penicillin in dentistry (antibiotics) - by shefali jain
TRANSCRIPT


INTRODUCTION
Greek word
Anti - against
Bios - life
Antibiotics are substances produced by microorganisms, which suppress the growth of or kill other microorganisms at very low concentrations
(K.D Tripathi- 5TH Edition)
Antibiotics are chemical substances produced by microorganisms having the property of inhibiting the growth or destroying other microorganisms in high dilution
(by Waksman)

HISTORY OF
ANTIBIOTICS
PERIOD OF
EMPERICAL
USE
EHRLICH”S
PHASE
of dye and
organometallic
compound
MODERN ERA.

PERIOD OF EMPERICAL
USE
In 17th and 18th century, there were no proper treatment
for diseases.
Chinese use plant and moulds to treat infected
wounds.
In india,Chalmugra oil is used to treat leprosy.
Chinchona bark for fever.
Egyptian use honey + lint used for dressing wound.

EHRLICH’S PHASE
OF DYE AND ORGANOMETALLIC COMPOUND
Ehrlich toyed with idea that if certain dyes could
selectively stain microbes ,they could selectively
toxic to these organism,tried methylene
blue,trypan red etc.
He developed arsenicals-Atoxyl for sleeping
sickness, Arsphenamine for syphilis.

MODERN ERA.
In 1935, Domagk demostrate the
therapeutic effect of Prontosil,
a sulfonamide dye, in pyogenic infection.
Sulfapyridine was first sulfonamide to be
marketed in 1938
Gerhard Domagk

Penicillin was discovered by chance in
1928
Flemings (1929) found that a diffusablesubstance was elaborated by Penicillium mould which destroy staphylococcus on culture plate.
He named this substance PENICILLIN but could not purify it.
Alexander Fleming

In the 1940s Waksman and his
colleagues undertook a systematic
search of Actinomycetes as a source
of antibiotics and discovered Streptomycin in 1944.
All three groups of scientists Domagk,Fleming -chain- Florey and Waksman recieved Nobel Prize for their discoveries.
Selman Waksman

1948- chlortetracycline
In 1957- Nystatin
In 1970- new 4 Quinolones
In 1980- Norfloxacin
In 1998- Smithkine beecham patented
Amoxicillin/clavunate potassium tablets .

CLASSIFICATION…DEPENDING ON CHEMICAL STRUCTURE
1.Sulfonamides and related drugs ( dapsone)2.Diaminopyrimidines( trimethoprim)3.Quinolone ( norfloxacin, ciprofloxacin)4.β-lactum antibiotics ( penicillin, cephalosporin)
5.Tetracyclines ( doxcycycline)6. Nitrobenzene derivative ( chloramphenicol)7. Aminoglycosides ( gentamycin, neomycin)8. Macrolide antibiotics ( erythromycin,Azithromycin)9. Polypeptide antibiotics ( polymyxin- B)
10.Nitrofuran derivatives (furazolidine)
11.Nitroimidazoles (metronidazole)
12. Polyene antibiotics (nystatin, Amphoterin–B)

DEPENDING ON
MECHANISM OF ACTION

TYPE OF ORGANISMS
AGAINST WHICH PRIMARILY
ACTIVEa) Antibacterial- penicillin, Aminoglycosides
b) Antifungal- Griseofulvin, Amphotericin B etc
c) Antiviral- Acyclovir, Zidovudine
d) Antiprotozoal- Chloroquine, metronidazole.
e) Anthelmintic- Niclosamide, Mebendazole.

SPECTRUM OF ACTIVITY
a) Narrow Spectrum – Penicillin–G, Streptomycin, Erythromycin
b) Broad Spectrum - Tetracycline , Chloramphenicol.
TYPE OF ACTION
a) Primarily Bacteriostatic- Sulfonamide, Tetracycline.
b) Primarily Bactericidal- Penicillin, Cephalosporin.
SOURCE OF ANTIBIOTICS
a) Fungi- Penicillin, Griseflovin
b) Bacteria- polymyxin B, Bacitracin
c) Actinomycetes- Aminoglycosides, Macrolides.

SELECTION OF ANTIMICROBIAL
AGENTPateint factor
• Age
• Renal and hepatic function.
• Local factor.
• Drug allergy.
• Imapired host defence.
• Pregnancy
Organism related factor
• Bacteriological sensitivity testing.
• Minimum inhibitory concentration,
• Minimum bactericidal concentration.
• Postantibiotic effect
Drug factor
• Spectrum of activity.
• Type of activity.
• Sensitvity of the organism
• Relative toxicity
• Pharmokinetic profile
• Route of
administration.

IDENTIFICATION OF CAUSATIVE ORGANISM
ANAEROBIC
BACTERIAAEROBIC BACTERIA
Gram-
positive
cocci
Gram-
negative
bacilli
Gram-
positive
cocci
Gram
negative
bacilli
sterptococcsstaphylococc
s
Viridians
b-hemolytics
Haemophilus influenzae
Escheria coli
Klebsiella
Eikenella corroden
streptococcus
Porphyromonas
Fusobacteria
provetella

ORGANISMS RESPONSIBLE FOR APICAL
ABSCESS
1. Streptococci species
2. Streptococci intermedius
3. Streptococci angiosus
4. Streptococci constellatus
5. Bacteroides species

ORGANISMS RESPONSIBLE FOR
PERIODONTAL DISEASE
1. Porphyromonas gingivalis
2. Actinobacillus actinomycetecomitans
3. Borrelia vicenti
4. Prevotella intermedia
5. Fusobacterium
(Mainly gram negative bacteria)

ORGANISMS RESPONSIBLE FOR
DENTAL CARIES
1. Strep. Mutans group
2. Strep. Salivarius
3. Actinomyces species
4. Lactobacilli

Aerobic bacteria plays an important role in theorigin of odontogenic infections.
Anaerobic gram-positive cocci are seen 1/3 of allodontogenic infections.
Gram-negative rods comprises of 50% ofodontogenic infections.

ORGANISM RELATED FACTORS
Clinical diagnosis
Bacteriologic examination
20
Cont…

Minimum Inhibitory Concentration (MIC)
21
MIC- The lowest concentration of an
antibiotic which prevent visible growth of a
bacterium determined in microwell culture
plate
FOR THERAPEUTIC PURPOSES :-
1. Peak concentration of antibiotics
should be three to four times of the
MIC.
2. Therefore the dosage prescribed
must be capable of establishing a
concentration of three to four times the
MIC.

Minimum bactericidal Concentration (MBC)
22
MBC- of antibiotics is determined by
subculturing
from tubes with no visible growth
A small difference between MIC and
MBC indicate
antibodies is primary bacteriocidal,
Large difference indicate bacteriostatic
action.
If sufficient drug is not given to reach
therapeutic levels, sub therapeutic levels
may mask the infection without killing the
microbes.

DRUG FACTORS
Spectrum of activity
Type of activity
Sensitivity of organism
Relative toxicity
Route of administration
Evidence of clinical efficacy
Cost
Pharmacokinetic profile23
Cont…

SPECTRUM ANTIBIOTIC
Narrowest antibacterial spectrum should be
chosen.
1. It minimizes the risk of superinfection.
2. Broad-spectrum antibiotic develop resistant against many
bacteria.
3. Use of narrow-spectrum antibiotics allow larger
proportion of the host flora to be maintained, by reducing
superinfection to minimum.

Type of activity
Use of bactericidal rather than a bacterostatic drug .
Bactericidal drugs are used for patients who are pathologically
immuosuppresed.
Bacterostatic they inhibit growth and reproduction of bacteria by inhibiting
protein synthesis.
Bactericidal they penetrate into bacterial cell and kill them.

Why we use bactericidal drug ?
1. Host resistance
2. Destroying microbes by antibiotic itself
3. Better than bacterostatic drugs
4. Greater flexibility in dosage

Eg:-
Bactericidal drugs such as penicillin or cephalosporin
should be used in immunodeficient patients instead of
bacteriostatic drugs, erythromycin or clindamycin.
If bacteriostatic drugs are given then bacteria in
immunocompromised patients will not be killed and
there will be chances for them to develop resistance.

PROPER TIME INTERVAL
Frequency of dosing is very important.
Each drug has its specific plasma half-life (t1/2), during
which one half of the absorbed dose is absorbed.
Usual and divided dosages is maintained.

PROPER ROUTE OF ADMINISTRATION
Drugs can be administered by variety of
routes but its choice depends on both drugs
as well as patient related factors.
Routes divided into:-
1. Local routes
2. Systemic routes

USE OF LEAST TOXIC ANTIBIOTIC
• Antibiotics are used for killing living bacteria but some
antibiotics kill bacteria's existing in normal flora and
thus are highly toxic.
Less toxic drug must be used which are equally
effective.

Eg:-
Bacteria which cause odontogenic infections areusually sensitive to penicillin and chloramphenicolHence, penicillin is preferable because of lowertoxicity.
• Second choice of drug.
1) Clindamycin
2) Erythromycin

COMBINED USE OF
ANTIBIOTICS Synergism
Reduction in adverse effects
Prevents emergence of resistance
Broadens the spectrum antimicrobial action
32
DISADVANTAGES
Casual outlook
Increased chances of superinfections
Emergence of resistance
Increased cost of therapy

PENICILLIN

History
1928 - Alexander Fleming
Bread mold (Penicillium notatum) growing on
petri dish
1939 - Florey, Chain, and Associates
Began work on isolating and synthesizing large
amounts of Penicillin.
1941 – introduced in antibacterial therapy

PENICILLINS
Beta- lactam antibiotics
Narrow spectrum antibiotics
Bactericidal
These have the greatest activity against gram-positive organisms, gram-negative cocci, and non- lactamase-producing anaerobes. However, they have little activity against gram-negative rods.
They are susceptible to hydrolysis by lactamases.
35
STRUCTURE

The penicillins are classified as -lactam drugs because of their unique four-
membered lactam ring.
All penicillins have the basic structure shown A thiazolidine ring (A) is attached
to a -lactam ring (B) that carries a secondary amino group (RNH–). can be
attached to the amino group.
Structural integrity of the 6-aminopenicillanic acid nucleus is essential for the
biologic activity of these compounds.
If the -lactam ring is enzymatically cleaved by bacterial -lactamases, the
resulting product, penicilloic acid, lacks antibacterial activity.

PENICILLINS
Natural Semi synthetic
38

CELL WALL SYNTHESIS IN
BACTERIA. The first stage, precursor formation, takes place in the cytoplasm. The
product, uridine diphosphate (UDP)- acetylmuramyl-pentapeptide, called a “Park nucleotide” accumulates in cells.
The PEPTIDOGLYCAN residues are linked together forming a long strand and UDP is split off.
The final step is cleavage of terminal D-aniline of peptide chain by transpeptidase; energy so released is utilised for establishment of cross linkage between peptide chains of neighbouring strands.
This cross linking provide stablity and rigidity to the cell wall.

Comparison of the structure and composition of gram-positive and
gram-negative cell walls.

Mechanism of action. Peptidoglycan synthesis(in last step) is inhibited by beta
lactam antibiotics.
Penicillin bind at the active site of the transpeptidase
enzyme that cross – links the peptidoglycan strands.
It does this by mimicking the D-alanyl-D-alanine
residues that would normally bind to this site.
Penicillin irreversibly inhibit the enzyme transpeptidase.
For the action of penicillin and cephalosporin ;these are
collectively termed Penicillin-binding protein (PBS) are
present on cell membrane of bacteria.
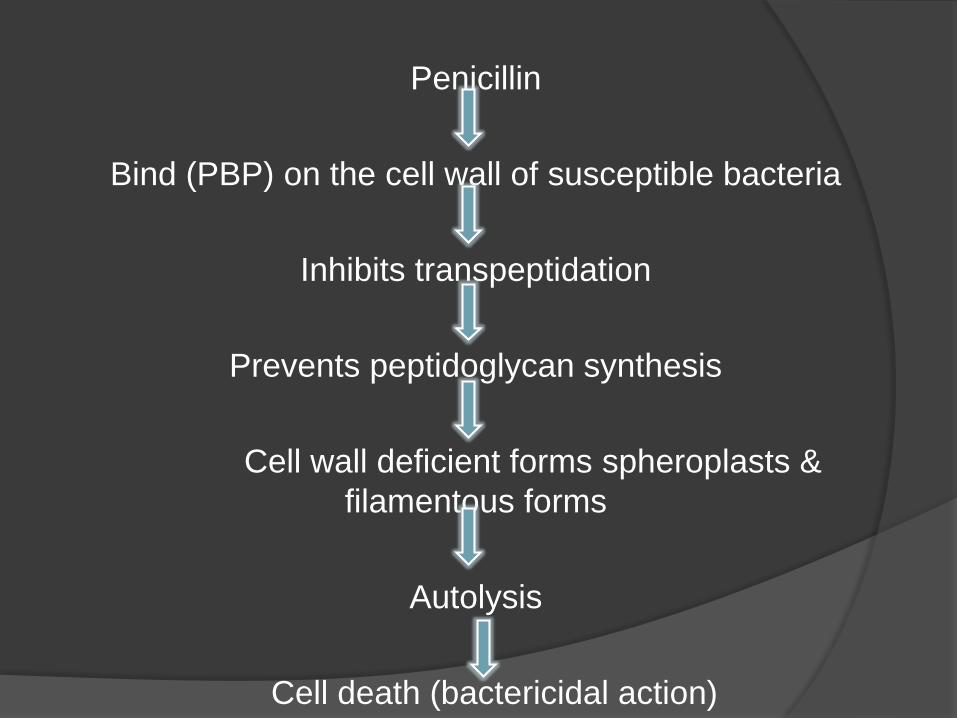
Penicillin
Bind (PBP) on the cell wall of susceptible bacteria
Inhibits transpeptidation
Prevents peptidoglycan synthesis
Cell wall deficient forms spheroplasts &
filamentous forms
Autolysis
Cell death (bactericidal action)

CLASSIFICATION-
PENICILLIN-
Natural Penicillins
• Penicillin G
Semi synthetic Penicillins
• Acid-resistant alternative to penicillin G
• (Penicillin V);
• Penicillinase-Resistant Penicillins
• (cloxacillin, Oxacillin, Methicillin)
• Extended-spectrum penicillins
• 1. Aminopenicillin-Ampicillin and Amoxycillin
• 2.Carboxypenicillin
• Carbenicillin, Ticarcillin
• 3.Ureidopenicillins-
• Piperacillin,Mezlocillin.
B-lactamaseinhibitors-
• Clavlanic acid
• Sublactam
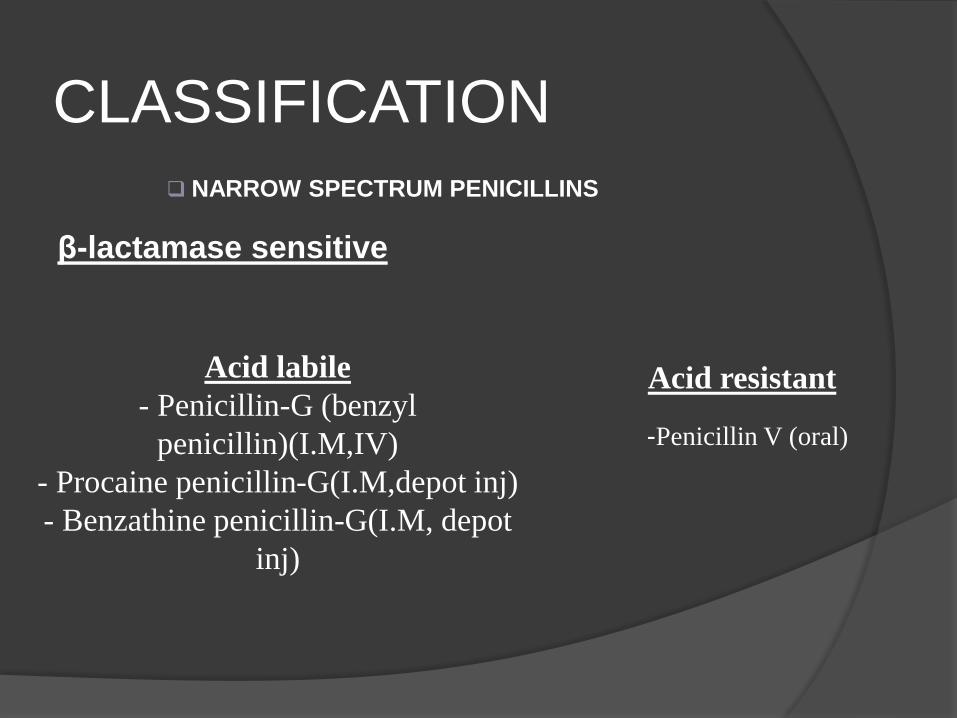
CLASSIFICATION
NARROW SPECTRUM PENICILLINS
β-lactamase sensitive
Acid resistant
-Penicillin V (oral)
Acid labile
- Penicillin-G (benzyl
penicillin)(I.M,IV)
- Procaine penicillin-G(I.M,depot inj)
- Benzathine penicillin-G(I.M, depot
inj)

β-lactamase resistant
Acid resistant
- Cloxacillin
- Dicloxacillin
- flucloxacillin
Acid labile
- Methicillin (I.M,I.V)
- Nafcillin (I.M,I.V)

EXTENDED SPECTRUM PENICILLINS
Acid resistant
• Aminopenicillins: Ampicillin, Amoxicillin, Bacampicillin,
Talampicillin
Acid labile (ANTIPSEUDOMONAL PENICILLINS)
• Carboxypenicillins: Carbenicillin, Ticarcillin
• Ureidopenicillins: Piperacillin, Mezlocillin, Azlocillin
BETA LACTAMASE INHIBITORS
• Sulbactam, Tazobactam, Clavulanic acid

Natural penicillins
Penicillin G is a narrow spectrum
antibiotic;
activity is primarily to gram positive bacteria and
few other.
Obtained from fermentations of the mold
Penicillium chrysogenum
Penicillin G (benzylpenicillin)
Penicillium

Cocci- streptococci (except enterococci)
staphylococcus aureus,
(gram negative cocci)
Neisseria gonorrhea
N. meningitis
Bacilli- B.anthracis
Corynebacteriumm diptheria,
Clostridium tetnai.
Actinomyces israelli(moderately sensitive)
Gram negative bacilli- E coli.
proteus.
Activity against these Microrganism-

Pharmacokinetics
It is relatively unstable in acid, thus the
bioavailability is low.
There is poor penetration into the cerebrospinal
(CSF), unless inflammation is present.
Active renal tubular secretion results in a short
half-life.

PharmacokineticsOral administration of Penicillin G:
Acid labile
About one-third of an orally administered dose of PnG is
absorbed from the intestinal tract under favorable conditions.
Gastric juice at pH 2 rapidly destroys the antibiotic.
Parenteral Administration of Penicillin G:
From I.M site absorption is rapid and complete
Peak plasma levels attained in 30min

DISTRIBUTIONPenicillin G is distributed widely, but the
concentration differs in various fluids and tissues.
Its apparent volume of distribution is ~0.35 L/kg.
Approximately 60% of penicillinG in plasma is
reversibly bound to albumin.
Significant amounts appear in liver, bile, kidney,
joint fluid, and lymph.

Cerebrospinal Fluid
Penicillin does not readily enter the CSF but
penetrates more easily with meningeal
inflammation.
The concentration attained usually reaches
5% of the value in plasma and thus is
therapeutically effective against susceptible
microorganisms.

EXCRETIONNormally, penicillin G is eliminated rapidly from the body, mainly by the kidney.
Approximately 60–90% of an intramuscular dose of penicillin G in aqueous solution is eliminated in the urine, largely within the first hour after injection.
The remainder is metabolized to penicilloic acid.
The t1/2 for elimination of penicillin G is ~30 minutes in normal adults.
Approximately 10% of the drug is eliminated by glomerularfiltration and 90% by tubular secretion

Unitage of Penicillin
The IU of penicillin is the specific penicillin activity
contained in 0.6 microgram of the crystalline sodium salt
of penicillin G.
Thus 1g= 1.6 million units
1 million unit= 0.6g

DOSES- 1. Sod.Penicillin G inj-
0.5-5 MU i.m./i.v. 6-12 Hourly
( BENZYL PEN 0.5-1MU in
Repository Penicillin G inj- these are insoluble salts of PnG which must be
given by deep i.m (Never i.v.) slowly at the site of inj.
2. Procaine Penicillin G inj- 0.5-1 MU( i.m) 12-24 hourly as aqueous
suspension.
( PROCAINE PENICILLIN-G 0.5 MU dry powder in vial)
It is a form of penicillin which is a combination of benzylpenicillin and
the local anaesthetic agent procaine. Following
deep intramuscular injection, it is slowly absorbed into the circulation
and hydrolysed to benzylpenicillin — thus it is used where prolonged low
concentrations of benzylpenicillin are required.
This combination is aimed at reducing the pain and discomfort associated
with a large intramuscular injection of penicillin. It is widely used in
veterinary settings.

Fortified procaine penicillin G inj- contain 3 lac U
procaine penicillin and 1 lac U sod. Penicillin G to
provide rapid as well as sustained blood level.
3. Benzathine benzylpenicillin-
Dose- Penidure LA12 Inj (12 lac unit)
It is the drug-of-choice when prolonged low
concentrations of benzylpenicillin are required and
appropriate, allowing prolonged antibiotic action over
2–4 weeks after a single IM dose
USES
58
Streptococcus pneumoniae infections
Meningococcal infections
Syphilis
Prophylaxis against Group A Streptococci
in patients with history of rheumatic heart
disease
Actinomycosis
Trench mouth

Therapeutic uses-
Gingivostomatitis, produced by the synergistic
action of Leptotrichia buccalis and fusospirochetes
that are present in the mouth, is readily treatable
with penicillin.
For simple “trench mouth,” 500 mg penicillin V
given every 6 hours for several days is usually
sufficient

Streptococcal Infections
Pharyngitis is the most common disease produced by S. pyogenes. Penicillin-resistant isolates of this organism have yet to be observed.
The preferred oral therapy is with penicillin V, 500 mg
every 6 hours for 10 days. Equal results are produced by the administration of 600,000 units of penicillin G procaine intramuscularly once daily for 10 days or by a single injection of 1.2 million units of penicillin G benzathine

Streptococcal Toxic Shock and
Necrotizing Fascitis
These life-threatening infections are best treated with
penicillin plus clindamycin (to decrease toxin synthesis).

Pneumococcal Infections
Penicillin G is the drug of choice for infections caused by sensitive strains of S. pneumoniae, but resistance is an increasing problem.
Thus, for pneumococcal pneumonia, a third-generation
cephalosporin or high-dose penicillin G (i.e., 20–24 million units daily by continuous intravenous infusion or in divided boluses every 2–3 hours) should be used until sensitivities are determined.
For parenteral therapy of sensitive isolates, penicillin G or penicillin G procaine is favored.
Therapy should be continued for 7–10 days, including 3–5 days after the patient is afebrile

Streptococcal Pneumonia, Arthritis,
Meningitis, and Endocarditis
These uncommon conditions should be treated with penicillin
G; daily doses of 12–20 million units are administered
intravenously for 2–4 weeks (4 weeks for endocarditis

Infections with Anaerobes
Many anaerobic infections are polymicrobial, and most of the organisms are sensitive to penicillin G.
An exception is the B. fragilis group, 75% of which may be resistant. Pulmonary and periodontal
infections usually respond well to penicillin G.
Mild-to-moderate infections at these sites may be treated with oral medication (either penicillin G or penicillin V 400,000 units four times daily).

Staphylococcal Infections
The vast majority of staphylococcal infections involve penicillinase-producing organisms.
Patients with staphylococcal infection should receive penicillinase-resistant penicillins (e.g., nafcillin or oxacillin).
Staphylococcal infections increasingly involve methicillin-resistant staphylococci, which are resistant to penicillin G,

Meningococcal Infections
Penicillin G is the drug of choice for meningococcal disease.
Patients should be treated with high doses of penicillin given
intravenously

Syphilis
Therapy of syphilis with penicillin G is highly effective.
Primary, secondary, and latent syphilis of<1 year’s
duration may be treated with penicillin G procaine (2.4
million units per day intramuscularly),plus probenecid
(1.0 g/day orally) to prolong the t1/2, for 10 days or
with 1–3 weekly
Intramuscular doses of 2.4 million units of penicillin G
benzathine (three doses in patients with HIV infection)

Adverse effects Hypersensitivity Reactions:
The basis of which is the fact that degradation products of penicillin
combine with host protein and become antigenic.
Jarisch- Herxheimer reaction: Penicillin injected in a syphillitic pateint
(secondary syphillis) may produce shivering , fever,myalgia,
exacerbation of lesions, even vascular collapse. This is due to sudden
release of spirochetal lytic products and last 12-72 hrs. It does not recur
and doesnot need inertuption of therapy.

Other adverse effects
Very high doses of penicillin G can
cause seizures in kidney failure.
Pain at I.M injection site
Nausea on oral ingestion
Thromboplebitis of injected vein

The major draw backs of benzylpenicillin are:
Inactivation by gastric acid
Short duration of action
Poor penetration into the CSF
Narrow spectrum of activity
Susceptibility to Penicillinase
Development of resistance
Possibility of anaphylaxis

Penicillin V ( acid resistance
to Penicillin –G) Orally active
Used for the treatment of bacteremia and oral infections
Higher minimum bactericidal concentration.
• DOSE:
• 250-500 mg. Given 6 hourly.
• Infants:60mg
• Crystapen-V, kaypen, 125, 250mg tab.

Penicillinase-resistant
penicillins(antistaphylococcal penicillins)
These congeners have side chains that protect the beta
lactam ring from attack by staphylococcal penicillinase
Indicated in infections caused by penicillinase producing
staphylococci (drugs of choice, except in MRSA)
Methicillin, Cloxacillin
Oxacillin, Nafcillin, Dicloxacillin

Penicillinase-resistant
penicillins(antistaphylococcal penicillins)Methicillin:
Acid labile
Not used clinically, except to identify resistant strains
MRSA is susceptible to Vancomycin/linezolid and rarely
Ciprofloxacin
It is highly penicillin resistant but not acid resistant- must be
injected.
Adverse reaction- haematuria, albuminuria, reversible
interistial nephritis.

Penicillinase-resistant penicillins…
Cloxacillin: Highly Penicillinase and Acid resistant
More active than methicillin
Less active against PnG sensitive organisms: should not be used as its
substitute
Incompletely but dependably absorbed (oral route)
>90% protein bound, eliminated primarily by kidney, also partly by liver
Plasma half life is about 1hr
Given in staphylococcus infection resistant to benzyl penicillin
Active against a variety of gram-negative bacilli as well.

Dose- 0.25, 0.5 g orally every 6 hourly,
For severe infections 0.25-1g may be injected
i.m or i.v.
BIOCLOX , CLOCILIN 0.25, 0.5g CAP.
0.5g/ vial injection
Ampicillin + cloxacillin –
Ampoxin- (ampicillin 125mg + cloxacillin 250mg)
Roscilox- (ampicillin 125mg + cloxacillin 250mg)

Extended spectrum penicillins.
Aminopenicillins:
Ampicillins:
Active against all organisms sensitive
to PnG; in addition, many gram-
negative bacilli

Extended spectrum penicillins Cont…

Extended spectrum
penicillins Cont…
Pharmacokinetics:
Acid resistant
Oral absorption is incomplete but adequate
Primary excretion is kidney, partly enterohepatic circulation
occurs
Plasma half life is 1hr
Uses:
UTI, RTI, Meningitis, Gonorrhoea, typhoid fever, bacillary dysentery,
Cholisystitis, Subacute bacterial endocarditis and Septicemias

Extended spectrum
penicillinsAdverse effects:
Diarrhoea(it is incompletely absorbed – the unabsorbed drug
irritates the lower intestine as well as causes marked alteration
of bacterial flora)
Rashes
Hypersensitivity
Interactions:
Hydrocortisone –inactivates ampicillin if mixed in the I.V solution
Oral contraceptive –failure of oral contraception
Probenecid –retards renal excretion

Extended spectrum
penicillins Bacampicillin –ester prodrug of ampicillin
Talampicillin, Pivampicillin and Hetacillin are other Prodrugs of ampicillin
DOSE-
Adult- 250- 500 mg every 6 hr
Child- 50-100 mg/kg given in equally divided doses every 6 hr
Maximum- 2-4 g/ day
Roscillin cap 500mg cap- 250 mg, inj 250 mg, inj 500 mg (ranbaxy)
D-syr 125mg/ml, 250mg/ml
Ampillin- Cap 250 mg, Cap 500mg, inj 250mg, 500mg
Ampicillin + cloxacillin –
Ampoxin- (ampicillin 125mg + cloxacillin 250mg)
Roscilox- (ampicillin 125mg + cloxacillin 250mg)
Ampicillin + sulbactam –
Ampitum inj ( ampicillin 1g + sulbactam 0.5g/ml)
( community accguired and hospital accquired pneumonia)

Amoxicillin:
Close congener of ampicillin but not a prodrug
Similar to it in all aspects except: Better oral absorption
Higher and sustained blood levels are produced
Incidence of diarrhoea is lower
Less effective against Shigella and H. influenzae
DOSE-
Amoxylin , 250, 500mg
Novamox 250,500mg
Mox 500mg,500mg
Symoxyl – LB 625 (500mg(amoxicillin )+ 60 million cell( lactobacilli sporogene
Stedmox- Tn(500mg(amoxicillin ) + 500mg( tinidazole)
Moxikind CV- kid (200mg(amoxicillin)+28.5mg( clavunaic acid)
Moxikind CV- 625 (500mg(amoxicillin)+125mg( clavunaic acid)
Agupen LB- (875(amoxicillin trihydrate)+125mg( clavunate K) + 60 million cell( lactobacilli sporogene)
Agupen LB- 625 (500mg(amoxicillin trihydrate)+125mg( clavunate K) + 60 million cell( lactobacilli sporogene)

Extended spectrum
penicillins2. Carboxypenicillins (Carbenicillin, Ticarcillin)
and
3. Ureidopenicillins (Piperacillin)

CARBEPENICILLIN
Penicillin conger.
Special feature- its activity against peudomonas
aeriginosa and indole positive Proteus.
It has Gram-negative coverage which
includes Pseudomonas aeruginosa but
limited Gram-positive coverage
Less active against- salmonella, E.coli,
Enterobacter.
Klebisella and gram positive cocci are remain
unaffected.

Uses-
Burns
Urinary infection.
Septecimia.
Uncomplicated gonorrhea

Pharmacokinetics
It is neither penicillinase resistant nor acid resistant.
Inactive orally.
Excreted rapidly in urine.
t ½ = 1hr
Dose= 1-2 g i.m, 1-5 g i.v.
Trade name-
Pyogen, Carbelin 1g, 5 g per vial inj

Extended spectrum
penicillins
These are called antipseudomonal penicillins
Piperacillin is more potent among these
Carbenicillin is less effective against Salmonella, E. Coli and
enterobacter but not active against Klebshiella and gram-positive
cocci
Piperacillin has good activity against Klebshiella, and is used
mainly in neutropenic/ immunocompromised patients having
serious gram-negative infections and in burns
UREIDOPENICLLINS- (PIPERACILLIN)

t ½ =1 hr.
Dose = 100-150 mg/kg/day.
Trade name=
Piprapen 1g, 2g vials
Pipracil inj 2g, 4g
Pipracillin+tazobactam ( noscomial infection )-
Novacillin plus (pipracillin Na 4g + tazobactam
0.5 g)

Beta-lactamase inhibitorsClavulanic acid, Sulbactam and Tazobactam
They contain beta-lactam ring but themselves, do not have
significant antibacterial activity.
Inactivate bacterial beta-lactamases and are used to
enhance the antibacterial actions of beta-lactam
antibiotics.

Beta-lactamase inhibitors Cont…
Clavulanic acid:
Obtained from Streptomyces clavuligerus.
It has beta lactam ring but no antibacterial activity of its own.
It inhibit wide variety Class II to class V of beta lactamase.
It is a progressive inhibitor : binding with beta lactamase is reversible
intially but becomes covalent later – inhibitition increasing with time.
Called a suicide inhibitor , it gets inactivated after binding to enzyme.

Pharmacokinetics-
Rapid oral absorption.
Bioavailability – 60%
t ½ = 1 hr
Pharmacokinetics matches amoxicillin
with which it is used.

Uses- Addition of clavunic acid restablises the activity of amoxicillin against
beta lactamase producing resistant Staph.aureus, H. inflenza,
N.Gonorrhoeae, E coli proteus, klebisella, salmonella and bacteria
Fragilis.
Coamoxiclav is indicated for
Odontogenic infection
Skin and soft tissue infection.
Respiratory tract infection.
Intra abdominal and gynaecological infection
Dose- Agumentin- Amoxicillin 250mg + Clavunic acid125mg ( TDS)
Agumentin – amoxicillin 1 g & clavunic acid 0.2 g vial. i.m /i.v
6-8 hourly for severe infection.

Adverse effect-
As same as amoxicillin alone.
Poor G.I tolerance.(specially in children)
Other side effect-
Candida stomatitis.
Vaginitis.
Rashes.
some cases of hepatic injury have been
reported

Sulbactam: Semisynthetic beta-lactamase inhibitor
Related chemically as well as in activity to clavulanic acid
It is also a progressive inhibitor
Combined with ampicillin.
On the weight basis , it is less potent than clavunic acid for most
type of enzymes, but the same level of inhibition can be obtained
at the higher concentration achieved clinically.
Oral absorption of sulbactam is inconsistent.
Therefore , it is preferably given parentally.
Dose – Sulbacin,
Ampitum : Ampicillin 1 g & sulbactam 0.5 g per vial inj.
Sulbacin 375 mg tab

Beta-lactamase inhibitors Cont…
Tazobactam:
Similar to Sulbactam
Pharmacokinetics matches with Piperacillin with which it is used for
used in severe infections like peritonitis, pelvic/urinary/respiratory
infections
However, the combination is not effective against piperacillin-
resistant Pseudomonas

They are available only in fixed combinations with
specific penicillins:
Ampicillin + Sulbactam (1g+0.5g I.V/I.M inj)
Amoxycillin + Clavulanic acid (250mg+125mg tab)
Piperacillin + Tazobactam sodium (2g+0.25g I.V/I.M
inj)

DRUG INTERACTION

DRUG INTER ACTIVITY
DRUG
POTENTIAL EFEECT MANAGEMENT
PENICILLIN CLASS Food Decrease / delayed GI
absorption of penicillin
GI Administer penicillin
at least
absorption of oral
penicillin's. 2 hours
before or after a
meal.
Tetracyclines
(doxycycline,
minocycline,
oxytetracycline)
Decreased effects of
penicillin
.Avoid combination.
Warfarin
(Anti coagulant,
thrombolytic)
Increased the effect of
warfarin with larger
dose of IV penicillin
Decrease warfarin dose
if necessary
Methorexate
(Antineoplastic agent)
Increase concentration
of methorexate ,
decrease effect of
penicillin,
Increase risk of
methotrexate toxicity
Monitor sign of toxicity,
Use of alternative
antibiotic (Ceftazidime)

Allopurinol Increased rate
of ampicillin
associated skin
rash
use alternative
drug if rash
develops.
Atenolol Decreased
effects of
atenolol
Separate
administration
times.
Monitor blood
pressure.
Increase
atenolol
dose if
necessary.

Poisioning and overdose-Drug Half life Toxic dose
/serum level
toxicity
Penicillin 30 min 10 million units/d IV,
or CSF > 5 mg/L
Seizures with single
high dose or chronic
excessive doses in
patients with renal
dysfunction
Methicillin 30 min Unknown Interstitial nephritis,
leukopenia
Nafcillin 1.0 h Unknown Neutropenia.
Ampicillin, amoxicillin 1.5 h Unknown Acute renal failure
caused by crystal
deposition
Carbenicillin 1.0–1.5 > 300 mg/kg/d or >
250 mg/L
Bleeding disorders
due to impaired
platelet function;
hypokalemia. Risk of
toxicity higher in
patients with renal
insufficiency
Piperacillin 0.6–1.2 > 300 mg/kg/d “
Ticarcillin 1.0–1.2 > 275 mg/kg/d “
Poisoning and drg overdose, Kent R.Olson. 5th edition.

Refrences-
Essential of medical pharmacology.
K D Tripathi. 5th edition
Manual of pharmacolgy and
therapeutics. Goodman and Glickman .
Poisoning and drug overdose, Kent
R.Olson. 5th edition
Katzung 9th edition.