pre-operative cardiac evaluation - cmcmac.in cme pdfs/18 dr. cijoy pre-operative medical... ·...
TRANSCRIPT

PRE-OPERATIVE MEDICAL EVALUATION IN THE SECONDARY CARE SETTING

OUTLINE
• Premise
• Purpose
• Principles
• Practice

PREMISE Indications and evidence for the Physician consultation

INDICATIONS

WHY WOULD A SURGEON REQUEST A PHYSICIAN CONSULT?
• Common practice – clinical and legal reasons
• Usually not specialty specific in secondary care
• Often implies comprehensive medical evaluation
• Rationale – high risk of medical complications post-operatively

FREQUENCY OF POSTOPERATIVE COMPLICATIONS
Complication Incidence (%)
Infection 14.3
Respiratory 9.5
Cardiac 4.5
Khuri SF, Daley J, Henderson W, Barbour G, Lowry P, Irvin G, et al. The National
Veterans Administration Surgical Risk Study: risk adjustment for the comparative
assessment of the quality of surgical care. J Am Coll Surg. 1995;180:519–31.

FREQUENCY OF POSTOPERATIVE COMPLICATIONS
Complication Incidence (%)
Infection 14.3
Wound 5.1
Pneumonia 3.6
Urinary tract 3.5
Systemic sepsis 2.1
Khuri SF, Daley J, Henderson W, Barbour G, Lowry P, Irvin G, et al. The National
Veterans Administration Surgical Risk Study: risk adjustment for the
comparative assessment of the quality of surgical care. J Am Coll Surg.
1995;180:519–31.

FREQUENCY OF POSTOPERATIVE COMPLICATIONS
Complication Incidence (%)
Respiratory 9.5
Pneumonia 3.6
Failure to wean from respirator in 48 hours
3.2
Unplanned intubation 2.4
Pulmonary embolus 0.3
Khuri SF, Daley J, Henderson W, Barbour G, Lowry P, Irvin G, et al. The National
Veterans Administration Surgical Risk Study: risk adjustment for the comparative
assessment of the quality of surgical care. J Am Coll Surg. 1995;180:519–31.

FREQUENCY OF POSTOPERATIVE COMPLICATIONS
Complication Incidence (%)
Cardiac 4.5
Pulmonary edema 2.3
Cardiac arrest 1.5
Myocardial infarction 0.7
Khuri SF, Daley J, Henderson W, Barbour G, Lowry P, Irvin G, et al. The National
Veterans Administration Surgical Risk Study: risk adjustment for the comparative
assessment of the quality of surgical care. J Am Coll Surg. 1995;180:519–31.

EVIDENCE

CONFLICTING REPORTS ON BENEFITS
Consultation
• Identify issues and recommend interventions
• Optimize medical conditions
• High clinician satisfaction
No Consultation
• Frequency of detection of new issues too less
• Cancel or delay in procedures
• May be over or under-utilized
Levinson W. Preoperative evaluations by an internist--are they worthwhile? West J Med 1984; 141:395. Macpherson DS, Lofgren RP. Outpatient internal medicine preoperative evaluation: a randomized clinical trial. Med Care 1994; 32:498 Devor M, Renvall M, Ramsdell J. Practice patterns and the adequacy of residency training in consultation medicine. J Gen Intern Med 1993; 8:554 Chen LM, Wilk AS, Thumma JR, et al. Use of medical consultants for hospitalized surgical patients: an observational cohort study. JAMA Intern Med 2014; 174:1470.
CONFLICTING REPORTS ON BENEFITS
Consultation • 3 cohort studies showed decreased
length of stay
• Slight reduction in overall costs
No Consultation
• 1 retrospective cohort showed no change; another increased
• Increased cost of consultation
Levinson W. Preoperative evaluations by an internist--are they worthwhile? West J Med 1984; 141:395. Macpherson DS, Lofgren RP. Outpatient internal medicine preoperative evaluation: a randomized clinical trial. Med Care 1994; 32:498 Devor M, Renvall M, Ramsdell J. Practice patterns and the adequacy of residency training in consultation medicine. J Gen Intern Med 1993; 8:554 Chen LM, Wilk AS, Thumma JR, et al. Use of medical consultants for hospitalized surgical patients: an observational cohort study. JAMA Intern Med 2014; 174:1470.

HIGHER MORTALITY?
• Slightly higher 30 day and 1 year mortality in those who had medical consultation pre-operatively
• Probably due to selection bias
Wijeysundera DN, Austin PC, Beattie WS, et al. Outcomes and processes of care related
to preoperative medical consultation. Arch Intern Med 2010; 170:1365.

EVIDENCE ON PRE-OPERATIVE PHYSICIAN EVALUATION
• Strong evidence is lacking
• Practice is widespread
• Legal implications abound
• Could improve outcomes

PURPOSE Goals of the Physician Consultation

GOALS OF PRE-OPERATIVE EVALUATION
Identify – Optimize – Manage
• Identifying unrecognized comorbid disease and risk factors for medical complications of surgery
• Optimizing the preoperative medical condition and medications
• Recognizing and treating potential complications
In all these, working effectively as a member of the pre and peri-operative team (including surgical and anesthesia colleagues)

PRINCIPLES Principles of the Physician Consultation

THE “TEN COMMANDMENTS”
1. Determine the question and respond to it.
2. Establish the urgency of the consultation and provide a timely response.
3. "Look for yourself"; confirm the history and physical examination and check test results.
4. Be as brief as appropriate; be definitive and limit the number of recommendations.
5. Be specific, including medication details.
Goldman L, Lee T, Rudd P. Ten commandments for effective consultations. Arch Intern Med
1983; 143:1753.

THE “TEN COMMANDMENTS”
6. Provide contingency plans; anticipate potential problems and questions.
7. Honor thy turf; don't steal other clinician's patients.
8. Teach with tact; consult, don't insult.
9. Talk is cheap and effective; direct verbal communication is crucial.
10. Follow-up to ensure that recommendations are followed.
Goldman L, Lee T, Rudd P. Ten commandments for effective consultations. Arch Intern Med
1983; 143:1753.
THE QUESTION
• Not clear often - try to determine
• 50% for ‘evaluation’ and 40% for ‘medical clearance’
• The myth of ‘clearance’ – ‘average risk’
• Concept of co-management
• If ‘clearance’ is asked for without a specific question, global pre-operative evaluation needed
Kleinman B, Czinn E, Shah K, et al. The value to the anesthesia-surgical care team of the
preoperative cardiac consultation. J Cardiothorac Anesth 1989; 3:682.

PRACTICE Approach for the Physician Consultation

APPROACH

APPROACH 1: Is the proposed procedure an emergency? If not, step 2.
2: Risk assessment
What are the risks involved? – investigate appropriately
3: Reversal of the correctable
Are any of these reversible? – make a time-bound plan
4: Reduction of complications
How can the expected complications be minimized? – appropriate interventions
5: Re-organize medications
What are the precautions regarding medications?
– instructions on starting, stopping, re-starting, reducing, increasing medications

‘RELATIVE RISK’
Step 1

EMERGENCY OR NOT?
• Which is a higher risk to life?
• Clinical risk stratification for documentation
• Proceed

RISK ASSESSMENT
Step 2

OVERALL RISK WHAT IS WRONG AND HOW BAD IS IT?
History – Known risk factors
• Effort tolerance - METS
• Past, personal and treatment
Examination – Known and unknown risk factors
• Assess status of known
• Unknown – eg: stenotic valvular lesion
Investigation - Known and unknown risk factors
• Identify unknown risk factors
• Assess status of known

HISTORY AND EXAMINATION

EFFORT TOLERANCE
• METS – metabolic equivalents
• One MET equals the oxygen consumption of a 70-kg, 40-year-old man in a resting state
• > 4 METS considered good
• Cycling, climbing 1 flight of stairs, walking 4 mph, yard work, sweeping floor/yard etc.
Fletcher GF, Balady G, Froelicher VF, Hartley LH, Haskell WL, Pollock ML.
Exercise standards. A statement for healthcare professionals from the American Heart
Association.
Circulation 1995;91:580-615.

HIGH RISK FACTORS AND THEIR IMPLICATIONS
System Risk factors Implications
Cardiovascular Unstable angina
Recent MI
Decompensated CHF
Significant arrhythmias
Severe valvular
disease
Perioperative cardiac
events

REVISED GOLDMAN CARDIAC RISK INDEX(RCRI)
6 independent risk factors Points
Cerebrovascular disease 1
Congestive heart failure 1
Creatinine level > 2.0 mg per dL (176.80 μmol per L) 1
Diabetes mellitus requiring insulin 1
Ischemic cardiac disease 1
Suprainguinal vascular surgery, intrathoracic surgery, or
intra-abdominal surgery
1
Total Score
Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a
simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999;
100:1043.
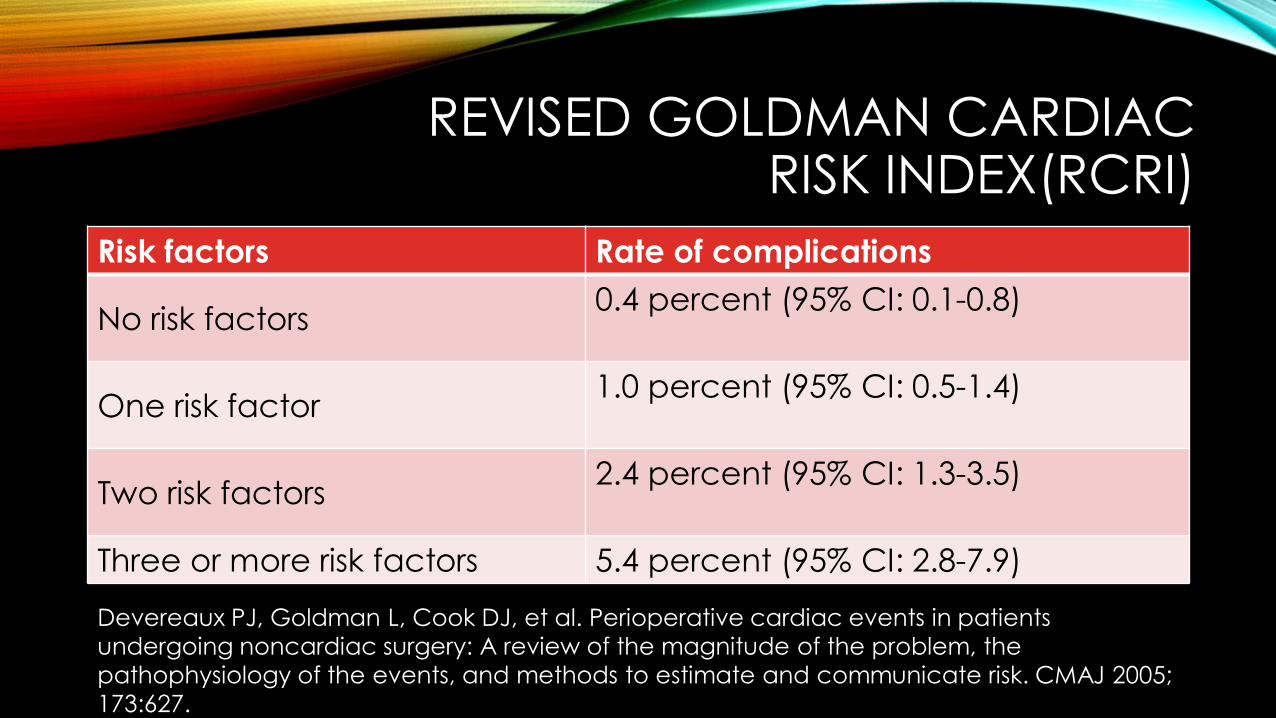
REVISED GOLDMAN CARDIAC RISK INDEX(RCRI)
Risk factors Rate of complications
No risk factors 0.4 percent (95% CI: 0.1-0.8)
One risk factor 1.0 percent (95% CI: 0.5-1.4)
Two risk factors 2.4 percent (95% CI: 1.3-3.5)
Three or more risk factors 5.4 percent (95% CI: 2.8-7.9)
Devereaux PJ, Goldman L, Cook DJ, et al. Perioperative cardiac events in patients
undergoing noncardiac surgery: A review of the magnitude of the problem, the
pathophysiology of the events, and methods to estimate and communicate risk. CMAJ 2005;
173:627.
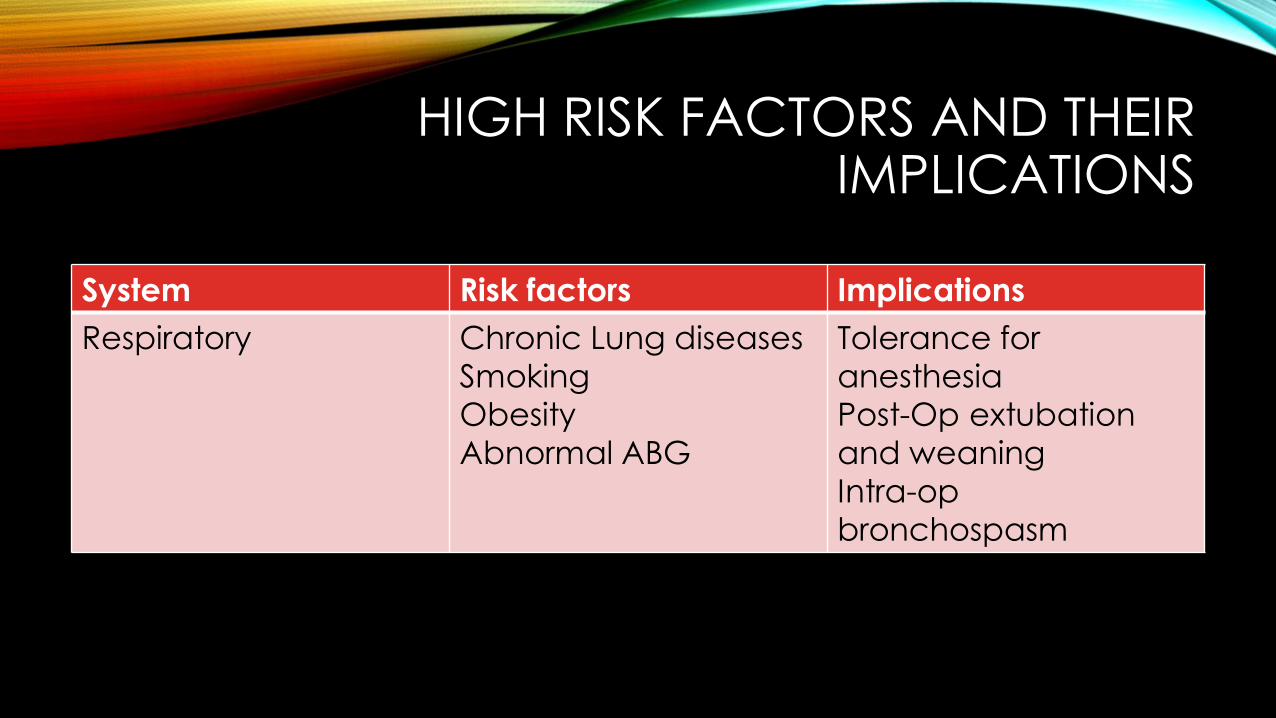
HIGH RISK FACTORS AND THEIR IMPLICATIONS
System Risk factors Implications
Respiratory Chronic Lung diseases
Smoking
Obesity
Abnormal ABG
Tolerance for
anesthesia
Post-Op extubation
and weaning
Intra-op
bronchospasm

HIGH RISK FACTORS AND THEIR IMPLICATIONS
System Risk factors Implications
Liver Hypoalbuminimia
Coagulopathy
Hemostasis
Wound healing
Nervous Neuro-muscular weakness
Previous CVA
Post-op extubation
and weaning
Perioperative vascular
events
Rheumatologic Active disease
On DMARDs
Medications –
interactions and
complications

HIGH RISK FACTORS AND THEIR IMPLICATIONS
System Risk factors Implications
Diabetes Requiring insulin
High HbA1C
Recent change in drugs
Complicated
Peri-operative
glycemic status
Peri-op vascular
events
Wound healing and
infections
Other endocrine Addison’s Disease
Uncontrolled hyperthyroidism
Hormone-related
crises

INVESTIGATIONS

PRE-OPERATIVE INVESTIGATIONS
Investigation Indication
ECG Signs or symptoms of CV disease
High risk surgery
Intermediate risk surgery with
cardiac risk factors
CXR Cardiopulmonary signs or
symptoms
Feely MA, Collins CS, Daniels PR, Kebede EB, Jatoi A, Mauck KF.
Preoperative testing before noncardiac surgery: guidelines and recommendations.
Am Fam Physician. 2013 Mar 15;87(6):414-8.
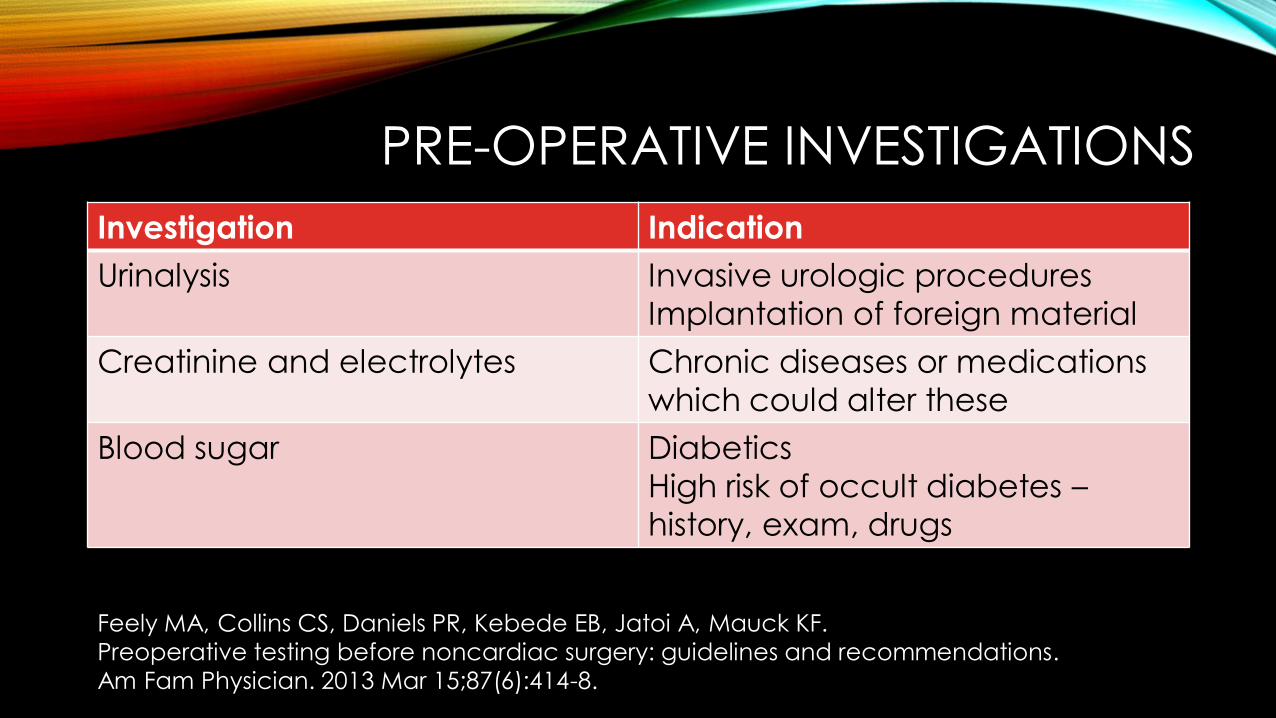
PRE-OPERATIVE INVESTIGATIONS
Investigation Indication
Urinalysis Invasive urologic procedures
Implantation of foreign material
Creatinine and electrolytes Chronic diseases or medications
which could alter these
Blood sugar Diabetics
High risk of occult diabetes –
history, exam, drugs
Feely MA, Collins CS, Daniels PR, Kebede EB, Jatoi A, Mauck KF.
Preoperative testing before noncardiac surgery: guidelines and recommendations.
Am Fam Physician. 2013 Mar 15;87(6):414-8.
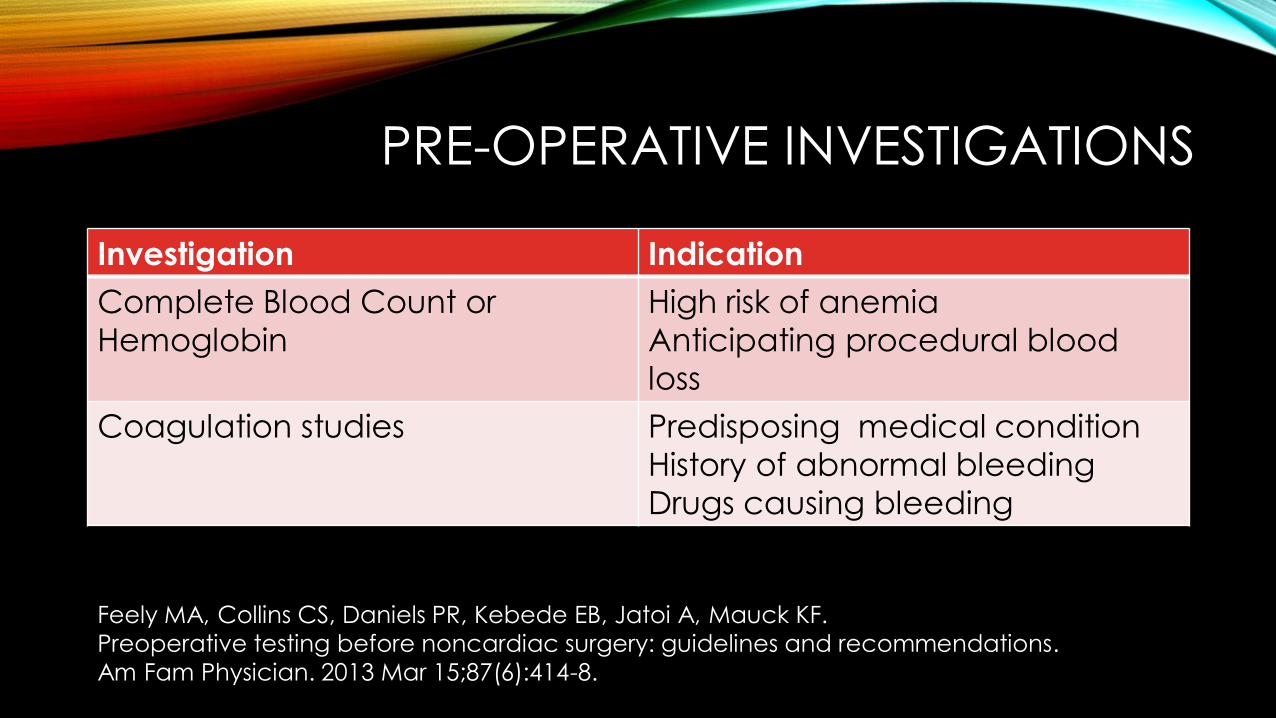
PRE-OPERATIVE INVESTIGATIONS
Investigation Indication
Complete Blood Count or
Hemoglobin
High risk of anemia
Anticipating procedural blood
loss
Coagulation studies Predisposing medical condition
History of abnormal bleeding
Drugs causing bleeding
Feely MA, Collins CS, Daniels PR, Kebede EB, Jatoi A, Mauck KF.
Preoperative testing before noncardiac surgery: guidelines and recommendations.
Am Fam Physician. 2013 Mar 15;87(6):414-8.

REVERSE RISK
Step 3
REVERSE RISK
• In reversible conditions
• Tailor drugs – eg. MDIs according to PFR, Beta blockade
• Delay (or abandon) procedure
• Plan interventions for risk mitigation – treatment of an ARI, CAG and revascularization, stop smoking

REDUCE COMPLICATIONS
Step 4

ANTICIPATE AND PREVENT
• Product support for CLD, hematological conditions, those on anti-platelets
• Avoiding tachycardia in those with angina, mitral stenosis
• Perioperative euglycemia

RE-ORGANIZE MEDICATIONS
Step 5

RE-ORGANIZE MEDICATIONS
• Which is to be stopped and when
• Which to be continued
• What precautions to be taken with regard to medications

APPROACH
THANK YOU

Copyright of this educational material rests with the author and
Christian Medical College, Vellore. Duplication, revision and
redistribution are not permitted. For any further clarification please
contact the concerned author
© reserved to author and Christian Medical College, Vellore