performance improvement a multidisciplinary team … · a multidisciplinary team approach to...
TRANSCRIPT

The Joint Commission Journal on Quality and Patient Safety
A Multidisciplinary Team Approach to Retained Foreign Objects
Performance Improvement
Retained foreign objects (RFOs) after a surgical procedureare one of the more dramatic medical errors that occur in
hospitalized patients1 These events can be associated with sig-nificant patient morbidity or mortality Furthermore they canhave a significant negative impact on provider as well as insti-tutional reputation and can result in litigation2 The frequencyof surgical RFOs is estimated to occur in 1of 1000 abdominaloperations or up to 1 of every 18000 operations performed34
These reports have evaluated the characteristics of procedurespatients or operative circumstances that predispose to RFOsGawande and colleagues performed the first case-control analy-sis and identified emergency procedures unplanned changes ina procedure and higher body-mass index (BMI) as significantrisk factors for surgical RFOs4 However not all reports of sur-gical RFOs have demonstrated an association with these riskfactors5
Although many authors have described the frequency typesand outcomes associated with surgical RFOs few havedescribed concerted institution-based efforts to reduce the fre-quency of these adverse events Gibbs stated that rather thanrelying on a single system prevention of RFOs warrants devel-opment of a multifaceted defense6 This article describes a mul-tidisciplinary effort implemented in all the operating rooms(ORs) and surgical procedural areas at the Mayo ClinicRochester (MCR) to address the issue of surgical RFOs
The RFO reduction effort was led by a leadership team composed of surgeons nurses quality management personnelsentinel event team members and administrative services person-nel The teamrsquos goal was to reduce the incidence of RFOs towardzero This single team addressed all elements of this initiative ina systematic fashion during the four-year period included in thisreport This effort is ongoing and has been divided into threephases defect analysis and policy review awareness and commu-nication and control and monitoring The RFO reduction efforthas resulted in a significant and sustained reduction in the fre-quency and types of surgical RFOs and has provided a model forall OR quality improvement (QI) efforts at MCR
Article-at-a-Glance
Background Retained foreign objects (RFOs) after surgicalprocedures are an infrequent but potentially devastatingmedical error The Mayo Clinic Rochester (MCR) under-took a quality improvement program to reduce the inci-dence of surgical RFOs Method A multidisciplinary multiphase approach was ini-tiated in 2005 The effort led by surgical nursing andadministrative institutional leaders was divided into threephases The first phase included a defect analysis and policyreview A detailed analysis of all RFOs (both true and nearmisses) was undertaken to identify patterns of failuresunique to our institution and operating room cultureSimultaneously a review of all relevant institutional policieswas performed with comprehensive revisions focusing onincreased clarity and inter- and intrapolicy consistency Thesecond phase involved increasing awareness and communi-cation among all operating room personnel including sur-geons residents nursing and allied health staff Theeducation program included all-staff conferences teamtraining simulation videos and daily education remindersand in-room audits Finally a monitoring and control phaseinvolved rapid leadership response teams to any eventsenhanced staff communication and policy reviewsResults When the program started MCR was averaging asurgical RFO every 16 days After the intervention the aver-age interval between RFO events increased to 69 days alevel of performance that has been sustained for more thantwo yearsDiscussion MCR experienced a significant and sustainedreduction in the incidents of RFOs attributed to the multi-disciplinary nature of the initiative the active engagementof institutional leadership and use of the principles ofenhanced communication between operating room staffmembers to improve operating room situational awareness
Robert R Cima MD MA Anantha Kollengode PhD MBA Amy S Storsveen RN BSN Cheryl AWeisbrod RN MS Claude Deschamps MD Mark B Koch MBA Debra Moore Sarah R Pool RN MS
123March 2009 Volume 35 Number 3
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
124 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
Quality Improvement Process SETTING
Approximately 50000 operations are per-formed annually in the 98 main ORs 3obstetrical ORs and 8 labor and deliverybirthing rooms on the MCR campus dis-tributed between two acute care hospitalsThe staff in the OR include more than 300surgeons and 450 anesthesia providersnearly 500 residents and 1500 nursing andallied health staff
The RFO reduction initiative was divid-ed into three distinct phases The time linesfor these phases are shown in Figure 1(right)
Phase I Defect Analysis and Policy Review The initial effort of our team was to per-
form a detailed analysis of all surgical RFOevents and any near-miss events reported to the institutionalsentinel event team at MCR during the calendar years2003ndash2006 The results of this analysis have been previouslyreported5 During the four-year analysis period 191168 oper-ations were performed There were 34 near-miss events and 34true RFOs Near misses were classified as events where therewas thought to be a retained object but none could be demon-strated by high-resolution intra- and postoperative imaging atrue RFO was defined as the unintentional retention of a for-eign object discovered after completion of the operation The34 items retained included 23 sponges 1 instrument 3 needlesand 7 miscellaneous items None of these RFOs occurred incases that were considered to be high-risk cases as previouslydefined by Gawande et al4 Another important finding was thatin 62 of the true RFO events the ldquocountsrdquo at the end of theoperations were considered correct Root cause analysis (RCA)performed on each RFO event demonstrated that a failure ofcommunication among OR team members was the most fre-quent contributor to the event Communication failures is oneof the most cited reasons for events leading to inadvertentpatient harm7ndash9 and many of the Joint Commission patientsafety standards are aimed at improving communication7
After the detailed defect analysis was performed a completereview of all procedures and policies relevant to OR efforts tomitigate RFOs was undertaken by surgical and nursing leader-ship First there was an effort to develop a single operationaldefinition of what was considered an RFO An RFO at MCRwas defined as follows
Any item that is unintentionally left within a patient anddiscovered by the patient care team after the primary opera-tive skin incision has been completely closed and final ster-ile dressing applied In cases of procedures that do not havean incision an item would be defined as an RFO if foundafter the operative team has completed the procedure
Second our team reviewed all policies and procedures relat-ed to the operative counting process The review of policiesincluded how an instrument and sponge count was to be per-formed who performed the count what was required to becounted how the count was documented how to reconcilemiscounts when they occurred how to manage intraoperativeimaging for possible RFOs and who is accountable forresponding to adverse events During this review process teammembers discovered that many of the policies had been amend-ed or altered over time in response to specific events without acomplete revision of the entire policy or consideration of howit related to other policies This type of ldquoone-off rdquo amendmentin response to specific events resulted in long and confusingpolicies that often had intra- and interpolicy contradictionsThe resulting differences made implementation of uniformpractices across the OR environment difficult In response tothese findings all relevant policies were revised by a leadershipteam composed of nursing and physician members These poli-cies were aligned with external standards and internal best prac-tices on the basis of the findings within the defect analysis10
Furthermore great effort was made to ensure intrapolicy andinterpolicy consistency Drafts of revised policies were distrib-
Figure 1 The time line for the three phases of the project are shown
Time Lines for the Three-Phase Project
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
125March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
uted to all OR personnel for their review to ensure clarity of thelanguage and identification of any deficiencies Once staff feed-back had been obtained the revised policies were submitted tothe appropriate surgery oversight and institutional committeesfor approval Finally a new policy and an education tool weredeveloped to assist OR staff on how to respond to a miscountor concern about the instance of an RFO This policy wasdesigned collaboratively by members of the departments ofradiology nursing and surgery (Figure 2 page 126)
Phase II Awareness and CommunicationAfter the detailed defect analysis and the policy and proce-
dure review were completed a multiphase broad-based com-munication and education campaign was initiated (Figure 3page 127) In the initial phase a mandatory all-staff meetingwas convened for all OR personnel This meeting included allstaff surgeons anesthesiologists resident physicians nursingstaff and allied health personnel In total more than 2500staff either attended the meeting or viewed delayed videorecordings During this meeting institutional surgical andnursing leadership discussed the data and findings from the sys-tematic defect analysis as well as a review of all the new policiesto be implemented to address the surgical RFOsMisconceptions about risk factors for RFO events and staffconcerns about processes of investigations of RFOs wereaddressed in this open forum The primary goal of the all-staffmeeting was to ensure that all team members understood thereality and scope of the problem and to improve the lines ofcommunication between the OR staff and leadership as well asamong the OR team members An unintended consequence ofthis effort was to highlight the low level and poor quality ofcommunication within the OR environment
The next step which also focused on team communicationand education was led by the department of hospital surgicalservices The Conscientious Count Campaign was designed asa multifaceted program to educate nurses certified surgicaltechnicians and surgical assistants on the proper countingtechniques and revised count policies It included productionof a video documenting the correct counting process whichwas reviewed at surgical services staff meetings The correctcounting process is based on the recommendations of theAssociation of Operating Room Nurses guidelines for countingsponges instruments and miscellaneous surgical items10 Theserecommendations discuss when counts are needed and howthey are performed which requires current visual and audiblecounts by two surgical services team members Additional edu-cation included team training in the Mayo Simulation Center
and in-room audits with immediate feedback provided byfrontline nurse managers Daily ldquoremindersrdquo of appropriatecounting technique policies and procedures were included instaff morning reports The standardized counting process wasimplemented across all surgical specialties and surgical unitsincluding labor and delivery after a month-long intense train-ing and education effort led by our OR nursing educators
Another initiative directed at improving situational aware-ness by all members of the OR team was use of a countingwhite board with standardized documentation criteria (Figure4 page 128) Designed by nursing leadership and refined withinput from all of the OR staff the white boards were placed inevery OR In the recognition that each specialty may haveunique counting needs magnetic labels for specialty specificitems were manufactured and placed on the white boards tospecifically track these unique items
The last phase of the education effort was the introductionof two ldquoRed Rulesrdquo These rules presented to and refined bythe OR staff and then adopted by the OR leadership group asinviolable rules of conduct in the OR were as follows
1 The Universal Protocol for patient identification and pro-cedural pauses11 must be followed
2 All counts of instruments and sponges must be performedby two team members in the standardized manner During theclosing pause the surgeon and residents are to stop all activityother than performing the required appropriate local woundexploration thus avoiding any interruptions of the countprocess
Unlike other organizations that have a formalized explora-tion of the entire abdominal or chest cavity our data did notdemonstrate retention of items in areas distant from the local-ized operative field and thus we concentrated our practice on afocused exploration in the region of operation These rules wereprinted and prominently displayed in all ORs after they wereshared with all surgeons residents anesthesiologists nursingand allied health personnel (Figure 5 page 129) Any teammember can invoke a Red Rule to stop the procedure in theinterest of patient safety OR leadership staff respond in realtime to the OR if there is any reported violation of the RedRules to support the staff in the room and ensure patient safety
Phase III Monitoring and ControlAfter the initial staff education program the team made the
transition in its efforts from monitoring and process controlFirst a rapid response event leadership team was formed Thisteam included surgeon nursing and administrative leadershipmembers Additional ad hoc members included quality man-
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
Figure 2 An incorrect-count decision tree was developed to assist operating room (OR) personnel in a standard approach to a miscount or possible retained for-eign object (RFO) event RN registered nurse NM nurse manager Q-read Quick read (a digital imaging system) CDM clinical documentation manager(application in the electronic medical record used for all ORndashrelated documentation)
An Incorrect Decision Tree
126
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
agement services nursing education and institutional sentinelevent personnel This team was informed of any near-miss orreal RFO event in the OR Within 12ndash24 hours of the event ameeting was convened that included the event response teamand all OR personnel involved in the incident including thesurgeons residents nurses and allied health staff The purposeof the meeting was to debrief all team members as to their rec-ollection of the events and circumstances contributing to theevent This process was not designed as a replacement for theformal sentinel event RCA or to assign responsibility for theevent Rather it was intended to quickly inform OR leadershipof the circumstances to determine areas of potential systemweakness Once the leadership team performed the analysis ofthe event a memo describing the circumstances of the eventand findings was prepared and shared with all OR personnelwithin 24ndash48 hours of the event (Table 1 page 130)Furthermore once the formal RCA was completed the find-ings were shared with the leadership team and then OR person-nel during the morning report
Another tactic to keep the OR staff aware of the RFO initia-tive was use of posters tracking the number of days since the lastRFO These posters were placed at the entrances to the ORs Inaddition RFO procedures and policies were randomlyreviewed by nursing leadership at staff morning reports Finallyquarterly all-staff meetings were held that focused on OR safe-ty team communication and RFO performance updates
ResultsThe impact of this multidisciplinaryeffort to reduce surgical RFO resultedin a significant decline in the frequencyof RFO events (Figure 6 page 131)Before initiating this effort we averagedan RFO or near miss once every 16days With the interventions the inter-val extended to an average of one RFOevery 69 days This level of perform-ance has been sustained for more thantwo years
Surgery involves multiple itemsincluding sponges needles and equip-ment These are counted as part of thebaseline count and in subsequentcounts that occur throughout the caseThe number of items routinely countedin a case often exceeds 100 uniqueitems Greenberg et al reported that
counting of multiple items is performed on average 16 timesper case each of these counts represents an opportunity forerror12 Assuming the potential for RFO opportunities is 25 peroperative case a defect per million opportunities (DPMO)analysis shows a decline from 052 to 011 per 1000 surgeriesIn other terms this represents an increase in the Sigma per-formance level of 56 to 60 (Figure 7 page 131) a process isconsidered to be at Six Sigma level when there are 34 DPMO
DiscussionMCR identified our rate of RFOs especially surgical spongesas a major quality and patient safety issue in 2005 A multidis-ciplinary multiphase approach was instituted with a goal of zeroRFOs This three-phased approach which consisted of detailedanalysis of our institutional experience including review andrevision of relevant policies broad and focused educational pro-grams and continuous participation and monitoring by surgi-cal and nursing leadership led to a significant reduction inRFOs within 2 years These efforts contributed to a reductionin the frequency of surgical RFOs from an average of one every16 days to one in 69 days
Surgical RFOs are often dramatic examples of medicalerrors They can lead to significant patient harm and (1) nega-tive impact to the reputations of both providers and health careorganizations and (2) negative financial impact due to financialwrite-offs and legal claims2 Frequently RFOs have been viewed
127March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
Figure 3 A multiphase broad-based awareness education campaign was initiated RFO retained foreignobject OR operating room
Phase II Awareness and Communication Plan 2007
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
128 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
as isolated unfortunate events that often lead to mitigationapproaches designed for the circumstances of each event Thisis a common problem with a sentinel event RCA approach toindividual events13 Some system and patient factors have beenassociated with a higher risk of RFOs (emergency cases changein the planned procedure and higher BMI patients)4 Howeverthe analysis of MCR RFOs did not reveal an association withthese factors5
Given the inability to identify any patient or proceduralcharacteristics that predisposed for RFOs at our institution amore broad-based approach to finding a solution was requiredAlthough much of the available literature regarding surgicalRFOs focuses on the types of objects retained and the circum-stances surrounding the events these sources lack recommen-dations about how institutions should analyze and improvetheir systems to minimize these events
The multidisciplinary team under the auspices of the surgi-cal quality assessment and safety committee led the initiative
toward zero RFOs As described this program was divided intothree phases (1) failure analysis and policy review (2) staffawareness and education (3) monitoring and control
The first phase required a detailed systematic evaluation ofour RFO experience This was coupled with a detailed reviewand revisions of existing policies and procedures in order toestablish clear definitions internally consistent policies andperformance expectations For example gaps were discoveredin our system processes in the event of a miscount and theresponse time for intraoperative films were inconsistent Thepolicy was simplified (Figure 2) and updated to reflect ldquoSTATrdquoorders for suspected RFOs and to require review of the film byradiologist and consultant or designee within 30 minutes Allintraoperative films requested to evaluate possible RFOs areordered as ldquorule out RFOrdquo The item missing is not specificallynoted on the x-ray request because this may predispose the radi-ologist to focus his or her initial read toward that object and toignore other findings Once read the radiologist calls into the
Figure 4 A sample OR white board is shown with labels designating the required place for the documentation of all counted items and pertinent patient infor-mation in the OR (patient information removed) In the lower right corner is a place for any items intentionally tucked into the wound and not under thedirect control of a member of the surgical team
Sample Operating Room (OR) White Board
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
129March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
OR and reviews all item seen on the film with the surgeon atwhich time the radiologist is specifically informed of what itemthe team believes is missing Response time for intraoperativeRFO films and adherence to policy were reviewed monthly bythe surgical quality assessment and safety committee to ensurecompliance
The second phase of the program was an intense education-al effort directed at all OR personnel regarding the scope anddetails of the RFO problem at MCR Again this wasapproached in phases The first was the all-staff meeting whichserved many purposes important to the success of this initiative
1 It ensured that all staff (physicians nurses and alliedhealth staff ) in the OR heard a single consistent messageregarding RFOs
2 It demonstrated a unified and engaged leadership team3 It articulated a clear and organized set of policies and pro-
cedures related to RFO reduction and prevention4 It set expected performance standards for all personnel in
the ORAll these elements are known to be essential for the successfulimplementation change within an organization13
Initiated at the same time as the all-staff meeting was anextensive education effort (Conscientious Count Campaign)
This education effort included daily morning report reviews ofthe appropriate and standardized counting protocols reviews ofrelated policies and in-room audits This program served toreinforce the training and performance of all OR personnel onthe standardized approach to counting and responding topotential RFO events Again this protracted education effortwhich stressed improving direct communication between allteam members to improve OR ldquosituational awarenessrdquo hasbeen shown to be one of the most important components forsuccessful institutional change14
The white board served as a tool to standardize documenta-tion of items used and any items that are tucked thus improv-ing the situational awareness of items placed in the surgicalfield Furthermore its use improved communication betweenOR staff members and was a more reliable mechanism thanhaving to rely on the surgical staff rsquos short-term memory It alsohelped in auditing the compliance to the new guidelines of doc-umenting counted and tucked items by nursing leadership per-forming daily observational audits The new counting anddocumentation policies and guidelines were implemented in allORs at the same time However development of specialty-spe-cific white boards were rolled out one specialty at a time after adetailed analysis of their unique instrumentation needsRandom audits are performed daily for 5 of the cases for eachspecialty by the specialty nurse manager The baseline counttucked item documentation and final counts are audited andcompliance has been 994 or higher for the latest quarter(third quarter 2008) In the event of a miscount compliancewith the established policies and procedures is determined anddocumented by specialty or overall surgical nursing leadershipImportantly all the information and findings are fed back tothe OR team members
The last phase of our effort demonstrated a new resolve byleadership to respond to RFO events Previously these eventswere addressed by the institutional sentinel event (SE) teamoften in isolation and without participation of key surgicalleaders (though these leaders were often invited to participate)The SE effort was often too focused on developing an RCA forthe individual event and did not address the broader culturaland communication issues that exist in the OR environmentNor did this process allow for active monitoring of the ORenvironment to identify the more latent safety issues Finallythe process was slow and the proposed solution to the eventwas often implemented some time after the event All theseissues reflect criticisms of the RCA process1516
To address these concerns a rapid leadership response teamwas formed to address the event within 24ndash36 hours with all
Figure 5 The Red Rules poster displayed in every operating room (OR) pro-vides the two inviolable rules of conduct in the OR The poster informs all staffmembers that adhering to appropriate counting policy is at a level of impor-tance equal to following the Universal Protocol to ensure patient safety
Red Rules Poster
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
130 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
personnel involved The clearly stated purpose of the meetingwas to understand the circumstances of the event and to not bepunitive or assign blame Important to the success of thesemeetings was the involvement of surgical and nursing leader-ship and the development of an open and secure environmentto share the events understand the failures and create plans toshare the lessons learned with all the OR personnel A summa-ry of the event and lessons learned were quickly disseminated ina written memo from the leadership group to all personnel andshared in all areas often within a few days of the event A non-punitive approach to addressing this type of medical error has
been shown to improve staff satisfaction performance andcommunication and to be integral to processes that supportinstitutional crisis management1718
A number of barriers to the success of this initiative wereidentified including poor interaction between the leadership ofthe different stakeholders no standardized institutional ordepartment response to RFO events and poor accountabilityfor addressing the problem of RFOs However the major bar-rier to success was a long-standing culture of poor communica-tion between our OR staff members The tradition of surgeonprimacy in the OR led to a culture lacking in basic communi-
Table 1 Examples of Key Information from Memos to Staff After a Retained Foreign Object (RFO) Event or Near Miss
Brief Description of Event
Near Miss Needle count off
intraoperative film ordered
patient closed because
patient condition before film
was reviewed
Near Miss Needle count off
after exhaustive search in
OR three different intra-op
films taken and needle not
found second exhaustive
search in OR yielded no
needle Patient closed and
survey film revealed needle
A counted-out (after final
pause) sponge was tucked to
protect the abdominal viscera
during closure resulting in a
retained sponge
Argon beam coagulatorrsquos grey
tape (nonndashradio opaque) was
replaced with black tip (radio
opaque) without any notifica-
tion from manufacturer The
tip was not removed and was
retained
Root Causes Identified
Patient condition
Communication gap among
OR staff and radiology
Technology limitation of
intraoperative film vs
survey film
Surgeonrsquos preference for a
particular trochar may or
may not have played a role
Use of sponge in a
nonrecommended fashion
as a viscera retainer
Not following existing cur-
rent policy for final count
and verbalizing tucked items
Communication lapse
between manufacturer and
users
Strengths Identified
Adherence to the
current process
Adherence to the
current process
Appropriate
interventions taken
Survey film of all
patients even when
counts are correct
Survey film of all
patients even when
counts are correct
Opportunities for
Improvement
Radiology process for
RFO rule-out
Communication between
OR staff and radiology
Review of policy for
missing microneedles
(definition process steps
for missing microneedle)
Standardization of
equipment
Training of new fellows and
residents on current best
practices
Communication among
OR staff
While the functionality of
the tape replacement was
improved to make it radio
opaque the change was
not communicated to the
users by the manufacturer
Next Steps Delineated
State in request ldquorule out an
RFOrdquo to expedite review in
less than 30 minutes
Do not move the patient from
OR if patient condition war-
rants to facilitate additional
films to rule out an RFO
Develop policy for
microneedles
Review laparoscopic
equipment available to the
surgical team and their
application to the procedure
being performed
Use rubber viscera retainers
or ldquofishrdquo for viscera retainer
Bag off all counted out
sponges in all specialties
Provide training for all new
residents and fellows
Notify all users throughout
the institution
Remove all mislabeled
equipment from supply
Contact manufacturer and
get issue resolved
Notify FDA
OR operating room FDA Food and Drug Administration
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
131March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
cation skills poor situational awarenessand concern about questioning thecourse of events in the OR This initia-tive helped our organization clarifyissues with our existing processes toavoid RFOs as well as design and imple-ment solutions However the mostimportant benefit was that it highlight-ed the underlying behavior and commu-nication failures between our staffmembers This finding drove the latterhalf of the initiative to focus on teachingand improving team communication
Summary and Conclusions In summary MCR identified the inci-dence of RFOs as a serious quality per-formance issue in the OR To addressthis problem a multidisciplinary leader-ship group was formed that took a sys-tematic evidence-based approach toanalyzing the factors contributing toRFO events Guided by institutionaldata OR leadership engaged the entireOR staff in a broad-based communica-tioneducation program and incorporat-ed system redesign to minimize futureRFOs
The OR environment is complexand manual counting of surgical items isan inherently error-prone process MCRcontinues to perform postoperative sur-vey films for all surgeries in which abody cavity is opened which we believeis the best defense currently available todetect unrecognized RFOs despite all ofour best efforts to improve the intraop-erative processes of counting and docu-mentation We believe that we havereached a performance boundary withour current process and await eitherimplementation of a new technology ora fundamental change in how our entiresurgical process is performed J
Figure 6 The frequency of potential RFO events declined significantly after the initiation of the reduc-tion effort We used a G-Chart which has significantly greater detection power over conventional bino-mial-based approaches particularly for infrequent events and low ldquodefectrdquo rates such as RFOs MCR wasaveraging a surgical RFO every 16 days which was extended to every 69 days as of October 2008
Days Between Potential Retained Foreign Object (RFO)Events January 2003ndashOctober 2008
Figure 7 The defects-per-million-opportunity analysis is shown assuming 25 chances (defect opportuni-ties) per surgical case for an error resulting in a retained foreign object
Defects per Million Opportunities (DPMO) and Sigma LevelMayo Clinic Rochester Minnesota 2003ndash2007
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
132 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
References1 Associated Press Towel Found in Dead Womanrsquos Body CBSNewscomAugust 6 2004 httpwwwcbsnewscomstories20040806healthprintable634558shtml (last accessed Jan 16 2009)2 Sowka MP The medical malpractice closed claims study Conducted bythe National Association of Insurance Commissioners Conn Med45109ndash115 Feb 19813 Gonzales-Ojeda A et al Retained foreign bodies following intra-abdom-inal surgery Hepatogastroenterology 46808ndash812 Mar 19994 Gawande AA et al Risk factors for retained instruments N Engl J Med348229ndash235 Jan 16 20035 Cima RR et al Incidence and characteristics of potential and actualretained foreign object events in surgical patients J Am Coll Surg 20780ndash87Jul 2008 Epub 2008 May 23 20086 Gibbs VC Preventable errors in the operating room Retained foreign bod-
ies after surgeryndashPart I Curr Probl Surg 44281ndash337 May 20077 Leonard M et al The human factor The critical importance of effectiveteamwork and communication Qual Saf Health Care 13(suppl 1)85ndash90Oct 20048 Lingard L et al Communication failures in the operating room Anobservational classification of recurrent types an events Qual Saf Health Care13330ndash334 Oct 20049 Donchin Y et al A look into the nature and causes of human errors in theintensive care unit Qual Saf Health Care 12143ndash147 Apr 200310 AORN Recommended Practices Committee Recommended practices forsponge sharps and instrument counts AORN J 83418 421ndash426 429ndash433Feb 200611 The Joint Commission Universal Protocol httpwwwjointcommissionorgPatientSafetyUniversalProtocol (last accessed Jan 16 2009) 12 Greenberg C et al The frequency and significance of discrepancies in thesurgical count Annal Surg 248337ndash341 Aug 200813 Lukas CV et al Transformational change in health care systems Anorganizational model Health Care Manage Rev 32309ndash320 OctndashDec 200714 Wang MC et al Redesigning health systems for quality Lessons fromemerging practices Jt Comm J Qual Patient Saf 32599ndash611 Nov 200615 Wu AW Lipshutz AK Pronovost PJ Effectiveness and efficiency ofroot cause analysis in medicine JAMA 299685ndash687 Feb 13 2008 16 Reason J Managing the Risks of Organizational Accidents Farnham UKAshgate 199717 Helmrich RL On error management Lessons from aviation BMJ320781ndash785 Mar 18 200018 Marx D Patient Safety and the ldquoJust Culturerdquo A Primer for Health CareExecutives Medical Event Reporting System for Transfusion Medicine Agency forHealthcare Research and Quality 2001 httppsnetahrqgovresourceaspxresourceID=1582 (last accessed Jan 16 2009)
Robert R Cima MD MA is Associate Professor Department of
Surgery Mayo Clinic Rochester Minnesota Anantha
Kollengode PhD MBA is Quality Analyst Quality
Management Services Amy S Storsveen RN BSN is Charge
Nurse and Cheryl A Weisbrod RN MS is Director Surgical
Services Claude Deschamps MD is Professor and Chairman
Department of Surgery Mark B Koch MBA is Associate
Administrator Administrative Services Debra Moore is Nursing
Analyst and Sarah R Pool RN MS is Nursing Educator
Surgical Services Please address correspondence to Robert R
Cima cimarobertmayoedu
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations

124 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
Quality Improvement Process SETTING
Approximately 50000 operations are per-formed annually in the 98 main ORs 3obstetrical ORs and 8 labor and deliverybirthing rooms on the MCR campus dis-tributed between two acute care hospitalsThe staff in the OR include more than 300surgeons and 450 anesthesia providersnearly 500 residents and 1500 nursing andallied health staff
The RFO reduction initiative was divid-ed into three distinct phases The time linesfor these phases are shown in Figure 1(right)
Phase I Defect Analysis and Policy Review The initial effort of our team was to per-
form a detailed analysis of all surgical RFOevents and any near-miss events reported to the institutionalsentinel event team at MCR during the calendar years2003ndash2006 The results of this analysis have been previouslyreported5 During the four-year analysis period 191168 oper-ations were performed There were 34 near-miss events and 34true RFOs Near misses were classified as events where therewas thought to be a retained object but none could be demon-strated by high-resolution intra- and postoperative imaging atrue RFO was defined as the unintentional retention of a for-eign object discovered after completion of the operation The34 items retained included 23 sponges 1 instrument 3 needlesand 7 miscellaneous items None of these RFOs occurred incases that were considered to be high-risk cases as previouslydefined by Gawande et al4 Another important finding was thatin 62 of the true RFO events the ldquocountsrdquo at the end of theoperations were considered correct Root cause analysis (RCA)performed on each RFO event demonstrated that a failure ofcommunication among OR team members was the most fre-quent contributor to the event Communication failures is oneof the most cited reasons for events leading to inadvertentpatient harm7ndash9 and many of the Joint Commission patientsafety standards are aimed at improving communication7
After the detailed defect analysis was performed a completereview of all procedures and policies relevant to OR efforts tomitigate RFOs was undertaken by surgical and nursing leader-ship First there was an effort to develop a single operationaldefinition of what was considered an RFO An RFO at MCRwas defined as follows
Any item that is unintentionally left within a patient anddiscovered by the patient care team after the primary opera-tive skin incision has been completely closed and final ster-ile dressing applied In cases of procedures that do not havean incision an item would be defined as an RFO if foundafter the operative team has completed the procedure
Second our team reviewed all policies and procedures relat-ed to the operative counting process The review of policiesincluded how an instrument and sponge count was to be per-formed who performed the count what was required to becounted how the count was documented how to reconcilemiscounts when they occurred how to manage intraoperativeimaging for possible RFOs and who is accountable forresponding to adverse events During this review process teammembers discovered that many of the policies had been amend-ed or altered over time in response to specific events without acomplete revision of the entire policy or consideration of howit related to other policies This type of ldquoone-off rdquo amendmentin response to specific events resulted in long and confusingpolicies that often had intra- and interpolicy contradictionsThe resulting differences made implementation of uniformpractices across the OR environment difficult In response tothese findings all relevant policies were revised by a leadershipteam composed of nursing and physician members These poli-cies were aligned with external standards and internal best prac-tices on the basis of the findings within the defect analysis10
Furthermore great effort was made to ensure intrapolicy andinterpolicy consistency Drafts of revised policies were distrib-
Figure 1 The time line for the three phases of the project are shown
Time Lines for the Three-Phase Project
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
125March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
uted to all OR personnel for their review to ensure clarity of thelanguage and identification of any deficiencies Once staff feed-back had been obtained the revised policies were submitted tothe appropriate surgery oversight and institutional committeesfor approval Finally a new policy and an education tool weredeveloped to assist OR staff on how to respond to a miscountor concern about the instance of an RFO This policy wasdesigned collaboratively by members of the departments ofradiology nursing and surgery (Figure 2 page 126)
Phase II Awareness and CommunicationAfter the detailed defect analysis and the policy and proce-
dure review were completed a multiphase broad-based com-munication and education campaign was initiated (Figure 3page 127) In the initial phase a mandatory all-staff meetingwas convened for all OR personnel This meeting included allstaff surgeons anesthesiologists resident physicians nursingstaff and allied health personnel In total more than 2500staff either attended the meeting or viewed delayed videorecordings During this meeting institutional surgical andnursing leadership discussed the data and findings from the sys-tematic defect analysis as well as a review of all the new policiesto be implemented to address the surgical RFOsMisconceptions about risk factors for RFO events and staffconcerns about processes of investigations of RFOs wereaddressed in this open forum The primary goal of the all-staffmeeting was to ensure that all team members understood thereality and scope of the problem and to improve the lines ofcommunication between the OR staff and leadership as well asamong the OR team members An unintended consequence ofthis effort was to highlight the low level and poor quality ofcommunication within the OR environment
The next step which also focused on team communicationand education was led by the department of hospital surgicalservices The Conscientious Count Campaign was designed asa multifaceted program to educate nurses certified surgicaltechnicians and surgical assistants on the proper countingtechniques and revised count policies It included productionof a video documenting the correct counting process whichwas reviewed at surgical services staff meetings The correctcounting process is based on the recommendations of theAssociation of Operating Room Nurses guidelines for countingsponges instruments and miscellaneous surgical items10 Theserecommendations discuss when counts are needed and howthey are performed which requires current visual and audiblecounts by two surgical services team members Additional edu-cation included team training in the Mayo Simulation Center
and in-room audits with immediate feedback provided byfrontline nurse managers Daily ldquoremindersrdquo of appropriatecounting technique policies and procedures were included instaff morning reports The standardized counting process wasimplemented across all surgical specialties and surgical unitsincluding labor and delivery after a month-long intense train-ing and education effort led by our OR nursing educators
Another initiative directed at improving situational aware-ness by all members of the OR team was use of a countingwhite board with standardized documentation criteria (Figure4 page 128) Designed by nursing leadership and refined withinput from all of the OR staff the white boards were placed inevery OR In the recognition that each specialty may haveunique counting needs magnetic labels for specialty specificitems were manufactured and placed on the white boards tospecifically track these unique items
The last phase of the education effort was the introductionof two ldquoRed Rulesrdquo These rules presented to and refined bythe OR staff and then adopted by the OR leadership group asinviolable rules of conduct in the OR were as follows
1 The Universal Protocol for patient identification and pro-cedural pauses11 must be followed
2 All counts of instruments and sponges must be performedby two team members in the standardized manner During theclosing pause the surgeon and residents are to stop all activityother than performing the required appropriate local woundexploration thus avoiding any interruptions of the countprocess
Unlike other organizations that have a formalized explora-tion of the entire abdominal or chest cavity our data did notdemonstrate retention of items in areas distant from the local-ized operative field and thus we concentrated our practice on afocused exploration in the region of operation These rules wereprinted and prominently displayed in all ORs after they wereshared with all surgeons residents anesthesiologists nursingand allied health personnel (Figure 5 page 129) Any teammember can invoke a Red Rule to stop the procedure in theinterest of patient safety OR leadership staff respond in realtime to the OR if there is any reported violation of the RedRules to support the staff in the room and ensure patient safety
Phase III Monitoring and ControlAfter the initial staff education program the team made the
transition in its efforts from monitoring and process controlFirst a rapid response event leadership team was formed Thisteam included surgeon nursing and administrative leadershipmembers Additional ad hoc members included quality man-
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
Figure 2 An incorrect-count decision tree was developed to assist operating room (OR) personnel in a standard approach to a miscount or possible retained for-eign object (RFO) event RN registered nurse NM nurse manager Q-read Quick read (a digital imaging system) CDM clinical documentation manager(application in the electronic medical record used for all ORndashrelated documentation)
An Incorrect Decision Tree
126
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
agement services nursing education and institutional sentinelevent personnel This team was informed of any near-miss orreal RFO event in the OR Within 12ndash24 hours of the event ameeting was convened that included the event response teamand all OR personnel involved in the incident including thesurgeons residents nurses and allied health staff The purposeof the meeting was to debrief all team members as to their rec-ollection of the events and circumstances contributing to theevent This process was not designed as a replacement for theformal sentinel event RCA or to assign responsibility for theevent Rather it was intended to quickly inform OR leadershipof the circumstances to determine areas of potential systemweakness Once the leadership team performed the analysis ofthe event a memo describing the circumstances of the eventand findings was prepared and shared with all OR personnelwithin 24ndash48 hours of the event (Table 1 page 130)Furthermore once the formal RCA was completed the find-ings were shared with the leadership team and then OR person-nel during the morning report
Another tactic to keep the OR staff aware of the RFO initia-tive was use of posters tracking the number of days since the lastRFO These posters were placed at the entrances to the ORs Inaddition RFO procedures and policies were randomlyreviewed by nursing leadership at staff morning reports Finallyquarterly all-staff meetings were held that focused on OR safe-ty team communication and RFO performance updates
ResultsThe impact of this multidisciplinaryeffort to reduce surgical RFO resultedin a significant decline in the frequencyof RFO events (Figure 6 page 131)Before initiating this effort we averagedan RFO or near miss once every 16days With the interventions the inter-val extended to an average of one RFOevery 69 days This level of perform-ance has been sustained for more thantwo years
Surgery involves multiple itemsincluding sponges needles and equip-ment These are counted as part of thebaseline count and in subsequentcounts that occur throughout the caseThe number of items routinely countedin a case often exceeds 100 uniqueitems Greenberg et al reported that
counting of multiple items is performed on average 16 timesper case each of these counts represents an opportunity forerror12 Assuming the potential for RFO opportunities is 25 peroperative case a defect per million opportunities (DPMO)analysis shows a decline from 052 to 011 per 1000 surgeriesIn other terms this represents an increase in the Sigma per-formance level of 56 to 60 (Figure 7 page 131) a process isconsidered to be at Six Sigma level when there are 34 DPMO
DiscussionMCR identified our rate of RFOs especially surgical spongesas a major quality and patient safety issue in 2005 A multidis-ciplinary multiphase approach was instituted with a goal of zeroRFOs This three-phased approach which consisted of detailedanalysis of our institutional experience including review andrevision of relevant policies broad and focused educational pro-grams and continuous participation and monitoring by surgi-cal and nursing leadership led to a significant reduction inRFOs within 2 years These efforts contributed to a reductionin the frequency of surgical RFOs from an average of one every16 days to one in 69 days
Surgical RFOs are often dramatic examples of medicalerrors They can lead to significant patient harm and (1) nega-tive impact to the reputations of both providers and health careorganizations and (2) negative financial impact due to financialwrite-offs and legal claims2 Frequently RFOs have been viewed
127March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
Figure 3 A multiphase broad-based awareness education campaign was initiated RFO retained foreignobject OR operating room
Phase II Awareness and Communication Plan 2007
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
128 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
as isolated unfortunate events that often lead to mitigationapproaches designed for the circumstances of each event Thisis a common problem with a sentinel event RCA approach toindividual events13 Some system and patient factors have beenassociated with a higher risk of RFOs (emergency cases changein the planned procedure and higher BMI patients)4 Howeverthe analysis of MCR RFOs did not reveal an association withthese factors5
Given the inability to identify any patient or proceduralcharacteristics that predisposed for RFOs at our institution amore broad-based approach to finding a solution was requiredAlthough much of the available literature regarding surgicalRFOs focuses on the types of objects retained and the circum-stances surrounding the events these sources lack recommen-dations about how institutions should analyze and improvetheir systems to minimize these events
The multidisciplinary team under the auspices of the surgi-cal quality assessment and safety committee led the initiative
toward zero RFOs As described this program was divided intothree phases (1) failure analysis and policy review (2) staffawareness and education (3) monitoring and control
The first phase required a detailed systematic evaluation ofour RFO experience This was coupled with a detailed reviewand revisions of existing policies and procedures in order toestablish clear definitions internally consistent policies andperformance expectations For example gaps were discoveredin our system processes in the event of a miscount and theresponse time for intraoperative films were inconsistent Thepolicy was simplified (Figure 2) and updated to reflect ldquoSTATrdquoorders for suspected RFOs and to require review of the film byradiologist and consultant or designee within 30 minutes Allintraoperative films requested to evaluate possible RFOs areordered as ldquorule out RFOrdquo The item missing is not specificallynoted on the x-ray request because this may predispose the radi-ologist to focus his or her initial read toward that object and toignore other findings Once read the radiologist calls into the
Figure 4 A sample OR white board is shown with labels designating the required place for the documentation of all counted items and pertinent patient infor-mation in the OR (patient information removed) In the lower right corner is a place for any items intentionally tucked into the wound and not under thedirect control of a member of the surgical team
Sample Operating Room (OR) White Board
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
129March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
OR and reviews all item seen on the film with the surgeon atwhich time the radiologist is specifically informed of what itemthe team believes is missing Response time for intraoperativeRFO films and adherence to policy were reviewed monthly bythe surgical quality assessment and safety committee to ensurecompliance
The second phase of the program was an intense education-al effort directed at all OR personnel regarding the scope anddetails of the RFO problem at MCR Again this wasapproached in phases The first was the all-staff meeting whichserved many purposes important to the success of this initiative
1 It ensured that all staff (physicians nurses and alliedhealth staff ) in the OR heard a single consistent messageregarding RFOs
2 It demonstrated a unified and engaged leadership team3 It articulated a clear and organized set of policies and pro-
cedures related to RFO reduction and prevention4 It set expected performance standards for all personnel in
the ORAll these elements are known to be essential for the successfulimplementation change within an organization13
Initiated at the same time as the all-staff meeting was anextensive education effort (Conscientious Count Campaign)
This education effort included daily morning report reviews ofthe appropriate and standardized counting protocols reviews ofrelated policies and in-room audits This program served toreinforce the training and performance of all OR personnel onthe standardized approach to counting and responding topotential RFO events Again this protracted education effortwhich stressed improving direct communication between allteam members to improve OR ldquosituational awarenessrdquo hasbeen shown to be one of the most important components forsuccessful institutional change14
The white board served as a tool to standardize documenta-tion of items used and any items that are tucked thus improv-ing the situational awareness of items placed in the surgicalfield Furthermore its use improved communication betweenOR staff members and was a more reliable mechanism thanhaving to rely on the surgical staff rsquos short-term memory It alsohelped in auditing the compliance to the new guidelines of doc-umenting counted and tucked items by nursing leadership per-forming daily observational audits The new counting anddocumentation policies and guidelines were implemented in allORs at the same time However development of specialty-spe-cific white boards were rolled out one specialty at a time after adetailed analysis of their unique instrumentation needsRandom audits are performed daily for 5 of the cases for eachspecialty by the specialty nurse manager The baseline counttucked item documentation and final counts are audited andcompliance has been 994 or higher for the latest quarter(third quarter 2008) In the event of a miscount compliancewith the established policies and procedures is determined anddocumented by specialty or overall surgical nursing leadershipImportantly all the information and findings are fed back tothe OR team members
The last phase of our effort demonstrated a new resolve byleadership to respond to RFO events Previously these eventswere addressed by the institutional sentinel event (SE) teamoften in isolation and without participation of key surgicalleaders (though these leaders were often invited to participate)The SE effort was often too focused on developing an RCA forthe individual event and did not address the broader culturaland communication issues that exist in the OR environmentNor did this process allow for active monitoring of the ORenvironment to identify the more latent safety issues Finallythe process was slow and the proposed solution to the eventwas often implemented some time after the event All theseissues reflect criticisms of the RCA process1516
To address these concerns a rapid leadership response teamwas formed to address the event within 24ndash36 hours with all
Figure 5 The Red Rules poster displayed in every operating room (OR) pro-vides the two inviolable rules of conduct in the OR The poster informs all staffmembers that adhering to appropriate counting policy is at a level of impor-tance equal to following the Universal Protocol to ensure patient safety
Red Rules Poster
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
130 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
personnel involved The clearly stated purpose of the meetingwas to understand the circumstances of the event and to not bepunitive or assign blame Important to the success of thesemeetings was the involvement of surgical and nursing leader-ship and the development of an open and secure environmentto share the events understand the failures and create plans toshare the lessons learned with all the OR personnel A summa-ry of the event and lessons learned were quickly disseminated ina written memo from the leadership group to all personnel andshared in all areas often within a few days of the event A non-punitive approach to addressing this type of medical error has
been shown to improve staff satisfaction performance andcommunication and to be integral to processes that supportinstitutional crisis management1718
A number of barriers to the success of this initiative wereidentified including poor interaction between the leadership ofthe different stakeholders no standardized institutional ordepartment response to RFO events and poor accountabilityfor addressing the problem of RFOs However the major bar-rier to success was a long-standing culture of poor communica-tion between our OR staff members The tradition of surgeonprimacy in the OR led to a culture lacking in basic communi-
Table 1 Examples of Key Information from Memos to Staff After a Retained Foreign Object (RFO) Event or Near Miss
Brief Description of Event
Near Miss Needle count off
intraoperative film ordered
patient closed because
patient condition before film
was reviewed
Near Miss Needle count off
after exhaustive search in
OR three different intra-op
films taken and needle not
found second exhaustive
search in OR yielded no
needle Patient closed and
survey film revealed needle
A counted-out (after final
pause) sponge was tucked to
protect the abdominal viscera
during closure resulting in a
retained sponge
Argon beam coagulatorrsquos grey
tape (nonndashradio opaque) was
replaced with black tip (radio
opaque) without any notifica-
tion from manufacturer The
tip was not removed and was
retained
Root Causes Identified
Patient condition
Communication gap among
OR staff and radiology
Technology limitation of
intraoperative film vs
survey film
Surgeonrsquos preference for a
particular trochar may or
may not have played a role
Use of sponge in a
nonrecommended fashion
as a viscera retainer
Not following existing cur-
rent policy for final count
and verbalizing tucked items
Communication lapse
between manufacturer and
users
Strengths Identified
Adherence to the
current process
Adherence to the
current process
Appropriate
interventions taken
Survey film of all
patients even when
counts are correct
Survey film of all
patients even when
counts are correct
Opportunities for
Improvement
Radiology process for
RFO rule-out
Communication between
OR staff and radiology
Review of policy for
missing microneedles
(definition process steps
for missing microneedle)
Standardization of
equipment
Training of new fellows and
residents on current best
practices
Communication among
OR staff
While the functionality of
the tape replacement was
improved to make it radio
opaque the change was
not communicated to the
users by the manufacturer
Next Steps Delineated
State in request ldquorule out an
RFOrdquo to expedite review in
less than 30 minutes
Do not move the patient from
OR if patient condition war-
rants to facilitate additional
films to rule out an RFO
Develop policy for
microneedles
Review laparoscopic
equipment available to the
surgical team and their
application to the procedure
being performed
Use rubber viscera retainers
or ldquofishrdquo for viscera retainer
Bag off all counted out
sponges in all specialties
Provide training for all new
residents and fellows
Notify all users throughout
the institution
Remove all mislabeled
equipment from supply
Contact manufacturer and
get issue resolved
Notify FDA
OR operating room FDA Food and Drug Administration
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
131March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
cation skills poor situational awarenessand concern about questioning thecourse of events in the OR This initia-tive helped our organization clarifyissues with our existing processes toavoid RFOs as well as design and imple-ment solutions However the mostimportant benefit was that it highlight-ed the underlying behavior and commu-nication failures between our staffmembers This finding drove the latterhalf of the initiative to focus on teachingand improving team communication
Summary and Conclusions In summary MCR identified the inci-dence of RFOs as a serious quality per-formance issue in the OR To addressthis problem a multidisciplinary leader-ship group was formed that took a sys-tematic evidence-based approach toanalyzing the factors contributing toRFO events Guided by institutionaldata OR leadership engaged the entireOR staff in a broad-based communica-tioneducation program and incorporat-ed system redesign to minimize futureRFOs
The OR environment is complexand manual counting of surgical items isan inherently error-prone process MCRcontinues to perform postoperative sur-vey films for all surgeries in which abody cavity is opened which we believeis the best defense currently available todetect unrecognized RFOs despite all ofour best efforts to improve the intraop-erative processes of counting and docu-mentation We believe that we havereached a performance boundary withour current process and await eitherimplementation of a new technology ora fundamental change in how our entiresurgical process is performed J
Figure 6 The frequency of potential RFO events declined significantly after the initiation of the reduc-tion effort We used a G-Chart which has significantly greater detection power over conventional bino-mial-based approaches particularly for infrequent events and low ldquodefectrdquo rates such as RFOs MCR wasaveraging a surgical RFO every 16 days which was extended to every 69 days as of October 2008
Days Between Potential Retained Foreign Object (RFO)Events January 2003ndashOctober 2008
Figure 7 The defects-per-million-opportunity analysis is shown assuming 25 chances (defect opportuni-ties) per surgical case for an error resulting in a retained foreign object
Defects per Million Opportunities (DPMO) and Sigma LevelMayo Clinic Rochester Minnesota 2003ndash2007
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
132 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
References1 Associated Press Towel Found in Dead Womanrsquos Body CBSNewscomAugust 6 2004 httpwwwcbsnewscomstories20040806healthprintable634558shtml (last accessed Jan 16 2009)2 Sowka MP The medical malpractice closed claims study Conducted bythe National Association of Insurance Commissioners Conn Med45109ndash115 Feb 19813 Gonzales-Ojeda A et al Retained foreign bodies following intra-abdom-inal surgery Hepatogastroenterology 46808ndash812 Mar 19994 Gawande AA et al Risk factors for retained instruments N Engl J Med348229ndash235 Jan 16 20035 Cima RR et al Incidence and characteristics of potential and actualretained foreign object events in surgical patients J Am Coll Surg 20780ndash87Jul 2008 Epub 2008 May 23 20086 Gibbs VC Preventable errors in the operating room Retained foreign bod-
ies after surgeryndashPart I Curr Probl Surg 44281ndash337 May 20077 Leonard M et al The human factor The critical importance of effectiveteamwork and communication Qual Saf Health Care 13(suppl 1)85ndash90Oct 20048 Lingard L et al Communication failures in the operating room Anobservational classification of recurrent types an events Qual Saf Health Care13330ndash334 Oct 20049 Donchin Y et al A look into the nature and causes of human errors in theintensive care unit Qual Saf Health Care 12143ndash147 Apr 200310 AORN Recommended Practices Committee Recommended practices forsponge sharps and instrument counts AORN J 83418 421ndash426 429ndash433Feb 200611 The Joint Commission Universal Protocol httpwwwjointcommissionorgPatientSafetyUniversalProtocol (last accessed Jan 16 2009) 12 Greenberg C et al The frequency and significance of discrepancies in thesurgical count Annal Surg 248337ndash341 Aug 200813 Lukas CV et al Transformational change in health care systems Anorganizational model Health Care Manage Rev 32309ndash320 OctndashDec 200714 Wang MC et al Redesigning health systems for quality Lessons fromemerging practices Jt Comm J Qual Patient Saf 32599ndash611 Nov 200615 Wu AW Lipshutz AK Pronovost PJ Effectiveness and efficiency ofroot cause analysis in medicine JAMA 299685ndash687 Feb 13 2008 16 Reason J Managing the Risks of Organizational Accidents Farnham UKAshgate 199717 Helmrich RL On error management Lessons from aviation BMJ320781ndash785 Mar 18 200018 Marx D Patient Safety and the ldquoJust Culturerdquo A Primer for Health CareExecutives Medical Event Reporting System for Transfusion Medicine Agency forHealthcare Research and Quality 2001 httppsnetahrqgovresourceaspxresourceID=1582 (last accessed Jan 16 2009)
Robert R Cima MD MA is Associate Professor Department of
Surgery Mayo Clinic Rochester Minnesota Anantha
Kollengode PhD MBA is Quality Analyst Quality
Management Services Amy S Storsveen RN BSN is Charge
Nurse and Cheryl A Weisbrod RN MS is Director Surgical
Services Claude Deschamps MD is Professor and Chairman
Department of Surgery Mark B Koch MBA is Associate
Administrator Administrative Services Debra Moore is Nursing
Analyst and Sarah R Pool RN MS is Nursing Educator
Surgical Services Please address correspondence to Robert R
Cima cimarobertmayoedu
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations

125March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
uted to all OR personnel for their review to ensure clarity of thelanguage and identification of any deficiencies Once staff feed-back had been obtained the revised policies were submitted tothe appropriate surgery oversight and institutional committeesfor approval Finally a new policy and an education tool weredeveloped to assist OR staff on how to respond to a miscountor concern about the instance of an RFO This policy wasdesigned collaboratively by members of the departments ofradiology nursing and surgery (Figure 2 page 126)
Phase II Awareness and CommunicationAfter the detailed defect analysis and the policy and proce-
dure review were completed a multiphase broad-based com-munication and education campaign was initiated (Figure 3page 127) In the initial phase a mandatory all-staff meetingwas convened for all OR personnel This meeting included allstaff surgeons anesthesiologists resident physicians nursingstaff and allied health personnel In total more than 2500staff either attended the meeting or viewed delayed videorecordings During this meeting institutional surgical andnursing leadership discussed the data and findings from the sys-tematic defect analysis as well as a review of all the new policiesto be implemented to address the surgical RFOsMisconceptions about risk factors for RFO events and staffconcerns about processes of investigations of RFOs wereaddressed in this open forum The primary goal of the all-staffmeeting was to ensure that all team members understood thereality and scope of the problem and to improve the lines ofcommunication between the OR staff and leadership as well asamong the OR team members An unintended consequence ofthis effort was to highlight the low level and poor quality ofcommunication within the OR environment
The next step which also focused on team communicationand education was led by the department of hospital surgicalservices The Conscientious Count Campaign was designed asa multifaceted program to educate nurses certified surgicaltechnicians and surgical assistants on the proper countingtechniques and revised count policies It included productionof a video documenting the correct counting process whichwas reviewed at surgical services staff meetings The correctcounting process is based on the recommendations of theAssociation of Operating Room Nurses guidelines for countingsponges instruments and miscellaneous surgical items10 Theserecommendations discuss when counts are needed and howthey are performed which requires current visual and audiblecounts by two surgical services team members Additional edu-cation included team training in the Mayo Simulation Center
and in-room audits with immediate feedback provided byfrontline nurse managers Daily ldquoremindersrdquo of appropriatecounting technique policies and procedures were included instaff morning reports The standardized counting process wasimplemented across all surgical specialties and surgical unitsincluding labor and delivery after a month-long intense train-ing and education effort led by our OR nursing educators
Another initiative directed at improving situational aware-ness by all members of the OR team was use of a countingwhite board with standardized documentation criteria (Figure4 page 128) Designed by nursing leadership and refined withinput from all of the OR staff the white boards were placed inevery OR In the recognition that each specialty may haveunique counting needs magnetic labels for specialty specificitems were manufactured and placed on the white boards tospecifically track these unique items
The last phase of the education effort was the introductionof two ldquoRed Rulesrdquo These rules presented to and refined bythe OR staff and then adopted by the OR leadership group asinviolable rules of conduct in the OR were as follows
1 The Universal Protocol for patient identification and pro-cedural pauses11 must be followed
2 All counts of instruments and sponges must be performedby two team members in the standardized manner During theclosing pause the surgeon and residents are to stop all activityother than performing the required appropriate local woundexploration thus avoiding any interruptions of the countprocess
Unlike other organizations that have a formalized explora-tion of the entire abdominal or chest cavity our data did notdemonstrate retention of items in areas distant from the local-ized operative field and thus we concentrated our practice on afocused exploration in the region of operation These rules wereprinted and prominently displayed in all ORs after they wereshared with all surgeons residents anesthesiologists nursingand allied health personnel (Figure 5 page 129) Any teammember can invoke a Red Rule to stop the procedure in theinterest of patient safety OR leadership staff respond in realtime to the OR if there is any reported violation of the RedRules to support the staff in the room and ensure patient safety
Phase III Monitoring and ControlAfter the initial staff education program the team made the
transition in its efforts from monitoring and process controlFirst a rapid response event leadership team was formed Thisteam included surgeon nursing and administrative leadershipmembers Additional ad hoc members included quality man-
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
Figure 2 An incorrect-count decision tree was developed to assist operating room (OR) personnel in a standard approach to a miscount or possible retained for-eign object (RFO) event RN registered nurse NM nurse manager Q-read Quick read (a digital imaging system) CDM clinical documentation manager(application in the electronic medical record used for all ORndashrelated documentation)
An Incorrect Decision Tree
126
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
agement services nursing education and institutional sentinelevent personnel This team was informed of any near-miss orreal RFO event in the OR Within 12ndash24 hours of the event ameeting was convened that included the event response teamand all OR personnel involved in the incident including thesurgeons residents nurses and allied health staff The purposeof the meeting was to debrief all team members as to their rec-ollection of the events and circumstances contributing to theevent This process was not designed as a replacement for theformal sentinel event RCA or to assign responsibility for theevent Rather it was intended to quickly inform OR leadershipof the circumstances to determine areas of potential systemweakness Once the leadership team performed the analysis ofthe event a memo describing the circumstances of the eventand findings was prepared and shared with all OR personnelwithin 24ndash48 hours of the event (Table 1 page 130)Furthermore once the formal RCA was completed the find-ings were shared with the leadership team and then OR person-nel during the morning report
Another tactic to keep the OR staff aware of the RFO initia-tive was use of posters tracking the number of days since the lastRFO These posters were placed at the entrances to the ORs Inaddition RFO procedures and policies were randomlyreviewed by nursing leadership at staff morning reports Finallyquarterly all-staff meetings were held that focused on OR safe-ty team communication and RFO performance updates
ResultsThe impact of this multidisciplinaryeffort to reduce surgical RFO resultedin a significant decline in the frequencyof RFO events (Figure 6 page 131)Before initiating this effort we averagedan RFO or near miss once every 16days With the interventions the inter-val extended to an average of one RFOevery 69 days This level of perform-ance has been sustained for more thantwo years
Surgery involves multiple itemsincluding sponges needles and equip-ment These are counted as part of thebaseline count and in subsequentcounts that occur throughout the caseThe number of items routinely countedin a case often exceeds 100 uniqueitems Greenberg et al reported that
counting of multiple items is performed on average 16 timesper case each of these counts represents an opportunity forerror12 Assuming the potential for RFO opportunities is 25 peroperative case a defect per million opportunities (DPMO)analysis shows a decline from 052 to 011 per 1000 surgeriesIn other terms this represents an increase in the Sigma per-formance level of 56 to 60 (Figure 7 page 131) a process isconsidered to be at Six Sigma level when there are 34 DPMO
DiscussionMCR identified our rate of RFOs especially surgical spongesas a major quality and patient safety issue in 2005 A multidis-ciplinary multiphase approach was instituted with a goal of zeroRFOs This three-phased approach which consisted of detailedanalysis of our institutional experience including review andrevision of relevant policies broad and focused educational pro-grams and continuous participation and monitoring by surgi-cal and nursing leadership led to a significant reduction inRFOs within 2 years These efforts contributed to a reductionin the frequency of surgical RFOs from an average of one every16 days to one in 69 days
Surgical RFOs are often dramatic examples of medicalerrors They can lead to significant patient harm and (1) nega-tive impact to the reputations of both providers and health careorganizations and (2) negative financial impact due to financialwrite-offs and legal claims2 Frequently RFOs have been viewed
127March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
Figure 3 A multiphase broad-based awareness education campaign was initiated RFO retained foreignobject OR operating room
Phase II Awareness and Communication Plan 2007
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
128 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
as isolated unfortunate events that often lead to mitigationapproaches designed for the circumstances of each event Thisis a common problem with a sentinel event RCA approach toindividual events13 Some system and patient factors have beenassociated with a higher risk of RFOs (emergency cases changein the planned procedure and higher BMI patients)4 Howeverthe analysis of MCR RFOs did not reveal an association withthese factors5
Given the inability to identify any patient or proceduralcharacteristics that predisposed for RFOs at our institution amore broad-based approach to finding a solution was requiredAlthough much of the available literature regarding surgicalRFOs focuses on the types of objects retained and the circum-stances surrounding the events these sources lack recommen-dations about how institutions should analyze and improvetheir systems to minimize these events
The multidisciplinary team under the auspices of the surgi-cal quality assessment and safety committee led the initiative
toward zero RFOs As described this program was divided intothree phases (1) failure analysis and policy review (2) staffawareness and education (3) monitoring and control
The first phase required a detailed systematic evaluation ofour RFO experience This was coupled with a detailed reviewand revisions of existing policies and procedures in order toestablish clear definitions internally consistent policies andperformance expectations For example gaps were discoveredin our system processes in the event of a miscount and theresponse time for intraoperative films were inconsistent Thepolicy was simplified (Figure 2) and updated to reflect ldquoSTATrdquoorders for suspected RFOs and to require review of the film byradiologist and consultant or designee within 30 minutes Allintraoperative films requested to evaluate possible RFOs areordered as ldquorule out RFOrdquo The item missing is not specificallynoted on the x-ray request because this may predispose the radi-ologist to focus his or her initial read toward that object and toignore other findings Once read the radiologist calls into the
Figure 4 A sample OR white board is shown with labels designating the required place for the documentation of all counted items and pertinent patient infor-mation in the OR (patient information removed) In the lower right corner is a place for any items intentionally tucked into the wound and not under thedirect control of a member of the surgical team
Sample Operating Room (OR) White Board
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
129March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
OR and reviews all item seen on the film with the surgeon atwhich time the radiologist is specifically informed of what itemthe team believes is missing Response time for intraoperativeRFO films and adherence to policy were reviewed monthly bythe surgical quality assessment and safety committee to ensurecompliance
The second phase of the program was an intense education-al effort directed at all OR personnel regarding the scope anddetails of the RFO problem at MCR Again this wasapproached in phases The first was the all-staff meeting whichserved many purposes important to the success of this initiative
1 It ensured that all staff (physicians nurses and alliedhealth staff ) in the OR heard a single consistent messageregarding RFOs
2 It demonstrated a unified and engaged leadership team3 It articulated a clear and organized set of policies and pro-
cedures related to RFO reduction and prevention4 It set expected performance standards for all personnel in
the ORAll these elements are known to be essential for the successfulimplementation change within an organization13
Initiated at the same time as the all-staff meeting was anextensive education effort (Conscientious Count Campaign)
This education effort included daily morning report reviews ofthe appropriate and standardized counting protocols reviews ofrelated policies and in-room audits This program served toreinforce the training and performance of all OR personnel onthe standardized approach to counting and responding topotential RFO events Again this protracted education effortwhich stressed improving direct communication between allteam members to improve OR ldquosituational awarenessrdquo hasbeen shown to be one of the most important components forsuccessful institutional change14
The white board served as a tool to standardize documenta-tion of items used and any items that are tucked thus improv-ing the situational awareness of items placed in the surgicalfield Furthermore its use improved communication betweenOR staff members and was a more reliable mechanism thanhaving to rely on the surgical staff rsquos short-term memory It alsohelped in auditing the compliance to the new guidelines of doc-umenting counted and tucked items by nursing leadership per-forming daily observational audits The new counting anddocumentation policies and guidelines were implemented in allORs at the same time However development of specialty-spe-cific white boards were rolled out one specialty at a time after adetailed analysis of their unique instrumentation needsRandom audits are performed daily for 5 of the cases for eachspecialty by the specialty nurse manager The baseline counttucked item documentation and final counts are audited andcompliance has been 994 or higher for the latest quarter(third quarter 2008) In the event of a miscount compliancewith the established policies and procedures is determined anddocumented by specialty or overall surgical nursing leadershipImportantly all the information and findings are fed back tothe OR team members
The last phase of our effort demonstrated a new resolve byleadership to respond to RFO events Previously these eventswere addressed by the institutional sentinel event (SE) teamoften in isolation and without participation of key surgicalleaders (though these leaders were often invited to participate)The SE effort was often too focused on developing an RCA forthe individual event and did not address the broader culturaland communication issues that exist in the OR environmentNor did this process allow for active monitoring of the ORenvironment to identify the more latent safety issues Finallythe process was slow and the proposed solution to the eventwas often implemented some time after the event All theseissues reflect criticisms of the RCA process1516
To address these concerns a rapid leadership response teamwas formed to address the event within 24ndash36 hours with all
Figure 5 The Red Rules poster displayed in every operating room (OR) pro-vides the two inviolable rules of conduct in the OR The poster informs all staffmembers that adhering to appropriate counting policy is at a level of impor-tance equal to following the Universal Protocol to ensure patient safety
Red Rules Poster
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
130 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
personnel involved The clearly stated purpose of the meetingwas to understand the circumstances of the event and to not bepunitive or assign blame Important to the success of thesemeetings was the involvement of surgical and nursing leader-ship and the development of an open and secure environmentto share the events understand the failures and create plans toshare the lessons learned with all the OR personnel A summa-ry of the event and lessons learned were quickly disseminated ina written memo from the leadership group to all personnel andshared in all areas often within a few days of the event A non-punitive approach to addressing this type of medical error has
been shown to improve staff satisfaction performance andcommunication and to be integral to processes that supportinstitutional crisis management1718
A number of barriers to the success of this initiative wereidentified including poor interaction between the leadership ofthe different stakeholders no standardized institutional ordepartment response to RFO events and poor accountabilityfor addressing the problem of RFOs However the major bar-rier to success was a long-standing culture of poor communica-tion between our OR staff members The tradition of surgeonprimacy in the OR led to a culture lacking in basic communi-
Table 1 Examples of Key Information from Memos to Staff After a Retained Foreign Object (RFO) Event or Near Miss
Brief Description of Event
Near Miss Needle count off
intraoperative film ordered
patient closed because
patient condition before film
was reviewed
Near Miss Needle count off
after exhaustive search in
OR three different intra-op
films taken and needle not
found second exhaustive
search in OR yielded no
needle Patient closed and
survey film revealed needle
A counted-out (after final
pause) sponge was tucked to
protect the abdominal viscera
during closure resulting in a
retained sponge
Argon beam coagulatorrsquos grey
tape (nonndashradio opaque) was
replaced with black tip (radio
opaque) without any notifica-
tion from manufacturer The
tip was not removed and was
retained
Root Causes Identified
Patient condition
Communication gap among
OR staff and radiology
Technology limitation of
intraoperative film vs
survey film
Surgeonrsquos preference for a
particular trochar may or
may not have played a role
Use of sponge in a
nonrecommended fashion
as a viscera retainer
Not following existing cur-
rent policy for final count
and verbalizing tucked items
Communication lapse
between manufacturer and
users
Strengths Identified
Adherence to the
current process
Adherence to the
current process
Appropriate
interventions taken
Survey film of all
patients even when
counts are correct
Survey film of all
patients even when
counts are correct
Opportunities for
Improvement
Radiology process for
RFO rule-out
Communication between
OR staff and radiology
Review of policy for
missing microneedles
(definition process steps
for missing microneedle)
Standardization of
equipment
Training of new fellows and
residents on current best
practices
Communication among
OR staff
While the functionality of
the tape replacement was
improved to make it radio
opaque the change was
not communicated to the
users by the manufacturer
Next Steps Delineated
State in request ldquorule out an
RFOrdquo to expedite review in
less than 30 minutes
Do not move the patient from
OR if patient condition war-
rants to facilitate additional
films to rule out an RFO
Develop policy for
microneedles
Review laparoscopic
equipment available to the
surgical team and their
application to the procedure
being performed
Use rubber viscera retainers
or ldquofishrdquo for viscera retainer
Bag off all counted out
sponges in all specialties
Provide training for all new
residents and fellows
Notify all users throughout
the institution
Remove all mislabeled
equipment from supply
Contact manufacturer and
get issue resolved
Notify FDA
OR operating room FDA Food and Drug Administration
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
131March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
cation skills poor situational awarenessand concern about questioning thecourse of events in the OR This initia-tive helped our organization clarifyissues with our existing processes toavoid RFOs as well as design and imple-ment solutions However the mostimportant benefit was that it highlight-ed the underlying behavior and commu-nication failures between our staffmembers This finding drove the latterhalf of the initiative to focus on teachingand improving team communication
Summary and Conclusions In summary MCR identified the inci-dence of RFOs as a serious quality per-formance issue in the OR To addressthis problem a multidisciplinary leader-ship group was formed that took a sys-tematic evidence-based approach toanalyzing the factors contributing toRFO events Guided by institutionaldata OR leadership engaged the entireOR staff in a broad-based communica-tioneducation program and incorporat-ed system redesign to minimize futureRFOs
The OR environment is complexand manual counting of surgical items isan inherently error-prone process MCRcontinues to perform postoperative sur-vey films for all surgeries in which abody cavity is opened which we believeis the best defense currently available todetect unrecognized RFOs despite all ofour best efforts to improve the intraop-erative processes of counting and docu-mentation We believe that we havereached a performance boundary withour current process and await eitherimplementation of a new technology ora fundamental change in how our entiresurgical process is performed J
Figure 6 The frequency of potential RFO events declined significantly after the initiation of the reduc-tion effort We used a G-Chart which has significantly greater detection power over conventional bino-mial-based approaches particularly for infrequent events and low ldquodefectrdquo rates such as RFOs MCR wasaveraging a surgical RFO every 16 days which was extended to every 69 days as of October 2008
Days Between Potential Retained Foreign Object (RFO)Events January 2003ndashOctober 2008
Figure 7 The defects-per-million-opportunity analysis is shown assuming 25 chances (defect opportuni-ties) per surgical case for an error resulting in a retained foreign object
Defects per Million Opportunities (DPMO) and Sigma LevelMayo Clinic Rochester Minnesota 2003ndash2007
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
132 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
References1 Associated Press Towel Found in Dead Womanrsquos Body CBSNewscomAugust 6 2004 httpwwwcbsnewscomstories20040806healthprintable634558shtml (last accessed Jan 16 2009)2 Sowka MP The medical malpractice closed claims study Conducted bythe National Association of Insurance Commissioners Conn Med45109ndash115 Feb 19813 Gonzales-Ojeda A et al Retained foreign bodies following intra-abdom-inal surgery Hepatogastroenterology 46808ndash812 Mar 19994 Gawande AA et al Risk factors for retained instruments N Engl J Med348229ndash235 Jan 16 20035 Cima RR et al Incidence and characteristics of potential and actualretained foreign object events in surgical patients J Am Coll Surg 20780ndash87Jul 2008 Epub 2008 May 23 20086 Gibbs VC Preventable errors in the operating room Retained foreign bod-
ies after surgeryndashPart I Curr Probl Surg 44281ndash337 May 20077 Leonard M et al The human factor The critical importance of effectiveteamwork and communication Qual Saf Health Care 13(suppl 1)85ndash90Oct 20048 Lingard L et al Communication failures in the operating room Anobservational classification of recurrent types an events Qual Saf Health Care13330ndash334 Oct 20049 Donchin Y et al A look into the nature and causes of human errors in theintensive care unit Qual Saf Health Care 12143ndash147 Apr 200310 AORN Recommended Practices Committee Recommended practices forsponge sharps and instrument counts AORN J 83418 421ndash426 429ndash433Feb 200611 The Joint Commission Universal Protocol httpwwwjointcommissionorgPatientSafetyUniversalProtocol (last accessed Jan 16 2009) 12 Greenberg C et al The frequency and significance of discrepancies in thesurgical count Annal Surg 248337ndash341 Aug 200813 Lukas CV et al Transformational change in health care systems Anorganizational model Health Care Manage Rev 32309ndash320 OctndashDec 200714 Wang MC et al Redesigning health systems for quality Lessons fromemerging practices Jt Comm J Qual Patient Saf 32599ndash611 Nov 200615 Wu AW Lipshutz AK Pronovost PJ Effectiveness and efficiency ofroot cause analysis in medicine JAMA 299685ndash687 Feb 13 2008 16 Reason J Managing the Risks of Organizational Accidents Farnham UKAshgate 199717 Helmrich RL On error management Lessons from aviation BMJ320781ndash785 Mar 18 200018 Marx D Patient Safety and the ldquoJust Culturerdquo A Primer for Health CareExecutives Medical Event Reporting System for Transfusion Medicine Agency forHealthcare Research and Quality 2001 httppsnetahrqgovresourceaspxresourceID=1582 (last accessed Jan 16 2009)
Robert R Cima MD MA is Associate Professor Department of
Surgery Mayo Clinic Rochester Minnesota Anantha
Kollengode PhD MBA is Quality Analyst Quality
Management Services Amy S Storsveen RN BSN is Charge
Nurse and Cheryl A Weisbrod RN MS is Director Surgical
Services Claude Deschamps MD is Professor and Chairman
Department of Surgery Mark B Koch MBA is Associate
Administrator Administrative Services Debra Moore is Nursing
Analyst and Sarah R Pool RN MS is Nursing Educator
Surgical Services Please address correspondence to Robert R
Cima cimarobertmayoedu
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations

March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
Figure 2 An incorrect-count decision tree was developed to assist operating room (OR) personnel in a standard approach to a miscount or possible retained for-eign object (RFO) event RN registered nurse NM nurse manager Q-read Quick read (a digital imaging system) CDM clinical documentation manager(application in the electronic medical record used for all ORndashrelated documentation)
An Incorrect Decision Tree
126
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
agement services nursing education and institutional sentinelevent personnel This team was informed of any near-miss orreal RFO event in the OR Within 12ndash24 hours of the event ameeting was convened that included the event response teamand all OR personnel involved in the incident including thesurgeons residents nurses and allied health staff The purposeof the meeting was to debrief all team members as to their rec-ollection of the events and circumstances contributing to theevent This process was not designed as a replacement for theformal sentinel event RCA or to assign responsibility for theevent Rather it was intended to quickly inform OR leadershipof the circumstances to determine areas of potential systemweakness Once the leadership team performed the analysis ofthe event a memo describing the circumstances of the eventand findings was prepared and shared with all OR personnelwithin 24ndash48 hours of the event (Table 1 page 130)Furthermore once the formal RCA was completed the find-ings were shared with the leadership team and then OR person-nel during the morning report
Another tactic to keep the OR staff aware of the RFO initia-tive was use of posters tracking the number of days since the lastRFO These posters were placed at the entrances to the ORs Inaddition RFO procedures and policies were randomlyreviewed by nursing leadership at staff morning reports Finallyquarterly all-staff meetings were held that focused on OR safe-ty team communication and RFO performance updates
ResultsThe impact of this multidisciplinaryeffort to reduce surgical RFO resultedin a significant decline in the frequencyof RFO events (Figure 6 page 131)Before initiating this effort we averagedan RFO or near miss once every 16days With the interventions the inter-val extended to an average of one RFOevery 69 days This level of perform-ance has been sustained for more thantwo years
Surgery involves multiple itemsincluding sponges needles and equip-ment These are counted as part of thebaseline count and in subsequentcounts that occur throughout the caseThe number of items routinely countedin a case often exceeds 100 uniqueitems Greenberg et al reported that
counting of multiple items is performed on average 16 timesper case each of these counts represents an opportunity forerror12 Assuming the potential for RFO opportunities is 25 peroperative case a defect per million opportunities (DPMO)analysis shows a decline from 052 to 011 per 1000 surgeriesIn other terms this represents an increase in the Sigma per-formance level of 56 to 60 (Figure 7 page 131) a process isconsidered to be at Six Sigma level when there are 34 DPMO
DiscussionMCR identified our rate of RFOs especially surgical spongesas a major quality and patient safety issue in 2005 A multidis-ciplinary multiphase approach was instituted with a goal of zeroRFOs This three-phased approach which consisted of detailedanalysis of our institutional experience including review andrevision of relevant policies broad and focused educational pro-grams and continuous participation and monitoring by surgi-cal and nursing leadership led to a significant reduction inRFOs within 2 years These efforts contributed to a reductionin the frequency of surgical RFOs from an average of one every16 days to one in 69 days
Surgical RFOs are often dramatic examples of medicalerrors They can lead to significant patient harm and (1) nega-tive impact to the reputations of both providers and health careorganizations and (2) negative financial impact due to financialwrite-offs and legal claims2 Frequently RFOs have been viewed
127March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
Figure 3 A multiphase broad-based awareness education campaign was initiated RFO retained foreignobject OR operating room
Phase II Awareness and Communication Plan 2007
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
128 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
as isolated unfortunate events that often lead to mitigationapproaches designed for the circumstances of each event Thisis a common problem with a sentinel event RCA approach toindividual events13 Some system and patient factors have beenassociated with a higher risk of RFOs (emergency cases changein the planned procedure and higher BMI patients)4 Howeverthe analysis of MCR RFOs did not reveal an association withthese factors5
Given the inability to identify any patient or proceduralcharacteristics that predisposed for RFOs at our institution amore broad-based approach to finding a solution was requiredAlthough much of the available literature regarding surgicalRFOs focuses on the types of objects retained and the circum-stances surrounding the events these sources lack recommen-dations about how institutions should analyze and improvetheir systems to minimize these events
The multidisciplinary team under the auspices of the surgi-cal quality assessment and safety committee led the initiative
toward zero RFOs As described this program was divided intothree phases (1) failure analysis and policy review (2) staffawareness and education (3) monitoring and control
The first phase required a detailed systematic evaluation ofour RFO experience This was coupled with a detailed reviewand revisions of existing policies and procedures in order toestablish clear definitions internally consistent policies andperformance expectations For example gaps were discoveredin our system processes in the event of a miscount and theresponse time for intraoperative films were inconsistent Thepolicy was simplified (Figure 2) and updated to reflect ldquoSTATrdquoorders for suspected RFOs and to require review of the film byradiologist and consultant or designee within 30 minutes Allintraoperative films requested to evaluate possible RFOs areordered as ldquorule out RFOrdquo The item missing is not specificallynoted on the x-ray request because this may predispose the radi-ologist to focus his or her initial read toward that object and toignore other findings Once read the radiologist calls into the
Figure 4 A sample OR white board is shown with labels designating the required place for the documentation of all counted items and pertinent patient infor-mation in the OR (patient information removed) In the lower right corner is a place for any items intentionally tucked into the wound and not under thedirect control of a member of the surgical team
Sample Operating Room (OR) White Board
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
129March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
OR and reviews all item seen on the film with the surgeon atwhich time the radiologist is specifically informed of what itemthe team believes is missing Response time for intraoperativeRFO films and adherence to policy were reviewed monthly bythe surgical quality assessment and safety committee to ensurecompliance
The second phase of the program was an intense education-al effort directed at all OR personnel regarding the scope anddetails of the RFO problem at MCR Again this wasapproached in phases The first was the all-staff meeting whichserved many purposes important to the success of this initiative
1 It ensured that all staff (physicians nurses and alliedhealth staff ) in the OR heard a single consistent messageregarding RFOs
2 It demonstrated a unified and engaged leadership team3 It articulated a clear and organized set of policies and pro-
cedures related to RFO reduction and prevention4 It set expected performance standards for all personnel in
the ORAll these elements are known to be essential for the successfulimplementation change within an organization13
Initiated at the same time as the all-staff meeting was anextensive education effort (Conscientious Count Campaign)
This education effort included daily morning report reviews ofthe appropriate and standardized counting protocols reviews ofrelated policies and in-room audits This program served toreinforce the training and performance of all OR personnel onthe standardized approach to counting and responding topotential RFO events Again this protracted education effortwhich stressed improving direct communication between allteam members to improve OR ldquosituational awarenessrdquo hasbeen shown to be one of the most important components forsuccessful institutional change14
The white board served as a tool to standardize documenta-tion of items used and any items that are tucked thus improv-ing the situational awareness of items placed in the surgicalfield Furthermore its use improved communication betweenOR staff members and was a more reliable mechanism thanhaving to rely on the surgical staff rsquos short-term memory It alsohelped in auditing the compliance to the new guidelines of doc-umenting counted and tucked items by nursing leadership per-forming daily observational audits The new counting anddocumentation policies and guidelines were implemented in allORs at the same time However development of specialty-spe-cific white boards were rolled out one specialty at a time after adetailed analysis of their unique instrumentation needsRandom audits are performed daily for 5 of the cases for eachspecialty by the specialty nurse manager The baseline counttucked item documentation and final counts are audited andcompliance has been 994 or higher for the latest quarter(third quarter 2008) In the event of a miscount compliancewith the established policies and procedures is determined anddocumented by specialty or overall surgical nursing leadershipImportantly all the information and findings are fed back tothe OR team members
The last phase of our effort demonstrated a new resolve byleadership to respond to RFO events Previously these eventswere addressed by the institutional sentinel event (SE) teamoften in isolation and without participation of key surgicalleaders (though these leaders were often invited to participate)The SE effort was often too focused on developing an RCA forthe individual event and did not address the broader culturaland communication issues that exist in the OR environmentNor did this process allow for active monitoring of the ORenvironment to identify the more latent safety issues Finallythe process was slow and the proposed solution to the eventwas often implemented some time after the event All theseissues reflect criticisms of the RCA process1516
To address these concerns a rapid leadership response teamwas formed to address the event within 24ndash36 hours with all
Figure 5 The Red Rules poster displayed in every operating room (OR) pro-vides the two inviolable rules of conduct in the OR The poster informs all staffmembers that adhering to appropriate counting policy is at a level of impor-tance equal to following the Universal Protocol to ensure patient safety
Red Rules Poster
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
130 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
personnel involved The clearly stated purpose of the meetingwas to understand the circumstances of the event and to not bepunitive or assign blame Important to the success of thesemeetings was the involvement of surgical and nursing leader-ship and the development of an open and secure environmentto share the events understand the failures and create plans toshare the lessons learned with all the OR personnel A summa-ry of the event and lessons learned were quickly disseminated ina written memo from the leadership group to all personnel andshared in all areas often within a few days of the event A non-punitive approach to addressing this type of medical error has
been shown to improve staff satisfaction performance andcommunication and to be integral to processes that supportinstitutional crisis management1718
A number of barriers to the success of this initiative wereidentified including poor interaction between the leadership ofthe different stakeholders no standardized institutional ordepartment response to RFO events and poor accountabilityfor addressing the problem of RFOs However the major bar-rier to success was a long-standing culture of poor communica-tion between our OR staff members The tradition of surgeonprimacy in the OR led to a culture lacking in basic communi-
Table 1 Examples of Key Information from Memos to Staff After a Retained Foreign Object (RFO) Event or Near Miss
Brief Description of Event
Near Miss Needle count off
intraoperative film ordered
patient closed because
patient condition before film
was reviewed
Near Miss Needle count off
after exhaustive search in
OR three different intra-op
films taken and needle not
found second exhaustive
search in OR yielded no
needle Patient closed and
survey film revealed needle
A counted-out (after final
pause) sponge was tucked to
protect the abdominal viscera
during closure resulting in a
retained sponge
Argon beam coagulatorrsquos grey
tape (nonndashradio opaque) was
replaced with black tip (radio
opaque) without any notifica-
tion from manufacturer The
tip was not removed and was
retained
Root Causes Identified
Patient condition
Communication gap among
OR staff and radiology
Technology limitation of
intraoperative film vs
survey film
Surgeonrsquos preference for a
particular trochar may or
may not have played a role
Use of sponge in a
nonrecommended fashion
as a viscera retainer
Not following existing cur-
rent policy for final count
and verbalizing tucked items
Communication lapse
between manufacturer and
users
Strengths Identified
Adherence to the
current process
Adherence to the
current process
Appropriate
interventions taken
Survey film of all
patients even when
counts are correct
Survey film of all
patients even when
counts are correct
Opportunities for
Improvement
Radiology process for
RFO rule-out
Communication between
OR staff and radiology
Review of policy for
missing microneedles
(definition process steps
for missing microneedle)
Standardization of
equipment
Training of new fellows and
residents on current best
practices
Communication among
OR staff
While the functionality of
the tape replacement was
improved to make it radio
opaque the change was
not communicated to the
users by the manufacturer
Next Steps Delineated
State in request ldquorule out an
RFOrdquo to expedite review in
less than 30 minutes
Do not move the patient from
OR if patient condition war-
rants to facilitate additional
films to rule out an RFO
Develop policy for
microneedles
Review laparoscopic
equipment available to the
surgical team and their
application to the procedure
being performed
Use rubber viscera retainers
or ldquofishrdquo for viscera retainer
Bag off all counted out
sponges in all specialties
Provide training for all new
residents and fellows
Notify all users throughout
the institution
Remove all mislabeled
equipment from supply
Contact manufacturer and
get issue resolved
Notify FDA
OR operating room FDA Food and Drug Administration
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
131March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
cation skills poor situational awarenessand concern about questioning thecourse of events in the OR This initia-tive helped our organization clarifyissues with our existing processes toavoid RFOs as well as design and imple-ment solutions However the mostimportant benefit was that it highlight-ed the underlying behavior and commu-nication failures between our staffmembers This finding drove the latterhalf of the initiative to focus on teachingand improving team communication
Summary and Conclusions In summary MCR identified the inci-dence of RFOs as a serious quality per-formance issue in the OR To addressthis problem a multidisciplinary leader-ship group was formed that took a sys-tematic evidence-based approach toanalyzing the factors contributing toRFO events Guided by institutionaldata OR leadership engaged the entireOR staff in a broad-based communica-tioneducation program and incorporat-ed system redesign to minimize futureRFOs
The OR environment is complexand manual counting of surgical items isan inherently error-prone process MCRcontinues to perform postoperative sur-vey films for all surgeries in which abody cavity is opened which we believeis the best defense currently available todetect unrecognized RFOs despite all ofour best efforts to improve the intraop-erative processes of counting and docu-mentation We believe that we havereached a performance boundary withour current process and await eitherimplementation of a new technology ora fundamental change in how our entiresurgical process is performed J
Figure 6 The frequency of potential RFO events declined significantly after the initiation of the reduc-tion effort We used a G-Chart which has significantly greater detection power over conventional bino-mial-based approaches particularly for infrequent events and low ldquodefectrdquo rates such as RFOs MCR wasaveraging a surgical RFO every 16 days which was extended to every 69 days as of October 2008
Days Between Potential Retained Foreign Object (RFO)Events January 2003ndashOctober 2008
Figure 7 The defects-per-million-opportunity analysis is shown assuming 25 chances (defect opportuni-ties) per surgical case for an error resulting in a retained foreign object
Defects per Million Opportunities (DPMO) and Sigma LevelMayo Clinic Rochester Minnesota 2003ndash2007
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
132 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
References1 Associated Press Towel Found in Dead Womanrsquos Body CBSNewscomAugust 6 2004 httpwwwcbsnewscomstories20040806healthprintable634558shtml (last accessed Jan 16 2009)2 Sowka MP The medical malpractice closed claims study Conducted bythe National Association of Insurance Commissioners Conn Med45109ndash115 Feb 19813 Gonzales-Ojeda A et al Retained foreign bodies following intra-abdom-inal surgery Hepatogastroenterology 46808ndash812 Mar 19994 Gawande AA et al Risk factors for retained instruments N Engl J Med348229ndash235 Jan 16 20035 Cima RR et al Incidence and characteristics of potential and actualretained foreign object events in surgical patients J Am Coll Surg 20780ndash87Jul 2008 Epub 2008 May 23 20086 Gibbs VC Preventable errors in the operating room Retained foreign bod-
ies after surgeryndashPart I Curr Probl Surg 44281ndash337 May 20077 Leonard M et al The human factor The critical importance of effectiveteamwork and communication Qual Saf Health Care 13(suppl 1)85ndash90Oct 20048 Lingard L et al Communication failures in the operating room Anobservational classification of recurrent types an events Qual Saf Health Care13330ndash334 Oct 20049 Donchin Y et al A look into the nature and causes of human errors in theintensive care unit Qual Saf Health Care 12143ndash147 Apr 200310 AORN Recommended Practices Committee Recommended practices forsponge sharps and instrument counts AORN J 83418 421ndash426 429ndash433Feb 200611 The Joint Commission Universal Protocol httpwwwjointcommissionorgPatientSafetyUniversalProtocol (last accessed Jan 16 2009) 12 Greenberg C et al The frequency and significance of discrepancies in thesurgical count Annal Surg 248337ndash341 Aug 200813 Lukas CV et al Transformational change in health care systems Anorganizational model Health Care Manage Rev 32309ndash320 OctndashDec 200714 Wang MC et al Redesigning health systems for quality Lessons fromemerging practices Jt Comm J Qual Patient Saf 32599ndash611 Nov 200615 Wu AW Lipshutz AK Pronovost PJ Effectiveness and efficiency ofroot cause analysis in medicine JAMA 299685ndash687 Feb 13 2008 16 Reason J Managing the Risks of Organizational Accidents Farnham UKAshgate 199717 Helmrich RL On error management Lessons from aviation BMJ320781ndash785 Mar 18 200018 Marx D Patient Safety and the ldquoJust Culturerdquo A Primer for Health CareExecutives Medical Event Reporting System for Transfusion Medicine Agency forHealthcare Research and Quality 2001 httppsnetahrqgovresourceaspxresourceID=1582 (last accessed Jan 16 2009)
Robert R Cima MD MA is Associate Professor Department of
Surgery Mayo Clinic Rochester Minnesota Anantha
Kollengode PhD MBA is Quality Analyst Quality
Management Services Amy S Storsveen RN BSN is Charge
Nurse and Cheryl A Weisbrod RN MS is Director Surgical
Services Claude Deschamps MD is Professor and Chairman
Department of Surgery Mark B Koch MBA is Associate
Administrator Administrative Services Debra Moore is Nursing
Analyst and Sarah R Pool RN MS is Nursing Educator
Surgical Services Please address correspondence to Robert R
Cima cimarobertmayoedu
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations

agement services nursing education and institutional sentinelevent personnel This team was informed of any near-miss orreal RFO event in the OR Within 12ndash24 hours of the event ameeting was convened that included the event response teamand all OR personnel involved in the incident including thesurgeons residents nurses and allied health staff The purposeof the meeting was to debrief all team members as to their rec-ollection of the events and circumstances contributing to theevent This process was not designed as a replacement for theformal sentinel event RCA or to assign responsibility for theevent Rather it was intended to quickly inform OR leadershipof the circumstances to determine areas of potential systemweakness Once the leadership team performed the analysis ofthe event a memo describing the circumstances of the eventand findings was prepared and shared with all OR personnelwithin 24ndash48 hours of the event (Table 1 page 130)Furthermore once the formal RCA was completed the find-ings were shared with the leadership team and then OR person-nel during the morning report
Another tactic to keep the OR staff aware of the RFO initia-tive was use of posters tracking the number of days since the lastRFO These posters were placed at the entrances to the ORs Inaddition RFO procedures and policies were randomlyreviewed by nursing leadership at staff morning reports Finallyquarterly all-staff meetings were held that focused on OR safe-ty team communication and RFO performance updates
ResultsThe impact of this multidisciplinaryeffort to reduce surgical RFO resultedin a significant decline in the frequencyof RFO events (Figure 6 page 131)Before initiating this effort we averagedan RFO or near miss once every 16days With the interventions the inter-val extended to an average of one RFOevery 69 days This level of perform-ance has been sustained for more thantwo years
Surgery involves multiple itemsincluding sponges needles and equip-ment These are counted as part of thebaseline count and in subsequentcounts that occur throughout the caseThe number of items routinely countedin a case often exceeds 100 uniqueitems Greenberg et al reported that
counting of multiple items is performed on average 16 timesper case each of these counts represents an opportunity forerror12 Assuming the potential for RFO opportunities is 25 peroperative case a defect per million opportunities (DPMO)analysis shows a decline from 052 to 011 per 1000 surgeriesIn other terms this represents an increase in the Sigma per-formance level of 56 to 60 (Figure 7 page 131) a process isconsidered to be at Six Sigma level when there are 34 DPMO
DiscussionMCR identified our rate of RFOs especially surgical spongesas a major quality and patient safety issue in 2005 A multidis-ciplinary multiphase approach was instituted with a goal of zeroRFOs This three-phased approach which consisted of detailedanalysis of our institutional experience including review andrevision of relevant policies broad and focused educational pro-grams and continuous participation and monitoring by surgi-cal and nursing leadership led to a significant reduction inRFOs within 2 years These efforts contributed to a reductionin the frequency of surgical RFOs from an average of one every16 days to one in 69 days
Surgical RFOs are often dramatic examples of medicalerrors They can lead to significant patient harm and (1) nega-tive impact to the reputations of both providers and health careorganizations and (2) negative financial impact due to financialwrite-offs and legal claims2 Frequently RFOs have been viewed
127March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
Figure 3 A multiphase broad-based awareness education campaign was initiated RFO retained foreignobject OR operating room
Phase II Awareness and Communication Plan 2007
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
128 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
as isolated unfortunate events that often lead to mitigationapproaches designed for the circumstances of each event Thisis a common problem with a sentinel event RCA approach toindividual events13 Some system and patient factors have beenassociated with a higher risk of RFOs (emergency cases changein the planned procedure and higher BMI patients)4 Howeverthe analysis of MCR RFOs did not reveal an association withthese factors5
Given the inability to identify any patient or proceduralcharacteristics that predisposed for RFOs at our institution amore broad-based approach to finding a solution was requiredAlthough much of the available literature regarding surgicalRFOs focuses on the types of objects retained and the circum-stances surrounding the events these sources lack recommen-dations about how institutions should analyze and improvetheir systems to minimize these events
The multidisciplinary team under the auspices of the surgi-cal quality assessment and safety committee led the initiative
toward zero RFOs As described this program was divided intothree phases (1) failure analysis and policy review (2) staffawareness and education (3) monitoring and control
The first phase required a detailed systematic evaluation ofour RFO experience This was coupled with a detailed reviewand revisions of existing policies and procedures in order toestablish clear definitions internally consistent policies andperformance expectations For example gaps were discoveredin our system processes in the event of a miscount and theresponse time for intraoperative films were inconsistent Thepolicy was simplified (Figure 2) and updated to reflect ldquoSTATrdquoorders for suspected RFOs and to require review of the film byradiologist and consultant or designee within 30 minutes Allintraoperative films requested to evaluate possible RFOs areordered as ldquorule out RFOrdquo The item missing is not specificallynoted on the x-ray request because this may predispose the radi-ologist to focus his or her initial read toward that object and toignore other findings Once read the radiologist calls into the
Figure 4 A sample OR white board is shown with labels designating the required place for the documentation of all counted items and pertinent patient infor-mation in the OR (patient information removed) In the lower right corner is a place for any items intentionally tucked into the wound and not under thedirect control of a member of the surgical team
Sample Operating Room (OR) White Board
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
129March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
OR and reviews all item seen on the film with the surgeon atwhich time the radiologist is specifically informed of what itemthe team believes is missing Response time for intraoperativeRFO films and adherence to policy were reviewed monthly bythe surgical quality assessment and safety committee to ensurecompliance
The second phase of the program was an intense education-al effort directed at all OR personnel regarding the scope anddetails of the RFO problem at MCR Again this wasapproached in phases The first was the all-staff meeting whichserved many purposes important to the success of this initiative
1 It ensured that all staff (physicians nurses and alliedhealth staff ) in the OR heard a single consistent messageregarding RFOs
2 It demonstrated a unified and engaged leadership team3 It articulated a clear and organized set of policies and pro-
cedures related to RFO reduction and prevention4 It set expected performance standards for all personnel in
the ORAll these elements are known to be essential for the successfulimplementation change within an organization13
Initiated at the same time as the all-staff meeting was anextensive education effort (Conscientious Count Campaign)
This education effort included daily morning report reviews ofthe appropriate and standardized counting protocols reviews ofrelated policies and in-room audits This program served toreinforce the training and performance of all OR personnel onthe standardized approach to counting and responding topotential RFO events Again this protracted education effortwhich stressed improving direct communication between allteam members to improve OR ldquosituational awarenessrdquo hasbeen shown to be one of the most important components forsuccessful institutional change14
The white board served as a tool to standardize documenta-tion of items used and any items that are tucked thus improv-ing the situational awareness of items placed in the surgicalfield Furthermore its use improved communication betweenOR staff members and was a more reliable mechanism thanhaving to rely on the surgical staff rsquos short-term memory It alsohelped in auditing the compliance to the new guidelines of doc-umenting counted and tucked items by nursing leadership per-forming daily observational audits The new counting anddocumentation policies and guidelines were implemented in allORs at the same time However development of specialty-spe-cific white boards were rolled out one specialty at a time after adetailed analysis of their unique instrumentation needsRandom audits are performed daily for 5 of the cases for eachspecialty by the specialty nurse manager The baseline counttucked item documentation and final counts are audited andcompliance has been 994 or higher for the latest quarter(third quarter 2008) In the event of a miscount compliancewith the established policies and procedures is determined anddocumented by specialty or overall surgical nursing leadershipImportantly all the information and findings are fed back tothe OR team members
The last phase of our effort demonstrated a new resolve byleadership to respond to RFO events Previously these eventswere addressed by the institutional sentinel event (SE) teamoften in isolation and without participation of key surgicalleaders (though these leaders were often invited to participate)The SE effort was often too focused on developing an RCA forthe individual event and did not address the broader culturaland communication issues that exist in the OR environmentNor did this process allow for active monitoring of the ORenvironment to identify the more latent safety issues Finallythe process was slow and the proposed solution to the eventwas often implemented some time after the event All theseissues reflect criticisms of the RCA process1516
To address these concerns a rapid leadership response teamwas formed to address the event within 24ndash36 hours with all
Figure 5 The Red Rules poster displayed in every operating room (OR) pro-vides the two inviolable rules of conduct in the OR The poster informs all staffmembers that adhering to appropriate counting policy is at a level of impor-tance equal to following the Universal Protocol to ensure patient safety
Red Rules Poster
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
130 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
personnel involved The clearly stated purpose of the meetingwas to understand the circumstances of the event and to not bepunitive or assign blame Important to the success of thesemeetings was the involvement of surgical and nursing leader-ship and the development of an open and secure environmentto share the events understand the failures and create plans toshare the lessons learned with all the OR personnel A summa-ry of the event and lessons learned were quickly disseminated ina written memo from the leadership group to all personnel andshared in all areas often within a few days of the event A non-punitive approach to addressing this type of medical error has
been shown to improve staff satisfaction performance andcommunication and to be integral to processes that supportinstitutional crisis management1718
A number of barriers to the success of this initiative wereidentified including poor interaction between the leadership ofthe different stakeholders no standardized institutional ordepartment response to RFO events and poor accountabilityfor addressing the problem of RFOs However the major bar-rier to success was a long-standing culture of poor communica-tion between our OR staff members The tradition of surgeonprimacy in the OR led to a culture lacking in basic communi-
Table 1 Examples of Key Information from Memos to Staff After a Retained Foreign Object (RFO) Event or Near Miss
Brief Description of Event
Near Miss Needle count off
intraoperative film ordered
patient closed because
patient condition before film
was reviewed
Near Miss Needle count off
after exhaustive search in
OR three different intra-op
films taken and needle not
found second exhaustive
search in OR yielded no
needle Patient closed and
survey film revealed needle
A counted-out (after final
pause) sponge was tucked to
protect the abdominal viscera
during closure resulting in a
retained sponge
Argon beam coagulatorrsquos grey
tape (nonndashradio opaque) was
replaced with black tip (radio
opaque) without any notifica-
tion from manufacturer The
tip was not removed and was
retained
Root Causes Identified
Patient condition
Communication gap among
OR staff and radiology
Technology limitation of
intraoperative film vs
survey film
Surgeonrsquos preference for a
particular trochar may or
may not have played a role
Use of sponge in a
nonrecommended fashion
as a viscera retainer
Not following existing cur-
rent policy for final count
and verbalizing tucked items
Communication lapse
between manufacturer and
users
Strengths Identified
Adherence to the
current process
Adherence to the
current process
Appropriate
interventions taken
Survey film of all
patients even when
counts are correct
Survey film of all
patients even when
counts are correct
Opportunities for
Improvement
Radiology process for
RFO rule-out
Communication between
OR staff and radiology
Review of policy for
missing microneedles
(definition process steps
for missing microneedle)
Standardization of
equipment
Training of new fellows and
residents on current best
practices
Communication among
OR staff
While the functionality of
the tape replacement was
improved to make it radio
opaque the change was
not communicated to the
users by the manufacturer
Next Steps Delineated
State in request ldquorule out an
RFOrdquo to expedite review in
less than 30 minutes
Do not move the patient from
OR if patient condition war-
rants to facilitate additional
films to rule out an RFO
Develop policy for
microneedles
Review laparoscopic
equipment available to the
surgical team and their
application to the procedure
being performed
Use rubber viscera retainers
or ldquofishrdquo for viscera retainer
Bag off all counted out
sponges in all specialties
Provide training for all new
residents and fellows
Notify all users throughout
the institution
Remove all mislabeled
equipment from supply
Contact manufacturer and
get issue resolved
Notify FDA
OR operating room FDA Food and Drug Administration
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
131March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
cation skills poor situational awarenessand concern about questioning thecourse of events in the OR This initia-tive helped our organization clarifyissues with our existing processes toavoid RFOs as well as design and imple-ment solutions However the mostimportant benefit was that it highlight-ed the underlying behavior and commu-nication failures between our staffmembers This finding drove the latterhalf of the initiative to focus on teachingand improving team communication
Summary and Conclusions In summary MCR identified the inci-dence of RFOs as a serious quality per-formance issue in the OR To addressthis problem a multidisciplinary leader-ship group was formed that took a sys-tematic evidence-based approach toanalyzing the factors contributing toRFO events Guided by institutionaldata OR leadership engaged the entireOR staff in a broad-based communica-tioneducation program and incorporat-ed system redesign to minimize futureRFOs
The OR environment is complexand manual counting of surgical items isan inherently error-prone process MCRcontinues to perform postoperative sur-vey films for all surgeries in which abody cavity is opened which we believeis the best defense currently available todetect unrecognized RFOs despite all ofour best efforts to improve the intraop-erative processes of counting and docu-mentation We believe that we havereached a performance boundary withour current process and await eitherimplementation of a new technology ora fundamental change in how our entiresurgical process is performed J
Figure 6 The frequency of potential RFO events declined significantly after the initiation of the reduc-tion effort We used a G-Chart which has significantly greater detection power over conventional bino-mial-based approaches particularly for infrequent events and low ldquodefectrdquo rates such as RFOs MCR wasaveraging a surgical RFO every 16 days which was extended to every 69 days as of October 2008
Days Between Potential Retained Foreign Object (RFO)Events January 2003ndashOctober 2008
Figure 7 The defects-per-million-opportunity analysis is shown assuming 25 chances (defect opportuni-ties) per surgical case for an error resulting in a retained foreign object
Defects per Million Opportunities (DPMO) and Sigma LevelMayo Clinic Rochester Minnesota 2003ndash2007
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
132 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
References1 Associated Press Towel Found in Dead Womanrsquos Body CBSNewscomAugust 6 2004 httpwwwcbsnewscomstories20040806healthprintable634558shtml (last accessed Jan 16 2009)2 Sowka MP The medical malpractice closed claims study Conducted bythe National Association of Insurance Commissioners Conn Med45109ndash115 Feb 19813 Gonzales-Ojeda A et al Retained foreign bodies following intra-abdom-inal surgery Hepatogastroenterology 46808ndash812 Mar 19994 Gawande AA et al Risk factors for retained instruments N Engl J Med348229ndash235 Jan 16 20035 Cima RR et al Incidence and characteristics of potential and actualretained foreign object events in surgical patients J Am Coll Surg 20780ndash87Jul 2008 Epub 2008 May 23 20086 Gibbs VC Preventable errors in the operating room Retained foreign bod-
ies after surgeryndashPart I Curr Probl Surg 44281ndash337 May 20077 Leonard M et al The human factor The critical importance of effectiveteamwork and communication Qual Saf Health Care 13(suppl 1)85ndash90Oct 20048 Lingard L et al Communication failures in the operating room Anobservational classification of recurrent types an events Qual Saf Health Care13330ndash334 Oct 20049 Donchin Y et al A look into the nature and causes of human errors in theintensive care unit Qual Saf Health Care 12143ndash147 Apr 200310 AORN Recommended Practices Committee Recommended practices forsponge sharps and instrument counts AORN J 83418 421ndash426 429ndash433Feb 200611 The Joint Commission Universal Protocol httpwwwjointcommissionorgPatientSafetyUniversalProtocol (last accessed Jan 16 2009) 12 Greenberg C et al The frequency and significance of discrepancies in thesurgical count Annal Surg 248337ndash341 Aug 200813 Lukas CV et al Transformational change in health care systems Anorganizational model Health Care Manage Rev 32309ndash320 OctndashDec 200714 Wang MC et al Redesigning health systems for quality Lessons fromemerging practices Jt Comm J Qual Patient Saf 32599ndash611 Nov 200615 Wu AW Lipshutz AK Pronovost PJ Effectiveness and efficiency ofroot cause analysis in medicine JAMA 299685ndash687 Feb 13 2008 16 Reason J Managing the Risks of Organizational Accidents Farnham UKAshgate 199717 Helmrich RL On error management Lessons from aviation BMJ320781ndash785 Mar 18 200018 Marx D Patient Safety and the ldquoJust Culturerdquo A Primer for Health CareExecutives Medical Event Reporting System for Transfusion Medicine Agency forHealthcare Research and Quality 2001 httppsnetahrqgovresourceaspxresourceID=1582 (last accessed Jan 16 2009)
Robert R Cima MD MA is Associate Professor Department of
Surgery Mayo Clinic Rochester Minnesota Anantha
Kollengode PhD MBA is Quality Analyst Quality
Management Services Amy S Storsveen RN BSN is Charge
Nurse and Cheryl A Weisbrod RN MS is Director Surgical
Services Claude Deschamps MD is Professor and Chairman
Department of Surgery Mark B Koch MBA is Associate
Administrator Administrative Services Debra Moore is Nursing
Analyst and Sarah R Pool RN MS is Nursing Educator
Surgical Services Please address correspondence to Robert R
Cima cimarobertmayoedu
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations

128 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
as isolated unfortunate events that often lead to mitigationapproaches designed for the circumstances of each event Thisis a common problem with a sentinel event RCA approach toindividual events13 Some system and patient factors have beenassociated with a higher risk of RFOs (emergency cases changein the planned procedure and higher BMI patients)4 Howeverthe analysis of MCR RFOs did not reveal an association withthese factors5
Given the inability to identify any patient or proceduralcharacteristics that predisposed for RFOs at our institution amore broad-based approach to finding a solution was requiredAlthough much of the available literature regarding surgicalRFOs focuses on the types of objects retained and the circum-stances surrounding the events these sources lack recommen-dations about how institutions should analyze and improvetheir systems to minimize these events
The multidisciplinary team under the auspices of the surgi-cal quality assessment and safety committee led the initiative
toward zero RFOs As described this program was divided intothree phases (1) failure analysis and policy review (2) staffawareness and education (3) monitoring and control
The first phase required a detailed systematic evaluation ofour RFO experience This was coupled with a detailed reviewand revisions of existing policies and procedures in order toestablish clear definitions internally consistent policies andperformance expectations For example gaps were discoveredin our system processes in the event of a miscount and theresponse time for intraoperative films were inconsistent Thepolicy was simplified (Figure 2) and updated to reflect ldquoSTATrdquoorders for suspected RFOs and to require review of the film byradiologist and consultant or designee within 30 minutes Allintraoperative films requested to evaluate possible RFOs areordered as ldquorule out RFOrdquo The item missing is not specificallynoted on the x-ray request because this may predispose the radi-ologist to focus his or her initial read toward that object and toignore other findings Once read the radiologist calls into the
Figure 4 A sample OR white board is shown with labels designating the required place for the documentation of all counted items and pertinent patient infor-mation in the OR (patient information removed) In the lower right corner is a place for any items intentionally tucked into the wound and not under thedirect control of a member of the surgical team
Sample Operating Room (OR) White Board
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
129March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
OR and reviews all item seen on the film with the surgeon atwhich time the radiologist is specifically informed of what itemthe team believes is missing Response time for intraoperativeRFO films and adherence to policy were reviewed monthly bythe surgical quality assessment and safety committee to ensurecompliance
The second phase of the program was an intense education-al effort directed at all OR personnel regarding the scope anddetails of the RFO problem at MCR Again this wasapproached in phases The first was the all-staff meeting whichserved many purposes important to the success of this initiative
1 It ensured that all staff (physicians nurses and alliedhealth staff ) in the OR heard a single consistent messageregarding RFOs
2 It demonstrated a unified and engaged leadership team3 It articulated a clear and organized set of policies and pro-
cedures related to RFO reduction and prevention4 It set expected performance standards for all personnel in
the ORAll these elements are known to be essential for the successfulimplementation change within an organization13
Initiated at the same time as the all-staff meeting was anextensive education effort (Conscientious Count Campaign)
This education effort included daily morning report reviews ofthe appropriate and standardized counting protocols reviews ofrelated policies and in-room audits This program served toreinforce the training and performance of all OR personnel onthe standardized approach to counting and responding topotential RFO events Again this protracted education effortwhich stressed improving direct communication between allteam members to improve OR ldquosituational awarenessrdquo hasbeen shown to be one of the most important components forsuccessful institutional change14
The white board served as a tool to standardize documenta-tion of items used and any items that are tucked thus improv-ing the situational awareness of items placed in the surgicalfield Furthermore its use improved communication betweenOR staff members and was a more reliable mechanism thanhaving to rely on the surgical staff rsquos short-term memory It alsohelped in auditing the compliance to the new guidelines of doc-umenting counted and tucked items by nursing leadership per-forming daily observational audits The new counting anddocumentation policies and guidelines were implemented in allORs at the same time However development of specialty-spe-cific white boards were rolled out one specialty at a time after adetailed analysis of their unique instrumentation needsRandom audits are performed daily for 5 of the cases for eachspecialty by the specialty nurse manager The baseline counttucked item documentation and final counts are audited andcompliance has been 994 or higher for the latest quarter(third quarter 2008) In the event of a miscount compliancewith the established policies and procedures is determined anddocumented by specialty or overall surgical nursing leadershipImportantly all the information and findings are fed back tothe OR team members
The last phase of our effort demonstrated a new resolve byleadership to respond to RFO events Previously these eventswere addressed by the institutional sentinel event (SE) teamoften in isolation and without participation of key surgicalleaders (though these leaders were often invited to participate)The SE effort was often too focused on developing an RCA forthe individual event and did not address the broader culturaland communication issues that exist in the OR environmentNor did this process allow for active monitoring of the ORenvironment to identify the more latent safety issues Finallythe process was slow and the proposed solution to the eventwas often implemented some time after the event All theseissues reflect criticisms of the RCA process1516
To address these concerns a rapid leadership response teamwas formed to address the event within 24ndash36 hours with all
Figure 5 The Red Rules poster displayed in every operating room (OR) pro-vides the two inviolable rules of conduct in the OR The poster informs all staffmembers that adhering to appropriate counting policy is at a level of impor-tance equal to following the Universal Protocol to ensure patient safety
Red Rules Poster
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
130 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
personnel involved The clearly stated purpose of the meetingwas to understand the circumstances of the event and to not bepunitive or assign blame Important to the success of thesemeetings was the involvement of surgical and nursing leader-ship and the development of an open and secure environmentto share the events understand the failures and create plans toshare the lessons learned with all the OR personnel A summa-ry of the event and lessons learned were quickly disseminated ina written memo from the leadership group to all personnel andshared in all areas often within a few days of the event A non-punitive approach to addressing this type of medical error has
been shown to improve staff satisfaction performance andcommunication and to be integral to processes that supportinstitutional crisis management1718
A number of barriers to the success of this initiative wereidentified including poor interaction between the leadership ofthe different stakeholders no standardized institutional ordepartment response to RFO events and poor accountabilityfor addressing the problem of RFOs However the major bar-rier to success was a long-standing culture of poor communica-tion between our OR staff members The tradition of surgeonprimacy in the OR led to a culture lacking in basic communi-
Table 1 Examples of Key Information from Memos to Staff After a Retained Foreign Object (RFO) Event or Near Miss
Brief Description of Event
Near Miss Needle count off
intraoperative film ordered
patient closed because
patient condition before film
was reviewed
Near Miss Needle count off
after exhaustive search in
OR three different intra-op
films taken and needle not
found second exhaustive
search in OR yielded no
needle Patient closed and
survey film revealed needle
A counted-out (after final
pause) sponge was tucked to
protect the abdominal viscera
during closure resulting in a
retained sponge
Argon beam coagulatorrsquos grey
tape (nonndashradio opaque) was
replaced with black tip (radio
opaque) without any notifica-
tion from manufacturer The
tip was not removed and was
retained
Root Causes Identified
Patient condition
Communication gap among
OR staff and radiology
Technology limitation of
intraoperative film vs
survey film
Surgeonrsquos preference for a
particular trochar may or
may not have played a role
Use of sponge in a
nonrecommended fashion
as a viscera retainer
Not following existing cur-
rent policy for final count
and verbalizing tucked items
Communication lapse
between manufacturer and
users
Strengths Identified
Adherence to the
current process
Adherence to the
current process
Appropriate
interventions taken
Survey film of all
patients even when
counts are correct
Survey film of all
patients even when
counts are correct
Opportunities for
Improvement
Radiology process for
RFO rule-out
Communication between
OR staff and radiology
Review of policy for
missing microneedles
(definition process steps
for missing microneedle)
Standardization of
equipment
Training of new fellows and
residents on current best
practices
Communication among
OR staff
While the functionality of
the tape replacement was
improved to make it radio
opaque the change was
not communicated to the
users by the manufacturer
Next Steps Delineated
State in request ldquorule out an
RFOrdquo to expedite review in
less than 30 minutes
Do not move the patient from
OR if patient condition war-
rants to facilitate additional
films to rule out an RFO
Develop policy for
microneedles
Review laparoscopic
equipment available to the
surgical team and their
application to the procedure
being performed
Use rubber viscera retainers
or ldquofishrdquo for viscera retainer
Bag off all counted out
sponges in all specialties
Provide training for all new
residents and fellows
Notify all users throughout
the institution
Remove all mislabeled
equipment from supply
Contact manufacturer and
get issue resolved
Notify FDA
OR operating room FDA Food and Drug Administration
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
131March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
cation skills poor situational awarenessand concern about questioning thecourse of events in the OR This initia-tive helped our organization clarifyissues with our existing processes toavoid RFOs as well as design and imple-ment solutions However the mostimportant benefit was that it highlight-ed the underlying behavior and commu-nication failures between our staffmembers This finding drove the latterhalf of the initiative to focus on teachingand improving team communication
Summary and Conclusions In summary MCR identified the inci-dence of RFOs as a serious quality per-formance issue in the OR To addressthis problem a multidisciplinary leader-ship group was formed that took a sys-tematic evidence-based approach toanalyzing the factors contributing toRFO events Guided by institutionaldata OR leadership engaged the entireOR staff in a broad-based communica-tioneducation program and incorporat-ed system redesign to minimize futureRFOs
The OR environment is complexand manual counting of surgical items isan inherently error-prone process MCRcontinues to perform postoperative sur-vey films for all surgeries in which abody cavity is opened which we believeis the best defense currently available todetect unrecognized RFOs despite all ofour best efforts to improve the intraop-erative processes of counting and docu-mentation We believe that we havereached a performance boundary withour current process and await eitherimplementation of a new technology ora fundamental change in how our entiresurgical process is performed J
Figure 6 The frequency of potential RFO events declined significantly after the initiation of the reduc-tion effort We used a G-Chart which has significantly greater detection power over conventional bino-mial-based approaches particularly for infrequent events and low ldquodefectrdquo rates such as RFOs MCR wasaveraging a surgical RFO every 16 days which was extended to every 69 days as of October 2008
Days Between Potential Retained Foreign Object (RFO)Events January 2003ndashOctober 2008
Figure 7 The defects-per-million-opportunity analysis is shown assuming 25 chances (defect opportuni-ties) per surgical case for an error resulting in a retained foreign object
Defects per Million Opportunities (DPMO) and Sigma LevelMayo Clinic Rochester Minnesota 2003ndash2007
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
132 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
References1 Associated Press Towel Found in Dead Womanrsquos Body CBSNewscomAugust 6 2004 httpwwwcbsnewscomstories20040806healthprintable634558shtml (last accessed Jan 16 2009)2 Sowka MP The medical malpractice closed claims study Conducted bythe National Association of Insurance Commissioners Conn Med45109ndash115 Feb 19813 Gonzales-Ojeda A et al Retained foreign bodies following intra-abdom-inal surgery Hepatogastroenterology 46808ndash812 Mar 19994 Gawande AA et al Risk factors for retained instruments N Engl J Med348229ndash235 Jan 16 20035 Cima RR et al Incidence and characteristics of potential and actualretained foreign object events in surgical patients J Am Coll Surg 20780ndash87Jul 2008 Epub 2008 May 23 20086 Gibbs VC Preventable errors in the operating room Retained foreign bod-
ies after surgeryndashPart I Curr Probl Surg 44281ndash337 May 20077 Leonard M et al The human factor The critical importance of effectiveteamwork and communication Qual Saf Health Care 13(suppl 1)85ndash90Oct 20048 Lingard L et al Communication failures in the operating room Anobservational classification of recurrent types an events Qual Saf Health Care13330ndash334 Oct 20049 Donchin Y et al A look into the nature and causes of human errors in theintensive care unit Qual Saf Health Care 12143ndash147 Apr 200310 AORN Recommended Practices Committee Recommended practices forsponge sharps and instrument counts AORN J 83418 421ndash426 429ndash433Feb 200611 The Joint Commission Universal Protocol httpwwwjointcommissionorgPatientSafetyUniversalProtocol (last accessed Jan 16 2009) 12 Greenberg C et al The frequency and significance of discrepancies in thesurgical count Annal Surg 248337ndash341 Aug 200813 Lukas CV et al Transformational change in health care systems Anorganizational model Health Care Manage Rev 32309ndash320 OctndashDec 200714 Wang MC et al Redesigning health systems for quality Lessons fromemerging practices Jt Comm J Qual Patient Saf 32599ndash611 Nov 200615 Wu AW Lipshutz AK Pronovost PJ Effectiveness and efficiency ofroot cause analysis in medicine JAMA 299685ndash687 Feb 13 2008 16 Reason J Managing the Risks of Organizational Accidents Farnham UKAshgate 199717 Helmrich RL On error management Lessons from aviation BMJ320781ndash785 Mar 18 200018 Marx D Patient Safety and the ldquoJust Culturerdquo A Primer for Health CareExecutives Medical Event Reporting System for Transfusion Medicine Agency forHealthcare Research and Quality 2001 httppsnetahrqgovresourceaspxresourceID=1582 (last accessed Jan 16 2009)
Robert R Cima MD MA is Associate Professor Department of
Surgery Mayo Clinic Rochester Minnesota Anantha
Kollengode PhD MBA is Quality Analyst Quality
Management Services Amy S Storsveen RN BSN is Charge
Nurse and Cheryl A Weisbrod RN MS is Director Surgical
Services Claude Deschamps MD is Professor and Chairman
Department of Surgery Mark B Koch MBA is Associate
Administrator Administrative Services Debra Moore is Nursing
Analyst and Sarah R Pool RN MS is Nursing Educator
Surgical Services Please address correspondence to Robert R
Cima cimarobertmayoedu
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations

129March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
OR and reviews all item seen on the film with the surgeon atwhich time the radiologist is specifically informed of what itemthe team believes is missing Response time for intraoperativeRFO films and adherence to policy were reviewed monthly bythe surgical quality assessment and safety committee to ensurecompliance
The second phase of the program was an intense education-al effort directed at all OR personnel regarding the scope anddetails of the RFO problem at MCR Again this wasapproached in phases The first was the all-staff meeting whichserved many purposes important to the success of this initiative
1 It ensured that all staff (physicians nurses and alliedhealth staff ) in the OR heard a single consistent messageregarding RFOs
2 It demonstrated a unified and engaged leadership team3 It articulated a clear and organized set of policies and pro-
cedures related to RFO reduction and prevention4 It set expected performance standards for all personnel in
the ORAll these elements are known to be essential for the successfulimplementation change within an organization13
Initiated at the same time as the all-staff meeting was anextensive education effort (Conscientious Count Campaign)
This education effort included daily morning report reviews ofthe appropriate and standardized counting protocols reviews ofrelated policies and in-room audits This program served toreinforce the training and performance of all OR personnel onthe standardized approach to counting and responding topotential RFO events Again this protracted education effortwhich stressed improving direct communication between allteam members to improve OR ldquosituational awarenessrdquo hasbeen shown to be one of the most important components forsuccessful institutional change14
The white board served as a tool to standardize documenta-tion of items used and any items that are tucked thus improv-ing the situational awareness of items placed in the surgicalfield Furthermore its use improved communication betweenOR staff members and was a more reliable mechanism thanhaving to rely on the surgical staff rsquos short-term memory It alsohelped in auditing the compliance to the new guidelines of doc-umenting counted and tucked items by nursing leadership per-forming daily observational audits The new counting anddocumentation policies and guidelines were implemented in allORs at the same time However development of specialty-spe-cific white boards were rolled out one specialty at a time after adetailed analysis of their unique instrumentation needsRandom audits are performed daily for 5 of the cases for eachspecialty by the specialty nurse manager The baseline counttucked item documentation and final counts are audited andcompliance has been 994 or higher for the latest quarter(third quarter 2008) In the event of a miscount compliancewith the established policies and procedures is determined anddocumented by specialty or overall surgical nursing leadershipImportantly all the information and findings are fed back tothe OR team members
The last phase of our effort demonstrated a new resolve byleadership to respond to RFO events Previously these eventswere addressed by the institutional sentinel event (SE) teamoften in isolation and without participation of key surgicalleaders (though these leaders were often invited to participate)The SE effort was often too focused on developing an RCA forthe individual event and did not address the broader culturaland communication issues that exist in the OR environmentNor did this process allow for active monitoring of the ORenvironment to identify the more latent safety issues Finallythe process was slow and the proposed solution to the eventwas often implemented some time after the event All theseissues reflect criticisms of the RCA process1516
To address these concerns a rapid leadership response teamwas formed to address the event within 24ndash36 hours with all
Figure 5 The Red Rules poster displayed in every operating room (OR) pro-vides the two inviolable rules of conduct in the OR The poster informs all staffmembers that adhering to appropriate counting policy is at a level of impor-tance equal to following the Universal Protocol to ensure patient safety
Red Rules Poster
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
130 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
personnel involved The clearly stated purpose of the meetingwas to understand the circumstances of the event and to not bepunitive or assign blame Important to the success of thesemeetings was the involvement of surgical and nursing leader-ship and the development of an open and secure environmentto share the events understand the failures and create plans toshare the lessons learned with all the OR personnel A summa-ry of the event and lessons learned were quickly disseminated ina written memo from the leadership group to all personnel andshared in all areas often within a few days of the event A non-punitive approach to addressing this type of medical error has
been shown to improve staff satisfaction performance andcommunication and to be integral to processes that supportinstitutional crisis management1718
A number of barriers to the success of this initiative wereidentified including poor interaction between the leadership ofthe different stakeholders no standardized institutional ordepartment response to RFO events and poor accountabilityfor addressing the problem of RFOs However the major bar-rier to success was a long-standing culture of poor communica-tion between our OR staff members The tradition of surgeonprimacy in the OR led to a culture lacking in basic communi-
Table 1 Examples of Key Information from Memos to Staff After a Retained Foreign Object (RFO) Event or Near Miss
Brief Description of Event
Near Miss Needle count off
intraoperative film ordered
patient closed because
patient condition before film
was reviewed
Near Miss Needle count off
after exhaustive search in
OR three different intra-op
films taken and needle not
found second exhaustive
search in OR yielded no
needle Patient closed and
survey film revealed needle
A counted-out (after final
pause) sponge was tucked to
protect the abdominal viscera
during closure resulting in a
retained sponge
Argon beam coagulatorrsquos grey
tape (nonndashradio opaque) was
replaced with black tip (radio
opaque) without any notifica-
tion from manufacturer The
tip was not removed and was
retained
Root Causes Identified
Patient condition
Communication gap among
OR staff and radiology
Technology limitation of
intraoperative film vs
survey film
Surgeonrsquos preference for a
particular trochar may or
may not have played a role
Use of sponge in a
nonrecommended fashion
as a viscera retainer
Not following existing cur-
rent policy for final count
and verbalizing tucked items
Communication lapse
between manufacturer and
users
Strengths Identified
Adherence to the
current process
Adherence to the
current process
Appropriate
interventions taken
Survey film of all
patients even when
counts are correct
Survey film of all
patients even when
counts are correct
Opportunities for
Improvement
Radiology process for
RFO rule-out
Communication between
OR staff and radiology
Review of policy for
missing microneedles
(definition process steps
for missing microneedle)
Standardization of
equipment
Training of new fellows and
residents on current best
practices
Communication among
OR staff
While the functionality of
the tape replacement was
improved to make it radio
opaque the change was
not communicated to the
users by the manufacturer
Next Steps Delineated
State in request ldquorule out an
RFOrdquo to expedite review in
less than 30 minutes
Do not move the patient from
OR if patient condition war-
rants to facilitate additional
films to rule out an RFO
Develop policy for
microneedles
Review laparoscopic
equipment available to the
surgical team and their
application to the procedure
being performed
Use rubber viscera retainers
or ldquofishrdquo for viscera retainer
Bag off all counted out
sponges in all specialties
Provide training for all new
residents and fellows
Notify all users throughout
the institution
Remove all mislabeled
equipment from supply
Contact manufacturer and
get issue resolved
Notify FDA
OR operating room FDA Food and Drug Administration
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
131March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
cation skills poor situational awarenessand concern about questioning thecourse of events in the OR This initia-tive helped our organization clarifyissues with our existing processes toavoid RFOs as well as design and imple-ment solutions However the mostimportant benefit was that it highlight-ed the underlying behavior and commu-nication failures between our staffmembers This finding drove the latterhalf of the initiative to focus on teachingand improving team communication
Summary and Conclusions In summary MCR identified the inci-dence of RFOs as a serious quality per-formance issue in the OR To addressthis problem a multidisciplinary leader-ship group was formed that took a sys-tematic evidence-based approach toanalyzing the factors contributing toRFO events Guided by institutionaldata OR leadership engaged the entireOR staff in a broad-based communica-tioneducation program and incorporat-ed system redesign to minimize futureRFOs
The OR environment is complexand manual counting of surgical items isan inherently error-prone process MCRcontinues to perform postoperative sur-vey films for all surgeries in which abody cavity is opened which we believeis the best defense currently available todetect unrecognized RFOs despite all ofour best efforts to improve the intraop-erative processes of counting and docu-mentation We believe that we havereached a performance boundary withour current process and await eitherimplementation of a new technology ora fundamental change in how our entiresurgical process is performed J
Figure 6 The frequency of potential RFO events declined significantly after the initiation of the reduc-tion effort We used a G-Chart which has significantly greater detection power over conventional bino-mial-based approaches particularly for infrequent events and low ldquodefectrdquo rates such as RFOs MCR wasaveraging a surgical RFO every 16 days which was extended to every 69 days as of October 2008
Days Between Potential Retained Foreign Object (RFO)Events January 2003ndashOctober 2008
Figure 7 The defects-per-million-opportunity analysis is shown assuming 25 chances (defect opportuni-ties) per surgical case for an error resulting in a retained foreign object
Defects per Million Opportunities (DPMO) and Sigma LevelMayo Clinic Rochester Minnesota 2003ndash2007
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
132 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
References1 Associated Press Towel Found in Dead Womanrsquos Body CBSNewscomAugust 6 2004 httpwwwcbsnewscomstories20040806healthprintable634558shtml (last accessed Jan 16 2009)2 Sowka MP The medical malpractice closed claims study Conducted bythe National Association of Insurance Commissioners Conn Med45109ndash115 Feb 19813 Gonzales-Ojeda A et al Retained foreign bodies following intra-abdom-inal surgery Hepatogastroenterology 46808ndash812 Mar 19994 Gawande AA et al Risk factors for retained instruments N Engl J Med348229ndash235 Jan 16 20035 Cima RR et al Incidence and characteristics of potential and actualretained foreign object events in surgical patients J Am Coll Surg 20780ndash87Jul 2008 Epub 2008 May 23 20086 Gibbs VC Preventable errors in the operating room Retained foreign bod-
ies after surgeryndashPart I Curr Probl Surg 44281ndash337 May 20077 Leonard M et al The human factor The critical importance of effectiveteamwork and communication Qual Saf Health Care 13(suppl 1)85ndash90Oct 20048 Lingard L et al Communication failures in the operating room Anobservational classification of recurrent types an events Qual Saf Health Care13330ndash334 Oct 20049 Donchin Y et al A look into the nature and causes of human errors in theintensive care unit Qual Saf Health Care 12143ndash147 Apr 200310 AORN Recommended Practices Committee Recommended practices forsponge sharps and instrument counts AORN J 83418 421ndash426 429ndash433Feb 200611 The Joint Commission Universal Protocol httpwwwjointcommissionorgPatientSafetyUniversalProtocol (last accessed Jan 16 2009) 12 Greenberg C et al The frequency and significance of discrepancies in thesurgical count Annal Surg 248337ndash341 Aug 200813 Lukas CV et al Transformational change in health care systems Anorganizational model Health Care Manage Rev 32309ndash320 OctndashDec 200714 Wang MC et al Redesigning health systems for quality Lessons fromemerging practices Jt Comm J Qual Patient Saf 32599ndash611 Nov 200615 Wu AW Lipshutz AK Pronovost PJ Effectiveness and efficiency ofroot cause analysis in medicine JAMA 299685ndash687 Feb 13 2008 16 Reason J Managing the Risks of Organizational Accidents Farnham UKAshgate 199717 Helmrich RL On error management Lessons from aviation BMJ320781ndash785 Mar 18 200018 Marx D Patient Safety and the ldquoJust Culturerdquo A Primer for Health CareExecutives Medical Event Reporting System for Transfusion Medicine Agency forHealthcare Research and Quality 2001 httppsnetahrqgovresourceaspxresourceID=1582 (last accessed Jan 16 2009)
Robert R Cima MD MA is Associate Professor Department of
Surgery Mayo Clinic Rochester Minnesota Anantha
Kollengode PhD MBA is Quality Analyst Quality
Management Services Amy S Storsveen RN BSN is Charge
Nurse and Cheryl A Weisbrod RN MS is Director Surgical
Services Claude Deschamps MD is Professor and Chairman
Department of Surgery Mark B Koch MBA is Associate
Administrator Administrative Services Debra Moore is Nursing
Analyst and Sarah R Pool RN MS is Nursing Educator
Surgical Services Please address correspondence to Robert R
Cima cimarobertmayoedu
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations

130 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
personnel involved The clearly stated purpose of the meetingwas to understand the circumstances of the event and to not bepunitive or assign blame Important to the success of thesemeetings was the involvement of surgical and nursing leader-ship and the development of an open and secure environmentto share the events understand the failures and create plans toshare the lessons learned with all the OR personnel A summa-ry of the event and lessons learned were quickly disseminated ina written memo from the leadership group to all personnel andshared in all areas often within a few days of the event A non-punitive approach to addressing this type of medical error has
been shown to improve staff satisfaction performance andcommunication and to be integral to processes that supportinstitutional crisis management1718
A number of barriers to the success of this initiative wereidentified including poor interaction between the leadership ofthe different stakeholders no standardized institutional ordepartment response to RFO events and poor accountabilityfor addressing the problem of RFOs However the major bar-rier to success was a long-standing culture of poor communica-tion between our OR staff members The tradition of surgeonprimacy in the OR led to a culture lacking in basic communi-
Table 1 Examples of Key Information from Memos to Staff After a Retained Foreign Object (RFO) Event or Near Miss
Brief Description of Event
Near Miss Needle count off
intraoperative film ordered
patient closed because
patient condition before film
was reviewed
Near Miss Needle count off
after exhaustive search in
OR three different intra-op
films taken and needle not
found second exhaustive
search in OR yielded no
needle Patient closed and
survey film revealed needle
A counted-out (after final
pause) sponge was tucked to
protect the abdominal viscera
during closure resulting in a
retained sponge
Argon beam coagulatorrsquos grey
tape (nonndashradio opaque) was
replaced with black tip (radio
opaque) without any notifica-
tion from manufacturer The
tip was not removed and was
retained
Root Causes Identified
Patient condition
Communication gap among
OR staff and radiology
Technology limitation of
intraoperative film vs
survey film
Surgeonrsquos preference for a
particular trochar may or
may not have played a role
Use of sponge in a
nonrecommended fashion
as a viscera retainer
Not following existing cur-
rent policy for final count
and verbalizing tucked items
Communication lapse
between manufacturer and
users
Strengths Identified
Adherence to the
current process
Adherence to the
current process
Appropriate
interventions taken
Survey film of all
patients even when
counts are correct
Survey film of all
patients even when
counts are correct
Opportunities for
Improvement
Radiology process for
RFO rule-out
Communication between
OR staff and radiology
Review of policy for
missing microneedles
(definition process steps
for missing microneedle)
Standardization of
equipment
Training of new fellows and
residents on current best
practices
Communication among
OR staff
While the functionality of
the tape replacement was
improved to make it radio
opaque the change was
not communicated to the
users by the manufacturer
Next Steps Delineated
State in request ldquorule out an
RFOrdquo to expedite review in
less than 30 minutes
Do not move the patient from
OR if patient condition war-
rants to facilitate additional
films to rule out an RFO
Develop policy for
microneedles
Review laparoscopic
equipment available to the
surgical team and their
application to the procedure
being performed
Use rubber viscera retainers
or ldquofishrdquo for viscera retainer
Bag off all counted out
sponges in all specialties
Provide training for all new
residents and fellows
Notify all users throughout
the institution
Remove all mislabeled
equipment from supply
Contact manufacturer and
get issue resolved
Notify FDA
OR operating room FDA Food and Drug Administration
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
131March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
cation skills poor situational awarenessand concern about questioning thecourse of events in the OR This initia-tive helped our organization clarifyissues with our existing processes toavoid RFOs as well as design and imple-ment solutions However the mostimportant benefit was that it highlight-ed the underlying behavior and commu-nication failures between our staffmembers This finding drove the latterhalf of the initiative to focus on teachingand improving team communication
Summary and Conclusions In summary MCR identified the inci-dence of RFOs as a serious quality per-formance issue in the OR To addressthis problem a multidisciplinary leader-ship group was formed that took a sys-tematic evidence-based approach toanalyzing the factors contributing toRFO events Guided by institutionaldata OR leadership engaged the entireOR staff in a broad-based communica-tioneducation program and incorporat-ed system redesign to minimize futureRFOs
The OR environment is complexand manual counting of surgical items isan inherently error-prone process MCRcontinues to perform postoperative sur-vey films for all surgeries in which abody cavity is opened which we believeis the best defense currently available todetect unrecognized RFOs despite all ofour best efforts to improve the intraop-erative processes of counting and docu-mentation We believe that we havereached a performance boundary withour current process and await eitherimplementation of a new technology ora fundamental change in how our entiresurgical process is performed J
Figure 6 The frequency of potential RFO events declined significantly after the initiation of the reduc-tion effort We used a G-Chart which has significantly greater detection power over conventional bino-mial-based approaches particularly for infrequent events and low ldquodefectrdquo rates such as RFOs MCR wasaveraging a surgical RFO every 16 days which was extended to every 69 days as of October 2008
Days Between Potential Retained Foreign Object (RFO)Events January 2003ndashOctober 2008
Figure 7 The defects-per-million-opportunity analysis is shown assuming 25 chances (defect opportuni-ties) per surgical case for an error resulting in a retained foreign object
Defects per Million Opportunities (DPMO) and Sigma LevelMayo Clinic Rochester Minnesota 2003ndash2007
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
132 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
References1 Associated Press Towel Found in Dead Womanrsquos Body CBSNewscomAugust 6 2004 httpwwwcbsnewscomstories20040806healthprintable634558shtml (last accessed Jan 16 2009)2 Sowka MP The medical malpractice closed claims study Conducted bythe National Association of Insurance Commissioners Conn Med45109ndash115 Feb 19813 Gonzales-Ojeda A et al Retained foreign bodies following intra-abdom-inal surgery Hepatogastroenterology 46808ndash812 Mar 19994 Gawande AA et al Risk factors for retained instruments N Engl J Med348229ndash235 Jan 16 20035 Cima RR et al Incidence and characteristics of potential and actualretained foreign object events in surgical patients J Am Coll Surg 20780ndash87Jul 2008 Epub 2008 May 23 20086 Gibbs VC Preventable errors in the operating room Retained foreign bod-
ies after surgeryndashPart I Curr Probl Surg 44281ndash337 May 20077 Leonard M et al The human factor The critical importance of effectiveteamwork and communication Qual Saf Health Care 13(suppl 1)85ndash90Oct 20048 Lingard L et al Communication failures in the operating room Anobservational classification of recurrent types an events Qual Saf Health Care13330ndash334 Oct 20049 Donchin Y et al A look into the nature and causes of human errors in theintensive care unit Qual Saf Health Care 12143ndash147 Apr 200310 AORN Recommended Practices Committee Recommended practices forsponge sharps and instrument counts AORN J 83418 421ndash426 429ndash433Feb 200611 The Joint Commission Universal Protocol httpwwwjointcommissionorgPatientSafetyUniversalProtocol (last accessed Jan 16 2009) 12 Greenberg C et al The frequency and significance of discrepancies in thesurgical count Annal Surg 248337ndash341 Aug 200813 Lukas CV et al Transformational change in health care systems Anorganizational model Health Care Manage Rev 32309ndash320 OctndashDec 200714 Wang MC et al Redesigning health systems for quality Lessons fromemerging practices Jt Comm J Qual Patient Saf 32599ndash611 Nov 200615 Wu AW Lipshutz AK Pronovost PJ Effectiveness and efficiency ofroot cause analysis in medicine JAMA 299685ndash687 Feb 13 2008 16 Reason J Managing the Risks of Organizational Accidents Farnham UKAshgate 199717 Helmrich RL On error management Lessons from aviation BMJ320781ndash785 Mar 18 200018 Marx D Patient Safety and the ldquoJust Culturerdquo A Primer for Health CareExecutives Medical Event Reporting System for Transfusion Medicine Agency forHealthcare Research and Quality 2001 httppsnetahrqgovresourceaspxresourceID=1582 (last accessed Jan 16 2009)
Robert R Cima MD MA is Associate Professor Department of
Surgery Mayo Clinic Rochester Minnesota Anantha
Kollengode PhD MBA is Quality Analyst Quality
Management Services Amy S Storsveen RN BSN is Charge
Nurse and Cheryl A Weisbrod RN MS is Director Surgical
Services Claude Deschamps MD is Professor and Chairman
Department of Surgery Mark B Koch MBA is Associate
Administrator Administrative Services Debra Moore is Nursing
Analyst and Sarah R Pool RN MS is Nursing Educator
Surgical Services Please address correspondence to Robert R
Cima cimarobertmayoedu
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
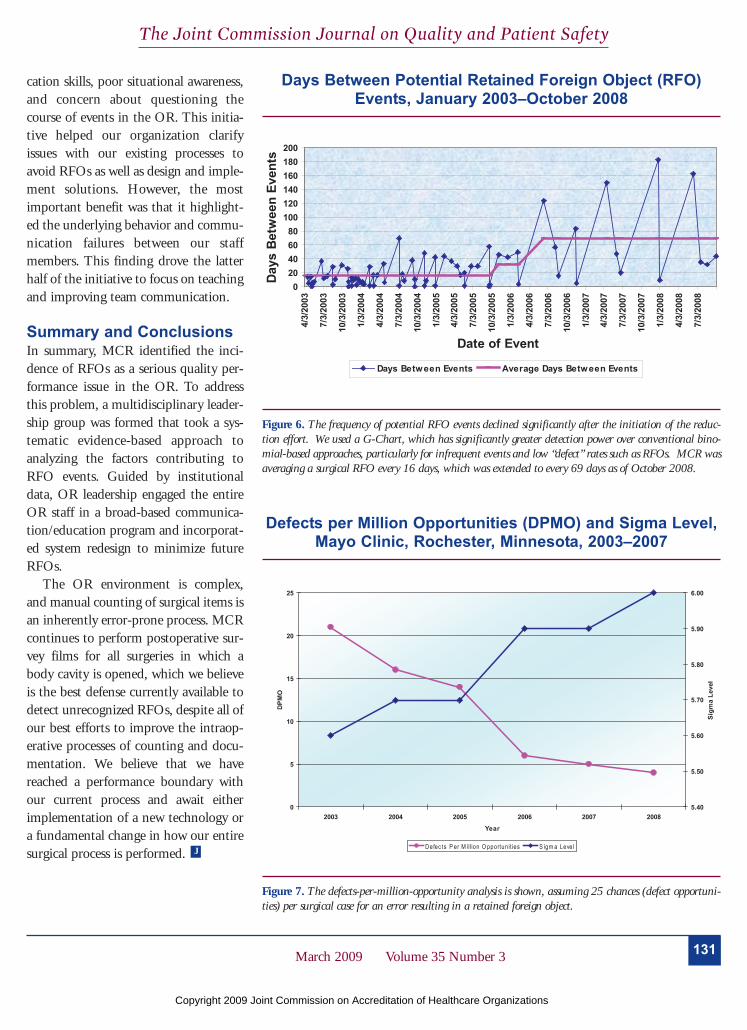
131March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
cation skills poor situational awarenessand concern about questioning thecourse of events in the OR This initia-tive helped our organization clarifyissues with our existing processes toavoid RFOs as well as design and imple-ment solutions However the mostimportant benefit was that it highlight-ed the underlying behavior and commu-nication failures between our staffmembers This finding drove the latterhalf of the initiative to focus on teachingand improving team communication
Summary and Conclusions In summary MCR identified the inci-dence of RFOs as a serious quality per-formance issue in the OR To addressthis problem a multidisciplinary leader-ship group was formed that took a sys-tematic evidence-based approach toanalyzing the factors contributing toRFO events Guided by institutionaldata OR leadership engaged the entireOR staff in a broad-based communica-tioneducation program and incorporat-ed system redesign to minimize futureRFOs
The OR environment is complexand manual counting of surgical items isan inherently error-prone process MCRcontinues to perform postoperative sur-vey films for all surgeries in which abody cavity is opened which we believeis the best defense currently available todetect unrecognized RFOs despite all ofour best efforts to improve the intraop-erative processes of counting and docu-mentation We believe that we havereached a performance boundary withour current process and await eitherimplementation of a new technology ora fundamental change in how our entiresurgical process is performed J
Figure 6 The frequency of potential RFO events declined significantly after the initiation of the reduc-tion effort We used a G-Chart which has significantly greater detection power over conventional bino-mial-based approaches particularly for infrequent events and low ldquodefectrdquo rates such as RFOs MCR wasaveraging a surgical RFO every 16 days which was extended to every 69 days as of October 2008
Days Between Potential Retained Foreign Object (RFO)Events January 2003ndashOctober 2008
Figure 7 The defects-per-million-opportunity analysis is shown assuming 25 chances (defect opportuni-ties) per surgical case for an error resulting in a retained foreign object
Defects per Million Opportunities (DPMO) and Sigma LevelMayo Clinic Rochester Minnesota 2003ndash2007
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations
132 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
References1 Associated Press Towel Found in Dead Womanrsquos Body CBSNewscomAugust 6 2004 httpwwwcbsnewscomstories20040806healthprintable634558shtml (last accessed Jan 16 2009)2 Sowka MP The medical malpractice closed claims study Conducted bythe National Association of Insurance Commissioners Conn Med45109ndash115 Feb 19813 Gonzales-Ojeda A et al Retained foreign bodies following intra-abdom-inal surgery Hepatogastroenterology 46808ndash812 Mar 19994 Gawande AA et al Risk factors for retained instruments N Engl J Med348229ndash235 Jan 16 20035 Cima RR et al Incidence and characteristics of potential and actualretained foreign object events in surgical patients J Am Coll Surg 20780ndash87Jul 2008 Epub 2008 May 23 20086 Gibbs VC Preventable errors in the operating room Retained foreign bod-
ies after surgeryndashPart I Curr Probl Surg 44281ndash337 May 20077 Leonard M et al The human factor The critical importance of effectiveteamwork and communication Qual Saf Health Care 13(suppl 1)85ndash90Oct 20048 Lingard L et al Communication failures in the operating room Anobservational classification of recurrent types an events Qual Saf Health Care13330ndash334 Oct 20049 Donchin Y et al A look into the nature and causes of human errors in theintensive care unit Qual Saf Health Care 12143ndash147 Apr 200310 AORN Recommended Practices Committee Recommended practices forsponge sharps and instrument counts AORN J 83418 421ndash426 429ndash433Feb 200611 The Joint Commission Universal Protocol httpwwwjointcommissionorgPatientSafetyUniversalProtocol (last accessed Jan 16 2009) 12 Greenberg C et al The frequency and significance of discrepancies in thesurgical count Annal Surg 248337ndash341 Aug 200813 Lukas CV et al Transformational change in health care systems Anorganizational model Health Care Manage Rev 32309ndash320 OctndashDec 200714 Wang MC et al Redesigning health systems for quality Lessons fromemerging practices Jt Comm J Qual Patient Saf 32599ndash611 Nov 200615 Wu AW Lipshutz AK Pronovost PJ Effectiveness and efficiency ofroot cause analysis in medicine JAMA 299685ndash687 Feb 13 2008 16 Reason J Managing the Risks of Organizational Accidents Farnham UKAshgate 199717 Helmrich RL On error management Lessons from aviation BMJ320781ndash785 Mar 18 200018 Marx D Patient Safety and the ldquoJust Culturerdquo A Primer for Health CareExecutives Medical Event Reporting System for Transfusion Medicine Agency forHealthcare Research and Quality 2001 httppsnetahrqgovresourceaspxresourceID=1582 (last accessed Jan 16 2009)
Robert R Cima MD MA is Associate Professor Department of
Surgery Mayo Clinic Rochester Minnesota Anantha
Kollengode PhD MBA is Quality Analyst Quality
Management Services Amy S Storsveen RN BSN is Charge
Nurse and Cheryl A Weisbrod RN MS is Director Surgical
Services Claude Deschamps MD is Professor and Chairman
Department of Surgery Mark B Koch MBA is Associate
Administrator Administrative Services Debra Moore is Nursing
Analyst and Sarah R Pool RN MS is Nursing Educator
Surgical Services Please address correspondence to Robert R
Cima cimarobertmayoedu
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations

132 March 2009 Volume 35 Number 3
The Joint Commission Journal on Quality and Patient Safety
References1 Associated Press Towel Found in Dead Womanrsquos Body CBSNewscomAugust 6 2004 httpwwwcbsnewscomstories20040806healthprintable634558shtml (last accessed Jan 16 2009)2 Sowka MP The medical malpractice closed claims study Conducted bythe National Association of Insurance Commissioners Conn Med45109ndash115 Feb 19813 Gonzales-Ojeda A et al Retained foreign bodies following intra-abdom-inal surgery Hepatogastroenterology 46808ndash812 Mar 19994 Gawande AA et al Risk factors for retained instruments N Engl J Med348229ndash235 Jan 16 20035 Cima RR et al Incidence and characteristics of potential and actualretained foreign object events in surgical patients J Am Coll Surg 20780ndash87Jul 2008 Epub 2008 May 23 20086 Gibbs VC Preventable errors in the operating room Retained foreign bod-
ies after surgeryndashPart I Curr Probl Surg 44281ndash337 May 20077 Leonard M et al The human factor The critical importance of effectiveteamwork and communication Qual Saf Health Care 13(suppl 1)85ndash90Oct 20048 Lingard L et al Communication failures in the operating room Anobservational classification of recurrent types an events Qual Saf Health Care13330ndash334 Oct 20049 Donchin Y et al A look into the nature and causes of human errors in theintensive care unit Qual Saf Health Care 12143ndash147 Apr 200310 AORN Recommended Practices Committee Recommended practices forsponge sharps and instrument counts AORN J 83418 421ndash426 429ndash433Feb 200611 The Joint Commission Universal Protocol httpwwwjointcommissionorgPatientSafetyUniversalProtocol (last accessed Jan 16 2009) 12 Greenberg C et al The frequency and significance of discrepancies in thesurgical count Annal Surg 248337ndash341 Aug 200813 Lukas CV et al Transformational change in health care systems Anorganizational model Health Care Manage Rev 32309ndash320 OctndashDec 200714 Wang MC et al Redesigning health systems for quality Lessons fromemerging practices Jt Comm J Qual Patient Saf 32599ndash611 Nov 200615 Wu AW Lipshutz AK Pronovost PJ Effectiveness and efficiency ofroot cause analysis in medicine JAMA 299685ndash687 Feb 13 2008 16 Reason J Managing the Risks of Organizational Accidents Farnham UKAshgate 199717 Helmrich RL On error management Lessons from aviation BMJ320781ndash785 Mar 18 200018 Marx D Patient Safety and the ldquoJust Culturerdquo A Primer for Health CareExecutives Medical Event Reporting System for Transfusion Medicine Agency forHealthcare Research and Quality 2001 httppsnetahrqgovresourceaspxresourceID=1582 (last accessed Jan 16 2009)
Robert R Cima MD MA is Associate Professor Department of
Surgery Mayo Clinic Rochester Minnesota Anantha
Kollengode PhD MBA is Quality Analyst Quality
Management Services Amy S Storsveen RN BSN is Charge
Nurse and Cheryl A Weisbrod RN MS is Director Surgical
Services Claude Deschamps MD is Professor and Chairman
Department of Surgery Mark B Koch MBA is Associate
Administrator Administrative Services Debra Moore is Nursing
Analyst and Sarah R Pool RN MS is Nursing Educator
Surgical Services Please address correspondence to Robert R
Cima cimarobertmayoedu
Copyright 2009 Joint Commission on Accreditation of Healthcare Organizations