose oral contraceptives with enzyme-inducing AEDs, assuming that enzymeinduction will lower oral contraceptivelevels. Oral contraceptives with higherdoses of ethinyl estradiol and progestinremain available but are infrequentlyused in practice for healthy women. Nodirect evidence supports contraceptiveefficacy in women with epilepsy receiv-ing enzyme-inducing AEDs. The USCenters for Disease Control and Preven-tion (CDC) Medical Eligibility Criteriafor Contraceptive Use classified certainAEDs (phenytoin, carbamazepine, phe-nobarbital, primidone, topiramate, andoxcarbazepine) as Category 3, meaningthat potential risks (eg, birth controlfailure) generally outweigh benefitsof use with oral contraceptives.19 Othercontraceptives should be encouraged
for women with epilepsy who are long-term users of these AEDs.
Oral contraceptives, as well as patches,rings, and implants, are no longer first-linecontraceptive methods for women withepilepsy who use enzyme-inducing AEDs(Table 7-1). For these women, a long-acting reversible contraceptive (LARC),such as the progestin implant or anintrauterine device (IUD), is an excellentchoice. The concentration of progestindelivered by the implant is high enoughthat efficacy is maintained with concom-itant use of an enzyme-inducing AED.The levonorgestrel IUD prevents preg-nancy by local hormonally mediatedchanges in cervical mucus and is notlikely to be impacted by enzyme-inducing AEDs. One reassuring prospec-tive UK registry study demonstrated apregnancy rate of 1.1 per 100 person-years for 56 women using the levonor-gestrel IUD with enzyme-inducingAEDs.20 IM medroxyprogesterone ace-tate is another LARC but is not a first-line option because it is associated withweight gain, bone density loss, anddelayed return of fertility.
PREGNANCYIntroductionEpilepsy is the most common neuro-logic disorder that requires continu-ous treatment during pregnancy, andAEDs are one of the most frequentchronic teratogen exposures. Approx-imately one-half million women withepilepsy are of childbearing age in theUnited States, and three to five birthsper thousand will be to women with epi-lepsy.21 However, the total number ofchildren exposed in utero to AEDs islikely considerably greater, given AED usefor headache, pain, and mood disorders.
AED treatment during pregnancy is aprecarious balancing act between terato-genic risks to the fetus and maintainingmaternal seizure control. However, preg-nancy registries and other prospective
KEY POINT
h Long-acting reversiblecontraceptives(including theprogestin implant) andintrauterine devices areexcellent choicesfor women withepilepsy receivingenzyme-inducingantiepileptic drugs.
702 www.ContinuumJournal.com June 2013
Pregnancy and Epilepsy
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

studies have provided invaluable infor-mation toward optimizing treatmentregimens and regarding the safety ofbreast-feeding. Previous study resultsand the recent American Academy ofNeurology (AAN) and American Epi-lepsy Society (AES) Practice Param-eter updates (available at www.neurology.org/content/73/2/133.full.pdf,www.neurology.org/content/73/2/142.full.pdf, and www.neurology.org/content/73/2/126.full.pdf ) are key con-siderations when counseling and treat-ing women with epilepsy during theirreproductive years.21Y23
Major CongenitalMalformations and MinorAnomaliesOffspring of women with epilepsy onAEDs are at an increased risk for majorcongenital malformations and minoranomalies. Minor anomalies are de-fined as structural deviations from thenorm that do not constitute a threat tohealth. Minor anomalies affect 6% to20% of infants born to women with epi-lepsy, approximately 2.5-fold the rate ofthe general population. Although not ofdirect health consequence, the findingof a minor anomaly should lead to en-hanced vigilance about the child’s healthand neurodevelopment.
Major congenital malformations aredefined as an abnormality of an essen-tial anatomical structure present at birththat interferes significantly with functionor requires major intervention. The re-
ported major congenital malformationrates in the general population varybetween 1.6% to 3.2%, and womenwithepilepsy who are not receiving AEDsshow similar major congenital malfor-mation rates. The average major con-genital malformation rates among allAED exposures vary between 3.1% to9%, approximately two- to threefoldhigher than the general population.24
Major congenital malformations mostcommonly associated with AED expo-sure include congenital heart disease,cleft lip/palate, urogenital defects, andneural tube defects. Since neural tubeclosure usually occurs between the thirdand fourth weeks of gestation, it isusually too late to adjust AEDs to avoidmalformations by the time most womenrealize they are pregnant (Table 7-2).
Antiepileptic DrugMonotherapiesInformation concerning the risks ofspecific AEDs for major congenitalmalformations has increased dramati-cally over the last 2 decades. Worldwidedata obtained from large prospectivepregnancy registries have demon-strated remarkably consistent find-ings for many of the AEDs. The 2009AAN-AES Practice Parameter updates onmanagement issues for women withepilepsyVfocus on pregnancy21 of-fered the following important conclu-sions about intrauterine first-trimesterexposure and risk for major congenitalmalformations (with parenthetical
TABLE 7-2 Relative Timing and Developmental Pathology ofCertain Malformations
Tissues Malformations Postconceptional Age
CNS Neural tube defect 28 d
Heart Ventricular septal defect 42 d
Face Cleft lip 36 d
Cleft maxillary palate 47Y70 d
703Continuum (Minneap Minn) 2013;19(3):697–714 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

confidence of conclusion): (1) val-proate exposure has higher risk ofmajor congenital malformations com-pared to carbamazepine (highly proba-ble) and compared to phenytoin orlamotrigine (possible); (2) comparedto untreated women with epilepsy,valproate as part of a polytherapy regi-men (probable) and as monotherapy(possible) contributes to the develop-ment of major congenital malformations;(3) AED polytherapy as compared tomonotherapy regimens contributes tothe development of major congenitalmalformations (probable); (4) carbamaz-epine does not substantially increase therisk of major congenital malformations inthe offspring of women with epilepsy(probable); and (5) there is a relationshipbetween the dose of valproate andlamotrigine and the risk of developmentof major congenital malformations in theoffspring of women with epilepsy (prob-able). Additionally, for specific types ofmajor congenital malformations, find-ings included the following: (1) phenyt-oin contributes to the risk of cleft palate(possible); (2) carbamazepine contrib-utes to the risk of posterior cleft palate(possible); (3) valproate contributes toneural tube defects and facial clefts (prob-able) and to hypospadias (possible); and(4) phenobarbital exposure in uterocontributes to cardiac malformations(possible).
Since this evidence-based review ofthe literature, several large, worldwideprospective pregnancy registries haveconsistently demonstrated a pattern ofamplified risk for the association of val-proate exposure during pregnancy anddevelopment of major congenital malfor-mations, and provided additional infor-mation on other AEDs that help furtherrefine estimates for teratogenicity risk inwomen with epilepsy (see Case 7-1).
The UK Epilepsy and PregnancyRegister reported on topiramate use in178 live births.27 Although the confi-
dence intervals (CIs) were wide, thispreliminary information noted a majorcongenital malformation rate of 4.8%formonotherapy use and an even higherrate for use of topiramate in polytherapyregimens. They also noted a particularlyhigher rate of oral clefts, approximately11 times their background rate, and ahigh rate of hypospadias. Oral cleft riskwith topiramate has been replicated inother studies.28
Data from the National Birth De-fects Prevention Study confirmed in-creased risks for valproate and neuraltube defects (odds ratio [OR] 9.7; 95%CI, 3.4Y27.5), oral clefts (OR 4.4; 95%CI, 1.6Y12.2), heart defects (OR 2.0;95% CI, 0.78Y5.3), and hypospadias (OR2.4; 95% CI, 0.62Y9.0).29 Increased riskswere also observed for carbamazepineand neural tube defects (OR 5.0; 95%CI, 1.9Y12.7). Similarly, the EuropeanSurveillance of Congenital Anomalies(EUROCAT) antiepileptic-study data-base, which is derived from population-based congenital anomaly registries, alsoreported significantly increased risks forvalproate monotherapy and spina bifida,atrial septal defect, cleft palate, hypospa-dias, polydactyly, and craniosynostosis.Spina bifida was the only specific majorcongenital malformation associated withcarbamazepine monotherapy comparedwith no AED use during pregnancy (OR2.6; 95% CI, 1.2Y5.3), but the risk wassmaller than for valproate.30
The North American AED PregnancyRegistry released findings compar-ing the risk of major congenital mal-formations among infants exposed todifferent AED monotherapies duringthe first trimester, compared to anunexposed reference group.31 Thelamotrigine monotherapy group waschosen as the exposed referencegroup for the other AEDs because ofa low rate of major congenital malfor-mations and tight CIs (2.0% [95% CI,1.4Y2.8]) (Table 7-331). This table
704 www.ContinuumJournal.com June 2013
Pregnancy and Epilepsy
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

KEY POINT
h Determining theindividual targetconcentration of anantiepileptic drug in awoman with epilepsybefore conception canbe a valuable toolfor therapeutic drugmonitoring duringpregnancy.
Case 7-1A 30-year-old, right-handed woman presented for epilepsy managementduring the first trimester of pregnancy. Seizure onset was at 8 years old,with habitual clinical seizures characterized by an aura ofdepersonalization, followed by speech arrest, altered awareness,and variable progression to a generalized tonic-clonic seizure, thenheadache and lethargy. Seizures tended to occur only with antiepilepticdrug (AED) tapering, nonadherence, or sleep deprivation. Her mostrecent seizure was 2 years ago. She received valproate monotherapy.
At an infertility evaluation with a gynecologist, the diagnosis ofpregnancy was made with estimated 4 weeks gestational age. She wasstarted on 1 mg of folic acid and a multivitamin. Her local neurologiststopped valproate suddenly, and the patient had a generalizedtonic-clonic seizure 3 days later. Lamotrigine was begun at 25 mgtwice a day. Eight days later, she was hospitalized for Stevens-Johnsonsyndrome.
After urgent consultation, levetiracetam extended release wasbegun at 500 mg twice a day and continued throughout pregnancy.The patient had another generalized tonic-clonic seizure at20 weeks gestational age due to nonadherence. Levetiracetamconcentrations were followed for therapeutic drug monitoring anddoses were increased, eventually reaching 1500 mg twice a dayby delivery. She gave birth to a healthy baby boy without complications;birth weight was 6 lbs, 6 oz, and Apgar scores were 8/8 at 1 and5 minutes, respectively. She breast-fed, and levetiracetam doses weredecreased back to 750 mg twice a day over the first month postpartum.
Comment. Lack of appropriate preconception planning and goodmedical advice can lead to an unnecessarily unstable situation andincreased risk for both the mother and developing baby. Lamotriginecannot be started quickly during pregnancy, and if a conversion tolamotrigine was contemplated, it should have been done beforeconception. Recent evidence supports a low relative risk of majorcongenital malformations with levetiracetam, which may be areasonable alternative when AEDs need to be introduced quicklyduring pregnancy.
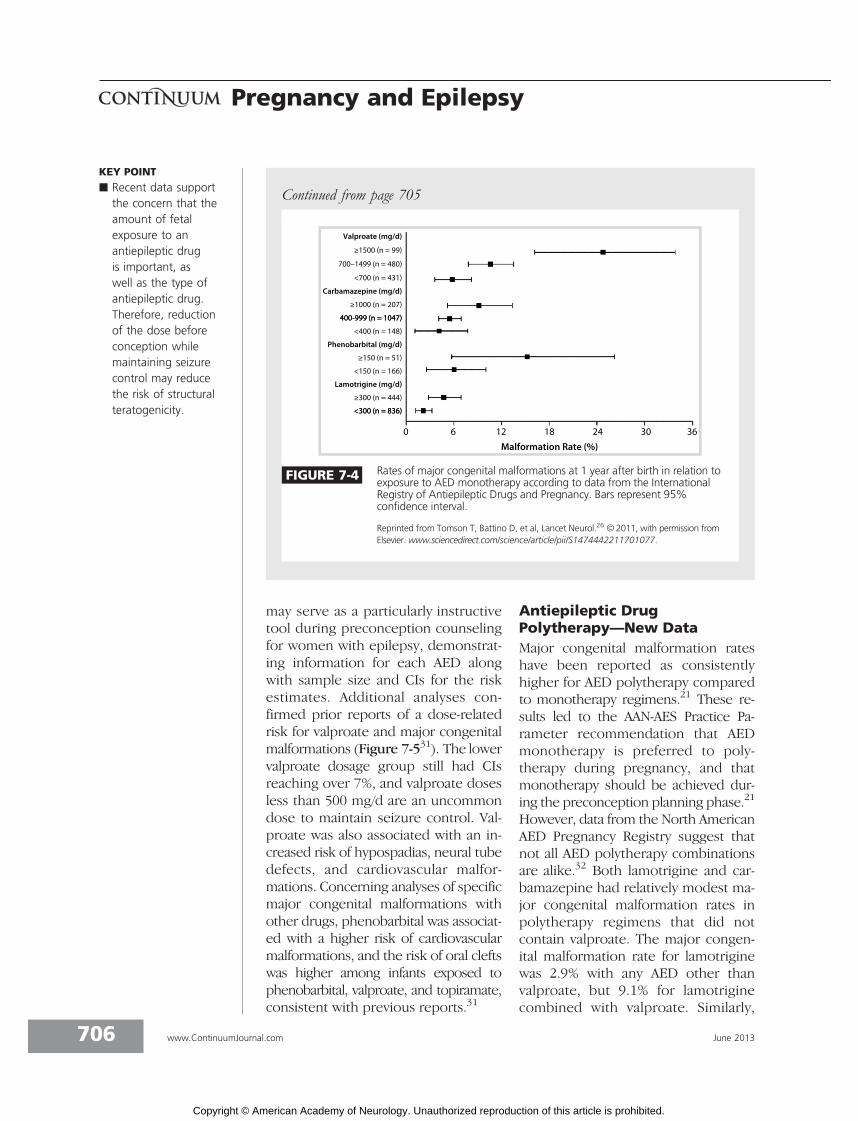
A recent report from the European and International Registryof Antiepileptic Drugs in Pregnancy (EURAP) confirmed that bothAED type and amount of exposure are important factors for teratogenicrisk during structural organogenesis.25 Major congenital malformationrates in pregnancies exposed to carbamazepine, lamotrigine, valproate,and phenobarbital were analyzed by dose at time of conception.The lowest rates of major congenital malformations occurred withlamotrigine at less than 300 mg/d (2.0%; 95% confidence interval[CI] 1.19Y3.24), which served as the comparator group. Risks ofmajor congenital malformations were higher with valproate andphenobarbital at all doses, and with carbamazepine at greater than400 mg/d. Additionally, an increase in major congenital malformationrates was observed with increasing doses for all of the four AEDs(Figure 7-426).
Continued on page 706
705Continuum (Minneap Minn) 2013;19(3):697–714 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
may serve as a particularly instructivetool during preconception counselingfor women with epilepsy, demonstrat-ing information for each AED alongwith sample size and CIs for the riskestimates. Additional analyses con-firmed prior reports of a dose-relatedrisk for valproate and major congenitalmalformations (Figure 7-531). The lowervalproate dosage group still had CIsreaching over 7%, and valproate dosesless than 500 mg/d are an uncommondose to maintain seizure control. Val-proate was also associated with an in-creased risk of hypospadias, neural tubedefects, and cardiovascular malfor-mations. Concerning analyses of specificmajor congenital malformations withother drugs, phenobarbital was associat-ed with a higher risk of cardiovascularmalformations, and the risk of oral cleftswas higher among infants exposed tophenobarbital, valproate, and topiramate,consistent with previous reports.31
Antiepileptic DrugPolytherapy—New DataMajor congenital malformation rateshave been reported as consistentlyhigher for AED polytherapy comparedto monotherapy regimens.21 These re-sults led to the AAN-AES Practice Pa-rameter recommendation that AEDmonotherapy is preferred to poly-therapy during pregnancy, and thatmonotherapy should be achieved dur-ing the preconception planning phase.21
However, data from the North AmericanAED Pregnancy Registry suggest thatnot all AED polytherapy combinationsare alike.32 Both lamotrigine and car-bamazepine had relatively modest ma-jor congenital malformation rates inpolytherapy regimens that did notcontain valproate. The major congen-ital malformation rate for lamotriginewas 2.9% with any AED other thanvalproate, but 9.1% for lamotriginecombined with valproate. Similarly,
KEY POINT
h Recent data supportthe concern that theamount of fetalexposure to anantiepileptic drugis important, aswell as the type ofantiepileptic drug.Therefore, reductionof the dose beforeconception whilemaintaining seizurecontrol may reducethe risk of structuralteratogenicity.
FIGURE 7-4 Rates of major congenital malformations at 1 year after birth in relation toexposure to AED monotherapy according to data from the InternationalRegistry of Antiepileptic Drugs and Pregnancy. Bars represent 95%confidence interval.
Reprinted from Tomson T, Battino D, et al, Lancet Neurol.26 B 2011, with permission fromElsevier. www.sciencedirect.com/science/article/pii/S1474442211701077.
Continued from page 705
706 www.ContinuumJournal.com June 2013
Pregnancy and Epilepsy
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

themajor congenital malformation ratefor carbamazepine was 2.5% with anyAED other than valproate, but 15.4%for carbamazepine combined with val-proate polytherapy.
Neurodevelopmental OutcomesStudies investigating cognitive outcomein children ofwomenwith epilepsy reportan increased risk of mental deficiency.33
Verbal scores on neuropsychometricmeasures may be selectively more in-volved. While AEDs appear to play themajor role, a variety of other factorscontribute to the cognitive problemsof children of women with epilepsy,including seizures, maternal focal sei-zure disorder, minor and major malfor-
mations, lower maternal education, andimpaired maternal-child relations.33
These risk factors may be additive oreven synergistic.
The 2009 AAN-AES Practice Parame-ter updates reported the followingconclusions about in utero exposurethroughout the entire pregnancy andrisk for poor cognitive outcomes: (1)cognition is not reduced in children ofuntreated women with epilepsy (prob-able); (2) carbamazepine does notincrease poor cognitive outcomes com-pared to unexposed controls (proba-ble); (3) monotherapy exposure tovalproate reduces cognitive outcomes(probable); (4) monotherapy exposureto phenytoin or phenobarbital reduces
TABLE 7-3 Risk of Major Congenital Malformations IdentifiedAmong Infants Who Had Been Exposed to a SpecificAntiepileptic Drug Monotherapy Regimen During
the First Trimester and Relative Risk of Major CongenitalMalformations Compared to Both Unexposed and to LamotrigineGroups: North America Pregnancy Registry 1997–2011a
Antiepileptic Drug
Major CongenitalMalformationb
% (95% CI)
Relative Riskto Unexposed(95% CI)
Relative Riskto Lamotrigine(95% CI)
Unexposedc 1.1 (0.37Y2.6) Reference
Lamotrigine 2.0 (1.4Y2.8) 1.8 (0.7Y4.6) Reference
Carbamazepine 3.0 (2.1Y4.2) 2.7 (1.0Y7.0) 1.5 (0.9Y2.5)
Phenytoin 2.9 (1.5Y5.0) 2.6 (0.9Y7.4) 1.5 (0.7Y2.9)
Levetiracetam 2.4 (1.2Y4.3) 2.2 (0.8Y6.4) 1.2 (0.6Y2.5)
Topiramate 4.2 (2.4Y6.8) 3.8 (1.4Y10.6) 2.2 (1.2Y4.0)
Valproate 9.3 (6.4Y13.0) 9.0 (3.4Y23.3) 5.1 (3.0Y8.5)
Phenobarbital 5.5 (2.8Y9.7) 5.1 (1.8Y14.9) 2.9 (1.4Y5.8)
Oxcarbazepine 2.2 (0.6Y5.5) 2.0 (0.5Y7.4) 1.1 (0.4Y3.2)
Gabapentin 0.7 (0.02Y3.8) 0.6 (0.07Y5.2) 0.3 (0.05Y2.5)
Zonisamide 0 (0.0Y3.3) n/a n/a
Clonazepam 3.1 (0.4Y10.8) 2.8 (0.5Y14.8) 1.6 (0.4Y6.8)
CI = confidence interval; n/a = not applicable.a Adapted with permission from Hernandez-Diaz, et al, Neurology.31 B 2012, American Academy ofNeurology. www.neurology.org/content/78/21/1692.abstract?sid=26e79fcc-ce6c-4ab4-ba71-218a72b67ece.
b Diagnosed during pregnancy or before 12 weeks after birth. Confirmed by review of medicalrecords.
c The unexposed internal comparison group were pregnant women not taking an antiepileptic drugwho were recruited from among the friends and family members of the enrolled women takingan antiepileptic drug.
707Continuum (Minneap Minn) 2013;19(3):697–714 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

cognitive outcomes (possible); and (5)AED polytherapy exposure reducescognitive outcomes as compared toAED monotherapy (probable).21
Since the 2009 AAN-AES PracticeParameter update, a few notable reportshave also contributed to our un-derstanding of factors affecting ad-verse neurodevelopmental outcomes.The Neurodevelopmental Effects ofAntiepileptic Drugs (NEAD) study wasa prospective, observational, multicen-ter study in the United States andUnited Kingdom and assessed theneurodevelopmental effects of in uteroexposure to four monotherapy groups(carbamazepine, valproate, phenytoin,and lamotrigine).34 The primary out-come was IQ at 6 years old, adjustedfor maternal IQ, AED type, AED stan-dardized dose, gestational age at birth,and use of periconceptional folate.Primary analysis included 305 mothersand 311 children, with 224 childrencompleting the 6-year follow-up. Multi-
variate analysis demonstrated thatvalproate-exposed children had lowerIQ at age 6 compared to those ex-posed to carbamazepine, lamotrigine,or phenytoin. High doses of valproatewere negatively correlated with IQ,verbal ability, nonverbal ability, mem-ory, and executive function, while theother AEDs did not have a dose effect.Interestingly, mean IQs were higher inthe children of mothers who tookpericonceptional folate (Figure 7-634).In addition, the neurodevelopmentresearch group from Liverpool andManchester reported preliminary find-ings that valproate may specifically beassociated with autism spectrum dis-order. In their small sample size, 6.3%of the children exposed to valproatemonotherapy had clinically diagnosedautism spectrum disorder, sevenfoldhigher than the control group and overtenfold higher than the reported inci-dence in the general population.35
Neonatal ComplicationsRecent reports suggest that there maybe increased risk for other neonatalcomplications for offspring of womenwith epilepsy on AEDs. Findings fromthe 2009 AAN-AES Practice Parameterupdate concluded the following: (1)neonates of women with epilepsytaking AEDs have an increased risk ofbeing small for gestational age ofabout twice the expected rate (probable);and (2) neonates of women with epi-lepsy have an increased risk of a 1-minuteApgar score of less than 7 of abouttwice the expected rate (possible).21
Since this parameter was released, astudy from Taiwan reported that sei-zures in women with epilepsy duringpregnancy were independently as-sociated with an approximate 1.5-foldincreased risk for preterm delivery orinfants being born small for gesta-tional age.36 A recent secondary analysisof the neonatal outcomes from theNEAD
KEY POINT
h Children born towomen with epilepsyreceiving valproateduring pregnancy areat a fivefold higherrisk of having amajor congenitalmalformation, lowerIQ, and possibly autismspectrum disorder.
FIGURE 7-5 Risk of major malformations by averagevalproate dose (mg) during the first trimester.
Reprinted with permission from Hernandez-Dıaz S, et al,Neurology.31 B 2012, American Academy of Neurology.www.neurology.org/content/78/21/1692.abstract?sid=26e79fcc-ce6c-4ab4-ba71-218a72b67ece.
708 www.ContinuumJournal.com June 2013
Pregnancy and Epilepsy
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

cohort reported that adverse neonataloutcome risks may differ between theAEDs; the OR for infants being bornsmall for gestational age was higher forthe valproate and carbamazepine groups,and reduced 1-minute Apgar scoresoccurred more frequently in the phe-nytoin and valproate groups.37
Seizures During PregnancyThe effect of pregnancy on seizure fre-quency is variable. Approximately 20%to 33% of pregnant women with epi-lepsy experience an increase in seizurefrequency, 7% to 25% experience a de-crease, and 50% to 83% have no signif-icant change.38 The physiologic changesand psychosocial adjustments that ac-company pregnancy can alter seizure fre-quency, including changes in sex-hormoneconcentrations, changes in AED metab-olism, sleep deprivation, and new stresses.Noncompliance with medications iscommon during pregnancy and is fre-quently due to the perception that AEDsduring pregnancy are harmful to thefetus. Teratogenic effects of AEDs, whilenot uncommon, are often exaggeratedor misrepresented. Proper education
about the risks of AEDs versus the risksof seizures can be very helpful inassuring compliance during pregnancy.
The risk of seizures to the fetusshould be discussed thoroughly withthe patient and other family members.Generalized tonic-clonic seizures cancause maternal and fetal hypoxia andacidosis, fetal heart-rate decelerations,and possibly miscarriages and still-births. Nonconvulsive seizures cancause trauma, which can result in rup-tured fetal membranes with an increasedrisk of infection, premature labor, andeven fetal death. In addition to thephysical risks of seizures to the develop-ing fetus, reemergence of seizures in awoman who had previously experi-enced seizure control can be devastating.Besides the immediate risk to herself andthe fetus, loss of driving privileges mayhave remarkable psychosocial impact.
Antiepileptic DrugManagementin Light of PharmacokineticChanges Intrapartumand PostpartumMaintaining seizure stability duringpregnancy depends on maintaining
FIGURE 7-6 Child IQ at 6 years of age, by exposure to maternal antiepileptic drug use andpericonceptional folate. Mean (95% confidence intervals) are shown for folate(solid lines) and no folate (dashed lines).
IQ = intelligence quotient.
Reprinted from Meador KJ, et al, Lancet Neurol.33 link.springer.com/article/10.1007/s11910-002-0013-6.
709Continuum (Minneap Minn) 2013;19(3):697–714 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

therapeutic AED concentrations. Thetarget concentration should be individ-ually determined in the preconceptionphase with respect to epilepsy historyand previous benchmark AED concentra-tions. During pregnancy, AED dosingbecomes complex and requires an in-tensive approach. Clearance of mostAEDs increases during pregnancy, re-sulting in decreased serum concentra-t ions (Table 7-4) .22 ,39 Severalphysiologic factors contribute to de-clining AED levels during pregnancy,including hepatic enzymatic inductionvia increased female sex steroid hor-mones, increased volume of dis-
tribution, decreased concentration ofalbumin and "1-acid glycoproteins, in-creased renal blood flow, and altera-tions in drug absorption (see Case 7-1).
The 2009 AAN-AES Practice Param-eter update concluded that pregnancycauses an increase in the clearanceand a decrease in the concentration oflamotrigine, phenytoin, and to a lesserextent carbamazepine (probable), anddecreases the level of levetiracetam andthe active oxcarbazepine metabolite, themonohydroxy derivative (possible).22
The magnitude of enhanced lamo-trigine clearance during pregnancy ex-ceeds the clearance described for most
TABLE 7-4 Alterations of Antiepileptic Drug Clearance and/or Concentrations DuringPregnancy: Summary of Class I, II, and III Studiesa
Antiepileptic Drug
ReportedIncreases inClearance
Reported Decreasesin TotalConcentrations
Reported Changes inFree Antiepileptic Drugsor Metabolites
Phenytoin 19%Y150% 60%Y70% Free phenytoin clearance increasedin trimester 3 by 25%; freephenytoin concentration decreasedby 16%Y40% in trimester 3
Carbamazepine -11%Y27% 0%Y12% No change
Phenobarbital 60% 55% Decrease in free phenobarbitalconcentration by 50%
Primidone Inconsistent Inconsistent Decrease in derived phenobarbitalconcentrations, with lowerphenobarbital/primidone ratios
Valproic acid Increased bytrimesters 2and 3
No reports No change in clearance of freevalproic acidFree fraction increased bytrimesters 2 and 3
Ethosuximide Inconsistent Inconsistent
Lamotrigine 65%Y230%,substantialinterindividualvariability
No reports 89% increase in clearance offree lamotrigine
Oxcarbazepine No reports Monohydroxyderivative ofoxcarbazepine andactive moietydecreased by 36%Y61%
No reports
Levetiracetam 243% 60% by trimester 3 No reportsa Reprinted from Pennell PB, Hovinga CA, Int Rev Neurobiol.39 B 2012, with permission from Elsevier. www.sciencedirect.com/science/article/pii/S0074774208000135.
710 www.ContinuumJournal.com June 2013
Pregnancy and Epilepsy
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

older AEDs because it is primarily elim-inated via hepatic glucuronidation,which is particularly susceptible toactivation during pregnancy because ofdirect effects of rising female sex steroidhormones levels. Both lamotrigine freeand total clearance were increasedduring all 3 trimesters, with peaks of94% (total) and 89% (free) in the thirdtrimester in a class I prospective ob-servational study of 53 pregnancies in53 women, using 305 samples through-out preconception baseline, pregnancy,and postpartum.40 Seizure frequencysignificantly increased when lamo-trigine levels decreased to 65% of thepreconceptional individualized targetlamotrigine concentration, supportingthe recommendation to monitor thelevels of AEDs, which decrease dur-ing pregnancy.40 Previous studies oflamotrigine during pregnancy noted arapid decrease in lamotrigine clearanceduring the early postpartum periodwith reports of symptomatic toxicity.Nonadherence to a standard lamotrigine
taper schedule has been shown to beassociated with a significantly higherrisk for postpartum toxicity.40 Mostother AED levels gradually increaseafter delivery and plateau by 10 weekspostpartum. The exact time course isnot well established for other AEDs, butAED doses should be adjusted andlevels should be followed during thepostpartum period.
BONE HEALTHBoth men and women with epilepsyhave elevated rates of fractures (two- tosixfold higher) compared to the generalpopulation.41 Although seizure-relatedinjuries may contribute to these ele-vated rates, AEDs independently con-tribute to this risk, especially theenzyme-inducing AEDs.41,42
Dual-energy x-ray absorptiometry(DXA) can assess bone mineral density.Depressed bone mineral density is themost significant predictor of fracture.Bone mineral density measurementsreveal osteopenia or osteoporosis in 38%
KEY POINT
h Therapeutic drugmonitoring ofantiepileptic drugconcentrations duringpregnancy isrecommended.Establishing theindividualized idealantiepileptic drugconcentration isimportant as a targetto maintain duringpregnancy. Dosagesof the antiepilepticdrug will need tobe readjusted in thepostpartum period.
Case 7-2A 60-year-old, right-handed woman was referred to reassess phenytoinuse for epilepsy in the setting of a recent osteoporosis diagnosis. Seizureonset was at 19 years old. Characteristic habitual clinical seizures beganwith an aura of things appearing surreal, followed by a generalizedtonic-clonic seizure. Initial antiepileptic drugs were phenobarbital, thenphenytoin, which eventually produced seizure freedom, althoughcomplications included gingival hyperplasia requiring surgical treatment,and the patient recently learned she had osteoporosis despite an intensivefitness regimen. Recent brain MRI also revealed moderate cerebellaratrophy and a left frontal cavernous malformation. Neurologicexamination was notable for difficulty with tandem gait and findingsof a mild distal polyneuropathy; 25-OH vitamin D levels were withinnormal limits. The patient was transitioned to lamotrigine and remainedseizure free. Her primary care physician was contacted to continue tofollow and manage her osteoporosis.
Comment. A common practice is to ‘‘leave well enough alone’’ whena patient has been seizure free. However, neurologists should be awareof increased risks for osteopenia and osteoporosis with chronic use ofenzyme-inducing antiepileptic drugs, especially phenytoin, and considersubstitution to prevent bone fracture.
711Continuum (Minneap Minn) 2013;19(3):697–714 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

to 60% of people with epilepsy receivingAEDs in specialty clinics, with longerduration of AED therapy associated withfurther decreased bone mineral density.Enzyme-inducing AEDs independentlyreduce bone mineral density.41
The effects of enzyme-inducing AEDsare thought to be related to their cyto-chrome P450 (CYP) enzyme inductionleading to accelerated metabolism ofvitamin D to inactivemetabolites and/orlower (free) estradiol levels.43 How-ever, some enzyme-inducing AEDs aremore consistently associated with in-creased fracture, decreased bone min-eral density, and alterations in bonemetabolism. For example, chronicphenobarbital is associated with de-creased active vitamin D levels, andcarbamazepine is not consistently as-sociated with decreased bone mineraldensity.41 On the other hand, phenyt-oin use has more consistently demon-strated properties of increased boneturnover in premenopausal womenwith epilepsy compared to other AEDs(valproate, lamotrigine, and even carba-mazepine).44 In another study, pre-menopausal women received one ofthese four AEDs for 1 year.45 In thephenytoin group, the biochemical pat-tern differed and demonstrated apattern consistent with hyperparathy-roidism and increased remodeling. Injust 1 year, significant bone mineraldensity loss (2.6%) was seen at thefemoral neck in the phenytoin group(Case 7-2).
SUMMARYOptimal treatment of women withepilepsy includes consideration of thecomplex interactions of female sexsteroid hormones with epilepsy andAEDs, and the potential risks of anyAED prescribed during pregnancy.Understanding these key factors en-hances the ability to make informedtreatment recommendations that will
provide improved seizure control withfewer adverse health effects for womenwith epilepsy during their reproductiveyears, and maximize chances for op-timal maternal and child outcomes afterAED treatment during pregnancy.
REFERENCES1. Harden CL, Pennell PB. Neuroendocrine
considerations in the treatment of menand women with epilepsy. Lancet Neurol2013;12(1):72Y83.
2. Herzog AG, Klein P, Ransil BJ. Three patternsof catamenial epilepsy. Epilepsia 1997;38(10):1082Y1088.
3. Mattson RH, Cramer JA, Caldwell BV,Siconolfi BC. Treatment of seizures withmedroxyprogesterone acetate: preliminaryreport. Neurology 1984;34(9):1255Y1258.
4. Herzog AG, Fowler KM, Smithson SD, et al.Progesterone vs placebo therapy for womenwith epilepsy: a randomized clinical trial.Neurology 2012;78(24):1959Y1966.
5. Klein P, Serje A, Pezzullo JC. Prematureovarian failure in women with epilepsy.Epilepsia 2001;42(12):1584Y1589.
6. Harden CL, Koppel BS, Herzog AG, et al.Seizure frequency is associated with ageof menopause in women with epilepsy.Neurology 2003;61(4):451Y455.
7. Harden CL, Pulver MC, Ravdin L,Jacobs AR. The effect of menopause andperimenopause on the course of epilepsy.Epilepsia 1999;40(10):1402Y1407.
8. Harden CL, Herzog AG, Nikolov BG, et al.Hormone replacement therapy in womenwith epilepsy: a randomized, double-blind,placebo-controlled study. Epilepsia 2006;47(9):1447Y1451.
9. HerzogAG. A relationship between particularreproductive endocrine disorders and thelaterality of epileptiform discharges inwomen with epilepsy. Neurology 1993;43(10):1907Y1910.
10. Azziz R, Carmina E, Dewailly D, et al. TheAndrogen Excess and PCOS Society criteriafor the polycystic ovary syndrome: thecomplete task force report. Fertil Steril2009;91(2):456Y488.
11. Pylvanen V, Pakarinen A, Knip M, Isojarvi J .Characterization of insulin secretion inValproate-treated patients with epilepsy.Epilepsia 2006;47(9):1460Y1464.
12. Morrell MJ, Hayes FJ, Sluss PM, et al.Hyperandrogenism, ovulatory dysfunction,
KEY POINT
h Although more researchis needed to understandunderlying mechanismsfor bone densityloss associated withantiepileptic drugs,awareness of riskfor osteopenia orosteoporosis shouldbe a considerationin antiepileptic drugselection andmaintenance.
712 www.ContinuumJournal.com June 2013
Pregnancy and Epilepsy
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
and polycystic ovary syndrome withvalproate versus lamotrigine. Ann Neurol2008;64(2):200Y211.
13. Morrell MJ, Flynn KL, Done S, et al.Sexual dysfunction, sex steroid hormoneabnormalities, and depression in womenwith epilepsy treated with antiepilepticdrugs. Epilepsy Behav 2005;6(3):360Y365.
14. Sukumaran SC, Sarma PS, Thomas SV.Polytherapy increases the risk of infertilityin women with epilepsy. Neurology 2010;75(15):1351Y1355.
15. Dansky LV, Andermann E, Andermann F.Marriage and fertility in epileptic patients.Epilepsia 1980;21(3):261Y271.
16. Artama M, Isojarvi JI, Raitanen J, et al.Birth rate among patients with epilepsy: anationwide population-based cohort studyin Finland. Am J Epidemiol 2004;159(11):1057Y1063.
17. Olafsson E, Hallgrimsson JT, Hauser WA,et al. Pregnancies of women with epilepsy:a population-based study in Iceland.Epilepsia 1998;39(8):887Y892.
18. Crawford P, Hudson S. Understandingthe information needs of women withepilepsy at different lifestages: results ofthe ‘Ideal World’ survey. Seizure 2003;12(7):502Y507.
19. Centers for Disease Control and Prevention(CDC). U S. Medical Eligibility Criteria forContraceptive Use, 2010. MMWR RecommRep 2010;59(RR-4):1Y86.
20. Bounds W, Guillebaud J. Observationalseries on women using the contraceptiveMirena concurrently with anti-epilepticand other enzyme-inducing drugs.J Fam Plann Reprod Health Care 2002;28(2):78Y80.
21. Harden CL, Meador KJ, Pennell PB, et al.Practice parameter update: managementissues for women with epilepsyVfocus onpregnancy (an evidence-based review):teratogenesis and perinatal outcomes:report of the Quality Standards Subcommitteeand Therapeutics and Technology AssessmentSubcommittee of the American Academy ofNeurology and American Epilepsy Society.Neurology 2009;73(2):133Y141.
22. Harden CL, Pennell PB, Koppel BS, et al.Practice parameter update: managementissues for women with epilepsyVfocus onpregnancy (an evidence-based review):vitamin K, folic acid, blood levels, andbreastfeeding: report of the QualityStandards Subcommittee and Therapeuticsand Technology Assessment Subcommitteeof the American Academy of Neurology and
American Epilepsy Society. Neurology 2009;73(2):142Y149.
23. Harden CL, Hopp J, Ting TY, et al. Practiceparameter update: management issues forwomen with epilepsyVfocus on pregnancy(an evidence-based review): obstetricalcomplications and change in seizurefrequency: report of the Quality StandardsSubcommittee and Therapeutics andTechnology Assessment Subcommittee ofthe American Academy of Neurology andAmerican Epilepsy Society. Neurology2009;73(2):126Y132.
24. Pennell PB. Antiepileptic drugs duringpregnancy: what is known and which AEDsseem to be safest? Epilepsia 2008;49(suppl 9):43Y55.
25. Tomson T, Battino D, Bonizzoni E, et al.Dose-dependent risk of malformationswith antiepileptic drugs: an analysis ofdata from the EURAP epilepsy andpregnancy registry. Lancet Neurol 2011;10(7):609Y617.
26. Tomson T, Battino D. Teratogenic effectsof antiepileptic drugs. Lancet Neurol 2012;11(9):803Y813.
27. Hunt S, Russell A, Smithson WH, et al.Topiramate in pregnancy: preliminaryexperience from the UK Epilepsy andPregnancy Register. Neurology 2008;71(4):272Y276.
28. Margulis AV, Mitchell AA, Gilboa SM, et al.Use of topiramate in pregnancy and risk oforal clefts. Am J Obstet Gynecol2012;207(5):405.e1Y405.e7.
29. Werler MM, Ahrens KA, Bosco JL, et al. Useof antiepileptic medications in pregnancyin relation to risks of birth defects. AnnEpidemiol 2011;21(11):842Y850.
30. Pennell PB. The devil is in the details: notall AED-associated major congenitalmalformations are equal. Epilepsy Curr2011;11(3):79Y81.
31. Hernandez-Dıaz S, Smith CR, Shen A, et al.Comparative safety of antiepileptic drugsduring pregnancy. Neurology 2012;78(21):1692Y1699.
32. Holmes LB, Mittendorf R, Shen A, et al.Fetal effects of anticonvulsant polytherapies:different risks from different drugcombinations. Arch Neurol 2011;68(10):1275Y1281.
33. Meador KJ. Neurodevelopmental effects ofantiepileptic drugs. Curr Neurol NeurosciRep 2002;2(4):373Y378.
34. Meador KJ, Baker GA, Browning N, et al.Fetal antiepileptic drug exposure and
713Continuum (Minneap Minn) 2013;19(3):697–714 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

cognitive outcomes at age 6 years (NEADstudy): a prospective observational study.Lancet Neurol 2013;12(3):244Y252.
35. Bromley RL, Mawer GE, Briggs M, et al.The prevalence of neurodevelopmentaldisorders in children prenatally exposedto antiepileptic drugs [published onlineahead of print January 31, 2013]. J NeurolNeurosurg Psychiatry 2013. doi:10.1136/jnnp-2012-304270.
36. Chen YH, Chiou HY, Lin HC, Lin HL. Affect ofseizures during gestation on pregnancyoutcomes in women with epilepsy. ArchNeurol 2009;66(8):979Y984.
37. Pennell PB, Klein AM, Browning N, et al.Differential effects of antiepileptic drugs onneonatal outcomes. Epilepsy Behav2012;24(4):449Y456.
38. EURAP Study Group. Seizure control andtreatment in pregnancy: observations fromthe EURAP epilepsy pregnancy registry.Neurology 2006;66(3):354Y360.
39. Pennell PB, Hovinga CA. Antiepileptic drugtherapy in pregnancy I: gestation-inducedeffects on AED pharmacokinetics. Int RevNeurobiol 2008;83:227Y240.
40. Pennell PB, Peng L, Newport DJ, et al.Lamotrigine in pregnancy: clearance,therapeutic drug monitoring, and seizurefrequency. Neurology 2008;70(22 pt 2):2130Y2136.
41. Brodie MJ, Mintzer S, Pack AM, et al. Enzymeinduction with antiepileptic drugs: causefor concern? Epilepsia 2013;54(1):11Y27.
42. Carbone LD, Johnson KC, Robbins J, et al.Antiepileptic drug use, falls, fractures,and BMD in postmenopausal women:findings from the women’s health initiative(WHI). J Bone Miner Res 2010;25(4):873Y881.
43. Pack AM, Morrell MJ, McMahon DJ, Shane E.Normal vitamin D and low free estradiollevels in women on enzyme-inducingantiepileptic drugs. Epilepsy Behav 2011;21(4):453Y458.
44. Pack AM, Morrell MJ, Marcus R, et al. Bonemass and turnover in women with epilepsyon antiepileptic drug monotherapy. AnnNeurol 2005;57(2):252Y257.
45. Pack AM, Morrell MJ, Randall A, et al. Bonehealth in young women with epilepsy afterone year of antiepileptic drug monotherapy.Neurology 2008;70(18):1586Y1593.
714 www.ContinuumJournal.com June 2013
Pregnancy and Epilepsy
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.