pigmentaryretinopathies with systemic associations · retardation, adenoma sebaceum, ash leaf spot,...
TRANSCRIPT

1/28/2019
1
Retinal Manifestations of Systemic Disease – Part 2
Sundeep Dev, MD
VRSF Retinal Update 2019
VitreoRetinal Surgery, PA
1
The Retina and Systemic diseases
Retinitis/Vasculitis
Vitreous cells
Serous detachments
Choroidal lesions
Pigmentary retinopathies
Choroidal folds/Choroidal masses
Retinal Vascular abnormalities
2
Pigmentary retinopathies with systemic associations
3
40 yo with unilateral VA loss. Va = 20/400
Other eye normal 4
5
Psudoretinitis pigmentosa
Syphillis
Other inflammatory disease – Lyme, AZOOR, DUSN
Phenothiazine toxicity
Congenital rubella
Autoimmune / Cancer associated retinopathy
Vitamin A deficiency
Resolved exudative detachment – VKH, toxemia of pregnancy
Retained foreign body after penetrating trauma 6

1/28/2019
2
Diffuse Unilateral Subacute Neuroretinitis (DUSN)
7
Diffuse Unilateral SubacuteNeuroretinitis (DUSN)
Unilateral progressive pigmentaryretinopathy, vascular attenuation, optic atrophy, vitritis
Baylisascarisprocyonis (raccoon parasite), Ancylostomacaninum (dog hookworm)
Fecal-oral route worm
8
Rubella
Can be unilateral or bilateral after congenital or acquired infection. “Salt and Pepper” appearance. Vision and ERG usually normal. Vessels usually normal. Cataract may be present. 9
Measles
Typically bilateral. More common after acquired infection. “Salt and pepper appearance”. ERG/VF diminished, but may recover. 10
Vitamin A Deficiency
Night blindness, severe dry eye. Common in children in developing world. Can occur after bariatric surgery, with malabsorption, or liver disease. ERG/VF changes. Pigmentary retinopathy. Treatment: Vitamin A. 11
Acute Zonal Occult Outer Retinopathy (AZOOR)
Late stage12

1/28/2019
3
Acute Zonal Occult Outer Retinopathy (AZOOR)
Typically young females in mid 30’s. Present with photopsias, scotomas, VF loss with ERG changes, minimal fundus changes with delayed development of zones of atrophic RPE. Start unilateral, but often become bilateral. Poor prognosis. 13
AZOOR
Early stage 14
Autoimmune Retinopathy – high degree of suspicion
15
HVF / multifocal ERG
16
Gardner’s syndrome
Familial polyposis coli –autosomal dominant 17
Systemic Diseases associated with Reitinitis Pigmentosa
Consider in young patients with RP
Refsum’s disease – recessive, associated with increased phytanic acid levels.
Hereditary abetalipoprotenemia –recessive, RP with fat intolerance, deficiency of vitamins A, D, E, and K
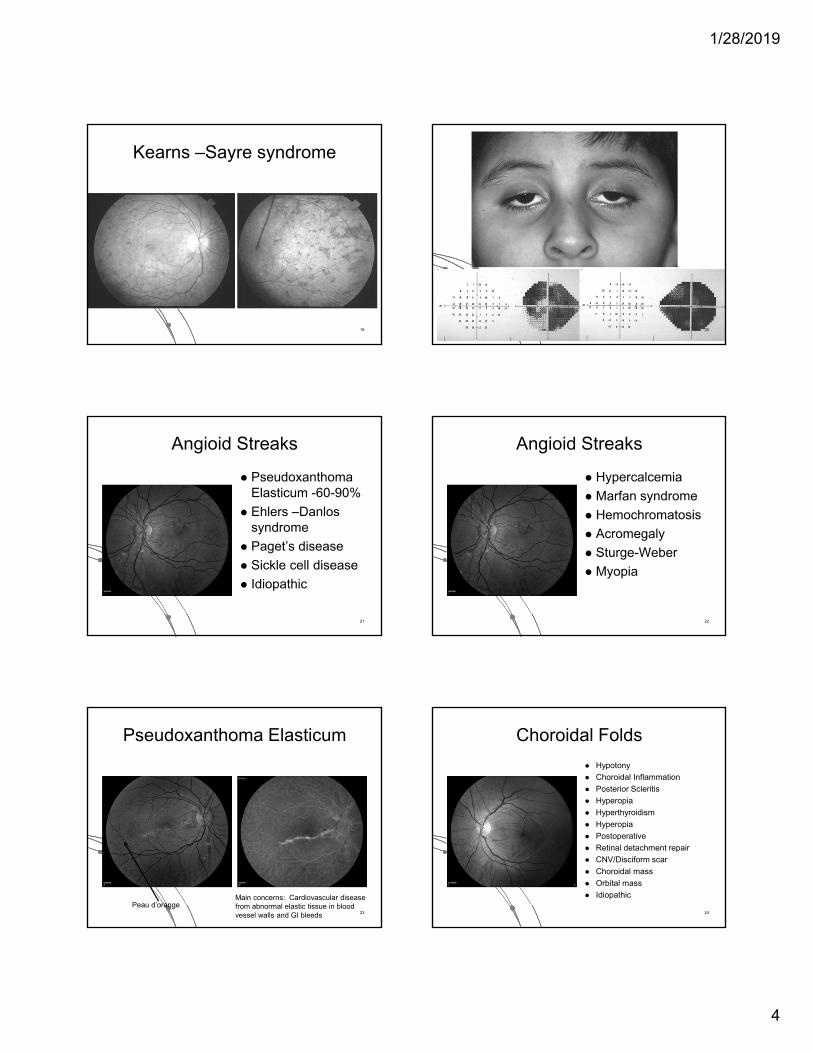
Kearns-Sayre syndrome - recessive, salt and pepper appearance, normal arterioles, CPEO, ptosis, heart block by age 15
18
1/28/2019
4
Kearns –Sayre syndrome
19 20
Angioid Streaks
Pseudoxanthoma Elasticum -60-90%
Ehlers –Danlossyndrome
Paget’s disease
Sickle cell disease
Idiopathic
21
Angioid Streaks
Hypercalcemia
Marfan syndrome
Hemochromatosis
Acromegaly
Sturge-Weber
Myopia
22
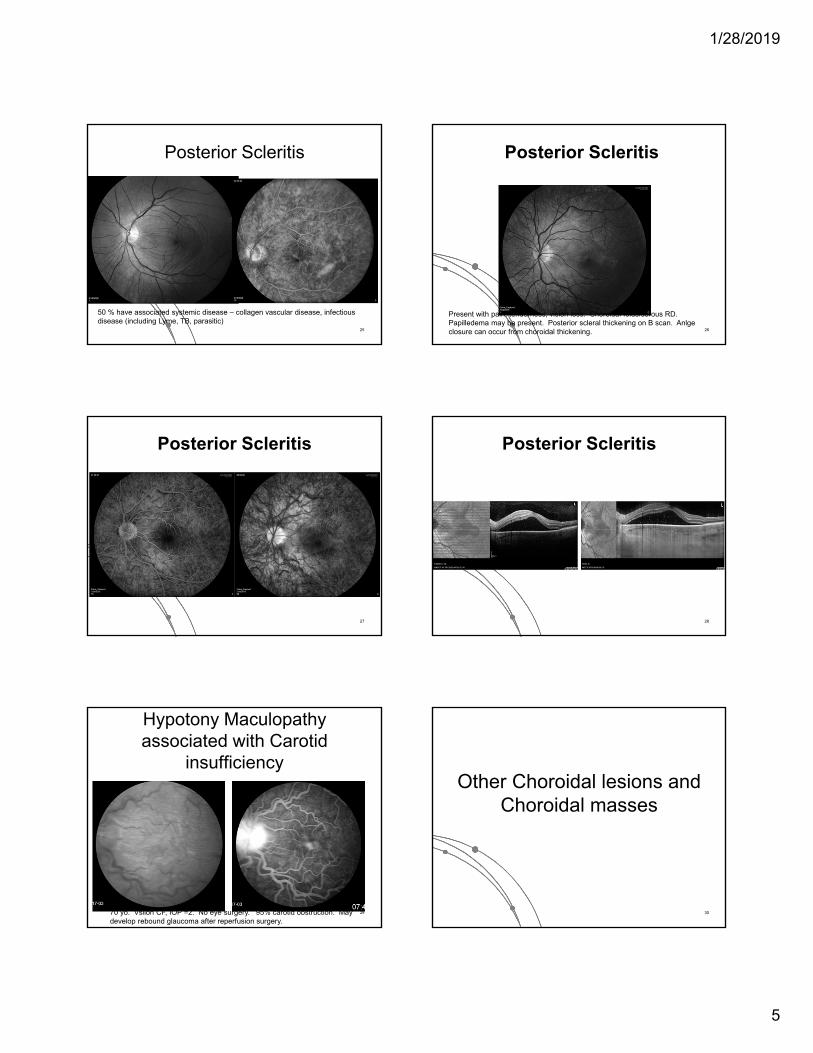
Pseudoxanthoma Elasticum
Peau d’orangeMain concerns: Cardiovascular disease from abnormal elastic tissue in blood vessel walls and GI bleeds 23
Choroidal Folds
Hypotony
Choroidal Inflammation
Posterior Scleritis
Hyperopia
Hyperthyroidism
Hyperopia
Postoperative
Retinal detachment repair
CNV/Disciform scar
Choroidal mass
Orbital mass
Idiopathic
24
1/28/2019
5
Posterior Scleritis
50 % have associated systemic disease – collagen vascular disease, infectious disease (including Lyme, TB, parasitic)
25
Posterior Scleritis
Present with pain, tenderness, vision loss. Choroidal folds/serous RD. Papilledema may be present. Posterior scleral thickening on B scan. Anlgeclosure can occur from choroidal thickening. 26
Posterior Scleritis
27
Posterior Scleritis
28
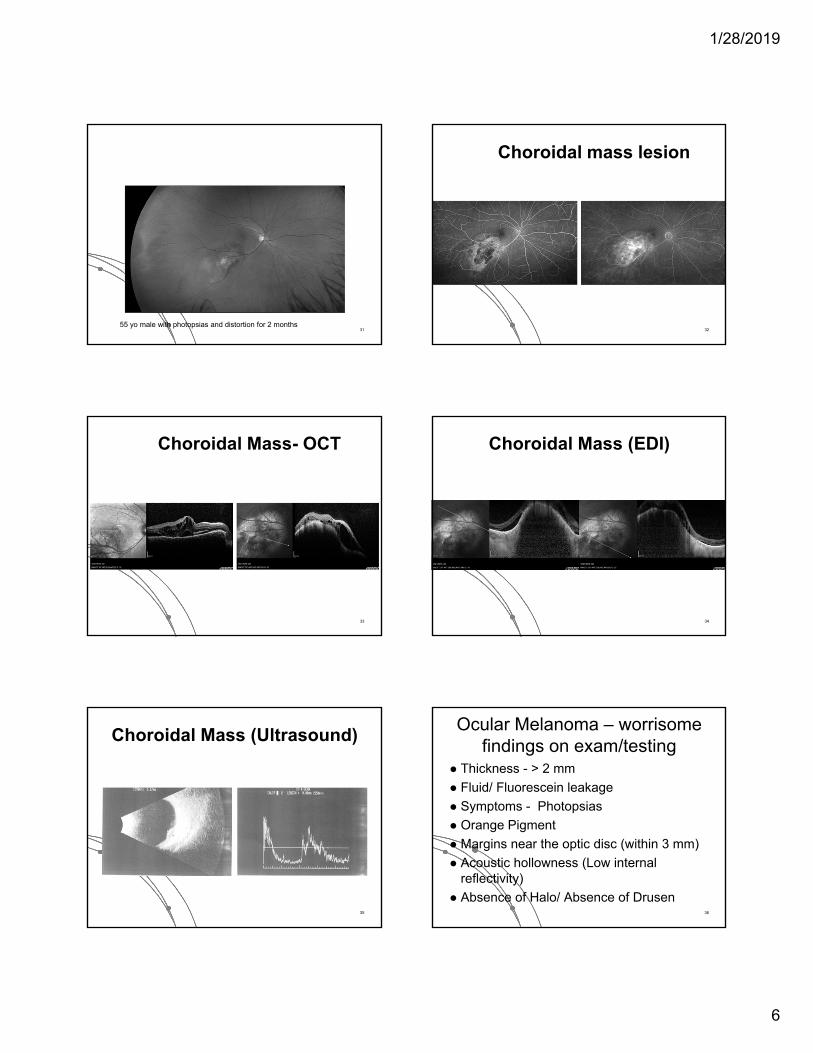
Hypotony Maculopathyassociated with Carotid
insufficiency
70 yo. Vsiion CF, IOP =2. No eye surgery. 95% carotid obstruction. May develop rebound glaucoma after reperfusion surgery.
29
Other Choroidal lesions and Choroidal masses
30
1/28/2019
6
55 yo male with photopsias and distortion for 2 months31
Choroidal mass lesion
32
Choroidal Mass- OCT
33
Choroidal Mass (EDI)
34
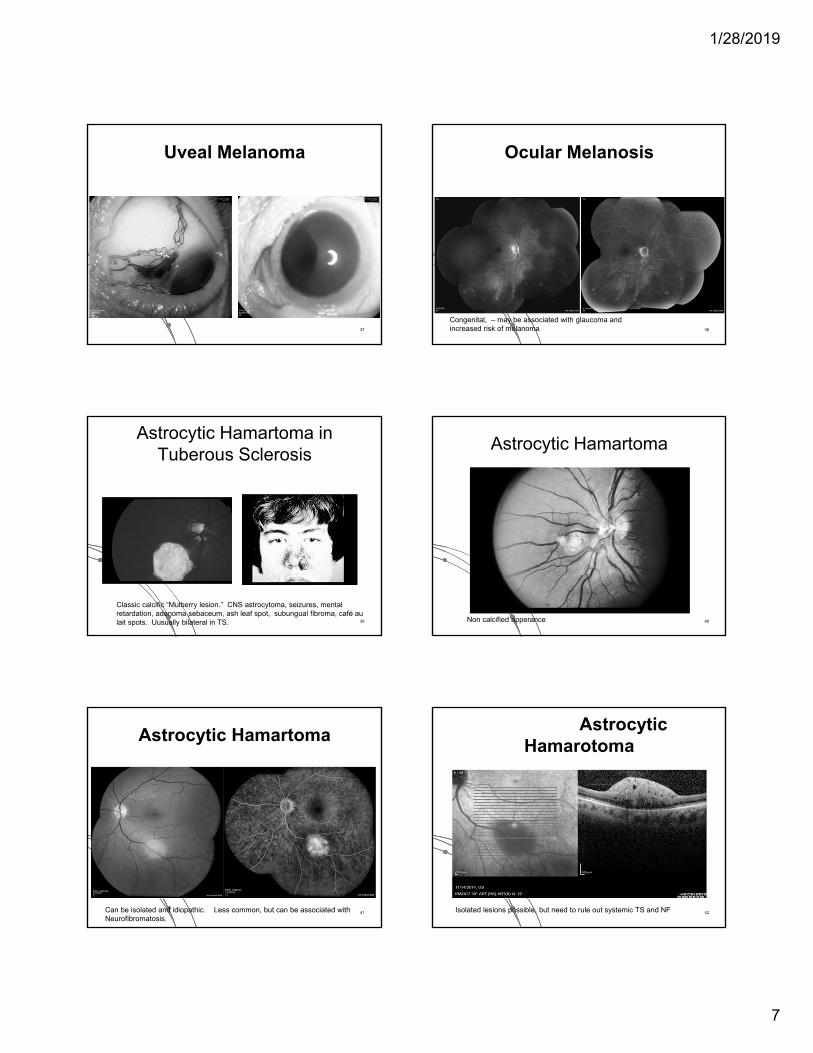
Choroidal Mass (Ultrasound)
35
Ocular Melanoma – worrisome findings on exam/testing
Thickness - > 2 mm
Fluid/ Fluorescein leakage
Symptoms - Photopsias
Orange Pigment
Margins near the optic disc (within 3 mm)
Acoustic hollowness (Low internal reflectivity)
Absence of Halo/ Absence of Drusen36
1/28/2019
7
Uveal Melanoma
37
Ocular Melanosis
Congenital, – may be associated with glaucoma and increased risk of melanoma 38
Astrocytic Hamartoma in Tuberous Sclerosis
Classic calcific “Mulberry lesion.” CNS astrocytoma, seizures, mental retardation, adenoma sebaceum, ash leaf spot, subungual fibroma, café au lait spots. Uusually bilateral in TS. 39
Astrocytic Hamartoma
Non calcified apperance 40
Astrocytic Hamartoma
Can be isolated and idiopathic. Less common, but can be associated with Neurofibromatosis.
41
Astrocytic Hamarotoma
Isolated lesions possible, but need to rule out systemic TS and NF 42
1/28/2019
8
Retinal capillary hemangioblastoma in Von Hippel-Lindau Syndrome
Often earliest manifestation of VHL. Mean age is 25. 42% unilateral. Most that have multifocal or bilateral, have VHL. Can also be isolated. Genetic testing is best way to screen for the condition.
43
Von Hippel Lindau disease
Feeder arteriole and draining venule. FA shows rapid filling and leakage. Va loss from exudation, traction, VH, NVG. Small ones can be observed. Laser/Cryo/Radiation/ surgical excision. +/- seteroids/ anti-VEGF. Prognosis depends on tumor size. 44
Wyburn-Mason Syndrome
Non-hereditary, Congenital Unilateral, can progress in childhood.- involves retina and midbrain – seizures, hemiparesis. Vision can be normal to severe loss due to intraretinal heme and NVG. No clear Rx. 45
Wyburn-Mason Syndrome
46
Cavernous Hemangioma
Benign vascular hamartoma. Most are sporadic, they can be autosomal dominant and associated with brain and skin hemangiomas. Grape like clusters with stagnant blood flow cause layering on FA. No leakage. Usually no Rx and asymptomatic unless traction or VH develops in which case cryo/laser may help. May involve optic nerve or macula.
47
20/20 OD 20/400 OS
Systemic Histiocystosis
48
1/28/2019
9
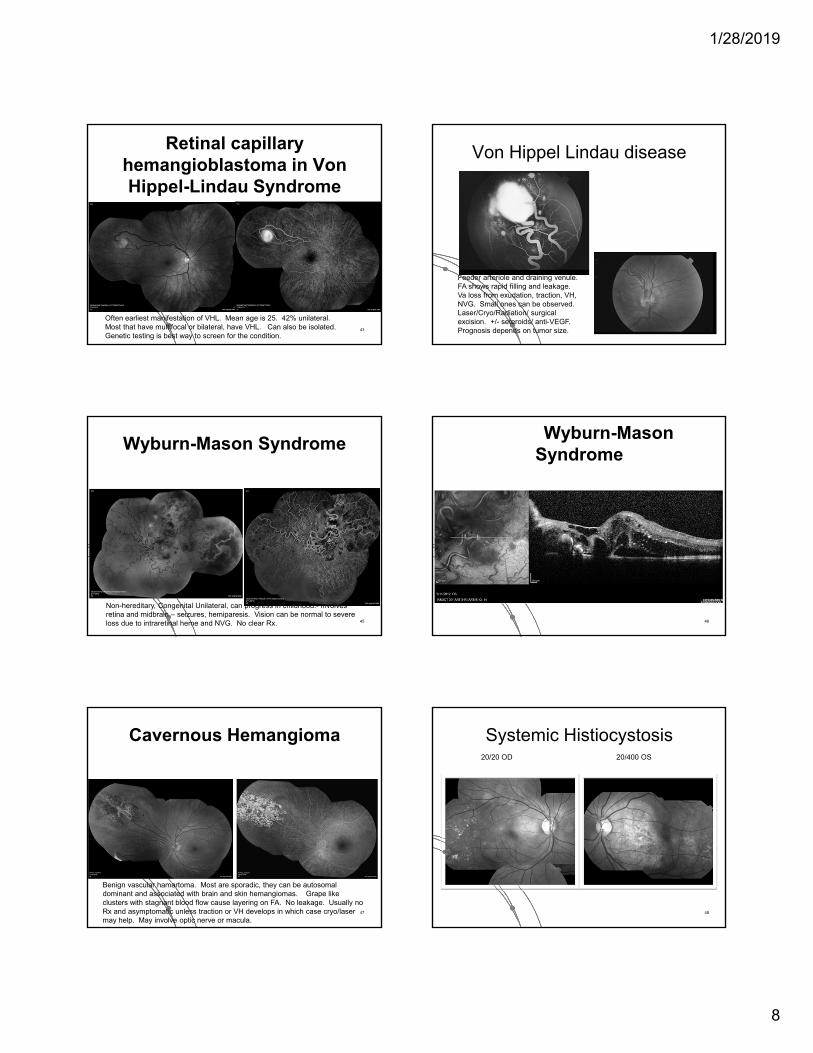
Sclerochoroidal Calcification
Most cases are idiopathic – should test patients for abnormal calcium-phosphorous metabolism. Check parathyroid hormone, vitamin D and calcium levels. Chronic Kidney disease can be associated.
49
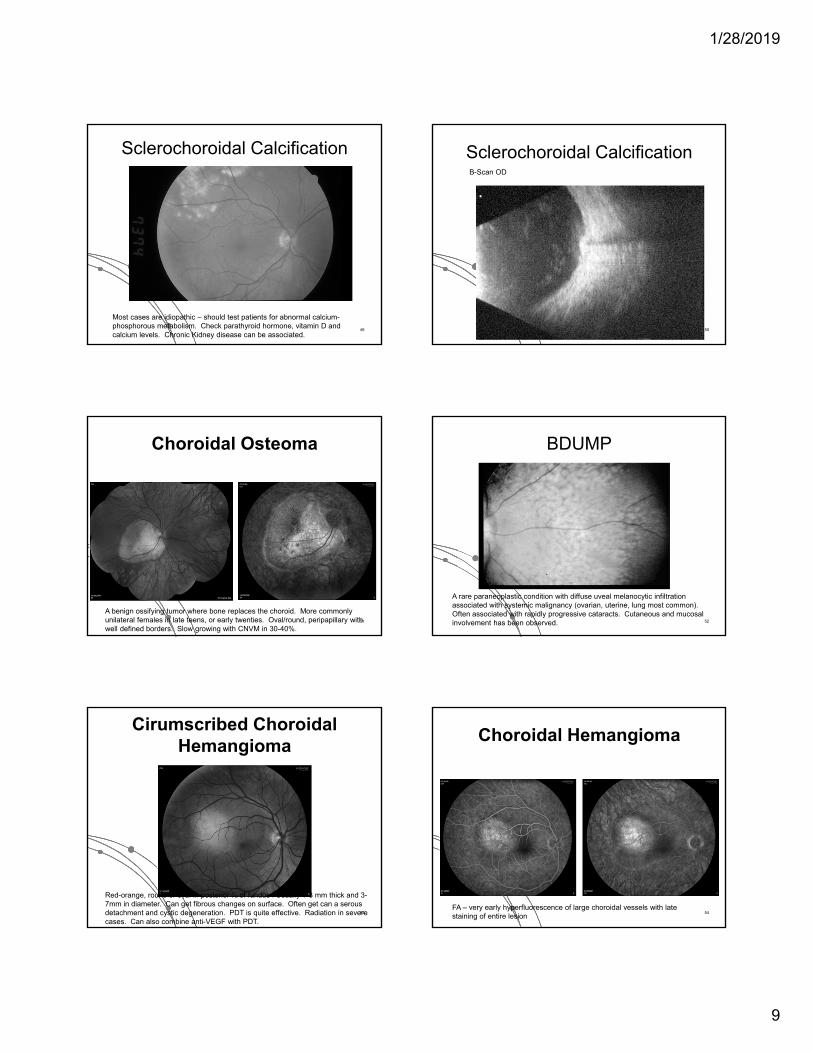
B-Scan OD
Sclerochoroidal Calcification
50
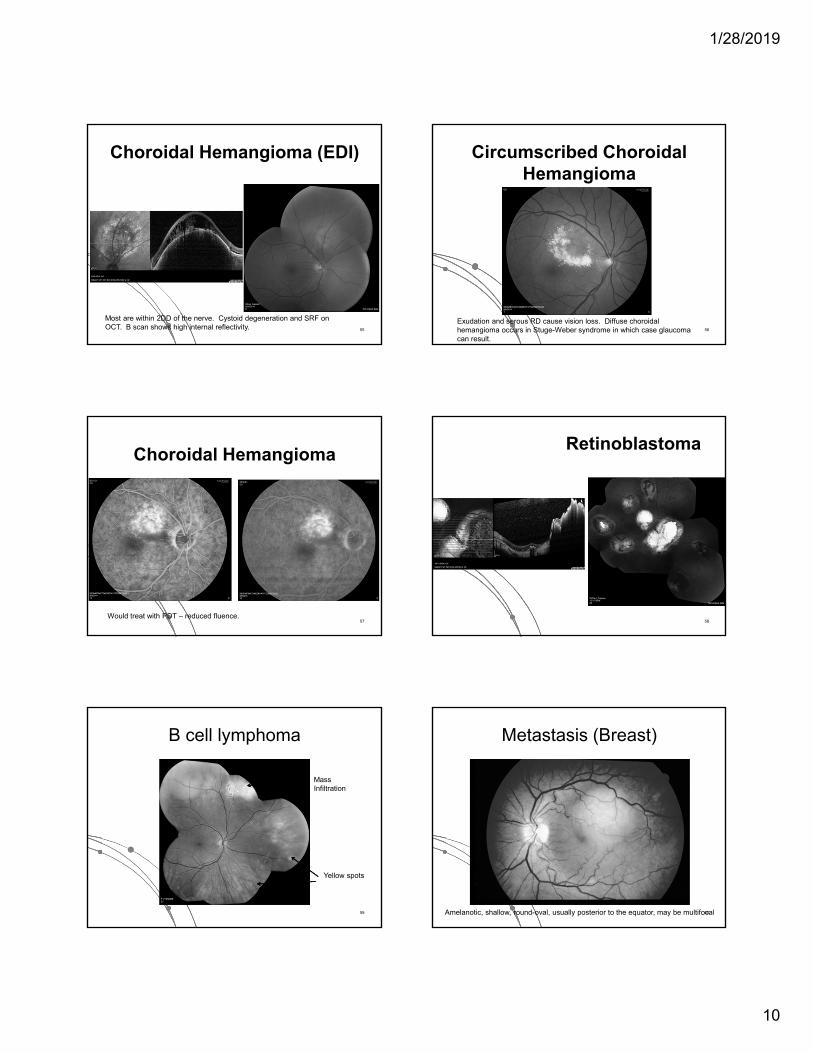
Choroidal Osteoma
A benign ossifying tumor where bone replaces the choroid. More commonly unilateral females in late teens, or early twenties. Oval/round, peripapillary with well defined borders. Slow growing with CNVM in 30-40%.
51
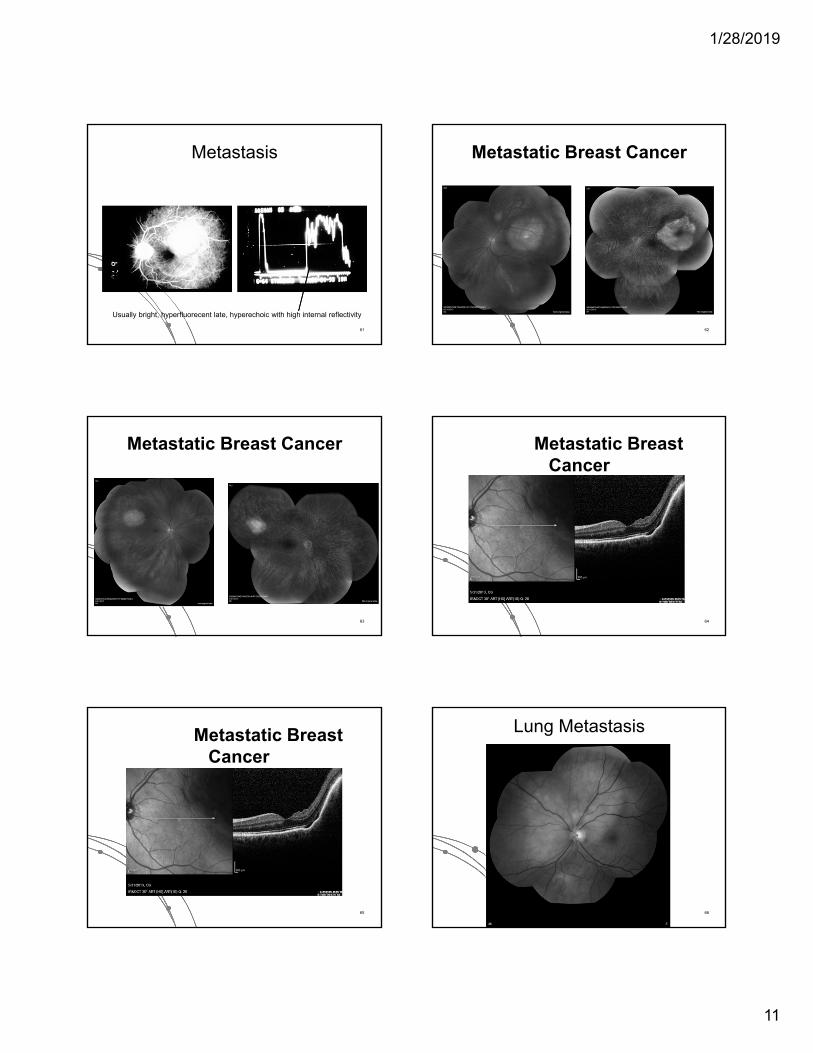
BDUMP
A rare paraneoplastic condition with diffuse uveal melanocytic infiltration associated with systemic malignancy (ovarian, uterine, lung most common). Often associated with rapidly progressive cataracts. Cutaneous and mucosal involvement has been observed. 52
Cirumscribed Choroidal Hemangioma
Red-orange, round or oval in posterior ½ of fundus . Usually 1-3 mm thick and 3-7mm in diameter. Can get fibrous changes on surface. Often get can a serous detachment and cystic degeneration. PDT is quite effective. Radiation in severe cases. Can also combine anti-VEGF with PDT.
53
Choroidal Hemangioma
FA – very early hyperfluorescence of large choroidal vessels with late staining of entire lesion
54
1/28/2019
10
Choroidal Hemangioma (EDI)
Most are within 2DD of the nerve. Cystoid degeneration and SRF on OCT. B scan shows high internal reflectivity. 55
Circumscribed Choroidal Hemangioma
Exudation and serous RD cause vision loss. Diffuse choroidal hemangioma occurs in Stuge-Weber syndrome in which case glaucoma can result.
56
Choroidal Hemangioma
Would treat with PDT – reduced fluence.57
Retinoblastoma
58
B cell lymphoma
Mass Infiltration
Yellow spots
59
Metastasis (Breast)
Amelanotic, shallow, round-oval, usually posterior to the equator, may be multifocal60
1/28/2019
11
Metastasis
Usually bright, hyperfluorecent late, hyperechoic with high internal reflectivity
61
Metastatic Breast Cancer
62
Metastatic Breast Cancer
63
Metastatic Breast Cancer
64
Metastatic Breast Cancer
65
Lung Metastasis
66
1/28/2019
12
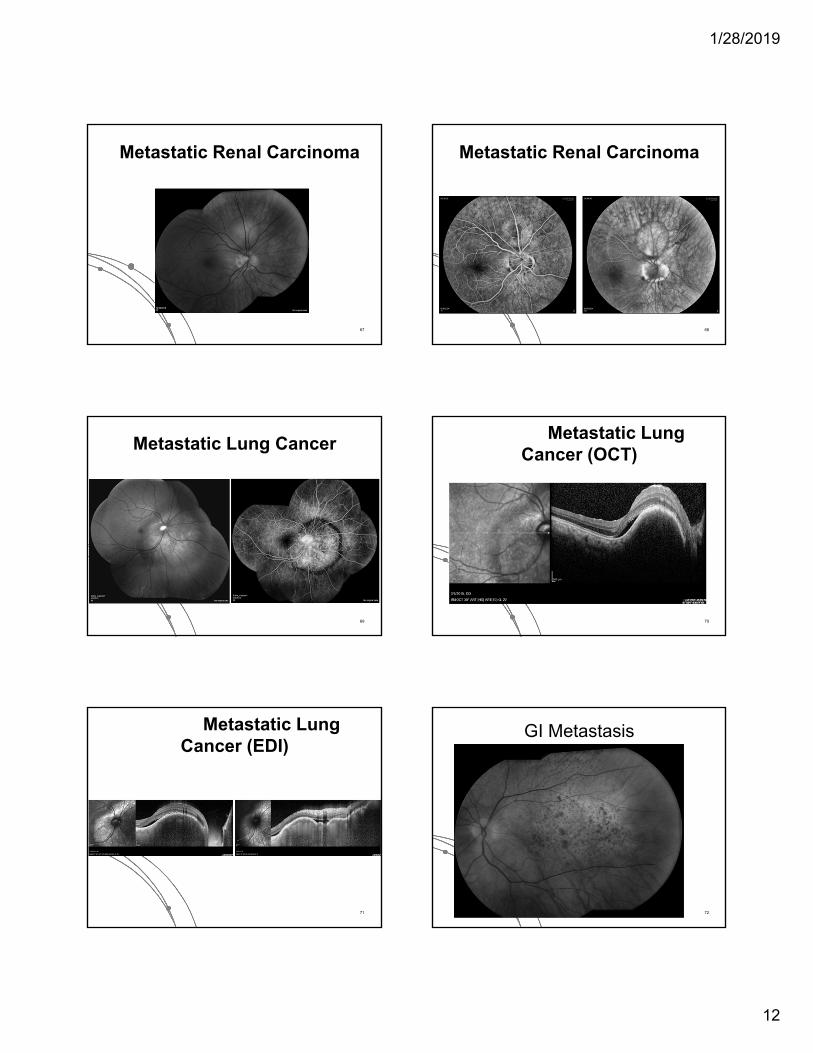
Metastatic Renal Carcinoma
67
Metastatic Renal Carcinoma
68
Metastatic Lung Cancer
69
Metastatic Lung Cancer (OCT)
70
Metastatic Lung Cancer (EDI)
71
GI Metastasis
72

1/28/2019
13
Macroaneurysm with old subretinal hemorrhage
73
Macroaneurysm
74
Varix
Will fluctuate with valsalva maneuver 75
Retinal Vascular Disorders
76
Cotton wool spot
50 yo with new blurry spot and no known medical problems 77
Cotton Wool spots Hypertension – usually DBP >110
Diabetes – seen in 44% of cases of DR
Retinal vein occlusion
Inflammatory – GCA, Wegener’s granulomatosis, Polyarteritisnodosa, Systemic Lupus, Scleroderma
Infectious – CMV, HIV retinopathy, Lyme, Toxoplasmosis, Mucormycosis, Leptospirosis
Coagulopathies – Sickle cell disease, omocysteinemia, Lupus anticoagulant syndrome, Proteins C, S, antithrombin III deficiencies
Embolic – Carotid and Cardiac disease
Miscellaneous – Migraine, severe anemia, Leukemia/lymphoproliferative disorders, Interferon therapy, Radiation, Purtscher’s retinopathy, Papilledema
78

1/28/2019
14
Hypertensive Crisis
79
Acute Leukocytic Leukemia
80
Multiple Myeloma
81
Purtscher’s Retinopathy
Classic is after crush injury, long bone fractures. Associated with pancreatitis, amniotic fluid embolism, collagen vascular disease, TTP.
ischemia
82
Radiation Retinopathy
83
Other Systemic Retinal Vascular Disease
84
1/28/2019
15
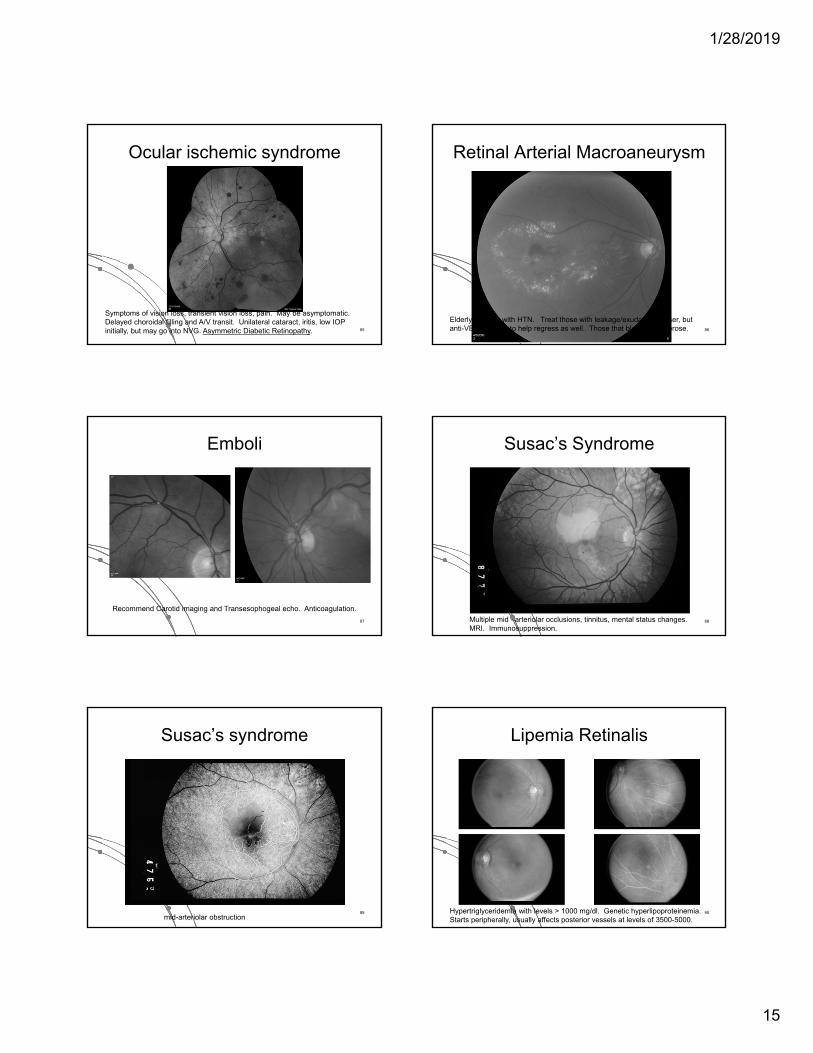
Ocular ischemic syndrome
Symptoms of vision loss, transient vision loss, pain. May be asymptomatic. Delayed choroidal filling and A/V transit. Unilateral cataract, iritis, low IOP initially, but may go into NVG. Asymmetric Diabetic Retinopathy. 85
Retinal Arterial Macroaneurysm
Elderly females with HTN. Treat those with leakage/exudation. Laser, but anti-VEGF seems to help regress as well. Those that bleed often fibrose. 86
Emboli
Recommend Carotid imaging and Transesophogeal echo. Anticoagulation.
87
Susac’s Syndrome
Multiple mid –arteriolar occlusions, tinnitus, mental status changes. MRI. Immunosuppression.
88
Susac’s syndrome
mid-arteriolar obstruction89
Lipemia Retinalis
Hypertriglyceridemia with levels > 1000 mg/dl. Genetic hyperlipoproteinemia. Starts peripherally, usually affects posterior vessels at levels of 3500-5000.
90

1/28/2019
16
Peripheral Retinal Neovascularization
91
Peripheral Retinal Neovascularization
Diabetes
Vein occlusion (branch)
Sickle cell retinopathy (SC)
Sarcoidosis
Drug abuse embolization/ talc retinopathy
Chronic uveitis/pars planitis
Vasculitis
Leukemia/anemia
Eales’ disease92
PDR
93
PDR after West Nile Virus
Diabetic Retinopathy rapidly progresses after ocular inflammatory disease94
Talc Retinopathy
95
SS Disease: Macular infarct
16 year old HM vision after Sickle crisis lead to NVG within 1 month 96
1/28/2019
17
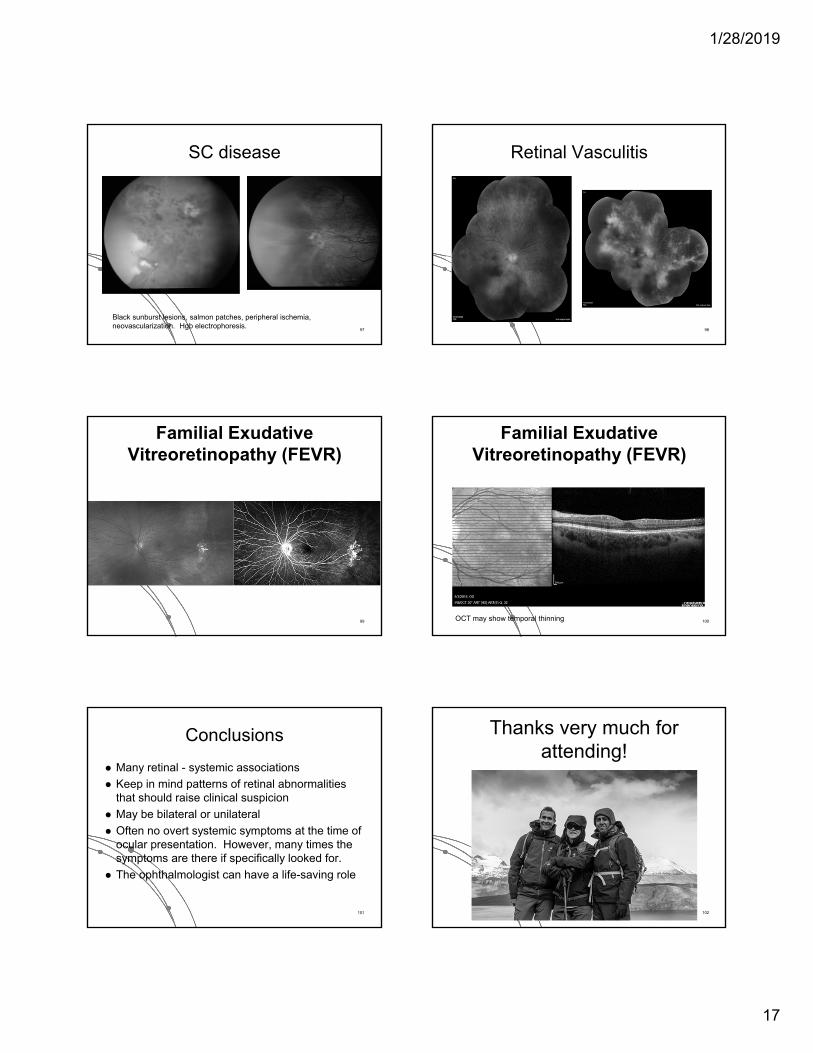
SC disease
Black sunburst lesions, salmon patches, peripheral ischemia, neovascularization. Hgb electrophoresis.
97
Retinal Vasculitis
98
Familial Exudative Vitreoretinopathy (FEVR)
99
Familial Exudative Vitreoretinopathy (FEVR)
OCT may show temporal thinning 100
Conclusions
Many retinal - systemic associations
Keep in mind patterns of retinal abnormalities that should raise clinical suspicion
May be bilateral or unilateral
Often no overt systemic symptoms at the time of ocular presentation. However, many times the symptoms are there if specifically looked for.
The ophthalmologist can have a life-saving role
101
Thanks very much for attending!
102