plasmodium species
TRANSCRIPT

PLASMODIUM SPECIES
PRESENTED BY : PRABIN SHAH , B.Sc. MLT 5th semester
Malaria parasite belong to the genus Plasmodium which include over 125 species infecting reptile, birds and mammals.Human parasite belong to subgenera P.(Plasmodium) and P.(Laverania).Malaria parasite infecting to human belongs to 4 species
P.(Laverania)falciparumP.(Plasmodium)vivax P.(Plasmodium)malariae P.(Plasmodium) ovale

Plasmodium falciparum It is found mainly in the hotter and more humid regions of the world. It is found in the tropical and sub tropical Africa and the parts of Central America and South America , Bangladesh, Nepal, Srilanka etc.
Plasmodium vivaxIt is widely distributed in the temprate and sub tropical areas (South America , Northern Africa, India, Nepal, Pakistan etc)

Plasmodium malarieIt has much lower prevalence than P.falciparum and P. vivax.It account for 25% of Plasmodium infection. It is found in the tropical and sub tropical regions (Guyana, India, Srilanka etc ).
Plasmodium ovale It is mainly found in West Africa , China, Indonesisa, Philippines, South East Asia. It accounts for 10% of infection.
LIFE CYCLE OF PLASMODIUM LIFE CYCLE OF PLASMODIUM SPECIESSPECIES

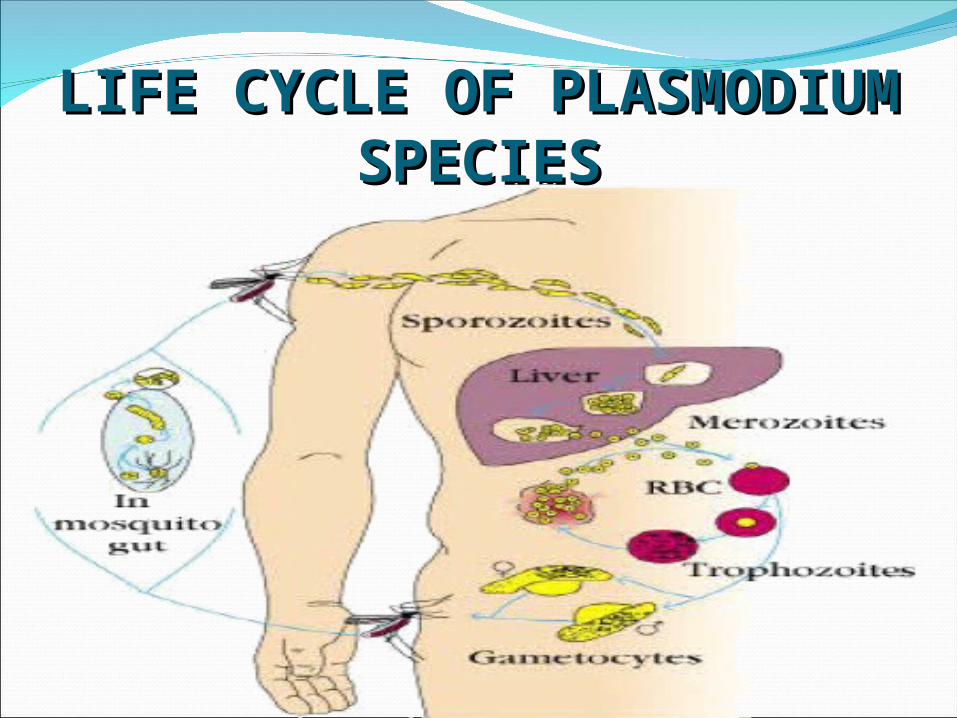
Malaria parasite exhibits a complex life cycle involving alternating cycles of asexual division occurring in man and sexual development in the mosquito. Definite host : Mosquito(Female anopheles)Intermediate host : Man
Sporozoite are the infective form of the parasite, they are present in the salivary glands of mosquito.
• Man get infection by biting of infected female mosquito.
•Proboscis of the mosquito pierces the skin and saliva containing sporozoites are injected directly to the blood stream.

The cycle in man comprises of following stages (a) Primary exoerythrocytic schizogony (b) Erythrocytic schizogony (c) Gametogony (d) Secondary exoerythrocytic schizogony
Primary exoerythrocytic schizogony• Within 1hour all the sporozoites leave the blood stream and enter into liver parenchyma cells.The elongated, spindle shaped bodies become rounded inside liver cells. • They undergo multiple nuclear division, followed by cytoplasmic division and develop into primary exoerythrocytic schizont. • When this schizogony is complete, liver cell ruptures and release merezoites into blood stream.
•Merozoites liberated from the primary exoerythrocytic schizogony enter the blood stream and invade the red cells where they multiply at the expense of the host cells. •Here they pass through the stages of trophozoite, schizonts and merozoites.•Depending on the species, 6-12 nuclei are produced followed by cytoplasmic division and red cells ruptures and releases merozoites.•Plasmodium falciparum differs from other species, where developing erythrocytic schizonts aggregate in the capillaries of the brain and other internal organs.

• After erythrocytic schizogony, some merozoites develop within red cells into male (microgametocyte) and female gametocytes (macrogametocyte).• Only mature gametocytes are found in the peripheral blood.• Host carrying gametocytes is known as carrier.• Microgametocyte of all 4 species are small, cytoplasm stain light blue and the nucleus is diffuse and enlarge.• Macrogametocyte are larger, cytoplasm stains deep blue and nucleus is compact and small.

•In case of P. vivax and P. ovale, some sporozites on entering into hepatocytes enter into a resting (dormant) stage before undergoing asexual multiplication.•The resting stage of the parasite is rounded, 4-6 µm in diameter, uninucleate and is known as hypnozoite.•After a period of weeks, months or years hypnozoites are reactivated to become secondary exoerythyic schizonts and release merozoites which infect RBC producing relapse of malaria.

Sexual cycle actually starts in the human host itself by the formation of gametocytes which are present in the peripheral blood.In the mosquito, only the mature sexual forms are capable of further development and rest die. From one microgametocyte eight thread-like filamentous structures called microgametes are formed by the process of exflagellation.The macrogametocyte develops into macrogamete, which fertilizes with microgamete within 20 mins – 2 hrs.

In next 24 hrs the zygote lengthens and matures into ookinete, which penetrate the epithelial lining of the stomach of mosquito and develops into oocyst.Sporozoites develop inside the oocyst which no. varies from a few hundred to few thousands in each oocyst.On about 10th day the oocyst is fully mature, ruptures and releases sporozoites in the body cavity of mosquito.The sporozoites are distributed through the body fluid to the various organs of the body except the ovaries.Sporozoites have special predilection for salivary glands and ultimately reach in maximum no. at which the mosquito is capable of infecting human.

Besides infection by the bite of infected female mosquito the infection may also be transmitted by
Transfusion of blood from a patient of malaria ( TRANSFUSION MALARIA)Transmission of infection to foetus in utero through some placental defect ( CONGENITAL MALARIA)By the use of contaminated syringes particularly in drug addicts.

The above conditions are also known as ‘trophozoite induced malaria’ where No primary & secondary exoerythrocytic schizogonyIncubation period is shortNo relapse.After incubation period patient develops malaria which consists of1.Febrile paroxysm 2.Anaemia3.Splenomegaly
It generally begins in the early afternoon and comprises of 3 successive stagesCold stage ( 15- 60 mins)Hot stage ( 2-6 hrs)Sweating stage The periodicity of attack varies within species as
P. vivax – 48 hrsP. ovale – 48 hrsP. malariae – 72 hrs

After a few paroxysms, anaemia of a microcyctic or a normocyctic hypochromic type develops because ofMechanical destruction of parasitized red cellsReduced erythropoiesis in the bone marrow Lysis and phagocytosis of uninfected red cells.
In addition, in a small no. of patients with malignant tertian malaria there is autoimmune destruction of red cells.
It is due to the massive proliferation of macrophages which phagocytize both parasitized and non-parasitized RBCsThe condition is characterized by massive and chronic splenomegaly with high levels of IgM, malaria antibody and circulating immune complexes and a moderately enlarged liver with hepatic sinusoidal lymphocytosisThe patient is usually anaemic (normocyctic) and has low white cell and platelet counts.

This is the most commonest cause of coma and death in falciparum malaria, particularly in children and non- immune adults
Many parasitized cells can be found in the capillaries of the brain and in the late stages, haemorrhaging from small blood vessels can occur.

It is a rare but acute condition in which there is a rapid and massive intravascular haemolysis of both parasitized and non parasitized red cellsIt results in haemoglobinaemia, haemoglobinuria and fall in haemoglobinThe urine appears dark red to brown- black due to the presence of free haemoglobin hence the name BLACKWATER FEVERIt can occur in non-immune adults with severe falciparum malaria and also as a complication of quinine treatment.

Disease Severity and Durationvivax ovale malariae falciparum
Incubation Period
8-27 8-27 16->40 6-25
Severity of Initial Paroxysms
moderate to severe
mild mild to moderate
severe
Average Parasitemia
20,000 9,000 6,000 50,000-500,000
Maximum Parasitemia
50,000 30,000 20,000 2,500,000
Typical Symptom Duration
3-8 weeks 2-3 weeks 3-24 weeks 2-3 weeks
Maximum Infection Duration
5-8 years 12-20 months
20-50 years 6-17 months
Anemia ++ + ++ ++++
Other Complications
- - Renal Cerebral
MICROSCOPYDiagnosis of malaria can be established by demonstration of malaria parasites in the bloodThick and thin smears of the blood are prepared on the same or different slidesBlood is taken by pricking a finger or ear lobule before starting treatment with antimalarialsFor preparation of thick smear a large drop of blood is taken on the slide and then spread in an area of 12 mm sq; dehaemoglobinization of thick smear is done by keeping the slide in distilled water in Koplin’s jar in vertical position for 5-10 mins till the slide become white and then dried in air.

All asexual erythrocytic stages as well as gametocytes can be seen in peripheral blood in infection with P. vivax , P. malariae and P. ovale but in P. falciparum infection , only the ring forms and crescent shaped gametocytes can be seen
The occurrence of multiple rings in an individual red blood cell with accole forms is diagnostic of P. falciparum infection

Both thick and thin smears can be stained by following stains:Leishman stainGiemsa stainField stainJ.S.B.(Jaswant singh ,Bhattacharjee ) stain

Schizont of P.malaria
Gametocyte of P.falciparum

Ring form of P.ovale
Ring form of P.vivax

RDTs are based on the detection of antigens derived from malaria patients in lysed blood, using immuno-chromatographic methods
Most frequently they employ a dipstick or test strip bearing monoclonal antibodies directed against the target parasite antigens
The tests can be performed in about 15 mins.
Histidine-rich protein 2 (HRP-2) is water soluble protein produced by trophozoites and young gametocytes of P. falciparum; commercial kits currently available detect HRP-2 from P. falciparum only
Parasite lactate dehydrogenase ( pLDH) is produced by asexual and sexual stages of malaria parasites

In QBC test, malaria parasites are concentrated by centrifuging blood in a special capillary tubeThe tube is coated with acridine orange and an anticoagulant which contains a small plastic cylinderFollowing centrifugation, the white cells, platelets and upper layer of the red cells which contain the malaria parasites can be found in the space between the float and inside wall of the capillaryWhen examined by fluorescence microscopy at × 600 magnification, the acridine orange stained malaria parasites fluresce green yellow against a dark red-black background with the nucleus of trophozoites and merozoites of schizonts fluorescing bright green.

Chloroquine was the standard treatment for acute malaria for many years. However, resistance to this drug in P. falciparum is widespreadQuinine is the most reliable alternative to chloroquine for the treatment of malaria caused by chloroquine-resistant strains. Tetracycline and clindamycin exhibit some anti-malarial activity and are used as an adjunct to quinine therapy; Mefloquine and halofantrine are also active against chloroquine resistant strains but resistant to these drugs has also been reportedChloroquine and quinine donot eliminate exoerythrocyctic parasites in the liver. For this primaquine (8-amino quinoline drug ) should be used. However, this drug may precipitate haemolysis in individuals deficient in the enzyme glucose-6-phosphate dehydrogenase.

Malaria can be controlled by the integration of following measures:Spraying the breeding sites with petroleum oils and Paris green as larvicidesUsing larcivorous fish, Gambusia affinis and a bacterium, Bacillus thuringiensis var. israelensis or serotype H14 of B. thuringiensis in breeding placesFlooding and flushing of breeding placesEliminating breeding places such lagoons and swampsAvoiding exposure to mosquito bites by various physiochemical meansUse of antimalarial prohylaxis chloroquine , pyrimethamine and proguanil Early diagnosis and prompt treatment of patients.

D.R.ARORA, B.ARORA Medical ParasitologyMonica Cheesbrough District Laboratory Practice in Tropical Countries Part 2www.google.comGodkar, Textbook of Medical Laboratory Technology
