pre-employment health packet · pre-employment health packet. ... official employee health use only...
TRANSCRIPT
BHSF 6321 Rev. 11/4/16
PRE-EMPLOYMENTHEALTH PACKET

BHSF #6155 Rev. 1/13
PRE-EMPLOYMENT INFORMATION SHEET
PR
INTE
D B
Y B
AP
TIS
T P
RIN
T S
HO
P 7
86-5
96-6
286
SOCIAL SECURITY #: _____ - _____ - ________ Date of Birth: _____ / _____ / 19_______ Employee ID#: ____________
NAME: ______________________________________________________________________________________________ (Last) (First) (Middle)
ADDRESS: ___________________________________________________________________________________________ (Street or Mailing) (City / ST) (Zip Code)
Home Phone: (_____) _____ - _________ Cell: (_____) _____ - _________ Email: _______________________________
Date of Hire #: ______ - ______ - ________ Job Title: ________________________ Department: __________________
ALLERGIES: __________________________________________________________ LATEX allergy : G Yes G No
Current MEDs: ________________________________________________________________________________________
Drug Screen Date: _________________ G Neg G Pos
DATE of Physical: _______ / ________ / ____________
Location: Please G (1) BoxG Baptist G South MIami G Doctors G Homestead G West Kendall G Mariners G BOS / BHE G Corporate
P
DO NOT WRITE BELOW THIS SECTION - OFFICIAL EMPLOYEE HEALTH USE ONLY
Examiner Signature:_____________________________________________
QUANTIFERON DATE / / q Neg q Pos
1

2BHSF #6148 Rev. 2/22/16
EMPLOYEE HEALTH SERVICES
VITALS AND VISION SHEET
Name: ________________________________________________________________________ Date: ________________
DOB: ___________________ G Male G Female Height: _______’ _______” Weight: __________ lbs
DO NOT WRITE BELOW THIS SECTION - FOR EMPLOYEE HEALTH OFFICE USE ONLY
BP: _______________________ Pulse: _____________________ Temperature: _________________
Date: _____________________ Recheck BP: _______________ Pulse: ______________________
Vision: Right Eye: ________ / ________ Left Eye: ________ / ________ Both Eyes: ________ / ________
With Contacts: ______________________________ With Glasses: ______________________________
COLOR BLIND TESTING - Ishihara Test Edition Date: ____________ PLATE No. NUMBER READ RESULTS / comments
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
Examining Practitioner: _______________________________________________ G PASS G FAIL

3
HEALTH HISTORY & SCREENING - STATEMENT
Name: __________________________________________________ Date: ___________________________________
DOB: __________________________________________ Last 4 Digits of Social Security #: XXX - XX - ___________
WELCOME TO BAPTIST HEALTH.
Employee Health Services is here to provide health care for you. We are available for consultation, medical referrals, care and treatment.
•Pleasetakeyourtimeandcarefullyreadthefollowinghealthhistoryform.
•Answerallquestions.Weareavailabletoassistyouifnecessary.
Please initial at the end of each statement: 1) Youranswerstothefollowingquestionsaretoassistinplacingyouinajobsafetoyouand
to others. _______ (Initials)
2) Iunderstandsuchinformationpertinenttomyjobdescriptionmaybemadeavailabletomy
supervisor. ________ (Initials)
3) I authorize Employee Health Services to perform any physical and/or laboratory examination,
whichisnecessarytoverifytheabsenceofcommunicablediseaseoranycondition,which
might impair the performance of my duties as an employee of BAPTIST HEALTH.
________ (Initials)
4) I understand that any offer of employment is contingent upon satisfactorily completing the
health assessment. _______ (Initials)
5) IherebyaffirmthattheinformationprovidedinthisHealthHistory&Screeningistrueand
correct. _____ (Initials)
Examiner Initials: _____________
PR
INTE
D B
Y B
AP
TIS
T P
RIN
T S
HO
P
Page 1 of 6 • BHSF #6151 Rev. 2/22/16

4
HEALTH HISTORY & SCREENINGName: __________________________________________________ Date: ___________________________________
DOB: __________________________________________ Last 4 Digits of Social Security #: XXX - XX - ___________
HISTORY1. Haveyoueverhadabackconditionorinjury?G No G YES Year: ___________________________________________
Listconditionorinjury: ________________________________________________________________________________________
Describe incidents: __________________________________________________________________________________________
__________________________________________________________________________________________________________
Didyouconsultwithaphysicianregardingyourbackproblem?G No G YES
Physician’s name: ____________________________________________ Specialty: ___________________________________
Describe type of treatment: ____________________________________________________________________________________
DidyouhaveanyX-RAY,MRI,and/orCT? _______________________________________________________________________
Previousbacksurgery? _______________________________________________________________________________________
2. Haveyoueverhadaneckconditionorinjury?G No G YES Year: ___________________________________________
Listconditionorinjury: ________________________________________________________________________________________
Describe incidents: __________________________________________________________________________________________
__________________________________________________________________________________________________________
Didyouconsultwithaphysicianregardingyourneckproblem?G No G YES Year: ______________________________
Physician’s name: ____________________________________________ Specialty: ___________________________________
Describe type of treatment: ____________________________________________________________________________________
DidyouhaveanyX-RAY,MRI,and/orCT? _______________________________________________________________________
Previousnecksurgery? _______________________________________________________________________________________
3. Doyoustillsuffereffectsfromtheback/neckproblemdescribedabove?G No G YES
4. If so, check symptoms and severity (1 - 10) you continue to experience at time : 1 = MILD - 10 = SEVERE
G _____ Weakness G _____ Tingling G _____ Dizziness G _____ Numbness
G _____ Headache G _____ Soreness after lifting G_____Painwithlifting G_____PainwithCoughing
G_____Tirednessafterwork
5. Doyoutakeanymedicationsforyourback/neckcondition?G No G YES
List of Medications: ___________________________________________ Howoftentaken: ______________________________
6. DoyouhavetroubleperformingtheActivitiesofDailyLiving?G No G YES
Describe limitations: _________________________________________________________________________________________
7. Haveyoueverbeenunabletoworkbecauseofconditionorinjury?G No G YES
Examiner Comment: _____________________________________________________________________________________________
Examiner Initials: ________________ Employee/Applicant Initials: ________________
Page 2 of 6 • BHSF #6151 Rev. 2/22/16

5
HEALTH HISTORY & SCREENING (CONTINUED)
Yes NoDO YOU HAVE OR HAD THE
FOLLOWING:RESPIRATORY CONDITION(S):
Applicant’s Comment Examiner’s Comment
1. Asthma
2. Emphysema
3. Bronchitis
4. Smoker?/HowLong?
5. Tuberculosis
6. Other
CARDAC CONDITION(S):
1. High Blood Pressure
2. Heart Condition
3. Congestive Heart Failure (CHF)
4. Open Heart Surgery
5. Heart Attack
6. Chest Pain
7. Other
NEURO/MUSCULAR, SKELETAL & JOINT CONDITION(S)
1. Hand/WristInjury;CarpalTunnel
2. Shoulder/ElbowInjury
3. Back Sprain
4. Back-Herniated Intervertebral Disc
5. Back-Surgical Procedure
6. Broken Bones
7. KneeInjury
8. AnkleInjury
9. Leginjury
10. Hip Disorder
11. Foot Problem
12. Amputation of Foot/Leg/Arm/Hand
13. Neckinjuryorpain
14. Orthopedic surgery
15. Poliomyelitis – Residual Disability
16. Arthritis/ Gout
17. Chronic Osteoarthritis
18. Other
COMMENTS: Please include any testing (x-ray, CT, MRI, etc.), Physician name and address, tel. # and fax #
______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
Examiner Initials: ________________ Employee/Applicant Initials: ________________
Name: ________________________________________________
Page 3 of 6 • BHSF #6151 Rev. 2/22/16

6
HEALTH HISTORY & SCREENING (CONTINUED)
Yes NoDO YOU HAVE OR HAD THE
FOLLOWING:ABDOMINAL CONDITION(S):
Applicant’s Comment Examiner’s Comment
1. Stomach and/or Intestinal disorder
2. IrritableBowelSyndrome
3. Colitis
4. Crohns
5. Gall Bladder
6. Ulcer
7. Kidney Disease
8. Hernia
9. Hepatitis
10. Liver Disease
11. Other
MEDICAL CONDITION(S):
1. Diabetes
2. Epilepsy / Seizure Disorder
3. Headaches / Migraines
4. HeadInjury
5. Vascular Disorder
6. Stroke (CVA)
7. Thrombophlebitis (Blood clot)
8. Anemia
9. Circulatory problems
10. Bleeding disorder
11. Cancer
12. Immunosuppressive condition
OTHER:
1. Deafness–total or partial hearing loss
2. Ear Condition
3. Eye Condition
4. Total or partial loss of sight
5. ColorBlind(ColorDeficiency)
PAST HISTORY:
1.
Are you currently or have you ever been under the supervision of IPN, PRN, or theDepartmentofHealth?Ifyes,pleaseexplain circumstances, including dates.
WOMEN ONLY:
1.Areyoupregnant?IfYES;Estimated date due: ______________
Name: ________________________________________________
Examiner Initials: ________________ Employee/Applicant Initials: ________________
Page 4 of 6 • BHSF #6151 Rev. 2/22/16

7
HEALTH HISTORY & SCREENING (CONTINUED)
Name: ________________________________________________
LIST ALL: Examiner Comments
Surgical Procedures: ____________________________________________________ _____________________________________
__________________________________________________________________ _____________________________________
Car Accident: _________________________________________________________ _____________________________________
__________________________________________________________________ _____________________________________
Other Accidents: ______________________________________________________ _____________________________________
__________________________________________________________________ _____________________________________
AnyotherIllnessorConditionnotlisted? ____________________________________________________________________________
Please Note: Baptist Health South Florida requires copies of any workman’s compensation/auto and any other accident claim, medical records and work releases.
HaveyoueverhadanyWorkers’Compensationinjuries/orclaims? G No G YES (describebelow)
Date Injury Company State
DidyoufilealawsuitagainstyouremployerinanyWorkers’Compensationcase? G No G YES
Willanyconditionlimityouinanywayintheperformanceofyourspecificjobdescription? G No G YES
EXPLAIN
______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
Examiner Initials: ________________ Employee/Applicant Initials: ________________
Please Note: The information you provide herein will be independently verified through our background check process. If you omit information or provide misleading or incorrect information you may be subject to corrective action, including the revocation of this job offer or termination.
Page 5 of 6 • BHSF #6151 Rev. 2/22/16

8
HEALTH HISTORY & SCREENING (CONTINUED)
ADA ACCOMMODATIONS:
1) Ihavereceived,read,andunderstandmyjobdescriptionaswellastheessentialfunctionsofthejob;IfeelIcan perform these functions. G No G YES
2) Willanypersonalphysical/emotionalconditionlimityouinanywayintheperformanceofyourspecificjob description? G No G YES (describebelow)
____________________________________________________________________________________________
____________________________________________________________________________________________
3)Haveyoueverbeenunabletoworkbecauseofanillness,injury,orcondition? G NO G YES(describebelow)
____________________________________________________________________________________________
____________________________________________________________________________________________
4)Doyouneedspecialaccommodation(s)toperformtheessentialfunctionsofthisjob? G NO G YES
COMMENTS: _______________________________________________________________________________________________
______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
GMandatoryInfluenzaReviewed HealthProviderInitials:_________
I CERTIFY THAT THIS HEALTH HISTORY IS TRUE AND COMPLETE AND THAT I DO NOT HAVE ANY ILLNESS, INJURY OR CHRONIC DISEASE OTHER THAN STATED WITHIN THIS DOCUMENT. I ACKNOWLEDGE THAT THE EXAMINER HAS REVIEWED THIS FORM WITH ME. I UNDERSTAND THAT FALSIFICATION OF AND/OR FAILURE TO PROVIDE ANY INFORMATION IS GROUNDS FOR IMMEDIATE DISMISSAL OR COULD RESULT IN DENIAL OF WORKERS COMPENSATION BENEFITS. I ALSO UNDERSTAND THAT THE JOB OFFER IS CONTINGENT UPON SUCCESSFUL COMPLETION OF AND VERIFICATION OF DATA PROVIDED IN THE POST OFFER SCREENING. I AUTHORIZE MEDICAL INFORMATION OBTAINED DURING MY SCREENING MAY BE DISCLOSED ONLY TO THE EXTENT NECESSARY, TO DETERMINE MY ABILITY TO PERFORM ESSENTIAL FUNCTIONS OF MY INTENDED POSITION. I UNDERSTAND THAT THIS SCREENING IS COMPLETED TO DETERMINE MY ABILITY TO PERFORM ESSENTIAL FUNCTIONS OF MY INTENDED POSITION AND DOES NOT CONSTITUTE A COMPLETE AND COMPREHENSIVE MEDICAL EXAMINATION. IT IS NOT INTENDED FOR USE TO DETERMINE THE STATUS OF MY OVERALL PERSONAL HEALTH.
Signature: _______________________________________________________________________ Date: _____________________
Examiner Print Name: _____________________________________________________________ Date: _____________________
Examiner Signature: _______________________________________________________________ Time: ____________________
Examiner Initials: ________________ Employee/Applicant Initials: ________________
Name: ________________________________________________
Page 6 of 6 • BHSF #6151 Rev. 2/22/16

Page 1 of 2 Form # 6109 Rev. 12/12
EMPLOYEE HEALTH SERVICESCONSENT to DRUG & ALCOHOL SCREENING
ANDRELEASE of BAPTIST HEALTH SOUTH FLORIDA
Print Name: ___________________________________ EMPLOYEE ID #:_____________ D.O.B.:____________
Statement of Policy
BaptistHealthSouthFloridaiscommittedtocreatingandmaintainingaworkplacefreeofsubstanceabuse.To that end, Baptist Health has developed a policy regarding the illegal use of drugs and the abuse of alcoholorprescriptiondrugsthatwebelievebestservestheinterestsofallemployees.Theillegaluseofdrugsorabuseofalcoholorprescriptiondrugswillnotbetolerated.ItisaviolationoftheBaptistHealthSouth Florida Drug-Free Workplace Policy for any applicant or employee to: 1) use, possess, sell, trade, offerforsale,oroffertobuyillegaldrugsorotherwiseengageintheillegaluseofdrugsonthejob;2)toreport toworkunder the influenceof illegaldrugsoralcohol; and3) touseprescriptiondrugs illegally.However,nothinginthispolicyprecludestheappropriateuseoflegallyprescribedmedications.EmployeesareadvisedthatthefollowingareunacceptableexplanationsforapositiveconfirmedtestresultandwillberejectedbytheMRO:1)expiredprescriptions(i.e.prescriptionswhichareolderthanone(1)yearfromthedate of the prescription and are unaccompanied by documentation from prescribing physician indicating continuedsuperviseduse);2)prescriptionswhicharewrittenforanyoneotherthantheemployee;3)over-thecounterherbalsupplementscontainingundisclosedcontrolledsubstancesforwhichtheemployeedoesnothaveavalidprescription;or4)over-the-countercontrolledsubstancespurchasedinaforeigncountry.
NOTE: EMPLOYEES ARE RESPONSBLE FOR ASKING THEIR DISPENSING PHARMACISTS ABOUT THE PHYSICAL AND MENTAL EFFECTS OF ANY MEDICATIONS, INCLUDING SIDE EFFECTS.
Conditions of Employment
AlljobapplicantsandemployeesmustexecutethisconsentandreleaseandmustcomplywiththetestingproceduresofBaptistHealthSouthFloridabeforetheywillbeconsideredforemployment.Applicantswhorefuse to execute this consentwill not be considered for employment byBaptistHealthSouthFlorida.Employeeswhorefusetoexecutethisconsentmaybesubjecttotermination.Noguaranteeismadethatanapplicantwhopassesthetestswillbehired.Applicantsoremployeeswhotestpositivefordrugsoralcoholmaybedeniedemploymentorsubjecttodisciplinaryaction,uptoandincludingtermination.
Confidentiality
All information, interviews, reports,statements,memoranda,anddrug test results,writtenorotherwise,receivedorproducedasaresultofBaptistHealthSouthFlorida’sdrug-testingprogramareconfidentialandwillbemaintainedintheemployee’sEmployeeHealthServicesfile.BaptistHealthSouthFloridawillnotreleaseanyinformationconcerningdrugtestresultswithoutawrittenconsentformsignedvoluntarilybythepersontested,unlesssuchreleaseiscompelledbyanadministrativelawjudge,ahearingofficer,oracourtofcompetentjurisdictionpursuanttoanappealtakenunderDrug-FreeWorkplaceAct(F.S.§440.102)orisdeemed appropriate by a professional or occupational licensing board in a related disciplinary proceeding.
9

Consent For Release of Drug & Alcohol Screening Results For Licensed Healthcare Practitioners
Iunderstandandacknowledgethat,ifIamaLicensedHealthcarePractitioners,(anypersonlicensedunderchapter457;chapter458;chapter459;chapter460;chapter461;chapter462;chapter463;chapter464;chapter465;chapter466;chapter467;partI,partII,partIII,partV,partX,partXIII,orpartXIVofchapter468;chapter478;chapter480;partIIIorpartIVofchapter483;chapter484;chapter486;chapter490;or chapter 491, Florida Statutes), I shall execute, prior to drug testing, a Consent For Release of Drug &AlcoholScreeningResults.ThepurposeofthisdisclosureissothatBaptistHealthSouthFloridaandImayfulfillourlegalandethicalobligationspursuanttoFloridaStatutesChapters456and464toreportlicenseeswhoareinviolationoftheseacts.ThisConsentforReleaseofDrug&AlcoholScreeningResultsauthorizesBaptistHealthSouthFloridatoreleasetheresultsofdrug&alcoholtestingonlytothefollowingagencies:1)theFloridaDepartmentofHealth;2)theInterventionProjectforNurses(“IPN”);and/or3)theProfessionalsResourceNetwork(“PRN”);or4)asmayberequiredpursuanttoFloridaStatutes§440.102.Thisconsentwillbe ineffect from thedateofexecutionof theConsent forReleaseofDrug&AlcoholScreeningResultsuntilthelatterofthefollowing:1)thesuccessfulcompletionofanIPNorPRNprogram;or 2) the conclusion of any investigation related hereto by the Florida Department of Health.
Consent to Submit to Test
I hereby consent to submit to the testing for drugs and/or alcohol as shall be determined by Baptist Health South Florida, for the purpose of determining the drug and/or alcohol content thereof.
IagreethatBaptistHealthSouthFloridamaycollectthespecimensforthesetestsandmayforwardthemtoalicensedorcertifiedlaboratorydesignatedbyBaptistHealthSouthFloridaforanalysis.Ifurtheragreeto and hereby authorize the release of said test results to Baptist Health South Florida.
I understand that my current use of drugs and alcohol in violation of Baptist Health South Florida’s Drug-Free Workplace Policy may prohibit me from being employed at Baptist Health South Florida, or may subjectmetodisciplinaryaction,uptoandincludingterminationofemployment.
I further agree that a reproduced copy of this pre-employment consent and release form shall have the same force and effect as the original.
I releaseBaptistHealthSouthFloridaandits trustees,officers,employeesandagentsfromanyandallclaims,liabilitiesandcausesofactionofanynaturewhatsoeverinconnectionwitha)thisconsent,b)theperformingofdrugandalcoholtestinconnectiontherewithandc)mynotbeingemployedbyBaptistHealthSouthFloridaif,inthesoleopinionofBaptistHealthSouthFlorida,IfailtomeetanyoftherequirementsestablishedbyBaptistHealthSouthFloridainconnectionwithsuchtests.
Ihavecarefullyreadtheforegoingandfullyunderstanditscontents.Iacknowledgethatmysigningofthisconsent and release form is a voluntary act on my part.
Dated this ____________ day of ___________________ 20____.
Signature of Applicant/Employee Print Name of Applicant/Employee
Name and Title of Witness (PRINT CLEARLY) Signature of Witness
Page 2 of 2 Form # 6109 Rev. 12/1210
BHSF #6149 Rev. 12/12
PR
INTE
D B
Y B
AP
TIS
T P
RIN
T S
HO
P 7
86-5
96-6
286
NAME:__________________________________ Last4digitsofSS#:_______________________
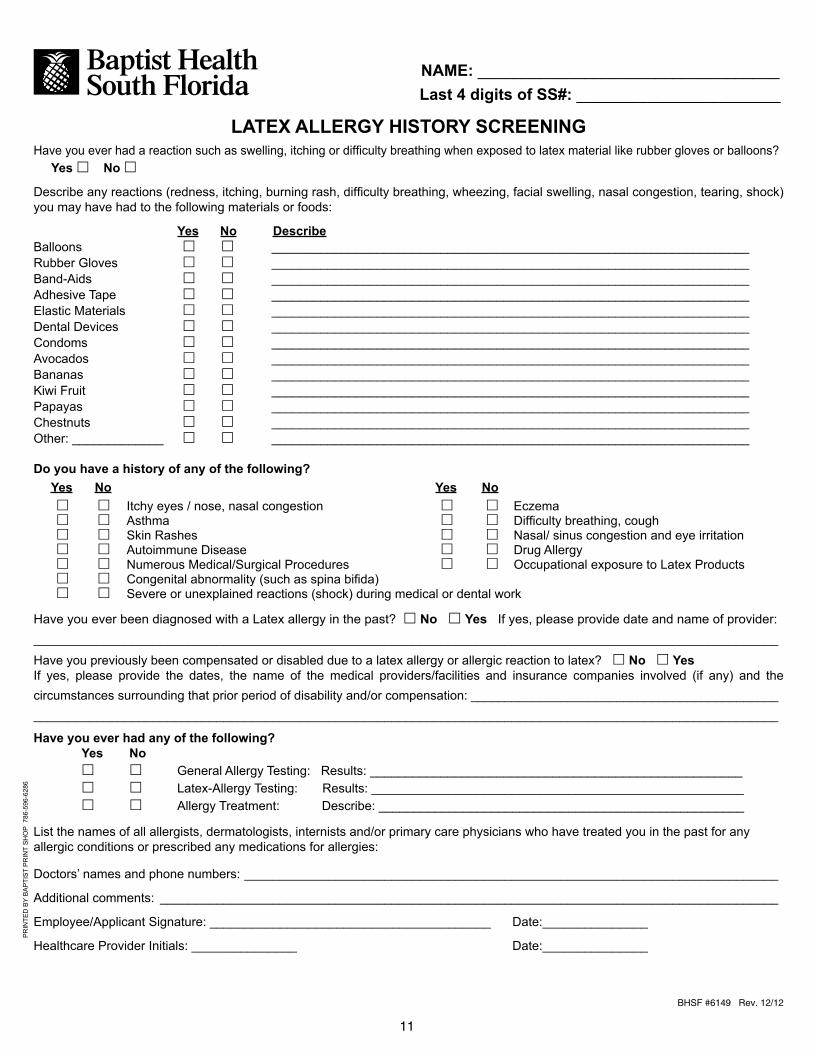
LATEXALLERGYHISTORYSCREENINGHave you ever had a reaction such as swelling, itching or difficulty breathing when exposed to latex material like rubber gloves or balloons? Yes £ No £
Describe any reactions (redness, itching, burning rash, difficulty breathing, wheezing, facial swelling, nasal congestion, tearing, shock) you may have had to the following materials or foods:
YesNo DescribeBalloons £ £ ____________________________________________________________________Rubber Gloves £ £ ____________________________________________________________________Band-Aids £ £ ____________________________________________________________________Adhesive Tape £ £ ____________________________________________________________________Elastic Materials £ £ ____________________________________________________________________Dental Devices £ £ ____________________________________________________________________Condoms £ £ ____________________________________________________________________Avocados £ £ ____________________________________________________________________Bananas £ £ ____________________________________________________________________Kiwi Fruit £ £ ____________________________________________________________________Papayas £ £ ____________________________________________________________________Chestnuts £ £ ____________________________________________________________________Other: _____________ £ £ ____________________________________________________________________
Doyouhaveahistoryofanyofthefollowing? Yes No Yes No £ £ Itchy eyes / nose, nasal congestion £ £ Eczema £ £ Asthma £ £ Difficulty breathing, cough £ £ Skin Rashes £ £ Nasal/ sinus congestion and eye irritation £ £ Autoimmune Disease £ £ Drug Allergy £ £ Numerous Medical/Surgical Procedures £ £ Occupational exposure to Latex Products £ £ Congenital abnormality (such as spina bifida) £ £ Severe or unexplained reactions (shock) during medical or dental work
Have you ever been diagnosed with a Latex allergy in the past? £ No £ Yes If yes, please provide date and name of provider:__________________________________________________________________________________________________________
Have you previously been compensated or disabled due to a latex allergy or allergic reaction to latex? £ No £ Yes If yes, please provide the dates, the name of the medical providers/facilities and insurance companies involved (if any) and the circumstances surrounding that prior period of disability and/or compensation: ______________________________________________________________________________________________________________________________________________________
Haveyoueverhadanyofthefollowing? Yes No £ £ General Allergy Testing: Results: _____________________________________________________ £ £ Latex-Allergy Testing: Results: _____________________________________________________ £ £ Allergy Treatment: Describe: ____________________________________________________
List the names of all allergists, dermatologists, internists and/or primary care physicians who have treated you in the past for any allergic conditions or prescribed any medications for allergies: Doctors’ names and phone numbers: ____________________________________________________________________________
Additional comments: ________________________________________________________________________________________
Employee/Applicant Signature: ________________________________________ Date:_______________
Healthcare Provider Initials: _______________ Date:_______________
11

12
Employee Health Services
MEDICAL QUESTIONNAIRE FORRESPIRATOR USERS
PART A. Section 2. (Mandatory) Questions 1 through 9 below must be answered by the employee who has been selected to use any type of respirator (please check “Yes” or “No”).
1. Do you currently smoke tobacco, or have you smoked tobacco in the last month: G Yes G No
2. Haveyoueverhadanyofthefollowingconditions?
a. Seizures(fits): G Yes G No
b. Diabetes (sugar disease): G Yes G No
c. Allergicreactionsthatinterferewithyourbreathing: G Yes G No
d. Claustrophobia (fear or closed in places) G Yes G No
e. Trouble smelling odors: G Yes G No
3. Haveyoueverhadanyofthefollowingpulmonaryorlungproblems?
a. Asbestosis: G Yes G No
b. Asthma: G Yes G No
c. Chronic bronchitis: G Yes G No
d. Emphysema: G Yes G No
e. Pneumonia: G Yes G No
f. Tuberculosis: G Yes G No
g. Silicosis: G Yes G No
h. Pneumothorax (collapsed lung): G Yes G No
i. Lung cancer: G Yes G No
j. Brokenribs: G Yes G No
k. Anychestinjuriesorsurgeries: G Yes G No
l. Any other lung problem that you’ve been told about: G Yes G No
Page1of2•BHSF6126Rev.1/25/16
Today’s Date: ___________________
Name: _______________________________________________________________________ Emp. ID#: ______________________
Job Title: __________________________________________________________ Last 4 digits of Emp. SS#: ______________________
Sex (Check one): G Male / G Female D.O.B.: ________________________ Height: ______ ft. ______ in. Weight: ____________ lbs
T Aphonenumber(includingareacode)whereyoucanbereachedbythehealthcareprofessionalwhoreviewsthisquestionnaire:
______________________________________________________________________________________________________
T What is the best time to phone you at this number: _____________________________________________________________
Hasyouremployertoldyouhowtocontactthehealthcareprofessionalwhowillreviewthisquestionnaire
(pleasecheck“Yes”or“No”)? G Yes G No
1. Checkthetypeofrespiratoryouwilluse(youmayselectmorethanonecategory): a. GN.R.orPdisposablerespirator(e.g.filter-mask,non-cartridgetypeonly) b. GOthertype(e.g.half-orfull-facepiecetype,powered-airpurifying,supplied-air,self-containedbreathingapparatus)
2. Haveyouwornarespirator(pleasecheck“Yes”or“No”)? G Yes G No
If“Yes”whattype(s): _________________________________________________________________________________________
___________________________________________________________________________________________________________
13
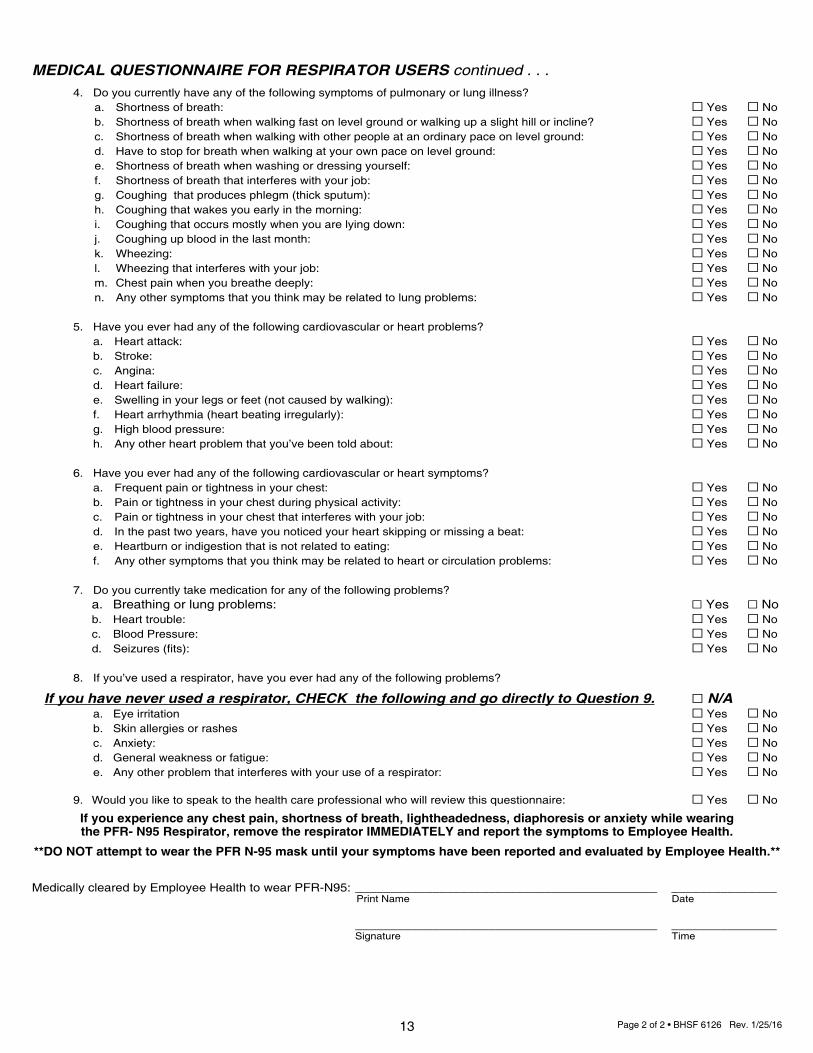
MEDICAL QUESTIONNAIRE FOR RESPIRATOR USERS continued . . . 4. Doyoucurrentlyhaveanyofthefollowingsymptomsofpulmonaryorlungillness? a. Shortness of breath: G Yes G No b. Shortnessofbreathwhenwalkingfastonlevelgroundorwalkingupaslighthillorincline? G Yes G No c. Shortnessofbreathwhenwalkingwithotherpeopleatanordinarypaceonlevelground: G Yes G No d. Havetostopforbreathwhenwalkingatyourownpaceonlevelground: G Yes G No e. Shortnessofbreathwhenwashingordressingyourself: G Yes G No f. Shortnessofbreaththatinterfereswithyourjob: G Yes G No g. Coughing that produces phlegm (thick sputum): G Yes G No h. Coughingthatwakesyouearlyinthemorning: G Yes G No i. Coughingthatoccursmostlywhenyouarelyingdown: G Yes G No j. Coughingupbloodinthelastmonth: G Yes G No k. Wheezing: G Yes G No l. Wheezingthatinterfereswithyourjob: G Yes G No m. Chestpainwhenyoubreathedeeply: G Yes G No n. Any other symptoms that you think may be related to lung problems: G Yes G No
5. Haveyoueverhadanyofthefollowingcardiovascularorheartproblems? a. Heart attack: G Yes G No b. Stroke: G Yes G No c. Angina: G Yes G No d. Heart failure: G Yes G No e. Swellinginyourlegsorfeet(notcausedbywalking): G Yes G No f. Heart arrhythmia (heart beating irregularly): G Yes G No g. High blood pressure: G Yes G No h. Any other heart problem that you’ve been told about: G Yes G No
6. Haveyoueverhadanyofthefollowingcardiovascularorheartsymptoms? a. Frequentpainortightnessinyourchest: G Yes G No b. Pain or tightness in your chest during physical activity: G Yes G No c. Painortightnessinyourchestthatinterfereswithyourjob: G Yes G No d. Inthepasttwoyears,haveyounoticedyourheartskippingormissingabeat: G Yes G No e. Heartburn or indigestion that is not related to eating: G Yes G No f. Any other symptoms that you think may be related to heart or circulation problems: G Yes G No
7. Doyoucurrentlytakemedicationforanyofthefollowingproblems? a. Breathing or lung problems: G Yes G No b. Heart trouble: G Yes G No c. Blood Pressure: G Yes G No d. Seizures(fits): G Yes G No
8. Ifyou’veusedarespirator,haveyoueverhadanyofthefollowingproblems?
If you have never used a respirator, CHECK the following and go directly to Question 9. G N/A a. Eye irritation G Yes G No b. Skin allergies or rashes G Yes G No c. Anxiety: G Yes G No d. Generalweaknessorfatigue: G Yes G No e. Anyotherproblemthatinterfereswithyouruseofarespirator: G Yes G No
9. Wouldyouliketospeaktothehealthcareprofessionalwhowillreviewthisquestionnaire: G Yes G No
If you experience any chest pain, shortness of breath, lightheadedness, diaphoresis or anxiety while wearing the PFR- N95 Respirator, remove the respirator IMMEDIATELY and report the symptoms to Employee Health.
**DO NOT attempt to wear the PFR N-95 mask until your symptoms have been reported and evaluated by Employee Health.**
MedicallyclearedbyEmployeeHealthtowearPFR-N95: ___________________________________________ _______________ Print Name Date
___________________________________________ _______________ Signature Time
Page2of2•BHSF6126Rev.1/25/16
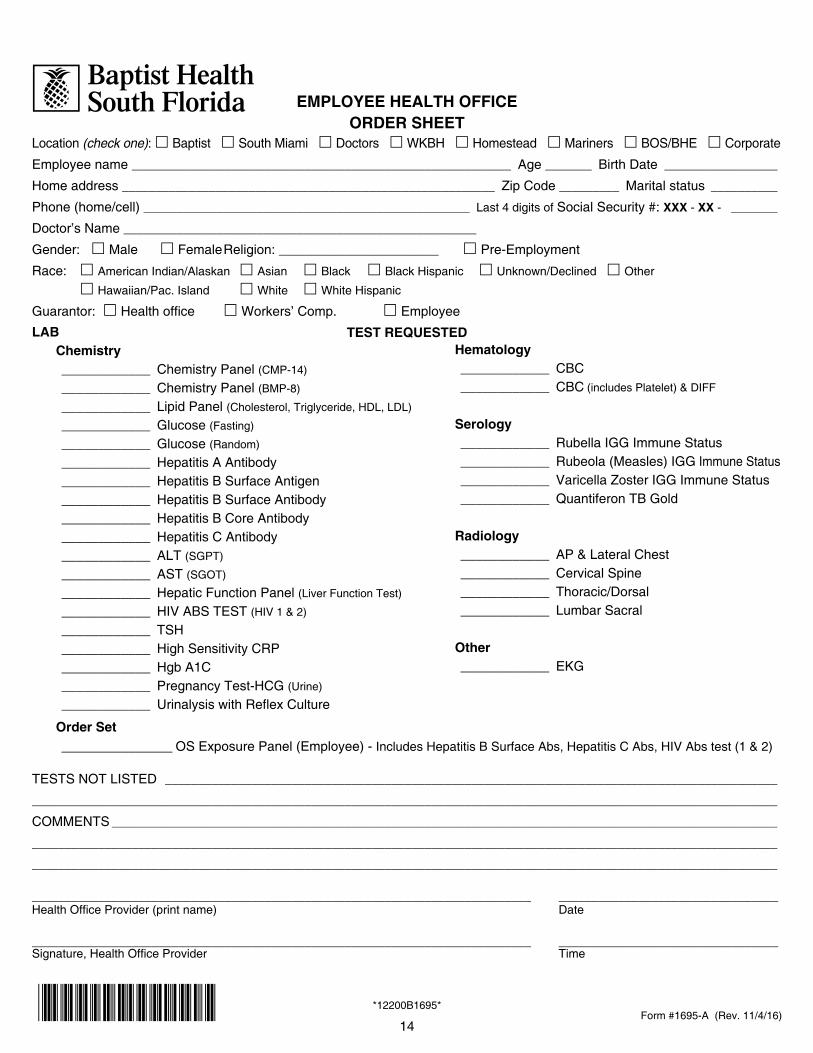
EMPLOYEE HEALTH OFFICEORDER SHEET
Location (check one): £ Baptist £ South Miami £ Doctors £ WKBH £ Homestead £ Mariners £ BOS/BHE £ Corporate
Employee name _________________________________________________________ Age _______ Birth Date _________________
Home address ________________________________________________________ Zip Code _________ Marital status __________
Phone (home/cell) _________________________________________________ Last 4 digits of Social Security #: XXX - XX - _______
Doctor’s Name _____________________________________________________
Gender: £ Male £ Female Religion: ________________________ £ Pre-Employment
Race: £ American Indian/Alaskan £ Asian £ Black £ Black Hispanic £ Unknown/Declined £ Other
£ Hawaiian/Pac.Island £ White £ White Hispanic
Guarantor: £Healthoffice £ Workers’ Comp. £ Employee
TEST REQUESTED
Form #1695-A (Rev. 11/4/16)
TESTS NOT LISTED ____________________________________________________________________________________________
________________________________________________________________________________________________________________
COMMENTS ____________________________________________________________________________________________________
________________________________________________________________________________________________________________
________________________________________________________________________________________________________________
___________________________________________________________________________ _________________________________HealthOfficeProvider(printname) Date
___________________________________________________________________________ _________________________________Signature,HealthOfficeProvider Time
*12200B1695*
Order Set _______________ OS Exposure Panel (Employee) - IncludesHepatitisBSurfaceAbs,HepatitisCAbs,HIVAbstest(1&2)
LAB Chemistry ____________ Chemistry Panel (CMP-14)
____________ Chemistry Panel (BMP-8)
____________ Lipid Panel (Cholesterol, Triglyceride, HDL, LDL)
____________ Glucose (Fasting)
____________ Glucose (Random)
____________ Hepatitis A Antibody ____________ Hepatitis B Surface Antigen ____________ Hepatitis B Surface Antibody ____________ Hepatitis B Core Antibody ____________ Hepatitis C Antibody ____________ ALT (SGPT)
____________ AST (SGOT)
____________ Hepatic Function Panel (Liver Function Test)
____________ HIV ABS TEST (HIV1&2) ____________ TSH ____________ High Sensitivity CRP ____________ Hgb A1C ____________ Pregnancy Test-HCG (Urine)
____________ UrinalysiswithReflexCulture
Hematology ____________ CBC ____________ CBC (includesPlatelet)&DIFF
Serology ____________ Rubella IGG Immune Status ____________ Rubeola (Measles) IGG Immune Status ____________ Varicella Zoster IGG Immune Status ____________ Quantiferon TB Gold
Radiology ____________ AP&LateralChest ____________ Cervical Spine ____________ Thoracic/Dorsal ____________ Lumbar Sacral
Other ____________ EKG
14
*12200B1695*

CONSENT TO TREATMENTI consent to all medical and surgical procedures and treatment, including but not limited to surgery, medical treatment, radiological examination, anesthesia, laboratory procedures, inpatient or outpatient services, and medications that may be performed,administeredorrenderedbyorunderthespecificorgeneralinstructionsofmyormychild’sphysiciansorsurgeonsduring this hospitalization or outpatient visit. In addition, I agree to abide by facility regulations designed to enhance the care and safety of patients, and I consent to the appropriate disposal of any specimen or other bodily materials removed during the course of my or my child’s treatment.
CONSENTIMIENTO PARA TRATAMIENTODoymiconsentimientoatodosycualquierprocedimiento,tratamientomedico,quirurgicosotratamientoquaincluyan,perono esten limitados a, cinugia, tratamiento medico, examinacion radiologica, anesthesia, servicios de laboratorio, servicios de “inpatientooutpatient”ymedicinasquepuedenserrealizados,administradosodadosporobajolasinstruccionesespecificaso generales del personal medico o de cirugia durante esta hospitalizacion o visita como paciente externo. Ademas, acuerdo aceptarlasregulacionesdeestecentro,regulacionesqueestandisenadasparafacilitarelcuidadoylasseguridaddelospacientesy,ademas,consientoalprocedimientoestablecidoparadisponerdecualquierespecimenodemiembrosremovidosduranteelcursodeltratamientodadoamipersonaoalademi(s)hijo(s)menores.
RELEASE OF INFORMATIONIauthorizethefollowingindividuals/healthcareproviderstoreleasecopiesofinformationintheirpossession,acquiredinthecourseofmyormychild’sexaminationandtreatment,tomyinsurancecarriersinconnectionwithmytreatmentforthepurposeof any insurance, Medicare or Medicaid payments:
-Thisfacilityanditsaffiliates -Utilizationreviewagenciesorauditors- Physicians - Other allied health professionals (Attending and Consulting)
PROPAGACION DE INFORMACIONAutorizo a los siguientes individuos/provedores de servicios de salud a dar copias de informacion sobre mi examen y tratamiento,oelexamenytratamientodemi(s)hijo(s)menores,ami(s)compania(s)desegurosconelprepositodepagosdeseguro, Medicare o Medicaid:
-EsteCentroysusafiliados -AgenciasoAuditoresde“Revisiondeutilizacion”-Medicos -Cualquierotroprofesionalsanitario (Primarios o consultores)
NOTICE OF PRIVACY PRACTICE AND RELEASE OF INFORMATIONIacknowledgethatIwasprovidedwithacopyoftheBaptistHealthNoticeofPrivacyPracticesdescribinghowBaptistHealthmayuseanddisclosemyhealthinformationunderthefederallaw.ProvidedthatBaptistHealthcontinuesitsgoodfaithefforttocomplywiththerequirementsofthefederalprivacylaw,Iherebyconsenttotheuseanddisclosureofmyhealthinformationforthepurposesandactivitiespermittedunderthefederalprivacylaw,whicharedescribedintheBaptistHealthNoticeofPrivacy Practices.
NOTIFICACION SOBRE LAS PRACTICAS DE PRIVACIDAD Y DIVULGACION DE INFORMACIONAcusoreciboquemehandadounacopiadelanotificacionsobrelasPracticasdePrivacidaddeBaptistHealthdescribiendocomo el Baptist Health segun la ley federal puede utilizar y dar a conocer informacion sobre mi salud. Siempre y cuando el BaptistHealthcontinuedebuenafeenesforzarseporcumplirconlosrequisitosdelaleyfederaldeprivacidad,consientomedianteelpresenteaqueseutiliceysedeaconocerinformacionsobremisaludparalospropositosyactividadespermitidoporlaleyfederaldeprivacidad,lacualsedescribeenlaNotificacionsobrelaspracticasdePrivacidaddeBaptistHealth.
____________________________________ XXX - XX - ____________Print Name/Nombre en letras de imprenta Last 4 Digits of SS#/ Últimos 4 dígitos del Seguro Social
____________________________________ __________ ____________________________________ __________Signature/Firma Date/Fecha Witness/Testigo Date/Fecha
Form #1695-B (Rev. 11/4/16)*10600B1695**12200B1695*
15

16
o Baptist o South Miami o Doctors o Homestead o Mariners o BOS / BHE o Corp
NAME: _______________________________________________ Last 4 Digits of SS#: XXX - XX - _________
I agree to abide by the policy of Baptist Health South Florida (BHSF) prohibiting the use, possession or sale of non-prescribednarcotics,perceptualdistorters,depressants,stimulants,marijuana,orothercontrolledsubstances.IunderstandthatevidenceofillegaldrugusagecouldaffectmyemploymentwiththeHospitalandIagreetoabidebyany decision made by the Hospital in this regard, I hereby give my voluntary consent to be medically examined and toprovideabloodand/orurinesamplewhichmaybetestedfordrugsoralcohol.Icertifythatthespecimengivenismy blood and/or urine, and that it is voluntary given for the purpose of the drug screen.
• Doyoucurrentlyuseprescribedornon-prescribedcontrolledsubstancesincludingnarcoticspainkillers,tranquilizers,sleepingmedication,appetitesuppressants,orotherstimulants?_________
• Haveyouusedanynon-prescribedcontrolledsubstancewithinthepast(a)six(6)months_________or, (b)five(5)years?_________
• Areyounowusinganyillegalcontrolledsubstances,includingheroin,cocaine,designerdrugs,perceptualdistorters,marijuanainanyform,orinhalants?_________
Please list ALL over the counter drugs (such as cough medicine, antihistamines, and anti-diarrheals) and prescription medication (including injections) you have taken (received) in the last four (4) weeks below.
OVER the COUNTER DRUGS / PRESCRIPTION DRUGS
Employee Health ServicesDRUG SCREEN NOTIFICATION OF MEDICATION(S)
SPECIFICBRAND NAME
MEDICATION/DRUG
REASON forMEDICATION
DOSAGESTRENGTH
per DAY
DATE and TIME of
LAST DOSE
HOW MANY DAYS USED
NameandaddressofPhysicianwhoprescribeddrug(s): ______________________________________________
____________________________________________________________________________________________Iherebyaffirmthattheinformationsetforthhereinistruetothebestofmyknowledgeandbelief,andIunderstandthiswillbecomeapartofmymedicalrecord.Iagreethatthatanyfalsestatementormisrepresentationonthisformsubjectsmeto ineligibilityforhire,andtodismissal ifhired.Further, IherebyreleaseandagreetoholdharmlessBaptistHealthSouthFlorida,itsofficer,agentsandemployeesfromanyliabilityconnectedwiththedrugscreenandthe use of the results thereof. I consent to take the drug screen.
Print Applicant/Donor’s Name: _______________________________________ Date: _____ / _____ /______
Applicant/Donor’s Signature: ________________________________________
Witness: ________________________________________________________
BHSF 6152 Rev. 2/7/1610800Y6152
BAPTIST HEALTH SOUTH FLORIDA
DRUG SCREEN NOTIFICATION OF MEDICATION(S)
*10800Y6152*
17
BHSF 6202 Rev. 2/7/1613025Y6202*13025Y6202*
PRE-EMPLOYMENT HEPATITIS-B IMMUNIZATION INFORMATION
Job Location: Please R (1) Box
q Baptist q South Miami q Doctors q WKBH q Homestead q Mariners q BOS / BHE q Corporate
Print Name: ____________________________________________________ Date: ______ / _____ / ________
Date of Birth: ____________________________ Last 4 Digits of SS#: ____________________________
Department: _______________________________ Position: ________________________________________
Home Phone: (_____) _____ - ______ Cell Phone: (_____) _____ - _____ Other Phone: (_____) _____ - _______
**************************************************************************************************************
Hepatitis-B Vaccine is offered to all employees having patient care contact and whenever other circumstances warrant it. High-risk areas are defined as all persons having contact with blood or body fluids.
Hepatitis-B Vaccine is a new genetically engineered vaccine. It is safe and effective and is not derived from human plasma. The vaccine is made from Brewer yeast.
During my post-offer health screening, I was advised of the above procedure. I had the opportunity to discuss it with the interviewing nurse. In addition, I was given literature regarding Hepatitis-B Vaccine.
If I accept a position at Baptist Health of South Florida, I will make an appointment to be seen within a week of my arrival to inform the Health Office nurse whether or not I wish to take advantage of this immunization. If I do not want the vaccine, I must sign a statement to that effect.
Applicant / Employee Signature: _________________________________ Date: _________________
Witness Signature: ____________________________________________ Date: _________________

18
BHSF 6203 Rev. 2/7/1611500Y6203*11500Y6203*
PRE-EMPLOYMENTPARTICULATE FILTER RESPIRATOR INFORMATION SHEET
Job Location: Please R (1) Box
q Baptist q South Miami q Doctors q Homestead q Mariners q BOS / BHE q Corporate
Print Name: ____________________________________________________ Date: ______ / _____ / ________
Date of Birth: ____________________________ Last 4 Digits of SS#: ____________________________
Department: _______________________________ Position: ________________________________________
Home Phone: (_____) _____ - ______ Cell Phone: (_____) _____ - _____ Other Phone: (_____) _____ - _______
**************************************************************************************************************
A Particulate Filter Respirator, (PFR-N95 MASK) is required to be worn by all employees having direct patient care/contact where there is a risk of exposure to Mycobacterium Tuberculosis (MTB).
During my Pre-Employment screening, I have been advised of the above policy and availability/requirement by NIOSH (National Institute for Occupational Safety and Health) for the use of the respirator mask. Baptist Hospital health care employees who meet the above criteria are to be fit tested for a Particulate Filter Respirator-PFR-N95.
I have been given literature to review regarding this mask, and have had the chance to discuss it with the interviewing Nurse.
Applicant / Employee Signature: _________________________________ Date: _________________
Witness Signature: ____________________________________________ Date: _________________

19
BAPTIST HEALTH SYSTEMSN-95 PARTICULATE FILTER
RESPIRATOR MASK (N-95 PFR)
G Iwearasize:__________________N-95 PARTICULATE FILTER RESPIRATOR MASK (N-95 PFR)
G IunderstandthatImustfitcheckthesealoftheN-95respiratormaskpriortoeachuse.ToplacetheN-95PFRrespiratormaskproperlyonmyfaceonestrapistobeplacedabovetheearandtheotherstrapgoesbelowtheearandthemaskisthenmoldedto my face.
G Iunderstand thatafitcheck isperformedby takingadeepbreath inand thenexhalingrapidly throughmymouth. Ifairis feltescapingfromaroundtheseal,themaskisreadjustedandthesameprocedureisrepeateduntilasealhasbeenestablished. This is to be done each time I place the N-95 PFR respirator mask on.
G IunderstandIamrequiredtoweartheN-95PFRrespiratormaskformyprotectionwhencaringforpatientswhoareonAirBorneisolationorwhenassisting / performing High Risk procedures (endotracheal suctioning / bronchoscopy) in patients suspected of having Tuberculosis.
G IunderstandifIloseorgainweight,havefacialsurgery,dentalworkoranyprocedurethatalterstheshapeofmyfaceandIamunabletosuccessfullycompleteafitcheck,IwillgotoEmployeeHealthServicestobere-fittested.
G IunderstandthatifIhaveanyfacialhairorbeardthatpreventsdirectcontactbetweenmyfaceandtheN-95PFRrespiratormaskIcannotwearthemask.
G Iwillnotknowinglyallowanotheremployee,whohasnotbeenfittested,intoanAirborneIsolationroom.IwillinsteadinstructthemtobefittestedinEmployeeHealthServices.IunderstandthatneitherthepatientnorfamilymembersaretoweartheN-95PFRrespirator mask.
G IunderstandthatifanAirborneisolationpatientistransportedtoanotherdepartment,thepatientistoweararegularsurgicalmaskand the mask should be changed about every 20 minutes to prevent aerosolization.
G IunderstandthatwhenthepatientonAirborneIsolationgoesoutsidetheisolationroomandwearsaregulartiesurgicalmaskthereisnoneedformetoweartheN-95PFRrespiratormask.IftheAFBisolationpatientisnotwearingthemaskIamtowearthe N-95 PFR respirator mask.
G IunderstandthatonlyoneN-95PFRrespiratormaskisrequiredforanentireshift(8to12hours)andthesamemaskmaybewornwhencaringformultipleAFBisolationpatients.
G IunderstandthatshouldtheintegrityoftheN-95PFRrespiratormaskbecomecompromised(becomessoiled,wetorthesealcannolongerbemaintained)IshoulddisposeofthemaskandobtainanewN-95PFRrespirator.
G IunderstandwhendisposingoftheN-95PFRrespiratoritcanbeplacedintheregulartrashunlessitissoiledwithvisiblebloodorbodyfluids(ThenIwillplaceitintheredbiomedicaltrashcontainer).
G IunderstandthatshouldIexperienceanychestpain,shortnessofbreath,light-headedness,diaphoresis,oranxietywhilewearingthePFRN-95Respirator,IamtoremovetheRespiratorASAPandreportthesymptomstotheEmployeeHealthOffice.IwillnotattempttowearthePFRn-95maskuntilmysymptomshavebeenreportedtoandIhavebeenevaluatedbytheEmployeeHealthOffice.
G IhavereadandansweredtheabovequestionsandhavebeengivenanopportunitytoaskquestionsregardingtheuseoftheN-95 PFR respirator mask.
Employee Name: ____________________________________________________________________ Date: __________________
Employee Signature: _________________________________________________________________ Time: _________________
Employee Health Services Representative’s Name: _________________________________________ Date: __________________
Representative’s Signature: ___________________________________________________________ Time: _________________
Designation: White - Employee Health, Canary - EmployeeBHSF 6122 Rev. 4/10
*11500Y6122**11500Y6122*

20
Pre-Employment ServicesCarbon Monoxide Testing Consent
Form #5342 Rev. 11/13
AtPre-EmploymentServices,newhiresor,inlimitedcases,existingemployeesareofferedtheopportunitytotake a Carbon Monoxide Breath test to determine their carbon monoxide status. Agreeing to take this voluntary testwillhelpusdetermineyoureligibilitytoreceivea$50creditperpayperiodonyourBaptistHealthSouthFlorida medical plan employee contribution. If your results are negative for carbon monoxide and you have no coveredadultdependentswhousetobacco,youwillreceivethecredit.Ifyourresultsarepositiveforcarbonmonoxideandyouarenotasmoker,youwillhavetheoptiontotakeanicotineurinetesttoconfirmyoursmokerstatus.Youwillbeineligibleforthemedicalplanemployeecontributioncreditifyoutestpositivefornicotine.AllsmokerswillreceiveaBHSFWellnessAdvantageStopSmokingpacketenclosedwithinformationaboutourSmokingCessationPrograms.Enrollingandcompletinganyoftheseprogramswithintherequiredtimeframewillallowustoupdateyourstatusasanon-smoker.
Print Name: _______________________________________ D.O.B. _____________ Last 4 Digits of SS# _________
By signing this form, I am giving consent to the Pre-Employment clinician to conduct a Carbon Monoxide Breath testtodeterminemycarbonmonoxidestatus.IunderstandthatmytestresultswillbesubmittedtoWellnessAdvantagefortracking,andcommunicatedtotheBenefitsDepartmentfordeterminingmyBHSFmedicalplanemployeecontribution.AlloftheinformationIprovideisstrictlyconfidential.Anypapercopiesofmyinformationwillbemaintainedinlockedfileswithlimitedaccess.
Employee Signature: _____________________________________________ Date: ____________________
Pre-Employment clinician: _________________________________________ Date: ____________________
To be completed by EHS Staff Carbon Monoxide Test Result: £ CO Negative £ CO Positive
Distribution: White-EmployeeHealth/Yellow-Candidate