pin point densities on abdominal x-ray
TRANSCRIPT
PICTURE OF THE MONTH
Pin Point Densities on Abdominal X-ray
Pankaj Gupta & Uma Debi & Yalaka Rami Reddy &
Babu Ram Thapa & Kaushal Kishor Prasad
Received: 20 November 2013 /Accepted: 13 January 2014# Dr. K C Chaudhuri Foundation 2014
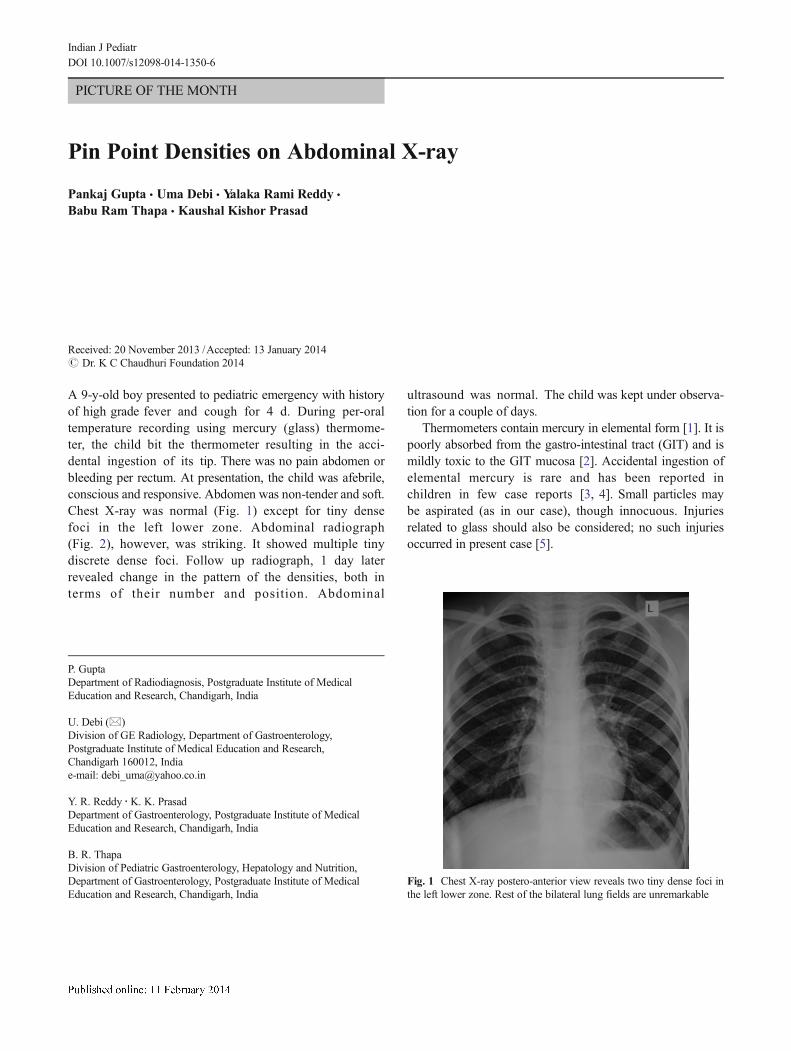
A 9-y-old boy presented to pediatric emergency with historyof high grade fever and cough for 4 d. During per-oraltemperature recording using mercury (glass) thermome-ter, the child bit the thermometer resulting in the acci-dental ingestion of its tip. There was no pain abdomen orbleeding per rectum. At presentation, the child was afebrile,conscious and responsive. Abdomen was non-tender and soft.Chest X-ray was normal (Fig. 1) except for tiny densefoci in the left lower zone. Abdominal radiograph(Fig. 2), however, was striking. It showed multiple tinydiscrete dense foci. Follow up radiograph, 1 day laterrevealed change in the pattern of the densities, both interms of their number and position. Abdominal
ultrasound was normal. The child was kept under observa-tion for a couple of days.
Thermometers contain mercury in elemental form [1]. It ispoorly absorbed from the gastro-intestinal tract (GIT) and ismildly toxic to the GIT mucosa [2]. Accidental ingestion ofelemental mercury is rare and has been reported inchildren in few case reports [3, 4]. Small particles maybe aspirated (as in our case), though innocuous. Injuriesrelated to glass should also be considered; no such injuriesoccurred in present case [5].
Fig. 1 Chest X-ray postero-anterior view reveals two tiny dense foci inthe left lower zone. Rest of the bilateral lung fields are unremarkable
P. GuptaDepartment of Radiodiagnosis, Postgraduate Institute of MedicalEducation and Research, Chandigarh, India
U. Debi (*)Division of GE Radiology, Department of Gastroenterology,Postgraduate Institute of Medical Education and Research,Chandigarh 160012, Indiae-mail: [email protected]
Y. R. Reddy :K. K. PrasadDepartment of Gastroenterology, Postgraduate Institute of MedicalEducation and Research, Chandigarh, India
B. R. ThapaDivision of Pediatric Gastroenterology, Hepatology and Nutrition,Department of Gastroenterology, Postgraduate Institute of MedicalEducation and Research, Chandigarh, India
Indian J PediatrDOI 10.1007/s12098-014-1350-6

Contribution BR Thapa will act as guarantor for this paper.
Conflict of Interest None.
Role of Funding Source None.
References
1. Vano-Galvan S, Jimenez-Garcia D, Vano-Galvan E, Jaen P. Accidentalsubcutaneous implant of mercury after thermometer trauma. J AmAcad Dermatol. 2009;61:535–7.
2. Ellabban MG, Ali R, Hart NB. Subcutaneous metallic mercury injec-tion of the hand. Br J Plast Surg. 2003;56:47–9.
3. Saxena R, Kumar A, Satkurunathan M. Mercury aspiration from abroken thermometer. BMJ Case Rep. 2009;2009.
4. Baudouin V, Bocquet N, RybojadM, LissakN, Broux F, GrallM, et al.Clinical quiz. Mercury poisoning in children. Pediatr Nephrol.1997;11:263–4.
5. Aprahamian N, Lee L, Shannon M, Hummel D, Johnston P, Kimia A.Glass thermometer injuries: It is not just about the mercury. PediatrEmerg Care. 2009;25:645–7.
Fig. 2 Abdominal radiograph reveals multiple tiny high density focidistributed in the periphery
Indian J Pediatr