peripheral arterial disease physicians awareness program
Post on 20-Dec-2015
219 views
TRANSCRIPT

Peripheral Arterial DiseasePeripheral Arterial Disease
Physicians Awareness ProgramPhysicians Awareness Program


3
ObjectivesObjectives
▪Increase the awareness of physicians (general practitioners, internists, cardiologists, and vascular surgeons) in Saudi Arabia about PAD
▪Educate physicians about the importance of risk reduction therapies, in order to close the care, knowledge and action gaps.

4
AgendaAgenda
Part I: Overview of Disease
▪ Atherothrombosis
▪ Epidemiology
▪ Management
Part II: Guidelines
▪ CV Risk Factor Reduction
( AHA/ACC, TASC II)

Part I – Overview of DiseasePart I – Overview of Disease

6
What is Atherosclerosis?What is Atherosclerosis?
Clogging, narrowing, and hardening of large and medium-sized arteries

7
What are the risk factors for Atherosclerosis?What are the risk factors for Atherosclerosis?
Non-Modifiable Risk Factors:Non-Modifiable Risk Factors: Male genderMale gender Advanced ageAdvanced age Family historyFamily history
Modifiable Risk Factors:Modifiable Risk Factors: Major Major SmokingSmoking HypertensionHypertension DiabetesDiabetes HyperlipidemiaHyperlipidemia
MinorMinor HomocystenemiaHomocystenemia ObesityObesity Hypercoaguable stateHypercoaguable state Physical inactivityPhysical inactivity

8
InflammationAccumulationof lipids
Normalartery
Smooth muscle cell progression,
plaque progression
Thrombus FormationThrombus Formation
Rupture of Fibrous Cap
Erosion of Endothelium
Erosion of Calcium Nodule
Intraplaque Hemorrhage
Pathophysiology of AtherothrombosisPathophysiology of Atherothrombosis
1. Munger MA et al. J Am Pharm Assoc. 2004;44(suppl 1):S5-S13.2. Libby P et al. Circulation. 2005;111:3481-3488.
AtherosclerosisAtherosclerosis +
Atherosclerosis leads to any number of four possible types of thrombus formation

9
Cerebrovascular disease
Coronary artery disease
Renal artery Diseases
Visceral arterial disease
Peripheral arterial disease• Intermittent claudication• Critical limb ischemia
Clinical Spectrum Clinical Spectrum
of Atherosclerosisof Atherosclerosis

10Munger MA et al. J Am Pharm Assoc. 2004;44(suppl 1):S5-S13.
Atherothrombosis: Atherothrombosis: Can Manifest in Multiple Vascular Beds Can Manifest in Multiple Vascular Beds
▪ Patients with atherothrombosis have thrombus formations that can manifest in multiple vascular beds throughout the body
▪ Atherothrombosis is a process that includes the following clinical consequences:
– Ischemic stroke, MI, and PAD

11
Atherothrombosis as a Cause of DeathAtherothrombosis as a Cause of Death“Burden of the disease”“Burden of the disease”
4.9%6.5%
9.1%
12.5%
19.1%
22.3%
0
5
10
15
20
25
Mo
rta
lity
(%
)
Athero-thrombosis
InfectiousDisease
Cancer Injuries PulmonaryDisease
AIDS
According to the World Health Organization in 2004 atherothrombosis* was the leading cause of death worldwide—more than AIDS and cancer combined1,2
According to the World Health Organization in 2004 atherothrombosis* was the leading cause of death worldwide—more than AIDS and cancer combined1,2
* Only includes ischemic heart disease and cerebrovascular disease.1. Bakhai A. Pharmacoeconomics. 2004;22(suppl 4):11-18.2. World Health Organization Report 2004. Available at: http://www.who.org. Accessed January 29, 2007.

Let’s Talk about Let’s Talk about PADPAD

13
AsymptomaticAsymptomatic
SymptomaticSymptomatic
•Intermittent claudicationIntermittent claudication•Critical Limb IschemiaCritical Limb Ischemia Pain at restPain at rest Tissue lossTissue loss GangreneGangrene
How do patients with PAD present?How do patients with PAD present?

14
How do patients with PAD present?How do patients with PAD present?

15
Symptomatic 10%
Asymptomatic 90%
How do patients with PAD present?How do patients with PAD present?

16
Ankle Brachial IndexAnkle Brachial Index

17
Calculating the Ankle-Brachial IndexCalculating the Ankle-Brachial Index
Higher right ankle pressure (dorsalis pedis or posterior tibial pulse)
Higher arm pressure (of either arm)
=
Right leg ABIRight leg ABI Left leg ABILeft leg ABI
Higher left ankle pressure (dorsalis pedis or posterior tibial pulse)
Higher arm pressure (of either arm)
=
ABI InterpretationABI Interpretation≤≤0.90 is diagnostic of peripheral arterial disease0.90 is diagnostic of peripheral arterial disease
Norgren L et al. Eur J Vasc Endovasc Surg. 2007;33(suppl 1):S1-S75.

18
Role of ABI in PADRole of ABI in PAD
▪ Confirms the diagnosis of PAD
▪ Detects significant PAD in (sedentary) asymptomatic patients
▪ Used in the differential diagnosis of leg symptoms to identify a vascular etiology
▪ Identifies patients with reduced limb function (inability to walk defined distances or at usual walking speed)
▪ Provides key information on long-term prognosis– A 3–6-fold increased risk of CV mortality with an ABI <0.90
▪ Provides further risk stratification– A lower ABI indicating worse prognosis
– A Framingham risk score between 10%–20%
▪ Highly associated with coronary and cerebral artery disease
Norgren L et al. Eur J Vasc Endovasc Surg. 2007;33(suppl 1):S1-S75.

Epidemiology of PADEpidemiology of PAD

20
19.1% 19.8%
Prevalence was estimated using different methods1. Meijer WT et al. Arterioscler Thromb Vasc Biol. 1998;18:185-192. 2. Diehm C et al. Atherosclerosis. 2004;172:95-105. 3. Selvin E et al. NHANES. Circulation. 2004;110:738-743.4. Criqui MH et al. Circulation. 1985;71:510-515.5. Hirsch AT et al. JAMA. 2001;286:1317-1324.
Prevalence of PADPrevalence of PAD
14.5%
29.0%
11.7%
4.3%
PARTNERSPARTNERS55
Age >70, or between 50–69 with history of diabetes or smoking
San DiegoSan Diego44
Mean Age=66DiehmDiehm22
Age ≥65RotterdamRotterdam11
Age >55NHANESNHANES33
Age ≥70NHANESNHANES33
Age >40
European Data US Data
11.7%
Saudi Data
Pilot StudyPilot Study66
Age >45
6. Alshaekh et al. SMJ. 2007;28:412-414

21
Why it is important to recognize Why it is important to recognize patients with PAD? patients with PAD?
PAD is a marker of PAD is a marker of systemicsystemic atherosclerosis atherosclerosis
Patients with either symptomatic or Patients with either symptomatic or asymptomatic PAD generally have asymptomatic PAD generally have widespread widespread arterial diseasearterial disease

22
CVD
16.6%CAD
44.6%8.4%
1.2%4.7%
1.6%
PAD
4.7%
The REACH Registry found overlapping manifestations of disease in patients with CAD, CVD, and PAD
The REACH Registry found overlapping manifestations of disease in patients with CAD, CVD, and PAD
sanofi-aventis and Bristol-Myers Squibb provide funding for the REACH Registry.The REACH Registry includes patients with conditions for which clopidogrel may not be indicated.Bhatt DL et al. JAMA. 2006;295:180-189.
18.3% of patients in the REACH Registry did not have manifestations of atherothrombosis, but were included based on risk factors
18.3% of patients in the REACH Registry did not have manifestations of atherothrombosis, but were included based on risk factors
Peripheral Arterial Disease: Peripheral Arterial Disease: Prevalence of Polyvascular diseasePrevalence of Polyvascular disease
Peripheral Arterial Disease:Prevalence of Polyvascular Disease
Adapted from: Bhatt DL et al. JAMA. 2006;295(2):180-189.
Coronary disease
Cerebrovasculardisease
Peripheralarterial disease
16.6%
1.2% 4.7%
44.6%
1.6%
8.4%
4.7%
15.9%
~16% of patients had manifestations of
atherothrombosis in more than one arterial bed

23
Long term Risk of MI & StrokeLong term Risk of MI & Stroke
PAD places individuals at high short term risk of MI, Stroke & Death

24
Survival of Patients With PADSurvival of Patients With PADS
urv
ival
(%
)
Follow-up (years)
Controls
IC
CLI
0 5 10 150
20
40
60
80
100
CLI=critical limb ischemia.IC=intermittent claudication.Norgren L et al. Eur J Vasc Endovasc Surg. 2007;33(suppl 1):S1-S75.
Life expectancy reduced 10 years in patients with
PAD
Mortality rate~ 25% at 5 years
~ 50% at 10 years~ 75% at 15 years

25
Natural HistoryNatural History
Annual risk :
- Mortality 6.8%
- MI 2.0%
- Intervention 1.0%
- Amputation 0.4%
Ouriel K, Lancet 2001; 358: 1257-64.

26
3.8
1.41.51.8
5.3
3.6
1.0
1.8
4.3
1.71.3
2.4
0
1
2
3
4
5
6
CV Death Nonfatal MI Nonfatal Stroke Death/MI/Stroke
CAD
CVD
PAD
sanofi-aventis and Bristol-Myers Squibb provide funding for the REACH Registry.The REACH Registry includes patients with conditions for which clopidogrel may not be indicated.Rates adjusted for age and risk factors.Steg G. Oral presentation at American College of Cardiology. 2006. Available at: http://acc06online.acc.org/sessions.aspx?date=12. Accessed January 28, 2007.
Major Adverse Cardiac Events in Symptomatic Patients Major Adverse Cardiac Events in Symptomatic Patients With CAD, CVD, or PAD at 1 YearWith CAD, CVD, or PAD at 1 Year
Patients with PAD experienced high CV mortalityPatients with PAD experienced high CV mortality
% o
f P
atie
nts
REACH Registry

27
1.2
Single Arterial BedSingle Arterial Bed Polyvascular Disease CAD + CVD + PAD
CAD alone
OverallPAD alone Overall
CVD alone
26.9(‡)
7.4
4.0
1.8
3.6
22.018.2(§)10.0(†)13.312.8
6.02.34.5(†)3.13.4
3.10.63.5(†)0.91.5
1.51.00.5(†)1.41.2
1.51.5 2.41.4
Major End Points as a Function of Single vs Multiple Major End Points as a Function of Single vs Multiple and Overlapping Locationsand Overlapping Locations
sanofi-aventis and Bristol-Myers Squibb provide funding for the REACH Registry. The REACH Registry includes patients with conditions for which clopidogrel may not be indicated.* TIA, unstable angina, other ischemic arterial event including worsening of peripheral arterial disease.
Steg G. Oral presentation at American College of Cardiology. 2006. Available at: http://acc06online.acc.org/sessions.aspx?date=12. Accessed January 28, 2007.
CV death / MI/ stroke/ hospitalization*
CV death / MI/ stroke
Non-fatal stroke
Non-fatal MI
CV death
REACH Registry
† P<0.001 (ref class: CAD alone)‡ P<0.001 (ref class: CAD + CVD)§ P<0.001 (ref class: PAD alone)
Risk doubles with polyvascular diseaseRisk doubles with polyvascular disease

28
Relationship Between ABI and Relationship Between ABI and Fatal and Non-fatal CV eventsFatal and Non-fatal CV events
The lower the ABI the higher the 5-year risk of a cardiovascular event The lower the ABI the higher the 5-year risk of a cardiovascular event
Od
ds
of
MI,
Str
oke
or
CV
dea
th
Baseline ABI
1.4
0
40
35
30
25
20
15
10
5
1.21.00.80.60.40.20.0
45
Mehler PS et al. Circulation. 2003;107:753-756. Norgren L et al. Eur J Vasc Endovasc Surg. 2007;33(suppl 1):S1-S75

29
All Cause Mortality as a All Cause Mortality as a Function of Baseline ABIFunction of Baseline ABI
Resnick HE et al. Circulation. 2004;109:733e739.Norgren L et al. Eur J Vasc Endovasc Surg. 2007;33(suppl 1):S1-S75.
0
10
20
30
40
50
60
70
Baseline ABI
Pe
rce
nt
(%)
▪ PAD patients with an ABI ≤0.90 are at increased risk for cardiovascular events and all cause mortality as ABI decreases
▪ Patients with an ABI >1.40 have underlying diseases, such as diabetes, renal insufficiency or other diseases that cause vascular calcification, or the tibial vessels at the ankle to become non-compressible
<0.60 0.60–<0.70
0.70–<0.80
0.80–<0.90
0.90–<1.0
1.0–<1.10
1.40–<1.50
1.50 Incom-pressible
There appears to be an inverse correlation between mortality and ABI There appears to be an inverse correlation between mortality and ABI

Management of PADManagement of PAD

31
What are the Goals of treating patients with PAD?What are the Goals of treating patients with PAD?
Relief symptomsRelief symptoms
Improve quality of lifeImprove quality of life
Limb salvageLimb salvage
Prolong survivalProlong survival

32
Strategies in treating patients with PADStrategies in treating patients with PAD
Improve Lower Limb CirculationImprove Lower Limb Circulation
Risk Factors Modification

33
Improve Lower Limb Circulation• Conservative (Exercise Program)Conservative (Exercise Program)• Intervention ( Revascularization)Intervention ( Revascularization) - Angioplasty +/- Stenting- Angioplasty +/- Stenting - Surgical Bypass - Surgical Bypass
Strategies in treating patients with PADStrategies in treating patients with PAD

34
Strategies in treating patients with PADStrategies in treating patients with PAD
Risk Factors Modification• Diet and weight controlDiet and weight control• ExerciseExercise• Antiplatlets Antiplatlets • Hypertension controlHypertension control• Diabetes controlDiabetes control• Lipid controlLipid control• Smoking CessationSmoking Cessation

Part II – Guidelines for Risk Part II – Guidelines for Risk Factors ModificationFactors Modification

36
AHA/ACCAHA/ACC

37
AHA/ACC formatAHA/ACC format

38
Weight Management
Encourage weight reduction/maintenance
Balance of physical activity, caloric intake, and formal Balance of physical activity, caloric intake, and formal behavioral programsbehavioral programs
Adapted from : ACC/AHA Guidelines for the Management of Patients With Peripheral Arterial Disease. J Am Coll Cardiol. 2006.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Goal:Goal: Body mass index:Body mass index: 18.5 to 24.9 kg/m² 18.5 to 24.9 kg/m²
Waist circumference:Waist circumference: men <40 inches men <40 inches
women < 35 incheswomen < 35 inches

39
Physical Activity
Moderate-intensity aerobic activity
Medically supervised programs for high risk
Adapted from : ACC/AHA Guidelines for the Management of Patients With Peripheral Arterial Disease. J Am Coll Cardiol. 2006.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Goal: Goal:
30 minutes, 7 days per week (minimum 5 days/week)30 minutes, 7 days per week (minimum 5 days/week)

40
Smoking
Ask about smoking
Advise to quit
Counseling
Referal to special program
Pharmacotherapy
Adapted from : ACC/AHA Guidelines for the Management of Patients With Peripheral Arterial Disease. J Am Coll Cardiol. 2006.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Goal: Goal:
Complete CessationComplete Cessation

41
Pharmacologic Risk Reduction Pharmacologic Risk Reduction StrategiesStrategies
ASA and other anti-platelet agentsASA and other anti-platelet agents
Hypertension ControlHypertension Control
Lipid ControlLipid Control
Diabetes ControlDiabetes Control
Angiotensin Converting Enzyme Inhibitors (ACE-I)Angiotensin Converting Enzyme Inhibitors (ACE-I)

42
Antiplatelet Therapy
Antiplatelet therapy is indicated to reduce the risk of myocardial infarction, stroke, or vascular death in individuals with atherosclerotic lower extremity PAD.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Adapted from : ACC/AHA Guidelines for the Management of Patients With Peripheral Arterial Disease. J Am Coll Cardiol. 2006.
▪ The Antithrombotic Trialists’ Collaboration involved 42 trials and 9716 patients with peripheral arterial disease.
▪ 23% reduction for adverse cardiovascular events, including myocardial infarction, stroke, or vascular death

43
Efficacy of Clopidogrel vs Aspirin in MI, Efficacy of Clopidogrel vs Aspirin in MI, Ischemic Stroke, or Vascular Death (N=19,185)Ischemic Stroke, or Vascular Death (N=19,185)11
Months of Follow-Up
Cu
mu
lati
ve
Eve
nt
Rat
e (%
)
0
4
8
12
16
Clopidogrel
Aspirin Overall Relative RiskReduction2
8.7%*
0 3 6 9 12 15 18 21 24 27 30 33 36
Aspirin
Clopidogrel
P=0.0452
* ITT analysis.1. CAPRIE Steering Committee. Lancet. 1996;348:1329-1339.2. Clopidogrel Prescribing Information.
Median Follow-up=1.91 years
Study subjects had either recent MI, recent
ischemic stroke, or established peripheral
arterial disease.
CAPRIE

44
Outcomes by Subgroup AnalysisOutcomes by Subgroup Analysis
* CAPRIE: primary combined end point (myocardial infarction, ischemic stroke, vascular death): RRR 8.7% (P=0.045) for patients with PAD, post-myocardial infarction, post-ischemic stroke. CAPRIE subgroup analysis: for PAD patients the secondary end point, myocardial infarction, was reduced by 23.8% (RRR).
† Since the CAPRIE Trial was not powered to evaluate the efficacy of individual sub-groups, it is not clear whether the differences in RRR across qualifying conditions are real or a result of chance. CAPRIE Steering Committee. Lancet. 1996;348:1329-1339.
-40 -30 -20 -10 0 10 20 30 40
PAD
All patients
Aspirin Better Clopidogrel Better
Mean & 95% CI
CAPRIE
Clopidogrel Reduced the Risk of MI/Ischemic Stroke/Cardiovascular Death in PAD Patients by 23.8%* Compared to ASA†

45
Antihypertensive Therapy
Antihypertensive therapy should be administered to
hypertensive patients with lower extremity PAD to a goal of less
than 140/90 mmHg (non-diabetics) or less than 130/80 mm/Hg
(diabetics and individuals with chronic renal disease) to reduce
the risk of myocardial infarction, stroke, congestive heart
failure, and cardiovascular death.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
Adapted from : ACC/AHA Guidelines for the Management of Patients With Peripheral Arterial Disease. J Am Coll Cardiol. 2006.

46
Lipid Lowering Therapy
Treatment with an HMG coenzyme-A reductase inhibitor
(statin) medication is indicated for all patients with peripheral
arterial disease to achieve a target LDL cholesterol of less than
100 mg/dl.
Adapted from : ACC/AHA Guidelines for the Management of Patients With Peripheral Arterial Disease. J Am Coll Cardiol. 2006.
▪ Cholesterol Treatment Trialists Coolaborators Meta-analysis data from 90 056 participants in 14 randomized trials of statins
▪ 21% reduction for adverse cardiovascular events, including myocardial infarction, stroke, or vascular death
(Lancet 2005; 366:1267-78)
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII

47
Treatment of diabetes in individuals with lower extremity PAD by administration of glucose control therapies to reduce the hemoglobin A1C to less than 7% can be effective to reduce microvascular complications and potentially improve cardiovascular outcomes.
Adapted from : ACC/AHA Guidelines for the Management of Patients With Peripheral Arterial Disease. J Am Coll Cardiol. 2006.
Diabetes Therapies
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII

48
ACE inhibitors
ACE inhibitors is indicated to reduce the risk of myocardial infarction, stroke, or vascular death in individuals with atherosclerotic lower extremity PAD.
Adapted from : ACC/AHA Guidelines for the Management of Patients With Peripheral Arterial Disease. J Am Coll Cardiol. 2006.
▪ The HOPE study involved 9297 AS patients.
▪ 25% reduction for adverse cardiovascular events, including myocardial infarction, stroke, or vascular death
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII

49
TASC IITASC II

50
Goals of TASC IIGoals of TASC II
▪ Update and expand the consensus statement from 2000
▪ Maintain focus on peripheral arterial disease
▪ Make the document accessible to a wider audience – Including primary care physicians
▪ Reduce the length of the document
▪ Inclusion of Europe, North America, Asia, Africa, Australia
Norgren L et al. Eur J Vasc Endovasc Surg. 2007;33(suppl 1):S1-S75.

51
TASC II Participating SocietiesTASC II Participating Societies
▪ American College of Cardiology
▪ American Diabetes Association
▪ American Podiatric Medical Association
▪ Canadian Society for Vascular Surgeons
▪ Cardiovascular and Interventional Radiology Society of Europe
▪ CoCaLis collaboration
▪ European Society for Vascular Surgery
▪ International Diabetes Federation
▪ International Union of Angiology
▪ Interventional Radiology Society of Australasia
▪ Japanese College of Angiology
▪ Society for Cardiovascular Angiography and Intervention
▪ Society for Vascular Surgery
▪ Society of Interventional Radiology
▪ Society for Vascular Medicine & Biology
▪ Vascular Society of Southern Africa
Norgren L et al. Eur J Vasc Endovasc Surg. 2007;33(suppl 1):S1-S75.

52
TASC Grade DefinitionTASC Grade Definition
Grade Definition
A ▪ Based on the criterion of at least 1 randomized controlled clinical trial as part of the body of literature of overall good quality and consistency addressing the specific recommendation
B ▪ Based on well-conducted clinical studies but no good quality randomized clinical trials on the topic of recommendation
C ▪ Based on evidence obtained from expert committee reports or opinions and/or clinical experiences of respected authorities (ie, no applicable studies of good quality)
TASC II
Norgren L et al. Eur J Vasc Endovasc Surg. 2007;33(suppl 1):S1-S75.

53
PAD Patients Are at Increased PAD Patients Are at Increased Risk for CV Ischemic EventsRisk for CV Ischemic Events
PAD Patients ≥50 Years and Older Initial Presentation*
SymptomaticSymptomatic
~40% of Patients ~40% of Patients
AsymptomaticAsymptomatic
~60% of Patients ~60% of Patients
The majority of PAD patients remain highly
underdiagnosed
The majority of PAD patients remain highly
underdiagnosed
* Excluding patients with an initial presentation of critical limb ischemia.Adapted from Hirsch AT et al. Available at: www.acc.org. Accessed January 26, 2007.Adapted from Norgren L et al. Eur J Vasc Endovasc Surg. 2007;33(suppl 1):S1-S75.
Up to 35% of PAD patients will have an MI/stroke or
die in the next 5 years
Up to 35% of PAD patients will have an MI/stroke or
die in the next 5 years
Limb MorbidityLimb Morbidity70%–80%70%–80%Stable claudication Stable claudication
10%–20%10%–20%Worsening claudicationWorsening claudication
5%–10%5%–10%Critical limb ischemiaCritical limb ischemia
MortalityMortality10%–15%10%–15%75% from CV causes75% from CV causes
5-year Outcomes5-year Outcomes
CV MorbidityCV Morbidity
20%20%Nonfatal CV event Nonfatal CV event (MI or stroke)(MI or stroke)

54
History and Physical Examination History and Physical Examination in Patients With Suspected PADin Patients With Suspected PAD
Grade Recommendations
B ▪ Individuals with risk factors for PAD, limb symptoms on exertion, or reduced limb function should undergo a vascular history to evaluate for symptoms of claudication or other limb symptoms that limit walking ability
B ▪ Patients at risk for PAD or patients with reduced limb function should also have a vascular examination evaluating peripheral pulses
B ▪ Patients with a history or examination suggestive of PAD should proceed to objective testing including an ABI
Norgren L et al. Eur J Vasc Endovasc Surg. 2007;33(suppl 1):S1-S75.

TASC II Guidelines – TASC II Guidelines – Ankle Brachial Index (ABI)Ankle Brachial Index (ABI)

56
Ankle-Brachial Index (ABI)Ankle-Brachial Index (ABI)
▪ The primary non-invasive screening test for PAD is the ankle-brachial index
▪ The American Diabetes Association recommends a screening with an ABI every 5 years in patients with diabetes
▪ The ABI should become a routine measurement in the primary care practice of medicine
TASC II
Norgren L et al. Eur J Vasc Endovasc Surg. 2007;33(suppl 1):S1-S75.

57
Grade ABI screening in the primary care setting
B ▪ All patients who have exertional leg symptoms
B ▪ All patients between the age of 50–69 and who have a cardiovascular risk factor (particularly diabetes or smoking)
B ▪ All patients age ≥70 years regardless of risk-factor status
C ▪ All patients with a Framingham risk score 10%–20%
TASC II
Ankle-Brachial Index (ABI)- Screening Ankle-Brachial Index (ABI)- Screening RecommendationsRecommendations
Norgren L et al. Eur J Vasc Endovasc Surg. 2007;33(suppl 1):S1-S75.

58
ABI for Assessing Systemic RiskABI for Assessing Systemic Risk
Secondary prevention†Secondary prevention†
• Evaluate the patient for symptoms of PAD
• Manage claudicationand CLI if present
• Evaluate the patient for symptoms of PAD
• Manage claudicationand CLI if present
High>20%High>20%
Low<10%Low
<10%
≤0.90≤0.90
Moderate20%–10%Moderate20%–10%
ABIABI
>0.90>0.90 Primary prevention*Primary prevention*
Cardiovascular 10-year risk score:
* Primary prevention=No antiplatelet therapy; LDL (low density lipoprotein) <130 mg/dL; appropriate blood pressure (<140/90 mmHg and <130/80 mmHg in diabetes/renal insufficiency).
† Secondary prevention=Prescribe antiplatelet therapy; LDL <100 mg/dL (<70 mg/dL in very high risk); appropriate blood pressure (<140/90 mmHg and <130/80 mmHg in diabetes/renal insufficiency).Norgren L et al. Eur J Vasc Endovasc Surg. 2007;33(suppl 1):S1-S75.
TASC II

TASC-II Guidelines for Risk ReductionTASC-II Guidelines for Risk Reduction

60
TASC Guidelines Recommend TASC Guidelines Recommend CV Risk Reduction and Symptom ReliefCV Risk Reduction and Symptom Relief
Evidence Basis for Selected Treatment RecommendationsEvidence Basis for Selected Treatment Recommendations
CV Risk ReductionCV Risk Reduction Treatment for Claudication*Treatment for Claudication*
Recommendations Grade Recommendations Grade
Smoking cessation A Supervised exercise training
A
Statin therapy A
Antihypertensive therapy A
Glucose control therapy C
Folate supplementation B
Antiplatelet therapy A
* To improve symptoms and increase walking distance.Norgren L et al. Eur J Vasc Endovasc Surg. 2007;33(suppl 1):S1-S75

61
Antiplatelet TherapyAntiplatelet Therapy
Grade Recommendations
A ▪ All symptomatic patients with or without a history of other cardiovascular disease should be prescribed an antiplatelet drug long term to reduce the risk of cardiovascular morbidity and mortality
A ▪ Aspirin is effective in patients with PAD who also have clinical evidence of other forms of cardiovascular disease (coronary or carotid)
C ▪ The use of aspirin in patients with PAD who do not have clinical evidence of other forms of cardiovascular disease can be considered
B ▪ Clopidogrel is effective in reducing cardiovascular events in a subgroup of patients with symptomatic PAD, with or without other clinical evidence of cardiovascular disease
Norgren L et al. Eur J Vasc Endovasc Surg. 2007;33(suppl 1):S1-S75.

62
So, Let’s wrap-up

63
Who should be screened for PAD?Who should be screened for PAD?
Age > 45 yearsAge > 45 years
Patients with Atherosclerotic risk factorsPatients with Atherosclerotic risk factors

64
What is the best way to screen?What is the best way to screen?
ABIABI
65
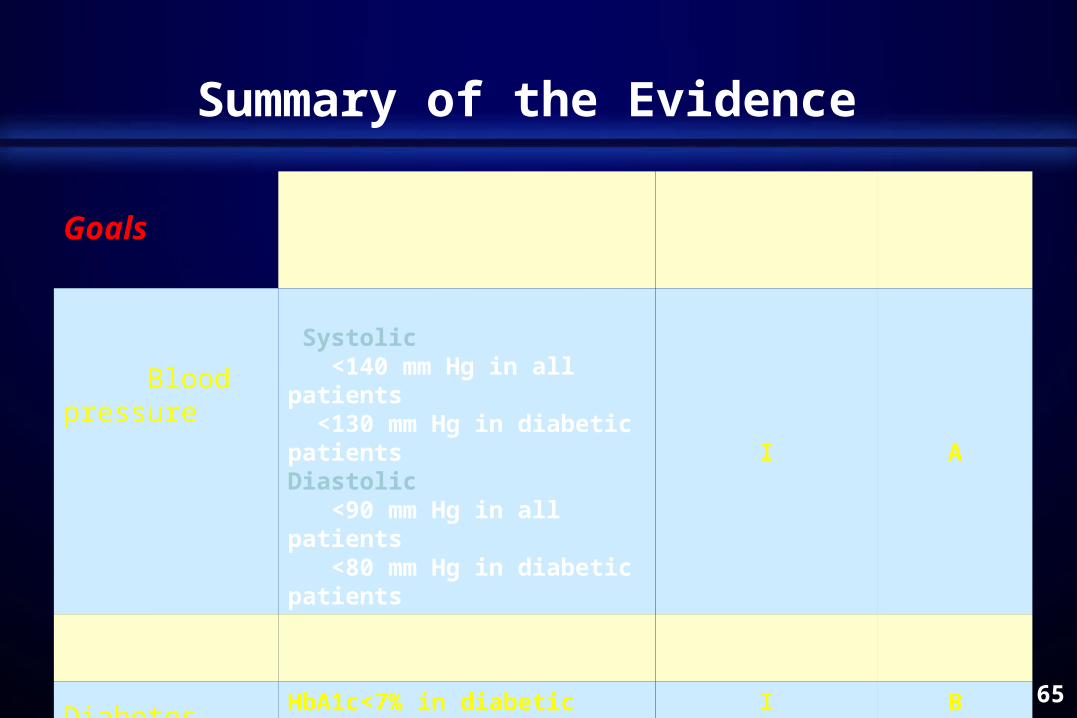
Summary of the Evidence
Goals
RecommendationClass of
recommendationLevel of evidence
Blood pressure
Systolic <140 mm Hg in all patients <130 mm Hg in diabetic patientsDiastolic <90 mm Hg in all patients <80 mm Hg in diabetic patients
I A
LDL-C LDL< 2.5 mmol/l in all patients I A
Diabetes HbA1c<7% in diabetic patients I B
Smoking Complete cessation in all patients I B
BMI 18.5-24.9 kg/m2 in all patients I B

66
Summary of the Evidence
Medications Recommendation
Class of recommendation
Level of evidence
Antiplatlets All patientsI A
Statins All patients I A
ACE inhibitors Symptomatic patientsAsymptomatic patients
I IIa
B B

67
Take home messageTake home message
▪ PAD is a marker for systemic atherosclerosis
▪ PAD is associated with increased risk of cardiovascular mortality and morbidity
▪ Majority of patients with PAD are asymptomatic
▪ Individuals with atherosclerotic risk factors should be screened for PAD (ABI measurement)
▪ Proven risk reduction therapy should be prescribed for patients with PAD

Thank Thank YouYou