predictors of imatinib failure in cml by prof. abinya
TRANSCRIPT

PREDICTORS OF IMATINIB FAILURE IN CML
Esther Musyoka Dindi, N.A.Othieno-Abinya, Grace W Kitonyi.
Department of Clinical Medicine and Therapeutics, University of Nairobi.

CML: Massive splenomegaly

The history of CML
1845
First description of CML
1865
Fowlers’s solution -1% arsenic trioxide
2001
Imatinib
1879
Staining methods for blood
1903 1953 19831965
Radiotherapy
Busulfan
Hydroxyurea
Interferon
1968
BMT
2006
Dasatinib,Nilotinib
2012
BosutinibPonatinib
1960:Nowell & Hungerford describe the Philadelphia Chromosome
1973:Janet Rowley describes the9:22 translocation
1999: After seminal preclinical work first clinical trials commence with STI571 (imatinib)
1845:John Hughes Bennett reported a “Case of Hypertrophy of the Spleen and Liver in which Death Took Place from Suppuration of the Blood” in the Edinburgh Medical Journal
Today:5 kinase
Inhibitorsdeveloped

What is Philadelphia process?
• Co-habitation between a man with a rich woman goes sore and leaves a very bitter man, even poorer than before.• He becomes violent


Watson and Crick


Background
Imatinib mesylate: A small molecule tyrosine kinase inihibitor Targets BCR-ABL,KIT, PDGFR, and stem cell
factor. Revolutionized the treatment of chronic
myeloid leukaemia (CML). Treatment failure with imatinib has been
demonstrated in approximately 10% to 15% of CML patients.

Imatinib---abl kinase interaction

Importance of monitoring
Early identification of patients at risk of failures is important so that they can be put on alternative treatments.
Predictors of failure in CML are yet to be fully established
Sokal, Hasford and EUTOS scores are being used to predict cytogenetic response in some centres.
No study had been carried out locally to determine response to imatinib,the magnitude of failure, and its possible predictors.

Objectives
• To determine the haematological response of CML patients receiving imatinib, the proportion of patients with hematological failure
• To describe the clinical and haematological characteristics of patients with hematological failure and compare them with those with optimal response.

Methodology
Study design: A cross-sectional descriptive study. Setting: The Nairobi Hospital GIPAP clinic.
Subjects: Philadelphia chromosome positive (Ph+ve) CML patients on imatinib therapy for at least 3 months

Information sought
• Socio-demographic parameters including age and sex
• Clinical parameters including presence of splenomegaly or hepatomegaly
• Laboratory parameters.• History of prior leukemia-targetted therapy• Duration between CML diagnosis and start of
imatinib

• Duration of CML from diagnosis• Duration on imatinib • Time taken to achieve complete
haematological response• Results of haematologic, cytogenetic or
molecular studies• Evidence of haematological treatment failure.

• Characteristics of patients with haematological failure were recorded and compared with those of patients with good response.

RESULTS
• 206 patients were included.• The mean age was 38.6years with a range of
14-85 years. There was slight male preponderance; 115(55.8%) and 91(44.2%) females.

Bone marrow findings at diagnosis
• Phase Number Percentage• Chronic 182 92.2• Accelerated 10 4.9• Blastic 2 1• Dry tap 1 0.5• Inconclusive 2 1

Results
• Complete hematologic response was attained within 3 months of imatinib therapy and sustained in 79.1%.
• 20.9% were found to have hematologic failure, and of these, 21% had primary failure with the rest having secondary failure.

Predictors of failure
Missed doses (60.5% vs 37.4%) Higher BCR-ABL concentration(mean of 81%
vs 68.2%) at diagnosis Longer durations between diagnosis and start
of therapy with imatinib. On logistic regression, only prolonged
duration between diagnosis and commencement of imatinib was an independent predictor of failure (OR 2.69(1.03-7.03 95%CI, p = 0.043).
• The Sokal and Hasford risk scores did not significantly predict for treatment outcome.
• EUTOS score was not applied in the majority

DISCUSSION

Estimated Annual Rate of Treatment Failure IRIS Estimated Annual Rate of Treatment Failure IRIS StudyStudy
General PopulationGeneral Population Complete Cytogenetic Complete Cytogenetic ResponseResponse
Year 1Year 1 3.3%3.3% 5.5%5.5%
Year 2Year 2 7.5%7.5% 2.3%2.3%
Year 3Year 3 4.8%4.8% 1.1%1.1%
Year 4Year 4 1.5%1.5% 0.4%0.4%
Year 5Year 5 0.9%0.9%
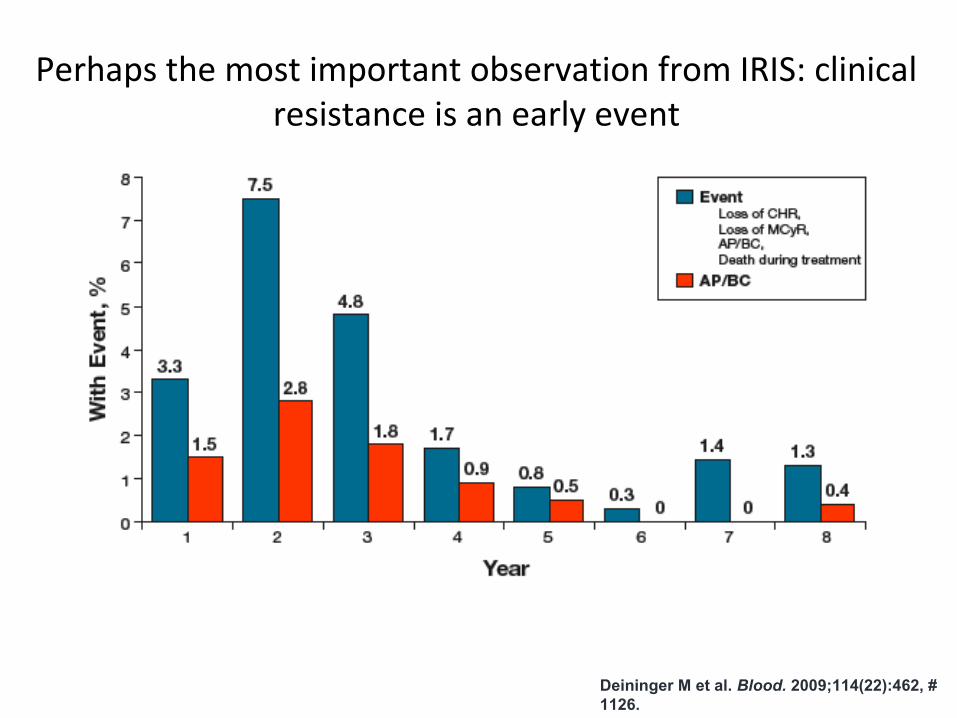
Perhaps the most important observation from IRIS: clinical resistance is an early event
Deininger M et al. Blood. 2009;114(22):462, # 1126.

CCyR expected @ 12mo for progression protection, MMR at 18mo for protection against any event
Hughes T et al Blood 116:3758-65, 2010Marin D, et al. Blood. 2008;112:4437-4444.
IRIS: Impact of transcript levels(CCyR equivalent
and MMR):
12 mo response: AP/BC progression
18 mo response: all events
Response at 12 months n Loss of CCyR
CCyR without MMR 95 24%
CCyR plus MMR 32 3%
Months Since Start of Imatinib Therapy
Loss
of C
CyR
(%
)
P = 0.04
0
20
40
60
80
100
0 6 12 18 24 30 36 42 48 54 60
Single-institution analysis of patients with CP CML (n = 224) showed significant loss of response in cases lacking MMR at 12mo
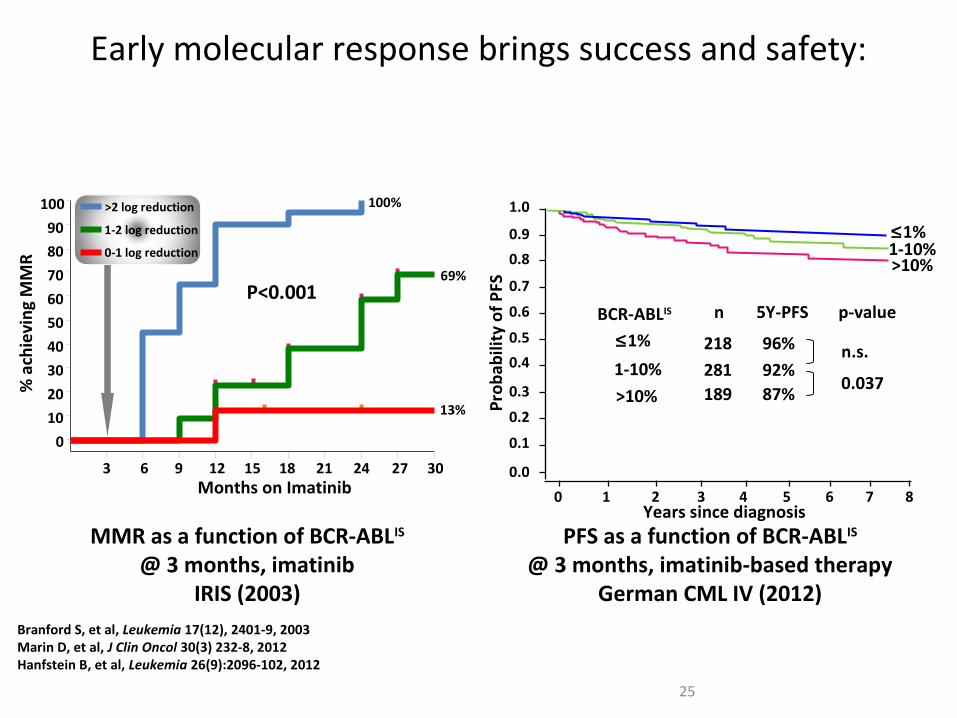
Early molecular response brings success and safety:
Branford S, et al, Leukemia 17(12), 2401-9, 2003Marin D, et al, J Clin Oncol 30(3) 232-8, 2012Hanfstein B, et al, Leukemia 26(9):2096-102, 2012
25
Months on Imatinib
% a
chie
ving
MM
R
50
60
70
80
90
100
20
30
40
10
0
P<0.00169%
100%
3 6 9 12 15 18 24 3021 27
13%
>2 log reduction
1-2 log reduction
0-1 log reduction
0.0
0 1 2 3 4 5 6 7 8
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Prob
abili
ty o
f PFS
>10%1-10%≤1%
BCR-ABLIS
≤1%
1-10%
>10%
n
218281189
5Y-PFS
96%92%87%
p-value
n.s.
0.037
Years since diagnosisPFS as a function of BCR-ABLIS
@ 3 months, imatinib-based therapy German CML IV (2012)
MMR as a function of BCR-ABLIS
@ 3 months, imatinibIRIS (2003)

Tyrosine kinase inhibitors are capable of inducing molecular and cytogenetic response but not hydroxyurea
Those on other therapies including hydroxyurea likely to have accumulated other cytogenetic/molecular abnormalities that could influence downstream signalling.Likely to have accumulated drug resistant mutants in line with Goldie-Coldman hypothesis

• Norton-Simon resistance could have applied to some extent

ACKNOWLEDGEMENTS
Esther Musyoka Dindi
Grace w. Kitonyi
Walter O Mwanda
The Nairobi Hospital CEO
Mary Kisingu and Mary Kiarie
Staff at Anderson Centre.