policies, procedures, guidelines and protocols · policies, procedures, guidelines and protocols...
TRANSCRIPT

Policies, Procedures, Guidelines and Protocols
Document Details
Title Guidelines for Pressure Ulcer Prevention and Management
Trust Ref No 969-31643
Local Ref (optional) Guidelines for Pressure Ulcer Prevention and Management V 3
Main points the document covers
Guidance on preventing and managing pressure ulceration. The guidelines will support the delivery of safe and effective care.
Who is the document aimed at? All healthcare professionals in contact with patients
Author Joy Tickle Tissue Viability Specialist
Approval process
Approved by (Committee/Director)
Clinical Policies Group
Approval Date 18/4/16
Initial Equality Impact Screening No
Full Equality Impact Assessment
No
Lead Director Director of Nursing and Quality
Category Clinical
Sub Category Policies relevant to all services
Review date 18/4/19
Distribution
Who the policy will be distributed to
Directors, Divisional Managers, Service Leads for dissemination to relevant staff within their areas
Method Publishing to the Trust Website, team meetings/briefings
Document Links
Required by CQC
Required by NHSLA
Other
Amendments History
No Date Amendment
1 Additional guidance incorporated covering the wider topic of pressure ulcer prevention and management including revised patient leaflet.
2
3
4
5
Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 1 April 2016
Contents
1. Introduction 2
2. Purpose 2
2.1 Accountability 2
3. Definitions 2
3.1 A Pressure Ulcer 2
3.2 Pressure 3
3.3 Shearing 3
3.4 Glossary 3
4. Duties 3
4.1 The Board of Directors 3
4.2 The Chief Executive 3
4.3 The Director of Nursing 3
4.4 Clinical Service manager and Professional Leads 4
4.5 Tissue Viability Service 4
4.6 All Staff 5
5. Pressure Ulcer Prevention and Management – Risk Assessment: Goals 5
5.1 Identifying at Risk Individuals 5
5.2 Risk Assessment 5
5.3 Waterlow Risk Assessment and Skin Assessment 5
5.4 Waterlow 6
5.5 Waterlow Assessment Tool 6
5.6 Preventative Care Plan 6
5.7 SSKIN Assessment 6
5.7.1 Patient Assessment 6
5.7.2 Nutritional Assessment and Management 6
5.8 Pain Assessment 7
5.9 Moving and Handling Techniques 7
5.10 Repositioning 7
5.11 Transportation 7
5.12 Pressure Ulcer Assessment 7
5.13 Ungradable Pressure Ulcers 8
5.14 Wound Assessment and Management 8
5.15 Reporting of Pressure Ulceration 8
5.16 Action against Advice 8
6. Consultation 8
7. Dissemination and Implementation 9
8. Monitoring Compliance 9
9. References 9
10. Associated Documents 10
11. Appendices 10

Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 2 April 2016
1 Introduction
Shropshire Community Health NHS Trust (SCHT) has a responsibility to make every effort to prevent patients developing pressure ulcers and associated conditions whilst in their care. In addition, the Trust has the responsibility to ensure that there are systemic measures in place to prevent the development of pressure ulcers and associated conditions and to assess and manage them if they should occur. The implications for patients who develop pressure ulcers are devastating in terms of the impact upon their health and social well-being. The cost to the Trust can be significant, in terms of treatment pressure ulcers cost the NHS over 3 million pounds a year with extended hospital stays and treatment. (NHS Midlands and East 2012).
2 Purpose
It is the overall purpose of this guideline to reduce the occurrence of pressure ulcers, but should they occur then they should be treated using the most up to date evidence based practice and treatment methods. This guideline aims to provide health professionals across Shropshire Community Health Economy with knowledge to inform and support their actions and decision-making ensuring they can provide the most effective preventative and/or treatment strategy.
This guideline is intended as a brief overview and should be read in conjunction with more detailed guidance from (NPUAP, EPUAP, 2014) and (NICE, 2014).
2.1 All healthcare professionals are accountable for their clinical practice. Managers are accountable for ensuring that they are aware of the extent of pressure ulcers within their area and for providing opportunity for appropriate support, education and training for staff. This policy recognises the need for a multidisciplinary approach and the provision of holistic care, which will lead to a reduction of the incidence of pressure ulcers within the county and more effective management of patients with pressure damage, ensuring safe and appropriate use of pressure relieving equipment.
3 Definitions
3.1 A pressure ulcer is a localized injury to the skin and/or underlying tissue usually over a bony prominence, as a result of pressure, or pressure in combination with shear (National Pressure Ulcer Advisory Panel (NPUAP), European Pressure Ulcer Advisory Panel (EUPAP), 2014). Most pressure ulcers are preventable if: the circumstances likely to result in an ulcer and those at risk are identified early, if appropriate preventative measures are implemented without delay. However, it is recognised that with recent improvements in reporting and investigation there are increasing incidence of pressure ulcers that are considered unavoidable (EPUAP 2014).
Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 3 April 2016
3.2 Pressure: Pressure occurs when soft tissue over a bony prominence is compressed between a hard surface and the bone causing pressure greater than the capillary pressure, resulting in localised ischemia.
3.3 Shearing: Shearing forces may occur when a patient slides down the bed. This action produces the destruction of the micro circulation by thrombosis of the vessels, particularly if the heels are dragged on the bed whilst being manoeuvred up the bed (Waterlow 2009). In the elderly, shearing can also contribute to epidermis and dermis separation, usually seen as blistering.
3.4 Glossary:
DTI Deep Tissue Injury
EPUAP European Pressure Ulcer Advisory Panel
NPUAP National Pressure Ulcer Advisory Panel
RCA Root Cause Analysis
S/DTI Serious Deep Tissue Injury
SCHT Shropshire Community Health Trust
SEO Specialist Equpiment Order Form
SI Serious Incident
SSKIN Skin, Surface, Keep Moving, Incontinence, Nutrition
TVS Tissue Viability Service
4 Duties
4.1 The Board of Directors are responsible for determining the governance arrangements of the Trust including effective risk management processes. It is responsible for ensuring that the necessary clinical policies, procedures and guidelines are in place to safeguard patients and reduce risk. In addition they will require assurance that clinical policies, procedures and guidelines are being implemented and monitored for effectiveness and compliance.
4.2 The Chief Executive has overall responsibility for patient safety and ensuring that there are effective risk management processes within the Trust which meet all statutory requirements and adhere to guidance issued by the Department of Health. The CEO holds each line manager accountable for meeting objectives and to work together towards meeting the objectives approved by the Board.
4.3 The Director of Nursing is the Executive with delegated responsibility for implementation of Governance arrangements within the Trust. The Director of Nursing and the Medical Director are responsible for overseeing the implementation of this document.

Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 4 April 2016
4.4 Clinical Service Managers and Professional Leads will, for their areas of responsibility, so far as is reasonably practical, ensure that this document is implemented by ensuring that:
This document is made available to all staff within their department, and that their staff comply.
There is adequate provision of suitable staffing levels, working conditions and environments.
Each team will have a registered nurse to act as a link nurse/champion for tissue viability to disseminate updates in care and be a link for their area to/from the Tissue Viability Service (TVS).
That their staff are properly informed and trained by ensuring that staff are released for training in undertaking skin assessment and risk assessment and complete the on line training package.
They lead the root cause analysis (RCA investigations of any pressure ulcers reported as a Serious Incident in their area and report the outcome of these at the appropriate forums).
They complete the investigation within 10 working days to comply with timeframes of reporting.
Representation from their areas of responsibility will be identified when an investigation of a Pressure Ulcer SI, using the RCA technique, is being held and presented at the appropriate forums.
Action plans and risk reduction measures resulting from the investigation of incidents and serious incidents are developed and implemented to prevent reoccurrence of SIs and there is feedback to their teams of the actions taken in response to investigations.
Action plans are monitored until all actions are completed and that the Patient Safety Manager and the Tissue Viability Service are kept informed of progress being made to ensure that Trust’s Risk Management System, the Strategic Executive Information System (STEIS) and the Serious Incident reporting system (SORD) system for the Commissioners are completed in a timely manner.
4.5 Tissue Viability Service
Are responsible so far as is reasonably practical for: Ensuring that this document reflects National and Commissioner’s Guidance, and is disseminated throughout the Trust.
Advising on the equipment used in the prevention and treatment of pressure ulcers ensuring it is appropriate and meets the needs of the patient.
Overseeing the RCA investigations of pressure ulcers reported as a SI to identify trends and report the outcome of these at the appropriate forums.
Maintaining the tissue viability database and provide and present reports as required.
Verifying all reported pressure ulcers, SI Grade 3 and 4 pressure ulcers, and complete tissue viability section of Datix.
Attend RCA challenge meetings to discuss all Grade 3 and 4 pressure ulcer incidents and jointly decide with the groups whether they are avoidable or unavoidable to health and what the level of harm to the trust will be.
Notifying the Professional leads via Datix to complete RCA on all verified Grade 3 and 4 pressure ulcers SI.
Monitor the Suspected Deep Tissue Injury (S/DTI) and make a decision and report on Datix re its status after two weeks or earlier (i.e. if an open ulcer Grade 3 or 4 or if still an S/TDI then it remains as an S/TDI).
Monitor alongside the managers and the governance team the level of harm for each pressure ulcer incident on Datix.

Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 5 April 2016
4.6 All Staff
All staff have a responsibility to ensure that they develop and maintain their knowledge and skills to undertake the duties and responsibilities for their post.
Healthcare professionals are responsible for ensuring that their practice and that of untrained staff they supervise comply with this document and that they receive appropriate training and support.
All staff are responsible for reporting all pressure ulcers Grade 2 and above as a serious incident (SI) within 24hrs of discovery on the electronic incident reporting system: DATIX and decide the level of harm to the trust, and that the Incident Management Policy including the Management of Serious Incidents is followed.
Duty of Candour: The regulatory Duty of Candour came into force in November 2014 as part of the Health and Social Care Regulations. This requires a verbal and written notification of the harm and circumstances where a patient suffers moderate, severe harm or death as a result of the care delivered. These notifications should be given to the patient or their representative where appropriate. The notification must include an apology. Moderate harm is defined as harm requiring a moderate increase in treatment. All pressure ulcers (Grade 2 and above) will require additional treatment, so the Duty of Candour will apply if the care delivered contributed to the development of the ulcer. In many instances an ulcer may develop, and it is not clear if this was due to the care, or other circumstances. In this instance the verbal notification should be given, and a decision made relating to the written notification once the circumstances have been investigated. It is a requirement that compliance with the duty should be recorded. This record should be kept using the incident form. Further details can be found: http://www.shropscommunityhealth.nhs.uk/rte.asp?id=10653&task=View&itemid=103
5 Pressure Ulcer Prevention and Management
Risk Assessment: Goals
5.1 To identify at risk individuals prevention and the specific factors placing them at risk. The EPUAP believes that there a number of issues associated with risk assessment tools. Risk assessment should be used as an adjunct to clinical judgement and not as a tool in isolation from other clinical features.
5.2 Risk Assessment: There should be clarification of a full risk assessment in patients to include general medical condition, skin assessment, mobility, moistness, incontinence, nutrition and pain. All strategies related to pressure damage should always be based on the best available evidence. Assessment of risk should be more than just the use of an appropriate risk assessment tool and should not lead to a prospective and inflexible approach to patient care.
5.3 All patients on admission to a caseload must have a Waterlow risk assessment (see appendix 1) and a full body skin assessment (see appendix 2) at their first visit or within 6 hours of admission to a community hospital and any tissue damage must be documented in the skin assessment section of the nursing care plan documentation. Whilst risk assessment should be performed immediately on entry into an episode of care this assessment may take time to fully complete if information is not readily available. Assessment should also be on-going and frequency of re-assessment should be dependent
Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 6 April 2016
on change in the patient’s condition within the environment. It is recommended to use a risk assessment tool as an aid of memoir, (NICE 2014).
5.4 The Waterlow pressure ulcer risk assessment scoring system has been shown to be the most frequently used system used in the UK. It must be made very clear that like all simplistic scoring systems it cannot scientifically predict with 100% accuracy the chance of a patient developing a pressure ulcer. What it can do, is ensure that all patients are assessed objectively to the same system and thereby placed in a priority order for preventative aids. It also provides evidence to manage the need to purchase equipment. The Waterlow assessment is another tool in the armoury of nurses, but it is not a replacement for their knowledge and their skills (Waterlow 2009).
5.5 A Waterlow assessment tool (see Appendix 1) must be used to assess the patient and the Waterlow score must be calculated and documented within the patient’s hand held notes. However, it is acknowledged that the Waterlow score must be used in conjunction with clinical judgement and when the patient’s condition changes and not in isolation. Patients who are identified as being at risk of developing pressure ulcers must have a multidisciplinary plan of care detailing interventions required, implemented and evaluated, in accordance with the National Institute of Health and Clinical Excellence clinical guidelines. The assessment of the patients risk, utilising the Waterlow score and practitioners clinical judgement must be undertaken no less than weekly throughout the episode of care and documented in the patient’s multidisciplinary notes. Additional assessments documenting both the Waterlow score and the practitioner’s clinical judgement must also be undertaken when changes in the patient’s medical condition or environment occur.
5.6 A preventative care plan for all patients assessed as at risk of developing pressure ulcers must be implemented, this should involve the patient and relative/carers, and must include a repositioning schedule. The Skin, Surface, Keep moving, Incontinence, Nutrition (SSKIN) care bundle should be implemented to monitor for early signs of tissue damage and verbal and written information provided to patients, relatives and carers. SSKIN care bundle can be found here: http://www.shropscommunityhealth.nhs.uk/content/doclib/10790.pdf http://www.shropscommunityhealth.nhs.uk/content/doclib/10791.pdf
5.7 SSKIN Assessment: To maintain and improve tissue tolerance to pressure in order to prevent injury. Skin condition should be inspected and documented daily and any changes should be recorded as soon as they are observed. Inspection must be documented. Initial skin assessment should take into account the following bony prominences: - sacrum, heels, hips, ankles, elbows, occiput, to identify early stages of pressure damage. Identify the condition of skin, dryness, cracking, erythema, maceration, fragility, heat and induration.
5.7.1 Patient assessment: History and physical examination should be undertaken alongside the assessment of the patient’s pressure ulcer. Patients overall physical and psycho-social health will affect the management and prevention of pressure ulcers.
5.7.2 Nutritional Assessment and Management: Ensure adequate dietary intake to prevent malnutrition to the extent that this is compatible with the individual’s wishes or condition. It is important that a full nutritional assessment be carried out for any patients who are at risk of developing a pressure ulcer. The assessment must consider general nutritional appearance, clinical condition, patient’s weight, height and percentage weight loss, usual and current dietary intake and any areas of concerns such as low levels of albumin, total protein or haemoglobin. If there are considerable nutritional concerns then discussions should be made with dieticians, GPs and the Tissue Viability Service. It has been cited that protein calorie malnutrition is a major factor in the development of pressure ulcers because it reduces the body’s ability to heal and repair itself (King 2003). Many elderly people, especially those who live alone or those with disabilities, may be malnourished. They are often deficit of minerals and vitamins in addition to being protein deficit (King 2003).
Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 7 April 2016
Nutritional supplements should be considered in order to improve their status and assist in the healing of pressure ulcers. A nationally recognised nutritional assessment tool is the ‘MUST’ assessment tool and this will incorporate the body mass index assessment and is recommended by SCHT, (BAPEN 2003). Hydration assessment, dehydration should be avoided in order to maintain an adequate circulating blood volume and good skin and tissue perfusion.
5.8 Pain Assessment: Assess all patients for pain related to the pressure ulcer, for its treatment and document. Manage pain by eliminating or controlling the source of pain (e.g. covering wounds, adjusting support services, repositioning), provide medication or other methods of pain relief as needed and appropriate. Seek specialist advice if necessary, use appropriate wound assessment tool to document and evaluate patient’s pain and treatments.
5.9 Moving and Handling Techniques: In all care settings individuals considered to be at risk of developing pressure ulcers should have a personalised written prevention plan which will include a pressure redistributing device. Benefit may be derived from a variety of pressure ulcer prevention devices. Please consult with the SCHT Community Equipment Service for further advice regarding pressure relieving equipment; Community Equipment Services, Unit D6, Hortonwood 7, Hortonwood, Telford, TF1 7GP. Tel; 01952 603838 email; [email protected]
5.10 Skin injury due to friction and shear forces should be minimised through correct positioning, transferring and repositioning techniques. Skin must be protected against the adverse effects of external mechanical forces, pressure, friction and shear. Any individual who is assessed to be at risk of developing pressure ulcers should be repositioned if it is medically safe to do so. Frequency of repositioning should be consistent with overall goals. Documentation to record repositioning should be consistently completed, (see appendix 4). As the patient’s condition improves, then the potential for improving mobility and activity status exist, rehabilitation efforts may be initiated, if consistent with the overall goals of therapy. Maintaining activity levels, mobility and range of movement is an appropriate goal for most individuals. All interventions and outcomes should be monitored and documented. Whenever possible avoid positioning patients directly on a pressure ulcer or directly on a bony prominence unless this is contra-indicated by their general treatment objectives, in which instance an adequate pressure relieving device (e.g. an alternating pressure device) should be implemented. Patients at risk of developing pressure ulcers because of the time spent sitting in a chair should be allocated a chair of the correct height in addition to a pressure relieving device (see appendices 5, 6 and 7). The period of time should be defined in the individual care plan but generally will not be more than two hours. Individuals, where appropriate, should be encouraged to reposition themselves if this is possible. Individuals at risk of pressure ulcers who are likely to spend substantial periods of time in a chair or wheelchair should generally be provided with a pressure redistributing device. Individuals who are able should be taught to redistribute weight every fifteen minutes. Periods spent immobile in chairs should be limited to 2 hours or less per session unless their clinical condition prevents doing so.
5.11 Transportation: Pressure ulcer prevention will include time spent in transit or time spent at appointments or during social activities. If a patient is at risk and has been advised to use a pressure reducing/relieving device then advice should be given to the patient about what to use during these times. Check if pressure reducing/relieving devices are available for patient appointments and/or seek advice from the SCHT Community Equipment Service. Patients must ensure that vehicle insurance companies are aware of any equipment being used during transportation, such as cushions.
5.12 Pressure ulcer assessment: Assess the pressure ulcer recording location, grade, size, wound bed, exudate, pain and status of surrounding skin. Care should be taken to identify undermining and sinus formation. All patients with wounds should have a Shropshire

Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 8 April 2016
Wound Care Assessment, completed by all clinical staff (see appendix 2). All pressure ulcers should be reassessed daily if the condition of the patient or if the wound deteriorates and re-evaluation of the treatment plan should be initiated.
5.13 Ungradable pressure ulcers: this is where the actual depth of the ulcer is completely obscured by slough (yellow, tan, grey, green, brown, and black, Eschar) in the wound bed (see appendix 3). Until enough slough is removed to expose the base of the wound, the true depth cannot be determined; Suspected Deep Tissue Injury S/DTI should be reported in the usual way through Datix. TVS will then decide the grade following wound debridement (normally after 2 weeks) when the ulcer depth can be established and the pressure ulcer accurately graded. NB: Pressure ulcers should not be reverse graded. When healing they should be documented as healing and the original grade.
5.14 Wound Assessment and management: All pressure ulcers should be assessed utilizing Shropshire’s wound care assessment form. The wounds should be assessed at each dressing change (see appendix 2). All pressure ulcers must be photographed in accordance with Shropshire’s Wound Photography Guideline (2016) http://www.shropscommunityhealth.nhs.uk/content/doclib/10640.pdf and an evidence based management plan implemented utilising the guidance within Shropshire’s wound care formulary (2016). www.telfordccg.nhs.uk/download.cfm?doc=docm93jijm4n9528 .
5.15 Reporting of pressure ulceration: All pressure ulcers grade 2 and above must be datix reported using the appropriate datix reporting form. All grade 3 and 4 pressure ulcers should be reported as a serious incident as per trust policy and procedure. All grade 3 and 4 pressure ulcers developed in an independent care home setting must be reported to the Care Quality Commission. Any pressure ulcer deterioration must also be reported via DATIX.
5.16 Action against Advice: Where healthcare professionals are unable to implement a plan of care due to service user non-concordance for whatever reason, this must be clearly documented. All attempts to mitigate potential risk, alternative/reduced strategies, encouragement, supervision, assistance, reassurance, support, education and on-going assessment must be documented. Non-concordance must be escalated to ward manager/matron/team leader.
6 Consultation
In the development of this guidance the following have been included in the consultation process:
Stephen Gregory, Director Nursing and Quality;
Catherine Ball, Tissue Viability Nurse;
George English, Clinical Lead for Community Nursing;
Claire Wheeler, Community Practice Teacher. Infection Prevention and Control Team
Carol Bayley, Community Equipment Service Manager
Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 9 April 2016
7 Dissemination and Implementation: These guidelines will be disseminated to all relevant clinical teams by:
a) Managers Informed via DATIX system who then confirm they have disseminated to staff as appropriate
b) Staff via Team Brief
c) Via Tissue Viability Link Nurses
d) Published to the staff zone of the trust website
e) Training and raising awareness will be included as part of the Wound Assessment and Management Study Seminars delivered by the Tissue Viability Service.
8 Monitoring Compliance
Tissue Viability Clinical Lead and team leaders will monitor compliance of these guidelines by:
a) Clinical audits, including clinical record keeping audit and wound care audit.
b) Responding to any incidences reported on the Trust incident reporting system and ensuring appropriate lessons learnt are identified and action plans implemented and completed.
c) Monitor feedback from clinical staff and that any concerns raised are addressed.
d) The Tissue Viability Service will provide a range of training and educational opportunities for all health care professionals.
All clinical healthcare staff must attend mandatory training on pressure ulcer prevention and management every 3 years, as changes are occurring within this speciality as a result of on-going research. This mandatory training will underpin the implementation of the policy.
9 References
European Pressure Ulcer Advisory Panel (2014) Pressure Ulcer Treatment Guidelines http://www.epuap.org/wp-content/uploads/2010/10/Quick-Reference-Guide-DIGITAL-NPUAP-EPUAP-PPPIA-16Oct2014.pdf
National Institute for Clinical Excellence (2014) The Prevention and treatment of Pressure Ulcers, London, NICE.
Pressure Ulcer grading chart NHS Midlands and East 2012 adapted from EPUAP/NPUAP (2009) European Pressure Ulcer Advisory Panel (2009) Pressure Ulcer Treatment Guidelines http://www.epuap.org/guidelines/Final_Quick_Treatment.pdf
Shropshire Tissue Viability Group (2016) Wound Management Formulary.
Waterlow J (2009) Pressure Ulcer Prevention http://www.judy-waterlow.co.uk/index.htm
King C L, Elia M, Stroud M A, Stratton R J. The Predicted Validity of The Malnutrition Universal Screening Tool (MUST) With Regard to Mortality and Length of Stay in Elderly Patients. Clinical Nutrition (2003) No 22
The British Association or Parenteral and Enteral Nutrition (2003) The MUST Explanatory Booklet BAPEN (2003)

Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 10 April 2016
10 Associated Documents
The following Trust policies should be read in conjunction with these guidelines:
Consent to Examination or Treatment Policy
Confidentiality Code of Practice
Information Security Policy
Incident Reporting Policy
Data Protection Policy
Records Management Policy
Clinical Record Keeping Policy
Pan West Midlands Policy and procedure for safeguarding adults NHS Number Retrieval, Verification and Use Procedure
SSKIN Booklet (Surface, Skin, Keep Moving, Incontinence, Nutrition)
http://www.shropscommunityhealth.nhs.uk/content/doclib/10790.pdf and http://www.shropscommunityhealth.nhs.uk/content/doclib/10791.pdf
These policies can be found in the Policy section of the Trust’s website: http://www.shropscommunityhealth.nhs.uk/rte.asp?id=10667
11 Appendices
Appendix 1 Waterlow risk assessment tool
Appendix 2 Wound assessment chart
Appendix 3 The EPUAP Guide to Pressure Ulcer Grading
Appendix 4 Repositioning Chart
Appendix 5 Flow chart to assist in the appropriate prescription of pressure reducing/relieving cushions for armchairs
Appendix 6 Flow chart to assist in the appropriate prescription of dynamic pressure relieving mattresses
Appendix 7 Flow chart to assist in the appropriate prescription of static pressure reducing mattresses
Appendix 8 Specialist Equipment Order Form

Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 11 April 2016
Appendix 1 Waterlow Risk Assessment Tool
Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 12 April 2016
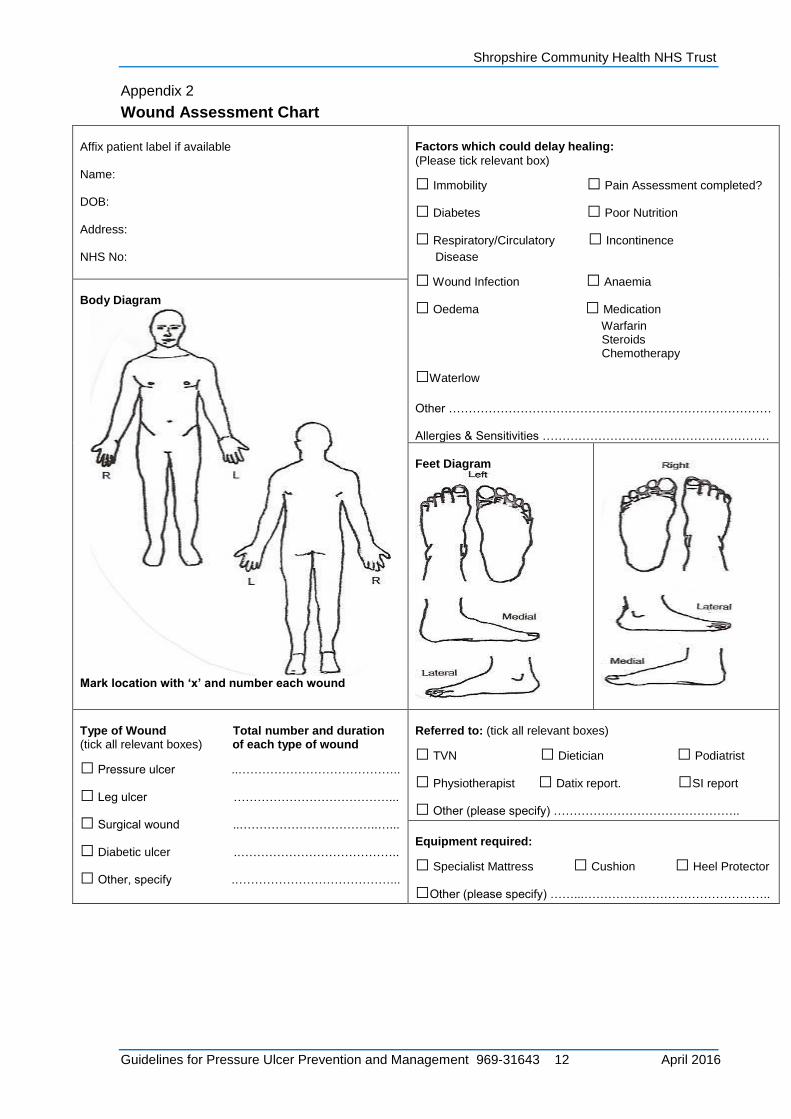
Appendix 2
Wound Assessment Chart
Affix patient label if available Name: DOB: Address: NHS No:
Factors which could delay healing:
(Please tick relevant box)
□ Immobility □ Pain Assessment completed?
□ Diabetes □ Poor Nutrition
□ Respiratory/Circulatory □ Incontinence
Disease
□ Wound Infection □ Anaemia
□ Oedema □ Medication
Warfarin Steroids Chemotherapy
□Waterlow
Other ……………………………………………………………………… Allergies & Sensitivities …………………………………………………
Body Diagram
Mark location with ‘x’ and number each wound
Feet Diagram
Type of Wound Total number and duration (tick all relevant boxes) of each type of wound
□ Pressure ulcer ..…………………………………..
□ Leg ulcer …………………………………...
□ Surgical wound ..……………………………..…...
□ Diabetic ulcer .…………………………………..
□ Other, specify .…………………………………...
Referred to: (tick all relevant boxes)
□ TVN □ Dietician □ Podiatrist
□ Physiotherapist □ Datix report. □SI report
□ Other (please specify) ………………………………………..
Equipment required:
□ Specialist Mattress □ Cushion □ Heel Protector
□Other (please specify) ……...………………………………………..
Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 13 April 2016
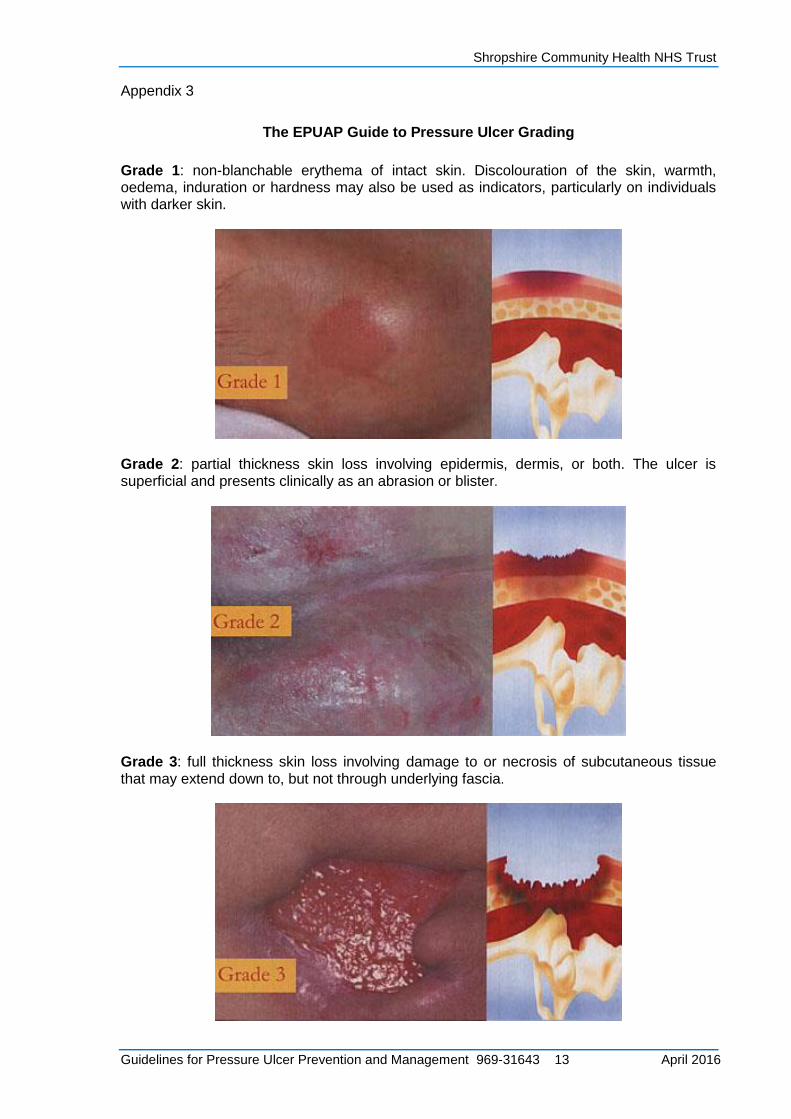
Appendix 3
The EPUAP Guide to Pressure Ulcer Grading
Grade 1: non-blanchable erythema of intact skin. Discolouration of the skin, warmth, oedema, induration or hardness may also be used as indicators, particularly on individuals with darker skin.
Grade 2: partial thickness skin loss involving epidermis, dermis, or both. The ulcer is superficial and presents clinically as an abrasion or blister.
Grade 3: full thickness skin loss involving damage to or necrosis of subcutaneous tissue that may extend down to, but not through underlying fascia.
Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 14 April 2016
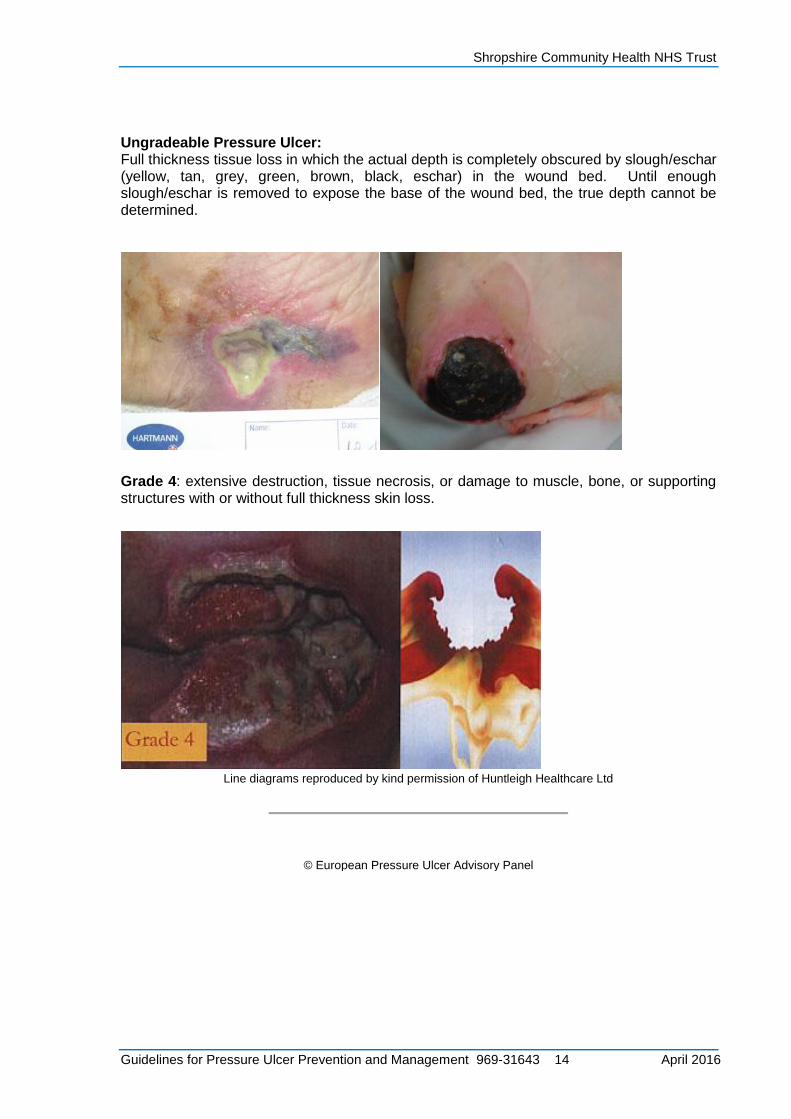
Ungradeable Pressure Ulcer: Full thickness tissue loss in which the actual depth is completely obscured by slough/eschar (yellow, tan, grey, green, brown, black, eschar) in the wound bed. Until enough slough/eschar is removed to expose the base of the wound bed, the true depth cannot be determined.
Grade 4: extensive destruction, tissue necrosis, or damage to muscle, bone, or supporting structures with or without full thickness skin loss.
Line diagrams reproduced by kind permission of Huntleigh Healthcare Ltd
© European Pressure Ulcer Advisory Panel
Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 15 April 2016
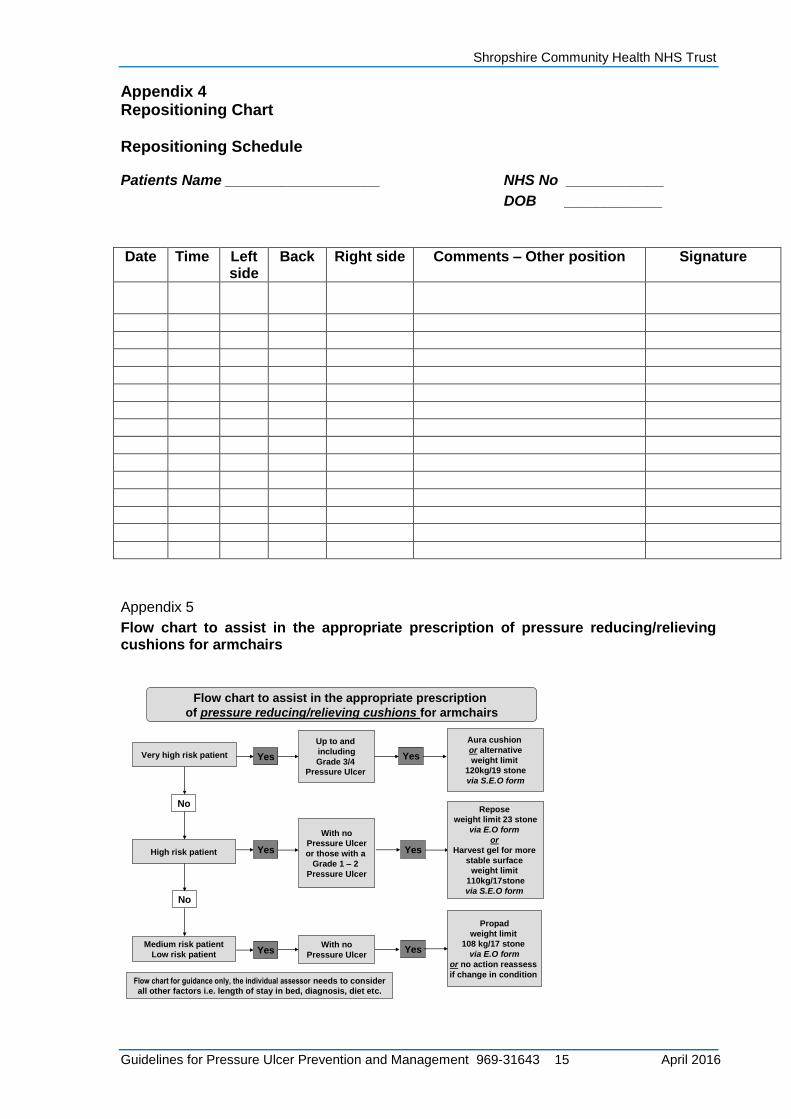
Appendix 4 Repositioning Chart Repositioning Schedule
Patients Name ___________________ NHS No ____________
DOB ____________
Date Time Left
side Back Right side Comments – Other position Signature
Appendix 5
Flow chart to assist in the appropriate prescription of pressure reducing/relieving cushions for armchairs
Flow chart to assist in the appropriate prescription
of pressure reducing/relieving cushions for armchairs
High risk patient
Medium risk patient
Low risk patient
Very high risk patient
No
No
Yes
Yes
YesWith no
Pressure Ulcer
Propad
weight limit
108 kg/17 stone
via E.O form
or no action reassess
if change in condition
Yes
With no
Pressure Ulcer
or those with a
Grade 1 – 2
Pressure Ulcer
Yes
Repose
weight limit 23 stone
via E.O form
or
Harvest gel for more
stable surface
weight limit
110kg/17stone
via S.E.O form
Up to and
including
Grade 3/4
Pressure Ulcer
Yes
Aura cushion
or alternative
weight limit
120kg/19 stone
via S.E.O form
Flow chart for guidance only, the individual assessor needs to consider
all other factors i.e. length of stay in bed, diagnosis, diet etc.

Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 16 April 2016
Appendix 6
Flow chart to assist in the appropriate prescription of dynamic pressure relieving mattresses
High risk patient
Medium risk patient
Yes Yes
Yes
With a
Grade 3 – 4
Pressure Ulcer
on heel &/or
other area
With a
Grade 3 – 4
Pressure Ulcer
With a
Grade 2 - 3
Pressure Ulcer
Yes
Yes
Nimbus 2
weight limit 250kg/39 stone
Autoexcel
weight limit 203kg/32 stone
or Tally Quattro weight limit
60kg/25 stone min 26kg/4stone
or Soft Form Premier Active
if a stable surface is needed
Flow chart to assist in the appropriate prescription
of dynamic pressure relieving mattresses via S.E.O form
Very high risk patient
Very high risk patient
No
No
Yes but no sore heel
Yes
Yes
With a
Grade 1 – 2
Pressure Ulcer
Yes
Alpha xcell
weight limit 140kg/22 stone
or High Spec Static Mattress
(see flow chart for static systems)
Nimbus 3
weight limit 250kg/39stone
or Quarto Prime
Flow chart for guidance only, the individual assessor needs to consider
all other factors i.e. length of stay in bed, diagnosis, diet etc.
Appendix 7
Flow chart to assist in the appropriate prescription of static pressure reducing mattresses
Very high risk patient
No
High risk patient
Medium risk patient
Low risk patient
No
Yes Yes
Yes
Yes
With a
Grade 3 – 4
Pressure Ulcer
With a
Grade 1 – 2
Pressure Ulcer
With no
Pressure Ulcer
Yes
Yes
Please refer to
dynamic systems
flow chart.
Repose overlay
via E.O form
or consider
dynamic systems
Memory foam if more
stable surface needed
via S.E.O form
Soft form mattress
or Propad
Waterlow 19
weight limit 165 kg/26 stone
or no action required
reassess if change
in condition
Flow chart to assist in the appropriate prescription
of static pressure reducing mattresses.
Flow chart for guidance only, the individual assessor needs to consider
all other factors i.e. length of stay in bed, diagnosis, diet etc.
With a
Grade 1 – 2 heel
Pressure Ulcer
Consider MSS heel pad
via S.E.O form
or Repose heel protector
via E.O form
Yes

Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 17 April 2016
Appendix 8
Specialist Equipment Order Form
12
13 Specialist Equipment Order Form
Please return form to: Community Equipment Services, Unit D6, Hortonwood 7, Hortonwood,
Telford TF1 7GP. Telephone: 01952 603838 Fax: 01952 603782
email: [email protected]
Please complete all sections of this form giving as much detail as possible.
Inadequately completed forms will be returned for completion, which will obviously delay the provision of the
appropriate equipment.
Patient Details:
Name: Date of Birth:
Address: NHS Number:
Telephone No:
Post Code:
Alternative contact name number and relationship:
Does the service user live alone?:
Any hazards if known:
G.P. Details:
Name: NHS Code:
Address:
Telephone No:
Assessing professional details:
Name: Agency:
Address:
Telephone No:
Date of Assessment:
Signature:
Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 18 April 2016
Describe current health status:
Diagnosis and prognosis: Height: Weight: Circumference of abdomen/girth: Mobility (please describe if they have the ability to achieve a change of position when lying or sitting. How they transfer,walk and move from lying to sitting) Present Skin Condition: Current Waterlow Score: Sore Grade: Sore Site: History of pressure sores: Site:………………… Grade:………………… No of Hours on Bedrest: No of Hours Sitting/Mobile: Number of handling transfers daily:
14 Clinical reasoning for equipment requested:
(Please include any consideration given to informal/formal carers)
Shropshire Community Health NHS Trust
Guidelines for Pressure Ulcer Prevention and Management 969-31643 19 April 2016
What Type of equipment is required:
Bed: Type: Cotsides: Type: Bumpers: Type: Mattress system: Type: Cushion: Type: (If cushion is required for a wheelchair, please request from Wheelchair Services) Stand aid: Type: Hoist Type: Sling: Type: Other: Supplier Info (if new please provide supporting literature): …………………………………………………..
Accommodation (Current):
Please describe access to property, where the equipment is to be sited and on which level. NB All beds are sited downstairs wherever possible, if not, an access visit is required to assess the environment and accessibility upstairs. Please ensure that there is sufficient space at the property to install bed appropriately. Arrangements made to install equipment and name of person who will demonstrate equipment: NB If care agency is involved, the demonstration must also include the care manager. Discharge Date: Care Package commencement date and name and contact number of agency:
Additional comments: