pustaka.unpad.ac.idpustaka.unpad.ac.id/wp-content/uploads/2015/10/deteksi-dini-lesi...panduan...
TRANSCRIPT

.__.._-----------

- - -- -----------------1iii
MANAGEMENT OF
ABNORMAL SMEAR LGSIL/HGSIL
.:. Key points:
• These are practices guidelines should not be
considered rule or standard of care
• Clinical care must always take into account the
individual patient
• Developed for US setting - all may not be
appropriate in other country
2001 Consensus Guidelines
Bethesda (ASCCP)
.:. Key points:
• These are practices guidelines should not be
considered rule or standard of care
• Clinical care must always take into account the
individual patient
28
Developed for USsetting - all may not be appropriate in
other country .
•:. The Bethesda System
• Terminologi pelaporan hasil tes Pap terbaru
yang berorientasi klinik
• Perkembangan:
1988: Pengembangan sistem pelaporan sebagai
sistem terminologi yang seragam untuk
panduan penatalaksanaan klinik.
1991: Modifikasi setelah implementasi
pengalaman klinik dan laboratorium aktual
2001: Re-evaluasi dengan adanya teknologi
dan penemuan baru
• Rekomendasi:
• Laporan sitopatologi adalah konsultasi medik
• Klasifikasi Papanicolaou sudah tidak layak
digunakan pada praktek diagnostik sitopatologi
modern
29

Sistem Bethesda berfungsi sebagai petunjuk pelaporan
sitopatologi serviksjvagina. Merupakan penyempurnaan
dari sistern Bethesda 1991. Termasuk metoda pengenalan
tes tambahan dan automatisasi .
• Rekomendasi final: khususnya penyempurnaan
adekuasi spesimen dan kategori umum .
•:. Pelaporan TBS
• Adekuasi spesime
• Kategori umum
• Interpretasi j hasil
30

32
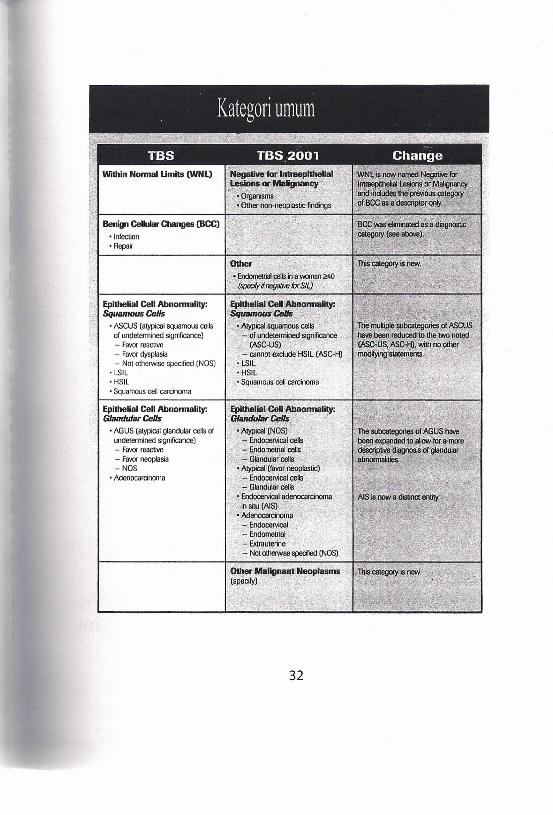
-Infection" I . Repair I1'.'"'' ,".c', .'
Epithelial Cell Abnonnality:Squamous Cells
• ASCUS (atypical squamous cellsof lWldelcnnined significance)- Favor reactive- Favordysplasia- NOI oiherwise specified (NOS)
• LSIL• HSIL• Squamous cel! carcinoma
Epithelial Cell Abnonnality:Glandular Cells
• AGUS (alypicaigiandlilar cells ofundetermined significance)- Favor reactive- Favor neoplasia- NOS
• Adenocarcinoma
II11
il

.:. Kategori Umum TBS 2001
Abnormalitas sel epitel
Sel skuamosa
• Atypical Squamous Cells (ASC):
• ASC-US, ASC-H (cannot exclude HGSIL)
• Low Grade Squamous Intraepithelial Lesion
(LGSIL)
• High Grade Squamous Intraepithelial Lesion
(HGSIL)
Karsinoma sel skuamosa
.:. Kategori Umum TBS 2001
Abnormalitas sel epitel
Sel glanduler
• Atipik (Not Otherwise Specified): sel endoserviks,
sel endometrium, sel glanduler
• Atipik (Favor neoplastic): sel endoserviks, sel
glanduler
• Adenokarsinoma insitu serviks (AIS)
Adenokarsinoma: endoserviks, endometrium, extrauterin,
NOS.
33

.:. Atypical Squamous Cell
• ASC-US of Undetermined Significance
• ASC-H Cannot exlude HSIL
.:. Tes Pap ASCUS
Tes Pap ASCUS dahulu dilaporkan:
Pap II (Papanicolaou)
Inkonklusif(Reagan)
Atipia sel (Richart)
.:. Atypical Squamous Cell-Undetermined Significance
Burden of disease in ASC-US
Individual risk of CIN 2,3 is 5 - 17%
Approximately 30-50% of CIN 2,3 occurs in
women with ASC Pap result
Risk of Ca. only about 1 : 1000
Management needs to take into account patient
/provider convenience, cost
34

2001 Consensus Guidelines
Management of ASC-US
• All three standard modalities are considered
safe & effective. Because of costs, and patient
convenience reflex HPV testing is prefered if
liquid based cytology or co-collection available
!
Treat according to grade
* IfHPV DNA (+) more aggressive follow-up recommended
35

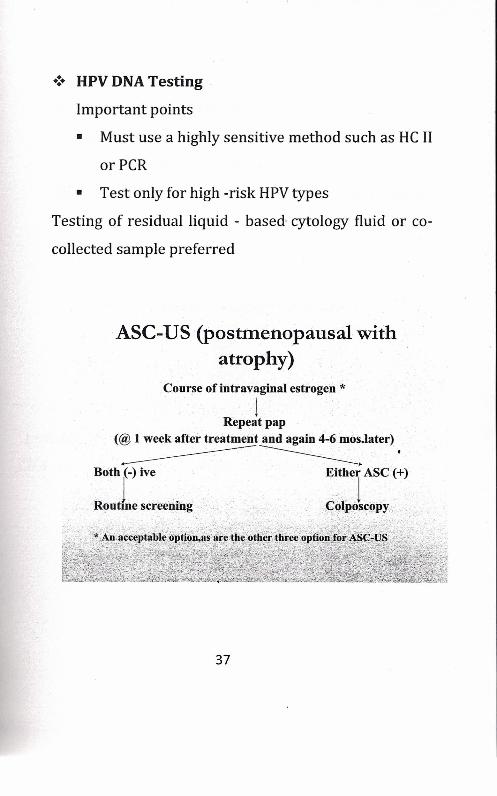
.:. HPV DNA Testing
Important points
• Must use a highly sensitive method such as HC II
orPCR
• Test only for high -risk HPV types
Testing of residual liquid - based cytology fluid or co-
collected sample preferred
ASC-US (postmenopausal withatrophy)
Course of intravaginal estrogen *1
Repeat pap(@ 1 week after treatment and again 4-'6mos.later)---------=------ .
Both (-) ive Either ASC (+)
R tl. .C ·1···1 .ou me screenmg· ... ;~ po?~copy. .
37

.:. Management of ASC-US
Immunosuppresed patients:
• Relatively few studies are available
Studies that are available show a high rate of biopsy
confirmed - CIN. High rate of high-risk HPV-DNA
positivity.
ASC-US(Immunosuppresed women)
IColposcopy *
*Includes all HIV-Infected women, irrespective of
CD4 count, HIV viral load, or antiretroviral therapy
38

::ct-
t-I
-~
IC
-IC
(l)
00
(j)
U
"
cY')
{;
CIl
= 0e~~
<::r;:
~I
=U
U
0'"
~~
Vl
-e<
- ~U..•Q..
0<

Women with ASC-H cytology
Colposcopy
CIN identified No CIN Identified
1Review all material
~Revised Dx ASr-H
Pap (6 & 12 mo)orHPV(12mo)
.:. Management of ASC
See and treat
Because of the potential for overtreatment, diagnostic
excisional procedures (LEEP) should not be routinely used in
the absence of biopsy confirmed CIN.
40

.:. Following an ASC-UScytology
• Repeat cytology with monolayer cytology at
ASC-US + threshold X 2 or one HPV test at 12
months, using Hybrid capture-2 at 1 pg +
threshold have high triage sensitivity for CIN 3
• A single + HPV test at 12 months has lower
referral to re-colposcopy than repeat cytology at
the ASC-US threshold
Repeat cytology at LSIL + threshold provides
inadequate sensitivity to detect CIN 3
.:. Liquid-based cytology
• Better specimen adequacy
o Unsatisfactory decreased 40-94 %
o Satisfactory but limited by decreased by 52-
96%
• Better detection of HSIL , LSIL
o 29-233 % more HSIL
o 65-110 % more LSIL
Decreased ASC-US
41

.:. Direct to VIAHSIL+ multisite outcome trials
• Increased detection
o 112,1 % LSIL
o 92,4 % HSIL
• True increase in detection both LSILand HSIL
o Fewer false positives
o Reduction in false negative rate
LB-cytologyas able to identify more biopsy proper HSIL+
.:. The Bethesda workshop 2001
Terminology changes for AGUS (Atypical Glandular
Undetermined Significance)
* The term of undetermined significance has been dropped ....
......AGUS is now atypical glandular cells or AGe
.:. Atypical glandular cells and Adenocarcinoma in
stu
.:. Glandular cells abnormalities:
• AGe (either endocervical, endometrium, or
glandular cells) not otherwise spesified (AGe
NOS)
• AGe (either endocervical or glandular cells)
• Favour neoplasia (AGe-favour neoplasia)42

Endocervical adenocarcinoma in situ (AIS)
Women with Atypical Glandular Cells (AGC)AGe Atypical endometrial cells
! !Endometrial sampling
.:. Recommendations managing women with AGe and
AIS
./ Colpsoscopy and endocervical sampling is
recommended with all subcategories of AGC
(exception if endometrial cell(+), should initially
be evaluated with endometrial sampling)
./ Women with AGC or AIS (+) is unacceptable
using repeat cervical cytology program
The preferred DxExProc. Is cold knife conization
43

Endocervical adenocarcinoma in situ (AIS)
Women with Atypical Glandular Cells (AGC)AGC Atypical endometrial cells
! 1Colposcopy (+endocervical sampling) Endometrial samplingand Endometrial sampling (~35 yrsor abn. Bleeding)
N'~'dl~" -R<fu," S_H"Initial Pap Initial Pap DX•.Excisional proc.ArC-NOS AGC-favour neoplasia- (cold knife cone)
.. ,~ ..·':qN1A:IS.··~o Ne?pl!l~.ia' ...., ,
. ',,' Rep~Jt~~t::\:"
'(i£~'~f~4=:~
.:. Recommendations managing women with AGe and
AIS
../ Colpsoscopy and endocervical sampling is
recommended with all subcategories of AGC
(exception if endometrial cell(+), should initially
be evaluated with endometrial sampling)
../ Women with AGC or AIS (+) is unacceptable
using repeat cervical cytology program
The preferred DxExProc. Is cold knife conization
43