new employee packet - the medical center · new employee packet ... if you are single and claim an...
TRANSCRIPT

New Employee Packet ( to print and compete before your f irst day)
You must turn this completed packet in at check-in on your first day of the new employee orientation program.
Use the Checklist below to make sure everything is complete.
Follow the Tax Form Guidelines on page 2 to assist you in filling out your tax forms correctly.
Leave Employee Number fields blank on these forms.
If you need additional assistance, please contact Human Resources at [email protected] or 270-745-1585
New Employee Paperwork Checklist
Employee Personal Information Sheet
Form I-9 (bring 2 forms of ID (example: driver’s license & Social Security card))
Form W-4
Form K-4
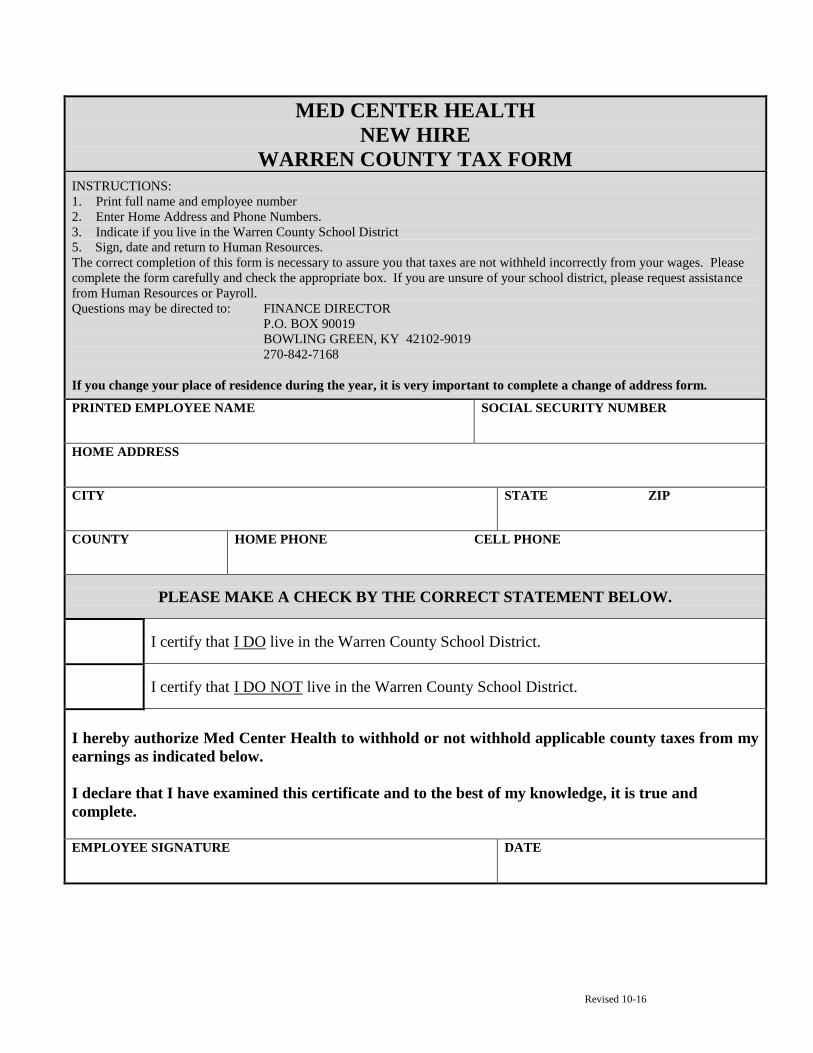
Warren County Tax Form
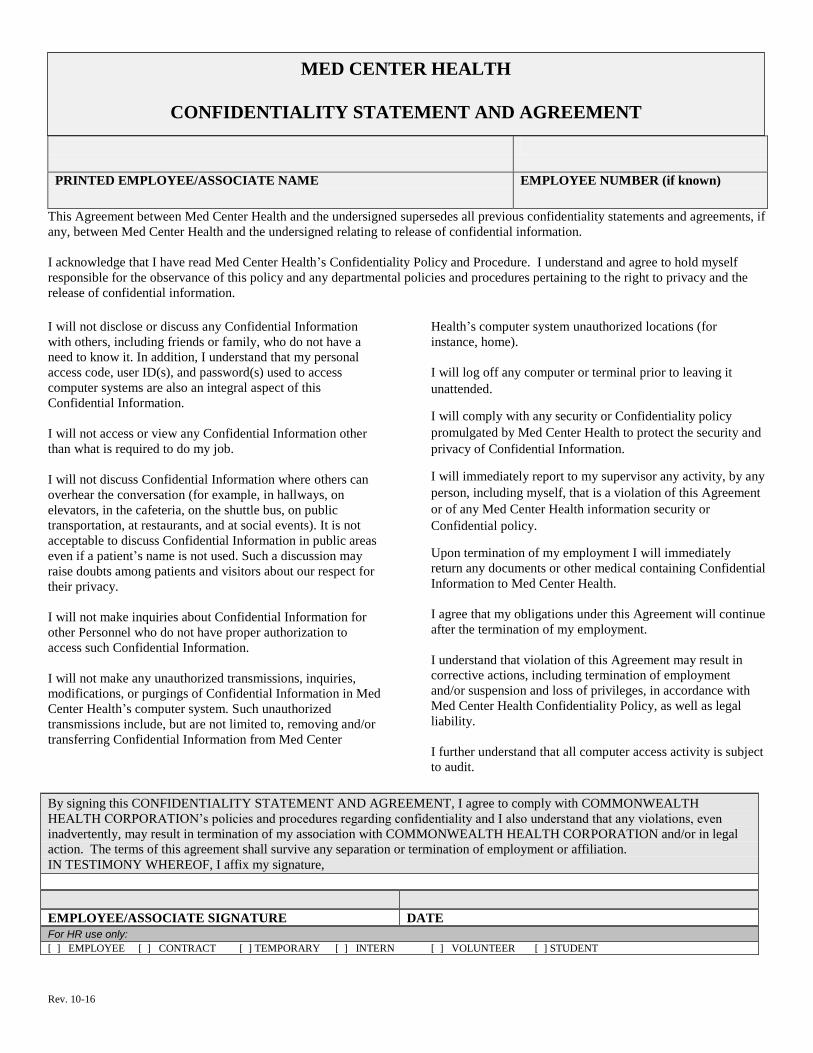
Confidentiality Statement and Agreement
Congratulations and welcome to the team!
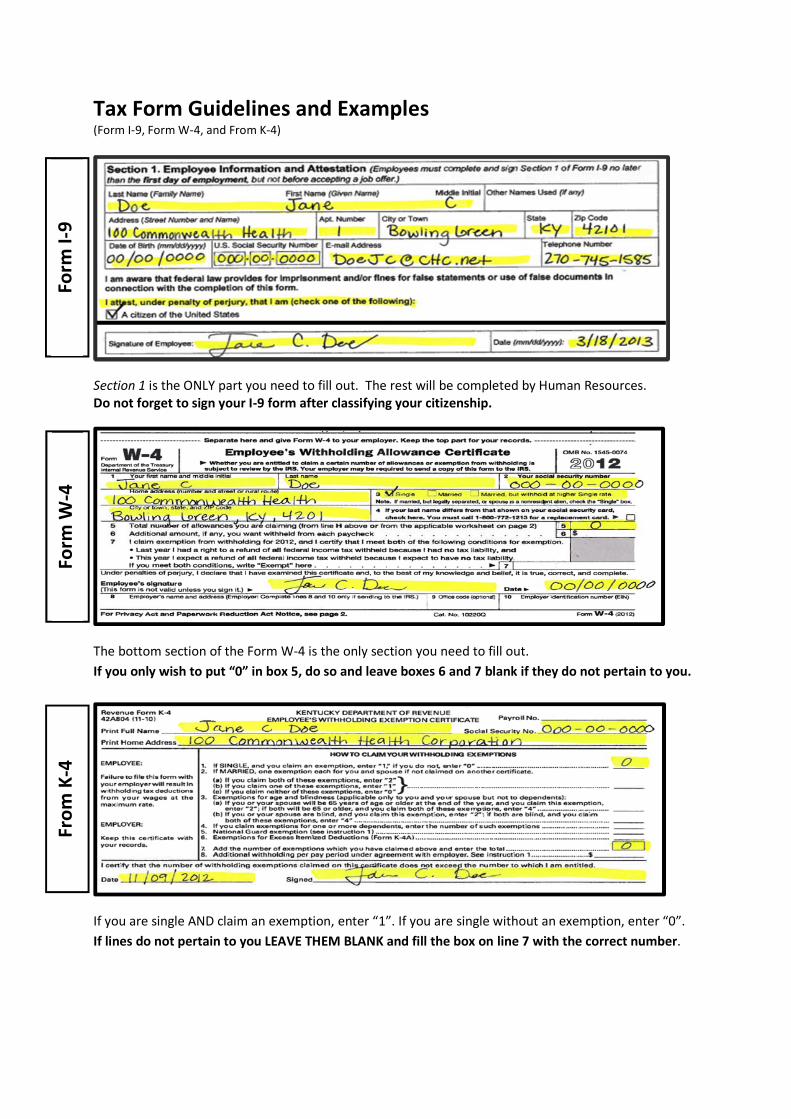
Tax Form Guidelines and Examples(Form I-9, Form W-4, and From K-4)
Section 1 is the ONLY part you need to fill out. The rest will be completed by Human Resources.Do not forget to sign your I-9 form after classifying your citizenship.
The bottom section of the Form W-4 is the only section you need to fill out.
If you only wish to put “0” in box 5, do so and leave boxes 6 and 7 blank if they do not pertain to you.
If you are single AND claim an exemption, enter “1”. If you are single without an exemption, enter “0”.
If lines do not pertain to you LEAVE THEM BLANK and fill the box on line 7 with the correct number.
Form
I-9
Form
W-4
Fro
mK
-4

Revised 12/12
MED CENTER HEALTH
EMPLOYEE PERSONAL INFORMATION SHEET
| | | | | | (if known) ______/_______/_______
EMPLOYEE NUMBER DATE
| | | | | | | | | | | | | | | | | | | | | | LAST NAME FIRST NAME
(print neatly & exactly as appears on your social security card)
| | | | | | | | | | | | | | | | | | | | | |
MIDDLE NAME PREFERRED NAME
( ) YOUR HOME PHONE ( ) YOUR CELL PHONE
DATE OF BIRTH ______/_______/_______ GENDER (check one) [ ] Male [ ] Female
MARITAL STATUS (check one)
PERSONAL E-MAIL ADDRESS [ ] Single [ ] Married
RACE (check one): VETERAN STATUS (check one):
[ ] White (0) Persons having origins in any of the original
peoples of Europe or the Middle East The Federal Contractor Veteran’s Employment Report program is
intended to assist the Department of Labor in determining whether
[ ] Black (1) Person having origins in any of the black
racial groups of Africa
special disabled and Vietnam-era veterans benefit from affirmative
actions in obtaining and advancing in employment. The information in
this section is voluntarily provided and will be kept confidential.
[ ] Asian or Pacific Islander (2) Persons having origins in any of the original
peoples of the Far East, Southeast Asia, Indian
Subcontinent, or the Pacific Islands
Disclosure or refusal to provide the information will not subject the
employee to adverse treatment and the information will be used only in
support of veteran’s programs in accordance with the regulation
implementing 38 U.S.C. 4212.
[ ] American Indian or Alaskan Native (3) Persons having origin in any of the original
peoples of North America, and who maintain
cultural identification through tribal affiliation
or community recognition
[ ] Not Applicable (2)
[ ] Special Disabled Veteran (7)
[ ] Veteran of the Vietnam-Era (6)
[ ] Desert Storm/Shield Veteran (8)
[ ] Hispanic (4) Persons of Mexican, Puerto Rican, Cuban,
Central or South American, or other Spanish
culture or origin, regardless of race
[ ] Other Veteran (9)
You may request a listing of Campaigns and Expeditions which qualify
for Veterans’ preference. [ ] Two or More Races (6) Persons of two or more races
combined
EMERGENCY CONTACT NAME: HOME PHONE # ( )
CELL PHONE # ( )
SHIRT SIZE: S M L XL XXL 3XL 4XL (circle one)
WORK PHONE # ( )
The above information is used for reporting purposes and will be maintained in your confidential personnel file.
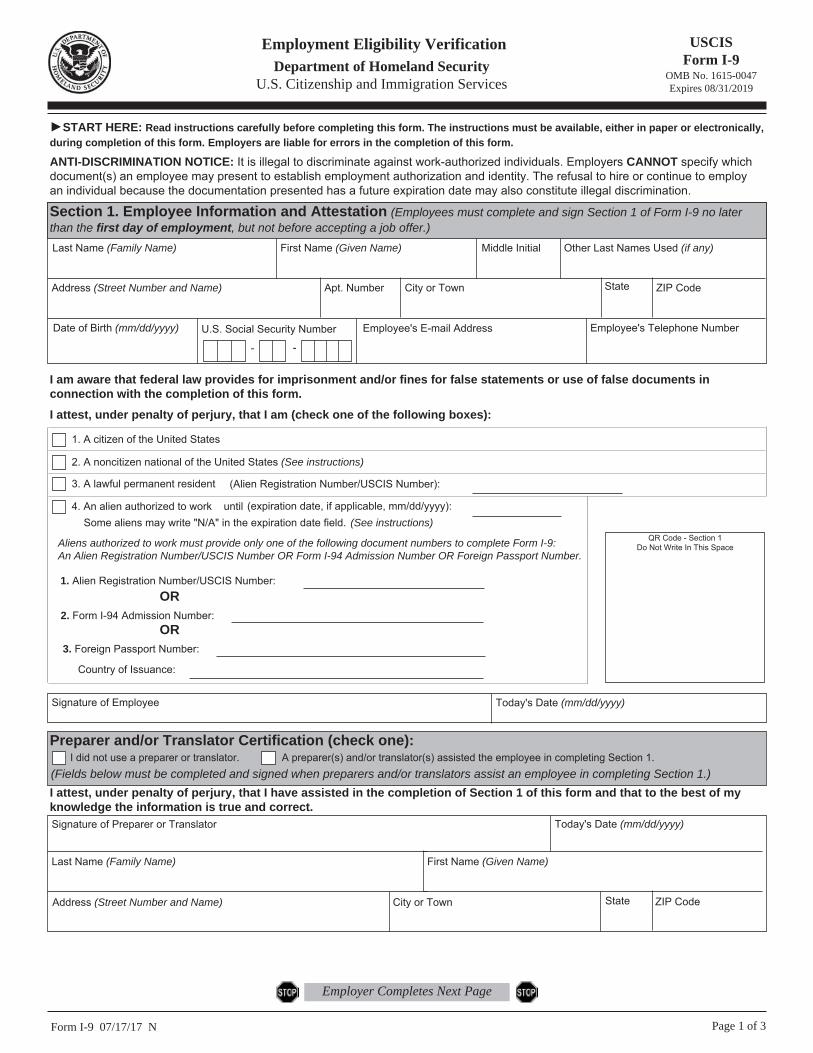
USCIS Form I-9
OMB No. 1615-0047 Expires 08/31/2019
Employment Eligibility Verification Department of Homeland Security
U.S. Citizenship and Immigration Services
Form I-9 07/17/17 N Page 1 of 3
►START HERE: Read instructions carefully before completing this form. The instructions must be available, either in paper or electronically, during completion of this form. Employers are liable for errors in the completion of this form.
ANTI-DISCRIMINATION NOTICE: It is illegal to discriminate against work-authorized individuals. Employers CANNOT specify which document(s) an employee may present to establish employment authorization and identity. The refusal to hire or continue to employ an individual because the documentation presented has a future expiration date may also constitute illegal discrimination.
Section 1. Employee Information and Attestation (Employees must complete and sign Section 1 of Form I-9 no later than the first day of employment, but not before accepting a job offer.)Last Name (Family Name) First Name (Given Name) Middle Initial Other Last Names Used (if any)
Address (Street Number and Name) Apt. Number City or Town State ZIP Code
Date of Birth (mm/dd/yyyy) U.S. Social Security Number
- -
Employee's E-mail Address Employee's Telephone Number
I am aware that federal law provides for imprisonment and/or fines for false statements or use of false documents in connection with the completion of this form.I attest, under penalty of perjury, that I am (check one of the following boxes):
1. A citizen of the United States
2. A noncitizen national of the United States (See instructions)
3. A lawful permanent resident
4. An alien authorized to work until (See instructions)
(expiration date, if applicable, mm/dd/yyyy):
(Alien Registration Number/USCIS Number):
Some aliens may write "N/A" in the expiration date field.
Aliens authorized to work must provide only one of the following document numbers to complete Form I-9: An Alien Registration Number/USCIS Number OR Form I-94 Admission Number OR Foreign Passport Number.
1. Alien Registration Number/USCIS Number:
2. Form I-94 Admission Number:
3. Foreign Passport Number:
Country of Issuance:
OR
OR
QR Code - Section 1 Do Not Write In This Space
Signature of Employee Today's Date (mm/dd/yyyy)
Preparer and/or Translator Certification (check one): I did not use a preparer or translator. A preparer(s) and/or translator(s) assisted the employee in completing Section 1.(Fields below must be completed and signed when preparers and/or translators assist an employee in completing Section 1.)I attest, under penalty of perjury, that I have assisted in the completion of Section 1 of this form and that to the best of my knowledge the information is true and correct.Signature of Preparer or Translator Today's Date (mm/dd/yyyy)
Last Name (Family Name) First Name (Given Name)
Address (Street Number and Name) City or Town State ZIP Code
Employer Completes Next Page
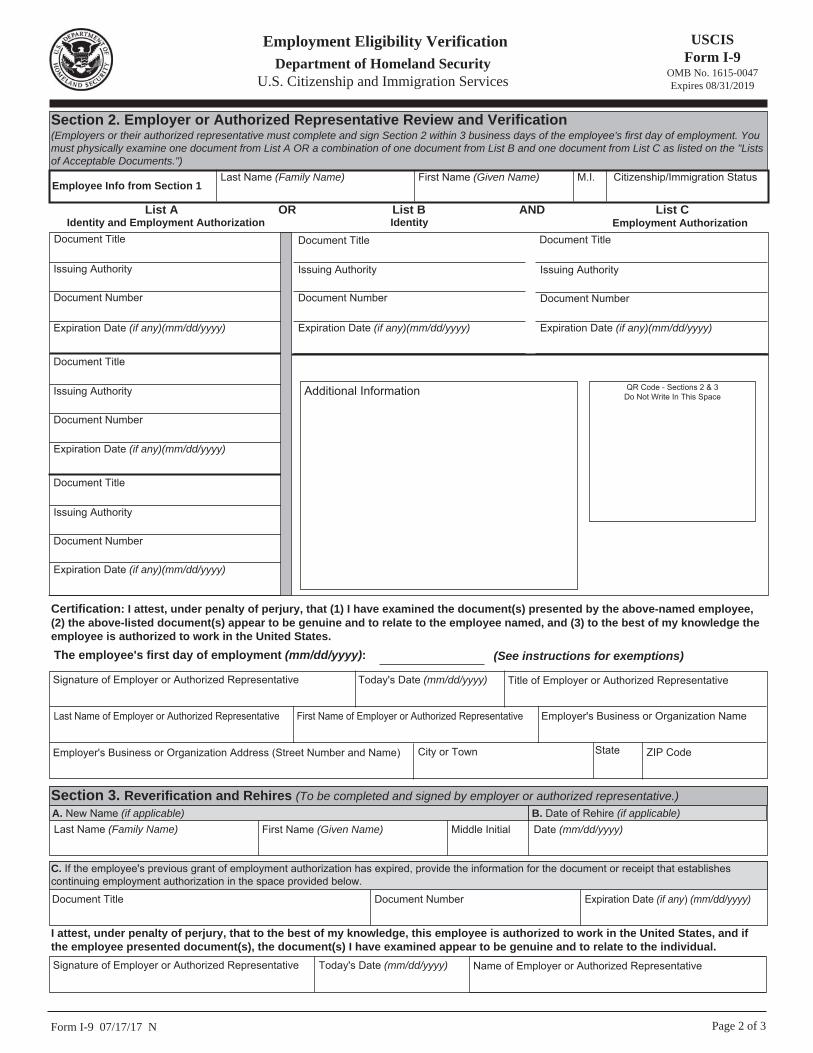
Form I-9 07/17/17 N Page 2 of 3
USCIS Form I-9
OMB No. 1615-0047 Expires 08/31/2019
Employment Eligibility Verification Department of Homeland Security
U.S. Citizenship and Immigration Services
Section 2. Employer or Authorized Representative Review and Verification (Employers or their authorized representative must complete and sign Section 2 within 3 business days of the employee's first day of employment. You must physically examine one document from List A OR a combination of one document from List B and one document from List C as listed on the "Lists of Acceptable Documents.")
Last Name (Family Name) M.I.First Name (Given Name)Employee Info from Section 1
Citizenship/Immigration Status
List AIdentity and Employment Authorization Identity Employment Authorization
OR List B AND List C
Additional Information QR Code - Sections 2 & 3 Do Not Write In This Space
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Certification: I attest, under penalty of perjury, that (1) I have examined the document(s) presented by the above-named employee, (2) the above-listed document(s) appear to be genuine and to relate to the employee named, and (3) to the best of my knowledge the employee is authorized to work in the United States. The employee's first day of employment (mm/dd/yyyy): (See instructions for exemptions)
Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Title of Employer or Authorized Representative
Last Name of Employer or Authorized Representative First Name of Employer or Authorized Representative Employer's Business or Organization Name
Employer's Business or Organization Address (Street Number and Name) City or Town State ZIP Code
Section 3. Reverification and Rehires (To be completed and signed by employer or authorized representative.)A. New Name (if applicable)Last Name (Family Name) First Name (Given Name) Middle Initial
B. Date of Rehire (if applicable)Date (mm/dd/yyyy)
Document Title Document Number Expiration Date (if any) (mm/dd/yyyy)
C. If the employee's previous grant of employment authorization has expired, provide the information for the document or receipt that establishes continuing employment authorization in the space provided below.
I attest, under penalty of perjury, that to the best of my knowledge, this employee is authorized to work in the United States, and if the employee presented document(s), the document(s) I have examined appear to be genuine and to relate to the individual. Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Name of Employer or Authorized Representative
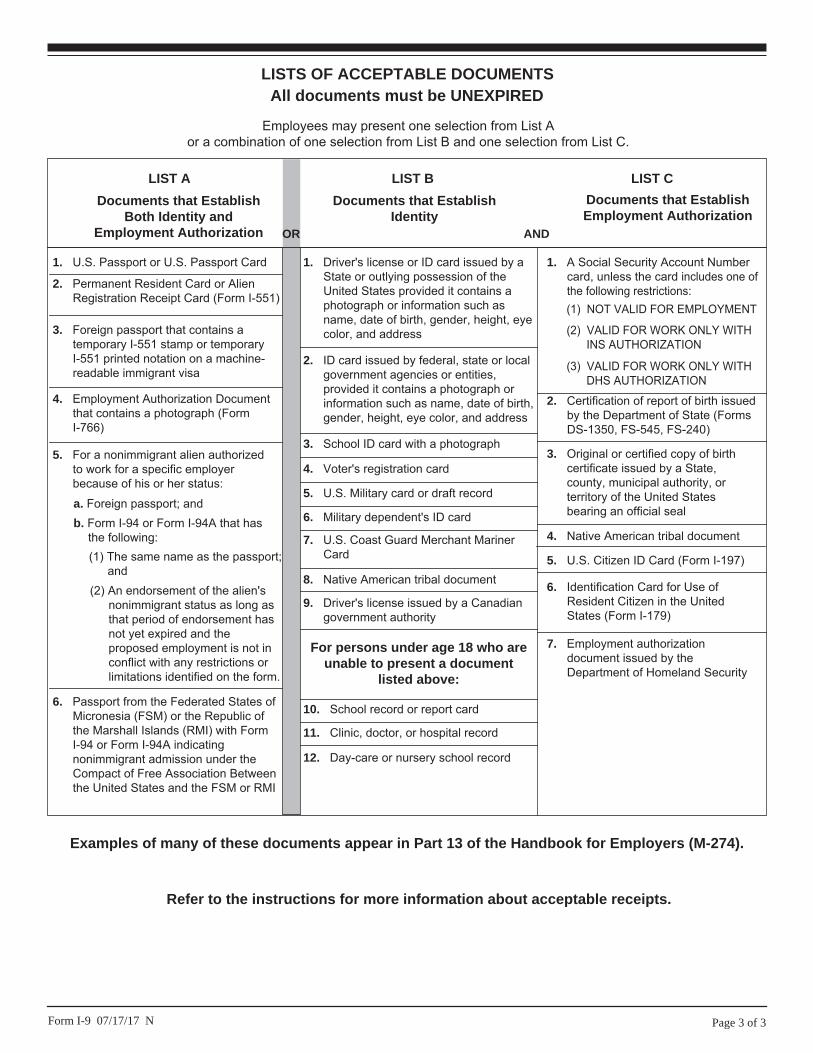
LISTS OF ACCEPTABLE DOCUMENTSAll documents must be UNEXPIRED
Employees may present one selection from List A or a combination of one selection from List B and one selection from List C.
LIST A
2. Permanent Resident Card or Alien Registration Receipt Card (Form I-551)
1. U.S. Passport or U.S. Passport Card
3. Foreign passport that contains a temporary I-551 stamp or temporary I-551 printed notation on a machine-readable immigrant visa
4. Employment Authorization Document that contains a photograph (Form I-766)
5. For a nonimmigrant alien authorized to work for a specific employer because of his or her status:
Documents that Establish Both Identity and
Employment Authorization
6. Passport from the Federated States of Micronesia (FSM) or the Republic of the Marshall Islands (RMI) with Form I-94 or Form I-94A indicating nonimmigrant admission under the Compact of Free Association Between the United States and the FSM or RMI
b. Form I-94 or Form I-94A that has the following:(1) The same name as the passport;
and(2) An endorsement of the alien's
nonimmigrant status as long as that period of endorsement has not yet expired and the proposed employment is not in conflict with any restrictions or limitations identified on the form.
a. Foreign passport; and
For persons under age 18 who are unable to present a document
listed above:
1. Driver's license or ID card issued by a State or outlying possession of the United States provided it contains a photograph or information such as name, date of birth, gender, height, eye color, and address
9. Driver's license issued by a Canadian government authority
3. School ID card with a photograph
6. Military dependent's ID card
7. U.S. Coast Guard Merchant Mariner Card
8. Native American tribal document
10. School record or report card
11. Clinic, doctor, or hospital record
12. Day-care or nursery school record
2. ID card issued by federal, state or local government agencies or entities, provided it contains a photograph or information such as name, date of birth, gender, height, eye color, and address
4. Voter's registration card
5. U.S. Military card or draft record
Documents that Establish Identity
LIST B
OR AND
LIST C
7. Employment authorization document issued by the Department of Homeland Security
1. A Social Security Account Number card, unless the card includes one of the following restrictions:
2. Certification of report of birth issued by the Department of State (Forms DS-1350, FS-545, FS-240)
3. Original or certified copy of birth certificate issued by a State, county, municipal authority, or territory of the United States bearing an official seal
4. Native American tribal document
6. Identification Card for Use of Resident Citizen in the United States (Form I-179)
Documents that Establish Employment Authorization
5. U.S. Citizen ID Card (Form I-197)
(2) VALID FOR WORK ONLY WITH INS AUTHORIZATION
(3) VALID FOR WORK ONLY WITH DHS AUTHORIZATION
(1) NOT VALID FOR EMPLOYMENT
Page 3 of 3Form I-9 07/17/17 N
Examples of many of these documents appear in Part 13 of the Handbook for Employers (M-274).
Refer to the instructions for more information about acceptable receipts.

-;=8!.$(!"'%&)#8]\]ZM!LM^MTWXUMV\[&!<]`!bVS!ZObSab!W\T]`[ObW]\!OP]cb!O\g!Tcbc`S!RSdSZ]^[S\ba!`SZObSR!b]!<]`[!L'.&!acQV!Oa!ZSUWaZObW]\!S\OQbSR!OTbS`!Wb!eOa!^cPZWaVSR&!U]!b]!
222")/0"(-1#&-/+'$(
C]ZXW[M&!8][^ZSbS!<]`[!L'.!a]!bVOb!g]c`!S[^Z]gS`!QO\!eWbVV]ZR!bVS!Q]``SQb!TSRS`OZ!W\Q][S!bOf!T`][!g]c`!^Og(!8]\aWRS`!Q][^ZSbW\U!O!\Se!<]`[!L'.!SOQV!gSO`!O\R!eVS\!g]c`!^S`a]\OZ!]`!TW\O\QWOZ!aWbcObW]\!QVO\USa(
7`MUX\QWV!NZWU!_Q\PPWTLQVO&!M]c![Og!QZOW[!SfS[^bW]\!T`][!eWbVV]ZRW\U!T]`!,*+2!WT!JW\P!]T!bVS!T]ZZ]eW\U!O^^Zg(
q!<]`!,*+1!g]c!VOR!O!`WUVb!b]!O!`STc\R!]T!ITT!TSRS`OZ!W\Q][S!bOf!eWbVVSZR!PSQOcaS!g]c!VOR!VW!bOf!ZWOPWZWbg&!IVL
q!<]`!,*+2!g]c!Sf^SQb!O!`STc\R!]T!ITT!TSRS`OZ!W\Q][S!bOf!eWbVVSZR!PSQOcaS!g]c!Sf^SQb!b]!VOdS!VW!bOf!ZWOPWZWbg(
?T!g]cn`S!SfS[^b&!Q][^ZSbS!WVTa!ZW\Sa!+&!,&!-&!.&!O\R!1!O\R!aWU\!bVS!T]`[!b]!dOZWRObS!Wb(!M]c`!SfS[^bW]\!T]`!,*+2!Sf^W`Sa!<SP`cO`g!+/&!,*+3(!ISS!FcP(!/*/&!JOf!LWbVV]ZRW\U!O\R!;abW[ObSR!JOf&!b]!ZSO`\![]`S!OP]cb!eVSbVS`!g]c!_cOZWTg!T]`!SfS[^bW]\!T`][!eWbVV]ZRW\U(
9MVMZIT!<V[\Z]K\QWV[?T!g]c!O`S\nb!SfS[^b&!T]ZZ]e!bVS!`Sab!]T!bVSaS!W\ab`cQbW]\a!b]!RSbS`[W\S!bVS!\c[PS`!]T!eWbVV]ZRW\U!OZZ]eO\QSa!g]c!aV]cZR!QZOW[!T]`!eWbVV]ZRW\U!T]`!,*+2!O\R!O\g!ORRWbW]\OZ!O[]c\b!]T!bOf!b]!VOdS!eWbVVSZR(!<]`!`SUcZO`!eOUSa&!eWbVV]ZRW\U![cab!PS!POaSR!]\!OZZ]eO\QSa!g]c!QZOW[SR!O\R![Og!\]b!PS!O!TZOb!O[]c\b!]`!^S`QS\bOUS!]T!eOUSa(
M]c!QO\!OZa]!caS!bVS!QOZQcZOb]`!Ob!<<<"067".4;#($&55!b]!RSbS`[W\S!g]c`!bOf!eWbVV]ZRW\U![]`S!OQQc`ObSZg(!8]\aWRS`
caW\U!bVWa!QOZQcZOb]`!WT!g]c!VOdS!O![]`S!Q][^ZWQObSR!bOf!aWbcObW]\&!acQV!Oa!WT!g]c!VOdS!O!e]`YW\U!a^]caS&![]`S!bVO\!]\S!X]P&!]`!O!ZO`US!O[]c\b!]T!\]\eOUS!W\Q][S!]cbaWRS!]T!g]c`!X]P(!!6TbS`!g]c`!<]`[!L'.!bOYSa!STTSQb&!g]c!QO\!OZa]!caS!bVWa!QOZQcZOb]`!b]!aSS!V]e!bVS!O[]c\b!]T!bOf!g]cn`S!VOdW\U!eWbVVSZR!Q][^O`Sa!b]!g]c`!^`]XSQbSR!b]bOZ!bOf!T]`!,*+2(!?T!g]c!caS!bVS!QOZQcZOb]`&!g]c!R]\nb!\SSR!b]!Q][^ZSbS!O\g!]T!bVS!e]`YaVSSba!T]`!<]`[!L'.(
D]bS!bVOb!WT!g]c!VOdS!b]]![cQV!bOf!eWbVVSZR&!g]c!eWZZ!`SQSWdS!O!`STc\R!eVS\!g]c!TWZS!g]c`!bOf!`Sbc`\(!?T!g]c!VOdS!b]]!ZWbbZS!bOf!eWbVVSZR&!g]c!eWZZ!]eS!bOf!eVS\!g]c!TWZS!g]c`!bOf!`Sbc`\&!O\R!g]c![WUVb!]eS!O!^S\OZbg(
8QTMZ[!_Q\P!U]T\QXTM!RWJ[!WZ!_WZSQVO!
[XW][M[&!?T!g]c!VOdS![]`S!bVO\!]\S!X]P!Ob!O!bW[S&!]`!WT!g]cn`S![O``WSR!O\R!g]c`!a^]caS!Wa!OZa]!e]`YW\U&!`SOR!OZZ!]T!bVS!W\ab`cQbW]\a!W\QZcRW\U!bVS!W\ab`cQbW]\a!T]`!bVS!Je]';O`\S`a)CcZbW^ZS!@]Pa!L]`YaVSSb!PST]`S!PSUW\\W\U(!
AWV_IOM!QVKWUM&!?T!g]c!VOdS!O!ZO`US!O[]c\b!]T!\]\eOUS!W\Q][S&!acQV!Oa!W\bS`Sab!]`!RWdWRS\Ra&!Q]\aWRS`![OYW\U!SabW[ObSR!bOf!^Og[S\ba!caW\U!<]`[!+*.*';I&!;abW[ObSR!JOf!T]`!?\RWdWRcOZa(!EbVS`eWaS&!g]c![WUVb!]eS!ORRWbW]\OZ!bOf(!E`&!g]c!QO\!caS!bVS!9SRcQbW]\a&!6RXcab[S\ba&!O\R!EbVS`!?\Q][S!L]`YaVSSb!]\!^OUS!-!]`!bVS!QOZQcZOb]`!Ob!222")/0"(-1#
'$%..!b]![OYS!ac`S!g]c!VOdS!S\]cUV!bOf!eWbVVSZR!T`][!g]c`!^OgQVSQY(!?T!g]c!VOdS!^S\aW]\!]`!O\\cWbg!W\Q][S&!aSS!FcP(!/*/!]`!caS!bVS!QOZQcZOb]`!Ob!222")/0"(-1#'$%..!b]!TW\R!]cb!WT!g]c!aV]cZR!ORXcab!g]c`!eWbVV]ZRW\U!]\!<]`[!L'.!]`!L'.F(!
AWVZM[QLMV\!ITQMV&!?T!g]cn`S!O!\]\`SaWRS\b!OZWS\&!aSS!D]bWQS!+-3,&!Ic^^ZS[S\bOZ!<]`[!
L'.!?\ab`cQbW]\a!T]`!D]\`SaWRS\b!6ZWS\a&!PST]`S!Q][^ZSbW\U!bVWa!T]`[(
EXMKQNQK!<V[\Z]K\QWV[
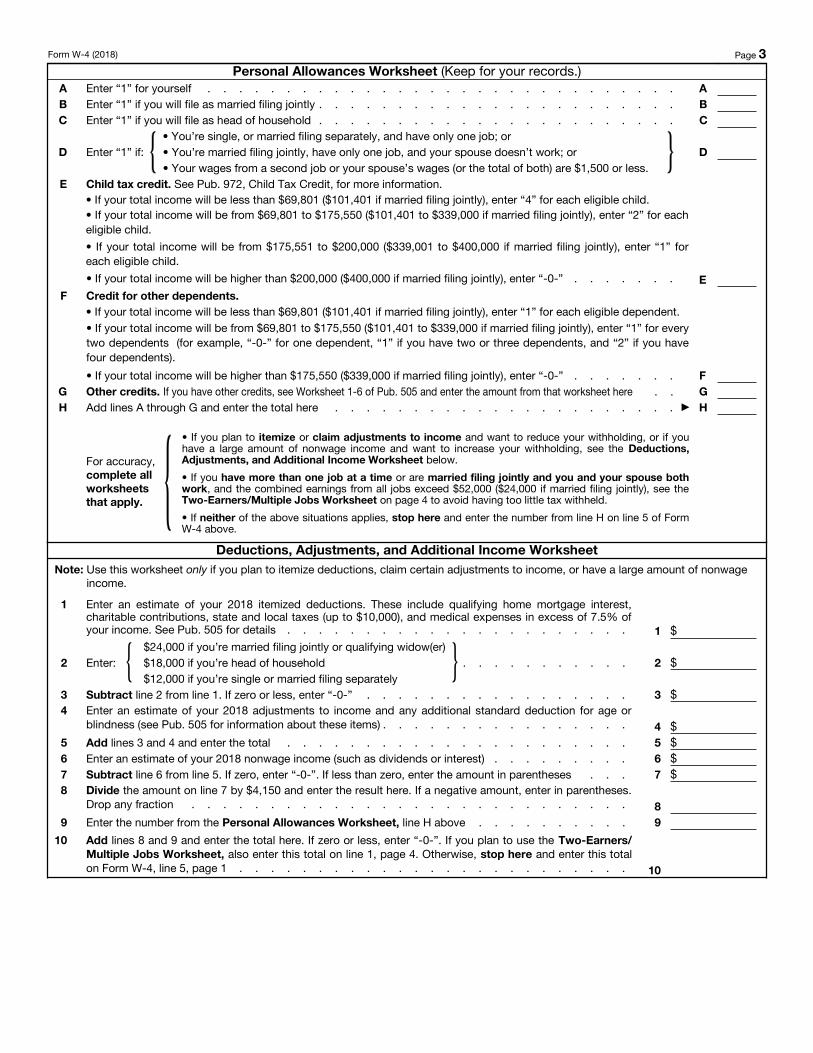
CMZ[WVIT!3TTW_IVKM[!GWZS[PMM\
8][^ZSbS!bVWa!e]`YaVSSb!]\!^OUS!-!TW`ab!b]!RSbS`[W\S!bVS!\c[PS`!]T!eWbVV]ZRW\U!OZZ]eO\QSa!b]!QZOW[(
?QVM!5&!',)+!4-!/497,/41+!51,)7,!348,%!
=S\S`OZZg&!g]c!QO\!QZOW[!VSOR!]T!V]caSV]ZR!TWZW\U!abObca!]\!g]c`!bOf!`Sbc`\!]\Zg!WT!g]cn`S!c\[O``WSR!O\R!^Og![]`S!bVO\!/*#!]T!bVS!Q]aba!]T!YSS^W\U!c^!O!V][S!T]`!g]c`aSZT!O\R!O!_cOZWTgW\U!W\RWdWRcOZ(!ISS!FcP(!/*+!T]`![]`S!W\T]`[ObW]\!OP]cb!TWZW\U!abObca(
?QVM!7&!5PQTL!\I`!KZMLQ\&!LVS\!g]c!TWZS!g]c`!bOf!`Sbc`\&!g]c![WUVb!PS!SZWUWPZS!b]!QZOW[!O!Q`SRWb!T]`!SOQV!]T!g]c`!_cOZWTgW\U!QVWZR`S\(!J]!_cOZWTg&!bVS!QVWZR![cab!PS!c\RS`!OUS!+1!Oa!]T!9SQS[PS`!-+!O\R![cab!PS!g]c`!RS^S\RS\b!eV]!ZWdSa!eWbV!g]c!T]`![]`S!bVO\!VOZT!bVS!gSO`(!J]!ZSO`\![]`S!OP]cb!bVWa!Q`SRWb&!aSS!FcP(!31,&!8VWZR!JOf!8`SRWb(!J]!`SRcQS!bVS!bOf!eWbVVSZR!T`][!g]c`!^Og!Pg!bOYW\U!bVWa!Q`SRWb!W\b]!OQQ]c\b&!T]ZZ]e!bVS!W\ab`cQbW]\a!]\!ZW\S!;!]T!bVS!e]`YaVSSb(!E\!bVS!e]`YaVSSb!g]c!eWZZ!PS!OaYSR!OP]cb!g]c`!b]bOZ!W\Q][S(!<]`!bVWa!^c`^]aS&!b]bOZ!W\Q][S!W\QZcRSa!OZZ!]T!g]c`!eOUSa!O\R!]bVS`!W\Q][S&!W\QZcRW\U!W\Q][S!SO`\SR!Pg!O!a^]caS&!Rc`W\U!bVS!gSO`(
?QVM!8&!5ZMLQ\!NWZ!W\PMZ!LMXMVLMV\[&!
LVS\!g]c!TWZS!g]c`!bOf!`Sbc`\&!g]c![WUVb!PS!SZWUWPZS!b]!QZOW[!O!Q`SRWb!T]`!SOQV!]T!g]c`!RS^S\RS\ba!bVOb!R]\nb!_cOZWTg!T]`!bVS!QVWZR!bOf!Q`SRWb&!acQV!Oa!O\g!RS^S\RS\b!QVWZR`S\!OUS!+1!O\R!]ZRS`(!J]!ZSO`\![]`S!OP]cb!bVWa!Q`SRWb&!aSS!FcP(!/*/(!J]!`SRcQS!bVS!bOf!eWbVVSZR!T`][!g]c`!^Og!Pg!bOYW\U!bVWa!Q`SRWb!W\b]!OQQ]c\b&!T]ZZ]e!bVS!W\ab`cQbW]\a!]\!ZW\S!<!]T!bVS!e]`YaVSSb(!E\!bVS!e]`YaVSSb&!g]c!eWZZ!PS!OaYSR!OP]cb!g]c`!b]bOZ!W\Q][S(!<]`!bVWa!^c`^]aS&!b]bOZ!W\Q][S!W\QZcRSa!OZZ!]T
EMXIZI\M!PMZM!IVL!OQ^M!8WZU!G%,!\W!aW]Z!MUXTWaMZ&!>MMX!\PM!_WZS[PMM\"[#!NWZ!aW]Z!ZMKWZL[&
<]`[!!#!"9S^O`b[S\b!]T!bVS!J`SOac`g!!?\bS`\OZ!HSdS\cS!IS`dWQS!
,8<7;A22B>!.6?55;71694!*77;@/902!+2=?6360/?2"!GPM\PMZ!aW]cZM!MV\Q\TML!\W!KTIQU!I!KMZ\IQV!V]UJMZ!WN!ITTW_IVKM[!WZ!M`MUX\QWV!NZWU!_Q\PPWTLQVO!Q[
[]JRMK\!\W!ZM^QM_!Ja!\PM!<DE&!HW]Z!MUXTWaMZ!UIa!JM!ZMY]QZML!\W!!!!!!!M]c`!TW`ab!\O[S!O\R![WRRZS!W\WbWOZ BOab!\O[S
>][S!ORR`Saa!$\c[PS`!O\R!ab`SSb!]`!`c`OZ!`]cbS%
8Wbg!]`!b]e\&!abObS&!O\R!N?F!Q]RS
*!!!!!HW]Z![WKQIT![MK]ZQ\a!V]UJMZ
+ IW\UZS CO``WSR CO``WSR&!Pcb!eWbVV]ZR!Ob!VWUVS`!IW\UZS!`ObS(
AW\M2!?T![O``WSR!TWZW\U!aS^O`ObSZg&!QVSQY!oCO``WSR&!Pcb!eWbVV]ZR!Ob!VWUVS`!IW\UZS!`ObS(p
, <N!aW]Z!TI[\!VIUM!LQNNMZ[!NZWU!\PI\![PW_V!WV!aW]Z![WKQIT![MK]ZQ\a!KIZL$!
KPMKS!PMZM&!HW]!U][\!KITT!0((%//*%)*)+!NWZ!I!ZMXTIKMUMV\!KIZL&!!!!!! "
- J]bOZ!\c[PS`!]T!OZZ]eO\QSa!g]cn`S!QZOW[W\U!$T`][!bVS!O^^ZWQOPZS!e]`YaVSSb!]\!bVS!T]ZZ]eW\U!!^OUSa%! ( ( ( -
. 6RRWbW]\OZ!O[]c\b&!WT!O\g&!g]c!eO\b!eWbVVSZR!T`][!SOQV!^OgQVSQY! ( ( ( ( ( ( ( ( ( ( ( ( ( ( . "
/ ?!QZOW[!SfS[^bW]\!T`][!eWbVV]ZRW\U!T]`!,*+2&!O\R!?!QS`bWTg!bVOb!?![SSb!JW\P!]T!bVS!T]ZZ]eW\U!Q]\RWbW]\a!T]`!SfS[^bW]\(
q!BOab!gSO`!?!VOR!O!`WUVb!b]!O!`STc\R!]T!ITT!TSRS`OZ!W\Q][S!bOf!eWbVVSZR!PSQOcaS!?!VOR!VW!bOf!ZWOPWZWbg&!IVL
q!JVWa!gSO`!?!Sf^SQb!O!`STc\R!]T!ITT!TSRS`OZ!W\Q][S!bOf!eWbVVSZR!PSQOcaS!?!Sf^SQb!b]!VOdS!VW!bOf!ZWOPWZWbg(
?T!g]c![SSb!P]bV!Q]\RWbW]\a&!e`WbS!o;fS[^bp!VS`S!( ( ( ( ( ( ( ( ( ( ( ( ( ( ( " /
K\RS`!^S\OZbWSa!]T!^S`Xc`g&!?!RSQZO`S!bVOb!?!VOdS!SfO[W\SR!bVWa!QS`bWTWQObS!O\R&!b]!bVS!PSab!]T![g!Y\]eZSRUS!O\R!PSZWST&!Wb!Wa!b`cS&!Q]``SQb&!O\R!Q][^ZSbS(
7UXTWaMMc[![QOVI\]ZM!!$JVWa!T]`[!Wa!\]b!dOZWR!c\ZSaa!g]c!aWU\!Wb(%!" 6I\M!"
0!!;[^Z]gS`na!\O[S!O\R!ORR`Saa!$7UXTWaMZ2!8][^ZSbS!P]fSa!2!O\R!+*!WT!aS\RW\U!b]!?HI!O\R!Q][^ZSbS!P]fSa!2&!3&!O\R!+*!WT!aS\RW\U!b]!IbObS!9W`SQb]`g!]T!DSe!>W`Sa(%
1!!<W`ab!RObS!]T!S[^Z]g[S\b
)(!!;[^Z]gS`!WRS\bWTWQObW]\!\c[PS`!$;?D%
8WZ!CZQ^IKa!3K\!IVL!CIXMZ_WZS!DML]K\QWV!3K\!AW\QKM$
<]`[!L'.!$,*+2% FOUS!*!
g]c`!eOUSa!O\R!]bVS`!W\Q][S&!W\QZcRW\U!W\Q][S!SO`\SR!Pg!O!a^]caS&!Rc`W\U!bVS!gSO`(
?QVM!9&!B\PMZ!KZMLQ\[&!M]c![WUVb!PS!OPZS!b]!`SRcQS!bVS!bOf!eWbVVSZR!T`][!g]c`!^OgQVSQY!WT!g]c!Sf^SQb!b]!QZOW[!]bVS`!bOf!Q`SRWba&!acQV!Oa!bVS!SO`\SR!W\Q][S!bOf!Q`SRWb!O\R!bOf!Q`SRWba!T]`!SRcQObW]\!O\R!QVWZR!QO`S!Sf^S\aSa(!?T!g]c!R]!a]&!g]c`!^OgQVSQY!eWZZ!PS!ZO`US`!Pcb!bVS!O[]c\b!]T!O\g!`STc\R!bVOb!g]c!`SQSWdS!eVS\!g]c!TWZS!g]c`!bOf!`Sbc`\!eWZZ!PS!a[OZZS`(!<]ZZ]e!bVS!W\ab`cQbW]\a!T]`!L]`YaVSSb!+'0!W\!FcP(!/*/!WT!g]c!eO\b!b]!`SRcQS!g]c`!eWbVV]ZRW\U!b]!bOYS!bVSaS!Q`SRWba!W\b]!OQQ]c\b(
6ML]K\QWV[$!3LR][\UMV\[$!IVL!3LLQ\QWVIT!<VKWUM!GWZS[PMM\
8][^ZSbS!bVWa!e]`YaVSSb!b]!RSbS`[W\S!WT!g]cn`S!OPZS!b]!`SRcQS!bVS!bOf!eWbVVSZR!T`][!g]c`!^OgQVSQY!b]!OQQ]c\b!T]`!g]c`!WbS[WhSR!RSRcQbW]\a!O\R!]bVS`!ORXcab[S\ba!b]!W\Q][S!acQV!Oa!?H6!Q]\b`WPcbW]\a(!?T!g]c!R]!a]&!g]c`!`STc\R!Ob!bVS!S\R!]T!bVS!gSO`!eWZZ!PS!a[OZZS`&!Pcb!g]c`!^OgQVSQY!eWZZ!PS!ZO`US`(!M]cn`S!\]b!`S_cW`SR!b]!Q][^ZSbS!bVWa!e]`YaVSSb!]`!`SRcQS!g]c`!eWbVV]ZRW\U!WT!g]c!R]\nb!eWaV!b]!R]!a](
M]c!QO\!OZa]!caS!bVWa!e]`YaVSSb!b]!TWUc`S!]cb!V]e![cQV!b]!W\Q`SOaS!bVS!bOf!eWbVVSZR!T`][!g]c`!^OgQVSQY!WT!g]c!VOdS!O!ZO`US!O[]c\b!]T!\]\eOUS!W\Q][S&!acQV!Oa!W\bS`Sab!]`!RWdWRS\Ra(
6\]bVS`!]^bW]\!Wa!b]!bOYS!bVSaS!WbS[a!W\b]!OQQ]c\b!O\R![OYS!g]c`!eWbVV]ZRW\U![]`S!OQQc`ObS!Pg!caW\U!bVS!QOZQcZOb]`!Ob!222")/0"(-1#'$%..(!?T!g]c!caS!bVS!QOZQcZOb]`&!g]c!R]\nb!\SSR!b]!Q][^ZSbS!O\g!]T!bVS!e]`YaVSSba!T]`!<]`[!L'.(
F_W%7IZVMZ['@]T\QXTM!=WJ[!GWZS[PMM\
8][^ZSbS!bVWa!e]`YaVSSb!WT!g]c!VOdS![]`S
bVO\!]\S!X]P!Ob!O!bW[S!]`!O`S![O``WSR!TWZW\U!X]W\bZg!O\R!VOdS!O!e]`YW\U!a^]caS(!?T!g]c!R]\nb!Q][^ZSbS!bVWa!e]`YaVSSb&!g]c![WUVb!VOdS!b]]!ZWbbZS!bOf!eWbVVSZR(!?T!a]&!g]c!eWZZ!]eS!bOf!eVS\!g]c!TWZS!g]c`!bOf!`Sbc`\!O\R![WUVb!PS!acPXSQb!b]!O!^S\OZbg(
<WUc`S!bVS!b]bOZ!\c[PS`!]T!OZZ]eO\QSa!g]cn`S!S\bWbZSR!b]!QZOW[!O\R!O\g!ORRWbW]\OZ!O[]c\b!]T!bOf!b]!eWbVV]ZR!]\!OZZ!X]Pa!caW\U!e]`YaVSSba!T`][!]\Zg!]\S!<]`[!L'.(!8ZOW[!OZZ!OZZ]eO\QSa!]\!bVS!L'.!bVOb!g]c!]`!g]c`!a^]caS!TWZS!T]`!bVS!VWUVSab!^OgW\U!X]P!W\!g]c`!TO[WZg!O\R!QZOW[!hS`]!OZZ]eO\QSa!]\!<]`[a!L'.!TWZSR!T]`!OZZ!]bVS`!X]Pa(!<]`!SfO[^ZS&!WT!g]c!SO`\!"0*&***!^S`!gSO`!O\R!g]c`!a^]caS!SO`\a!",*&***&!g]c!aV]cZR!Q][^ZSbS!bVS!e]`YaVSSba!b]!RSbS`[W\S!eVOb!b]!S\bS`!]\!ZW\Sa!/!O\R!0!]T!g]c`!<]`[!L'.&!O\R!g]c`!a^]caS!aV]cZR!S\bS`!hS`]!$o'*'p%!]\!ZW\Sa!/!O\R!0!]T!VWa!]`!VS`!<]`[!L'.(!ISS!FcP(!/*/!T]`!RSbOWZa(
6\]bVS`!]^bW]\!Wa!b]!caS!bVS!QOZQcZOb]`!Ob!222")/0"(-1#'$%..!b]![OYS!g]c`!eWbVV]ZRW\U![]`S!OQQc`ObS(
FQX2!?T!g]c!VOdS!O!e]`YW\U!a^]caS!O\R!g]c`!W\Q][Sa!O`S!aW[WZO`&!g]c!QO\!QVSQY!bVS!oCO``WSR&!Pcb!eWbVV]ZR!Ob!VWUVS`!IW\UZS!`ObSp!P]f!W\abSOR!]T!caW\U!bVWa!e]`YaVSSb(!?T!g]c!QV]]aS!bVWa!]^bW]\&!bVS\!SOQV!a^]caS!aV]cZR!TWZZ!]cb!bVS!FS`a]\OZ!6ZZ]eO\QSa!L]`YaVSSb!O\R!QVSQY!bVS!oCO``WSR&!Pcb!eWbVV]ZR!Ob!VWUVS`!IW\UZS!`ObSp!P]f!]\!<]`[!L'.&!Pcb!]\Zg!]\S!a^]caS!aV]cZR!QZOW[!O\g!OZZ]eO\QSa!T]`!Q`SRWba!]`!TWZZ!]cb!bVS!9SRcQbW]\a&!6RXcab[S\ba&!O\R!6RRWbW]\OZ!?\Q][S!L]`YaVSSb(
<V[\Z]K\QWV[!NWZ!7UXTWaMZ7UXTWaMM[$!LW!VW\!KWUXTM\M!JW`!0$!1$!WZ!
)(&!HW]Z!MUXTWaMZ!_QTT!KWUXTM\M!\PM[M!
JW`M[!QN!VMKM[[IZa&
AM_!PQZM!ZMXWZ\QVO&!;[^Z]gS`a!O`S
`S_cW`SR!Pg!ZOe!b]!`S^]`b!\Se!S[^Z]gSSa!b]!O!RSaWU\ObSR!IbObS!9W`SQb]`g!]T!DSe!>W`Sa(!;[^Z]gS`a![Og!caS!<]`[!L'.&!P]fSa!2&!3&!O\R!+*!b]!Q][^Zg!eWbV!bVS!\Se!VW`S!`S^]`bW\U!`S_cW`S[S\b!T]`!O!\SeZg!VW`SR!S[^Z]gSS(!6!\SeZg!VW`SR!S[^Z]gSS!Wa!O\!S[^Z]gSS!eV]!VOa\nb!^`SdW]caZg!PSS\!S[^Z]gSR!Pg!bVS!S[^Z]gS`&!]`!eV]!eOa!^`SdW]caZg!S[^Z]gSR!Pg!bVS!S[^Z]gS`!Pcb!VOa!PSS\!aS^O`ObSR!T`][!acQV!^`W]`!S[^Z]g[S\b!T]`!Ob!ZSOab!0*!Q]\aSQcbWdS!ROga(!;[^Z]gS`a!aV]cZR!Q]\bOQb!bVS!O^^`]^`WObS!IbObS!9W`SQb]`g!]T!DSe!>W`Sa!b]!TW\R!]cb!V]e!b]!acP[Wb!O!Q]^g!]T!bVS!Q][^ZSbSR!<]`[!L'.(!<]`!W\T]`[ObW]\!O\R!ZW\Ya!b]!SOQV!RSaWU\ObSR!IbObS!9W`SQb]`g!]T!DSe!>W`Sa!$W\QZcRW\U!T]`!K(I(!bS``Wb]`WSa%&!U]!b]!<<<")*-"//7".4;#564.6)27#*77#
,2514=,67(
?T!O\!S[^Z]gS`!Wa!aS\RW\U!O!Q]^g!]T!<]`[!L'.!b]!O!RSaWU\ObSR!IbObS!9W`SQb]`g!]T!DSe!>W`Sa!b]!Q][^Zg!eWbV!bVS!\Se!VW`S!`S^]`bW\U!`S_cW`S[S\b!T]`!O!\SeZg!VW`SR!S[^Z]gSS&!Q][^ZSbS!P]fSa!2&!3&!O\R!+*!Oa!T]ZZ]ea(!
4W`!0&!;\bS`!bVS!S[^Z]gS`na!\O[S!O\R!ORR`Saa(!?T!bVS!S[^Z]gS`!Wa!aS\RW\U!O!Q]^g!]T!bVWa!T]`[!b]!O!IbObS!9W`SQb]`g!]T!DSe!>W`Sa&!S\bS`!bVS!ORR`Saa!eVS`S!QVWZR!ac^^]`b!OUS\QWSa!aV]cZR!aS\R!W\Q][S!eWbVV]ZRW\U!]`RS`a(!
4W`!1&!?T!bVS!S[^Z]gS`!Wa!aS\RW\U!O!Q]^g!]T!bVWa!T]`[!b]!O!IbObS!9W`SQb]`g!]T!DSe!>W`Sa&!S\bS`!bVS!S[^Z]gSSna!TW`ab!RObS!]T!S[^Z]g[S\b&!eVWQV!Wa!bVS!RObS!aS`dWQSa!T]`!^Og[S\b!eS`S!TW`ab!^S`T]`[SR!Pg!bVS!S[^Z]gSS(!?T!bVS!S[^Z]gS`!`SVW`SR!bVS!S[^Z]gSS!OTbS`!bVS!S[^Z]gSS!VOR!PSS\!aS^O`ObSR!T`][!bVS!S[^Z]gS`na!aS`dWQS!T]`!Ob!ZSOab!0*!ROga&!S\bS`!bVS!`SVW`S!RObS(
4W`!)(&!;\bS`!bVS!S[^Z]gS`na!S[^Z]gS`!WRS\bWTWQObW]\!\c[PS`!$;?D%(
<]`[!L'.!$,*+2% FOUS!+
CMZ[WVIT!3TTW_IVKM[!GWZS[PMM\!$ASS^!T]`!g]c`!`SQ]`Ra(%
3 ;\bS`!o+p!T]`!g]c`aSZT! ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( 3
4 ;\bS`!o+p!WT!g]c!eWZZ!TWZS!Oa![O``WSR!TWZW\U!X]W\bZg ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( 4
5 ;\bS`!o+p!WT!g]c!eWZZ!TWZS!Oa!VSOR!]T!V]caSV]ZR ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( 5
6 ;\bS`!o+p!WT4
q!M]cn`S!aW\UZS&!]`![O``WSR!TWZW\U!aS^O`ObSZg&!O\R!VOdS!]\Zg!]\S!X]P5!]`
q!M]cn`S![O``WSR!TWZW\U!X]W\bZg&!VOdS!]\Zg!]\S!X]P&!O\R!g]c`!a^]caS!R]Sa\nb!e]`Y5!]`
q!M]c`!eOUSa!T`][!O!aSQ]\R!X]P!]`!g]c`!a^]caSna!eOUSa!$]`!bVS!b]bOZ!]T!P]bV%!O`S!"+&/**!]`!ZSaa(
6
7 5PQTL!\I`!KZMLQ\&!ISS!FcP(!31,&!8VWZR!JOf!8`SRWb&!T]`![]`S!W\T]`[ObW]\(
q!?T!g]c`!b]bOZ!W\Q][S!eWZZ!PS!ZSaa!bVO\!"03&2*+!$"+*+&.*+!WT![O``WSR!TWZW\U!X]W\bZg%&!S\bS`!o.p!T]`!SOQV!SZWUWPZS!QVWZR(!
q!?T!g]c`!b]bOZ!W\Q][S!eWZZ!PS!T`][!"03&2*+!b]!"+1/&//*!$"+*+&.*+!b]!"--3&***!WT![O``WSR!TWZW\U!X]W\bZg%&!S\bS`!o,p!T]`!SOQV!
SZWUWPZS!QVWZR(
q! ?T!g]c`! b]bOZ! W\Q][S!eWZZ!PS! T`][!"+1/&//+!b]!",**&***! $"--3&**+!b]!".**&***! WT![O``WSR!TWZW\U! X]W\bZg%&!S\bS`!o+p! T]`!
SOQV!SZWUWPZS!QVWZR(
q!?T!g]c`!b]bOZ!W\Q][S!eWZZ!PS!VWUVS`!bVO\!",**&***!$".**&***!WT![O``WSR!TWZW\U!X]W\bZg%&!S\bS`!o'*'p ( ( ( ( ( ( ( 7
8 5ZMLQ\!NWZ!W\PMZ!LMXMVLMV\[&
q!?T!g]c`!b]bOZ!W\Q][S!eWZZ!PS!ZSaa!bVO\!"03&2*+!$"+*+&.*+!WT![O``WSR!TWZW\U!X]W\bZg%&!S\bS`!o+p!T]`!SOQV!SZWUWPZS!RS^S\RS\b(!
q!?T!g]c`!b]bOZ!W\Q][S!eWZZ!PS!T`][!"03&2*+!b]!"+1/&//*!$"+*+&.*+!b]!"--3&***!WT![O``WSR!TWZW\U!X]W\bZg%&!S\bS`!o+p!T]`!SdS`g!
be]!RS^S\RS\ba!!$T]`!SfO[^ZS&!o'*'p!T]`!]\S!RS^S\RS\b&!o+p!WT!g]c!VOdS!be]!]`!bV`SS!RS^S\RS\ba&!O\R!o,p!WT!g]c!VOdS!
T]c`!RS^S\RS\ba%(
q!?T!g]c`!b]bOZ!W\Q][S!eWZZ!PS!VWUVS`!bVO\!"+1/&//*!$"--3&***!WT![O``WSR!TWZW\U!X]W\bZg%&!S\bS`!o'*'p ( ( ( ( ( ( ( 8
9 B\PMZ!KZMLQ\[&!?T!g]c!VOdS!]bVS`!Q`SRWba&!aSS!L]`YaVSSb!+'0!]T!FcP(!/*/!O\R!S\bS`!bVS!O[]c\b!T`][!bVOb!e]`YaVSSb!VS`S ! ( ( 9
; 6RR!ZW\Sa!6!bV`]cUV!=!O\R!S\bS`!bVS!b]bOZ!VS`S! ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( !" ;
<]`!OQQc`OQg&!KWUXTM\M!ITT!_WZS[PMM\[!\PI\!IXXTa&
q!?T!g]c!^ZO\!b]!Q\MUQbM!]`!KTIQU!ILR][\UMV\[!\W!QVKWUM!O\R!eO\b!b]!`SRcQS!g]c`!eWbVV]ZRW\U&!]`!WT!g]c!VOdS! O! ZO`US! O[]c\b! ]T! \]\eOUS! W\Q][S! O\R! eO\b! b]! W\Q`SOaS! g]c`! eWbVV]ZRW\U&! aSS! bVS! 6ML]K\QWV[$!3LR][\UMV\[$!IVL!3LLQ\QWVIT!<VKWUM!GWZS[PMM\!PSZ]e(
q!?T!g]c!PI^M!UWZM!\PIV!WVM!RWJ!I\!I!\QUM!]`!O`S!UIZZQML!NQTQVO!RWQV\Ta!IVL!aW]!IVL!aW]Z![XW][M!JW\P!_WZS&!O\R!bVS!Q][PW\SR!SO`\W\Ua!T`][!OZZ! X]Pa!SfQSSR!"/,&***!$",.&***!WT![O``WSR!TWZW\U!X]W\bZg%&!aSS!bVS!F_W%7IZVMZ['@]T\QXTM!=WJ[!GWZS[PMM\!]\!^OUS!.!b]!Od]WR!VOdW\U!b]]!ZWbbZS!bOf!eWbVVSZR(
q!?T!VMQ\PMZ!]T!bVS!OP]dS!aWbcObW]\a!O^^ZWSa&![\WX!PMZM!O\R!S\bS`!bVS!\c[PS`!T`][!ZW\S!>!]\!ZW\S!/!]T!<]`[!L'.!OP]dS(
6ML]K\QWV[$!3LR][\UMV\[$!IVL!3LLQ\QWVIT!<VKWUM!GWZS[PMM\
AW\M2!KaS!bVWa!e]`YaVSSb!-,*3!WT!g]c!^ZO\!b]!WbS[WhS!RSRcQbW]\a&!QZOW[!QS`bOW\!ORXcab[S\ba!b]!W\Q][S&!]`!VOdS!O!ZO`US!O[]c\b!]T!\]\eOUS!W\Q][S(
)!!
;\bS`! O\! SabW[ObS! ]T! g]c`! ,*+2! WbS[WhSR! RSRcQbW]\a(! JVSaS! W\QZcRS! _cOZWTgW\U! V][S! []`bUOUS! W\bS`Sab&!QVO`WbOPZS!Q]\b`WPcbW]\a&!abObS!O\R!Z]QOZ!bOfSa!$c^!b]!"+*&***%&!O\R![SRWQOZ!Sf^S\aSa!W\!SfQSaa!]T!1(/#!]T!g]c`!W\Q][S(!ISS!FcP(!/*/!T]`!RSbOWZa! ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ) "
* ;\bS`4
",.&***!WT!g]cn`S![O``WSR!TWZW\U!X]W\bZg!]`!_cOZWTgW\U!eWR]e$S`%
"+2&***!WT!g]cn`S!VSOR!]T!V]caSV]ZR
"+,&***!WT!g]cn`S!aW\UZS!]`![O``WSR!TWZW\U!aS^O`ObSZg
!( ( ( ( ( ( ( ( ( ( ( * "
+ E]J\ZIK\!ZW\S!,!T`][!ZW\S!+(!?T!hS`]!]`!ZSaa&!S\bS`!o'*'p! ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( + "
,! ;\bS`!O\!SabW[ObS!]T!g]c`!,*+2!ORXcab[S\ba! b]! W\Q][S!O\R!O\g!ORRWbW]\OZ!abO\RO`R!RSRcQbW]\! T]`!OUS!]`!PZW\R\Saa!$aSS!FcP(!/*/!T]`!W\T]`[ObW]\!OP]cb!bVSaS!WbS[a% ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( , "
- 3LL!ZW\Sa!-!O\R!.!O\R!S\bS`!bVS!b]bOZ! ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( - "
. ;\bS`!O\!SabW[ObS!]T!g]c`!,*+2!\]\eOUS!W\Q][S!$acQV!Oa!RWdWRS\Ra!]`!W\bS`Sab% ( ( ( ( ( ( ( ( ( . "
/ E]J\ZIK\!ZW\S!0!T`][!ZW\S!/(!?T!hS`]&!S\bS`!o'*'p(!?T!ZSaa!bVO\!hS`]&!S\bS`!bVS!O[]c\b!W\!^O`S\bVSaSa! ( ( ( / "
0! 6Q^QLM!bVS!O[]c\b!]\!ZW\S!1!Pg!".&+/*!O\R!S\bS`!bVS!`SacZb!VS`S(!?T!O!\SUObWdS!O[]c\b&!S\bS`!W\!^O`S\bVSaSa(!9`]^!O\g!T`OQbW]\! ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( 0
1 ;\bS`!bVS!\c[PS`!T`][!bVS!CMZ[WVIT!3TTW_IVKM[!GWZS[PMM\$!ZW\S!>!OP]dS! ( ( ( ( ( ( ( ( ( ( 1
)(!
!
3LL!ZW\Sa!2!O\R!3!O\R!S\bS`!bVS!b]bOZ!VS`S(!?T!hS`]!]`!ZSaa&!S\bS`!o'*'p(!?T!g]c!^ZO\!b]!caS!bVS!F_W%7IZVMZ['
@]T\QXTM!=WJ[!GWZS[PMM\$!OZa]!S\bS`!bVWa!b]bOZ!]\!ZW\S!+&!^OUS!.(!EbVS`eWaS&![\WX!PMZM!O\R!S\bS`!bVWa!b]bOZ!]\!<]`[!L'.&!ZW\S!/&!^OUS!+! ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( )(

<]`[!L'.!$,*+2% FOUS!,!
F_W%7IZVMZ['@]T\QXTM!=WJ[!GWZS[PMM\
AW\M2!KaS!bVWa!e]`YaVSSb!-,*3!WT!bVS!W\ab`cQbW]\a!c\RS`!ZW\S!>!T`][!bVS!CMZ[WVIT!3TTW_IVKM[!GWZS[PMM\!RW`SQb!g]c!VS`S(
)! ;\bS`! bVS! \c[PS`! T`][! bVS! CMZ[WVIT! 3TTW_IVKM[! GWZS[PMM\$! ZW\S! >&! ^OUS! -! $]`&! WT! g]c! caSR! bVS!6ML]K\QWV[$!3LR][\UMV\[$!IVL!3LLQ\QWVIT!<VKWUM!GWZS[PMM\!]\!^OUS!-&!bVS!\c[PS`!T`][!ZW\S!+*!]T!bVOb!e]`YaVSSb%! ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( )
*! <W\R!bVS!\c[PS`!W\!FIJTM!)!PSZ]e!bVOb!O^^ZWSa!b]!bVS!?BG7EF!^OgW\U!X]P!O\R!S\bS`!Wb!VS`S(!;W_M^MZ$!WT!g]cn`S![O``WSR!TWZW\U!X]W\bZg!O\R!eOUSa!T`][!bVS!VWUVSab!^OgW\U!X]P!O`S!"1/&***!]`!ZSaa!O\R!bVS!Q][PW\SR!eOUSa!T]`!g]c!O\R!g]c`!a^]caS!O`S!"+*1&***!]`!ZSaa&!R]\nb!S\bS`![]`S!bVO\!o-p! ( ( ( ( ( ( ( ( ( ( ( ( ( *
+! ?T!ZW\S!+!Wa!UWZM!\PIV!WZ!MY]IT!\W!ZW\S!,&!acPb`OQb!ZW\S!,!T`][!ZW\S!+(!;\bS`!bVS!`SacZb!VS`S!$WT!hS`]&!S\bS`!o'*'p%!O\R!]\!<]`[!L'.&!ZW\S!/&!^OUS!+(!6W!VW\!caS!bVS!`Sab!]T!bVWa!e]`YaVSSb!( ( ( ( ( ( ( ( ( ( ( ( +
AW\M2!?T!ZW\S!+!Wa!TM[[!\PIV!ZW\S!,&!S\bS`!o'*'p!]\!<]`[!L'.&!ZW\S!/&!^OUS!+(!8][^ZSbS!ZW\Sa!.!bV`]cUV!3!PSZ]e!b]!TWUc`S!bVS!ORRWbW]\OZ!eWbVV]ZRW\U!O[]c\b!\SQSaaO`g!b]!Od]WR!O!gSO`'S\R!bOf!PWZZ(
, ;\bS`!bVS!\c[PS`!T`][!ZW\S!,!]T!bVWa!e]`YaVSSb! ( ( ( ( ( ( ( ( ( ( ( ,
- ;\bS`!bVS!\c[PS`!T`][!ZW\S!+!]T!bVWa!e]`YaVSSb! ( ( ( ( ( ( ( ( ( ( ( -
. E]J\ZIK\!ZW\S!/!T`][!ZW\S!.! ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( .
/ <W\R!bVS!O[]c\b!W\!FIJTM!*!PSZ]e!bVOb!O^^ZWSa!b]!bVS!;<9;7EF!^OgW\U!X]P!O\R!S\bS`!Wb!VS`S! ( ( ( ( ( / "
0 @]T\QXTa!ZW\S!1!Pg!ZW\S!0!O\R!S\bS`!bVS!`SacZb!VS`S(!JVWa!Wa!bVS!ORRWbW]\OZ!O\\cOZ!eWbVV]ZRW\U!\SSRSR! ( ( ( 0 "
1!
!
!
6Q^QLM!ZW\S!2!Pg!bVS!\c[PS`!]T!^Og!^S`W]Ra!`S[OW\W\U!W\!,*+2(!<]`!SfO[^ZS&!RWdWRS!Pg!+2!WT!g]cn`S!^OWR!SdS`g!
,! eSSYa!O\R!g]c!Q][^ZSbS! bVWa! T]`[! ]\!O! RObS! W\! ZObS!6^`WZ! eVS\! bVS`S! O`S! +2!^Og!^S`W]Ra! `S[OW\W\U! W\!
,*+2(!;\bS`!bVS!`SacZb!VS`S!O\R!]\!<]`[!L'.&! ZW\S!0&!^OUS!+(!JVWa! Wa!bVS!ORRWbW]\OZ!O[]c\b!b]!PS!eWbVVSZR!
T`][!SOQV!^OgQVSQY! ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( 1 "
FIJTM!)
@IZZQML!8QTQVO!=WQV\Ta
?T!eOUSa!T`][!?BG7EF!^OgW\U!X]P!O`Sr
;\bS`!]\!!ZW\S!,!OP]dS
!"*!!'!!!!"/&*** */&**+!!'!!!!!!3&/** +3&/*+!!'!!!!+3&*** ,
+3&**+!!'!!!!,0&/** -,0&/*+!!'!!!!-1&*** .-1&**+!!'!!!!.-&/** /.-&/*+!!'!!!!//&*** 0//&**+!!'!!!!0*&*** 10*&**+!!'!!!!1*&*** 21*&**+!!'!!!!1/&*** 31/&**+!!'!!!!2/&*** +*2/&**+!!'!!!!3/&*** ++3/&**+!!'!!+-*&*** +,
+-*&**+!!'!!+/*&*** +-+/*&**+!!'!!+0*&*** +.+0*&**+!!'!!+1*&*** +/+1*&**+!!'!!+2*&*** !!+0+2*&**+!!'!!+3*&*** +1+3*&**+!!'!!,**&*** +2,**&**+!O\R!]dS`!!!!!! +3
3TT!B\PMZ[
?T!eOUSa!T`][!?BG7EF!^OgW\U!X]P!O`Sr
;\bS`!]\!!ZW\S!,!OP]dS
"*!!'!!!!"1&*** *1&**+!!'!!!!+,&/** +
+,&/*+!!'!!!!,.&/** ,,.&/*+!!'!!!!-+&/** --+&/*+!!'!!!!-3&*** .-3&**+!!'!!!!//&*** ///&**+!!'!!!!1*&*** 01*&**+!!'!!!!2/&*** 12/&**+!!'!!!!3*&*** 23*&**+!!'!!+**&*** 3
+**&**+!!'!!+*/&*** +*+*/&**+!!'!!++/&*** ++++/&**+!!'!!+,*&*** +,+,*&**+!!'!!+-*&*** +-+-*&**+!!'!!+./&*** +.+./&**+!!'!!+//&*** +/+//&**+!!'!!+2/&*** +0+2/&**+!O\R!]dS` +1
FIJTM!*
@IZZQML!8QTQVO!=WQV\Ta
?T!eOUSa!T`][!;<9;7EF!^OgW\U!X]P!O`Sr
;\bS`!]\!!ZW\S!1!OP]dS
!"*!!' ",.&-1/ !!!!!!!!".,*,.&-10!!'!!!!2,&1,/ /**2,&1,0!!'!!+1*&-,/ 3+*
+1*&-,0!!'!!-,*&-,/ +&***-,*&-,0!!'!!.*/&-,/ +&--*.*/&-,0!!'!!0*/&-,/ +&./*0*/&-,0!O\R!]dS` +&/.*
3TT!B\PMZ[
?T!eOUSa!T`][!;<9;7EF!^OgW\U!X]P!O`Sr
;\bS`!]\!!ZW\S!1!OP]dS
"*!!' "1&*** ".,*1&**+!!'!!!!!-0&+1/ /**
-0&+10!!'!!!!13&31/ 3+*13&310!!'!!+/.&31/ +&***
+/.&310!!'!!+31&.1/ +&--*+31&.10!!'!!.31&.1/ +&./*.31&.10!O\R!]dS` +&/.*
CZQ^IKa!3K\!IVL!CIXMZ_WZS!DML]K\QWV!
3K\!AW\QKM&!LS!OaY!T]`!bVS!W\T]`[ObW]\!]\!bVWa!T]`[!b]!QO``g!]cb!bVS!?\bS`\OZ!HSdS\cS!ZOea!]T!bVS!K\WbSR!IbObSa(!?\bS`\OZ!HSdS\cS!8]RS!aSQbW]\a!-.*,$T%$,%!O\R!0+*3!O\R!bVSW`!`SUcZObW]\a!`S_cW`S!g]c!b]!^`]dWRS!bVWa!
W\T]`[ObW]\5!g]c`!S[^Z]gS`!caSa!Wb!b]!RSbS`[W\S!g]c`!TSRS`OZ!W\Q][S!bOf!eWbVV]ZRW\U(!<OWZc`S!b]!^`]dWRS!O!^`]^S`Zg!Q][^ZSbSR!T]`[!eWZZ!`SacZb!W\!g]c`!PSW\U!b`SObSR!Oa!O!aW\UZS!^S`a]\!eV]!QZOW[a!\]!eWbVV]ZRW\U!OZZ]eO\QSa5!^`]dWRW\U!T`OcRcZS\b!W\T]`[ObW]\![Og!acPXSQb!g]c!b]!^S\OZbWSa(!H]cbW\S!caSa!]T!bVWa!W\T]`[ObW]\!W\QZcRS!UWdW\U!Wb!b]!bVS!9S^O`b[S\b!]T!@cabWQS!T]`!QWdWZ!O\R!Q`W[W\OZ!ZWbWUObW]\5!b]!QWbWSa&!abObSa&!bVS!9Wab`WQb!]T!8]Zc[PWO&!O\R!
K(I(!Q][[]\eSOZbVa!O\R!^]aaSaaW]\a!T]`!caS!W\!OR[W\WabS`W\U!bVSW`!bOf!ZOea5!O\R!b]!bVS!9S^O`b[S\b!]T!>SOZbV!O\R!>c[O\!IS`dWQSa!T]`!caS!W\!bVS!DObW]\OZ!9W`SQb]`g!]T!DSe!>W`Sa(!LS![Og!OZa]!RWaQZ]aS!bVWa!
W\T]`[ObW]\!b]!]bVS`!Q]c\b`WSa!c\RS`!O!bOf!b`SObg&!b]!TSRS`OZ!O\R!abObS!OUS\QWSa!b]!
S\T]`QS!TSRS`OZ!\]\bOf!Q`W[W\OZ!ZOea&!]`!b]!TSRS`OZ!ZOe!S\T]`QS[S\b!O\R!W\bSZZWUS\QS!
OUS\QWSa!b]!Q][POb!bS``]`Wa[(
M]c!O`S\nb!`S_cW`SR!b]!^`]dWRS!bVS!W\T]`[ObW]\!`S_cSabSR!]\!O!T]`[!bVObna!acPXSQb!b]!bVS!FO^S`e]`Y!HSRcQbW]\!6Qb!c\ZSaa!bVS!T]`[!RWa^ZOga!O!dOZWR!EC7!Q]\b`]Z!\c[PS`(!7]]Ya!]`!`SQ]`Ra!`SZObW\U!b]!O!T]`[!]`!Wba!W\ab`cQbW]\a![cab!PS
`SbOW\SR!Oa!Z]\U!Oa!bVSW`!Q]\bS\ba![Og!PSQ][S![ObS`WOZ!W\!bVS!OR[W\Wab`ObW]\!]T!O\g!?\bS`\OZ!HSdS\cS!ZOe(!=S\S`OZZg&!bOf!`Sbc`\a!O\R!`Sbc`\!W\T]`[ObW]\!O`S!Q]\TWRS\bWOZ&!Oa!`S_cW`SR!Pg!8]RS!aSQbW]\!0+*-(!
JVS!OdS`OUS!bW[S!O\R!Sf^S\aSa!`S_cW`SR!b]!Q][^ZSbS!O\R!TWZS!bVWa!T]`[!eWZZ!dO`g!RS^S\RW\U!]\!W\RWdWRcOZ!QW`Qc[abO\QSa(!<]`!SabW[ObSR!OdS`OUSa&!aSS!bVS!W\ab`cQbW]\a!T]`!g]c`!W\Q][S!bOf!`Sbc`\(
?T!g]c!VOdS!acUUSabW]\a!T]`![OYW\U!bVWa!T]`[!aW[^ZS`&!eS!e]cZR!PS!VO^^g!b]!VSO`!T`][!g]c(!ISS!bVS!W\ab`cQbW]\a!T]`!g]c`!W\Q][S!bOf!`Sbc`\(

Revenue Form K-442A804 (11-13)
KENTUCKY DEPARTMENT OF REVENUEEMPLOYEE’S WITHHOLDING EXEMPTION CERTIFICATE Payroll No. __________________________
Print Full Name ________________________________________________________________________ Social Security No. ___________________________
Print Home Address ____________________________________________________________________________________________________________________
HOW TO CLAIM YOUR WITHHOLDING EXEMPTIONS
1. If SINGLE, and you claim an exemption, enter “1,” if you do not, enter “0” .............................................................. ________2. If MARRIED, one exemption each for you and spouse if not claimed on another certificate.
(a) If you claim both of these exemptions, enter “2” (b) If you claim one of these exemptions, enter “1” ................................................................................................ ________ (c) If you claim neither of these exemptions, enter “0”3. Exemptions for age and blindness (applicable only to you and your spouse but not to dependents): (a) If you or your spouse will be 65 years of age or older at the end of the year, and you claim this exemption, enter “4”; if both will be 65 or older, and you claim both of these exemptions, enter “8”.................................. ________ (b) If you or your spouse are blind, and you claim this exemption, enter “4”; if both are blind, and you claim both of these exemptions, enter “8” ......................................................................................................................... ________4. If you claim exemptions for one or more dependents, enter the number of such exemptions ................................ ________5. National Guard exemption (see instruction 1) ............................................................................................................... ________6. Exemptions for Excess Itemized Deductions (Form K-4A) ............................................................................................ ________
7. Add the number of exemptions which you have claimed above and enter the total .................................................8. Additional withholding per pay period under agreement with employer. See instruction 1 ..........................$ _____________
I certify that the number of withholding exemptions claimed on this certificate does not exceed the number to which I am entitled.
Date _________________________________ Signed___________________________________________________________________________________
}EMPLOYEE:
Failure to file this form with your employer will result in withholding tax deductions from your wages at the maximum rate.
EMPLOYER:
Keep this certificate with your records.
INSTRUCTIONS
1. NUMBER OF EXEMPTIONS—Do not claim more than the correct number of exemptions. However, if you have unusually large amounts of itemized deductions, you may claim additional exemptions to avoid excess withholding. You may also claim an additional exemption if you will be a member of the Kentucky National Guard at the end of the year. If you expect to owe more income tax for the year than will be withheld, you may increase the withholding by claiming a smaller number of exemptions or you may enter into an agreement with your employer to have additional amounts withheld. If you claim more than 10 exemptions this information is sent to the Department of Revenue. 2. CHANGES IN EXEMPTIONS—You may file a new certificate at any time if the number of your exemptions INCREASES. You must file a new certificate within 10 days if the number of exemptions previously claimed by you DECREASES for any of the following reasons. (a) You are divorced or legally separated from your spouse for whom you have been claiming an exemption or your spouse claims his or her own exemption on a separate certificate. (b) The support of a dependent for whom you claimed exemption is taken over by someone else, so that you no longer expect to furnish more than half the support for the year. (c) Your itemized deductions substantially decrease and a Form K-4A has previously been filed. OTHER DECREASES in exemption, such as the death of a spouse or a dependent, do not affect your withholding until the next year, but require the filing of a new certificate by December 1 of the year in which they occur.
3. DEPENDENTS—To qualify as your dependent (line 4 on reverse), a person (a) must receive more than one-half of his or her support from you for the year, and (b) must not be claimed as an exemption by such person’s spouse, and (c) must be a citizen of the United States, or a resident of the United States, Canada, or Mexico, or (d) must have lived with you for the entire year as a member of your household or be related to you as follows:• your child, stepchild, legally adopted child, foster child (if he lived in your
home as a member of the family for the entire year), grandchild, son-in-law, or daughter-in-law;
• your father, mother, or ancestor of either, stepfather, stepmother, father-in-law, or mother-in-law;
• your brother, sister, stepbrother, stepsister, brother-in-law, or sister-in-law;• your uncle, aunt, nephew, or niece (but only if related by blood). 4. PENALTIES—Penalties are imposed for willfully supplying false information or willful failure to supply information which would reduce the withholding exemption.
www.revenue.ky.gov
Revised 10-16
MED CENTER HEALTH
NEW HIRE
WARREN COUNTY TAX FORM
INSTRUCTIONS:
1. Print full name and employee number
2. Enter Home Address and Phone Numbers.
3. Indicate if you live in the Warren County School District
5. Sign, date and return to Human Resources.
The correct completion of this form is necessary to assure you that taxes are not withheld incorrectly from your wages. Please
complete the form carefully and check the appropriate box. If you are unsure of your school district, please request assistance
from Human Resources or Payroll.
Questions may be directed to: FINANCE DIRECTOR
P.O. BOX 90019
BOWLING GREEN, KY 42102-9019
270-842-7168
If you change your place of residence during the year, it is very important to complete a change of address form.
PRINTED EMPLOYEE NAME SOCIAL SECURITY NUMBER
HOME ADDRESS
CITY STATE ZIP
COUNTY HOME PHONE CELL PHONE
PLEASE MAKE A CHECK BY THE CORRECT STATEMENT BELOW.
I certify that I DO live in the Warren County School District.
I certify that I DO NOT live in the Warren County School District.
I hereby authorize Med Center Health to withhold or not withhold applicable county taxes from my
earnings as indicated below.
I declare that I have examined this certificate and to the best of my knowledge, it is true and
complete.
EMPLOYEE SIGNATURE DATE
Rev. 10-16
This Agreement between Med Center Health and the undersigned supersedes all previous confidentiality statements and agreements, if
any, between Med Center Health and the undersigned relating to release of confidential information.
I acknowledge that I have read Med Center Health’s Confidentiality Policy and Procedure. I understand and agree to hold myself
responsible for the observance of this policy and any departmental policies and procedures pertaining to the right to privacy and the
release of confidential information.
I will not disclose or discuss any Confidential Information
with others, including friends or family, who do not have a
need to know it. In addition, I understand that my personal
access code, user ID(s), and password(s) used to access
computer systems are also an integral aspect of this
Confidential Information.
I will not access or view any Confidential Information other
than what is required to do my job.
I will not discuss Confidential Information where others can
overhear the conversation (for example, in hallways, on
elevators, in the cafeteria, on the shuttle bus, on public
transportation, at restaurants, and at social events). It is not
acceptable to discuss Confidential Information in public areas
even if a patient’s name is not used. Such a discussion may
raise doubts among patients and visitors about our respect for
their privacy.
I will not make inquiries about Confidential Information for
other Personnel who do not have proper authorization to
access such Confidential Information.
I will not make any unauthorized transmissions, inquiries,
modifications, or purgings of Confidential Information in Med
Center Health’s computer system. Such unauthorized
transmissions include, but are not limited to, removing and/or
transferring Confidential Information from Med Center
Health’s computer system unauthorized locations (for
instance, home).
I will log off any computer or terminal prior to leaving it
unattended.
I will comply with any security or Confidentiality policy
promulgated by Med Center Health to protect the security and
privacy of Confidential Information.
I will immediately report to my supervisor any activity, by any
person, including myself, that is a violation of this Agreement
or of any Med Center Health information security or
Confidential policy.
Upon termination of my employment I will immediately
return any documents or other medical containing Confidential
Information to Med Center Health.
I agree that my obligations under this Agreement will continue
after the termination of my employment.
I understand that violation of this Agreement may result in
corrective actions, including termination of employment
and/or suspension and loss of privileges, in accordance with
Med Center Health Confidentiality Policy, as well as legal
liability.
I further understand that all computer access activity is subject
to audit.
By signing this CONFIDENTIALITY STATEMENT AND AGREEMENT, I agree to comply with COMMONWEALTH
HEALTH CORPORATION’s policies and procedures regarding confidentiality and I also understand that any violations, even
inadvertently, may result in termination of my association with COMMONWEALTH HEALTH CORPORATION and/or in legal
action. The terms of this agreement shall survive any separation or termination of employment or affiliation.
IN TESTIMONY WHEREOF, I affix my signature,
EMPLOYEE/ASSOCIATE SIGNATURE DATE
For HR use only:
[ ] EMPLOYEE [ ] CONTRACT [ ] TEMPORARY [ ] INTERN [ ] VOLUNTEER [ ] STUDENT
PRINTED EMPLOYEE/ASSOCIATE NAME EMPLOYEE NUMBER (if known)
MED CENTER HEALTH
CONFIDENTIALITY STATEMENT AND AGREEMENT