phosphorus -...
TRANSCRIPT

STUDIES OF CALCIUM AND PHOSPHORUSMETABOLISM
XIV. THE RELATION OF ACID-BASE BALANCETO PHOSPHATEBALANCEFOLLOWINGINGESTION OF PHOSPHATES.1
By WILLIAM T. SALTER, RAY F. FARQUHARSON2 ANiDOROTHYM. TIBBETTS
(From the Medical Clinic of the Massachusetts General Hospital, Boston)
(Received for publication November 23, 1931)
OUTLINEA. IntroductionB. Plan of StudyC. Experimental MethodsD. Experimental Results
I. The Influence of Dietary Potential Acidity on Inorganic PhosphorusMetabolism.
a. The Phosphorus Balanceb. Partition between Urine and Feces
II. The Influence of Ingested Phosphate on Total Fixed Base Metab-olism
a. Neutralization of Phosphate within the Bowelb. Neutralization of Phosphate in Urine
i. Acid Phosphateii. Basic Phosphate
E. DiscussionF. Conclusions
The effect of phosphate-feeding upon the calcium metabolism of manhas been reported in experiments previously described in this journal (1).It appeared that over a relatively short period (ten days) the addition ofinorganic phosphate to the control diet produced no obvious alteration ofthe endogenous calcium excretion, fecal or urinary. This was truewhether the phosphate administered was acid phosphate (mono-sodium),basic phosphate (di-sodium), or a mixture of these two salts. Suchadditions to the neutral control diet, however, did produce definitealterations in the total acid-base economy of the body, not previouslydescribed, which it is the purpose of this paper to report.
The chemical principles which present themselves as the logical guidesto such studies of mineral metabolism have long been recognized, but it isonly within recent years that work like that of Gamble, Blackfan, and
1 Aided financially in part by the Lead Fund of the Harvard School ofPublic Health.
2 Alexander McPhedran Research Fellowship in Clinical Medicine, Uni-versity of Toronto.
39126

ACID-BASE BALANCEAND PHOSPHATEBALANCE
Hamilton (2) has afforded a sound scientific interpretation of the saltaction of acid-producing salts. Much emphasis has hitherto been laidupon alterations in the economy of fixed base or upon the fate of thespecific ions administered. The comparative rOle of phosphate in thisprocess has received but little scrutiny, however, particularly as reflectedin the metabolism of phosphate at various levels of acid elimination.Some authors (3) have suggested that when inorganic phosphate is fed,the metabolic fate of the phosphorus is to some degree predetermined bythe potential acidity of the salt fed. Sodium acid phosphate is, indeed, anatural physiological waste product: does the administration of this acidsalt provoke diuresis or loss of fixed base? The companion buffer saltdisodium phosphate exists in all body fluids. What is the effect of itsadministration on bodily economy?
PLAN OF STUDY
In order to determine the effect of the potential acidity of ingestedphosphate upon its assimilation and subsequent fate, we have studiedthree adult humans whose clinical conditions are described in the addenda.These subjects were placed on a potentially neutral diet, low in phosphoruscontent, which was continued (essentially) unvaried throughout theexperiment. One week was allowed in each case to permit the body toreadjust itself to this constant diet before the experiment was begun.After control levels of excretion had been determined, weighed amounts ofchemically pure inorganic phosphate were added to the diet, and theresulting change in excretion observed. Three types of inorganicorthophosphate were fed, viz., sodium acid phosphate, disodium phos-phate, and an equimolecular mixture of the two. The object was toadminister as much phosphate as possible without producing catharsis.Subject RN was given these salts in sequence, so that there are twoobservations on acid phosphate (subjects WNand RN).
Because of the well recognized lag in excretion following the adminis-tration of most medication, the metabolism of phosphorus was followedafter the inorganic phosphate was omitted. In all cases, the resumptionof control excretion levels indicated that a "steady state" had again beenreached in the second period following the last in which phosphate wasfed. In this paper, therefore, the acid-base balance was struck as soonas the phosphate balance had approached its former level. It wasessential in so doing not to delay too long lest the immediate metabolicresponse to phosphate feeding be obscured by subsequent readjustments.In evaluating the response of the organism to these phosphate additions,it is assumed that the effect of the control diet on the total metabolismremained constant; and that increases in the potential acidity of the diet(in the form of added phosphate) would be reflected by correspondingalterations in acid excretion.
392

W. T. SALTER, R. F. FARQUHARSONAND D. M. TIBBETTS
In these experiments the method suggested by Sherman and Gettler(4) for calculating the potential acidity of food-stuffs was utilized, andthe relative amounts of various food-stuffs so balanced that the totalpotential acidity (when oxidized) would be zero. The actual arithmeticaloperations and sources of error have been illustrated elsewhere (5). Theuse of such a " control " diet, constantly continued throughout the experi-ment, obviates any gross errors due to inaccuracy in the composition ofthe food. Our control diets were low in calcium and phosphorus butadequate with respect to other inorganic salts, vitamins, fat, carbo-hydrate, protein, and total caloric content.
EXPERIMENTALMETHODS
The technic followed in these experiments has been given in a de-scription of the special study ward on which our subjects were kept (6).Ammonia and titratable acidity were, as usual, determined within a fewhours after mixing of the combined twenty-four-hour urine. Thepossibility of an important change occurring under these conditions wasexcluded (7) by comparing the twenty-four-hour analysis with thesummated results of successive specimens freshly voided.
Diuresis was excluded by recording nude weight at the same time eachday, and showing this to be constant. The time of the experiments wasthe early (New England) spring months when perspiring was at a mini-mum. Basal metabolic rates were determined with the Benedict-Rothapparatus.
The analytical methods employed were outlined in our previouspublication (1). Through the courtesy of Dr. Arlie V. Bock the bloodCO2 level of subject RNwas established (with the apparatus of Neill andVan Slyke) before and at the end of acid phosphate administration.Haldane's negative experiment (8) determining the effect on blood C02 oflarge doses of basic phosphate obviated the necessity of such determi-nations in the basic phosphate experiments.
EXPERIMENTALRESULTS
Our analysis of the experimental results is based upon the assumptionthat when an organism exhibits a constant excretion in response to aconstantly continued "control " dietary regimen, additions to the dietwill be reflected by changes in excretion, the quantitative value of whichshould be measured from the original excretion-level. In presentingresults, therefore, emphasis has been laid in this paper upon intakes oroutputs over and above the corresponding figures for the preliminary"control" (basal) diet. The justification for this procedure will appearin the results cited below.
In presenting these results, furthermore, we have departed from theusual procedure of sharply separating analytical figures from the dis-
393

ACID-BASE BALANCEAND PHOSPHATEBALANCE
cussion of their significance. This method seemed advisable because thepaper is in essence a mathematical analysis of metabolic balances andderived equivalents. The massed results of the laboratory determi-nations may be had (for reference) in our previous paper (1).
I. The influence of the potential acidity of ingesta on inorganic phosphorusmetabolism
Studies on the storage of calcium and phosphorus in rickets havedemonstrated that the potential acidity of the diet is an important factorin phosphate metabolism. Zucker, Johnson, and Barnett (3) reportedthat the change in the acidity of diets from the alkaline toward the acidside might result in healing of the rachitic lesions. Conversely, McClendon(9) reported that adding alkali to a diet increased its power to producerickets. The fact that most rickets-producing diets are potentiallyalkaline is of significance.
Most illuminating from this point of view are experiments whichdetermine the fate of phosphate of known potential acidity added to aconsistently continued basal or control diet. Karelitz and Shohl (10), instudying the metabolism of phosphate in rachitic rats to whose diet (apotentially alkaline one) acid phosphate was added, found that thisaddition resulted in a reversed excretion ratio between urine and feces.In the period preceding the feeding of phosphate only 7 per cent of theexcretion was urinary, whereas with increase of phosphate in the diet theurinary moiety was about half, being increased both relatively and in anabsolute sense. Despite the fact that their animals were in a state ofphosphorus starvation, only one-fourth of the phosphate eaten wasretained on this diet (which was potentially alkaline, even though acidphosphate had been added). The possibility that the greater excretionof phosphate in the urine under a more acid regimen might be due togreater absorption from the intestines was investigated in man byZucker (11), who added NaOHand HCl to the control diet; which,however, was evidently potentially acidic as indicated by a titratableacidity of over 700 cc. N/1O acid daily. The greater absorption andretention of phosphorus under the influence of acid was also confirmed byScheer (12).
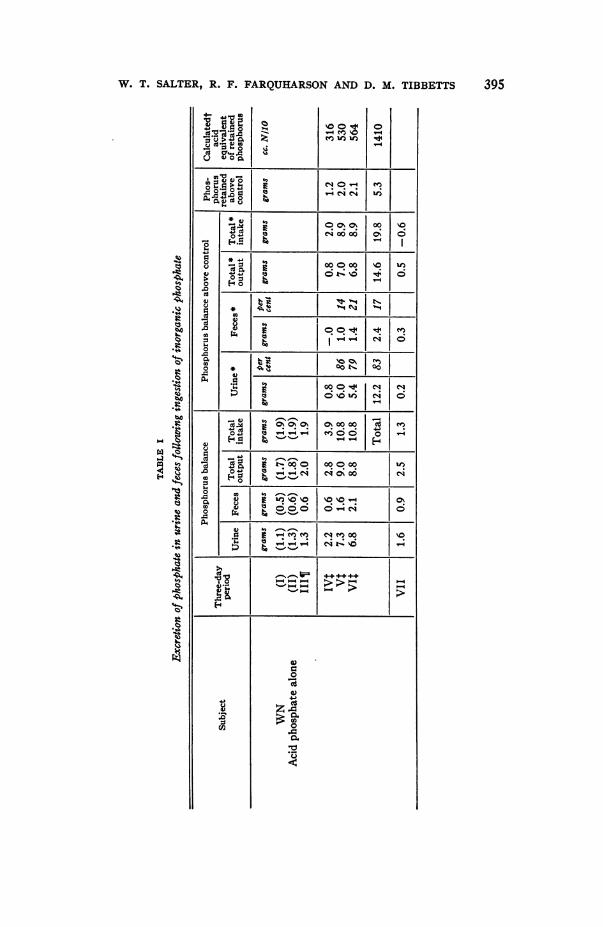
From the massed analytical results previously published (1), thephosphate determinations have been abstracted and combined in TableI to indicate the respective phosphorus balances for the three types ofsalt fed, i.e., acid, basic, and the equimolecular mixture of the two.Stress is laid upon the values headed "balance above control," becausethese derived values indicate the extent of fluctuation above the basallevel. In italics (beside the excretion figures for each three-day period)is given the relative participation (expressed as percentage) of urine andfeces, respectively, in the combined phosphate excretion for that period.
394
W. T. SALTER, R. F. FARQUHARSONAND D. M. TIBBETTS
4- 4J.0 O
4 e. 0-.I
\0 0 -Im- 0e Uf) if)
0
*)4 )41.o -. 0 0> O| u|
cd 4)
IeSXI ot -oo | 6|
0 . O -| o |
4) il> 0
,0 0*0 ~co~ ~ ~ ~ ~ ot. 0
C 00OI.I teI04~~~~~~~~~~~~~~~~~.
04. 4 °°O 0 0-1I
d~~~~~~C Ia4tJ
4)
co 4)
V o o
13 C-if# C-t! 064) .~~~~~~~C
.4
:34)
4)
00
4)
04-co
z
*t0
395
¢i
Q0c4)
CZ
Q4%3
*t
41.
Q'4)
I.)
H
'O
FN
.

ACID-BASE BALANCE
4-
Z in 14 0% 00
8 , o~ e4
-) co
CU
0 %'-Cla4)0
AND PHOSPHATEBALANCE
W- tooo4N 000 C 4'-4
1
0
I:dj0.-04 _0 C
-o-S -s bI O
4 4-
4) 0Cf ).14 4
cU
e~~' NI F-°C"| ^.c° * tr 1N1 ___ %ONt1I41)
.0
0 _______ r1 0. _
.0 -
0 e
o * $ O0o00~ N 00 _____00 00--0000j j'O+ d8~~~~~~~~~ eq C4 V-4 C) I
.0 U
d Sal r +XnI~\00 O 15tN..31
4.8 \0 00 lq.jtbu0.0\0C ) o
p4
j x o* vt-. OO OO'I)
-~~~~~~~-.d C .oo . J t1 o. oo|oo ir-4 CU OoU)0 0-i-54 i'i U-00 0
C -3 :1 c
4 q'0 00 t- .t- -\0~ 3 0%\# 00
4)4
CUE __4)gg > i- ¢
0
~~~~~~~~-4
,0:suz
UL)00
4L)4-C
coz I4
040.
a
0
UL)CU
0
0.
0
CU
396

0 Cd0 n>v onlC Xo=lsQ 0 1 t
Ca I 'lo t t
Cc*c w 18o 1v v E 1b>t1>1~~~~0
40.0 I t3 . I 11b O4
0 o 0 e n tCSei
Cdf^X4-> AX.d
397W. T. SALTER, R. F. FARQUHARSONAND D. M. TIBBETTS
Q
;i
Cd4JCd
Cd
CdCL)4J
biO
0 Cd'M --4
Cd Cd
t
00
0
cn 0= uCd W.
rn4J0
0
x
. ._
040 C:¢;4
-0C:Cdu(ACd
.00.6.40
E0N 4i
P-.xE (D
4i
1.4 CidCd =- ol
:3 mu 04) 1=0
a
E -a= UDo cdw
4.)u4)
.0(A
4- 4i wM$ 0 E
.c (L).0 0Cd .Cd .5 .0
7i .o.> a
u Cd (V w=1 0-aCa4. 4.4
u 0 a

ACID-BASE BALANCEAND PHOSPHATEBALANCE
The corrected phosphorus balance appears in the next column (next tothe last). The final column indicates the acid equivalent of the phos-phorus retained, calculated with reference to blood pH = 7.4; alkaliretention is indicated (in the basic phosphate experiment, subject RN) byminus signs.
The first two experiments (subjects WNand RN) are devoted tosodium acid phosphate, the third to disodium phosphate; and the fourthto an equimolecular mixture of the two.
When inorganic phosphate is fed, does the potential acidity of the salt fedinfluence the phosphorus balance?
In sodium acid phosphate experiment WN, 5.3 grams out of the 19.8grams of phosphorus fed were presumably retained, i.e., 27 per cent. Insodium acid phosphate experiment RN, 1.9 grams out of the 14.2 grams ofphosphorus fed were presumably retained, i.e., 13 per cent. The averageof the two experiments is 20 per cent (roughly one-fifth) presumablyretained.
In disodium phosphate experiment RN, 5.0 grams out of the 19.6grams of phosphorus fed were presumably retained, i.e., 25 per cent(roughly one-fourth).
In the equimolecular phosphate experiment LZ, 3.0 grams of the 9.9grams of phosphorus fed were presumably retained, i.e., 30 per cent(roughly one-third).
One might summarize these various results by stating that irrespectiveof the potential acidity of the inorganic phosphate fed, one-fourth of thephosphate fed is presumably retained in these relatively short obser-vations.
When inorganic phosphorus is fed, what is the partition of phosphate excretedin urine and feces?
It will be observed that considerable fluctuations occurred fromperiod to period in the division of phosphate between urine and feces. Itwill be more profitable, therefore, to consider the total excretion for eachexperiment.
In sodium acid phosphate experiment WN, 2.4 grams out of the 14.6grams of phosphorus recovered appeared in the feces, i.e., 17 per cent;leaving 83 per cent as urinary. In the duplicate experiment on subjectRN, 2.7 grams out of the 12.3 grams of phosphorus recovered appeared inthe feces, i.e., 22 per cent; leaving 78 per cent as urinary. The averagevalues for sodium acid phosphate excretion, therefore, are fecal, 19 percent (roughly one-fifth), and urinary, 81 per cent (roughly four-fifths).
In disodium phosphate experiment RN, 4.6 grams out of the 14.1grams of phosphorus recovered appeared in the feces, i.e., 33 per cent(roughly one-third); leaving 67 per cent (roughly two-thirds) as urinary.
398

W. T. SALTER, R. F. FARQUHARSONAND D. M. TIBBETTS
In the equimolecular mixture experiment LZ, 1.7 grams out of the6.9 grams recovered appeared in the feces, i.e., 25 per cent (roughly one-fourth); leaving 75 per cent (roughly three-fourths) as urinary.
One might summarize these results by stating that irrespective ofthe potential acidity of the extra inorganic phosphate fed, one-fourth ofthe excreted phosphorus is fecal. During the control periods, on apotentially-neutral mixed diet, one-third of the total phosphorus ex-cretion was fecal.
The net result of the phosphorus balance presented in Table I is(first) that irrespective of the potential acidity of the salt fed, one-fourthof the phosphorus is retained; and (secondly) that irrespective of thepotential acidity of the salt fed, one-fourth of the excreted phosphorus isfecal.
II. The influence of the potential acidity of iigesta upon total fixed basemetabolism
The relation of phosphate excretion to the excretion of total acid,especially from the viewpoint of its bearing on urinary acidity, hasoccupied the interests of many investigators of acid-base economy.Folin (13) in 1903, in discussing the acidity of urine, pointed out theconvenience of the assumption that the titratable acidity of urine is dueto acid phosphate. The classical work of Henderson (14) on the ex-cretion of acid catabolites emphasized the importance of using thehydrion concentration of the blood as a point of reference in titrating acidexcretion; and clarified the significance of urinary hydrion concentrationin terms of the titration curve of orthophosphoric acid. The chemicalmechanisms by which phosphate is metabolized, however, demand furtherclarification.
The neutralization of phosphate within the bowelWhenan inorganic salt or acid is fed, fixed base is added or withdrawn
by the intestinal juices so that the potential acidity of the original salt isaltered. If the potential acidity be far removed from neutrality, thisprocess may be spoken of as "neutralization" of the salt by the bowel.The analogy is admittedly crude: first, because the pH to which the salt isneutralized is not known exactly; and secondly, because complex organicbuffer-substances within the gut make exact physicochemical reasoningimpossible. Nevertheless, such a concept may be profitably applied tothe fate of ingested phosphate when analyses are made on aqueousextracts of fecal ash by assuming that "neutralization " occurs withreference to blood pH = 7.4, or intestinal pH = 8. It is not easy todecide which of these hydrogen ion values is the preferable referencepoint. Fortunately, however, the base bound by phosphate betweenthese two limits is relatively small and either point may, therefore, beused for practical purposes.
399

ACID-BASE BALANCEAND PHOSPHATEBALANCE
The original potential acidity of the phosphorus found (in feces) can becalculated as its base equivalent, i.e., 1.8 times the mols of phosphorusinvolved. When fecal fixed base is determined, the extent of "neutral-ization" of the unabsorbed inorganic phosphate may be estimated.From the massed analytical data previously published (1), the values forfecal phosphorus and fecal fixed base have been abstracted; and arepresented in Table II for comparison. Because of fluctuations fromperiod to period only totals are discussed.
In sodium acid phosphate experiment WN, the extra fixed base (967cc. N/10) more than neutralized the potential acidity (b) of the phosphatepresent (637 cc. N/10, referred to pH = 7.4). The extra base (c) is infact greater than the molal equivalent (a) of the extra phosphoruspresent (768 cc. M/10). In sodium acid phosphate experiment RN, theextra fixed base (897 cc. N/1O) more than neutralized the potential acidity(b) of the phosphate present (718 cc. N/10, referred to pH = 7.4). Theextra base in this instance is approximately equal to the molal equivalentof the extra phosphorus present (865 cc. M/10).
These results may be explained on the basis that the acid phosphatewhich escaped absorption (or was re-excreted) was excreted chiefly in theform of disodium phosphate. The figures, indeed, indicate for WNafraction excreted as tertiary phosphate, and for RN a small fractionexcreted as primary phosphate. Such differences, however, are probablynot significant in a metabolic procedure of this sort.
In the disodium phosphate experiment RN, the extra fecal phosphorus(a = 994 cc. M/10) would theoretically have carried with it, if excretedunchanged, 1988 cc. N/tO fixed base (i.e., sodium). The extra fixed base(c) actually found (2167 cc. N/tO) is in fair agreement, and indicates thatthis phosphate was excreted chiefly in the form in which it was fed.
The conclusion indicated by these three experiments is that fecalinorganic phosphate was excreted chiefly as the disodium salt irrespectiveof the form in which it was fed. It is interesting that Berg (15) believedcalcium phosphate to be excreted by bowel in tribasic form. It is clear,however, that such a condition cannot be ascribed to the total fixed base ofthe feces when phosphate is fed. The fact that calcium is a weaker basethan sodium may explain this apparent discrepancy.
The neutralization of phosphate in the urineIn the preceding section, the base equivalent of the fecal phosphate
excreted was found to serve as a rough measure of the extra fixed baseexcreted (by bowel) when inorganic phosphate was fed. In the case ofurinary excretion, an even more precise relationship exists-at least foracid phosphate. For the sake of clearness and brevity the analyticalvalues for individual successive periods have been omitted from TablesIII and IV, and only the summated values (representing nine consecutive
400

W. T. SALTER, R. F. FARQUHARSONAND D. M. TIBBETTS 401
LZ.0,0
o
0H-
a In 00o V# )o --
0%
C\00
0H
Id,:0 to oo40
aS Os oo ,v No o
0J 0
d s d oo| oo| r
0
C)03as ,> a>
'0 *>
0A4¢dA S I '4 S|0'0 a4Z
U)-r)-.0004f)0%>*O 0 %0) e4-ie~
4i cd1w-4 -0Cm4 0
St10-c0 --:-> 0
U H
5. t0c.o0
.0 -3Cdc0d0 -
C)
*0Un
CuU-)co0
V
0Clcn
4-)Cd
01U)0
Cu
Ei._
la0
C,)

ACID-BASE BALANCEAND PHOSPHATEBALANCE
0ON m to r-so o0000o o
Cd0H
=1N. (7"> too to ;So
oo ooo 0 i, t e
0~~~~~~~%
V4-) 0* 00 No(D
,v,vV3 ON CN0%~0
0d404ru°E ffi i e
'-
.n 0 00
0~~~~~~~U4) HW-
00g~~~~~
co-o
A0ao, > ce0 00 0'-4
e.0
-0
aL)
04-
Cl)0
(A0:E~~~~~~E
.:
402
*o
_0U)1.'
%..
*ltz;a)
II
¢.
u0
0
a .o n-0
'. >
ooSiCo
0 'n0 c0, a)
1- 0 cd
* 4-4 CIS

W. T. SALTER, R. F. FARQUHARSONAND D. M. TIBBETTS
days) are presented. Because of lack of adequate analytical data, theintermediate experiment with an equimolecular mixture of phosphates isnot discussed.
Acid phosphate in urineWhen an acid salt is absorbed and excreted, the kidney must excrete
additional fixed base in order to neutralize it to the pH of the urine. Theamount of extra fixed base excreted would be the base equivalent of thesalt excreted provided that the kidney did not exercise its powers of base-conservation either by increased titratable acidity or by ammonia output.Titratable acidity might, indeed, be expected to play a large r6le in theelimination of phosphate, but the observations of Marriott and Howland(16) would lead one to expect the amount of extra ammonia to be rathersmall. The sum of these two increases should indicate the extra fixedbase saved by the kidney, and this sum should be subtracted from thebase equivalent of the extra urinary phosphate in order to estimate theincrease to be expected in urinary fixed base. When this is done, inTable III and Figure 1, comparison with the analytical results shows a
TABLE III
The urinary fixed base response to acid phosphate feeding can be predicted quantitatively
Patient WN Patient RN
Excretion values above control levels Extra base Extra fixed Extr base Extra fixedexcreted as base excreted as basephosphate conserved phosphate conserved
cc. NIIO cc. NIIO cc. NIIO cc. NIlOExtra phosphorus excreted, P, in cc. M/10... 3927 3110
Its base-equivalent, 1.8 X P.7190 5698
Extra ammonia excreted, N 465 - 20Increased titratable acid, T.+ 1868 + 1230
Extra base saved, N + T.2333 2333 1210 1210
Predicted excretion of fixed base= 1.8 X P-(N + T) 4857 4488
Actual analytical finding .4615 4290
difference which is not over 5 per cent in either of the two experimentspresented. The difference, in fact, is probably less than the maximalerror to be expected from the combination of chemical analyses involved.The detailed analytical figures are appended in Table IIIA.
This calculation involves the tacit assumption that the underlying" control " acid-base metabolism (in response to the basal " control " diet)
403

ACID-BASE BALANCEAND PHOSPHATEBALANCE
remains undisturbed by the addition of phosphate. The results make itlikely that the premise is justified.
I-c0m
0
P-
0
0
Z\tVt
Urinary Acid-Base Balance with-Acid Phosphate M\edication
FIG. 1. PATIENT WN-THEACTUAL INCREASE IN URINARY FIXED BASE ISAPPROXIMATELYEQUIVALENTTO THAT THEORETICALLY PREDICTED.
The control excretions are pictured at the left of the chart. The super-imposed phosphorus excretion is indicated by the hatched areas.
Basic phosphate in urineThe foregoing prediction of fixed base excretion depended upon the
assumption that the underlying general trend of inorganic salt metabolismremained undisturbed by the feeding of acid phosphate. When given a
constant control diet, each subject had eventually arrived at a plateaulevel of excretion for the several dietary constituents measured. The
0I)
I-i
OL0
|;lo
404

W. T. SALTER, R. F. FARQUHARSONAND D. M. TIBBETTS
0"
-.
% t- -.4 V-'u N'40
M000~'-4@SWo o ~~~~oON
g Eg 0 %|NNS
e ¢0
.d Cd C4 C4C4 0
i! ] -^ ( >> 5 4C4 V.
0 b
Cu) gl,uI.eg
,0
03euo0t.- 00
.0
0~~~~~~~0
in
4):3
;u
z
405
oe
0o
x
4)C.)
"at
1*4
¢'41
rz
'ul

ACID-BASE BALANCEAND PHOSPHATEBALANCE
-4 00 0 40
';2 oo o°o g o
II
amenMwa Z- IRWo qd 0 ~o|00004i t o co % t
o d Cd : O eq 0°4tX i0
W~~~~~~~~~~~I.E ~~~~!NOe.0 0
00~~~~~~~iA0X $. m0
0~~~~~~~~~0
u, 'd~
> F 4 :3 C~43 ,
.0
4i ~ ~ ~ -4
0~
.C z
406
'I)
'.4
0
U)
144
_4
,_
1 4-Ot." ti m
(d.0

W. T. SALTER, R. F. FARQUHARSONAND D. M. TIBBETTS
various factors which had determined the height of the plateau level are,of course, no better understood than are the factors which determined thephosphorus balance itself. The addition of acid phosphate to the controldiet, merely produced an incremental change in the excretion plateauvalues which was assumed to be additive.
This assumption could not be maintained, however, when basicphosphate was fed. Table IV indicates that a fundamental shift in the
TABLE IV
(Patient RN)-Phosphate balance and acid-base balance following the ingestion of disodiumphosphate
Output
Intake Urine. Feces. Total. Balance RemarksChange Change Changefrom from from
control control controllevel level level
Phosphorusgrams... 19.6 9.5 4.6 14.2 (4.9)*
cc. N/tOanion. . . 11560 5600 2712 8320 (2890)*
Per cent... 100 49 24 72 28
Titratable acid Gamble's " base economy."cc. N/1O... -1090 -1732 642 More alkalinity appears in
the urine than was fed
Ammoniacc. N/1O... -1041
Titratable acid Henderson's "total acid," theplus am- best measure of saving of fixedmonia base, apparently indicates
cc. N.I.... -2773 much less saving of fixed base
Fixed base A large positive fixed-basecc. N1...... 12670 2565 2167 4732 7938 balancePer cent... 100 20 17 37 63
Total anion Gamble's "total acid" drops,(calculated).. -208 even though there are 5600
milliequivalents additionalHPO4present
* This figure has been modified by a slight correction for refused food.
electrolytes of the body occurred when the alkaline salt was administered.In short, the fundamental excretion plateau was altered. That this wasso is suggested by several facts shown in the table. More titratablealkalinity appeared in the urine than the alkali equivalent of the salt fed.Henderson's "total acid" (14), which is the best measure of saving of
27
407

ACID-BASE BALANCEAND PHOSPHATEBALANCE
fixed base, indicated less base economy than before; but on the contrarythe actual analyses showed a large positive fixed base balance. More-over, Gamble's "total acid" (17) (i.e., total anion) dropped from itscontrol le'vl 1, despite the fact that much extra phosphate ion was present.
This last fact makes it seem likely that the extra phosphate wasexcreted in preference to other anions (e.g., chloride or carbonate).Unfortunately, it was not possible in this study to have a completeanalytical synopsis of anion excretion. Such observations would ofnecessity entail analyses for the high carbonate content of alkaline urines(described by Gamble (18)). Our findings, inadequate as they are, arereported here to show the need of more detailed study, which the phe-nomenon merits in view of its bearing upon the effect of alkaline diuretics.
DISCUSSION
This investigation was undertaken with the supposition that phos-phate and acid exerted reciprocal effects upon their mutual and respectivemetabolisms. The object of this study was to measure the extent of thismutual influence when inorganic phosphate was fed to adult humans overa relatively short period.
The first question to be answered was: Howdoes the potential acidityof the inorganic phosphate fed affect the assimilation of phosphorus?The answer given by these experiments is essentially negative. Nodefinite influence of potential acidity could be discerned upon theabsorption or retention of inorganic phosphorus.
The second question to be answered was: How does the potentialacidity of the inorganic phosphate fed affect the fixed base metabolismwhile the extra phosphate is being excreted? In analyzing this problem,two rational mechanisms were encountered which explained quantitativelythe excretion of total fixed base (i.e., cation considered in its r8le as anelectrolyte, apart from its alkaline properties). The first of these assumedthat fecal phosphate was excreted chiefly as disodium phosphate, re-gardless of its potential acidity when fed. The second of these assumedthat when the kidney failed to neutralize acid phosphate completely(either with ammonia or by altering titratable acidity), the deficiencywas made up quantitatively by draught upon the body's reserve stores offixed base.
It is of passing interest that the subjects here described apparentlyretained about one-fourth of the phosphate fed (irrespective of thepotential acidity of the salt administered). Of more moment is thediscrepancy between the respective amounts of acid (or base) recoveredand the corresponding portions of phosphate recovered. In the acidphosphate experiments four-fifths of the extra phosphate was found inexcreta, in which only one-third of the corresponding acid could bemeasured. In the basic phosphate experiment, three-fourths of the
408

W. T. SALTER, R. F. FARQUHARSONAND D. M. TIBBETTS 409
administered phosphate was recovered, but only about one-third of thefixed base.
CONCLUSIONS
The influence of the ingestion of sodium acid phosphate and disodiumphosphate on the balance of inorganic electrolyte was studied in subjectson a constant, potentially neutral diet.
1. About one-fourth of the phosphate fed was stored. Approximatelyone-fourth of the excess phosphate excretion was fecal.
2. Fecal inorganic phosphate was excreted chiefly as the dibasic saltirrespective of the form in which it was fed.
3. With acid phosphate there was an increased excretion of inorganicbase which was mainly urinary. It was equivalent to the theoreticalamount of base necessary to neutralize the excess phosphoric acidexcretion, not conserved by titratable acidity and ammonia.
4. This simple mechanism, however, did not hold when disodiumphosphate was administered. The mechanisms here involved are notyet obvious.
BIBLIOGRAPHY
1. Farquharson, R. F., Salter, W. T., and Aub, J. C., J. Clin. Invest., 1931, x,251. Studies of Calcium and Phosphorus Metabolism. XIII. TheEffect of Ingestion of Phosphates on the Excretion of Calcium.
2. Gamble, J. L., Blackfan, K. D., and Hamilton, B., J. Clin. Invest., 1924-5,i, 359. A Study of the Diuretic Action of Acid-Producing Salts.
3. Zucker, T. F., Johnson, W. C., and Barnett, M., Proc. Soc. Exp. Biol. andMed., 1922, xx, 20. The Acid-Base Ratio of the Diet in RicketsProduction.
4. Sherman, H. C., and Gettler, A. O., J. Biol. Chem., 1912, xi, 323. TheBalance of Acid-Forming and Base-Forming Elements in Foods, and itsRelation to Ammonia Metabolism.
5. Salter, W. T., Fulton, C., and Angier, F., J. Nutrition, 1931, iv, 1. Studiesof Calcium and Phosphorus Metabolism. XI. The Calculation of Acid-Base Content of the Diet.
6. Bauer, Walter, and Aub, Joseph C., J. Am. Dietet. Assoc., 1927, iii, 106.Studi_s of Inorganic Salt Metabolism. I. The Ward Routine andMethods.
7. Salter, W. T., Farquharson, R. F., and Tibbetts, D. M., Observations onUrinary Acid and Ammonia Excretion with Controlled Diet. To bepublished.
8. Haldane, J. B. S., J. Physiol., 1921, lv, 265. Experiments on the Regula-tion of the Blood's Alkalinity. II.
9. McClendon, J. F., Am. J. Physiol., 1922, lxi, 373. Calcium PhosphateMetabolism in the Diagnosis of Rickets.
10. Karelitz, S., and Shohl, A. T., J. Biol. Chem., 1927, lxxiii, 665. Rickets inRats. II. The Effect of Phosphate Added to the Diet of RicketicRats.
11. Zucker, T. F., Proc. Soc. Exp. Biol., and Med., 1921, xviii, 272. The Rela-tion of Acid Base Equilibrium in the Body to Excretion of Phosphorusand Calcium.
ACID-BASE BALANCEAND PHOSPHATEBALANCE
12. Scheer, K., Jahrb. f. Kinderh., 1922, xcvii, 130. Die Beeinflussbarkeitder Spasmophilie durch Salzsauremilch.
13. Folin, Otto, Am. J. Physiol., 1905, xiii, 66. Laws Governing the ChemicalComposition of Urine.
14. Henderson, L. J., J. Biol. Chem., 1911, ix, 403. A Critical Study of theProcess of Acid Excretion.
15. Berg, Ragnar, Biochem. Ztschr., 1911, xxx, 107-143. Ober die Ausscheid-ung von per os eingefuihrten Phosphaten, besonders der Calcium-phosphate.
16. Marriott, W. McK., and Howland, John, Arch. Int. Med., 1918, xxii, 477.The Influence of Acid Phosphate on the Elimination of Ammonia in theUrine.
17. Gamble, J. L., Ross, G. S., and Tisdall, F. F., J. Biol. Chem., 1923, lvii, 665(footnote 10). The Metabolism of Fixed Base during Fasting.
18. Gamble, J. L., J. Biol. Chem., 1922, li, 295. Carbonic Acid and Bicarbon-ate in Urine.
DESCRIPTION OF PATIENTS
A brief description of each of the patients used in this investigation follows:WN: A married female of 34 years of age, weighing 89 kilos, suffering from
chronic atrophic arthritis of 2 years' duration. (M. G. H. number 289324.)RN: A single female of 39 years of age, weighing 56 kilos, suffering from
rheumatic heart disease (mitral stenosis), chronic bronchitis, and bronchialasthma. During the period of observation she had no cough, her chest wasclear, and there were no signs of myocardial failure. (M. G. H. number286369.)
LZ: A male, aged 18, weighing 60 kilos, recovering from chronic multipleneuritis; confined to bed because of weakness of extremities, but feeling well.(M. G. H. number 274029.)
410