phar 722 pharmacy practice iii obesity and weight control spring 2006
TRANSCRIPT

Phar 722Pharmacy Practice III
Obesity and Weight Control
Spring 2006
Study Guide for the Material on Obesity1. For obesity, know: a. causes; b. reasons for the increase in numbers of obese individuals;
c. role in maintaining good health;d. potential role of peroxisomes and hormonal/cytokine control.
2. What are the problems with maintaining desired weight?
3. For reducing diets, know:a. their biochemical validity, where applicable;b. their relative nutritional value;c. properly designed liquid diets;d. criteria for determining if a diet is a “fad” diet.
4. For artificial sweeteners and fat replacements, know:a. their underlying chemistry (peptide, carbohydrate, heterocycle, etc.)b. the underlying chemistry of the fat replacements.
5. Be able to state the medical outcomes from bariatric surgery and liposuction.
6. Be able to do the following calculations: a. kcal (Calorie) yield/gram of fat, protein and carbohydrate in a foodb. BMI

Nothing is Really New! It is a commonly received notion that hard study is the unhealthy
element of college life. But from tables of mortality of Harvard University, collected by Professor Pierce from the last triennial catalogue, it is clearly demonstrated that the excess of deaths for the first 10 years after graduation is found in that portion of each class inferior in scholarship. Every one who has seen the curriculum knows that where Æschylus and political economy injures one, late hours and rum punches use up a dozen, and that the two little fingers are heavier than the loins of Euclid. Dissipation is a swift and sure destroyer, and every young man who follows it is, as the early flower, exposed to untimely frost. A few hours of sleep each night, high living and plenty of smashes make war upon every function of the human body. The brain, the heart, the lungs, the liver, the spine, the limbs, the bones, the flesh, every part and faculty are over tasked, worn and weakened by the terrific energy of passion loosed from restraint until, like a dilapidated mansion, the earthly house of this tabernacle falls into ruinous decay.
—Scientific American, September 1918

Not all fat is created equal.
Saturated, unsaturated, what’s the difference?...You can’t pack as much fat into a serving of food made with unsaturated fats and you can’t store as much extra weight in your body when the triglycerides are kinky. With fats, kinky is good, straight is bad.”
—Chemical & Engineering News, August 12, 2002, p 64.

Obesity Trends* Among U.S. AdultsBRFSS, 1985
No Data <10% 10%–14%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)

Obesity Trends* Among U.S. AdultsBRFSS, 1986
No Data <10% 10%–14%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)
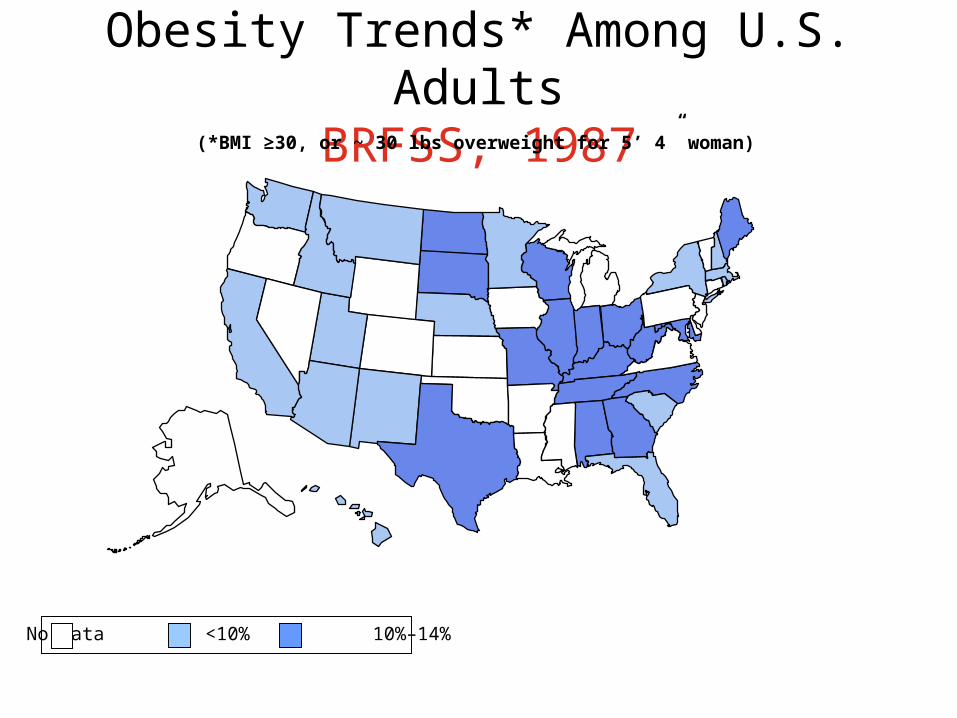
Obesity Trends* Among U.S. AdultsBRFSS, 1987
No Data <10% 10%–14%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)

Obesity Trends* Among U.S. AdultsBRFSS, 1988
No Data <10% 10%–14%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)

Obesity Trends* Among U.S. AdultsBRFSS, 1989
No Data <10% 10%–14%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)

Obesity Trends* Among U.S. AdultsBRFSS, 1990
No Data <10% 10%–14%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)

Obesity Trends* Among U.S. AdultsBRFSS, 1991
No Data <10% 10%–14% 15%–19%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)

Obesity Trends* Among U.S. AdultsBRFSS, 1992
No Data <10% 10%–14% 15%–19%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)

Obesity Trends* Among U.S. AdultsBRFSS, 1993
No Data <10% 10%–14% 15%–19%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)

Obesity Trends* Among U.S. AdultsBRFSS, 1994
No Data <10% 10%–14% 15%–19%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)
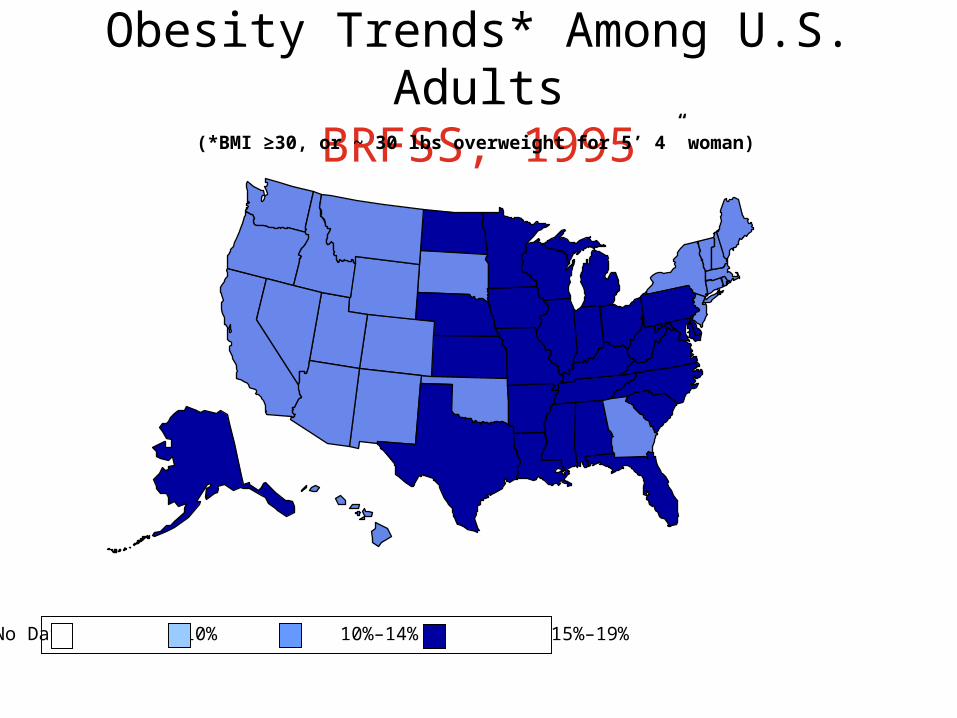
Obesity Trends* Among U.S. AdultsBRFSS, 1995
No Data <10% 10%–14% 15%–19%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)

Obesity Trends* Among U.S. AdultsBRFSS, 1996
No Data <10% 10%–14% 15%–19%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)

Obesity Trends* Among U.S. AdultsBRFSS, 1997
No Data <10% 10%–14% 15%–19% ≥20
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)

Obesity Trends* Among U.S. AdultsBRFSS, 1998
No Data <10% 10%–14% 15%–19% ≥20
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)

Obesity Trends* Among U.S. AdultsBRFSS, 1999
No Data <10% 10%–14% 15%–19% ≥20
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)
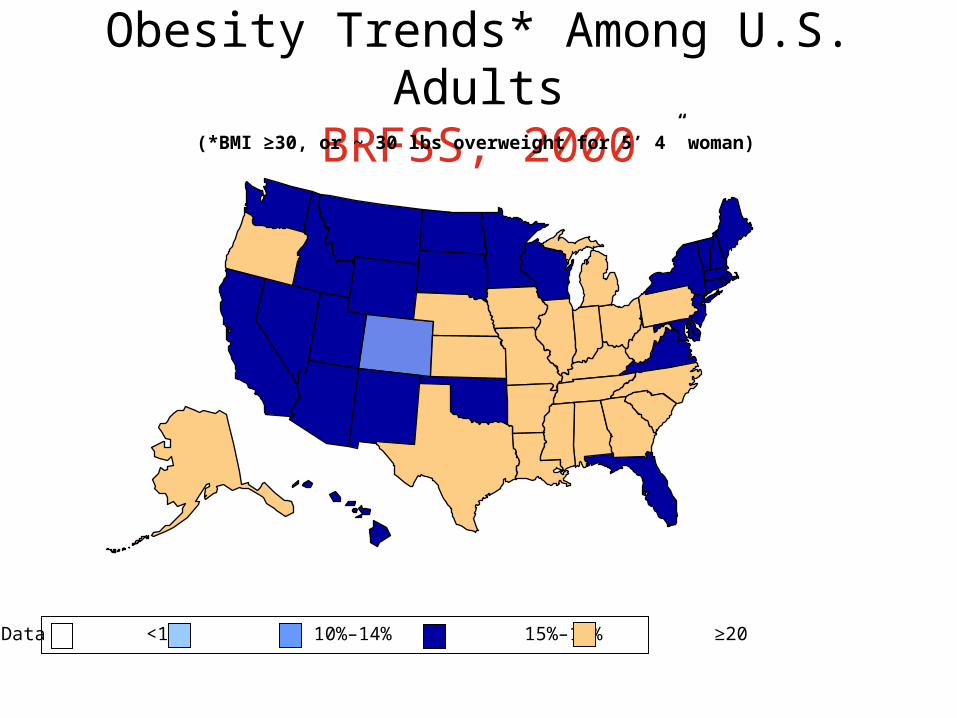
Obesity Trends* Among U.S. AdultsBRFSS, 2000
No Data <10% 10%–14% 15%–19% ≥20
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)
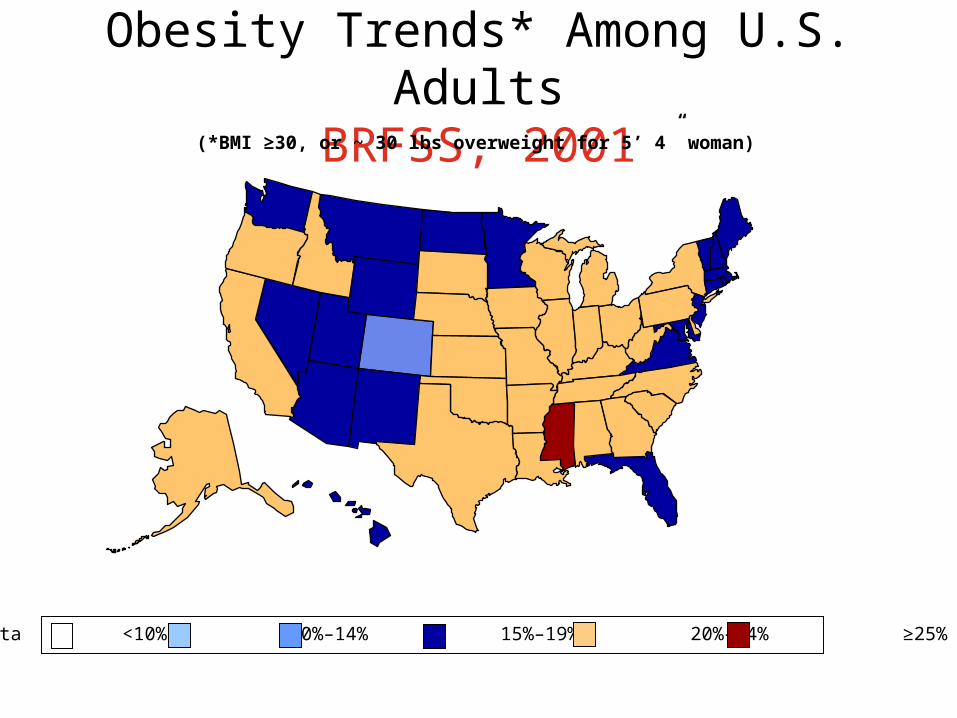
Obesity Trends* Among U.S. AdultsBRFSS, 2001
No Data <10% 10%–14% 15%–19% 20%–24% ≥25%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)

Source: Behavioral Risk Factor Surveillance System, CDC
(*BMI 30, or ~ 30 lbs overweight for 5’4” person)
No Data <10% 10%–14% 15%–19% 20%–24% ≥25%
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” woman)
Obesity Trends* Among U.S. AdultsBRFSS, 2002
No Data <10% 10%–14% 15%–19% 20%-24% 25%
Source: Behavioral Risk Factor Surveillance System, CDC
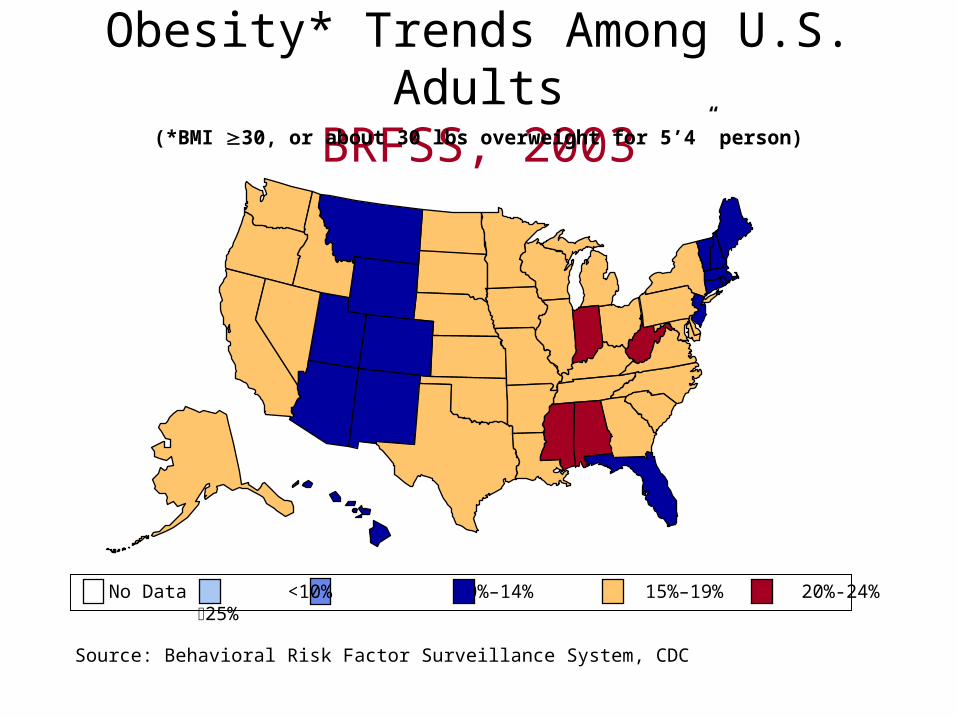
Obesity* Trends Among U.S. AdultsBRFSS, 2003(*BMI 30, or about 30 lbs overweight for 5’4” person)

Obesity is a Global Problem!

What is Historical Ideal Weight?
• Examine the female figure in the Renaissance-era paintings.– They would not be hired as today’s fashion
models.
• Who were the ideal male and female, particularly in the lower economic groups?– Male: Somewhat overweight (paunch) because it
meant the male could afford food.– Female: Husky because she could bear children
and return to farmwork or maintain the household.

What is Ideal Weight-Today?• In the United States, this concept was
originally developed by the Metropolitan Life Insurance Co. who developed a set of tables that were the standard used by physicians and dieticians. These may be too conservative. The body mass index (BMI) is the current standard, but the numbers for all indices are based on retrospective studies.

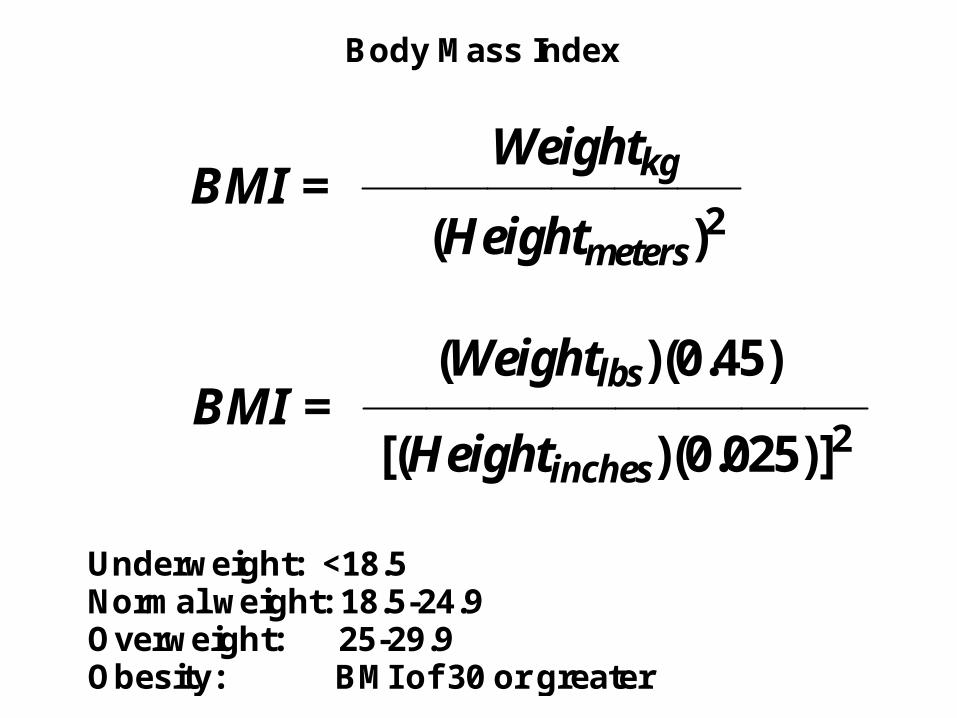
Body Mass Index
BMI =Weightkg
(Heightmeters)2
BMI =(Weightlbs)(0.45)
[(Heightinches)(0.025)]2
Underweight: <18.5Normal weight: 18.5-24.9Overweight: 25-29.9Obesity: BMI of 30 or greater


Women’s Health Initiative Results• Among post menopausal women, a low-fat dietary pattern did
not result in a statistically significant reduction in invasive breast cancer risk over an 8.1 year average follow-up period.– JAMA, 295: 629-642, 2006
• In this study, a low-fat dietary pattern intervention did not reduce the risk of colorectal cancer in postmenopausal women during 8.1 years of follow-up.– JAMA, 295: 643-654, 2006
• Over a mean of 8.1 years, a dietary intervention that reduced total fat intake of vegetables, fruits and grains did not significantly reduce the risk of CHD, stroke, or CVD in post menopausal women and achieved only modest effects on CVD risk factor, suggesting that more focused diet and lifestyle interventions may be neededto improve risk factors and reduce CVD risk.– JAMA, 295: 655-666, 2006

Why so many diseases associated with obesity?
• Adipocytes make fat a very dynamic tissue.• Every adipocyte is serviced by capillaries.• Found in adipose tissue is a large
concentration of macrophages.• Between the adipocytes and macrophages,
there is formation and release of:– Leptin– Resistin– TNF-α (Tissue Necrosis Factor)– IL-6 (Interleukin-6)
• Adipocyte contain peroxisome-linked steroid receptors.
Alternate Measure of Obesity “Waist to Hip Ratio”
Narrowest area of waist in inchesWidest area of hips in inches
Guidelines state the male WHR should be less than 0.95 and female less than 0.80. Some research shows that people with “apple-shaped” bodies (with more weight around the waist) have visceral fat and face more health risks such as Type 2 Diabetes, hypercholesterolemia, and heart disease as compared with those with “pear-shaped” bodies who carry more weight around the hips and have subcutaneous fat.NOTE: Liposuction does not normally remove visceral
fat.

Visceral versus Subcutaneous Fat
Keep a Sense of Perspective• Several health professionals now are looking at
weight as one of several health variables. Other variables include:– Normal or elevated serum lipid levels– Maintain an active physical life style– Normal blood pressure– Does NOT smoke– Does NOT show a family history of type 2 diabetes or heart
disease
• This person may not have to be concerned even if the height-weight tables or the person’s BMI indicate being overweight. The type of food being consumed is important.
• Weight reduction is indicated for people with the listed risk factors.
Causes of Obesity• Excess Adipose Tissue
– This is based on a model which states that the number of adipocytes will stay constant. The more adipocytes people form as youngsters, the more will be the problems with weight control. Adipocytes can be thought of as fuel storage tanks. They are designed to store triglycerides (fat). We can empty them and, thereby, lose weight, but the empty adipocytes will fill back up with consumption of excess calories.
– There is lack of agreement as to the age when the number of adipocytes becomes critical. At one time pregnant women were told that they should not gain more than 20 lbs during their pregnancy. Sometimes this limitation led to malnourished infants. After birth, the first two years may not be critical although eating habits and taste development may be important variables.

Causes of Obesity-Continued
• Shifts in Eating Habits– On the average Americans have increased
their caloric consumption by about 100 Calories (kcal) each day. Paralleling this increase is a decrease in physical activity or increase in sedentary lifestyle. This is happening to both adults and children.
• See picture from our local newspaper.


100 Cal/day excess• Do the following calculation:
• 100 Cal/day x 365 days/year = 36,500 Cal/year
• 36,500 Cal/year ÷ 7,000 Cal/lb = 5 lbs/year
• 5 lbs/year x 20 years = 100 lbs weight gain
• Exacerbating Variable– As we age, we need fewer daily calories to
maintain our weight. (See later slide.)

Impact of Sedentary Behavior
• Science (307, 530-531, January 28, 2005) carried a report that sedentary behavior in individuals prone to gain weight can result in an excess of 350 Calories per day.

Note decrease in dietary
calcium.
Fructose has beenImplicated as a cause of obesity.


Causes of Obesity-Continued
• Social Class– This is controversial, but the facts are that individuals
in the lower economic classes have a greater problem with controlling body weight than those in the upper economic class. There are a variety of explanations ranging from a poor understanding of good eating habits, lack of access to a variety of foods particularly in the inner city where there is a shortage of large food markets, to other medical problems which may make it difficult to earn a decent wage and have the money to purchase a variety of nutritious foods.

Causes of Obesity-Continued
• Ethnicity (Genetics?)– There is evidence that within the United States,
obesity is more likely found in specific ethnic groups. Part of this may be related to economic social class described in the preceding section. This is not the complete answer.
– Others argue from an evolutionary viewpoint. These groups are better able to survive famine because they use their food calories more efficiently. Some call this the “thrifty gene theory.” When foods become more readily available, their metabolism still behaves as if famine is eminent.
Causes of Obesity-Continued
• Hormone Imbalances– This can be quite complex and range from
hypothyroidism, pituitary imbalances, diabetes, estrogen imbalances, etc.

Genetics and Obesity
• Overweight parents produce overweight children– It must be remembered that it is only in recent human
history that we have had an abundance of food whenever we want it. Thus, our ancestors who had adipose tissue had better chances of surviving a famine. Heavier women had enough resources to nurse their infants and survive to care for the child and give birth to another infant. Remember that the location of body fat (adipocytes) is important. Adipose tissue in the hips, buttocks and thighs cause fewer complications than adipose tissue in the abdominal region. This is an example of the thrifty gene model.

Genetics and Obesity-Continued• Fat Gene Model
– It has been observed that individuals consuming identical diets and participating in identical physical activity will not produce the same weight gain or loss. Based on the brown fat model in rodents, it has been assumed that humans can "burn off" excess calories rather than always storing them as triglycerides in adipocytes.
– Recently, there are reports of a gene that controls the proton flux
across the mitochondrion inner membrane. When excess calories are consumed, a protein that uncouples oxidative phosphorylation is synthesized. Remember that in uncoupling oxidative phosphorylation, the respiratory chain continues to receive electrons from aerobic glycolysis, β-oxidation and the Krebs Cycle and reduce oxygen, but no ATP is produced. The oxidative reactions continue because there is no ATP build up to inhibit the ATP synthetase enzymes and stop the reaction.
– Individuals lacking the ability to make this protein produce ATP which, as ATP concentration increases, stops the Krebs Cycle by feedback control. Thus, in these individuals excess food is converted to triglycerides rather than being "burned off."

Thermogenesis

Possible Key Receptors• Peroxisome proliferator-activated
receptors (PPAR)
• What are Peroxisomes?– These are subcellular organelles.
• What are the functions of Peroxisomes?– glycerolipid synthesis– cholesterol biosynthesis– cholesterol breakdown forming bile acids– fatty-acid β-oxidation (w/o ATP production)

Classification of PPARs• PPARα
– Found in cardiac muscle cells and those organs where gluconeogenesis occurs (liver, intestine, renal cortex)
– Prefers polyunsaturated fatty acids.– Leukotriene B4 (LTB4) is a “potent” natural
ligand. (NOTE: LTB4 is an integral part of the inflammatory process.)
– Has anti-inflammatory properties.– The fibric acids (indicated for
hypertriglyceridemia) - gemfibrozil (Lopid™) and fenofibrate (Tricor™) - act at this receptor.

Classification of PPARs-continued• PPARβ
– Activated by fatty acids, but its function(s) is/are not well understood.
• .PPARγ– Found in white adipose tissue and immune cells.– Considered to be the “master regulator” of adipocyte
differentiation.– Has antiinflammatory properties.– The thiazolidinediones (indicated for insulin resistant
type 2 diabetes) - rosiglitazone (Avandia™) and pioglitazone (Actos™) act at this receptor.

More on PPARs• PPARγ Coactivator 1 (PGC-1)
(R. Taylor, New England Journal of Medicine, 350:7, 639-641, February 13, 2004.)
• A polymorph of the coactivator has been found in patients with type 2 diabetes. Overwight people with a family history of type 2 diabetes have decreased expression of PGC-1 even when glucose tolerance still is normal.
• One manifestation of the PGC-1 polymorph is significantly reduced mitochondria activity. This leads to lipid accumulation and might partially explain insulin resistance.

Hormones/Cytokines and Obesity
• Insulin – required for– Transport of glucose into muscle and adipose
tissue.• Muscle: Glucose either is stored as glycogen or
metabolized in the aerobic and anaerobic glycolytic pathways.
• Adipocyte: Glucose can be aerobically metabolized, converted to triglyceride or interconverted via the pentose phosphate pathways.
– Required for release of dietary triglycerides from chylomicrons and endogenous triglycerides from VLDL.
• Hypertriglceridemia is one of the complications seen in uncontrolled diabetes

Hormones/Cytokines and Obesity-continued
• NOTE: Much of the work with cytokine role in obesity is done with mice. There have been problems extrapolating the mice results with pharmacological studies in humans.
• Leptin– This cytokine (adipokine) is synthesized primarily in adipose tissue and released from
that tissue. It travels to the hypothalamus to “inform” the body about the quantity of fat stores in the body. In mice, leptin suppresses appetite. Unfortunately, the situation appears more complicated in humans. Nevertheless, some forms of obesity may be caused by defects in the gene that forms leptin or in the cytokine’s ability to communicate with the hypothalamus.
• Resistin– This cytokine (adipokine) is synthesized in adipose tissue in mice and macrophages
in humans. It maintains blood glucose levels during fasting. In obesity, it may contribute to insulin resistance seen in Type 2 Diabetes.
• Ghrelin– First discovered in 1999, it is secreted primarily by the stomach and duodenum. In
contrast with leptin whose release appears to be constant, ghrelin is secreted in a pulsatile manner. It is released when food is needed and then falls off with the intake of food. It is elevated in patients on low calorie diets causing to desire food. Its production is reduced after gastric bypass surgery which may explain satiation in these patients.
Weight Control and Reduction• It ain’t easy!!!
• It is difficult to lose excess weight!
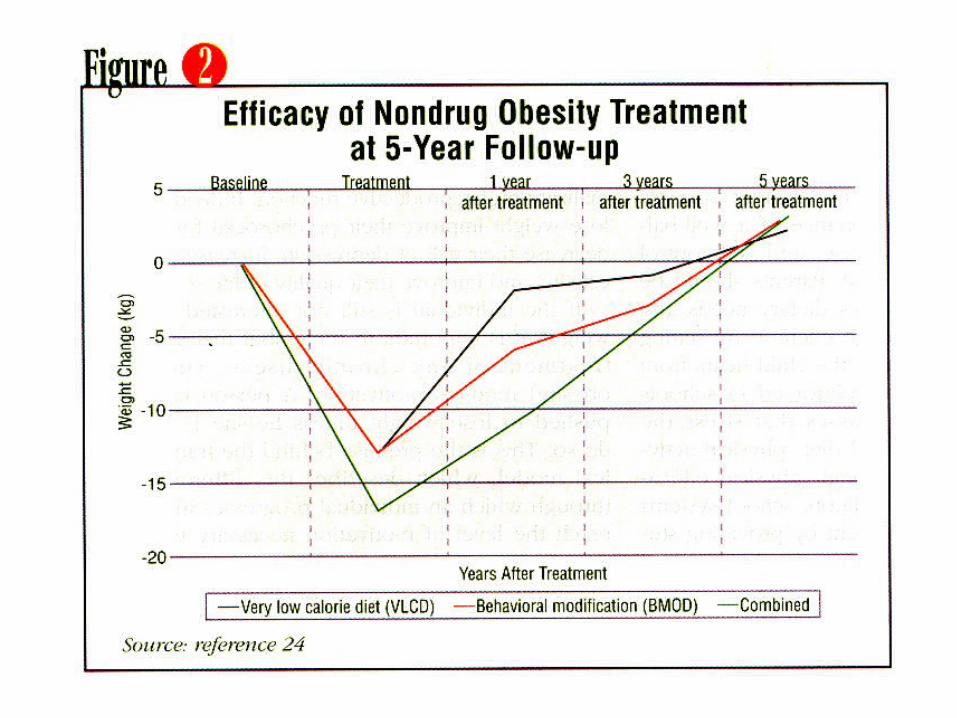
• Once lost, it is difficult to maintain the desired weight. (See next slide.)
• It is difficult to maintain current weight, particularly as one ages.
• Methods include:– Drugs (not too successful, but the
American goal is “take a pill and all will be well.”


Weight Control-Drug Therapy• Phentermine (Ionamin™)
– Approved in1959 for short term appetite suppression. It was part of the infamouse phen-fen or phen-dexfen combination. Fenfluramine was approved in 1973 followed by dexfenfluramine (Redux). The combination of phentermine and either one of the other drugs was never approved by the FDA, especially for long term control of weight. One of the main adverse reactions to this combination developed abnormalities of the heart valve. Some were asymptomatic, others required surgery and some died. Additional work indicated that fenfluramine/dexfenfluramine were the causative agents, not phentermine. It was part of the phen-fen combination. Both drugs inhibit serotonin release.
– The prototype design for phentermine is amphetamine/dextroamphetamine (Dexadrine™) and is a centrally acting sympathomimetic

Drug Therapy-Continued
• Sibutramine (Meridia™)– It acts by inhibiting reuptake of serotonin
and norepinephrine. Its pharmacology is complicated because two of the metabolites also are active. There are significant cardiovascular problems including hypertension. Italy has removed the drug from its market. However, a European Union committee concluded that the drug’s benefits outweigh the risks.

Drug Therapy-Continued• Orlistat (Xenical™-prescription, AlliTM-otc)
– It inhibits lipase in the intestinal tract preventing triglyceride digestion and absorption. While of limited effectiveness (2 - 5% greater weight loss that diet along), it causes intestinal discomfort including steatorrhea. Patients are advised to take vitamin supplement containing the fat soluble vitamins (A, D, E, K) when taking Orlistat. (A patient probably should take a vitamin supplement when on any weight-reduction program.

Drug Therapy-Continued• Bupropion (Wellbutrin™)
– It is an antidepressant that might help patients who eat excessively when depressed. The results are mixed.
• Topiramate (Topamax™)– This drug is indicated for seizures also seems
to cause weight loss.
• Metformin (Glucaphage™)– This is one of the leading drugs dispensed in
the United States for Type 2 Diabetes. Weight loss has been reported by patients taking this drug.
Drug Therapy-Continued• Mesotherapy
– This is an unapproved therapy that is popular in Europe and South American and becoming more used in the United States. The patient receives 100 - 500 skin deep injections of aminophylline, isoproteranol and a sweet clover extract directly into adipose tissue, usually in the hips and thighs. It is supposed to “melt” the fat which then is released slowly into the body where it either is oxidized in the lipid metabolic cycles or excreted, probably in the bile. Most mesotherapists require diet and exercise programs.

Drug Therapy-Concluded
• Rimonabant (Acompilia™)
N
N
CH3
C
Cl
Cl
Cl
NH
O
N
Rimonabant (AcompiliaTM)
More on Rimonabant• Rimonabant was developed based on one of the
cannabinoid receptors. Ligands for these receptors seem to treat addiction and satiation. – This experimental drug has been evaluated for both
smoking cessation and obesity. Related compounds are being evaluated as agents for positron emission tomography (PET) scans of the central nervous system.
– Its Log P and Log D (pH 7.0) is 4.81, meaning that it is very lipophilic.
– Approval has been delayed.– In recent reports, the positive results must be weighed
against the fact that fewer than 2/3 of patients completed the trial (NEJM, 353: 2121-34, 2005) or 50% completed (JAMA, 295: 761-775, 2006)
– Clinical trials also reported some incidences of depression in patients.

Weight Control-Diet• Diet requires great patience. • Peer support is very helpful. • For most diet will work. • The trick is to not fall for the fad diets.• Most valid diets tend towards complex
carbohydrate and high bulk for several reasons.
• Taking a vitamin-mineral supplement might be advised for the lower calorie diet. It has been estimated that it is very difficult for people to obtain their vitamin–mineral RDA on a diet of 1,200 Calories or less.

Diet-Calorie Calculations
• Carbohydrate 4 Calories (kcal)/g
• Lipid 9 Calories (kcal)/g
• Protein 4 Calories (kcal)/g
• Multiple the weight in grams/serving size for each biochemical food group by their respective calories per gram, total and round to the nearest five calories. You should obtain the same number as found in the table.
Are complex carbohydrate, high bulk diets the most effective?
• There are fewer calories per gram (4 Calories/gm versus 9 Calories/gm for lipids).
• The number of calories could even be less/gm depending on the amount of poorly digestible fiber present in the food.
• These diets help lower serum lipid levels. This is important for people with hyperlipidemias.

So why don’t we demand this type of diet?
• It must be remembered that we like the texture of lipid containing foods sliding over our tongues.
• This is considered to be an evolutionary adaptation.
• Our ancestors who consumed lipid containing foods received more Calories per gram and, therefore, gained weight. This allowed them to better survive famines.

Valid versus Fad Diet?• Biochemical Valid Diets
– They make sense biochemically and nutritionally.
– Weight loss averages 1 - 2 lbs per week.– It recognizes that the a person’s former
excess weight will return unless the person monitors what is eaten and maintains an active life lifestyle.

Valid versus Fad Diet?-continued• Fad Diet Characteristics (One or more of
these will be the focus of the diet.)– Magic or miracle foods that burn fat.– Bizarre quantities of only one food or type of
food.– Rigid menus involving a limited selection of foods
that must be eaten.– Specific food combinations.– Rapid weight loss (more than 2 lbs per week).– Lack of medical warnings (i.e. diabetics and
hypertensives should seek medical advice before beginning the diet program).
– No emphasis on physical activity.

Examples of Fad Reducing Diets-1
• “The New Beverly Hills Diet”– Combine or separate certain foods so your body
will thoroughly digest every nutrient in each food (This diet claims that this will make you leaner because your stomach and intestines won’t create any fatty buildup.)
– A limited number of food groups, including just fruits and baked potatoes for the first three days.
– Promises to take off up to 15 pounds in 35 days (up to 3 lbs/week)

Examples of Fad Reducing Diets-2• “Sugar Busters™ (authored by three physicians - so
it must be valid - right? Wrong! The nutrition training of physicians and nurses is worse than that of pharmacists.)
– Too much sugar is the major reason for weight gain due to insulin’s regulatory effects on body fat storage. (Remember, insulin is fat sparing, but let’s not carry this to extremes.)
– Calories do not regulate weight gain or loss. (Calories have a major role unless there is an endocrine disorder. Even where there is a genetic predisposition for obesity, caloric intake and expenditure are important variables.)
– Promises that you can eat most foods in normal quantities or even larger quantities than you presently consume. Carbohydrate containing foods should be reduced.

Examples of Fad Reducing Diets-3• “Mastering the Zone” (authored by a Ph.D. - so it
must be valid - right? Wrong?)
– Most people suffer from an insulin imbalance that causes them to gain excess weight.
– By eating protein, carbohydrates and fat in the proportions described in the Zone guidelines, the insulin imbalance will be corrected, leading to weight loss.
– Promises that the dieter can indulge in food usually considered “taboo” such as red meat and fatty foods.
– Protein 30%; Carbohydrate 40%; and Fat 30%.

Examples of Fad Reducing Diets-4
• “Dr. Atkins’ New Diet Revolution”; • South Beach Diet
– The South Beach Diet can be considered another in the series of low carbohydrate diets. The focus is not so much reduction of all dietary carbohydrate, but a reduction in foods with high glycemic indices. The author of this diet (an M.D.) states that there is greater insulin release and, therefore, rapid intake of glucose into the adipose tissue, when eating foods with a high glycemic index. (In the adipocyte, glucose is converted into triglycerides.)

Atkins & South Beach Diets-continued
• Weight gain is caused by eating a diet high in sugar and refined carbohydrate that boosts insulin production which converts these foods into body fat. (There is some truth to this statement.)
• The diet focuses on increased intake of protein.• By avoiding carbohydrates and sugars, your body
will automatically burn fat for energy. (Remember that the body needs glucose for brain metabolism and for a multitude of other uses. It also uses glucose for “quick energy.” The “new Atkins Diet” and “South Beach Diet” does have some carbohydrate in it.)
• No hunger in-between meals.• Significant improvements in cholesterol and blood
pressure. (Most weight loss regimens will show improvements in these conditions.)
• Protein 30%; Carbohydrate 40%; and Fat 30%.

Liquid Protein Diets• These products provide approximately
400 Calories per day and consist of hydrolyzed, protein with a high biological value. The purpose is to keep the patient in positive nitrogen balance. There is little insulin produced with this type of product. They are indicated for the severe obese patient.

Fat Substitutes• Add the smooth feel we like in our foods.• Salatrim™ (Nabisco)
– An artificial triglyceride composed of stearic acid and short chain fatty acids. Because stearic acid is poorly absorbed and the short chain fatty acids contain less calories, Salatrim is claimed to have only 5 Calories/gm.
• Problem: It is not suitable for frying foods
• Olestra™ (Proctor and Gamble)– This product is not a triglyceride, but it is a non-
digestible product consisting of a mixture of sucrose esterified with six to eight fatty acids.
• Advantage: Because it is non-digestible, it is "calorie free.“ It can be used in frying.

Fat Substitutes-concluded
• Simplesse™ (NutraSweet Company)– A dried milk protein extracted from whey.
The protein has been "engineered" into very small spherical particles that slide by each other like ball bearings and mimic the feel of fat.
• Advantage: It has the "feel" of fat in the mouth. It has only 1.5 Calories/gm.
• Problem: Being a protein, it cannot carry flavors that normally dissolve in fat and are released when eaten.

Artificial Sweeteners
• These originally were marketed to patients diagnosed with diabetes mellitus. Their marketing in low and zero calorie products is fairly recent.
• The first group show that a sugars are not the only structure that can ellicit a strong response from the taste receptors that detect sweetness.


Bariatric Surgery• Removal of a section of the small intestine.
– Except for malignancies and scar tissue (Crohn’s Disease, etc) from chronic inflammatory diseases, removal a section of the small intestine for the treatment of obesity is rarely done. What results is a variety of malabsorption syndromes and liver disease.
• Intestinal bypass– This is not often done and is considered
temporary. A section of the small intestine was bypassed for a period of time. When the desired weight was obtained, the bypassed section was reconnected. Obviously, each of these procedures is major surgery with long recovery times.


NEJM 351:26, 2683-93, December 22, 2004

Figure 3. Incidence of Hypertriglyceridemia, Low HDL-C andHypercholesterolemia.NEJM, 351:26, 2683-93, December 22, 2004.

Figure 4. Recovery from Hypertriglyceridemia, Low HDL-C andHypercholesterolemia.NEJM, 351:26, 2683-93, December 22, 2004

NEJM, 351:26, 2683-93, December 22, 2004.

Bariatric Surgery-continued
• Meta-analysis based on 136 published studies on 22,094 patients.– 61.2% lost “excess” weight– Type 2 Diabetes completely resolved
76.8%– Hyperlipidemia improved in 70%– Hypertension resolved in 61.7%– Obstructive sleep apnea resolved in 85.7%
• The article did not indicate years following surgery for the above results.
» JAMA, 292:14, 1724-1737, October 13, 2004

Bariatric Surgery-1 year later
• Among Medicare beneficiearies, the risk of early death after bariatric surgery is considerably higher than previously suggested and associated with advancing age, male sex and lower surgeon volume of bariatric procedures. Patients aged 65 years or older had a substantially higher risk of death within the early postoperative period than younger patients.– JAMA, 294: 1903-1908, October 19, 2005
Bariatric Surgery-1 year later
• Increases in hospital use after surgery appear to be related to the use Roux-en-Y gastric bypass. Payers, clinicians, and patients must consider the not-inconsequental (consequental?) rate of rehospitalization after this surgery.– JAMA, 294: 1918-1924, October 19, 2005

Bariatric Surgery-Continued Possible Effect on Drug Absorption
• Most drug absorption is in the small intestine with its greater surface area.
• Some speculation that prodrugs relying on acid hydrolysis might be affected may have varied absorption because of decreased gastric acid in the “pouch”.– No significant clinical problems reported.
• Drug dosing based on body weight may need to be monitored as weight is lost.
• No definitive studies on drug absorption have been done with a population of bariatric surgery patients.
• Drugs that normally are monitored regularly (coumadin, digoxin, etc) should be followed closely following bariatric surgery.
• The drug therapy for most bariatric surgical patients usually can be monitored based on therapeutic outcome.
Bariatric Surgery-Continued Possible Effect on Nutrient Absorption
• Recognized need for vitamin B12 (cyanocobalamin) supplements either by injection, nasal or 25,000 units orally. B12 requires instrinsic factor produced in the stomach for its absorption.
• Iron deficiency common in menstruating women because iron absorption occurs in the lower stomach.

Bariatric Surgery-concluded• These procedures can be done
laproscopically and are considered successful if done by a properly trained surgeon. From 1992 to 2003 the estimated number of the latter type of surgery has increased from 18,000 to about 103,000 procedures. There is money to be made!
• Remember, it appears that ghellin release is reduced following gastric bypass surgery causing reduced appetite in these patients.

Any Benefits from Liposuction??
• Liposuction does NOT seem to be beneficial in terms of common markers most likely because it removes subcutaneous fat.– Plasma glucose– Insulin resistance– Hyperlipidemia– Hypertension– Onset of Type 2 Diabetes
» NEJM, 350:25, 2542-2544, 2549-57, June 16, 2004

Exercise and Weight Reduction• It is not as straight forward as one might
assume.• There are at least three reasons for a
program of regular exercise or physical activity.– Cardiovascular fitness– A major component of weight control– A feeling of well being and feeling good about
one’s self.
• There is a biochemical reason why the recommendation is to schedule 30 – 60 minutes of exercise daily along with keeping physically active throughout the day.

Exercise and Weight Reduction-continuedRespiratory Exchange Ratio (RER)
Respiratory Exchange Ratio =Vol CO2 produced
Vol O2 consumed
Determined from the ratio of CO2/O2 inhaled to CO2/O2 exhaled.
C15H31COOH + 23 O2 16 CO2 + 16 H2O 16 CO2/23 O2 = ca 0.7
RER = 0.7 for 100 percent oxidation of palmitate.
RER = 1.0 for 100 percent oxidation of glucose
C6H12O6 + 6 O2 6 CO2 + 6 H2O 6 CO2/6 O2

Exercise and Weight Reduction-continued
• Biochemical Facts:– At rest (sedentary life style):
• Body prefers to metabolize triglyceride (9 Cal/gm) rather than carbohydrate (4 Cal/gm).
– Sudden increase in physical activity:• Body begins to oxidize carbohydrate. Why?
– 0.7 L of O2 required to oxidize one gm of carbohydrate.
– 2.03 L of oxygen required to oxidize one gm of triglyceride.
Exercise and Weight Reduction-continued
• Implication:– Heart and lungs CANNOT "instantly" adjust to the increased
oxygen demand required to oxidatively metabolize triglyceride.
– Fatty acids are not "instantly" available. Fatty acids are obtained by hydrolysis of triglycerides stored in the adipocytes. Then the fatty acids must be attached to serum albumin for the trip to the skeletal muscle. In contrast, muscle glycogen quickly provides glucose as an "instant fuel.“
– It is estimated that during the first few minutes of exercise, up to 80 percent or more of fuel used may be glycogen with metabolism dropping from 100 percent of the fuel for a resting muscle to 20 percent for initial activity.
– Over about 45 minutes, the carbohydrate/fatty acid ratio shifts from 80/20 to about 50/50. After about 60 minutes the ratio shifts to about 20/80 as the body protects its now diminished glycogen stores.

Weight Reduction-continued
• Summary:– The "fuel" consumed in an hour of endurance activity will be about
30 percent triglyceride and 70 percent carbohydrate.
• Implications for weight control:– Goal: Remove one lb. of body fat.– Requires: 3,500 Cal (kcal) of activity if only triglycerides are
metabolized.– In Reality: Because of the carbohydrate consumption that occurs
during physical activity, the total caloric expenditure will be 11,700. To meet this goal, the person would have to run about 120 miles and eat no fat.
• Conclusion:– Moderate exercise will consume more body triglyceride than
intense exercise because the latter's oxygen requirement will cause the body to start using carbohydrate for fuel.
– The amount of dietary fat must be monitored carefully.