peripheral t-cell lymphoma with unique immunologic features
TRANSCRIPT

831
Peripheral T-cell Lymphoma with Unique Immunologic Features Anwar Sheikha, M.R.C.P., M.R.C.Path., F.C.A.P., F.R.C.P.A.,* Mansour AI-Janadi, M.D.,t Abdulaziz AI-Saigh, F.R.C.S.I.,S Tarek Malatani, F.R.C.S.(C),$ and Syed Raziuddin, Ph.D., M.R.C. Path§
Background. The autologous mixed lymphocyte re- action (AMLR) is an important immunoregulatory phe- nomenon in human immune disorders. The authors have determined the phenotype and assessed the response of malignant lymph node T-cells, from histologically and immunologically proven cases of peripheral T-cell lym- phoma, in AMLR and allogeneic mixed lymphocyte reac- tion (MLR) and studied the secretion of lymphokines.
The proliferative response, tritiated 3H- thymidine incorporation assay, was used to determine the AMLR and allogeneic MLR of the responding T-cells. An interleukin-2 (IL-Z)-dependent T-cell line (CTLL) was used for the production of IL-2 by phytohemagglutinin- stimulated T-cells in a cytotoxic assay. B-cell growth and differentiation factor activity of T-cells was studied by enzyme-linked immunosorbent assay.
The AMLR of malignant lymph node T- cells was increased characteristically in 12 of the 14 lym- phoma cases studied; however, that of the blood T-cells was decreased. The allogeneic MLR of the malignant lymph node T-cells and blood-purified T-cells of the eight cases investigated was decreased. Expression or defi- ciency of CD2 and CD3 antigens on malignant T-cells did not show any difference in the AMLR assay.
This study demonstrates an impor- tant tendency of malignant T-cells from patients with pe- ripheral T-cell lymphoma to proliferate in AMLR. The highly augmented AMLR but deficient allogeneic MLR observed in these malignant T-cells indicate that autolo- gous recognitive events may play an important role in the immunopathogenesis of this human disease. Cancer
Methods.
Results.
Conclusions.
1993; 71:831-8.
~~
From the Departments of *Clinical and Laboratory Hematology, tlnternal Medicine, SSurgeiy, and §Clinical Immunology, King Saud University Medical College and Asir Central Hospital, Abha, Saudi Arabia,
Address for reprints: Anwar Sheikha, M.B.Ch.B., M.R.C.P., M.R.C.Path., F.C. A.P., F.R.C.P. A., Head, Department of Clinical and Laboratory Hematology, King Saud University Mechcal College, Abha, P.O. Box 641, Saudi Arabia.
Accepted for publication July 6, 1992.
Key words: peripheral T-cell lymphoma, autologous mixed lymphocyte reaction, interleukin-2, lymphokines, malignant T-cells.
The immune response in patients with cancer is a com- plex phenomenon that involves a balanced action of regulator cells. This balance is particularly important in the response of the body against foreign antigens, in which the regulator cells switch the immune reaction on or off. It also may regulate self-tolerance and self- surveillance. T-lymphocytes, mediators of cell-me- diated immunity, play a key role in this regulation.
The human autologous mixed lymphocyte reaction (AMLR) is a unique phenomenon of cellular communi- cation. It constitutes activation, proliferation, and dif- ferentiation of T-cells subsequent to specific recognition of self-determinants on non-T-cells.' Abnormalities of the immune system and AMLR have been reported to play a role in the pathogenesis and clinical course of several autoimmune diseases and some lymphoprolifer- ative disorder^.'-^
The discovery of interleukin-2 (IL-2; T-cell growth factor) has made a significant contribution to the study of the functions of various T-cell subsets. IL-2 and its receptor (IL-2R) play a central role in T-cell activation and proliferation.6 IL-2 activity and IL-2R expression are also important in the immune response in a variety of malignant diseasw6
Peripheral T-cell non-Hodgkin lymphoma is a unique T-cell proliferative disorder caused by malig- nant proliferation of T-cell subsets in the enlarged lymph nodes. With the use of well-characterized rnono- clonal antibodies (MoAb) against T-cells, both CD4+ helper/inducer and CD8+ suppressor/cytotoxic T-cell lymphomas have been allocated into meaningful cate- gories.'-" These T-cell neoplasms are of exceptional in- terest because any alteration in the T-cell phenotype and function has been found to affect both cell-me- diated and humoral immunity." Although detailed

832 CANCER February 1 , 1993, Volume 71, No. 3
data on cell morphologic characteristics, histopatho- logic features, and phenotype are available for a large series of patients with well-defined peripheral T-cell lymphomas and other T-cell malignant neoplasms,'-" T-cell functional studies (IL-2R expression on mitogen- activated T-cells, JL-2 activity, and AMLR) on malig- nant lymph node T-cells are lacking. In the current study, we have performed the T-cell functional studies of 14 patients with histopathologically and immunologi- cally confirmed peripheral T-cell lymphomas.
Materials and Methods
Pa tien ts
The 14 patients studied were admitted to either Abha General Hospital or Asir Central Hospital, Abha, Saudi Arabia. The diagnosis was based on the results of cervi- cal lymph node biopsy, plus, in few cases, bone marrow examination. Classification of the non-Hodgkin lym- phoma was based on the Rappaport system.'* Eight pa- tients with the diagnosis of tuberculosis and enlarged lymph nodes were used as patient control subjects. These patients did not have malignant diseases. The healthy control subjects studied were age and sex matched and had no history of recent illnesses.
MoAb Studies
The percentage of T-cells and their subsets from the lymph node cells (LNC) was determined with MoAb with the use of the indirect immunofluorescence tech- nique, previously described elsewhere in detail.I3 The following MoAb, purchased from Ortho Diagnostics (Raritan, NJ), were used in these studies: OKT3 (CD3+, pan T-cells), OKT4 (CD4+, helper/inducer T-cells), OKT6 (CDlS, thymocytes), OKT8 (CD8+, suppressor/ cytotoxic T-cells), OKT9 (CD71+, transferrin recep- tors), OKTlO (CD38+, activation antigens), OKTl 1 (CD2+, erythrocyte rosetting pan T-cells), and OKIa 1 (HLA-DR+, activation antigens). Anti-Tac (CD25+, IL- 2 receptor) MoAb was provided by Dr. Thomas A. Waldmann (National Institutes of Health, Be- thesda, MD).
T-cell and Non-T-cell Preparations
Peripheral blood lymphocytes, obtained by standard Histopaque-1077 (Sigma Chemical Co., St. Louis, MO) density gradient centrifugations, were separated into T- cell and non-T-cell fractions by the sheep erythrocyte rosetting technique, as described earlier. l4 The T-cell preparation contained 92-95 % OKT3+ cells, whereas the non-T-cells contained 65-74% surface immuno-
globulin-positive cells (B-cells), 15-20% OKMI+ cells (monocytes), and less than 5% OKT3f cells.
Mononuclear cell suspensions were prepared from the LNC of patients with lymphoma with Histopaque- 1077 gradient centrifugation. These cells showed 87- 98% staining with either OKT4 or OKT8 MoAb, con- firming their T-cell nature. For the eight patients with tuberculosis, T-cells (93% OKT3f) were prepared from LNC by the erythrocyte rosetting technique and Histo- paque- 1077 gradient centrifugation.
T-cel l Proliferative Responses
The proliferative response of T-cells was studied as de- scribed earlier.I4 In brief, T-cell cultures were estab- lished in triplicate and consisted of 2.5 X lo5 cellsin 200 pl of RPMI 1640 medium (Flow Laboratories, UK). Phytohemagglutinin (PHA), at 2 pg/ml, and concanav- alin A, at 5 pg/ml, were used as stimulators. The cells were cultured in flat-bottomed microtiter culture plates for a total period of 72 hours at 37°C in 5% carbon dioxide and air. Eighteen hours before termination of the incubation period, 1 pCi of tritiated 3H-thymidine (Amersham Radio-chemicals, United Kingdom) was added to each culture well. At the end of the incubation period, the cells were harvested, and incorporation of 3H-thymidine was measured in a Beckman LS 9800 liquid scintillation counter (Beckman, UK). The data are expressed as the difference between counts per minute (cpm) from mitogen-stimulated cultures and cpm from nonstimulated cultures.
Autologous Mixed Lymphocyte Reaction
The non-T-cell preparations were pretreated with 50 &ml of mitomycin C (Sigma) for 45 minutes at 37°C and washed three times before use. A representative AMLR culture consisted of 2.5 X l o5 T-cells (LNC or peripheral blood lymphocytes) as responders and 2.5 X lo5 mitomycin C-treated non-T-cells (peripheral blood lymphocytes) as stimulators, in 200 p1 of RPMI- 1640 supplemented with 2 mM glutamine, 25 mM HEPES buffer (Flow Laboratories, United Kingdom), and 10% heat-inactivated human serum." All cultures in triplicate were incubated in round-bottom microtiter plates at 37°C in 5% carbon dioxide and air for a total period of 6 days; 3H-thymidine was added (1 pCi/well) 18 hours before harvest with a Flow Titertek cell har- vester, and incorporation of radiolabeled compound into DNA was measured in a Beckman LS 9800 liquid scintillation counter. Backgrounds consisted of T-cell fractions cultured in media supplemented with serum alone. The data are expressed as the difference (cpm) between the cpm from cultures containing responding

T-cell Function in Malignant Lymphoma/Sheikha et al . 833
T-cells plus autologous stimulating non-T-cells and the cpm from cultures containing responding T-cells alone.
Allogeneic Mixed Lymphocyte Reaction
Allogeneic mixed lymphocyte reactions (MLR) were es- tablished by culturing T-cells (LNC or peripheral blood lymphocytes for patients) with mitomycin C-treated non-T-cells of normal healthy control subjects. The cell concentrations and culture conditions used in alloge- neic MLR were the same as described for AMLR.
IL-2R Expression and IL-2 Activity
CD4+ and CD8+ T-cells were purified from normal CD3+ total T-cells by a panning technique using OKT8 and OKT4 MoAb, respectively, as described earlier.l4 T-cell cultures from purified normal blood and LNC of patients with lymphoma identical to those for prolifera- tion were established and stimulated for 48 hours with PHA (2 pg/ml). Cells were examined for the presence of IL-2R with anti-Tac MoAb, with the use of the indi- rect immunofluorescence te~hnique . '~ IL-2 activity from the culture supernatants was measured in a stan- dard proliferation assay,14 with the use of an IL-2-de- pendent CTLL cell line developed by Dr. Verner Paet- kau (University of Alberta, Edmonton, Canada). Units of IL-2 activity were defined as U (reciprocal titer of test sample at 30% of maximal counts/minute stan- dard)/(reciprocal titer at 30% maximal counts/minute) x 100.
B-Cell Growth Factor and B-Cell Differentia tion Factor
T-cells of patients and control subjects (2.5 X 105/ml) were incubated in RPMI-1640 medium with 5 X mercaptoethanol, 1 0°/0 heat-inactivated AB serum, 2 mmol L-glutamine, 100 pg/ml of streptomycin, and 100 U/ml of penicillin with 2 pg/ml of PHA for 72 hours at 37°C. The supernatants of the stimulated T- cells were recovered and analyzed for B-cell growth factor (BCGF) and B-cell differentiation factor (BCDF) activity.
BCGF activity was analyzed from the T-cell-stimu- lated supernatants on normal B-cell proliferation by in- corporation of 3H-thymidine, according to the costimu- lator assay described re~ent1y.I~
BCDF activity, immunoglobulin (Ig) G and IgM se- cretion, was deteimined with Staphylococcus aureus Co- wan I-stimulated normal B-cells and T-cell superna- tants. IgG and IgM secretion from these cultures after 7 days of incubation was estimated by the standard en- zyme-linked immunosorbent assay described ear- lie^-.'^,'^
Results
The cervical lymph node biopsy specimens from all 14 patients exhibited the characteristic histologic features required for the diagnosis of non-Hodgkin malignant lymphoma. The clinical data and histopathologic classi- fication of lymphomas are shown in Table 1. All pa- tients were Saudi nationals. The outstanding clinical manifestations in all patients were fever, anorexia, weight loss, and, in some patients, night sweats and bone pain. Patients 3, 4, and 13 were hypogammaglo- bulinemic (low serum IgG, IgA, and IgM levels), and Patient 8 had elevated IgM levels, diagnosed as IgM hypergammaglobulinemia (serum IgG level, 226 mg/ dl; IgA level, 123 mg/dl; and IgM level, 1184 mg/dl). All other patients had normal serum immunoglobulin levels.
The lymph nodes were the most frequent site of involvement at presentation. Eight of the 14 patients had generalized peripheral lymphadenopathy. Large mediastinal masses were observed in four older patients by radiologic examination. Bone marrow biopsy speci- mens showed malignant cell infiltration in five cases. All 14 cases demonstrated a diffuse pattern of lym- phoid infiltration with no evidence of a follicular pat- tern in lymph node biopsy specimens on light micro- scopic examination. Using the Rappaport system of clas- sification of malignant non-Hodgkin lymphomas,'* we classified six cases as diffuse, poorly differentiated lym- phocytic lymphoma; four cases as diffuse, well-differ- entiated lymphoma; three cases as diffuse mixed lym- phocytic lymphoma; and only one case as diffuse large cell histiocytic lymphoma.
The immunologic identification of LNC, performed in each case with well-characterized MoAb, is summa- rized in Table 2 . The abnormal LNC did not exhibit surface immunoglobulin-positive or OKBl -positive (MoAb to detect B-cells, Ortho Diagnostics) cells. None of the cells from LNC showed reactivity with anti- kappa or anti-lambda immunoglobulin light chains (data not shown). The designation of all 14 cases as T-cell lymphomas was based on reactivity of LNC sus- pension (87-98%0) with T-cell reagents OKT3, OKT4, OKT8, or OKTll, along with the lack of expression of B-cell lineage markers. According to the MoAb staining pattern, eight cases were CD4+ helper/inducer T-cell lymphomas, five cases were CD8+ suppressor/cyto- toxic T-cell lymphomas, and one case, with positive re- sults for both OKT4 and OKT8 MoAb, was classified as a CD4+ CD8+ helper-suppressor T-cell lymphoma. All cases tested had negative results for OKT6, which is considered to be a marker for CD1+ thymocytes. A striking heterogeneity of pan T-cell antigen expression, defined by OKT3 (CD3+) and OKTll (CD2+) MoAb,

834 CANCER February 1, 2993, Volume 71, No. 3
Table 1. Clinical Data and Histopathologic Features of Patients With Peripheral T-cell Lymphoma
Leukocyte count Hepatomegaly/ Presenting Mediastinal Histologic features mass classification
Patient Age no. (yr) Sex (x 109/1) splenomegaly
WDL 1 36 M 7.2 -/+ AIC 2 70 F 11.4 -/+ AIC + WDL 3 75 M 18.0 +/+ AIC BM t MLL
WDL 4 49 F 10.2 -/+ AC PDL 5 39 M 8.4 -/+ AC MLL 6 41 M 10.5 -/- AC WDL 7 40 F 6.8 +/+ AIC BM
8 27 M 8.2 -/+ AC PDL 9 73 M 21.0 +/+ AIC BM + MLL
PDL 10 35 M 13.6 -/- AC PDL 11 38 M 8.3 -/- AC
12 64 M 9.5 -/+ AIC PDL 13 60 M 10.2 +/+ AIC BM + PDL
LCL 14 68 M 16.7 +/+ AIC BM
-
-
-
-
-
~
-
-
~
-
A: axillary; I: inguinal; C: cervical lymphadenopathy; EM: bone marrow involvement PDL: diffuse, poorly differentiated lymphocytic lymphoma; MLL diffuse, mixed lymphocytic lymphoma; WDL: diffuse, well-differentiated lymphoma; LCL: diffuse, large cell histiocytic lymphoma.
was observed. Thus, although the cases had a typical CD4+ or CD8+ functional T-cell phenotype, they dif- fered in expressing typical CD2+ or CD3+ pan T-anti- gens. One case expressed CD71+ transferrin receptor, and six expressed CD38f activation antigen. The HLA- DR+ (0KIal-t) and anti-Tac+ (IL-2 receptors) antigens, also believed to be markers of activated T-cells, were present in most cases. However, the degree of CD38, OKIal, and anti-Tac antigen expression varied by case.
T-cells from LNC of 14 patients with T-cell lym- phoma and 8 patients with tuberculosis were cultured with PHA or concanavalin A, and proliferation was
measured after 72 hours. As shown in Figure 1, incorpo- ration of 3H-thymidine, resulting from PHA and conca- navalin A stimulation, varied in all patients. In fact, there was no major difference in responsiveness to stim- ulation by PHA or concanavalin A. Likewise, no corre- lation was observed between T-cell phenotype and function.
A considerable body of evidence suggests that T- cells recognize determinants on autologous cells speci- fied by genes of the major histocompatibility complex.' Whenever possible, AMLR will be related to the recogni- tion of self-major histocompatibility complex determi-
Table 2. Immunophenotyping of Lymph Node Cells From Patients With Peripheral T-cell Lymphoma*
Patient OKT3 OKT4 OKT6 OKT8 OKT9 OKTlO OKTll OKIal Anti-Tac no. CD3+ CD4+ CDl+ CD8+ CD71+ CD38+ CD2+ HLA-DR+ IL-2R+
1 94 93 3 1 14 86 83 2 91 92 1 0 3 3 8 3 2 98 2 1 1 8 92 4 97 90 2 0 11 81 91 5 88 96 0 2 0 9 85 6 0 89 0 1 4 0 84 7 3 94 0 2 91 83 78 8 12 91 4 2 5 76 87 9 93 2 1 90 0 0 2
10 92 1 1 98 2 13 92 11 4 1 2 94 2 86 94 12 88 3 0 91 2 82 87 13 94 3 1 87 6 11 5 14 95 87 2 93 1 16 8
74 81 83 10 6
58 66 71
2 5
81 23 17 63
62 73 47 72 12 39 72 58 63 0
58 31 22 52
LNC: lymph node cells; CD: cluster differentiation. * The results represent the percentage of cells in each LNC suspension bearing the designated monoclonal antibody.

T-cell Function in Malignant LymphomalSheikha et al .
70 -
- 60' m s
2
x 5 50-
835
70 - ; 60- 2 X
f 5 0 - 0 - c - *
4 0 - 0 ; 30-
0 c .- P- E % 20 - z I-
I I m
10 -
0
0
0 0 0
0 3 0 c
0 0
C
0
C
A A
A
A A
A
A A A A A A
A
A
0' I
LNC ( T - c e l l s ) LNC (T -ce l l s ) Blood T-cel ls Lymphoma Tu bcrmlos is Normal
0 A
0 A A A
0 0 0 A
0 A 0 A
0 A
0
0
0
0 0 0
3
0
C O
0
A
A
A
A
A A
A
A A
A
0: P H A Response : A: Con A Response
Figure 1. T-cell proliferative responses. Each point represents data for a single patient or control subject.
nants, which occurs in the normal immune response. Furthermore, in several disease states associated with immunologic abnormalities, the AMLR is abnormal.'-5 These results suggest the importance of AMLR in the regulation of the immune response. Therefore, we have determined the AMLR of malignant LNC T-cells and purified blood T-cells of all 14 patients with peripheral T-cell lymphoma, which were cultured with autologous non-T-cells. In the control AMLR experiments, purified lymph node and blood T-cells of eight patients with tuberculosis (as patient control subjects) and blood T- cells of 11 normal healthy subjects, cultured with autol- ogous non-T-cells, were investigated. The AMLR data are summarized in Figure 2. As shown, CD4+, CD8+, or CD4+ CD8+ malignant T-cells (LNC) with non-T- cells (blood) responded well in AMLR. Although indi- vidual cases differed in their overall responses in AMLR, it was clear that AMLR was highly increased in 12 of the 14 T-cell lymphoma cases. On the contrary, purified blood T-cells of all the T-cell lymphoma cases cultured with autologous non-T-cells demonstrated a deficient AMLR. The purified lymph node and blood T-cells of the eight patients with tuberculosis, which were cultured with autologous non-T-cells, also demon- strated a diminished AMLR. The cells containing CD4+, CD8+, or CD4+ CD8+ malignant lymph node
T-cells cultured alone without autologous non-T-cells demonstrated little proliferation (background cpm,
Furthermore, we also determined the allogeneic MLR in which lymph node and blood T-cells of the eight patients with peripheral T-cell lymphoma were cultured with allogeneic normal control non-T-cells. The allogeneic MLR of patients with tuberculosis could not be tested because the number of T-cells from LNC was not sufficient for these studies to be performed. Figure 3 presents the allogeneic MLR data of patients and healthy control subjects. The most striking finding was that the allogeneic MLR of all patients with periph- eral T-cell lymphoma was highly depressed as com- pared with that of healthy control subjects.
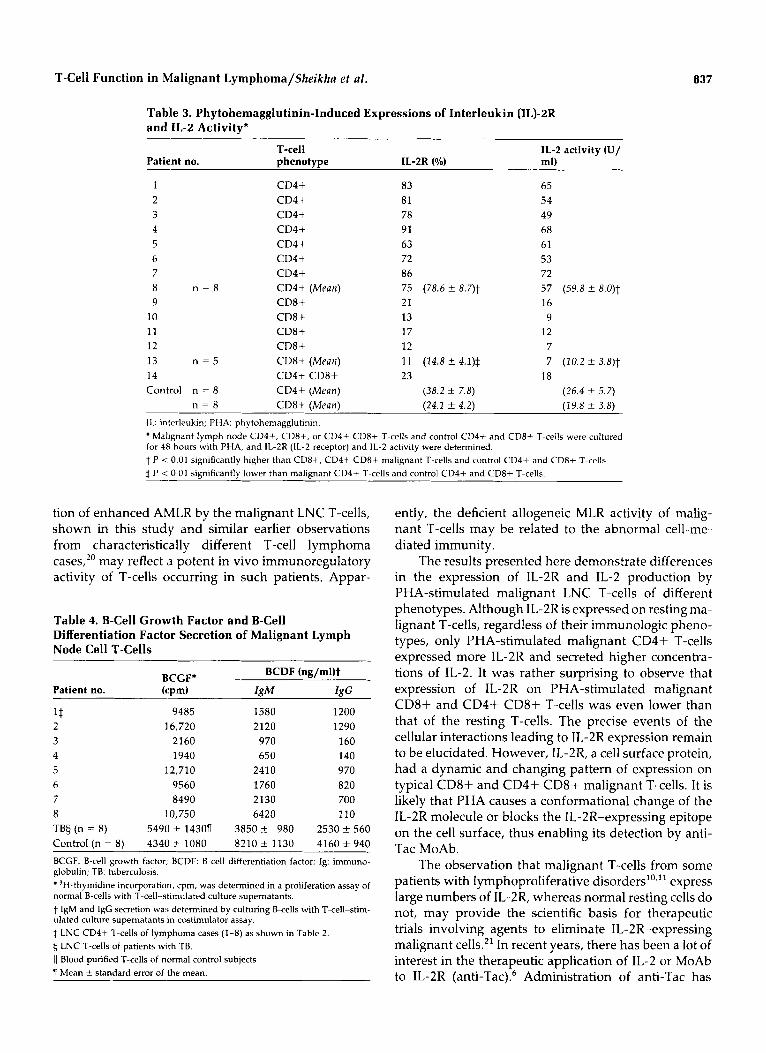
As shown in Table 2, malignant resting LNC T-cells (CD4+, CD8+, or CD4+ CD8+) expressed IL-2R. We have determined the expressions of IL-2R and IL-2 ac- tivity of these malignant LNC and normal CD4+ and CD8+ T-cells after stimulation for 48 hours with PHA. The data shown in Table 3 demonstrate that the malig- nant LNC CD4+ T-cells (Patients 1-8) expressed a higher percentage of IL-2R on cells and secreted more IL-2 after PHA stimulation. However, malignant LNC CD8+ cells (Patients 9-13) and CD4+ CD8+ T-cells
800-1750).
A
A A A A A A A
A A
A
A M L R
... ..
X m o o o c D O x x x m m m .
O D C O x x 0 Lnc BLOOD LNC BLOOD BLOOD T-ce l l T-cel l T-cell T-cell T-ce l l
Lymphoma Tuberculosis Normal
Figure 2. AMLR. Each point represents data for a single patient or control subject. AMLR activity was determined by culturing purified T-cells with autologous mitomycin C-treated non-T-cells. CD2- deficient and CD3-dehcient LNC T-cells from lymphoma cases did not show any major differences in AMLR response.

836 CANCER February 1 , 1993, Volume 71, No. 3
(Patient 14) expressed very few IL-2R and secreted lower concentrations of IL-2, as compared with malig- nant CD4+ T-cells and normal blood T-cells. There was no correlation between prior expression of IL-2R and the expression of IL-2R after PHA stimulation of these malignant LNC T-cells.
T-cells produce BCGF and BCDF. These two lym- phokines are crucial in humoral immunity. They pro- vide a stimulus for proliferation and differentiation of B-cells to secrete immunoglobulins. Because IL-2 pro- duction was increased greatly in LNC CD4+ T-cells of the respective patients with lymphoma, we next sought to determine BCGF and BCDF activity of eight patients with CD4+ malignant LNC (Patients 1-8). These data are shown in Table 4. It was evident that, except for Patients 3 and 4, who had hypogammaglobulinemia, all others secreted highly elevated levels of BCGF. It is of interest, however, that these malignant LNC CD4+ T-cells (except in Patient 8) were deficient in BCDF ac- tivity to stimulate normal B-cells to secrete IgM and IgG, as compared with T-cells from patients with tuber- culosis or healthy control subjects. The malignant LNC CD4-t T-cells of Patient 8 with IgM hypergammaglo- bulinemia secreted more BCGF and IgM but not IgG.
Discussion
The malignant LNC T-cells of patients with peripheral T-cell lymphoma were investigated for IL-2R expres- sion, IL-2 production, and their proliferative capacity in AMLR and allogeneic MLR. We have demonstrated that the AMLR of responding malignant LNC T-cells was increased characteristically as compared with that of normal control subjects and patients with tuberculo- sis. However, these malignant LNC T-cells were defi- cient in allogeneic MLR, similar to the blood T-cells. Thus, the malignant LNC T-cells play an important role in T-cell autoreactivity in AMLR. The AMLR may prove to be a major tool for differentiating neoplastic from reactive cells and probably will provide additional in- sights into cell-cell interactions and the sequences lead- ing from benign to malignant clonal expansion of T- cells. It was shown further that the PHA-stimulated malignant LNC CD4+ T-cells expressed a significantly higher percentage of IL-2R and secreted more IL-2 as compared with malignant LNC of CD8+ or CD4+ CD8f T-cell phenotype and CD4+ or CD8+ normal T-cells. The role of IL-2R and IL-2 secretion in lym- phoid neoplasms is of major interest. In these T-cell neoplasms, a high level of IL-2R expression and IL-2 secretion by PHA-stimulated malignant CD4+ T-cells appears to be important in characterizing this neo- plasm. It also is anticipated that studies of this nature will add greatly to our understanding of the pathogene- sis of T-cell proliferative disorders with distinctive phe-
40
35
- n 2 30 X
E 0" 25 u
c c .-
20 8 g
5 10
C
15 c .- P-
I- I I n
5
0
MLR 0
a
0 .
0 . 0 0 . 0
LNC BLOOQ BLOOD BLOOD T-cell T-cell T-cell T-cell
Lymphoma Normal Tuberculosis
Figure 3 . Allogeneic MLR. Each point represents data for a single patient or control subject. Allogeneic MLR actlvity was determined by culturing purified T-cells with allogeneic mitomycin C-treated normal non-T-cells.
notypes and will lead to more specific treatment modali- ties.
One of our patients (Patient 8) had IgM hypergam- maglobulinemia, a feature that has not been reported previously in patients with peripheral T-cell lym- phoma, which may result from malignant CD4+ helper T-cells or defective T-cell regulation of B-cell function in antibody synthesis. IgM hypergammaglobulinemia has been reported in a few cases of leukemia16 and im- munodeficiency with chronic lymphaden~pathy. '~ None of our patients had a history of prior immune disorders or lymphoproliferative malignant neoplasms. Three of our patients had hypogammaglobulinemia, which has been reported previously in some cases of T-cell malignant neoplasms, including peripheral T-cell lymphomas."
The AMLR measures a self-recognition event man- ifested by proliferation of T-cells when they are cul- tured with autologous non-T-cells.' Deficiency of AMLR occurs in mice that are genetically susceptible to autoimmune disorders and lymph~proliferation.'~ A de- ficient AMLR was demonstrated in humans with sev- eral autoimmune diseases,'f2 chronic lymphocytic leu- kemia,3 Hodgkin d i ~ e a s e , ~ and B-cell non-Hodgkin l y m p h ~ m a . ~ AMLR deficiency has been shown to be related to a defective T-cell re~ponse . ' ,~ Our demonstra-
T-cell Function in Malignant Lymphoma/Sheikha et al. 837
Table 3. Phytohemagglutinin-Induced Expressions of Interleukin (IL)-2R and IL-2 Activity*
T-cell IL-2 activity (U/ Patient no. phenotype IL-2R (%) ml)
1 2 3 4 5 6 7 8 n = 8 9
10 11 12 13 n = 5 14
CD4+ CD4+ CD4+ CD4+ CD4+ CD4+ CD4+ CD4+ (Mean) CD8+ CD8+ CD8+ CD8+ CD8+ (Mean) CD4+ CD8+
83 81 78 91 63 72 86 75 (78.6 f 8.7)t 21 13 17 12 11 (14.8 ? 4.1)$ 23
65 54 49 68 61 53 72 57 (59.8 f 8.0)t 16 9
12 7 7 (10.2 f 3.8)$
18 Control n = 8 CD4+ (Mean) (38.2 f 7.8) (26.4 +- 5.7)
n = 8 CD8+ (Mean) (24.1 f 4.2) (29.8 f 3.8) IL: interleukin; FHA: phytohemagglutinin.
Malignant lymph node CD4+, CD8+, or CD4+ CD8+ T-cells and control C D 4 i and CD8+ T-cells were cultured for 48 hours with PHA, and L 2 R (IL-2 receptor) and IL-2 activity were determined. t P < 0.01 significantly higher than CD8+, CD4+ CD8+ malignant T-cells and control C D 4 i and CD8+ T-cells. t P < 0 01 sianificantlv lower than malienant CD4+ T-cells and control CD4+ and CD8+ T-cells.
tion of enhanced AMLR by the malignant LNC T-cells, shown in this study and similar earlier observations from characteristically different T-cell lymphoma cases,*O may reflect (3 potent in vivo immunoregulatory activity of T-cells occurring in such patients. Appar-
Table 4. B-Cell Growth Factor and B-Cell Differentiation Factor Secretion of Malignant Lymph Node Cell T-Cells
BCDF (ng/ml)t BCGF' Patient no. (cpm)
1$ 9485 1580 1200 2 16,720 2120 1290 3 2160 970 160 4 1940 650 140 5 1.2,710 2410 970 6 9560 1760 820 7 8490 2130 700 8 1 0,750 6420 110 TBh (n = 8) 5490 f 14307 3850 f 980 2530 f 560 Control (n = 8) 4340 f 1080 8210 f 1130 4160 f 940 BCGF: B-cell growth factor, BCDF: B-cell differentiation factor; Ig: immuno- globulin; TB: tuberculosis.
'H-thymidine incorporation, cpm, was determined in a proliferation assay of normal B-cells with T-cell-stimulated culture supernatants. t IgM and IgG secretion was determined by culturing B-cells with T-cell-stim- ulated culture Supernatants in costimulator assay. $ LNC C D 4 i T-cells of lymphoma cases (1-8) as shown in Table 2. 5 LNC T-cells of patients with TB. I1 Blood purified T-cells of normal control sublects 1 Mean f standard error of the mean.
ently, the deficient allogeneic MLR activity of malig- nant T-cells may be related to the abnormal cell-me- diated immunity.
The results presented here demonstrate differences in the expression of IL-2R and IL-2 production by PHA-stimulated malignant LNC T-cells of different phenotypes. Although IL-2R is expressed on resting ma- lignant T-cells, regardless of their immunologic pheno- types, only PHA-stimulated malignant CD4+ T-cells expressed more IL-2R and secreted higher concentra- tions of IL-2. It was rather surprising to observe that expression of IL-2R on PHA-stimulated malignant CD8+ and CD4f CD8f T-cells was even lower than that of the resting T-cells. The precise events of the cellular interactions leading to IL-2R expression remain to be elucidated. However, IL-2R, a cell surface protein, had a dynamic and changing pattern of expression on typical CD8f and CD4+ CD8+ malignant T-cells. It is likely that PHA causes a conformational change of the IL-2R molecule or blocks the IL-2R-expressing epitope on the cell surface, thus enabling its detection by anti- Tac MoAb.
The observation that malignant T-cells from some patients with lymphoproliferative disordersl0," express large numbers of IL-2R, whereas normal resting cells do not, may provide the scientific basis for therapeutic trials involving agents to eliminate IL-2R-expressing malignant cells.'' In recent years, there has been a lot of interest in the therapeutic application of IL-2 or MoAb to IL-2R (anti-Tac).6 Administration of anti-Tac has

838 CANCER February 7, 1993, Volume 71, No. 3
been attempted in adult T-cell lymphoma leukemia, in which the malignant T-cells expressed elevated levels of IL-2R.6 A transient response was observed in two patients and a remission lasting 6 months in a third patient6 Studies also have been initiated to define the value of anti-Tac in the treatment of aplastic anemia, after Zoumbos et a1.22 demonstrated that some patients with aplastic anemia have large numbers of circulating IL-2R-positive T-cells. Several other studies have indi- cated that IL-2R also were expressed on a variety of other neoplastic cells, B-cell lymphomas,23 Reed-Stern- berg cells in Hodgkin disease, and cells of monocyte- macrophage lineage.23,24 The precise physiologic role of the IL-2R on B-cells, Reed-Sternberg cells, and cells of monocyte-macrophage lineage is not known. Demon- stration of IL-2R on peripheral T-cell lymphomas and other non-T-cell malignant neoplasms, in which IL-2R are expressed on malignant cells, may be an appropriate situation for this form of therapy.6 Because of the de- fective expression of IL-2R and IL-2 activity in PHA- stimulated malignant CD8+ or CD4+ CD8+ T-cells, it would be interesting to know whether therapeutic mo- dalities differ in such patients.
In conclusion, an immunologic spectrum exists in peripheral T-cell lymphomas, with malignant LNC T- cells demonstrating increased AMLR activity and defi- cient allogeneic MLR activity, and malignant CD4+ T- cells expressing an increased percentage of PHA-in- duced IL-2R and increased IL-2 secretion. It was interesting to observe that malignant LNC CD4+ T- cells of patients without humoral immunodeficiency secreted highly increased levels of BCGF but were defi- cient in BCDF activity. We also demonstrated that hy- pogammaglobulinemia (Patients 3 and 4) and IgM hy- pergammaglobulinemia (Patient 8) observed in these patients with peripheral T-cell lymphomas were asso- ciated closely with a T-cell defect regarding secretion of two important lymphokines, BCGF and BCDF. The in- creased AMLR activity of malignant LNC T-cells indi- cates an important biologic role of AMLR in the im- mune response of this disease.
References
Weksler ME, Moody CE, Kozak RW. Autologous mixed lym- phocyte reaction. Adz) I r r i f r r i i i r d 1981; 31:271-321. Smith JB, De-Horatius RJ. Deficient autologous mixed lympho- cyte culture reaction correlates with disease activity in systemic lupus erythematosus and rheumatoid arthritis. Cliu E x p Im-
Smith JB, Knowlton RP, Koons LS. Immunologic studies in chronic lymphocytic leukemia: defective stimulation of T cell proliferation in autologous mixed lymphocyte culture. / Nut1 Cancer I n s t 1977; 58:579-85. Engleman EG, Benike C], Hoppe RT, Kaplan HS, Berberich FR. Autologous mixed lymphocyte reaction in patients with Hodg- kin's disease. / Clirr I I I D E S ~ 1980; 66:149-58.
I?IlttIol 1982; 481155562.
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
Smith JB, Knowlton RP, Harris DT. Functional aspects of T cells from patients with non-Hodgkin's lymphoma: response to self, TNP-modified and alloantigens. Caiicer 1983; 52:1160-4. Waldmann TA. The structure, function and expression of inter- leukin-2 receptors o n normal and malignant lymphocytes. Scicrrce 1986; 232:727-32. Pinkus GS, Said JW. Characterization of non-Hodgkin's lym- phoma using multiple cell markers. Am ] Pathol 1978; 94:349- 80. Knowles DM 11, Halper JP. Human T cell malignancies: correla- tive, histopathologic, immunologic and cytochemical analysis of 23 cases. Ani / Pathcil 1982; 106:187-203. Weiss LM, Crabtree GS, Rouse RV, Warnke RA. Morphologic and immunologic characterization of 50 peripheral T cell lym- phomas. Ail7 / Pnthol 198.5; 118:316-24. Foon KA, Todd RF. Immunologic classification of leukemia and lymphoma. Blood 1986; 68:l-31. Sheibani K, Winberg CD, De-Velde SV, Blayney DW, Rappaport H. Distribution of lymphocytes with interleukin-2 receptor (TAC antigen) in reactive lymphoproliferative processes, Hodg- kin's disease and non-Hodgkin's lymphomas: an immunohisto- logical study of 300 cases. Am / Pafliol 1987; 127:27-37. Rappaport H. Tumors of the hematopoietic system. In: Atlas of tumor pathology, section 3, fascicle 8. Washington, D.C.: U.S. Armed Forces Institute of Pathology, 1966:91-206. Raziuddin S, Hussain NK, Latif ABA. A monoclonal antibody and functional study of malignant T cells of a patient with sup- pressor T cell lymphoma. Cliii Ininiuriol Imrnnrloparkol 1987;
Raziuddin S, Sheikha AK. Phenotypic and functional T cell sub- set abnormalities in patients with aplastic anemia and hypo- gammaglobulinemia. Br J HRPnlatol 1988; 70:283-7. Raziuddin S, Sheikha A, Teklu B. Humoral immunodeficiency in T cell chronic lymphocytic leukemia: an immunologic assess- ment. Carrrcr 1991; 67:2518-22. Mayer L, Kwan SP, Thompson C. Evidence for a defect in switch T cells in patients with immunodeficiency and IgM hypergam- maglobulinemia. N €fig1 / M r d 1986; 314:409-13. Fiorilli M, Russo G, Paganelli R. Hypogammaglobulinemia with hyper IgM, severe T cell defect and abnormal recirculation of OKT4+ lymphocytes in a girl with chronic lymphadenopathy. Cliri l i m i i ~ r ~ o 1 Iiriiriirriopafhol 1986; 38:256-64. Durham JC, Stephens DS, Rimland D, Nassar VH, Spiral TJ. Common variable hypogammaglobulinemia complicated by an unusual T-suppressor/cytotoxic cell lymphoma. Cancer 1987;
Hom JT, Tala1 N. Decreased syngeneic mixed lymphocyte reac- tion in autoimmune susceptible mice. Scaiid ] Inirnunol 1982;
Raziuddin S, Malatani T, Al-Sedairy S, Al-Saigh A. Peripheral T cell lymphomas: immunophenotype, lymphokine production, and immunologic functional characteristics of the lymph node malignant T cells. Am ] Patliol 1991; 139:1181-9. Strauchen ]A, Breakstone BA. IL-2 receptor expression in hu- man lymphoid lesions: immunohistochernical study of 166 cases. Am / Puthol 1987; 126:500-12. Zoumbos NC, Gascon P, Djeu J, Frost SR, Young NS. Circulat- ing activated suppressor T lymphocytes in aplastic anemia. N E q l Med 1985; 312:257-65. Linder J, Daley DT, Armitage JO, Kay DH, Klassen LW, Weisen- berger 0. Interleukin-2 receptor (Tac) expression in non-Hodg- kin's lymphoma [abstract]. Lab Irioest 1985; 52:39A. Pizzolo G, Chilosi M, Semenzato G, Caligaris-Cappio F, Fiore- Donato L, Perona G, et al. lmmunohistological analysis of Tac antigen expression in tissues involved by Hodgkin's disease. Br ] Carirrr 1984; 50:415-7.
451230-4.
59~271-6.
15:195-?03.