pediatric brain tumors - boston university medical campus ... · pdf fileoverview •...
TRANSCRIPT
Pediatric Brain TumorsPediatric Brain Tumors
Asim Mian M.D.Asim Mian M.D.
OverviewOverview••
Pediatric brain tumors(PBT) are 15Pediatric brain tumors(PBT) are 15--20% of all brain tumors.20% of all brain tumors.••
Second most common pediatric tumor. Only leukemia more Second most common pediatric tumor. Only leukemia more common.common.
••
Overall, Overall, supratentorialsupratentorial
and and infratentorialinfratentorial
tumors occur in equal tumors occur in equal frequency.frequency.
••
SupratentorialSupratentorial
more common <2yrs; more common <2yrs; infratentorialinfratentorial
more more common 4common 4--10yrs; equally common after 10yrs age.10yrs; equally common after 10yrs age.
••
Clinical Presentation:Clinical Presentation:••
InfantsInfants--Increasing head circumference, lethargy, nausea Increasing head circumference, lethargy, nausea and vomiting.and vomiting.
••
ChildrenChildren--Also may have headaches, ↓visual acuity, Also may have headaches, ↓visual acuity, seizures, cranial nerve palsies, endocrine dysfunction.seizures, cranial nerve palsies, endocrine dysfunction.
ImagingImaging••
CT can be used for initial screening.CT can be used for initial screening.
••
MRI is superior and essential if CT finds MRI is superior and essential if CT finds abnormality or inconclusive.abnormality or inconclusive.••
MR spectroscopy can be useful: Elevated MR spectroscopy can be useful: Elevated CholineCholine and depressed NAA peaks(higher and depressed NAA peaks(higher cholinecholine, more , more
likeylikey
tumor to be high grade).tumor to be high grade).
ClassificationClassification
••
Posterior Posterior fossafossa
••
SupratentorialSupratentorial••
IntraparenchymalIntraparenchymal••
SellarSellar//SuprasellarSuprasellar••
ExtraExtra--axialaxial
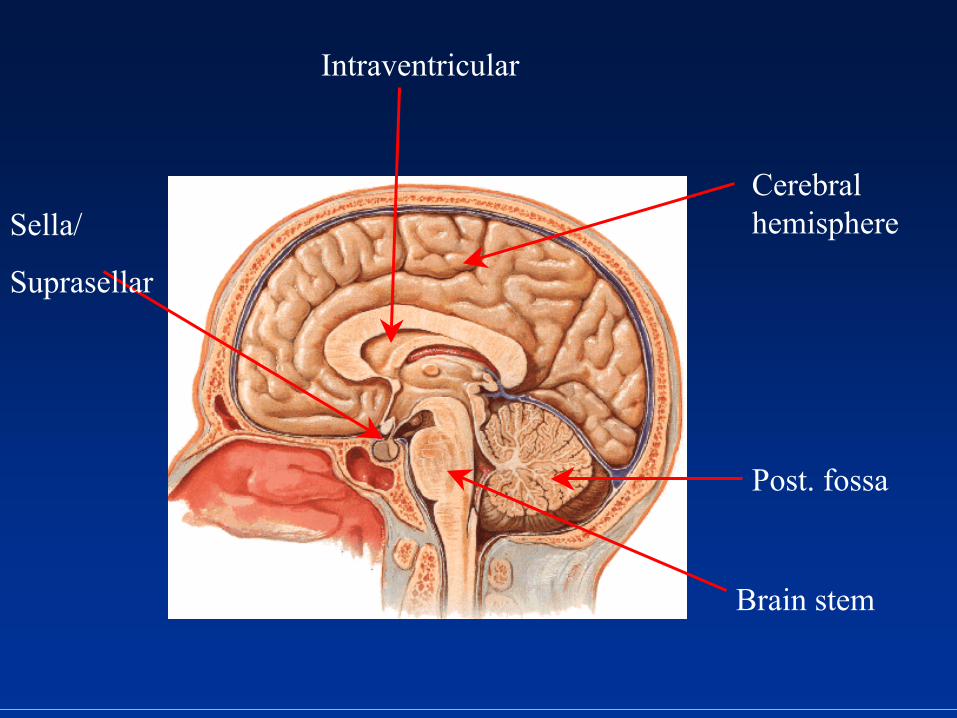
Post. fossa
Cerebral hemisphere
Intraventricular
Brain stem
Sella/
Suprasellar
ClassificationClassificationPosterior Posterior fossafossa••
AstrocytomaAstrocytoma••
MedulloblastomaMedulloblastoma••
EpendymomaEpendymoma••
Brainstem Brainstem gliomaglioma
DermoidDermoid//EpidermoidEpidermoidSchwannomaSchwannoma//MeningiomaMeningioma
(NF2)(NF2)
ClassificationClassificationSupratentorialSupratentorial
••
IntraparenchymalIntraparenchymal••
AstrocytomaAstrocytoma••
EpendymomaEpendymoma••
DesmoplasticDesmoplastic
neuroepithelialneuroepithelial
tumor (DIG)tumor (DIG)••
DysembryoplasticDysembryoplastic
neuroepithelialneuroepithelial
tumortumor••
GangliogliomaGanglioglioma//GangliocytomaGangliocytoma••
TeratomaTeratoma••
Primitive Primitive NeuroectodermalNeuroectodermal
Tumor (PNET)Tumor (PNET)••
Atypical Atypical teratoidteratoid//rhabdoidrhabdoid
tumorstumors
ClassificationClassificationSupratentorialSupratentorial
••
ExtraExtra--axialaxial••
Choroid plexus Choroid plexus papillomapapilloma/carcinoma/carcinoma••
LangerhansLangerhans
cell cell histiocytosishistiocytosis••
EpidermoidEpidermoid//DermoidDermoid••
ArachnoidArachnoid
cystcyst••
MetastasisMetastasis
ClassificationClassification••
SupratentorialSupratentorial
••
SellarSellar//SuprasellarSuprasellar••
CraniopharyngiomaCraniopharyngioma••
AstrocytomaAstrocytoma••
RathkeRathke
cleft cystcleft cyst••
Germ cell tumorsGerm cell tumors••
Hypothalamic Hypothalamic hamartomahamartoma••
LangerhansLangerhans
cell cell histioctyosishistioctyosis••
Pituitary adenomaPituitary adenoma
InfratentorialInfratentorial TumorsTumors AstrocytomaAstrocytoma
(Juvenile (Juvenile PilocyticPilocytic))
••
Most common pediatric brain tumor: 40Most common pediatric brain tumor: 40--50% 50% of intracranial of intracranial neoplasmsneoplasms••
60% located in posterior 60% located in posterior fossafossa••
M=FM=F••
Typically occurs between 5Typically occurs between 5--15yrs of age.15yrs of age.••
Clinical findings: Early morning headaches, Clinical findings: Early morning headaches, vomiting (worsens over time). Ataxia, vomiting (worsens over time). Ataxia, papilledemapapilledema
••
25yr survival rate of 90% following successful 25yr survival rate of 90% following successful surgerysurgery
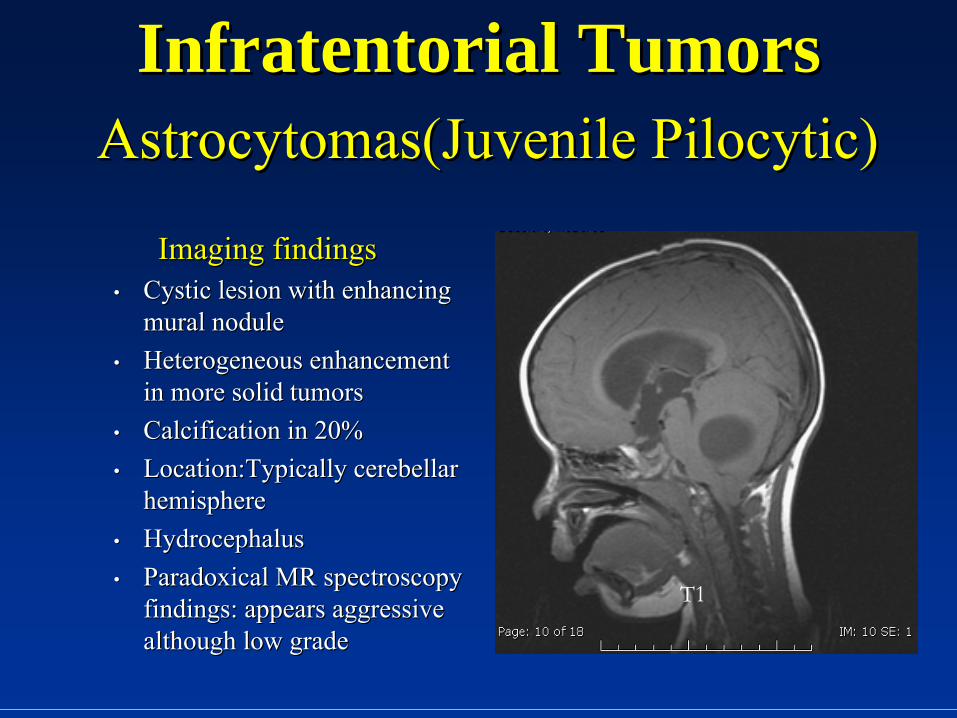
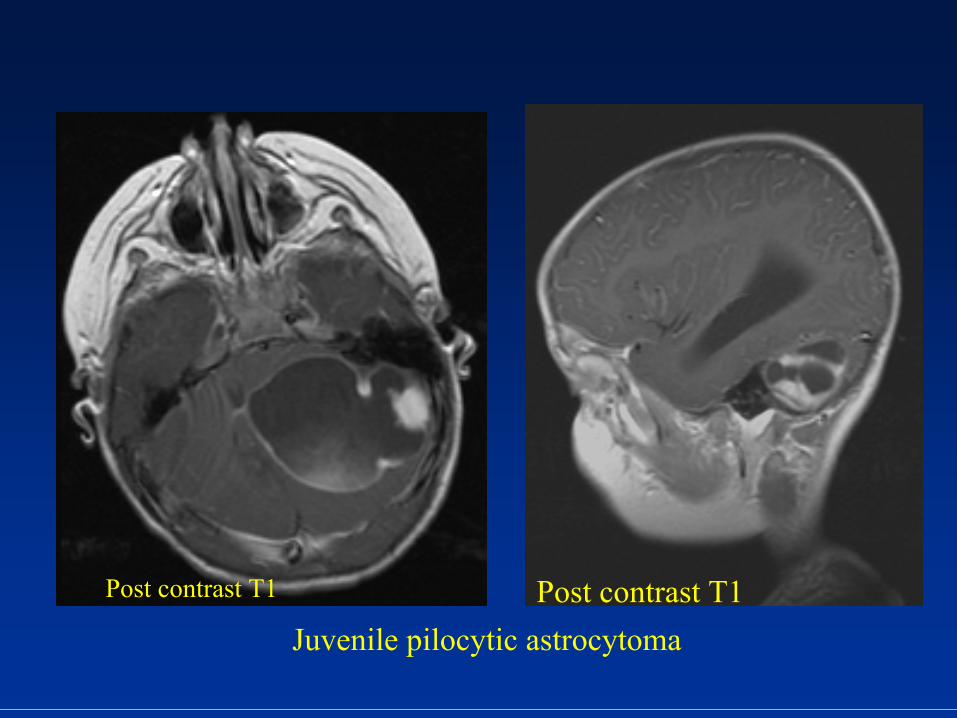
InfratentorialInfratentorial TumorsTumors AstrocytomasAstrocytomas(Juvenile (Juvenile PilocyticPilocytic))
Imaging findingsImaging findings••
Cystic lesion with enhancing Cystic lesion with enhancing mural nodulemural nodule
••
Heterogeneous enhancement Heterogeneous enhancement in more solid tumorsin more solid tumors
••
Calcification in 20%Calcification in 20%••
Location:Typically Location:Typically cerebellarcerebellar
hemispherehemisphere••
HydrocephalusHydrocephalus••
Paradoxical MR spectroscopy Paradoxical MR spectroscopy findings: appears aggressive findings: appears aggressive although low gradealthough low grade
T1
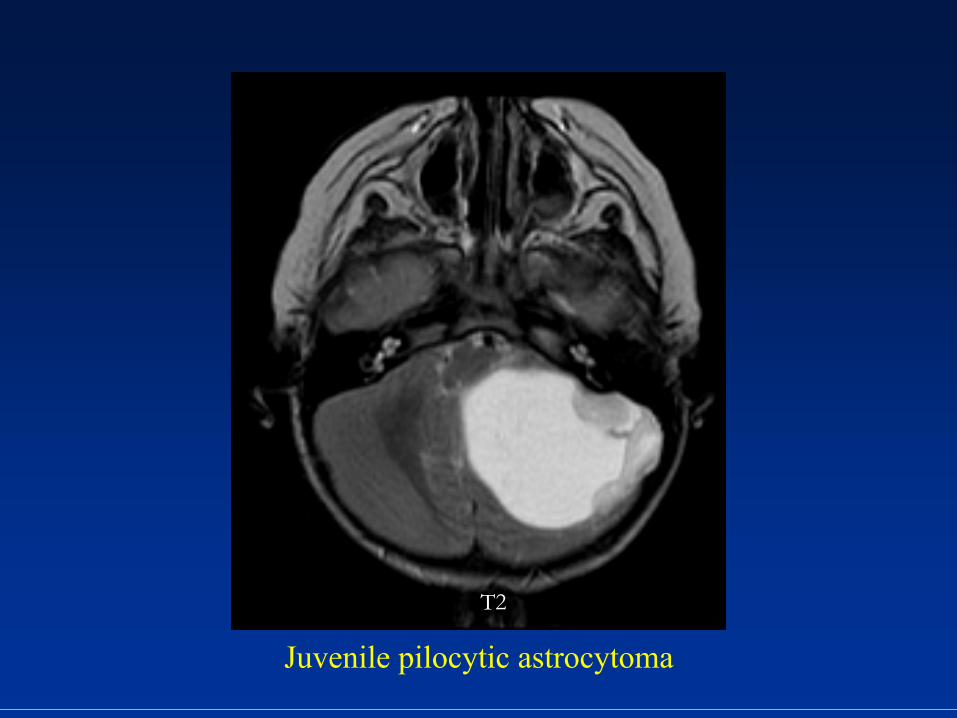
T2
Juvenile pilocytic
astrocytoma
Juvenile pilocytic
astrocytoma
Post contrast T1 Post contrast T1
InfratentorialInfratentorial TumorsTumors
MedulloblastomaMedulloblastoma (PNET)(PNET)
••
Highly malignant, undifferentiated tumorHighly malignant, undifferentiated tumor••
1515--20% of pediatric brain tumors20% of pediatric brain tumors••
Occur in 4Occur in 4--11yr age group and peaks at age 511yr age group and peaks at age 5••
Males 2Males 2--4 times more likely to be affected4 times more likely to be affected••
1/3 have subarachnoid 1/3 have subarachnoid metsmets; drop ; drop metsmets
to spine(40%)to spine(40%)••
IntraventricularIntraventricular
tumor from roof of 4tumor from roof of 4thth
ventricle ventricle
(superior (superior medullarymedullary
velum), velum), vermisvermis••
Midline in children; Laterally located in older Midline in children; Laterally located in older children, adultschildren, adults
InfratentorialInfratentorial TumorsTumors MedulloblastomaMedulloblastoma(PNET)(PNET)
••
Clinical findings: Short duration of symptoms Clinical findings: Short duration of symptoms with nausea, vomiting, headaches, ataxiawith nausea, vomiting, headaches, ataxia
••
Increasing head size, lethargy in children less Increasing head size, lethargy in children less then 1yr of agethen 1yr of age
••
NondisseminatedNondisseminated: 60: 60--70% 5yr survival70% 5yr survival••
Disseminated: 36% 5yr survivalDisseminated: 36% 5yr survival
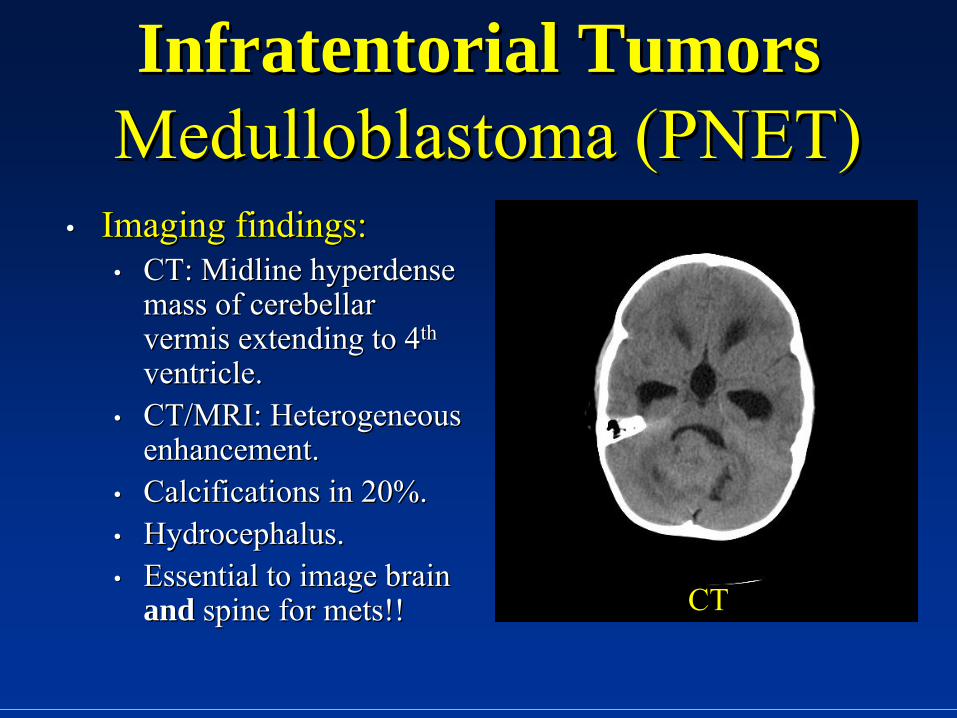
InfratentorialInfratentorial TumorsTumors MedulloblastomaMedulloblastoma
(PNET)(PNET)••
Imaging findings:Imaging findings:••
CT: Midline CT: Midline hyperdensehyperdense mass of mass of cerebellarcerebellar
vermisvermis
extending to 4extending to 4thth
ventricle.ventricle.••
CT/MRI: Heterogeneous CT/MRI: Heterogeneous enhancement.enhancement.
••
Calcifications in 20%.Calcifications in 20%.••
Hydrocephalus.Hydrocephalus.••
Essential to image brain Essential to image brain andand spine for spine for metsmets!!!! CT
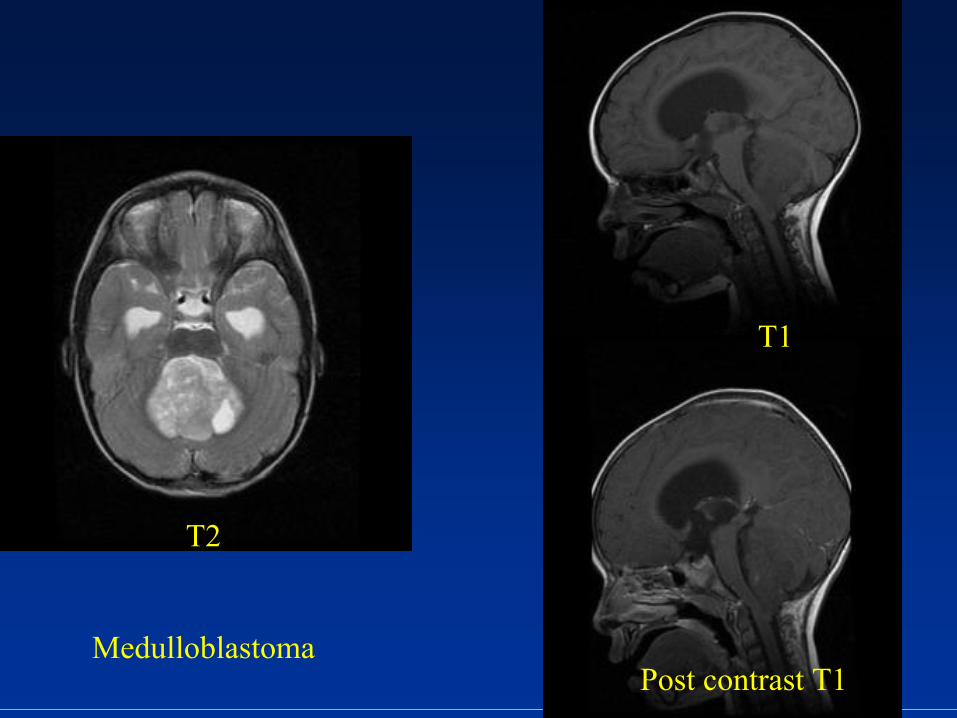
Medulloblastoma
T2
T1
Post contrast T1
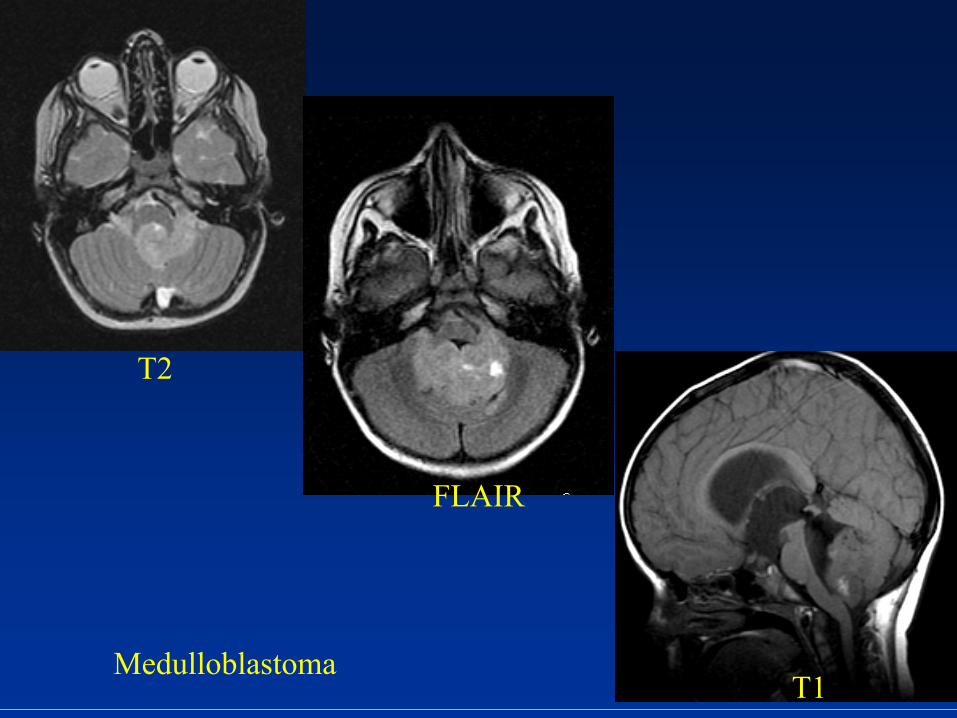
Medulloblastoma
T2
FLAIR
T1
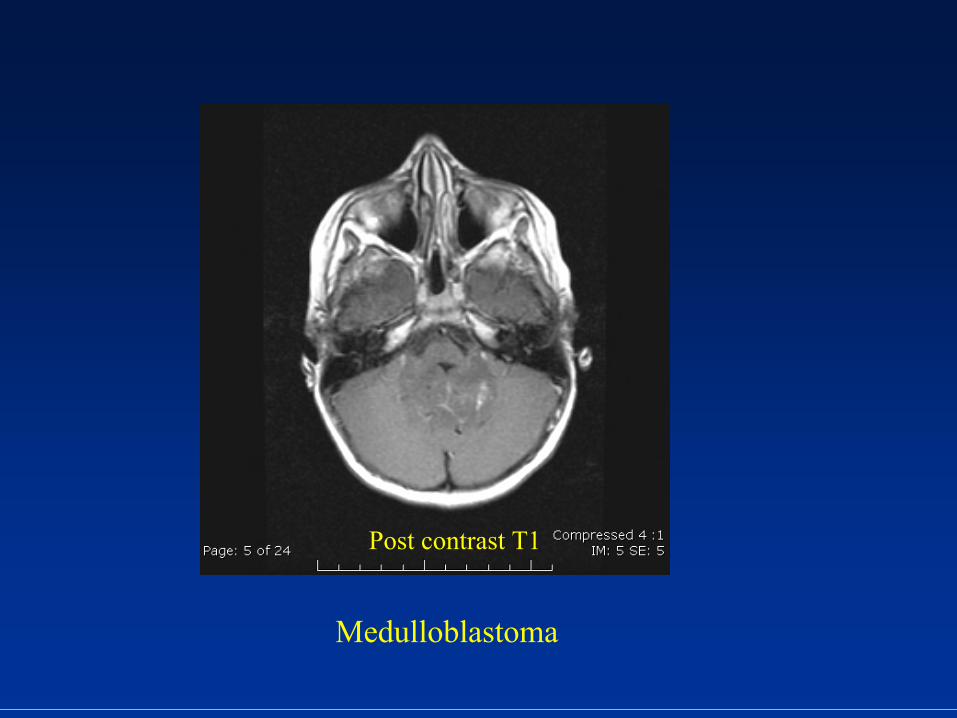
Medulloblastoma
Post contrast T1
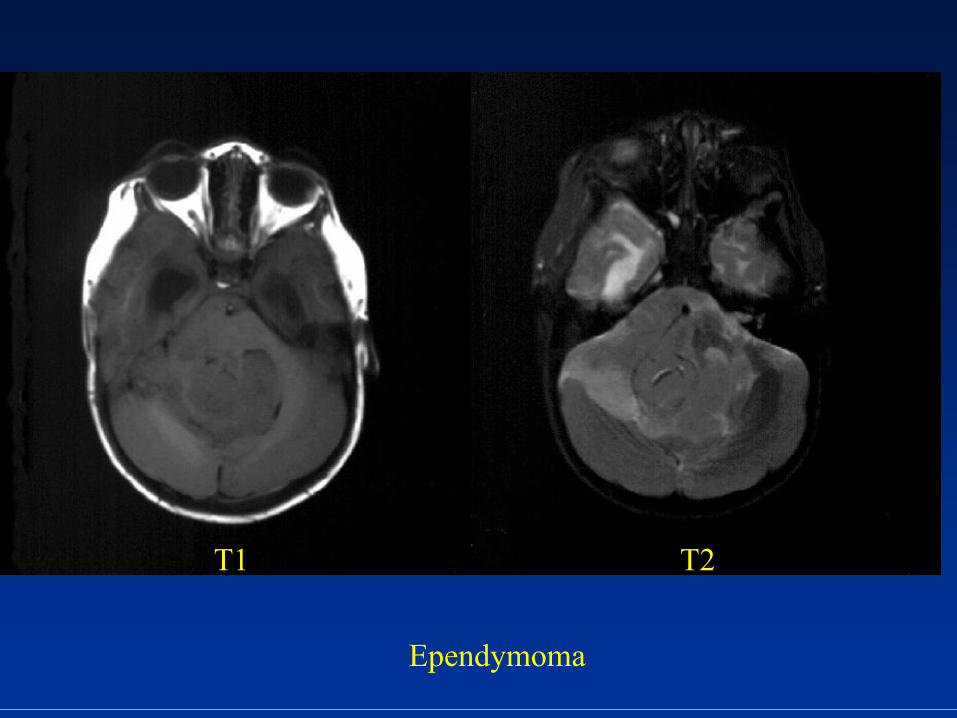
InfratentorialInfratentorial TumorsTumors EpendymomaEpendymoma
••
~10% of primary brain tumors in children~10% of primary brain tumors in children••
70% are infratentorial/30% 70% are infratentorial/30% supratentorialsupratentorial••
Slight increased incidence in malesSlight increased incidence in males••
2 age peaks: 12 age peaks: 1--5yrs and ~35yrs5yrs and ~35yrs••
Location: Location: VermisVermis, floor of 4, floor of 4thth
ventricle extending into ventricle extending into
ventricleventricle••
“Plastic” tumor that conforms to ventricle and “Plastic” tumor that conforms to ventricle and extrudes through Foramen of extrudes through Foramen of LuschkaLuschka
••
Clinical findings: Headaches, vomiting, ataxiaClinical findings: Headaches, vomiting, ataxia••
6060--70% 5yr survival70% 5yr survival

InfratentorialInfratentorial TumorsTumors EpendymomaEpendymoma
Imaging findings:Imaging findings:••
44thth
ventricle tumor that ventricle tumor that may extend through FOLmay extend through FOL
••
Calcifications common Calcifications common (50%)(50%)
••
HydrocephalusHydrocephalus••
CT/MRI: Heterogeneous CT/MRI: Heterogeneous enhancementenhancement
••
Gradient echo images Gradient echo images demonstrate blooming demonstrate blooming from calcificationsfrom calcifications CT
Ependymoma
T1 T2
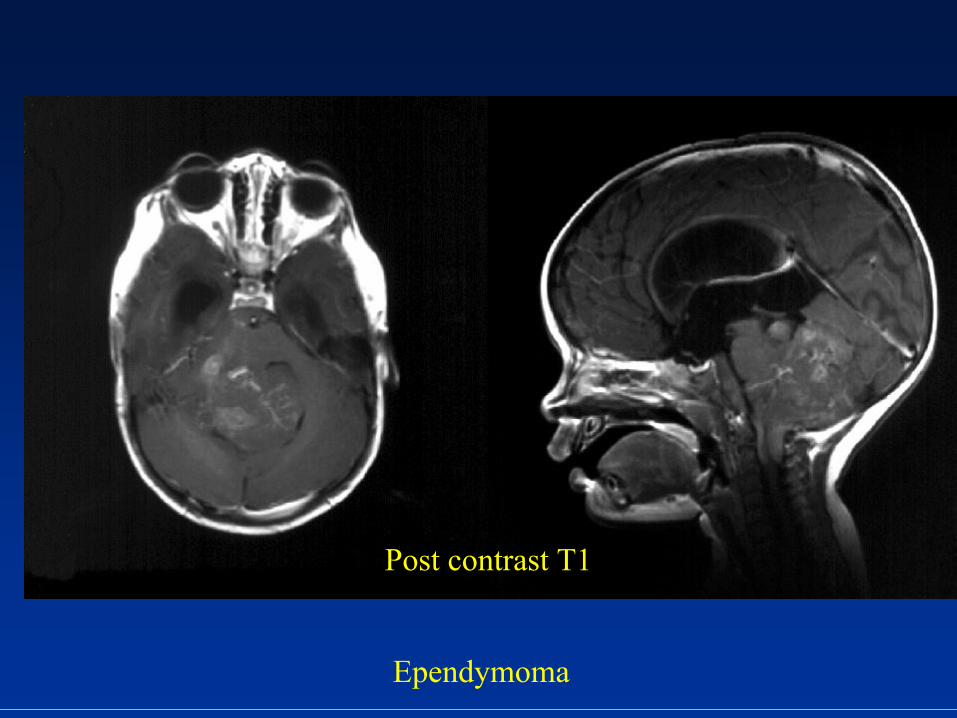
Post contrast T1
Ependymoma
InfratentorialInfratentorial TumorsTumors Brainstem Brainstem gliomaglioma
••
15% of pediatric CNS tumors and 2015% of pediatric CNS tumors and 20--30% of 30% of infratentorialinfratentorial
tumorstumors
••
80% high grade: 20% low grade80% high grade: 20% low grade••
M=FM=F••
Typically between 3Typically between 3--10yrs of age10yrs of age••
Location: Pons>>midbrain>medullaLocation: Pons>>midbrain>medulla••
4 types: Diffuse, focal, 4 types: Diffuse, focal, exophyticexophytic, , cervicomedullarycervicomedullary••
Prognosis and treatment depend on type with diffuse Prognosis and treatment depend on type with diffuse having poor prognosis, focal better prognosishaving poor prognosis, focal better prognosis
••
BG can be confused with brainstem encephalitisBG can be confused with brainstem encephalitis
InfratentorialInfratentorial TumorsTumors Brainstem Brainstem gliomasgliomas
••
TectalTectal
gliomasgliomas
are subtype with better are subtype with better prognosisprognosis
••
Brainstem “tumors” related to NF1 Brainstem “tumors” related to NF1 nonagressivenonagressive
••
Clinical: Hydrocephalus, cranial nerve VI and Clinical: Hydrocephalus, cranial nerve VI and VII palsiesVII palsies
InfratentorialInfratentorial TumorTumor
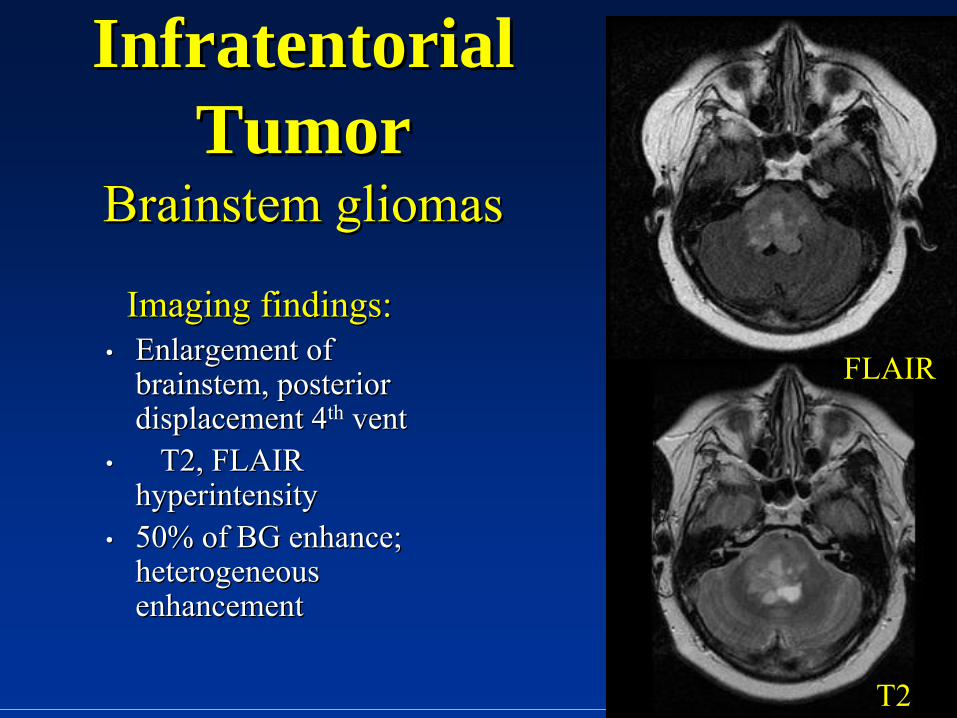
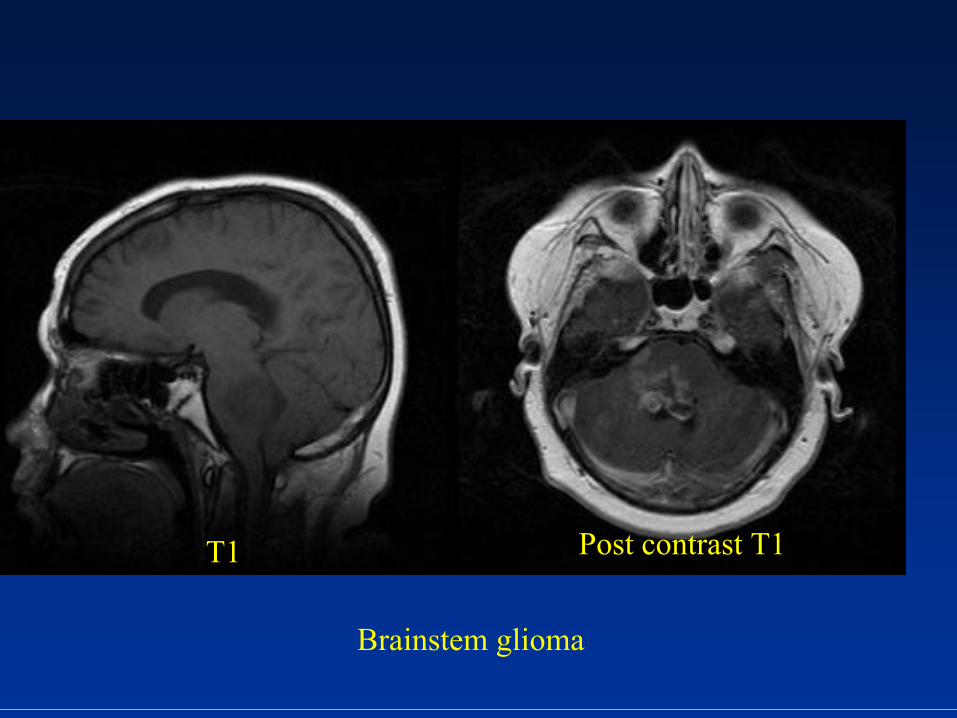
Brainstem Brainstem gliomasgliomas
Imaging findings:Imaging findings:••
Enlargement of Enlargement of brainstem, posterior brainstem, posterior displacement 4displacement 4thth
ventvent••
�T2, FLAIR �T2, FLAIR hyperintensityhyperintensity
••
50% of BG enhance; 50% of BG enhance; heterogeneous heterogeneous enhancementenhancement
FLAIR
T2
Brainstem glioma
T1 Post contrast T1
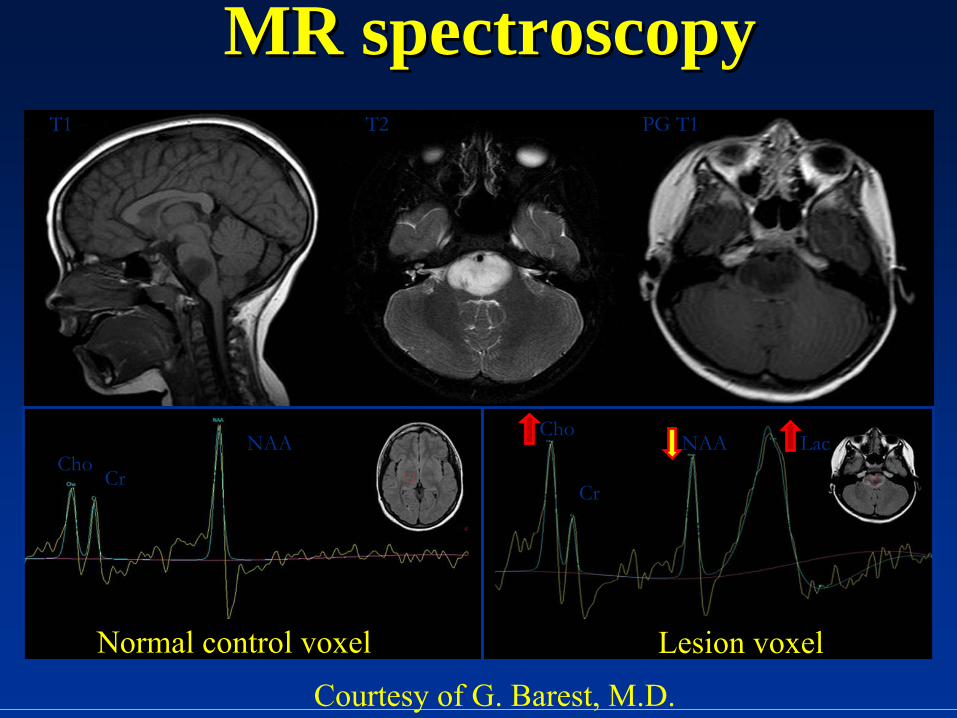
MR spectroscopyMR spectroscopy
Normal control voxel Lesion voxel
ChoCr
NAACho
Cr
NAA Lac
T1 T2 PG T1
Courtesy of G. Barest, M.D.
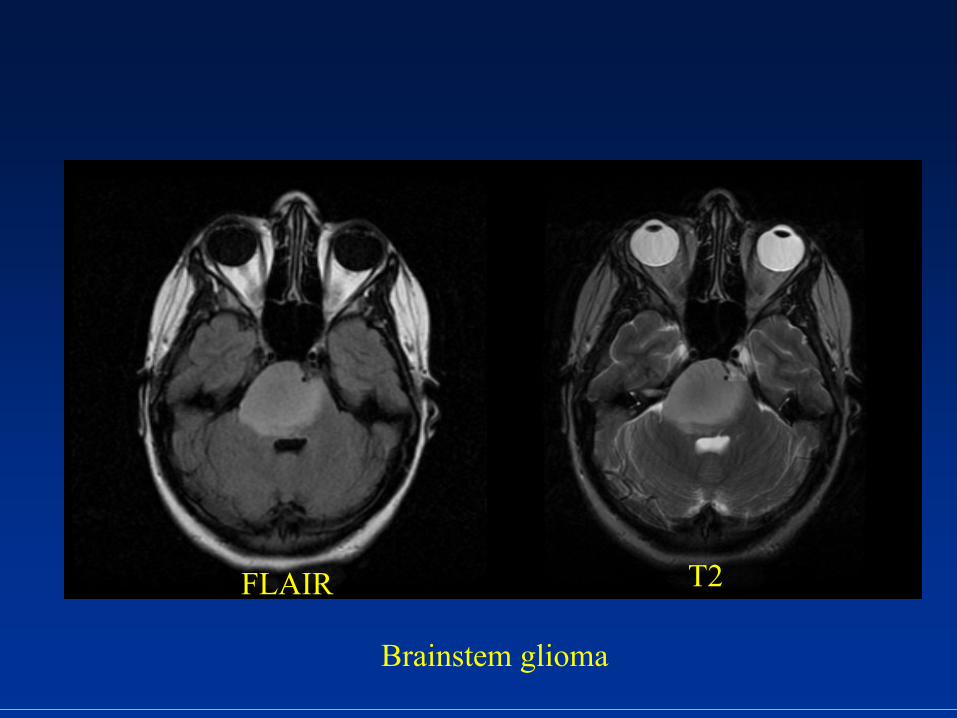
Brainstem glioma
FLAIR T2
Post contrast T1
SupratentorialSupratentorial TumorsTumors AstrocytomaAstrocytoma
••
30% of hemispheric tumors. Most common cerebral 30% of hemispheric tumors. Most common cerebral hemispheric tumorhemispheric tumor
••
Peak incidence at 7Peak incidence at 7--8yrs age8yrs age••
Slight male predominanceSlight male predominance••
Low grade Low grade astrocytomasastrocytomas
more common more common ••
GlioblastomaGlioblastoma
MultiformeMultiforme
(GBM) (GBM) ––
WHO IV/IV ~ 20%WHO IV/IV ~ 20%••
Typically involve basal ganglia, thalamusTypically involve basal ganglia, thalamus••
Can be multiCan be multi--centriccentric••
Clinical: Seizures, focal neurologic deficits, headachesClinical: Seizures, focal neurologic deficits, headaches

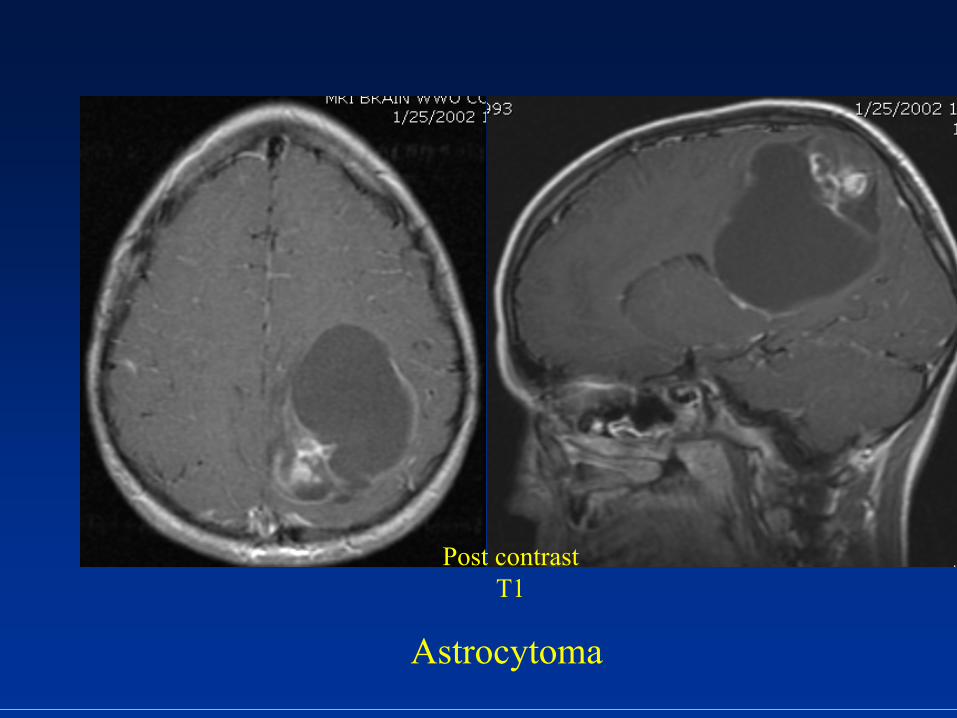
SupratentorialSupratentorial TumorsTumors AstrocytomasAstrocytomas
Imaging findings:Imaging findings:
••
Can appear like JPA.Can appear like JPA.••
Solid tumors have variable degrees Solid tumors have variable degrees enhancementenhancement
••
Pilocytic
Pilocytic astrocytomas astrocytomas ��� T2, ��� T2, FLAIR signal but minimal FLAIR signal but minimal surrounding edema.surrounding edema.
•• Low grade: Little to no Low grade: Little to no enhancementenhancement
••
High grade: Heterogeneous with High grade: Heterogeneous with areas of necrosisareas of necrosis
FLAIR
Astrocytoma
Post contrast T1
SupratentorialSupratentorial TumorsTumorsOther less common Other less common astrocytomasastrocytomas::
••
SubependymalSubependymal
Giant cell (SGCA): Giant cell (SGCA): ••
Associated with tuberous sclerosisAssociated with tuberous sclerosis••
Low gradeLow grade••
Arises near foramen of Arises near foramen of MonroMonro••
HydrocephalusHydrocephalus
••
PleomorphicPleomorphic
XanthoastrocytomaXanthoastrocytoma
(PXA):(PXA):••
Similar to Similar to DesmoplasticDesmoplastic
Infantile Infantile GangliogliomaGanglioglioma
(DIG); low grade(DIG); low grade••
Peripheral cerebral hemispherePeripheral cerebral hemisphere••
Typically in adolescents, young adultsTypically in adolescents, young adults
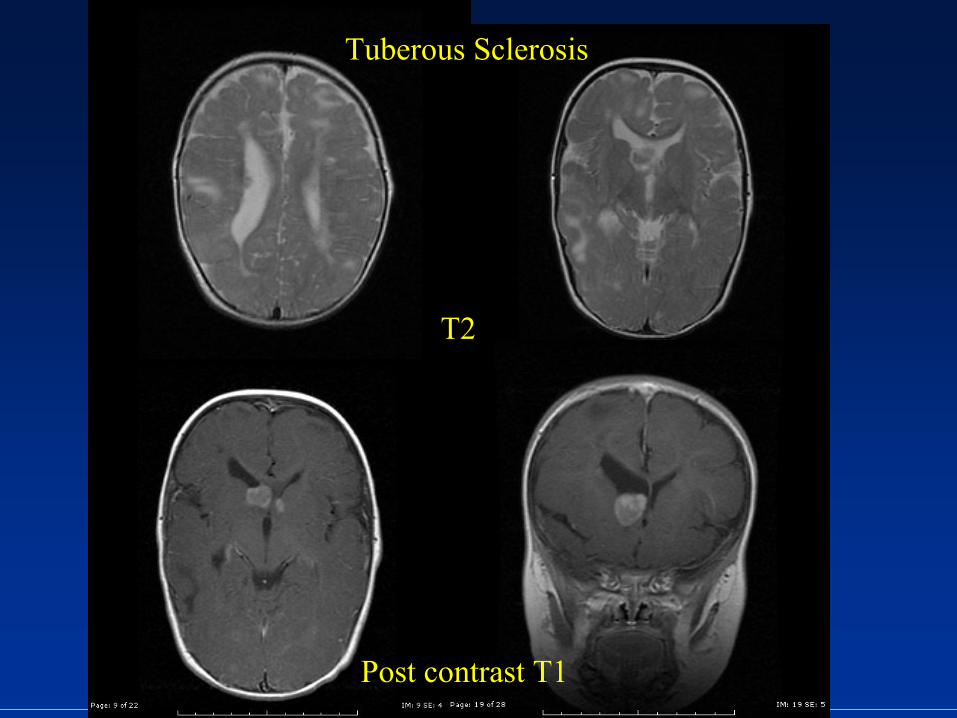
Tuberous Sclerosis
T2
Post contrast T1

SupratentorialSupratentorial TumorsTumors EpendymomaEpendymoma
••
30% of 30% of ependymomasependymomas••
Peak incidence between 1Peak incidence between 1--5yrs age5yrs age••
HistologicallyHistologically
similar to similar to infratentorialinfratentorial
ependymomasependymomas••
Typically in Typically in periventricularperiventricular
white matter and NOT white matter and NOT intraventricularintraventricular
(metastatic spread uncommon)(metastatic spread uncommon)
••
Clinical: Increased intracranial pressure, ataxia, Clinical: Increased intracranial pressure, ataxia, seizuresseizures
••
5 yr survival: 80% w/total resection 5 yr survival: 80% w/total resection 4040--60% w/subtotal resection60% w/subtotal resection
SupratentorialSupratentorial TumorsTumors EpendymomaEpendymoma
Imaging findings:Imaging findings:
••
Variable appearance on CT Variable appearance on CT or MRIor MRI
••
Slightly Slightly hyperdensehyperdense
on CT on CT w/calcifications (50%)w/calcifications (50%)
••
Heterogeneous enhancement Heterogeneous enhancement with cystic areaswith cystic areas
••
Typically seen in frontal lobeTypically seen in frontal lobe
SupratentorialSupratentorial TumorsTumors DesmoplasticDesmoplastic
Infantile Infantile
GangliogliomaGanglioglioma••
Arises from Arises from subpialsubpial
astrocytesastrocytes••
Found between 1Found between 1--24 months age w/peak at 324 months age w/peak at 3--6 6 months. Occasionally seen from 5months. Occasionally seen from 5--17yrs17yrs
••
M/F: 1.7/1M/F: 1.7/1••
Cortically based tumor noduleCortically based tumor nodule••
Clinical: �Head size, bulging fontanels, seizuresClinical: �Head size, bulging fontanels, seizures••
Greater then 75% survival after 15yrs w/complete Greater then 75% survival after 15yrs w/complete resectionresection
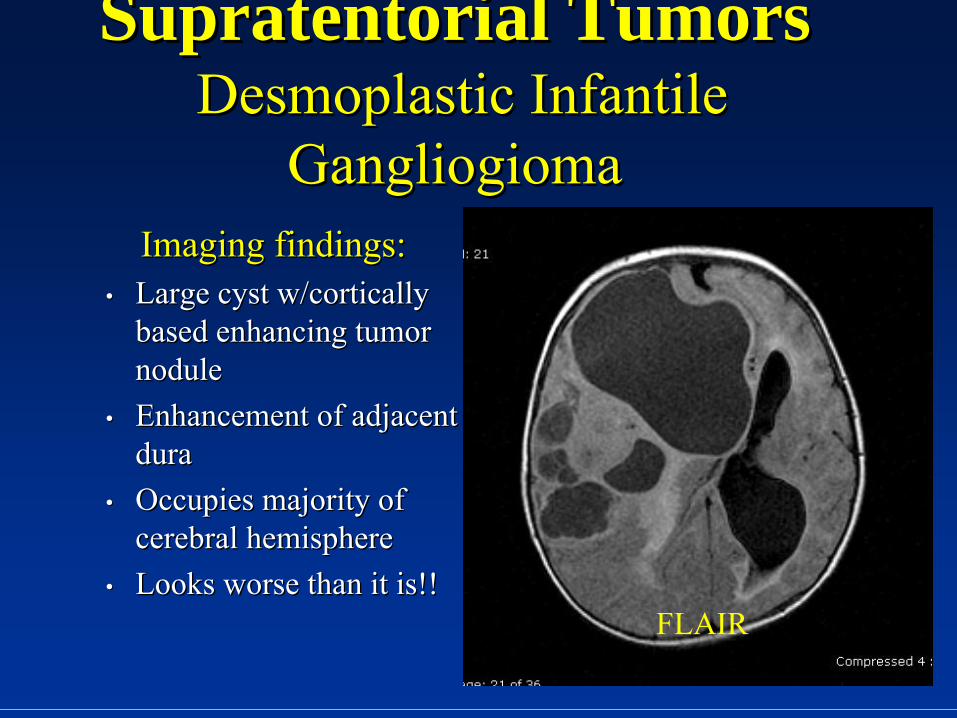
SupratentorialSupratentorial TumorsTumors DesmoplasticDesmoplastic
Infantile Infantile
GangliogiomaGangliogiomaImaging findings:Imaging findings:
••
Large cyst w/cortically Large cyst w/cortically based enhancing tumor based enhancing tumor nodule nodule
••
Enhancement of adjacent Enhancement of adjacent duradura
••
Occupies majority of Occupies majority of cerebral hemispherecerebral hemisphere
••
Looks worse than it is!!Looks worse than it is!!FLAIR
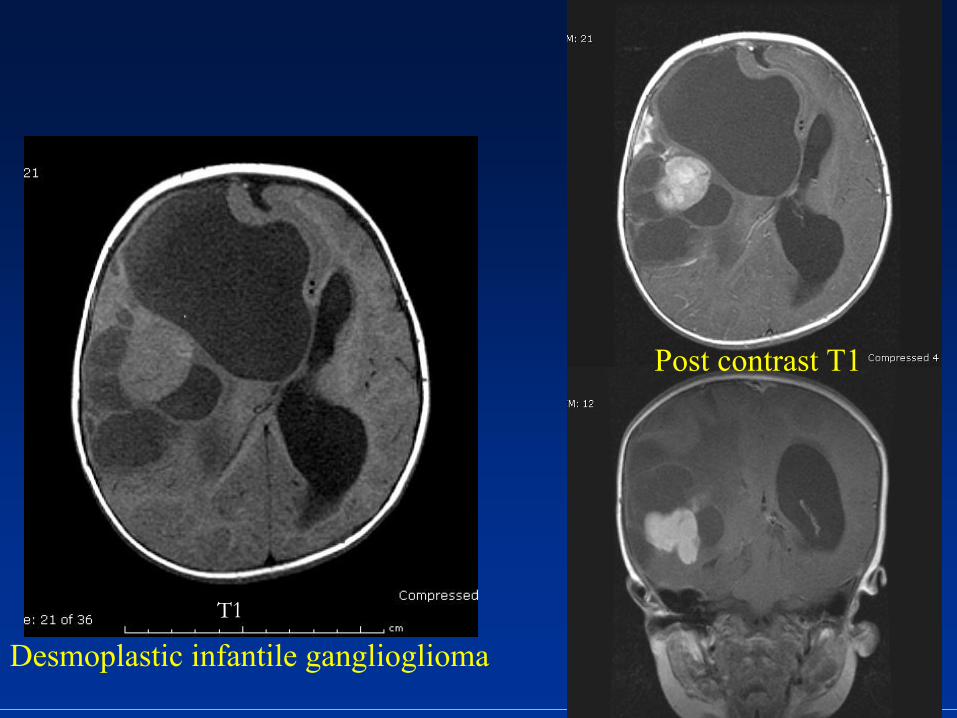
Desmoplastic
infantile gangliogliomaT1
Post contrast T1
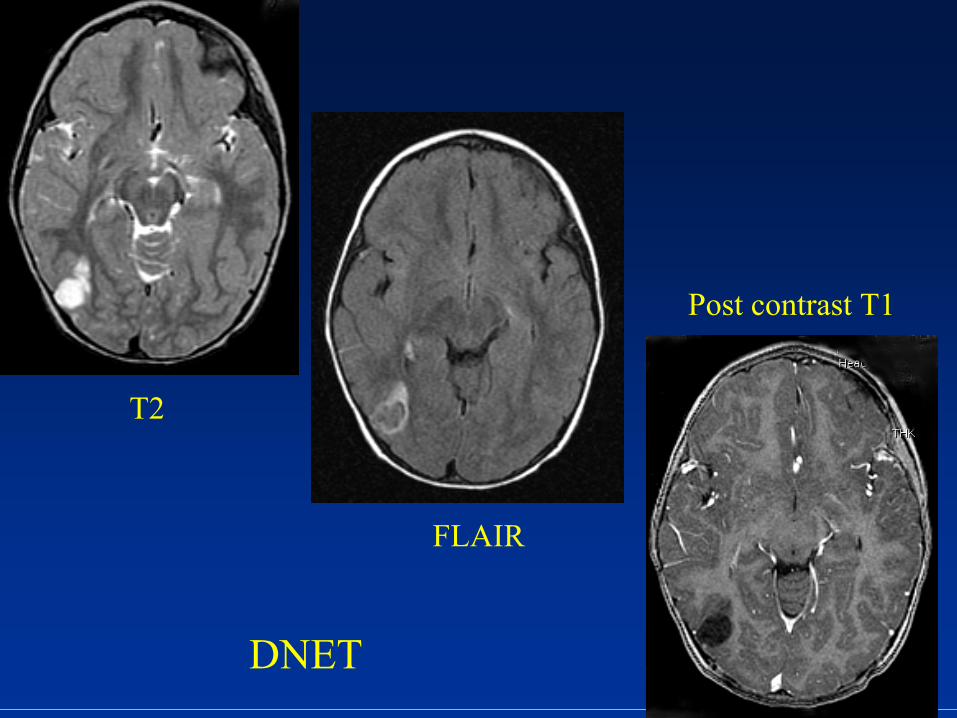
SupratentorialSupratentorial TumorsTumors DysembryoplasticDysembryoplastic
NeuroepithelialNeuroepithelial
Tumor (DNET)Tumor (DNET)••
Benign tumor of cerebral cortexBenign tumor of cerebral cortex
••
Cause of 20% cases of medically refractory Cause of 20% cases of medically refractory epilepsyepilepsy
••
60% in temporal lobe, 30% frontal lobe60% in temporal lobe, 30% frontal lobe••
Solid and cystic tumorsSolid and cystic tumors
••
Scalloping of inner table skullScalloping of inner table skull••
Associated w/cortical Associated w/cortical dysplasiadysplasia
••
Slow to No growth!Slow to No growth!
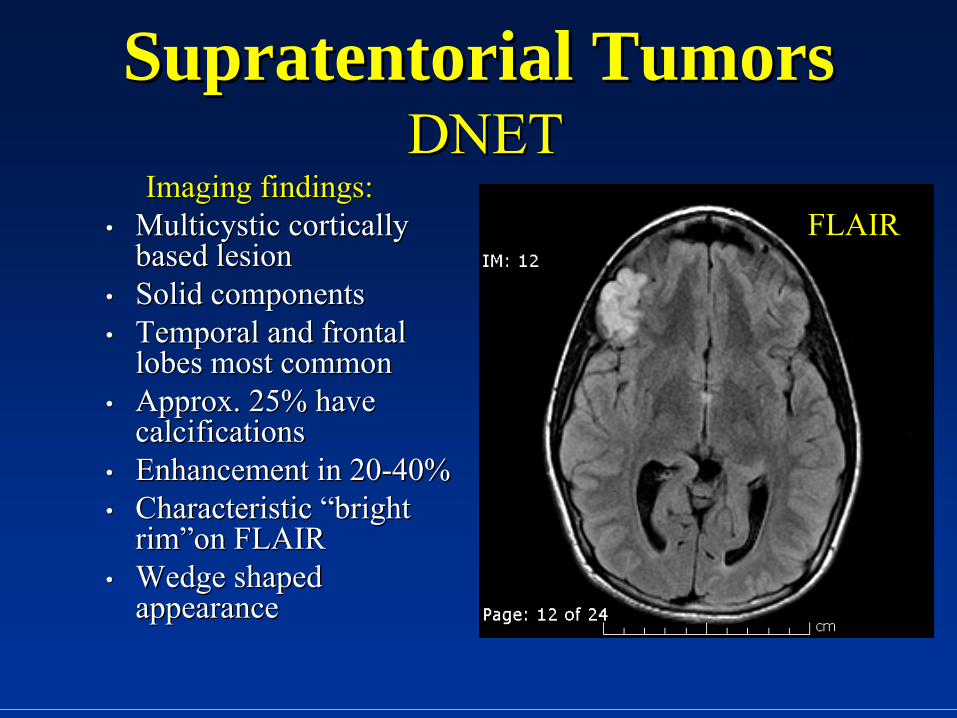
SupratentorialSupratentorial TumorsTumors DNETDNET
Imaging findings:Imaging findings:••
MulticysticMulticystic
cortically cortically based lesionbased lesion
••
Solid componentsSolid components••
Temporal and frontal Temporal and frontal lobes most commonlobes most common
••
Approx. 25% have Approx. 25% have calcificationscalcifications
••
Enhancement in 20Enhancement in 20--40%40%••
Characteristic “bright Characteristic “bright rim”on FLAIRrim”on FLAIR
••
Wedge shaped Wedge shaped appearanceappearance
FLAIR
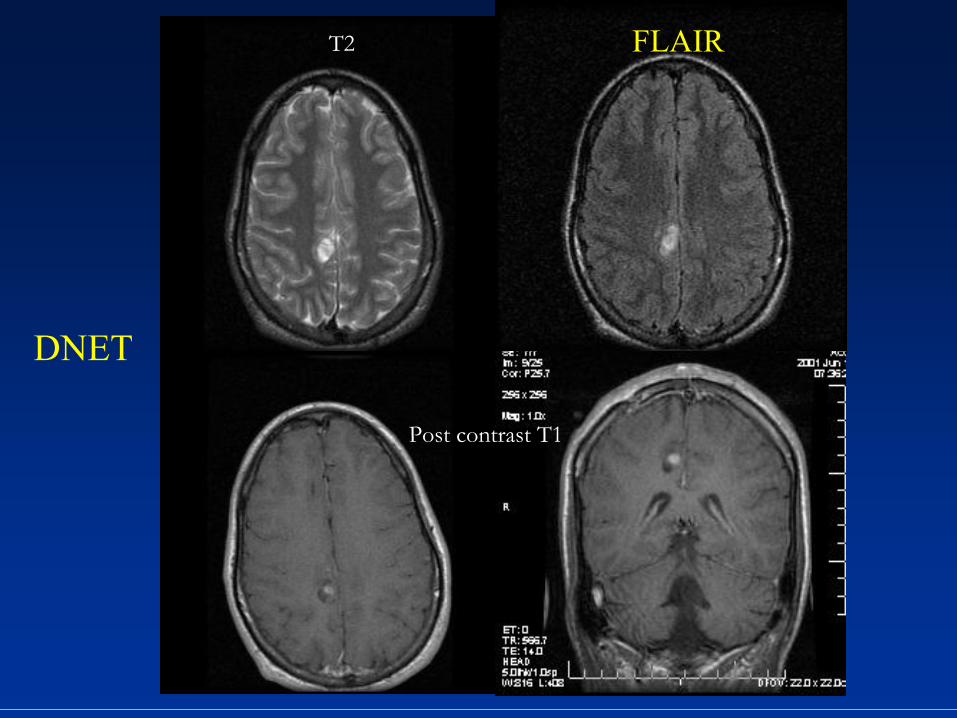
DNET
T2 FLAIR
Post contrast T1
DNET
T2
FLAIR
Post contrast T1
SupratentorialSupratentorial TumorsTumors GangliogliomaGanglioglioma//GangliocytomaGangliocytoma
••
Mixed neuronalMixed neuronal--glialglial
tumorstumors••
3% brain tumors in children3% brain tumors in children
••
Found in adolescentsFound in adolescents••
Associated with Associated with mesialmesial
temporal sclerosistemporal sclerosis
••
Most common in temporal, parietal, frontal lobesMost common in temporal, parietal, frontal lobes••
Difference between GG and GC is histologicalDifference between GG and GC is histological
••
Clinical: Partial complex seizuresClinical: Partial complex seizures
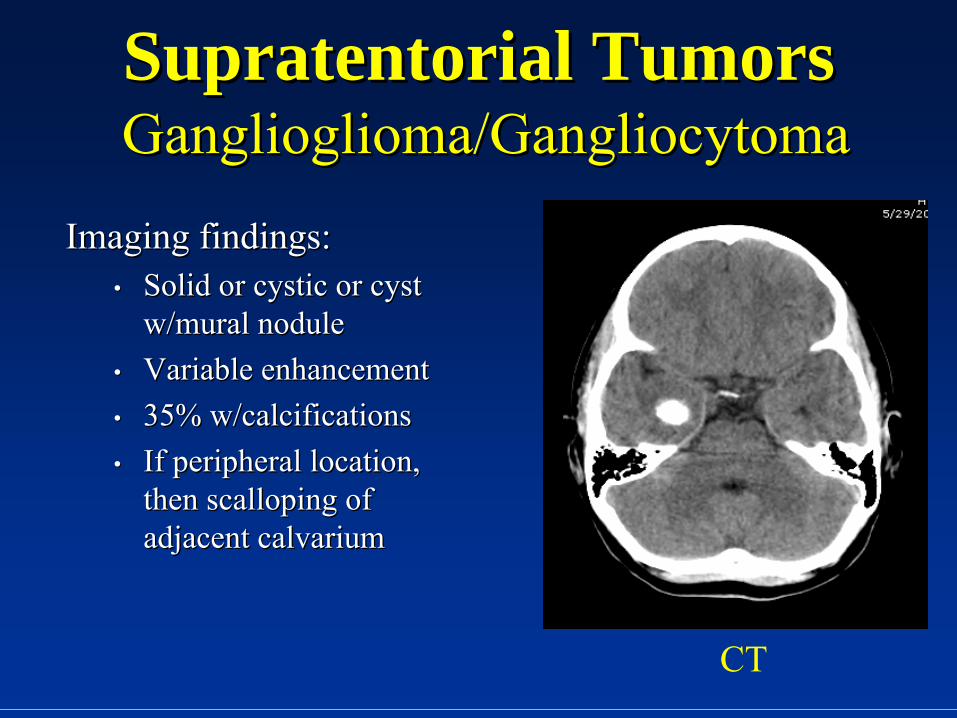
SupratentorialSupratentorial TumorsTumors GangliogliomaGanglioglioma//GangliocytomaGangliocytoma
Imaging findings:Imaging findings:••
Solid or cystic or cyst Solid or cystic or cyst w/mural nodulew/mural nodule
••
Variable enhancementVariable enhancement••
35% w/calcifications35% w/calcifications••
If peripheral location, If peripheral location, then scalloping of then scalloping of adjacent adjacent calvariumcalvarium
CT
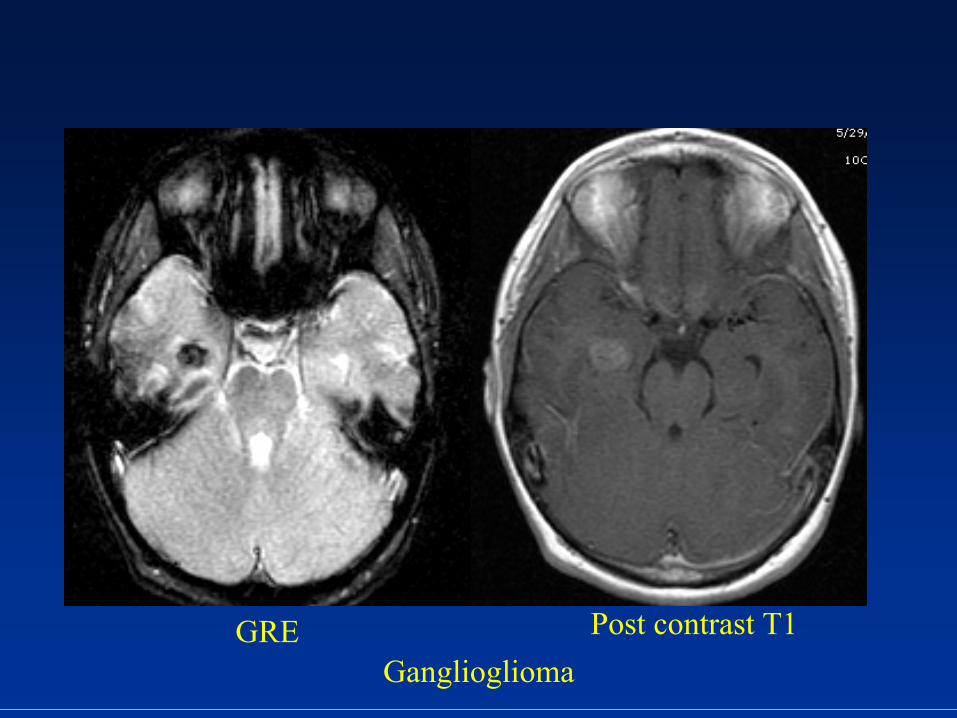
GangliogliomaGRE Post contrast T1
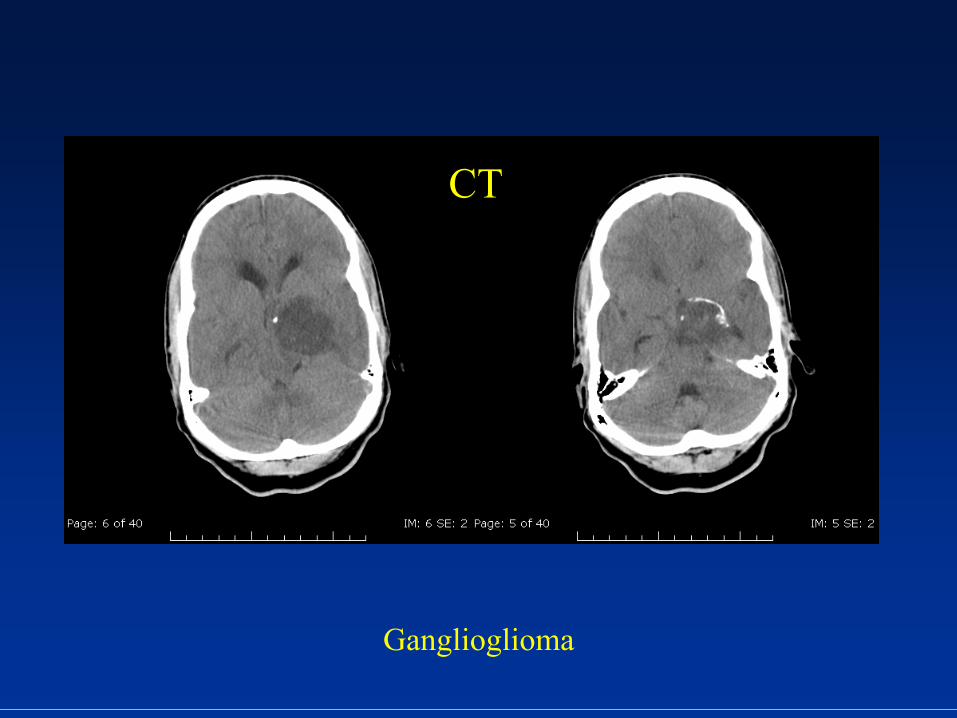
Ganglioglioma
CT
SupratentorialSupratentorial TumorsTumors TeratomaTeratoma
••
22--5% of tumors in children less then 155% of tumors in children less then 15••
Midline lesion typically in pineal gland, third Midline lesion typically in pineal gland, third ventricleventricle
••
More common in malesMore common in males••
Most are benignMost are benign
••
Clinical: HydrocephalusClinical: Hydrocephalus
SupratentorialSupratentorial TumorsTumors TeratomasTeratomas
Imaging findings:Imaging findings:••
Midline mass with Midline mass with calcifications and fatcalcifications and fat
••
Enhancement of soft Enhancement of soft tissue componentstissue components
••
Malignant Malignant teratomasteratomas have more have more vasogenicvasogenic edema, irregular, less edema, irregular, less
well definedwell defined
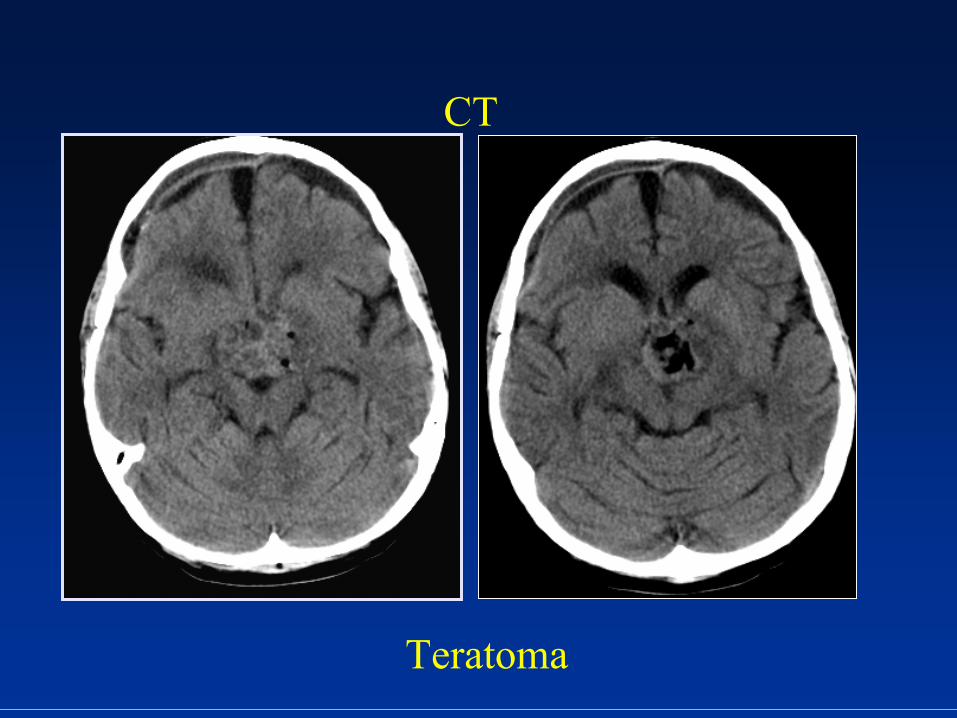
Teratoma
CT
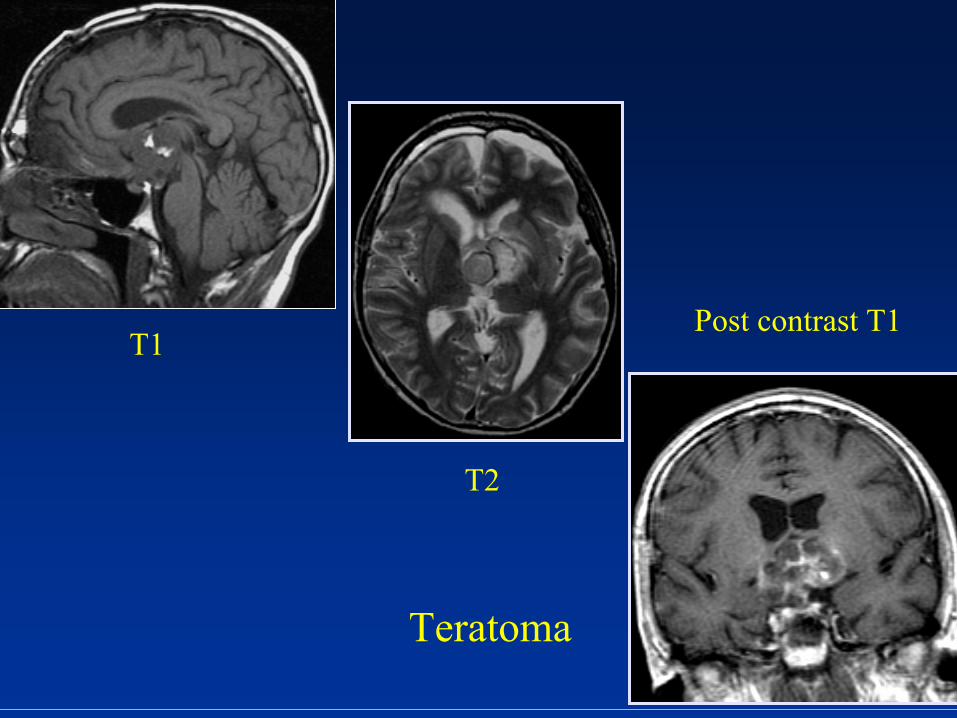
Teratoma
T1
T2
Post contrast T1
SupratentorialSupratentorial TumorsTumors
ExtraExtra--axialaxial••
Choroid plexus Choroid plexus papillomapapilloma/carcinoma/carcinoma••
LangerhansLangerhans
cell cell histiocytosishistiocytosis••
EpidermoidEpidermoid//DermoidDermoid••
ArachnoidArachnoid
cystcyst••
MetastasisMetastasis
SupratentorialSupratentorial TumorsTumors Choroid plexus Choroid plexus papillomapapilloma/carcinoma/carcinoma
••
Arise from epithelium of choroid plexusArise from epithelium of choroid plexus••
5% of 5% of supratentorialsupratentorial
tumorstumors••
Typically age 1Typically age 1--5yrs5yrs••
Male predominanceMale predominance••
CP carcinomas are 30CP carcinomas are 30--40% choroid plexus tumors40% choroid plexus tumors••
Most common in Most common in trigonetrigone
of left lateral ventricleof left lateral ventricle••
CPC more irregular and invasive then CPP but CPC more irregular and invasive then CPP but diagnosis is histologicaldiagnosis is histological
••
Clinical: HydrocephalusClinical: Hydrocephalus
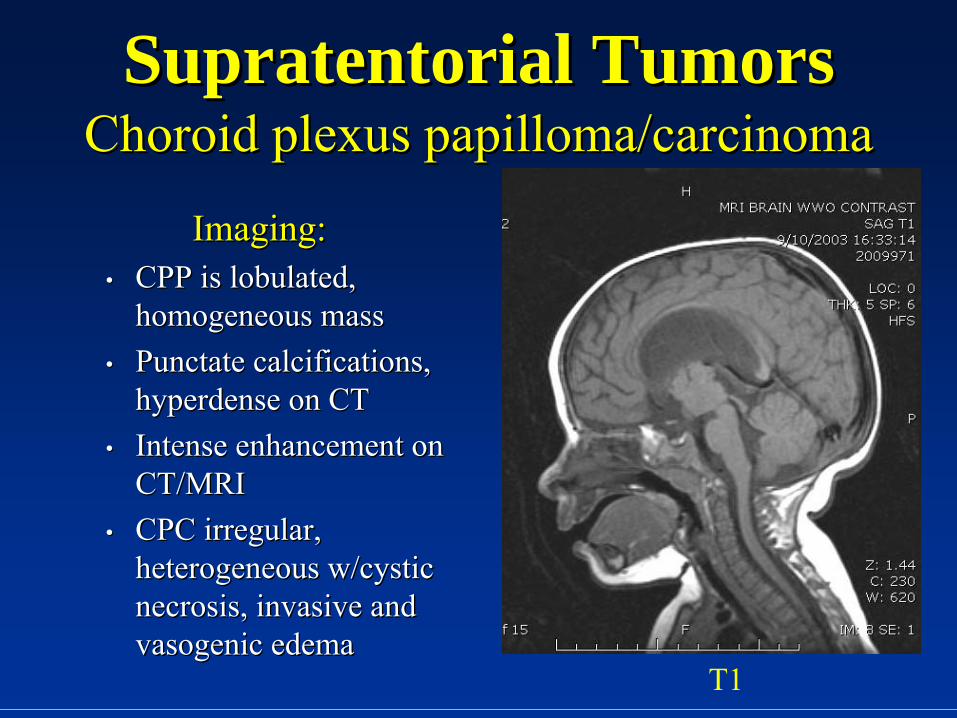
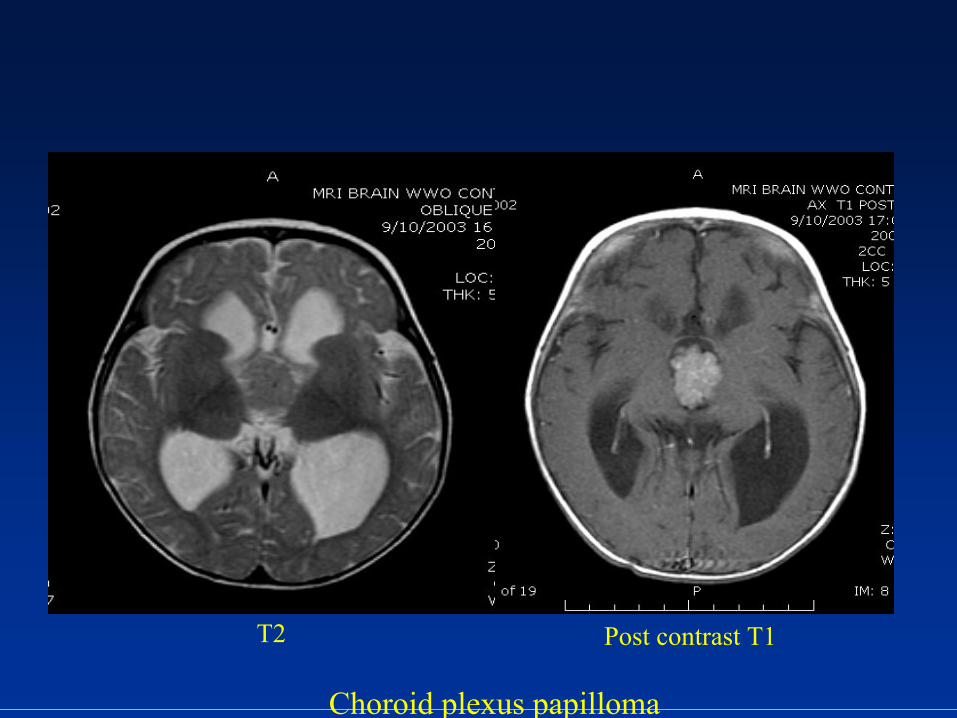
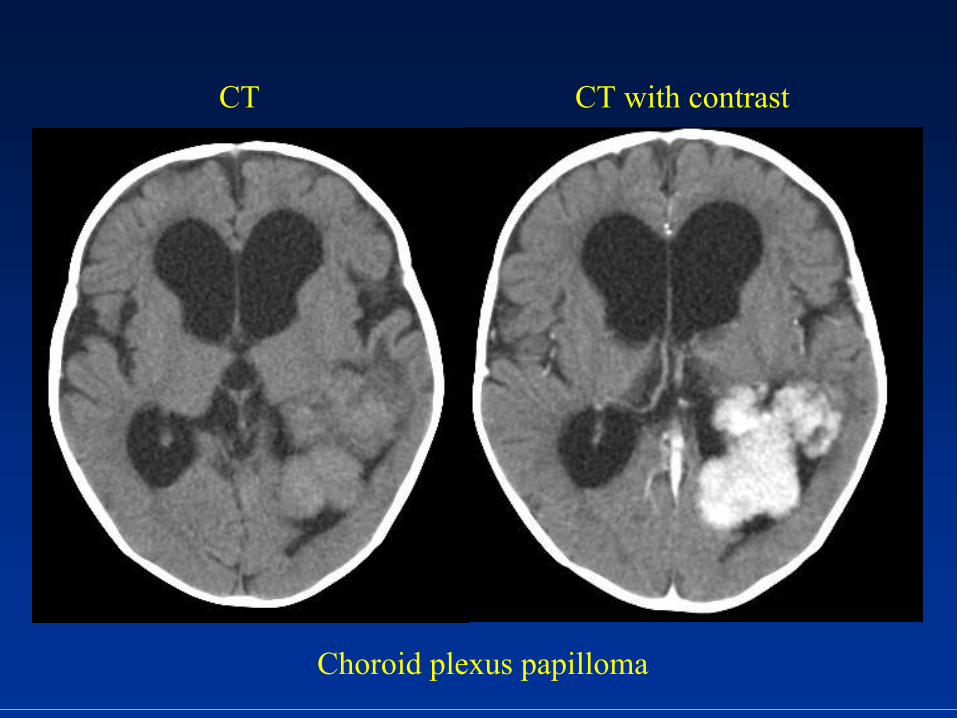
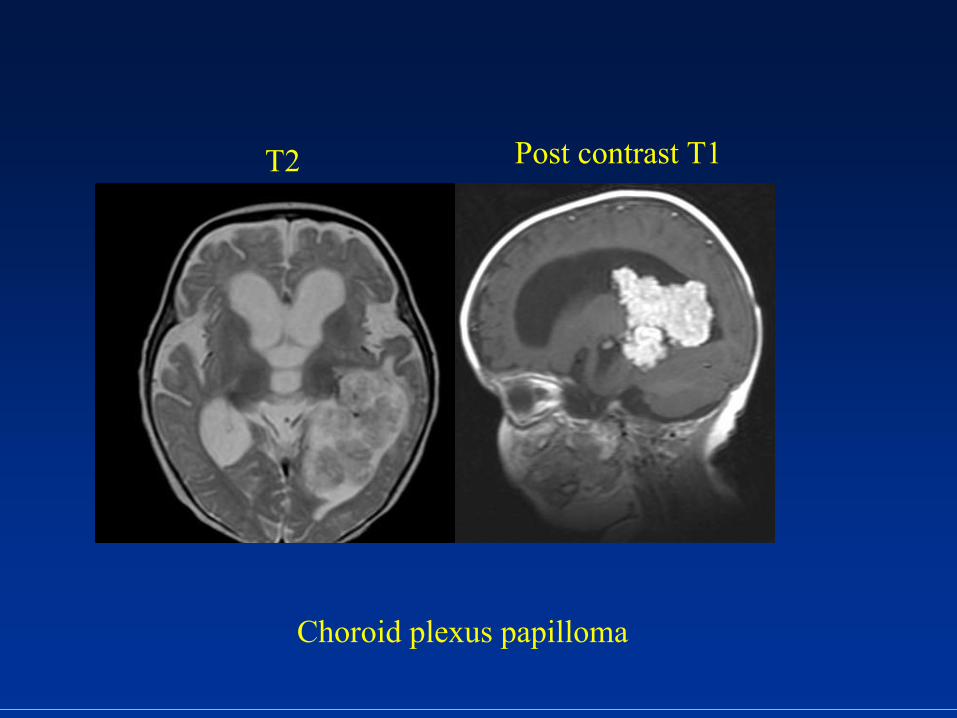
SupratentorialSupratentorial TumorsTumors Choroid plexus Choroid plexus papillomapapilloma/carcinoma/carcinoma
Imaging:Imaging:••
CPP is CPP is lobulatedlobulated, , homogeneous masshomogeneous mass
••
PunctatePunctate
calcifications, calcifications, hyperdensehyperdense
on CTon CT
••
Intense enhancement on Intense enhancement on CT/MRICT/MRI
••
CPC irregular, CPC irregular, heterogeneous w/cystic heterogeneous w/cystic necrosis, invasive and necrosis, invasive and vasogenicvasogenic
edemaedema
T1
T2 Post contrast T1
Choroid plexus papilloma
Choroid plexus papilloma
CT CT with contrast
Choroid plexus papilloma
T2 Post contrast T1
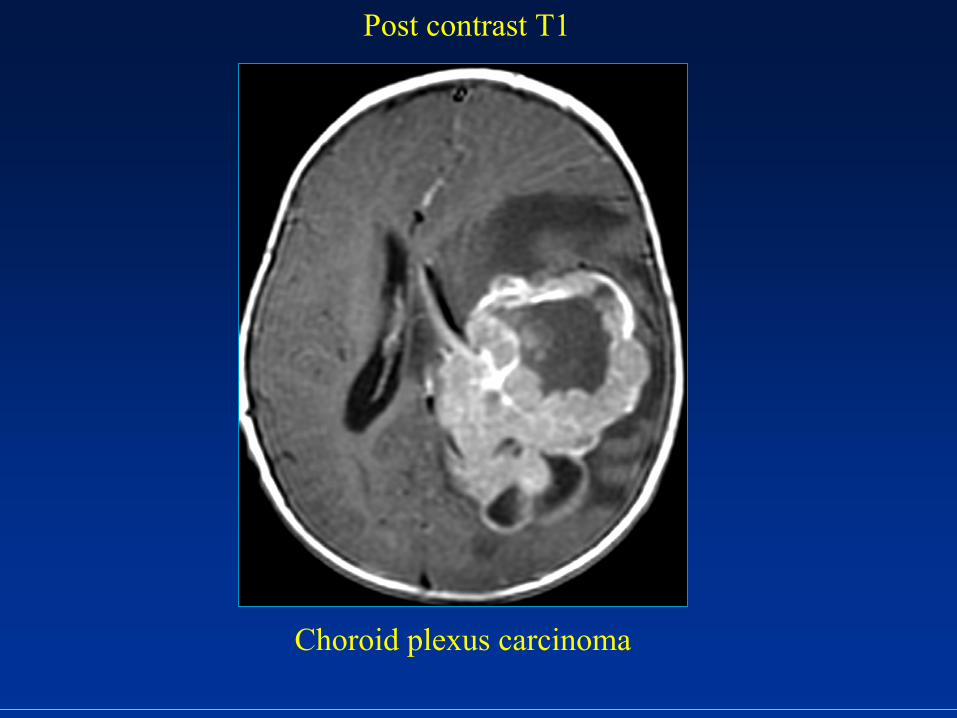
Choroid plexus carcinoma
Post contrast T1
SupratentorialSupratentorial TumorsTumors LangerhansLangerhans
cell cell histiocytosishistiocytosis
••
LCH disorder of LCH disorder of reticuloendothelialreticuloendothelial
systemsystem••
Rarely involves CNSRarely involves CNS
••
In In calvariumcalvarium, , expansileexpansile
erosive soft tissue erosive soft tissue mass w/”beveled edges” and intense mass w/”beveled edges” and intense enhancementenhancement
••
IntracraniallyIntracranially, similar to gray matter?????, similar to gray matter?????••
MRI: MRI: hypointensehypointense
on FLAIR and T2; intense on FLAIR and T2; intense
enhancementenhancement
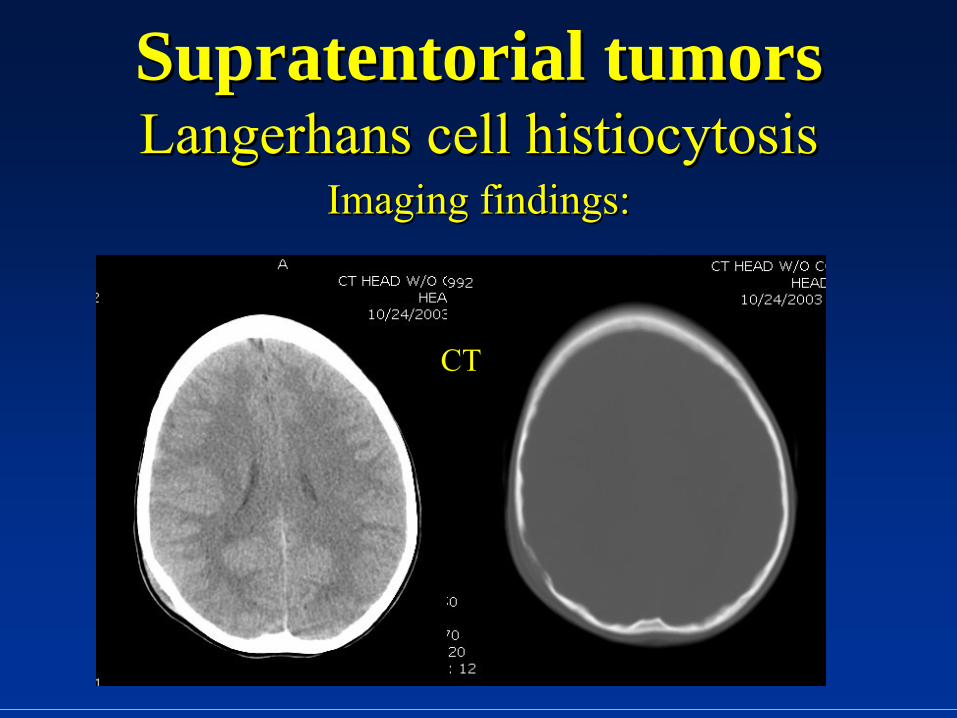
SupratentorialSupratentorial tumorstumors LangerhansLangerhans
cell cell histiocytosishistiocytosis
Imaging findings:Imaging findings:
CT
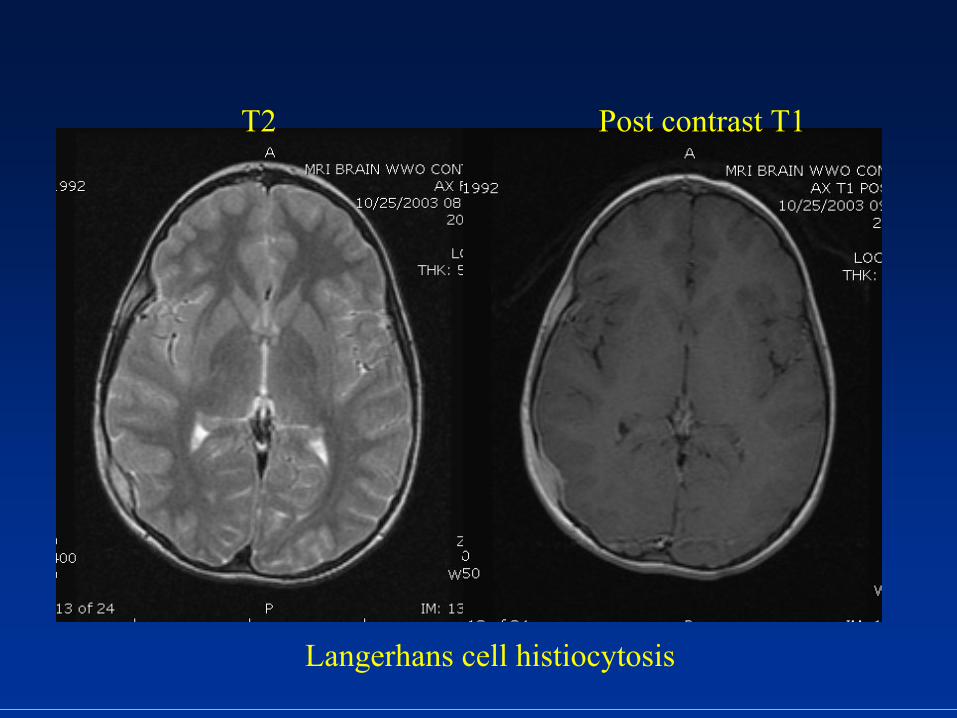
Langerhans
cell histiocytosis
T2 Post contrast T1
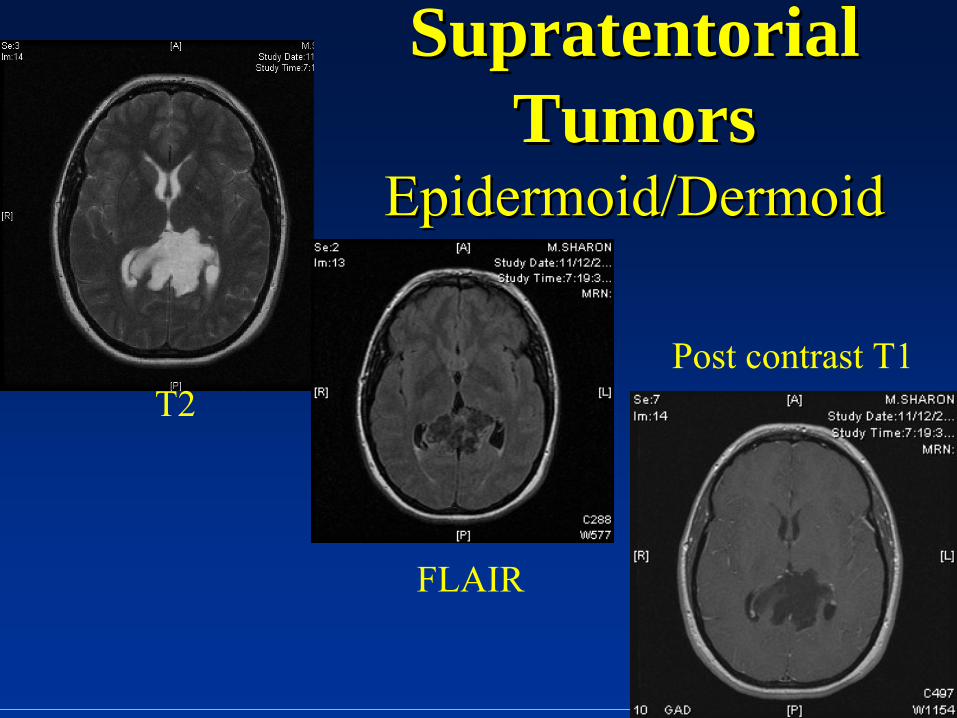
SupratentorialSupratentorial TumorsTumors
EpidermoidEpidermoid//DermoidDermoid
T2
FLAIR
Post contrast T1
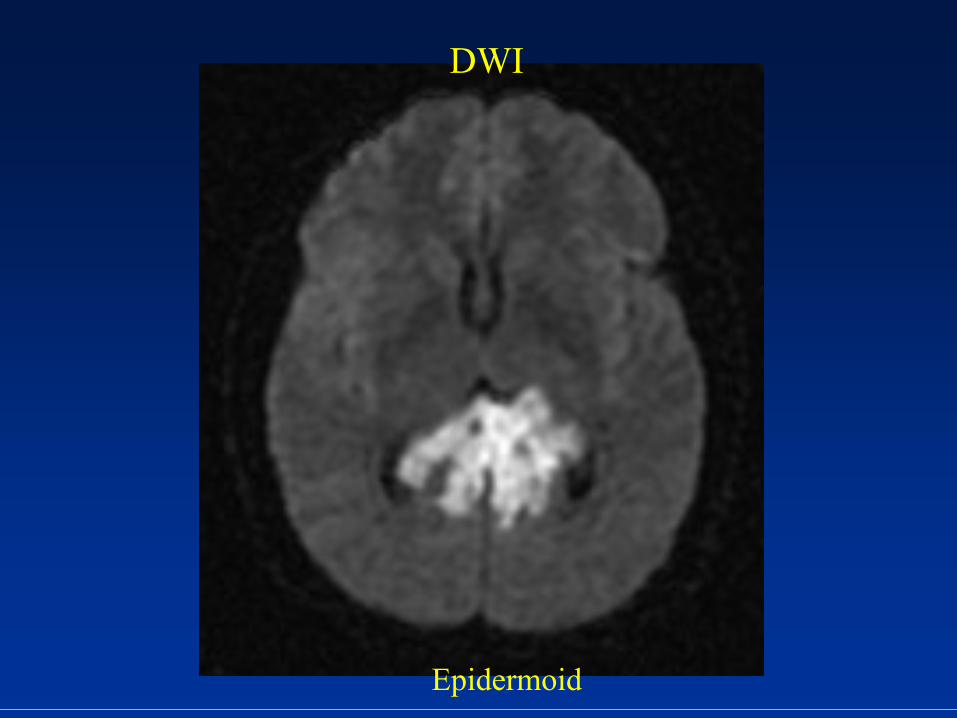
Epidermoid
DWI
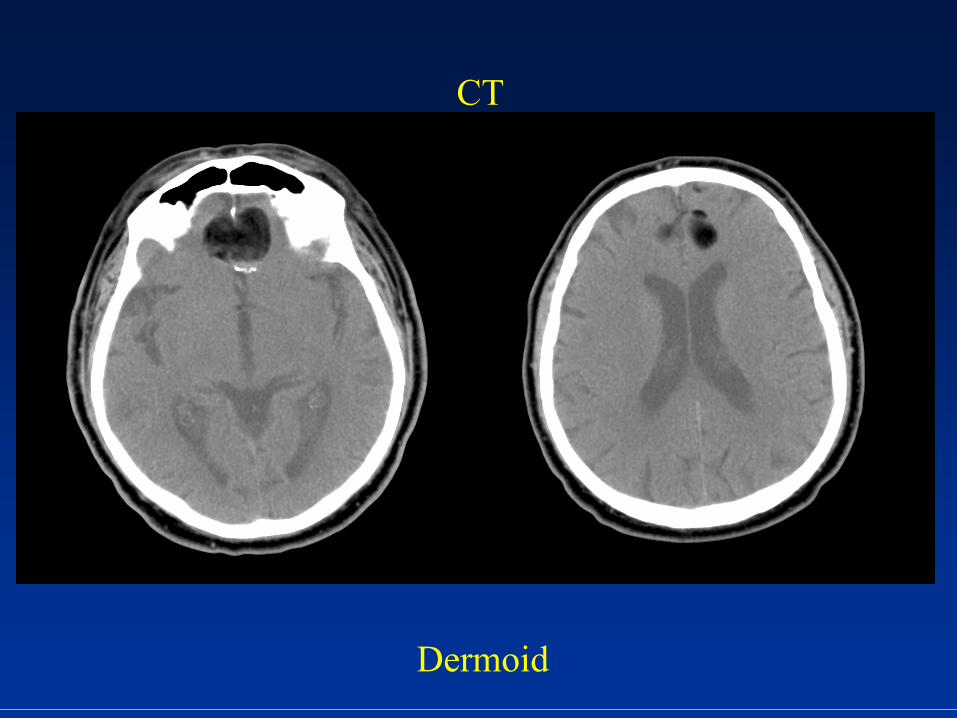
Dermoid
CT
SupratentorialSupratentorial TumorsTumorsSellarSellar//SuprasellarSuprasellar
••
CraniopharyngiomaCraniopharyngioma••
AstrocytomaAstrocytoma••
RathkeRathke
cleft cystcleft cyst••
Germ cell tumorGerm cell tumor••
Hypothalamic Hypothalamic hamartomahamartoma••
LangerhansLangerhans
cell cell histioctyosishistioctyosis••
Pituitary adenomaPituitary adenoma
Common Presentations of Common Presentations of Hypothalamic and Hypothalamic and Pituitary LesionsPituitary Lesions
••
HypopituitarismHypopituitarism
––
craniopharyngiomacraniopharyngioma••
Diabetes Diabetes insipidusinsipidus
––
LCH, GCT, LCH, GCT, craniocranio
••
Precocious puberty Precocious puberty ––
hamartomahamartoma
of tuber of tuber cinereumcinereum, hypothalamic , hypothalamic gliomaglioma
••
Amenorrhea Amenorrhea ––
pituitary adenoma, pituitary adenoma, RathkeRathke cleft cystcleft cyst
SupratentorialSupratentorial TumorsTumors CraniopharyngiomasCraniopharyngiomas
••
Thought to arise from remnant of Thought to arise from remnant of craniopharyngealcraniopharyngeal
ductduct••
AdamantinomatousAdamantinomatous
(children) and papillary (adults) (children) and papillary (adults) typestypes
••
15% 15% supratentorialsupratentorial
tumors, 50% tumors, 50% suprasellarsuprasellar
tumorstumors••
2 peaks: 102 peaks: 10--14 yrs age; 414 yrs age; 4thth
to 6to 6thth
decade of lifedecade of life
••
Most common in malesMost common in males••
Clinical: Headaches, visual disturbances, diabetes Clinical: Headaches, visual disturbances, diabetes insipidusinsipidus
••
Diff. Diff. DxDx.: .: RathkeRathke
cleft cysts, hemorrhagic pituitary cleft cysts, hemorrhagic pituitary adenomasadenomas
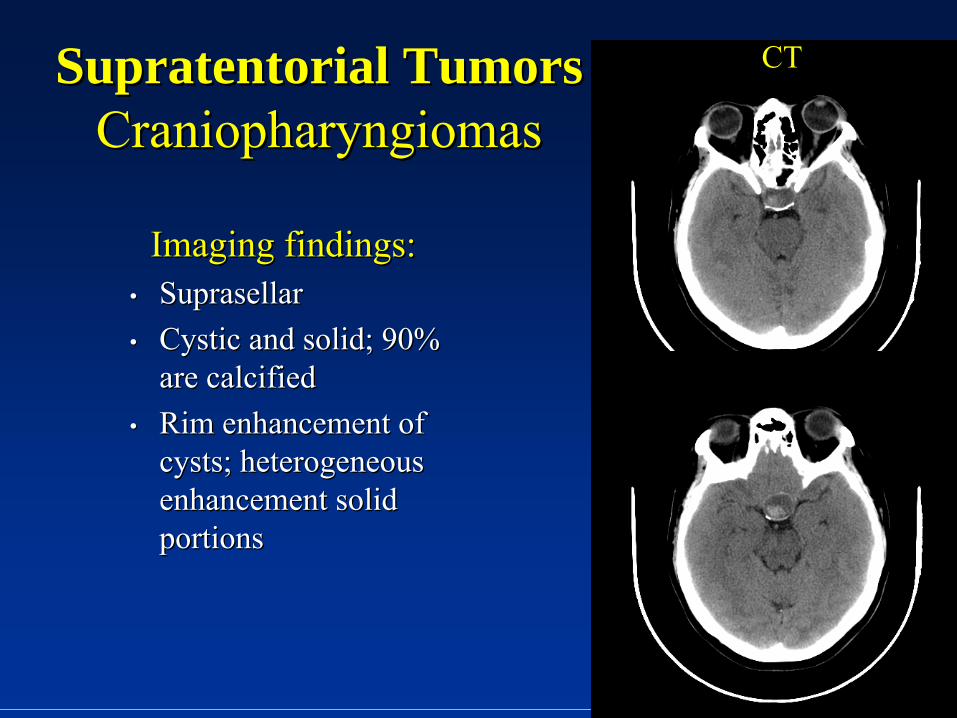
SupratentorialSupratentorial TumorsTumors CraniopharyngiomasCraniopharyngiomas
Imaging findings:Imaging findings:••
SuprasellarSuprasellar••
Cystic and solid; 90% Cystic and solid; 90% are calcifiedare calcified
••
Rim enhancement of Rim enhancement of cysts; heterogeneous cysts; heterogeneous enhancement solid enhancement solid portionsportions
CT

Craniopharyngioma
T2 GRE

Post contrast T1T1Craniopharyngiom
SupratentorialSupratentorial TumorsTumors RathkeRathke
Cleft cystCleft cyst
••
Benign epithelial lined cyst in Benign epithelial lined cyst in sellasella••
Arises from remnants of Arises from remnants of RathkeRathke
pouchpouch••
Arises in pituitary gland with frequent Arises in pituitary gland with frequent suprasellarsuprasellar extensionextension
••
Rare in childrenRare in children••
Clinical: Clinical: ••
Typically asymptomaticTypically asymptomatic••
Symptomatic patients present with headaches, pituitary Symptomatic patients present with headaches, pituitary dysfunctiondysfunction
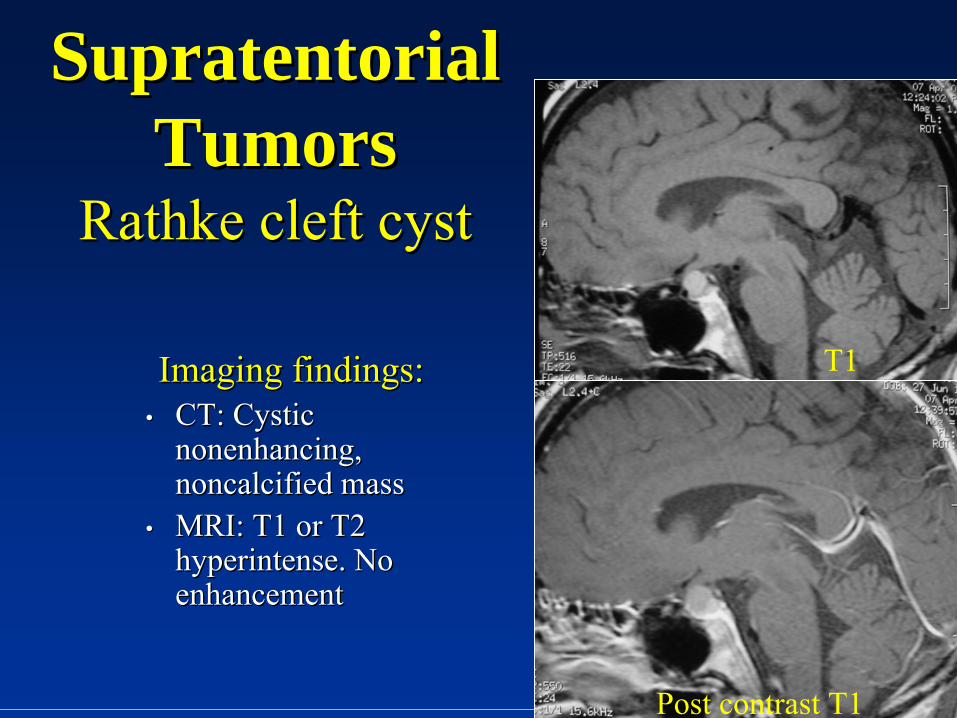
SupratentorialSupratentorial TumorsTumors
RathkeRathke
cleft cystcleft cyst
Imaging findings:Imaging findings:••
CT: Cystic CT: Cystic nonenhancingnonenhancing, , noncalcifiednoncalcified
massmass
••
MRI: T1 or T2 MRI: T1 or T2 hyperintensehyperintense. No . No enhancementenhancement
Post contrast T1
T1
SupratentorialSupratentorial TumorsTumors AstrocytomaAstrocytoma
••
SuprasellarSuprasellar
type arises from optic chiasm or type arises from optic chiasm or hypothalamushypothalamus
••
Many tumors in optic nerve are JPAMany tumors in optic nerve are JPA••
M=FM=F
••
Presents from 2Presents from 2--4yrs age4yrs age••
3030--50% have family history of NF150% have family history of NF1
••
Clinical: Hydrocephalus, decreased vision, Clinical: Hydrocephalus, decreased vision, pituitary dysfunction (short stature)pituitary dysfunction (short stature)
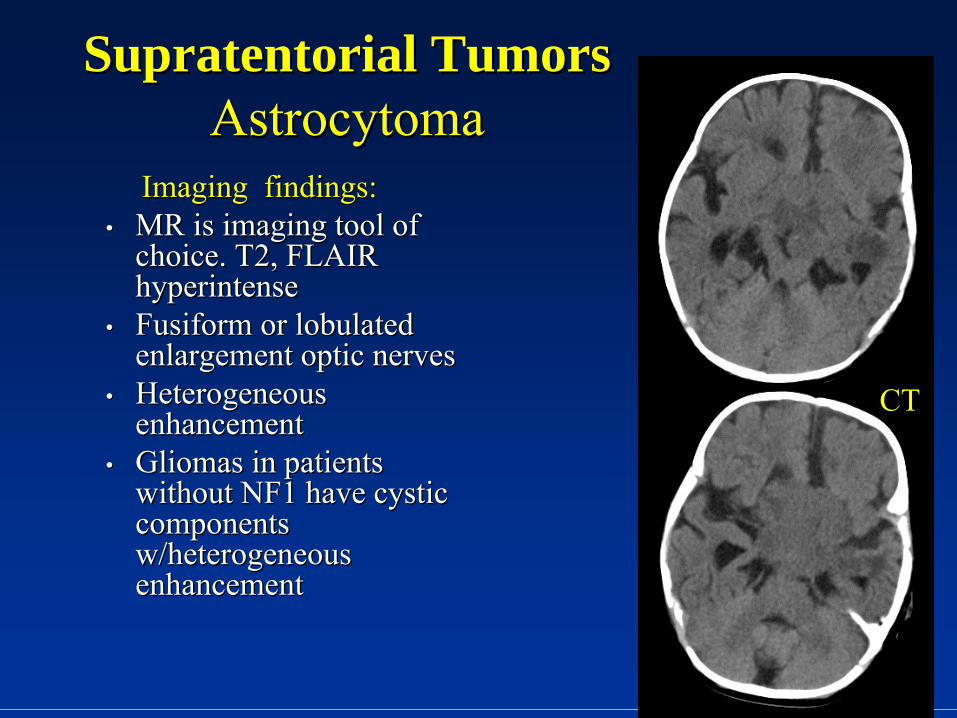
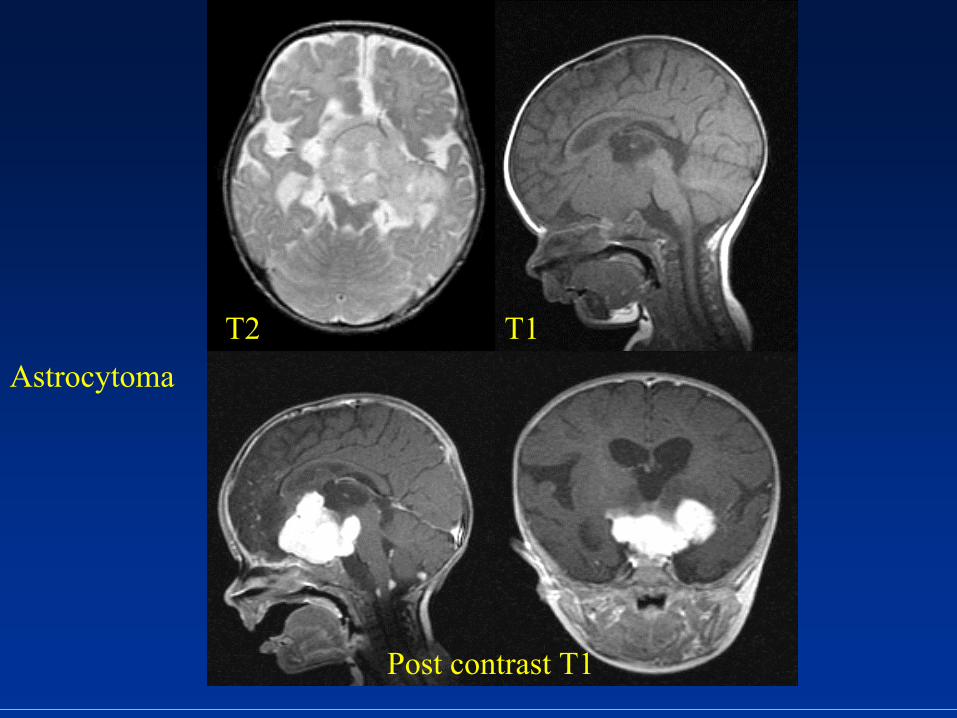
SupratentorialSupratentorial TumorsTumors AstrocytomaAstrocytoma
Imaging findings:Imaging findings:••
MR is imaging tool of MR is imaging tool of choice. T2, FLAIR choice. T2, FLAIR hyperintensehyperintense
••
FusiformFusiform
or or lobulatedlobulated enlargement optic nervesenlargement optic nerves
••
Heterogeneous Heterogeneous enhancementenhancement
••
GliomasGliomas
in patients in patients without NF1 have cystic without NF1 have cystic components components w/heterogeneous w/heterogeneous enhancementenhancement
CT
Post contrast T1
T2 T1Astrocytoma
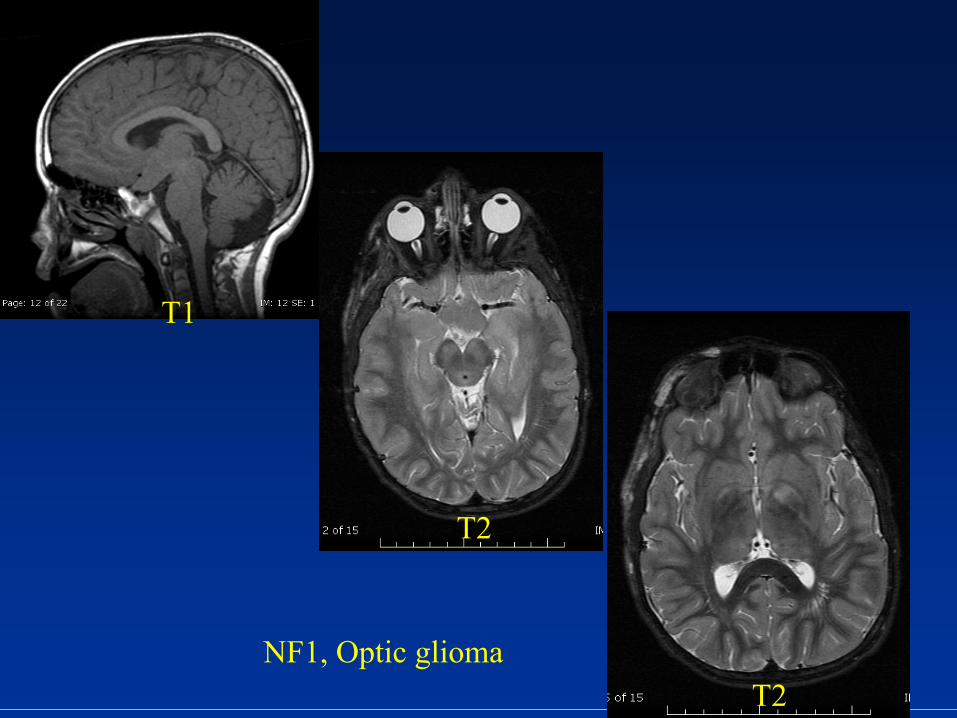
NF1, Optic glioma
T1
T2
T2
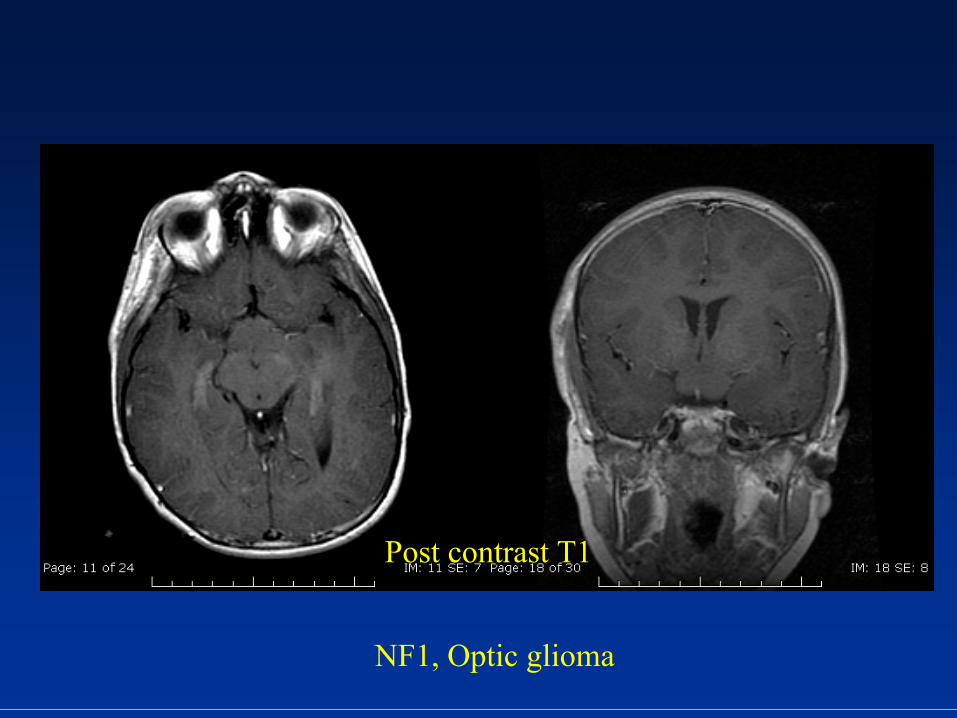
Post contrast T1
NF1, Optic glioma
SupratentorialSupratentorial TumorsTumors Germ cell tumorsGerm cell tumors
••
Originate in hypothalamus and extend into Originate in hypothalamus and extend into infundibuluminfundibulum
••
GerminomaGerminoma
most common most common histologichistologic
type.type.••
35% 35% suprasellarsuprasellar; 60% pineal; 60% pineal••
M=F in M=F in suprasellarsuprasellar
germinomasgerminomas
(10:1 in pineal (10:1 in pineal region tumors)region tumors)
••
Clinical: Typically present w/diabetes Clinical: Typically present w/diabetes insipidusinsipidus••
If child presents w/DI but imaging negative, 2 repeat If child presents w/DI but imaging negative, 2 repeat studies at 6 month intervals should be performed!!!! Initial studies at 6 month intervals should be performed!!!! Initial germinomagerminoma
may be too small for visualization!!!may be too small for visualization!!!
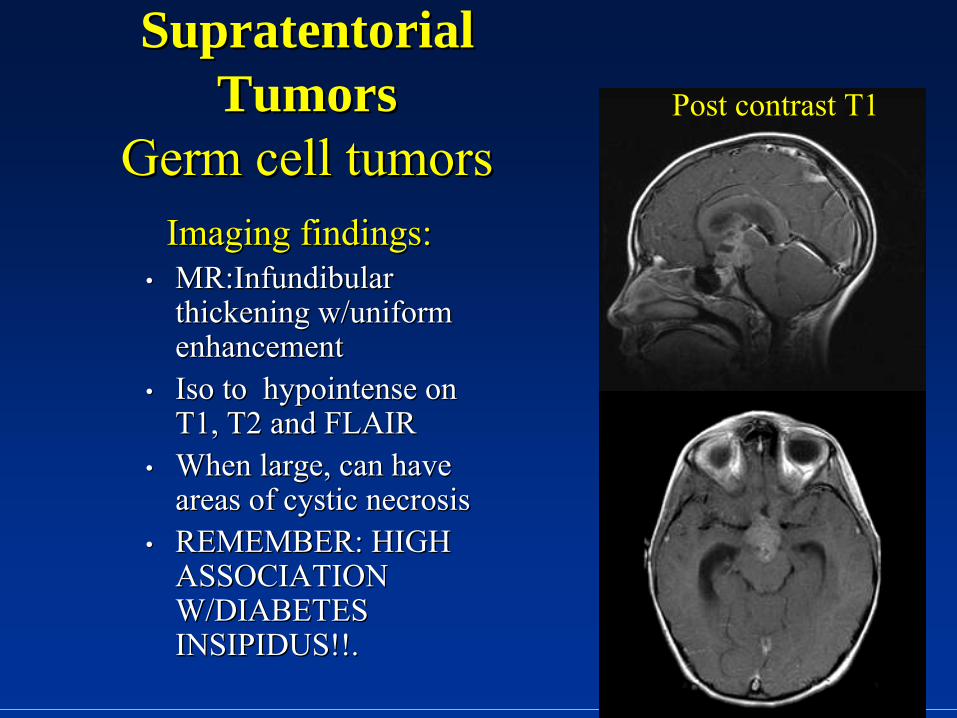
SupratentorialSupratentorial TumorsTumors
Germ cell tumorsGerm cell tumorsImaging findings:Imaging findings:
••
MR:MR:InfundibularInfundibular thickening w/uniform thickening w/uniform
enhancementenhancement••
IsoIso
to to hypointensehypointense
on on T1, T2 and FLAIRT1, T2 and FLAIR
••
When large, can have When large, can have areas of cystic necrosisareas of cystic necrosis
••
REMEMBER: HIGH REMEMBER: HIGH ASSOCIATION ASSOCIATION W/DIABETES W/DIABETES INSIPIDUS!!.INSIPIDUS!!.
Post contrast T1
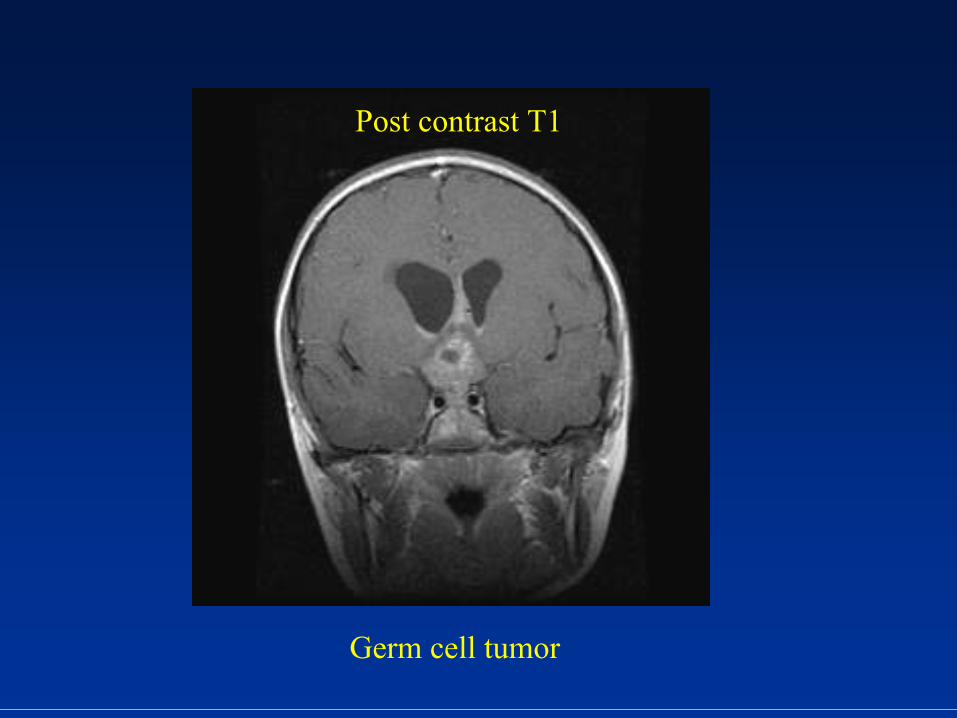
Post contrast T1
Germ cell tumor
SupratentorialSupratentorial TumorsTumors Hypothalamic Hypothalamic HamartomaHamartoma
••
HeterotopicHeterotopic
gray matter generally located in tuber gray matter generally located in tuber cinereum cinereum
••
Can originate from floor third ventricle, Can originate from floor third ventricle, mamillarymamillary bodies bodies
••
Can be sessile or Can be sessile or pedunculatedpedunculated••
Presents between 1Presents between 1--3yrs age; M=F3yrs age; M=F••
Large lesions cause Large lesions cause gelasticgelastic
seizures; small lesions seizures; small lesions have precocious pubertyhave precocious puberty
••
Found in 33% of patients w/precocious pubertyFound in 33% of patients w/precocious puberty••
Treatment is hormonal therapyTreatment is hormonal therapy
SupratentorialSupratentorial TumorsTumors
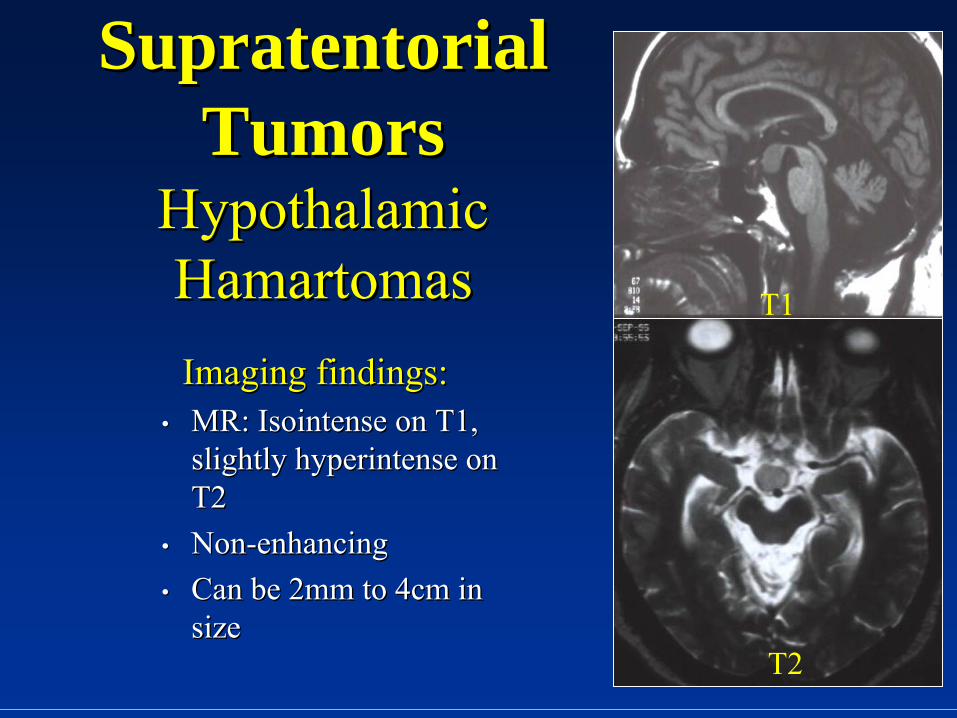
Hypothalamic Hypothalamic HamartomasHamartomasImaging findings:Imaging findings:
••
MR: MR: IsointenseIsointense
on T1, on T1, slightly slightly hyperintensehyperintense
on on
T2T2••
NonNon--enhancingenhancing••
Can be 2mm to 4cm in Can be 2mm to 4cm in sizesize
T1
T2
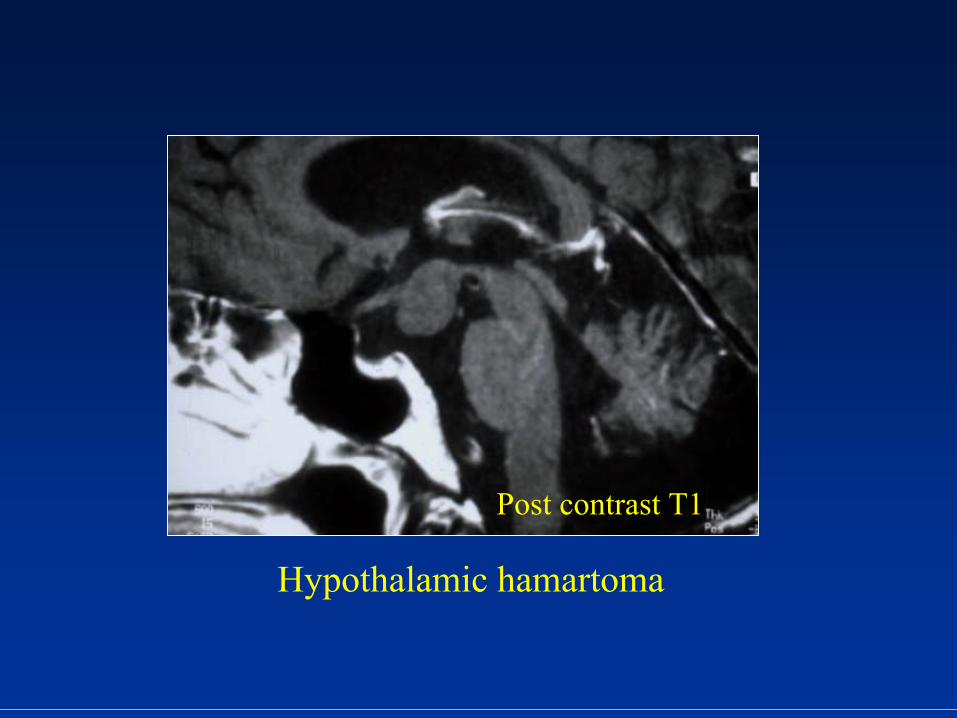
Post contrast T1
Hypothalamic hamartoma
SupratentorialSupratentorial TumorsTumors LangerhansLangerhans
cell cell histiocytosishistiocytosis
••
Most common manifestation of LCHMost common manifestation of LCH••
CNS presentation is more common in patients CNS presentation is more common in patients with multiwith multi--systemic diseasesystemic disease
••
GranulomasGranulomas
in the subarachnoid space which in the subarachnoid space which infiltrate hypothalamus/infiltrate hypothalamus/infundibuluminfundibulum
••
Clinical: Diabetes Clinical: Diabetes insipidusinsipidus
(5% of patients on (5% of patients on diagnosis and up to 50% on followdiagnosis and up to 50% on follow--up exams)up exams)
SupratentorialSupratentorial TumorsTumors LangerhansLangerhans
cell cell histiocytosishistiocytosis
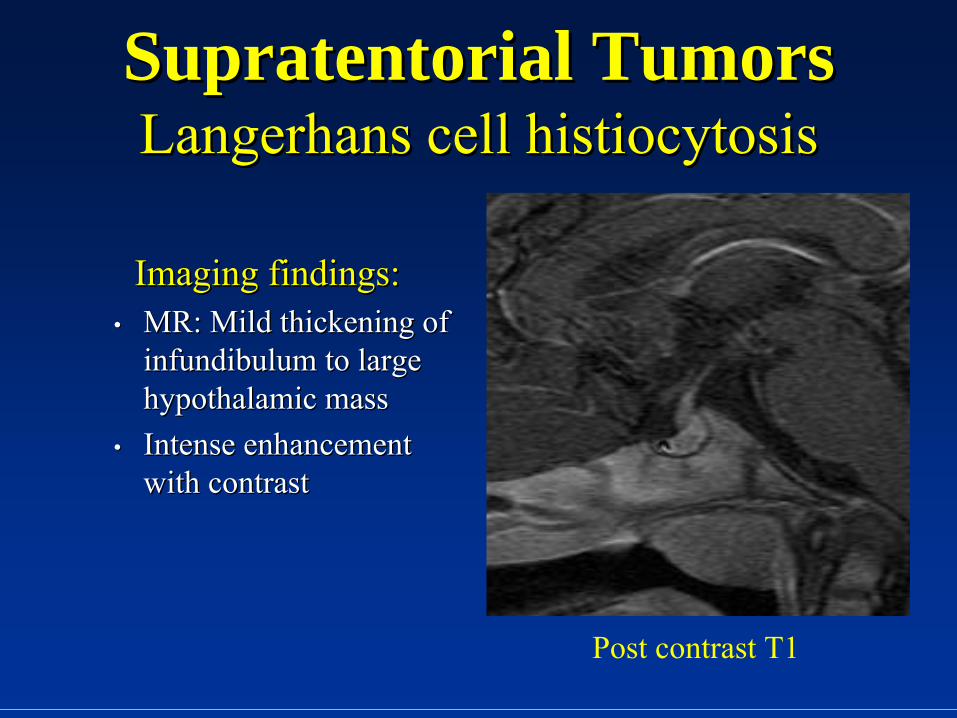
Imaging findings:Imaging findings:••
MR: Mild thickening of MR: Mild thickening of infundibuluminfundibulum
to large to large
hypothalamic masshypothalamic mass••
Intense enhancement Intense enhancement with contrastwith contrast
Post contrast T1

ReferencesReferences••
Grossman RI, Grossman RI, YousemYousem
DM. In: DM. In: NeuroradiologyNeuroradiology. Ed. Mosby, Philadelphia, . Ed. Mosby, Philadelphia, 20032003
••
Osborn AG. In: Diagnostic Imaging Brain. Ed. Elsevier Saunders, Osborn AG. In: Diagnostic Imaging Brain. Ed. Elsevier Saunders, 20042004••
BarkovichBarkovich
JA. In: Pediatric JA. In: Pediatric NeuroradiologyNeuroradiology. Ed. Elsevier Saunders, 2007. Ed. Elsevier Saunders, 2007••
Pediatric central nervous system germ cell tumors: a review. OncPediatric central nervous system germ cell tumors: a review. Oncologist. ologist. 2008 Jun;13(6):6902008 Jun;13(6):690--9.9.
••
ElidaElida
VázquezVázquez, , AmparoAmparo
CastelloteCastellote, , JoaquimJoaquim
PiquerasPiqueras, Pedro , Pedro OrtuñoOrtuño, José , José SánchezSánchez--Toledo, Toledo, PerePere
NoguésNogués, and Javier , and Javier LucayaLucaya
Second Malignancies in Pediatric Patients: Imaging Findings and Second Malignancies in Pediatric Patients: Imaging Findings and Differential DiagnosisDifferential Diagnosis RadioGraphicsRadioGraphics
2003; 23: 11552003; 23: 1155--1172. 1172. ••
Kelly K. Kelly K. KoellerKoeller
and Glenn D. Sandbergand Glenn D. Sandberg
From the Archives of the AFIP: Cerebral From the Archives of the AFIP: Cerebral IntraventricularIntraventricular NeoplasmsNeoplasms: : RadiologicRadiologic--Pathologic CorrelationPathologic Correlation RadioGraphicsRadioGraphics
2002; 22: 14732002; 22: 1473--1505. 1505.
Thank You.Thank You.