pre-operative evaluation · 2012. 8. 19. · pre-operative evaluation andrea meyer-lindenberg...
TRANSCRIPT
1
Pre-operativeevaluation
Andrea Meyer-LindenbergClinic of Small Animal Surgery and Reproduction
Ludwig-Maximilians-University Munich
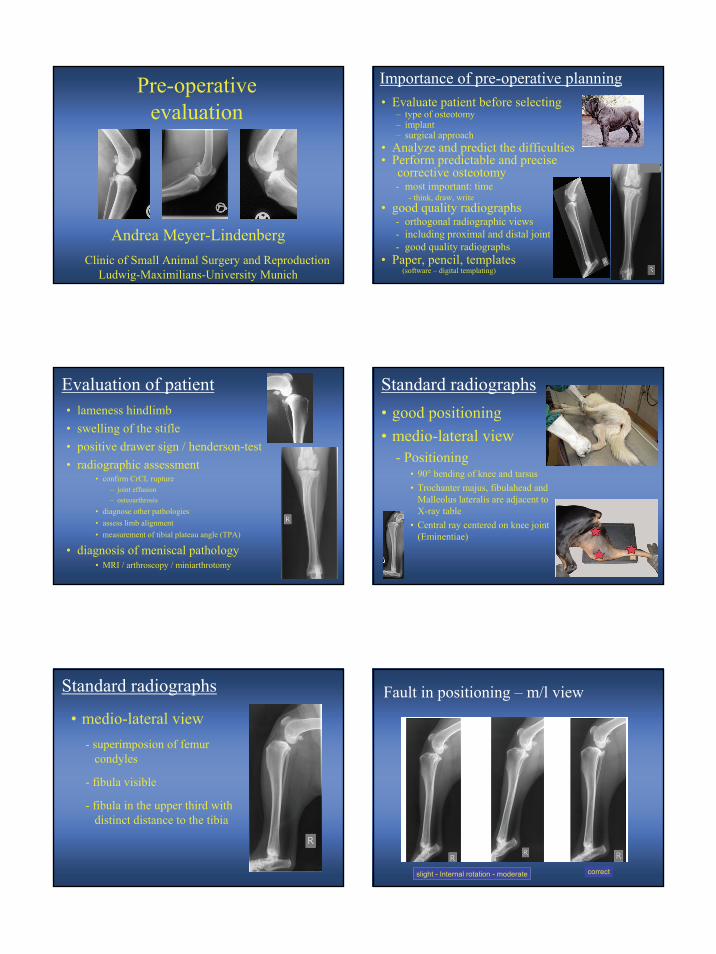
Importance of pre-operative planning• Evaluate patient before selecting
– type of osteotomy– implant– surgical approach
• Analyze and predict the difficulties• Perform predictable and precise
corrective osteotomy- most important: time
- think, draw, write• good quality radiographs
- orthogonal radiographic views- including proximal and distal joint- good quality radiographs
• Paper, pencil, templates(software – digital templating)
Evaluation of patient• lameness hindlimb• swelling of the stifle• positive drawer sign / henderson-test• radiographic assessment
• confirm CrCL rupture– joint effusion– osteoarthrosis
• diagnose other pathologies• assess limb alignment• measurement of tibial plateau angle (TPA)
• diagnosis of meniscal pathology• MRI / arthroscopy / miniarthrotomy
Standard radiographs• good positioning• medio-lateral view
- Positioning• 90° bending of knee and tarsus• Trochanter majus, fibulahead and
Malleolus lateralis are adjacent to X-ray table
• Central ray centered on knee joint(Eminentiae)
• medio-lateral view- superimposion of femur
condyles
- fibula visible
- fibula in the upper third withdistinct distance to the tibia
Standard radiographs Fault in positioning – m/l view
slight - Internal rotation - moderate correct
2
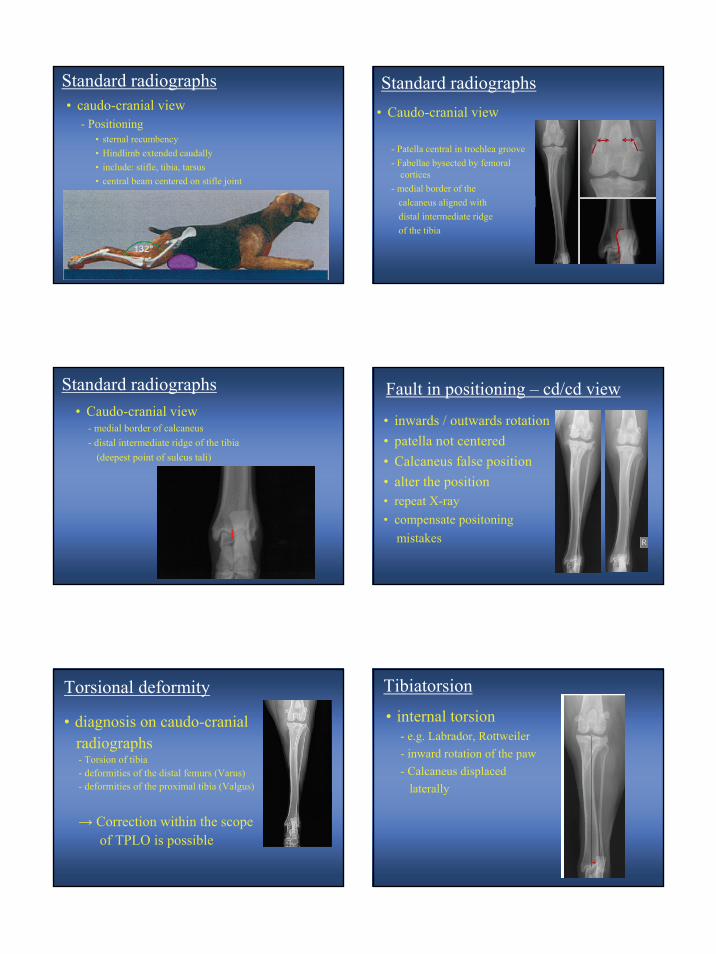
• caudo-cranial view- Positioning
• sternal recumbency• Hindlimb extended caudally• include: stifle, tibia, tarsus• central beam centered on stifle joint
Standard radiographs
• Caudo-cranial view
- Patella central in trochlea groove- Fabellae bysected by femoral
cortices- medial border of the
calcaneus aligned withdistal intermediate ridgeof the tibia
Standard radiographs
• Caudo-cranial view- medial border of calcaneus- distal intermediate ridge of the tibia
(deepest point of sulcus tali)
Standard radiographs
• inwards / outwards rotation • patella not centered• Calcaneus false position• alter the position• repeat X-ray• compensate positoning
mistakes
Fault in positioning – cd/cd view
Torsional deformity
• diagnosis on caudo-cranialradiographs- Torsion of tibia- deformities of the distal femurs (Varus)- deformities of the proximal tibia (Valgus)
→ Correction within the scopeof TPLO is possible
Tibiatorsion
• internal torsion- e.g. Labrador, Rottweiler- inward rotation of the paw- Calcaneus displaced
laterally
3
• external torsion- large breeds- outward rotation of the paw- calcaneus displaced
medially
R
Tibiatorsion
• Frontal plane• no deformity
Assessment of limb alignment
mMPTA: 94°medial proximal mechanicaltibia angle
mMDTA: 96°medial distal mechanicaltibia angle
Dismukes, Vet. Surg, 2008
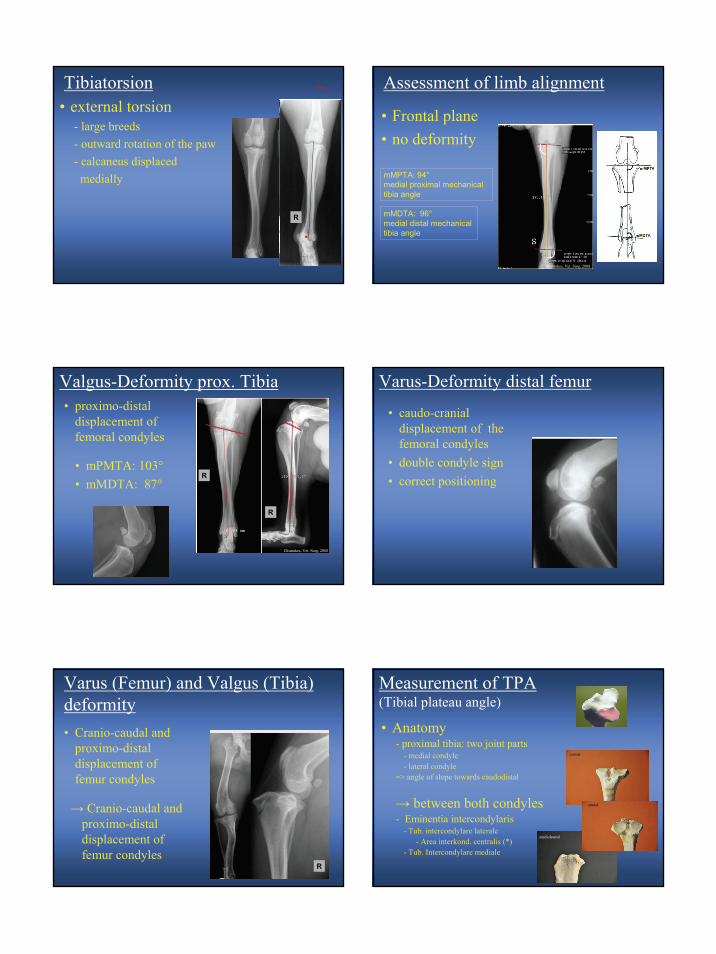
Valgus-Deformity prox. Tibia• proximo-distal
displacement of femoral condyles
• mPMTA: 103°• mMDTA: 87°
R
R
Dismukes, Vet. Surg, 2008
• caudo-cranialdisplacement of thefemoral condyles
• double condyle sign• correct positioning
Varus-Deformity distal femur
Varus (Femur) and Valgus (Tibia) deformity• Cranio-caudal and
proximo-distaldisplacement of femur condyles
R
→ Cranio-caudal and proximo-distaldisplacement of femur condyles
Measurement of TPA(Tibial plateau angle)
• Anatomy- proximal tibia: two joint parts
- medial condyle- lateral condyle
=> angle of slope towards caudodistal
→ between both condyles- Eminentia intercondylaris
- Tub. intercondylare laterale- Area interkond. centralis (*)
- Tub. Intercondylare mediale
*
cranial
mediolateral
caudal
4
Measurement of TPA(Tibial plateau angle)
• Anatomy (important points)- cranial margin
- Tub. Tibiae
- Margin of joint surface- cranial / caudal edge of
med. tibial condyle→ Tibia plateau line
- Midpoint between medial and lateral intercondylartubercles
mediolateral Measurment of TPA (Tibial plateau angle)
• 1. mechanical axisof the tibia
– midpoint between the two(medial and lateral)intercondylar tubercles
– Centre of Os tali
• 2. identifying tibia plateau- Standard method
- tibial plateau line- joining cranial and caudaledges of the medial tibialcondyle
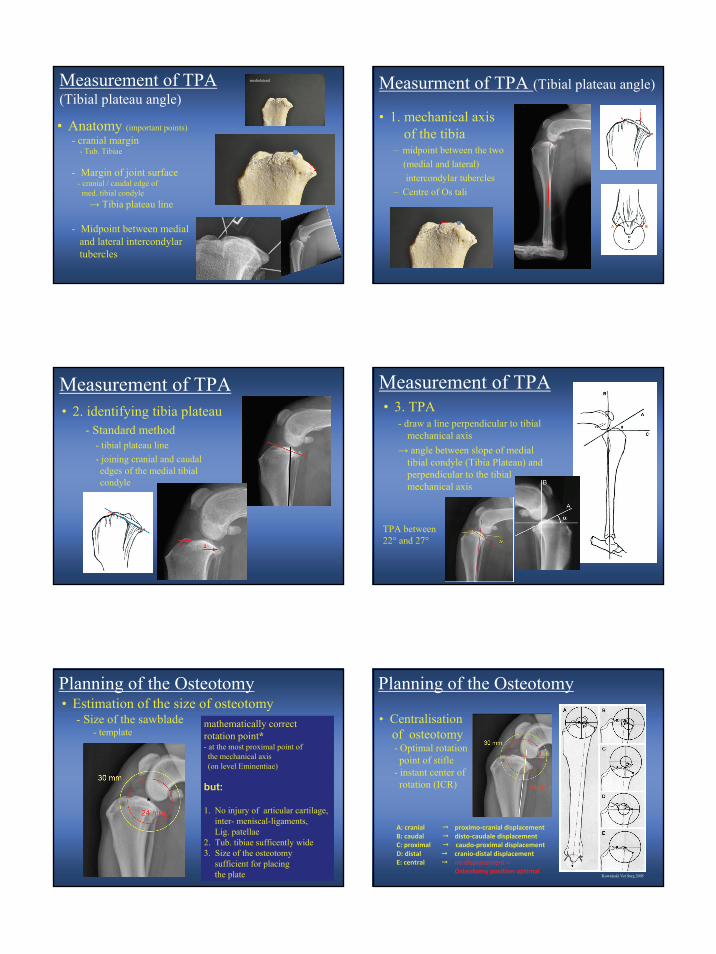
Measurement of TPA• 3. TPA
- draw a line perpendicular to tibialmechanical axis
→ angle between slope of medial tibial condyle (Tibia Plateau) and perpendicular to the tibialmechanical axis
Measurement of TPA
TPA between22° and 27°
Planning of the Osteotomy• Estimation of the size of osteotomy
- Size of the sawblade- template
mathematically correctrotation point*- at the most proximal point of the mechanical axis(on level Eminentiae)
but:
1. No injury of articular cartilage, inter- meniscal-ligaments, Lig. patellae
2. Tub. tibiae sufficently wide3. Size of the osteotomy
sufficient for placingthe plate
*
• Centralisationof osteotomy- Optimal rotation point of stifle
- instant center of rotation (ICR)
Planning of the Osteotomy
A: cranial proximo‐cranial displacementB: caudal disto‐caudale displacementC: proximal caudo‐proximal displacementD: distal cranio‐distal displacementE: central no displacement =
Osteotomy position optimalKowaleski Vet Surg 2005
5
• Size and shape of thetuberositas tibiae
• distance from onset of Lig. patellae to osteotomy (D2)
- trapezoid- width increasing from
proximal to distal
• D2 - 1 cm at least
D2
Planning of the Osteotomy• Mistakes
- „reversed trapezoid“- tibial tuberosity too narrow
Osteotomy too far distal
=> danger of fracture=> femoral-tibial-impingment
*
Planning of the Osteotomy
• Size of the proximalfragment- enough place for plating
• 30 mm sawblade
Planning of the Osteotomy
• Size of osteotomy- not damage any structures→ CENTER THE OSTEOTOMY
- preserve tibial tuberosity width→ CHECK THE TUBEROSITY THICKNESS
AND SHAPE
- leave room for plate application→ CHECK THE SIZE OF THE PROXIMAL
FRAGMENT
Planning of the Osteotomy - Checklist
Estimation of the Rotation• Estimation of the TPA √• Estimation of the sawblade size √
↓
Schedule table↓
mm Rotation Post OP-TPA of 6°
• measure distance of theplanned osteotomy froma reference point
• origin of the Lig. patellae
• to osteotomy cut
Planning of the Osteotomy• Next steps:
(transfer correct osteotomy from x-ray to surgery)
6
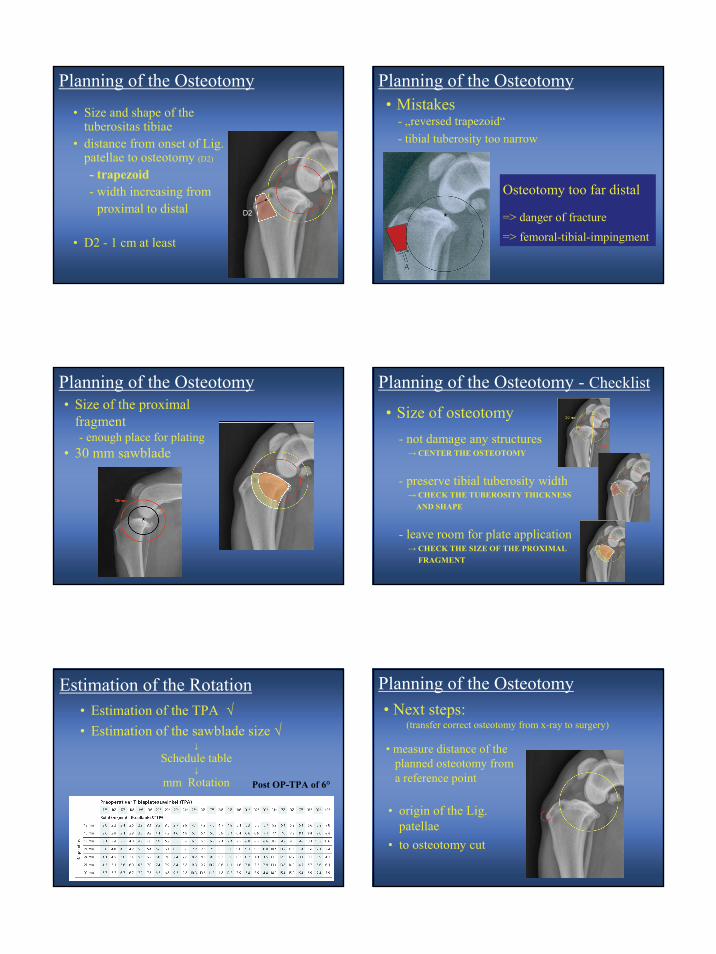
• Using 2 marks• Marking of the osteotomy points
Measurement „D1“:Distance from origin of theLig. patellae to the most proximalpoint of the osteotomy
Measurement „D2“:Distance from origin of theLig. patellae to the osteotomy point on line perpendicularly to tibialtuberosity
Planning of the Osteotomy
Measurement D3:From caudal tibial plateau to the most caudal aspect of theosteotomy- needle marks caudal border(joint cavity) of medial collateralligament
• Marking of the Osteotomy Points
Planning of the Osteotomy
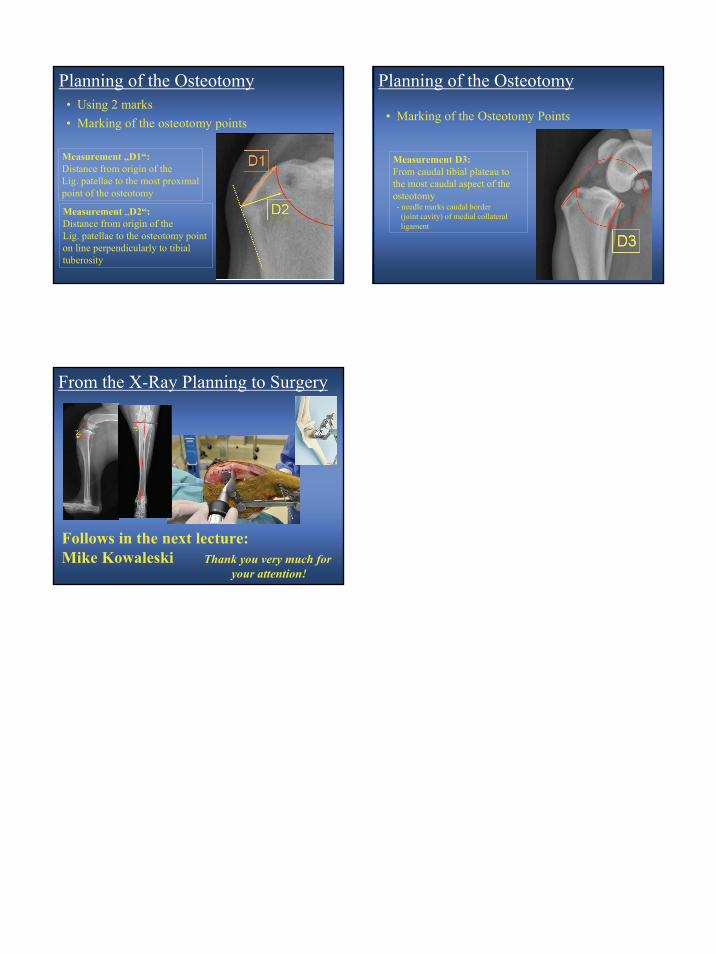
From the X-Ray Planning to Surgery
Follows in the next lecture: Mike Kowaleski Thank you very much for
your attention!