patient access policy - whatdotheyknow
TRANSCRIPT

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 1
BIRMINGHAM CHILDREN’S HOSPITAL NHS FOUNDATION TRUST
PATIENT ACCESS POLICY
Purpose This policy is designed to clarify the processes and procedures that all Trust staff should adhere to in order to ensure that all patients have equitable access to the Trust‟s elective services in line with Government targets.
Performance and Capability Management
In the event that staff fail adhere to these processes and procedures, the policy will be used to correct performance alongside the Trust Disciplinary and Capability policies.
Policy Statement Birmingham Children‟s Hospital NHS Foundation Trust is committed to ensuring that all children who require access to our elective services are treated in an equitable and professional manner.
Stakeholder Groups Chief Operating Officer Deputy Chief Operating Officer Director of Performance and Planning Clinical Access Group Access Improvement Group Consultants Directorate Management Patient Access Team Medical Secretaries Lorenzo Training Team IM&T Commissioners
Related Policies & Procedures DNA Policy Standard Operating Procedure for booking and
grading new Outpatient Appointments Lorenzo – 18 Week Pathway End User Guide Cancelled Operations Policy
Standard Operation Procedures for Choose & Book
Bed Management Policy

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 2
Version Date Author Comment (Identify any significant changes to the procedural document)

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 3
Contents:
Executive Summary 4
About this document 5
General Points 5
REFERRAL TO TREATMENT – DEFINITIONS 18 WEEK WAIT 6
REFERRAL TO TREATMENT (RTT) – STANDARDS 13
Performance Management 19
Data Quality 19
OUTPATIENT - DEFINITIONS 20
Performance Management 24
Data Quality 24
CHOOSE AND BOOK (CAB) – DEFINITIONS AND STANDARDS 25
Performance Management 27
CONSULTANT TO CONSULTANT REFERRAL – STANDARDS 28
Performance Management 29 INPATIENT – DEFINITION AND STANDARDS 30
Performance Management 37
Data Quality 37
DIAGNOSTIC – DEFINITION AND STANDARDS 38
CANCELLED OPERATIONS – STANDARDS 43
Performance Management 43
Data Quality 43
PATIENTS WITH SUSPECTED ABD DIAGNOSED CANCER – REFERRAL MANAGEMENT 44
CANCER WAITS – STANDARDS 55
Performance Management 59
Data Quality 59
PERFORMANCE MANAGEMENT 60
GOVERNANCE 62
ROLES AND RESPONSIBILIITES 63
EDUCATION, TRAINING AND SUPPORT 71
APPENDIX 1: 18 WEEK RTT OUTCOME SHEET 73
APPENDIX 2: 18 WEEK RTT OPTIONS 75
APPENDIX 3: IPTADMS FORM 77
APPENDIX 4: DATA ITEMS IN NATIONAL CANCER WAITING TIMES MONITORING
DATASET – INCLUDES INDICATION OF WHETHER THESE ARE MANDATORY OR
OPTIONAL 77
APPENDIX 5: MDT ALERT TO INCOMING PATIENTS 81
APPENDIX 6: DIAGNOSTICS PERFORMANCE MANAGEMENT PROCESS 84
APPENDIX 7: 18 WEEK BREACH EXCEPTION REPORT TEMPLATE 86
APPENDIX 8: LEGITIMATE WAITS AND UNNECESSARY WAITS 87

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 4
EXECUTIVE SUMMARY This policy outlines the Birmingham Children‟s Hospital NHS Foundation Trust process for managing patients who are waiting for elective treatment. It aims to support the delivery of the Trust‟s key strategic aims to „provide access to all who choose or need Birmingham Children‟s Hospital services‟ and is underpinned by a culture of clinically led decision making. This key strategic aim is to support the 18 week universal pledge which is now a legal right for patients, as set out in the NHS Constitution and the NHS Operating Framework. This commitment should be delivered for every patient, in every speciality and in every organisation unless the patient chooses otherwise or it is not their best clinical interest.
This policy aims to support the Trust in working to meet the key principles of:
Giving priority to clinical urgent patients and treating everyone else equitably.
Ensuring fair and equal access to services for all patients. Avoiding unnecessary delays to patients‟ treatment pathways by meeting and
improving maximum waiting times set by the Department of Health for all groups of patients.
Recognising waiting times as a measure of quality and delay as a failure to meet a quality standard.
Aiming to negotiate appointment and admission dates and times with patients whenever possible.
To ensure the effective management of waiting lists the policy aims to:
Be patient centred, not target focused. Be a tool to support services in managing capacity and demand. Measure one patient pathway and support the management of waiting times along
the whole patient pathway.
Be simple to use and clear about roles and responsibilities. Ensure that no patient waits longer than the national standard of 18 weeks from
referral to treatment. NOTE: For patients not on an 18 week pathway, no patient should wait longer than:
6 weeks - diagnostics 13 weeks - outpatients 26 weeks - inpatients

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 5
About this document
1. The policy has been divided into short sections, which can be updated as necessary with the approval of the Clinical Access Group.
2. The policy will be updated as further guidance becomes available 3. The policy includes “standard” sections that can be detached for quick reference.
4. The format of the policy allows individuals to access specific sections related to a
particular pathway. As a result some subjects will be repeated in more than one area.
General Points
1. All waiting lists must be held and managed on Lorenzo. 2. Any potential breach of waiting times standards must be notified to the
immediate line manager and the Directorate Management Team as soon as it is identified.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 6
REFERRAL TO TREATMENT – DEFINITIONS 18 WEEK WAIT
REFERRAL TO TREATMENT – DEFINITIONS 18 WEEK WAIT Overview
The 18 week target applies to pathways that do or might involve medical or surgical consultant-led care. It sets a maximum time of 18 weeks from the point of initial referral to the start of first definitive treatment for all patients who want it, and for whom it is clinically appropriate. These rules are not exhaustive. Frequently asked questions (FAQs) are available at www.18weeks.nhs.uk which is updated regularly and recommended as giving more detail. If in doubt, the principle of providing excellent care without unnecessary delay should be followed, together with those of reasonableness, honesty and good communication.
Clock starts
The clock starts:
In the case of a referral from primary care or a self-referral, the clock starts ticking when the patient either converts their Unique Booking Reference Number (UBRN), attempts to convert their UBRN or when the paper referral is received at the Call Centre.
If the referral is from another service or another acute provider, then clock start details must be obtained from the referring organisation via an Inter Provider Transfer Administrative Minimum Dataset [IPTAMDS] form.
If the patient is converting from a private patient to NHS, the clock starts on the date BCH accepts the referral.
Note: If a patient has not been through the prior approval process (for example Welsh patients) the 18 week clock starts ticking from the date the referral is received and the clock continues ticking while approval is sought. A referral from primary care starts an 18 week clock if it is expected that:
The patient will be assessed and, if appropriate, treated before responsibility is transferred back to the referring health professional.
Any treatment will or might be carried out by a medical or surgical consultant-led service irrespective of setting. (Referrals to nurse consultants and allied health professionals are not covered under

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 7
REFERRAL TO TREATMENT – DEFINITIONS 18 WEEK WAIT 18 weeks).
The patient requires diagnostic services and it is anticipated that the patient will be assessed and might, if appropriate, be treated by a medical or surgical consultant-led service, before responsibility is transferred back to the referring health professional.
Examples of referrals which may start an 18 week clock are those from:
General Practitioners. General dental practitioners. Optometrists and Orthoptists.
Walk-in Centres. National Screening programmes. Patients returning from watchful waits. Other consultants. Self referral – where these pathways have been agreed locally by
commissioners and providers. Consultant to consultant (or consultant-led services) referrals start a clock, specifically for:
New conditions identified by the consultant. Separate treatments not originally in the treatment plan.
Clock stops
The clock stops:
When first definitive treatment begins - the clock stops on the date that the patient receives the first definitive treatment intended to manage his or her condition.
On inpatient or day case admission - the clock stops on the day of admission, providing the treatment is not cancelled. If the admission is for a diagnostic procedure the clock continues ticking.
When a clinical decision is made that treatment is not required - the clock stops on the date that the clinical decision is communicated to the patient.
When a patient chooses to decline treatment - the clock stops on the date that the patient declines treatment.
For treatment provided in an outpatient setting - the clock stops on the day the patient attended their appointment if treatment was provided.
When a period of active monitoring (watchful wait) is commenced.
Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 8
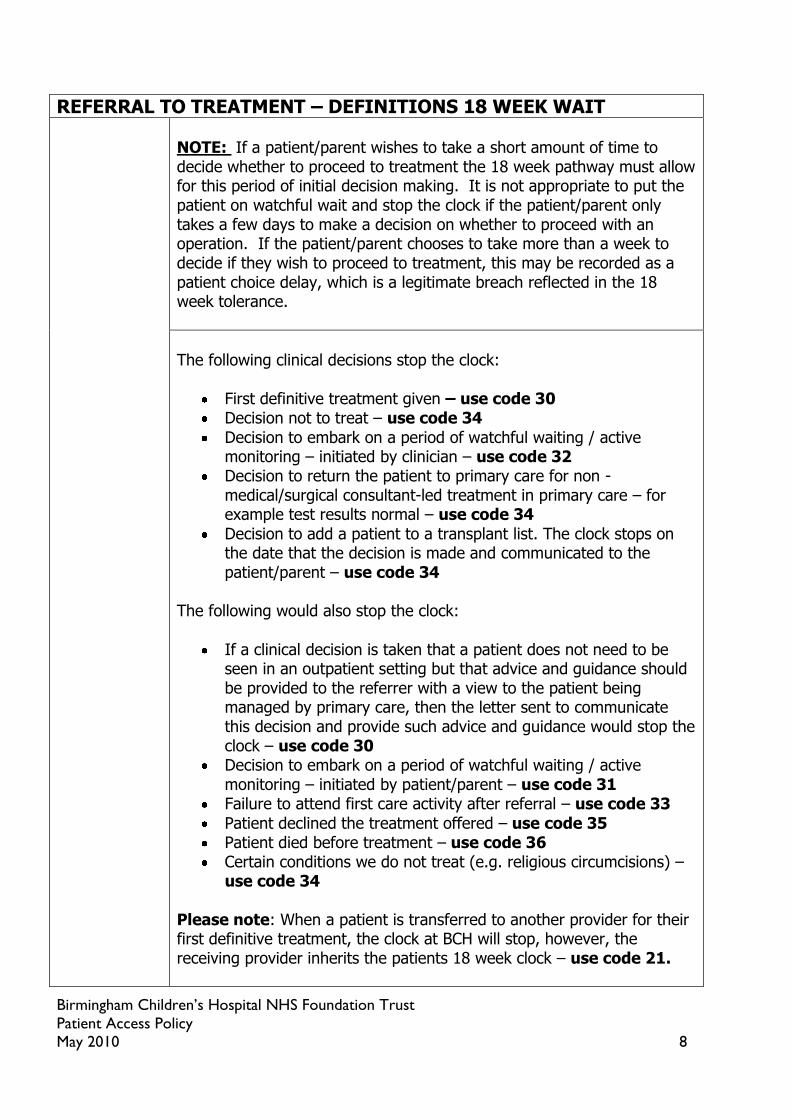
REFERRAL TO TREATMENT – DEFINITIONS 18 WEEK WAIT NOTE: If a patient/parent wishes to take a short amount of time to decide whether to proceed to treatment the 18 week pathway must allow for this period of initial decision making. It is not appropriate to put the patient on watchful wait and stop the clock if the patient/parent only takes a few days to make a decision on whether to proceed with an operation. If the patient/parent chooses to take more than a week to decide if they wish to proceed to treatment, this may be recorded as a patient choice delay, which is a legitimate breach reflected in the 18 week tolerance.
The following clinical decisions stop the clock:
First definitive treatment given – use code 30 Decision not to treat – use code 34
Decision to embark on a period of watchful waiting / active monitoring – initiated by clinician – use code 32
Decision to return the patient to primary care for non -medical/surgical consultant-led treatment in primary care – for example test results normal – use code 34
Decision to add a patient to a transplant list. The clock stops on the date that the decision is made and communicated to the patient/parent – use code 34
The following would also stop the clock:
If a clinical decision is taken that a patient does not need to be seen in an outpatient setting but that advice and guidance should be provided to the referrer with a view to the patient being managed by primary care, then the letter sent to communicate this decision and provide such advice and guidance would stop the clock – use code 30
Decision to embark on a period of watchful waiting / active monitoring – initiated by patient/parent – use code 31
Failure to attend first care activity after referral – use code 33
Patient declined the treatment offered – use code 35 Patient died before treatment – use code 36 Certain conditions we do not treat (e.g. religious circumcisions) –
use code 34 Please note: When a patient is transferred to another provider for their first definitive treatment, the clock at BCH will stop, however, the receiving provider inherits the patients 18 week clock – use code 21.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 9
REFERRAL TO TREATMENT – DEFINITIONS 18 WEEK WAIT First definitive treatment
First definitive treatment can be:
Inpatient or day case treatment. Diagnostic tests turned into therapeutic procedures during the
investigation. The fitting of a medical device.
Outpatient treatment (medical or surgical consultant-led treatment irrespective of setting) if no subsequent inpatient or day-case admission is expected.
First-line treatment – less intensive treatments or medical management attempted with the intention of avoiding more invasive procedures or treatment.
Therapy (for example physiotherapy) or healthcare science interventions (for example hearing aid fitting), if that is what the consultant decides is the intervention intended to manage the patient‟s disease, condition or injury and avoid further intervention.
NOT clock starts
Referrals from primary care to the following services DO NOT START a clock:
Therapy, healthcare science or mental health services that are not medical or surgical consultant-led including multi-disciplinary teams and community teams run by mental health trusts -irrespective of setting.
Diagnostic services if the referral is not part of a „straight-to-test‟ arrangement.
Primary dental services provided by dental students in hospital settings.
NOT clock stops
The following examples DO NOT STOP a clock:
Administration of pain relief or therapy before a surgical procedure takes place, or other steps to manage a patient‟s condition in advance of first definitive treatment.
Consultant to consultant referrals where underlying condition remains unchanged.
The clock does not stop if a provider rejects a referral stating that their service is not appropriate for this patient. The referrer must re-refer the patient to an appropriate service without delay – the 18 week clock is still ticking.
The mere act of making a tertiary referral or a referral from one

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 10
REFERRAL TO TREATMENT – DEFINITIONS 18 WEEK WAIT provider to another (if first definitive treatment has not been given).
Referral to treatment [RTT] status
The RTT status shows:
If an 18-week clock is ticking. Where the patient is on the pathway - clock start, clock stop, start
of watchful wait/active monitoring.
If the RTT status is not recorded or cannot be derived, then it is not possible to track a patient properly along their 18 week pathway, to ensure they receive treatment within 18 weeks.
Legitimate exceptions and delays
Patients waiting for inpatient or day case treatment will be able to choose to pause their clock for social reasons (for example holidays). BCH uses the suspension functionality on Lorenzo to record clock pauses. Clock pauses for social reasons are not allowed for outpatients or diagnostics.
What if it is not clinically appropriate to treat the patient within 18 weeks?
In some cases, treatment within 18 weeks may not be possible for clinical reasons. For example:
If a series of tests must be done in sequence (planned sequence). When a second condition presents itself that needs to be treated
before the first. The second condition starts a new 18 week clock. However, the first condition‟s 18 week clock is still ticking.
Any patients for whom there is a genuine clinical uncertainty about the diagnosis should not be put on watchful waiting. The clock will keep ticking until a diagnosis is confirmed and first definitive treatment is given.
Patient is not sure about proceeding with treatment
If a patient is uncertain about going ahead with treatment, it may be appropriate to discharge the patient and refer them back to their GP, where their ongoing care will continue to be managed within primary care. Referral back to the GP in this scenario would stop the 18 week clock – use code 35. If and when the patient feels ready for treatment they can ask their GP to re-refer them and a new 18 week clock should start at the point when the patient and GP agreed to re-refer for treatment.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 11
REFERRAL TO TREATMENT – DEFINITIONS 18 WEEK WAIT Non-admitted pathway: Patients who choose to delay treatment.
Some patients will turn down reasonable appointments for social reasons, for example, to go on extended holiday or for work commitments. There are no clock pauses for non-admitted patients. If a patient chooses to cancel their appointment their 18 week clock continues Patients should be referred back to their GP/referrer if they repeatedly cancel or defer appointments. The consultant should always review the patient‟s notes before the patient is referred back to their GP/referrer. BCH must be certain that discharging the patient back to their GP is not contrary to the patient‟s best clinical interest.
Admitted pathway: Patients who choose to delay treatment.
Patients on an admitted pathway can pause their 18 week clock if this is their choice (for example for social reasons / holidays) – use the suspension option on Lorenzo. The clock is paused for the duration of the time between the earliest reasonable offer and the date from which the patient makes themselves available again for admission. A clock may also be paused where the patient has declined two reasonable offers for admission (2 reasonable offers is a choice of 2 dates and a minimum of 3 weeks‟ notice).
DNA [did not attend]
Any patient who has been offered reasonable choice who did not attend their first appointment after initial referral will have their clock nullified. Providers will need to be able to demonstrate that the appointment offer was clearly communicated to the patient. If a patient DNA‟s an appointment, the consultant should be informed and will need to make a clinical decision as to whether a further appointment is offered. A new 18 week clock should start from the date contact is made with the patient/parent.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 12
REFERRAL TO TREATMENT – DEFINITIONS 18 WEEK WAIT Performance Management
A key principle for 18 weeks is that any decision taken which means the patient will not receive their treatment in 18 weeks, however legitimate that wait is, should be explicitly communicated to the patient and subsequently to their GP / referrer. As patients on an admitted pathway can pause their 18 week clock for social reasons/ holidays etc....as the provider we need to ensure that the patient is aware that the delay may mean that they do not receive their treatment within 18 weeks.
Legitimate Waits (see appendix 8):
Patient chose to wait longer than 18 weeks for their first definitive treatment
Patient non-cooperation (DNA‟s). The provider must ascertain communications with the patient were effective and received in good time
Not in the patient‟s best clinical interest (waiting longer than 18 weeks is clinically appropriate)
Data Quality
PCTs and providers will need to be able to demonstrate (to an auditor or the Care Quality Commission or in the event of a patient complaint) that cases taking longer than 18 weeks to start first definitive treatment are legitimate waits.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 13
REFERRAL TO TREATMENT [RTT] STANDARDS The 18 week referral to treatment (RTT) pathway treats the patient‟s journey from referral to first definitive treatment as one joined-up waiting time. The RTT pathway is based on clock starts and clock stops. Broadly speaking, the 18-week clock:
Starts when a patient is referred for an assessment and, if appropriate, treatment by a medical or surgical consultant-led service - irrespective of setting.
Stops when first definitive treatment begins, a clinical decision is made that
treatment is not required or when a patient declines treatment.
General
The specific standards for each stage of treatment (outpatient, diagnostic, inpatient or day case) must all be followed. This includes:
Recording and grading a referral/addition to the list. Agreeing all offers of appointment/admission with the
patient.
Ensuring reasonable offers are made – 2 different appointment dates, with a minimum of 3 weeks notice.
Minimising hospital-initiated cancellations.
Data quality
The following data items must be recorded for every patient. If they are not provided all staff who come in to contact with the patient, who are then informed of the relevant data, are responsible for recording them:
Registered GP
NHS number Ethnic coding Overseas visitor status Contact telephone numbers School
Measurement
It is not possible to measure the referral to treatment time and the Trust‟s compliance with the 18-week standard unless the 18 week pathway details are recorded. The essential elements that must be recorded at all times are:
The clock start The RTT status

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 14
REFERRAL TO TREATMENT [RTT] STANDARDS Clock start as a new outpatient
If the patient is referred directly to BCH as an outpatient, then the clock starts on either:
The date that the Choose and Book Unique Booking Reference Number [UBRN] is converted into an appointment, or
The date the GP referral letter is received at BCH. If the referral is from an interface service or another acute provider, then the clock has started outside BCH and clock start details must be obtained from the referring organisation via an Inter Provider Transfer Administrative Minimum Dataset [IPTAMDS] form as BCH inherits the existing 18 week clock. It is the responsibility of the Call Centre staff to obtain the IPTAMDS form data via telephone or email. If the referral is for a new condition a new 18 week clock should be started.
Clock start as a follow- up outpatient
A patient‟s 18 week clock may start as a follow up outpatient, for example, after a period of watchful waiting. The outcome sheet must be completed by the clinician for every outpatient attendance so that these clock starts can be identified. Call Centre staff should input the outcome sheet within one working day of clinic attendance. Any outcome sheets with data missing are sent to the Medical Secretaries for completion by the clinicians. Clinic outcome forms returned to medical secretaries should either:
1) Have the outcome updated on Lorenzo by the
Medical Secretary by the end of the working week in which the outpatient appointment occurred.
2) Have the outcome clarified on the outcome sheet and returned to the Call Centre by the end of the working week in which the outpatient appointment occurred. The Call Centre staff should then update Lorenzo accordingly within one working day.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 15
REFERRAL TO TREATMENT [RTT] STANDARDS Clock start as an inpatient
If the patient is placed directly on the inpatient-day case waiting list, then the clock start date (decision to start a new treatment), must be obtained and recorded as part of the waiting list record.
Referral to Treatment [RTT] status
The RTT status shows where the patient is on the pathway. It identifies clock starts and clock stops. If the RTT status is unknown, it is assumed that a clock is still ticking.
RTT status – Outpatients
In an outpatient setting, the RTT status is provided when the clinician completes the 18 week RTT details on the outcome sheet (appendix 1). It is the clinician‟s responsibility to complete the RTT status on the outcome sheet for all patients, whether new or follow up. 18 Week RTT Code options can be found at appendix 2.
The Call Centre staff transfer the information onto Lorenzo within one working day. Any outcome sheets with data missing are sent to the Medical Secretaries for completion by the clinicians. Clinic outcome forms returned to medical secretaries should either:
3) Have the outcome updated on Lorenzo by the Medical Secretary by the end of the working week in which the outpatient appointment occurred.
4) Have the outcome clarified on the outcome sheet and returned to the Call Centre by the end of the working week. The Call Centre staff should then update Lorenzo accordingly within one working day.
Inter-Provider Transfers
A minimum dataset must accompany every patient transferred between providers. This must include the current clock start and RTT status and must be obtained for:
Referrals or transfers from other hospitals Referrals and direct additions to the list from interface
services
Internal referrals from other consultants for the condition

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 16
REFERRAL TO TREATMENT [RTT] STANDARDS the patient was referred.
A minimum data set must be provided for:
Patients transferred or referred to another provider. Patients transferred back to their local hospital for post-
operative care.
All internal referral for existing and non-existing pathways. Medical secretaries are responsible for obtaining the minimum data set information and the Call Centre is responsible for inputting the data onto Lorenzo Note: Patients who have been seen in the private sector as private patients and who now wish to transfer to NHS care, do not have an 18-week clock running until the provider accepts them. The transfer must be agreed with the patient‟s PCT, following the principles of prior approval.
Delays to the 18 week pathway This section summarises the recommended actions for patients who are either medically unfit to proceed or who choose to delay their 18 week pathway. Any removal from the list must be discussed with the consultant/AHP and must be communicated by letter to the patient, GP and/referrer.
DNA at 1st outpatient appointment
If a patient DNAs the 1st outpatient appointment after initial referral will have their clock nullified. The consultant will be informed and will make a clinical decision whether a further appointment is offered. If a further appointment is to be offered a new 18 week clock should start on the date when contact is made with the patient.
DNA at inpatient admission
If a patient DNAs an inpatient admission, the consultant will be informed and will make a clinical decision whether a further admission is offered. The clock keeps ticking until the clinician makes a decision.
Cancer and suspected cancer patients will always be offered another date.
Any other patients will either be offered another admission date or referred back to their GP/referrer, based on the

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 17
REFERRAL TO TREATMENT [RTT] STANDARDS outcome of the clinician‟s decision.
DNA – protection for patients
In order to support the DNA policy whereby patients are referred back to GPS if they DNA, each Directorate team must make sure that the following are in place:
The patient has been made a reasonable offer. There are processes in place to make it simple and easy
for patients to cancel or reschedule their appointments or admissions or to notify of last minute problems (for example transport not arriving).
It has been made clear to the patient through any verbal and all written communication about the appointment/admission that the patient may be returned to the care of the GP if he or she DNA‟s.
For any request where the patient, GP or other referrer believes that this was not a true DNA the request should be discussed with the Directorate Management Team before the patient is re-instated. Further action will be taken at the discretion of the Clinician.
Patient-initiated cancellation for Outpatients, Diagnostic, Inpatient, Day Case or Pre-operative Assessment
If the patient has agreed a date and then cancelled it an agreed second date will be arranged in consultation with the patient. If the patient cancels again the patient should be informed that the referral will be reviewed by the clinician. If a patient cancels and does not want another appointment, the referral should be returned to the clinician for review.
Cancellations by the hospital for Outpatients, Diagnostic, Inpatient, Day Case or Pre-operative Assessment
Cancellations by the hospital must be kept to a minimum. The 18 week clock does not stop for a hospital-initiated cancellation. The patient must be rebooked and treated within 28 calendar days for elective inpatient/day cases cancelled on the day of the agreed admission date, or a date prior to the end of their 18 week pathway – whichever is the earliest.
Patient Choice for Outpatients,
The patient should be given 2 reasonable offers - a choice of 2 dates and a minimum of 3 weeks‟ notice.
Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 18
REFERRAL TO TREATMENT [RTT] STANDARDS Diagnostic, Inpatient, Day Case or Pre-operative Assessment
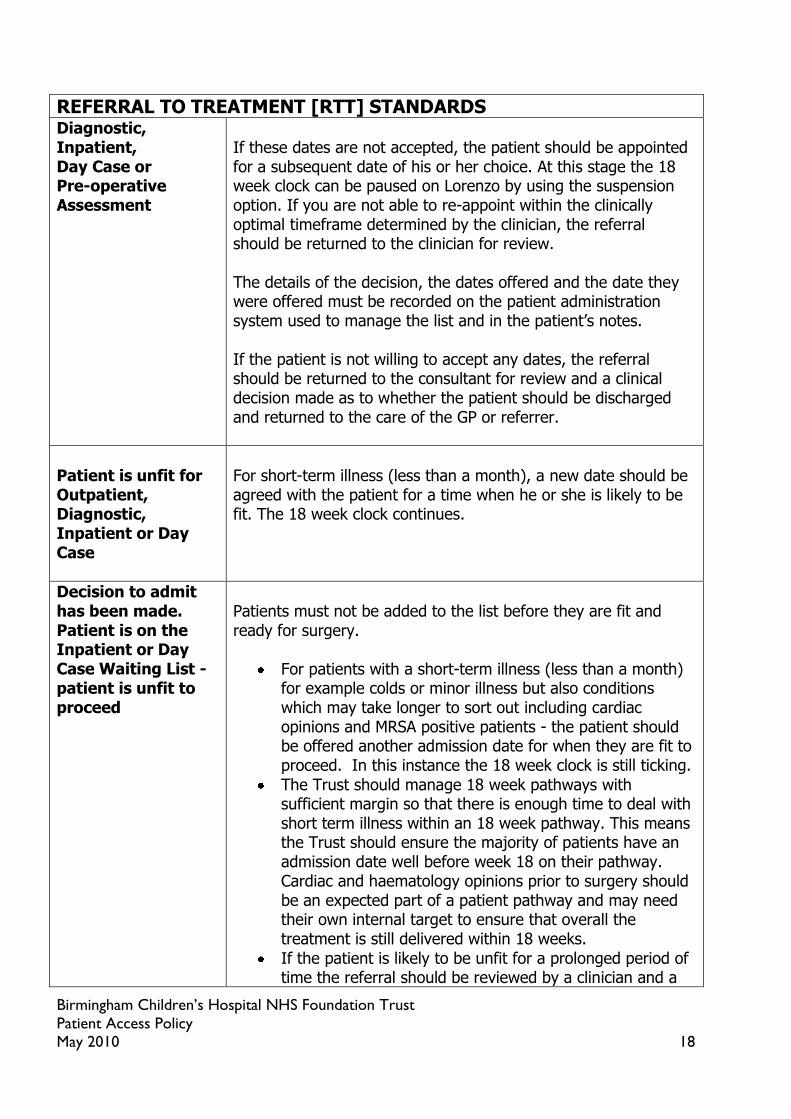
If these dates are not accepted, the patient should be appointed for a subsequent date of his or her choice. At this stage the 18 week clock can be paused on Lorenzo by using the suspension option. If you are not able to re-appoint within the clinically optimal timeframe determined by the clinician, the referral should be returned to the clinician for review. The details of the decision, the dates offered and the date they were offered must be recorded on the patient administration system used to manage the list and in the patient‟s notes. If the patient is not willing to accept any dates, the referral should be returned to the consultant for review and a clinical decision made as to whether the patient should be discharged and returned to the care of the GP or referrer.
Patient is unfit for Outpatient, Diagnostic, Inpatient or Day Case
For short-term illness (less than a month), a new date should be agreed with the patient for a time when he or she is likely to be fit. The 18 week clock continues.
Decision to admit has been made. Patient is on the Inpatient or Day Case Waiting List - patient is unfit to proceed
Patients must not be added to the list before they are fit and ready for surgery.
For patients with a short-term illness (less than a month) for example colds or minor illness but also conditions which may take longer to sort out including cardiac opinions and MRSA positive patients - the patient should be offered another admission date for when they are fit to proceed. In this instance the 18 week clock is still ticking.
The Trust should manage 18 week pathways with sufficient margin so that there is enough time to deal with short term illness within an 18 week pathway. This means the Trust should ensure the majority of patients have an admission date well before week 18 on their pathway. Cardiac and haematology opinions prior to surgery should be an expected part of a patient pathway and may need their own internal target to ensure that overall the treatment is still delivered within 18 weeks.
If the patient is likely to be unfit for a prolonged period of time the referral should be reviewed by a clinician and a
Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 19
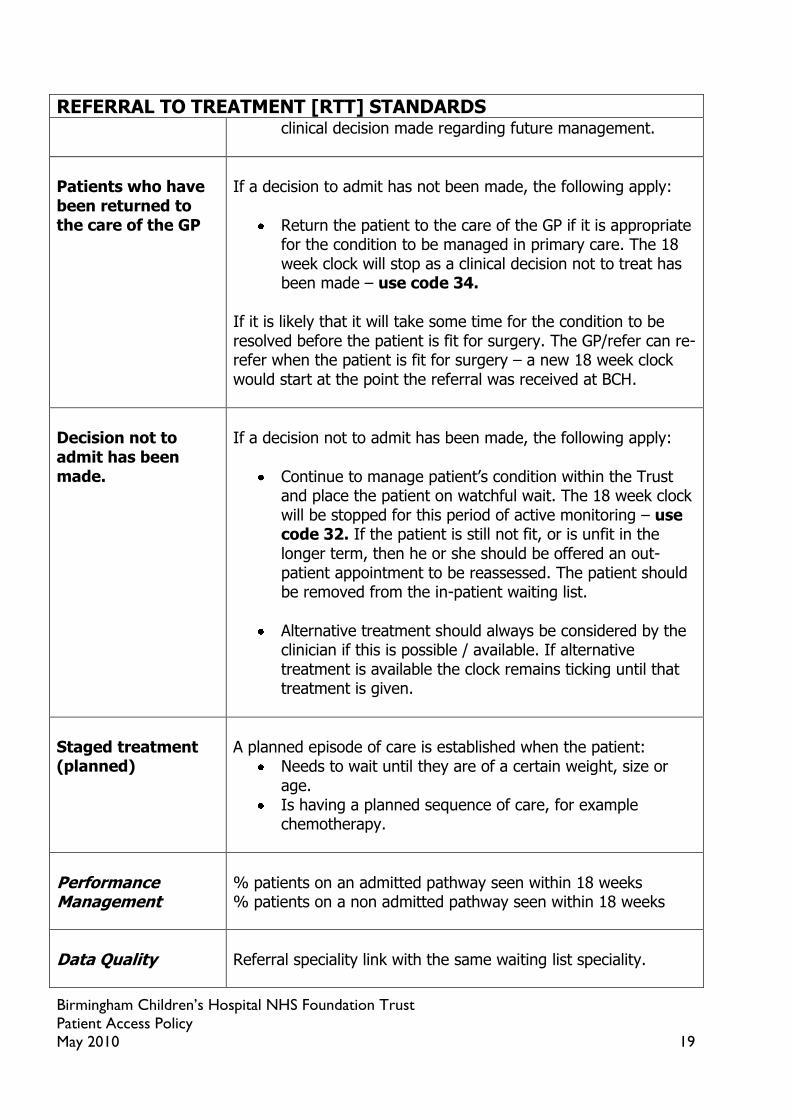
REFERRAL TO TREATMENT [RTT] STANDARDS clinical decision made regarding future management.
Patients who have been returned to the care of the GP
If a decision to admit has not been made, the following apply:
Return the patient to the care of the GP if it is appropriate for the condition to be managed in primary care. The 18 week clock will stop as a clinical decision not to treat has been made – use code 34.
If it is likely that it will take some time for the condition to be resolved before the patient is fit for surgery. The GP/refer can re-refer when the patient is fit for surgery – a new 18 week clock would start at the point the referral was received at BCH.
Decision not to admit has been made.
If a decision not to admit has been made, the following apply:
Continue to manage patient‟s condition within the Trust and place the patient on watchful wait. The 18 week clock will be stopped for this period of active monitoring – use code 32. If the patient is still not fit, or is unfit in the longer term, then he or she should be offered an out-patient appointment to be reassessed. The patient should be removed from the in-patient waiting list.
Alternative treatment should always be considered by the clinician if this is possible / available. If alternative treatment is available the clock remains ticking until that treatment is given.
Staged treatment (planned)
A planned episode of care is established when the patient:
Needs to wait until they are of a certain weight, size or age.
Is having a planned sequence of care, for example chemotherapy.
Performance Management
% patients on an admitted pathway seen within 18 weeks % patients on a non admitted pathway seen within 18 weeks
Data Quality
Referral speciality link with the same waiting list speciality.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 20
OUTPATIENT – DEFINITIONS (18 weeks is the Trust‟s delivery standard).
For patients not on an 18 week pathway, no patient should wait longer than 13 weeks for outpatients. Start of wait (clock start)
Choose and Book referral – when the patient converts their UBRN (unique booking reference number).
Manual referral – the date the referral is received at the Call Centre.
Reasonable offer of appointment
The Department of Health‟s definition of a „reasonable offer‟ is that it gives the patient a minimum of 3 weeks‟ notice and a choice of 2 dates if the offer is made verbally.
Note: An offer can be made with less than 2 weeks‟ notice. This is only considered reasonable if the patient accepts it. The patient cannot, however, be penalised for declining an offer made with less than 3 weeks‟ notice. The offer is not reasonable if the patient had told the Trust that he or she would not be available at that time.
Waiting time reset [for patients not on an 18 week pathway]
If the patient declines 2 reasonable offers.
If the patient cancels or reschedules the appointment after accepting it.
If the patient DNA‟s. In Lorenzo the waiting time restarts from the date of the DNA.
Note: the waiting time is not reset if the hospital has rescheduled the appointment or the patient turns down an offer that was not reasonable. Waiting time resets are not allowed under the 18 week rule.
Cancellations
Patient gives notice that they are unable to attend their appointment.
DNA
Patient fails to attend and does not give notice.
2WW 2 week waits. This standard applies to patients referred by their GP with urgent suspected cancer.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 21
OUTPATIENT STANDARDS Referrals Pooled referrals Named referrals
If the referral is made by telephone, Choose and Book or paper it is the responsibility of the person who received the referral to make sure it is recorded on Lorenzo within one working day.
Pooled referrals will be allocated according to capacity or according to clinical need and then capacity.
Named referrals are initially allocated to the addressee or according to clinical need.
Data quality
The following data items must be recorded for every patient. If they are not provided all staff who come in to contact with the patient, who are then informed of the relevant data, are responsible for recording them:
Registered GP NHS number
Ethnic coding Overseas visitor status Contact telephone numbers School
Grading the referral
All non-Choose and Book referrals must be forwarded to the Call Centre for booking within one working day of receipt at the Trust for registration and addition to the waiting list in preparation for grading. Note: It is the responsibility of the Consultant to accept, re-direct or reject any referral. If the clinician delegates any of these tasks s/he is still responsible for all the clinical and administrative consequences of these decisions. If a referral has been directed to an inappropriate consultant or sub-speciality the referral must be returned to the Call Centre within one working day for them to amend the data entry on Lorenzo. The Call Centre should then forward the referral to the appropriate consultant within one working day. This does not stop the clock.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 22
Note: a GP referral that has been redirected from one consultant to another more appropriate consultant remains a GP referral. It does not become a consultant to consultant referral as the patient has not yet been seen and the start of the 18 week clock does not change. Each speciality and Directorate Management Team must ensure that there are agreed arrangements for reviewing and grading every consultant‟s referrals within 5 days. This includes ensuring there is cover in place to review referrals/provide advice guidance when the Consultant is away from the Trust. This applies for every speciality in every case.
Rejecting a referral
Choose and Book – patients referred to an inappropriate service will be rejected on Choose and Book and removed from the waiting list – use code 34 Paper referrals – referrals made to an inappropriate service will be returned to the referrer and removed from the waiting list – use code 34
Booking and Choice
All patients are entitled to receive reasonable offers – a choice of 2 dates and a minimum of 3 weeks‟ notice. Patients may be offered short-notice appointments, but they can decline them without this affecting their 18 week clock waiting time. The Call Centre will attempt to make reasonable contact with the patient on two occasions by telephone. If attempts to contact the patient by telephone are unsuccessful, an appointment date and time should be sent out via mail. If the allocated appointment is unsuitable the patient is advised to contact the Call Centre to make alternative arrangements. All urgent appointments must be sent first class post.
Cancellations and DNA’s (Did not attend)
Cancellations and DNA‟s affect the calculation of waiting times and must be correctly recorded on Lorenzo.
Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 23
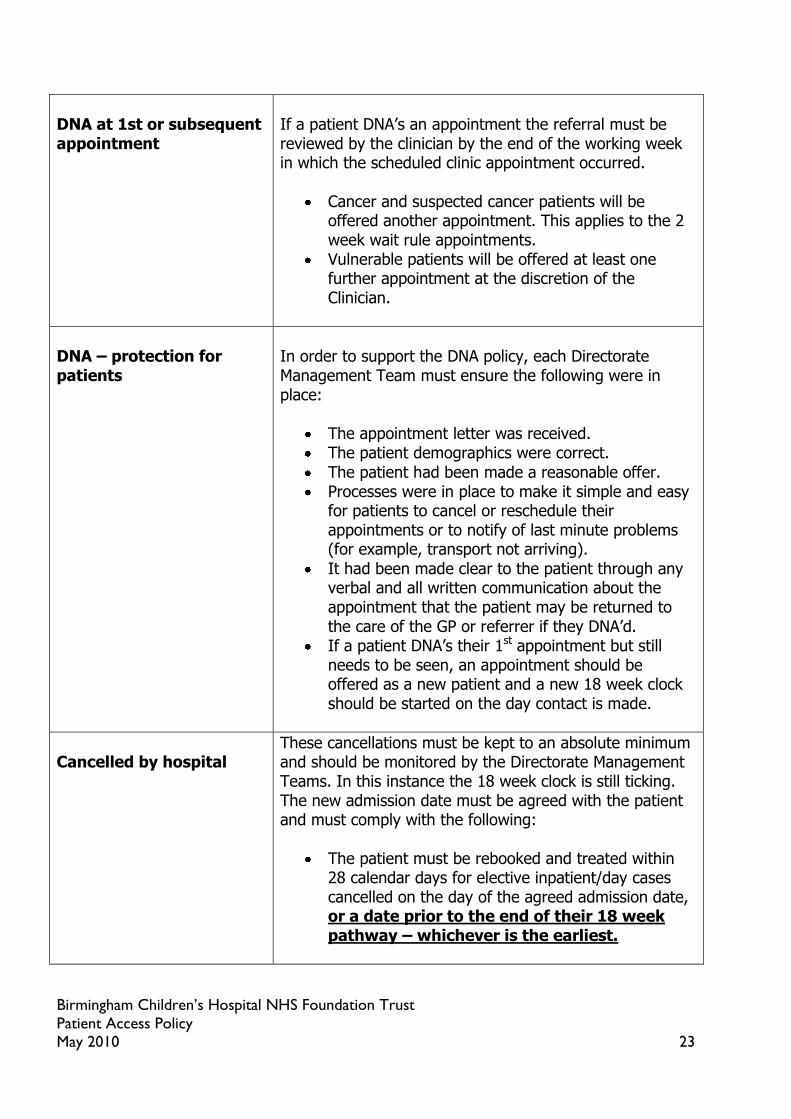
DNA at 1st or subsequent appointment
If a patient DNA‟s an appointment the referral must be reviewed by the clinician by the end of the working week in which the scheduled clinic appointment occurred.
Cancer and suspected cancer patients will be offered another appointment. This applies to the 2 week wait rule appointments.
Vulnerable patients will be offered at least one further appointment at the discretion of the Clinician.
DNA – protection for patients
In order to support the DNA policy, each Directorate Management Team must ensure the following were in place:
The appointment letter was received. The patient demographics were correct.
The patient had been made a reasonable offer. Processes were in place to make it simple and easy
for patients to cancel or reschedule their appointments or to notify of last minute problems (for example, transport not arriving).
It had been made clear to the patient through any verbal and all written communication about the appointment that the patient may be returned to the care of the GP or referrer if they DNA‟d.
If a patient DNA‟s their 1st appointment but still needs to be seen, an appointment should be offered as a new patient and a new 18 week clock should be started on the day contact is made.
Cancelled by hospital
These cancellations must be kept to an absolute minimum and should be monitored by the Directorate Management Teams. In this instance the 18 week clock is still ticking. The new admission date must be agreed with the patient and must comply with the following:
The patient must be rebooked and treated within 28 calendar days for elective inpatient/day cases cancelled on the day of the agreed admission date, or a date prior to the end of their 18 week pathway – whichever is the earliest.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 24
Cancelled by patient
If the patient agreed a date and subsequently cancelled it, an agreed second date should be arranged in liaison with the patient – the 18 week clock is still ticking.
If the patient cancels again the patient should be informed that the referral will be reviewed by the clinician – the 18 week clock is still ticking.
If a patient cancels and does not want another appointment, the referral should be returned to the clinician for review. The 18 week clock is stopped if the decision is to return the patient to the GP/referrer.
Performance Management
Waiting time for 1st outpatient appointment following GP referral
Data Quality
Patients who have had a referral opened in the last month with no activity or waiting list entry attached to that referral.
Date entered onto Lorenzo following receipt of referral.
Date appointment made or date of appointment (notice period).

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 25
Choose and Book Definitions: Choose and Book (CAB)
Choose and Book is a secure method of booking an appointment, which offers the patient a choice of Provider, date and time.
Directory of Services (DOS)
The Directory of Services is a national system at the heart of Choose and Book, which allows a GP to locate services and facilitates the patient being booked into an appropriate clinic.
Choice of provider
It is the patient‟s right (since April 2008) to be offered a choice of provider by the GP at point of referral. The local PCT menu available to the GP on the DOS is a list of the services commissioned by the PCT. The Free Choice menu allows the patient to choose to go anywhere in the country that meets DH standards. There will be a local primary care menu for services offered by primary care. There will be a national menu for services offered by a secondary care.
Directable Booking Service (DBS)
The patient can book on line either directly with the GP/referrer or via the telephone appointment line or via the internet (health space), using a password and unique booking reference number (UBRN). The GP‟s choice of services determines the clinic slots that the patient can book into. The patient can change or cancel their appointment using the same methods.
Indirectly Bookable Services (IBS)
The patient has to phone in to the chosen provider to book, reschedule or cancel an appointment – using a password and UBRN.
CHOOSE AND BOOK [CAB] STANDARDS
Booking the appointment
A referral through CAB will start a clock when the UBRN is converted by:
The patient booking an appointment.
Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 26
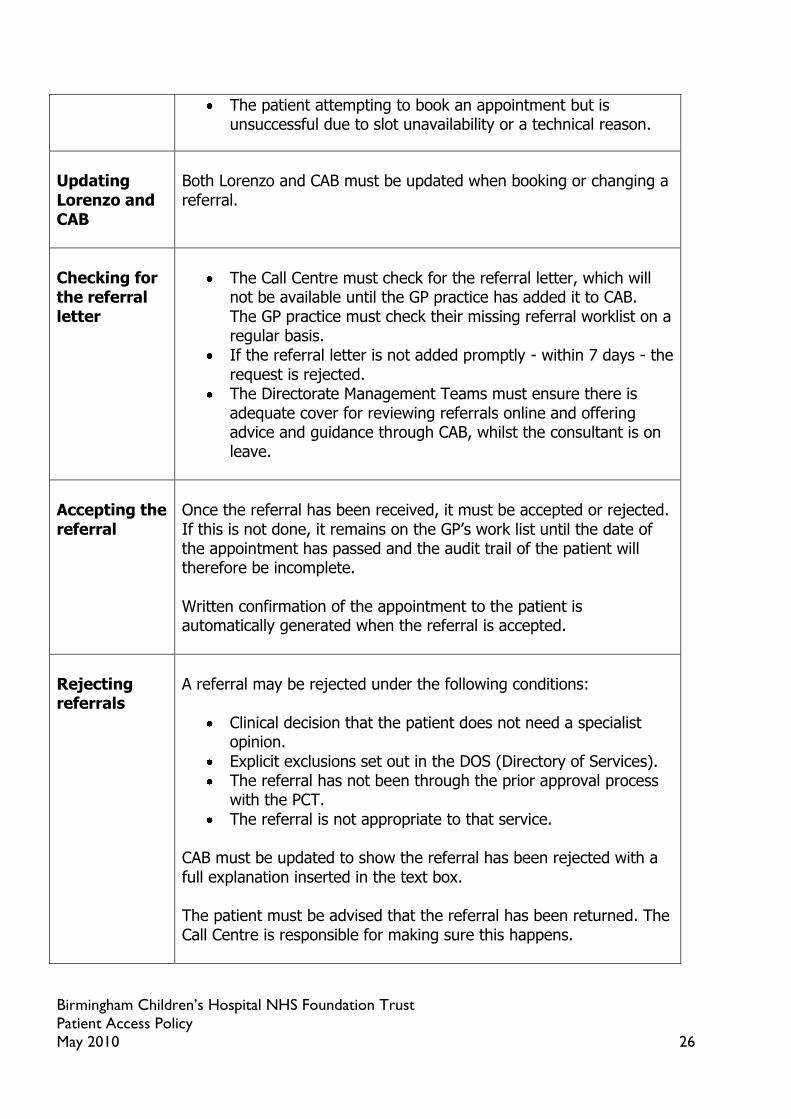
The patient attempting to book an appointment but is unsuccessful due to slot unavailability or a technical reason.
Updating Lorenzo and CAB
Both Lorenzo and CAB must be updated when booking or changing a referral.
Checking for the referral letter
The Call Centre must check for the referral letter, which will not be available until the GP practice has added it to CAB. The GP practice must check their missing referral worklist on a regular basis.
If the referral letter is not added promptly - within 7 days - the request is rejected.
The Directorate Management Teams must ensure there is adequate cover for reviewing referrals online and offering advice and guidance through CAB, whilst the consultant is on leave.
Accepting the referral
Once the referral has been received, it must be accepted or rejected. If this is not done, it remains on the GP‟s work list until the date of the appointment has passed and the audit trail of the patient will therefore be incomplete. Written confirmation of the appointment to the patient is automatically generated when the referral is accepted.
Rejecting referrals
A referral may be rejected under the following conditions:
Clinical decision that the patient does not need a specialist opinion.
Explicit exclusions set out in the DOS (Directory of Services). The referral has not been through the prior approval process
with the PCT.
The referral is not appropriate to that service. CAB must be updated to show the referral has been rejected with a full explanation inserted in the text box. The patient must be advised that the referral has been returned. The Call Centre is responsible for making sure this happens.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 27
Rescheduling appointments by the Trust
Patients who have booked through CAB have, by definition have chosen their appointments to fit in with their other commitments. Rescheduling must be kept to an absolute minimum.
Unavailability on Choose and Book
If a patient is unable to book an appointment due to the unavailability of slots, the Trust on receipt of an email from TAL must:
Contact the Directorate Management Team to ensure more slots are available to CAB.
Phone the patient within 48 working hours to negotiate an appointment. The appointments we offer must be 2 reasonable offers (a choice of 2 dates and a minimum of 3 weeks‟ notice).
If capacity issues cannot be resolved they must be escalated to the Deputy Chief Operating Officer and the Director of Performance.
Performance Management
% services directly bookable % slot availability No of patients not negotiated within 48 hours

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 28
CONSULTANT TO CONSULTANT REFERRAL STANDARDS Patients referred to and seen by a Consultant in a particular speciality may subsequently require an outpatient appointment with another Consultant. These referrals must be managed as follows:
Clinical related referrals
Once a patient has been offered a „choice‟ for a first outpatient appointment and has chosen a provider, the patient has entered into the care pathway on which he/she remains throughout the episode of care. Consequently, if following a consultation a Consultant feels the patient requires an opinion from another Consultant (whether this is in another speciality or within the same speciality) for the condition the patient was originally referred, the Consultant must refer the patient, copying the letter to the GP/referrer for information. This letter must include the 18 week minimum data set – appendix 3.
If the consultant refers to another consultant at BCH (internal referral) the 18 week clock remains ticking from the original referral date.
If the consultant refers to another consultant outside of BCH (external referral) the 18 week clock is still ticking and is inherited by the receiving Trust.
The receiving Consultant must give the referral the same priority as other GP referrals. These secondary referrals will be booked as new attendances with the referral source recorded as referred by consultant. The 18 week clock will continue from the original referral date if the underlying condition remains unchanged. A 2nd opinion requested after a clock stop will initiate a new 18 week clock.
Unrelated referrals
If during investigation and/or treatment of the original condition/referral reason, a separate unrelated condition is identified and the patient is referred on to a new speciality a new 18 week clock will start.
Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 29
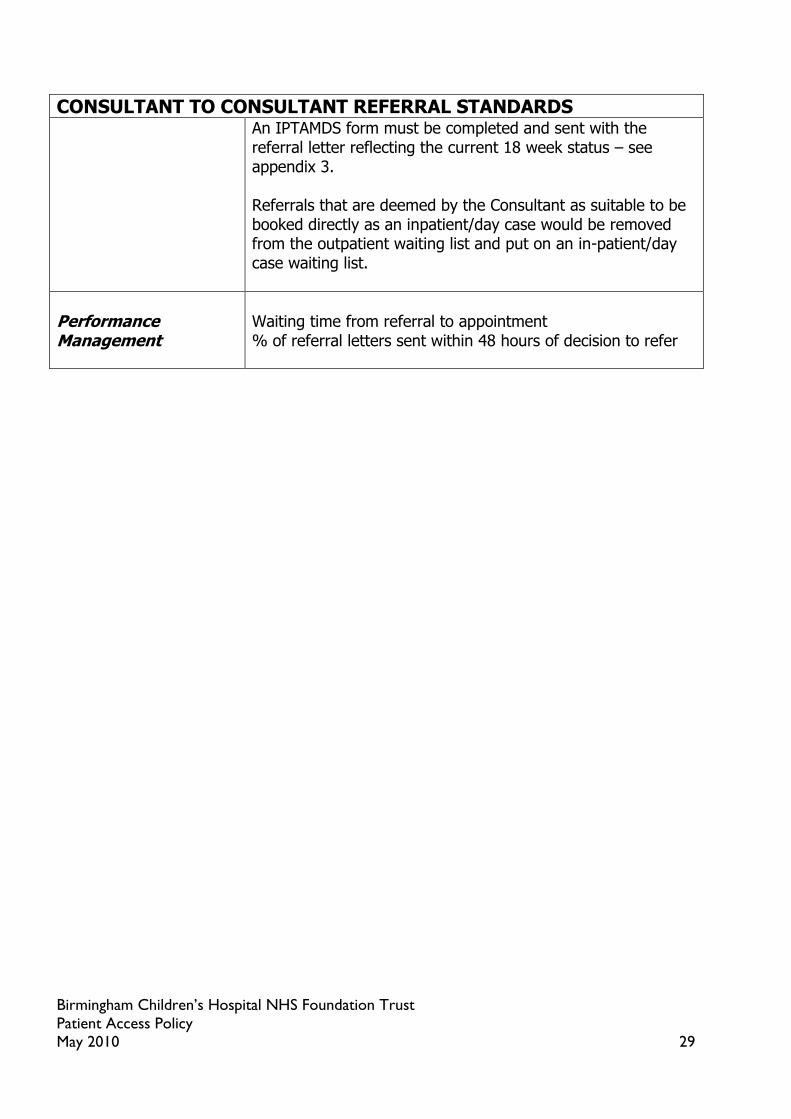
CONSULTANT TO CONSULTANT REFERRAL STANDARDS An IPTAMDS form must be completed and sent with the referral letter reflecting the current 18 week status – see appendix 3. Referrals that are deemed by the Consultant as suitable to be booked directly as an inpatient/day case would be removed from the outpatient waiting list and put on an in-patient/day case waiting list.
Performance Management
Waiting time from referral to appointment % of referral letters sent within 48 hours of decision to refer

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 30
INPATIENT – DEFINITIONS (18 weeks is the Trust‟s delivery standard).
For patients not on an 18 week pathway, no patient should wait longer than 26 weeks an inpatient admission.
Start of wait – Inpatient and day case stage (18 week clock start at initial referral)
When the decision to admit is agreed following a consultant meeting, speciality meeting or an out-patient appointment. The decision to admit date to be used is the date of the meeting or appointment.
Structure of list
Elective Admission List Entry
Waiting list admission. A patient admitted electively from a waiting list having been given no date of admission at a time a decision was made to admit.
Booked admission. A patient admitted having been given a date at the time the decision to admit was made, determined mainly on the grounds of resource availability.
Planned admission. A patient admitted, having been given a date or approximate date at the time the decision to admit was made. This is usually part of a planned sequence of clinical care determined mainly on social or clinical criteria (for example, check cystoscopy). Note: regular day and night admissions should be counted as planned after the first admission, with PATIENT placed on the ELECTIVE ADMISSION LIST between admissions. The date of the DECISION TO ADMIT for regular day and night admissions is the date when arrangements were made for the next admission. It is often the date when the PATIENT was last discharged from hospital.
INPATIENT – STANDARDS
Additions to the list
Patients must be fit, available and ready for surgery or admission for treatment when added to the list.
Patients must have agreed that they want the operation / procedure.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 31
Patients must be available to come in within reasonable notice and should have been asked about personal circumstances that might delay their admission.
Patients must not be added to the waiting list to „reserve‟ a place while they get fit or make up their minds about treatment.
If a patient/parent wishes to take a short amount of time to decide whether to proceed to treatment the 18 week pathway must allow for this period of initial decision making. It is not appropriate to put the patient on watchful wait and stop the clock if the patient/parent only takes a few days to make a decision on whether to proceed with an operation. If the patient/parent chooses to take more than a week to decide if they wish to proceed to treatment, this may be recorded as a patient choice delay, which is a legitimate breach reflected in the 18 week tolerance.
For patients who have had a private outpatient appointment who have then elected to have NHS inpatient treatment, the 18 week clock start date is the date the Trust accepts the referral. In some cases this may not be the same date as the decision to admit date. These patients must be pre-screened prior to listing. A comment should be made on Lorenzo stating that the patient had been seen privately in the past. Bilateral Procedures:
Patient is added to waiting list for the first procedure. Once the procedure is undertaken the clock would stop – use code 30.
The patient would then attend an outpatient appointment for a post operative clinical review where a decision will be taken as to when the patient is ready to be listed for the 2nd procedure. If the patient is ready to undergo the 2nd procedure this will be the start of a new 18 week clock.
Data quality
The following data items must be recorded for every patient. If they are not provided all staff who come in to contact with the patient, who are then informed of the relevant data, are responsible for recording them:
Registered GP NHS number Ethnic coding Overseas visitor status Contact telephone numbers

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 32
School
When the patient is added on to the list
Additions to the waiting list will be recorded on Lorenzo within 24 working hours of decision to admit. The consultant must make sure through one of the following ways that patients understand that they have been added to the list:
Letter Clinical consultation Telephone confirmation
Adding diagnostic and therapeutic procedures to the list
All diagnostic codes or part-diagnostic codes must be clearly identified on the inpatient or day case waiting list using clinical coding. Admission to the ward for a diagnostic procedure does not stop the 18 week clock. Clinical specialities are expected to maintain, with the help of the Clinical Coding Department, a set of appropriate codes used to identify any diagnostic procedures carried out. These codes must be used when adding diagnostic procedures to the waiting list.
Selecting for admission
Clinically urgent patients must have priority.
Planned admissions must come in at the clinically appropriate time. A Monitoring List report is provided on a weekly basis which highlights patients 6 weeks prior to their clinically appropriate admit by date. The 18 week clock does not start until the clinically appropriate time has been reached.
All other patients will be admitted in turn.
Under 18 week rules, this is based on the 18-week RTT waiting time which takes into account any time already spent waiting in outpatients and diagnostics.
Clock pauses
A clock may be paused only where a decision to admit has been made, and the patient has declined at least 2 reasonable appointment offers for admission. The clock is paused for the duration of the time between the earliest reasonable offer and the date from which the patient makes themselves available again for admission.
Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 33
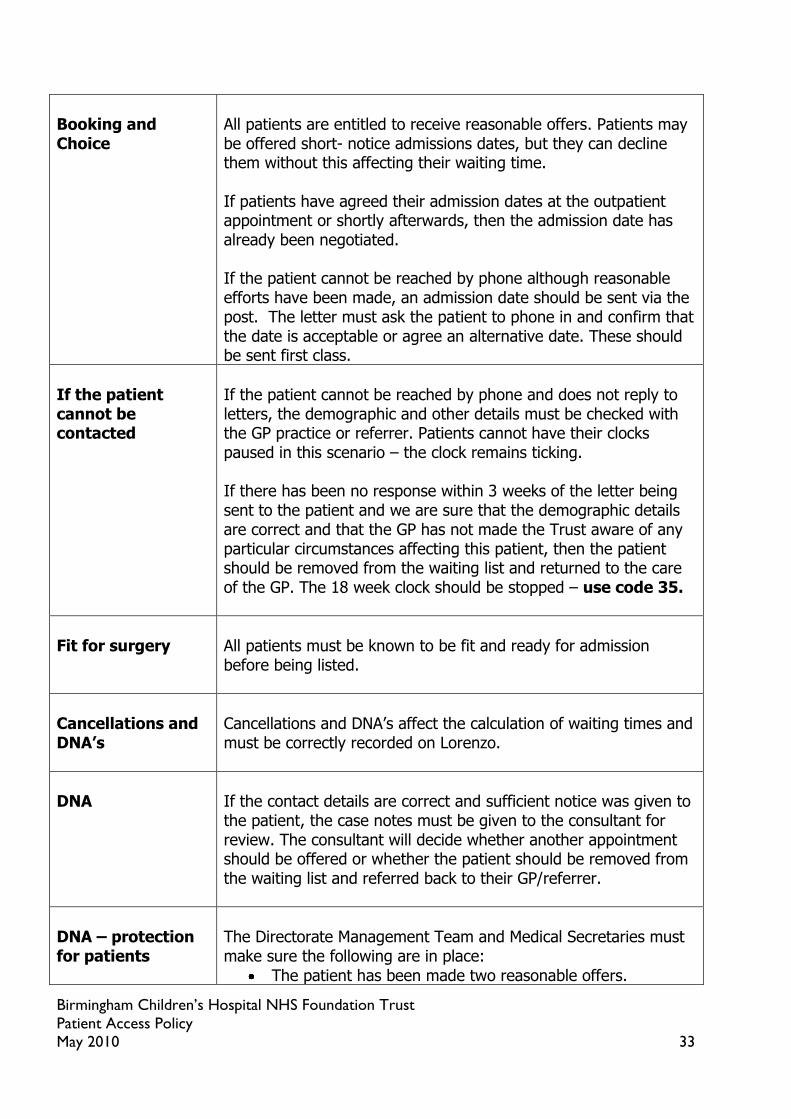
Booking and Choice
All patients are entitled to receive reasonable offers. Patients may be offered short- notice admissions dates, but they can decline them without this affecting their waiting time. If patients have agreed their admission dates at the outpatient appointment or shortly afterwards, then the admission date has already been negotiated. If the patient cannot be reached by phone although reasonable efforts have been made, an admission date should be sent via the post. The letter must ask the patient to phone in and confirm that the date is acceptable or agree an alternative date. These should be sent first class.
If the patient cannot be contacted
If the patient cannot be reached by phone and does not reply to letters, the demographic and other details must be checked with the GP practice or referrer. Patients cannot have their clocks paused in this scenario – the clock remains ticking. If there has been no response within 3 weeks of the letter being sent to the patient and we are sure that the demographic details are correct and that the GP has not made the Trust aware of any particular circumstances affecting this patient, then the patient should be removed from the waiting list and returned to the care of the GP. The 18 week clock should be stopped – use code 35.
Fit for surgery
All patients must be known to be fit and ready for admission before being listed.
Cancellations and DNA’s
Cancellations and DNA‟s affect the calculation of waiting times and must be correctly recorded on Lorenzo.
DNA
If the contact details are correct and sufficient notice was given to the patient, the case notes must be given to the consultant for review. The consultant will decide whether another appointment should be offered or whether the patient should be removed from the waiting list and referred back to their GP/referrer.
DNA – protection for patients
The Directorate Management Team and Medical Secretaries must make sure the following are in place:
The patient has been made two reasonable offers.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 34
There are processes in place to make it simple and easy for patients to cancel or reschedule their admissions or to notify last-minute problems (for example transport not arriving).
It had been made clear to the patient through any verbal and all written communication about the appointment that the patient may be returned to the care of the GP or referrer if they DNA‟d.
If the GP/referrer believes that it was not a true DNA then the patient should be reinstated on the waiting list from the original referral date.
Cancelled by hospital
These cancellations must be kept to an absolute minimum and will be monitored by the Directorate Management Teams. The new admission date must be agreed with the patient. The 18 week clock keeps ticking if treatment has not been provided. The patient must be rebooked and treated within 28 calendar days for elective inpatient/day cases cancelled on the day of the agreed admission date, or a date prior to the end of their 18 week pathway – whichever is the earliest.
Cancelled by patient
If the patient cancels with a reasonable explanation the patient will be remain on the waiting list. A further admission date should be offered within the 18 week pathway – the clock remains ticking. If there is a second patient cancellation and it was a routine admission, a clinical decision will be made regarding the future management of the patient. If the patient is to be removed from the waiting list the Medical Secretaries will advise the Central Admissions Team who will then remove the patient from the waiting list and stop the clock. The Medical Secretaries will send a letter to the GP/referrer/patient advising them of the consultant‟s decision. A copy of the letter will be filed in the patient‟s case notes. If there is a second cancellation but the patient is deemed clinically urgent the future management will be decided by the clinician. If a social concern or a child protection issue exists, a second appointment or admission date will always be offered.
Last minute cancellations of
These are defined cancellations on the day of admission or after admission. The standard is that the patient must be rebooked and

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 35
planned surgery by hospital
treated within 28 calendar days for elective inpatient/day cases cancelled on the day of the agreed admission date, or a date prior to the end of their 18 week pathway – whichever is the earliest. Any potential cancellations, other than for clinical reasons, must be escalated to the Directorate Management Team and Consultant before the patient is cancelled.
Removal from list
Patients may be removed for the following reasons:
Patient decides not to proceed with the treatment. Patient is removed for reasons described in the DNA policy. Patient is removed following a clinical decision not to
proceed. Removals are completed on Lorenzo by the Central Admissions Team when they have received written confirmation from the Medical Secretaries or Directorate Management Team. This must include:
Patient‟s Demographic details. Name of Consultant. Date of planned admission. Reason for removal.
In all cases the Consultant must be made aware of the removal and discussions must take place. A letter must be sent to the patient and copied to the GP and the referrer if it was not the GP.
Recording clinical suspensions and clock pauses
Suspensions must be correctly recorded on RMS and must never be deleted. Suspending affects the calculation of waiting times.
Suspensions, admission dates and self-deferrals
A patient must not be offered a date of admission that falls inside a period of suspension where the patient is unavailable. A patient must not be suspended retrospectively after an admission date has been agreed.
Patients with long
If the patient is likely to be unfit for a prolonged period of time

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 36
periods of suspension – clinical
and unable to attend, the Medical Secretary should make the consultant aware so that he/she can review the case notes. It is the responsibility of the consultant, in discussion with the patient, to decide if the patient should be offered an out-patient appointment to be reassessed or be discharged and returned to the care of the GP/referrer.
The GP/refer can then re-refer the patient when they are fit for surgery. A new 18 week clock would start on receipt of the referral at BCH.
Patients with long periods of suspension – choice
If the patient is unsure about proceeding with treatment the patient‟s notes should be reviewed by the consultant and the patient should either be seen again in out-patients or returned to the care of the GP.
Patients who refuse a reasonable offer date due to choice
For in-patients and day cases, if the patient is unable to commit to a date due to a holiday/social reasons even though two reasonable offers have been made, the clock can be paused from the date of the first reasonable offer to the date from which the patient makes themselves available again.
Transfers between consultants
If the patient has been added to a particular consultant‟s waiting list, he or she has the right to remain on that list with the consultant, without prejudice to the waiting time. If the patient has been added to a pooled list and it has been explained from the start that this is a pooled list, then he or she can reasonably be offered treatment with any suitably qualified consultant.
Reasons for clock pauses
Pauses should not exceed more than 6 months without a
future plan.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 37
Performance Management
Waiting time for inpatient admission following decision to admit. % patients clinically graded as urgent seen within appropriate time.
Data Quality
Patient on as “planned” without an admit by date. Patients with no admission type.
Patients whose waiting list type has been changed. % of patients by waiting list type by speciality –
reviewed monthly against agreed tolerance levels.
Patients whose waiting list specialty does not match the specialty of the linked referral.
Patients who are suspended but the comments field is blank.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 38
DIAGNOSTIC – DEFINITIONS Diagnostic “Diagnostic” means a test or procedure used to identify a
person‟s disease or condition and which allows a medical diagnosis to be made.
Therapeutic A “therapeutic procedure” is defined as a procedure that involves actual treatment of a person‟s disease, condition or injury.
Diagnostic or therapeutic?
Some procedures are intended as diagnostic up until a point during the procedure, when the healthcare professional makes a decision to undertake a therapeutic treatment at the same time. These procedures should still be reported in Department of Health returns as diagnostic. Some procedures will include both a diagnostic test and therapeutic treatment. If the procedure is part-diagnostic or intended to be part-diagnostic, these should be counted as diagnostic procedures. Note: A list of tests and OPCS codes for inpatient or day case procedures can be found in the Department of Health‟s publication Diagnostics Census: Guidance on completing the “diagnostic waiting times” census. Version 3 – March 2007.
Start of diagnostic wait When the request for a diagnostic test or procedure is made. This is the date that the request was initiated and not the date when it was received in the department. The date on the request card or the electronic equivalent is the simplest proxy. If the patient is waiting for a diagnostic test to be carried out as an inpatient or day case, e.g. endoscopy, then the start of the wait is the date of decision to admit. If the patient is waiting as an outpatient, e.g. for neurophysiology, then the start of the wait is the date the referral was made. The 18 week clock could still be ticking until first definitive treatment is provided.
Adjustment to wait If a patient cancels or misses an appointment for a diagnostic test/procedure, the 6 week clock can be restarted. The 18 week clock is still ticking until first definitive treatment is provided. If the provider cancels the appointment, the diagnostic waiting time is not affected.
Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 39
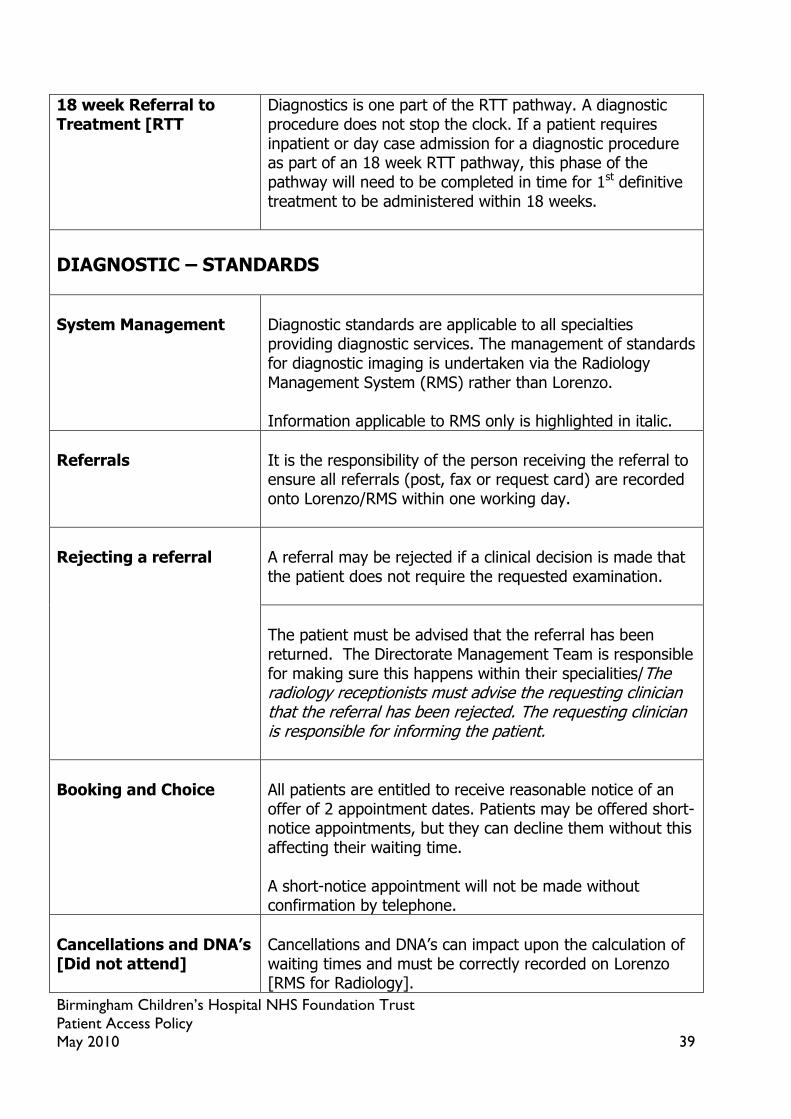
18 week Referral to Treatment [RTT
Diagnostics is one part of the RTT pathway. A diagnostic procedure does not stop the clock. If a patient requires inpatient or day case admission for a diagnostic procedure as part of an 18 week RTT pathway, this phase of the pathway will need to be completed in time for 1st definitive treatment to be administered within 18 weeks.
DIAGNOSTIC – STANDARDS
System Management
Diagnostic standards are applicable to all specialties providing diagnostic services. The management of standards for diagnostic imaging is undertaken via the Radiology Management System (RMS) rather than Lorenzo. Information applicable to RMS only is highlighted in italic.
Referrals
It is the responsibility of the person receiving the referral to ensure all referrals (post, fax or request card) are recorded onto Lorenzo/RMS within one working day.
Rejecting a referral
A referral may be rejected if a clinical decision is made that the patient does not require the requested examination.
The patient must be advised that the referral has been returned. The Directorate Management Team is responsible for making sure this happens within their specialities/The radiology receptionists must advise the requesting clinician that the referral has been rejected. The requesting clinician is responsible for informing the patient.
Booking and Choice
All patients are entitled to receive reasonable notice of an offer of 2 appointment dates. Patients may be offered short-notice appointments, but they can decline them without this affecting their waiting time. A short-notice appointment will not be made without confirmation by telephone.
Cancellations and DNA’s [Did not attend]
Cancellations and DNA‟s can impact upon the calculation of waiting times and must be correctly recorded on Lorenzo [RMS for Radiology].

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 40
DNA at first or subsequent appointment
If a patient DNA‟s an appointment the referral must be reviewed by the requesting clinician. Cancer and suspected cancer patients will be offered another appointment. Vulnerable patients will be offered at least one further appointment at the discretion of the Clinician.
DNA – protection for patients
Each Directorate Management Team must make sure that the following are in place:
The appointment letter was received. The correct demographics are recorded. The patient has been made a reasonable offer – offer
of 2 appointment dates.
There are processes in place to make it simple and easy for patients to cancel or reschedule their appointments or to notify last minute problems [for example, transport not arriving].
It has been made clear to the patient through any verbal and all written communication about the appointment that the patient may be returned to the care of the requesting clinician if he or she DNA‟s.
If a patient DNA‟s they are removed from the waiting list by the Central Admissions Team and the requesting clinician is notified. The clinician will re-assess the request and if a subsequent appointment is required the patient is put back on the waiting list as a new patient.
Cancelled by hospital
The patient‟s waiting time is not affected – the clock is still ticking. These cancellations must be kept to an absolute minimum and will be monitored by the Directorate Management Teams. The new date must be agreed with the patient.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 41
Last minute cancellations of planned diagnostics by hospital
These are defined as cancellations on the day of admission or after admission. The standard is that the patient must be rebooked and treated within 28 calendar days for elective inpatient/day cases cancelled on the day of the agreed admission date, or a date prior to the end of their 18 week pathway – whichever is the earliest.
These cancellations must be kept to an absolute minimum.
Any potential cancellations, other than for clinical reasons, must be escalated to the Directorate Management Team and the requesting clinician before the patient is cancelled.
Cancelled by patient
If the patient cancels and still requires an appointment the patient remains on the waiting list. The 6 week clock will re-start from the date of the cancelled appointment. The 18 week clock will not reset.
If there is a second patient cancellation and it was a routine admission the Central Admissions Team/radiology receptionists will remove the patient from the waiting list and a letter will be sent to the requesting clinician advising them of the outcome. A copy of this letter will also be filed in the case notes.
If there is a second cancellation but the patient is deemed clinically urgent, the future management of the patient will be decided by the clinician.
Note: If a social concern or a child protection issue exists, a further appointment or admission date will always be offered.
If a patient cancels and does not want an appointment, the referral will be returned to the requesting clinician and they will be removed from the waiting list.
Removal from list Patients may be removed for the following reasons:
Patient decides not to proceed with the treatment.
Patient is removed for reasons described in the DNA policy.
Patient is removed following a clinical decision not to proceed.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 42
If the patient has been TCI‟d the medical secretaries/ radiology receptionists must provide written confirmation to the Central Admissions Team to remove the patient from the list on Lorenzo. This must include:
Patient‟s Demographic details Name of Consultant Date of planned admission Reason for removal
Removals are completed on RMS by the radiology receptionists. In all cases the requesting clinician must be made aware of the removal.
Recording Pauses
Non-admitted Pathway:
Clock pauses on a non admitted pathway cannot be used to manually adjust the patient‟s wait time.
Admitted Pathway:
Clock pauses can be applied to an admitted pathway and can be used to adjust the 18 week wait time. The wait time can only be adjusted if there is clear evidence that the patient was offered 2 reasonable dates
Pauses can only be applied for social reasons Pauses cannot be applied for clinical reasons
Suspensions, admission dates and self-deferrals
A patient must not be offered a date of admission that falls inside a period of suspension where the patient is unavailable. A patient must not be suspended retrospectively after an admission date has been agreed. Suspensions must not exceed 6 months without a future plan.
Patients with long periods of suspension – clinical
Patients must not be removed arbitrarily from the list. The situation must be in discussion with the requesting clinician. If the patient has been removed from the list the requesting clinician can re-request if and when appropriate.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 43
CANCELLED OPERATIONS STANDARDS The NHS standard, effective from April 2002 says:
Patients should not have their elective operations cancelled on the day of admission or after admission for non-clinical reasons.
If the operation is cancelled, then the patient must be given a firm date for admission that is within 28 days of the cancelled date. If this is not done, then patients are entitled to have their operations performed at a provider and on a date of their choice funded by the original provider.
Analysis of cancellations
Directorate Management Teams must review cancelled operations weekly and take effective action to reduce the numbers. Root causes analysis will be carried out for all cancelled operations and reviewed monthly.
Re-dating patients A new and appropriate date must be agreed with the patient when he or she is cancelled. For patients who have been admitted, it must be agreed with them before they leave hospital. For patients who are cancelled on the day of admission and before they come into the hospital, it must be agreed with them at the time that they are cancelled (in the same phone call)
Second cancellation
If a patient is cancelled for non-clinical reasons they cannot be cancelled more than once. Any potential cancellation for the second time must be escalated explicitly to the Directorate Management Teams before cancellation.
Performance Management
% operations cancelled on the day as % of overall FCEs % cancellations on the day readmitted within 28 days Number of root cause analysis to ensure all cancelled operations are investigated. Number of patients whose operation is cancelled more than once.
Data Quality Reporting times

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 44
PATIENTS WITH SUSPECTED AND DIAGNOSED CANCER - REFERRAL MANAGEMENT All cancer patient pathways should be dealt with according to the principles laid out in the DH document „Going Further on Cancer Waits‟ v6.5 (2009).
TWO WEEK WAIT STANDARD – DEFINITIONS
Two week standard from urgent GP/GDP referral for suspected cancer Overview There should be a maximum 2 week wait from an urgent GP/GDP
referral for suspected cancer to first hospital assessment.
Start of wait The clock starts when the GP refers a patient for urgent investigation of symptoms, when a malignant diagnosis is suspected. See (clock starts) section below for the precise clock start point.
Clock starts A 2 week pathway starts when the Trust receives the referral (recorded as the CANCER REFERRAL TO TREATMENT PERIOD START DATE). This original referral can be received either:
Direct from the General Medical Practitioner/General Dental Practitioner (ORIGINAL REFERRAL REQUEST RECEIVED DATE)
Via Choose & Book, in which case the UBRN CONVERSION DATE (the Unique Booking Reference Number conversion date for an appointment) would mark the start of the period.
Referrals from primary care to the following services start 2 week clocks:
Medical or surgical consultant-led services irrespective of setting
Straight to test – the GP refers the patient to a secondary care consultant and refers for the test at the same time.
Referrals to nurse consultants and allied health professionals are not covered under 2 weeks
Examples of referrals which may start an 2 week clock are:
Referrals from General Practitioners & General Dental Practitioners for suspected malignancy labelled as urgent, even if the two week wait is not mentioned specifically in the referral communication.
Referrals to National Screening programmes

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 45
TWO WEEK WAIT STANDARD – DEFINITIONS Clock stops The clock stops when:
The period end is when the patient is seen for the first time by a consultant or in a diagnostic clinic following the referral receipt. This is recorded as DATE FIRST SEEN.
Once a referral to secondary care has been made:
A patient cannot be referred back to the GP: - if they are unable to accept an appointment within 2
weeks. Once a referral has been received by secondary care it should not be returned due to patient unavailability
- after a DNA of their first appointment - after a single appointment cancellation - after multiple (2 or more) cancellations, unless this has
been agreed with the patient (by cancelling an appointment a patient has shown a willingness to engage with the NHS)
- if they are not immediately fit for diagnostics/treatments needed
- if they have not made contact after a first DNA within a given time period,
- if they have been referred under the 2ww by a GP inappropriately (the GP should be asked to withdraw an inappropriate referral in this scenario).
A patient can be referred back to their GP if: - a consultant thinks the two week wait‟ referral is
inappropriate and this has been discussed with the GP and the GP has agreed to withdraw the two week wait referral status
- after multiple (2 or more) DNAs but not after 2 non attendances where one non attendance is due to a cancellation.
Clock Pauses The pauses permissible in this pathway are the same as in the outpatient phase of the 18 week system i.e.: Pause for DNA of initial outpatient appointment
If a patient does not turn up (i.e. gives no notice) for the outpatient appointment/diagnostic clinic that would have been recorded as DATE FIRST SEEN then the clock can be stopped from the date of the receipt of the referral (recorded as the CANCER REFERRAL TO TREATMENT PERIOD START DATE) to the date the patient rebooks their appointment as shown below
DNA is defined as a patient failing to attend an

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 46
TWO WEEK WAIT STANDARD – DEFINITIONS appointment/admission without prior notice.
Cancellations (defined as a patient giving any notice that they are unable to attend an appointment) do not pause the pathway.
Key Access Considerations
A patient should be referred by their GP at the earliest opportunity. Receipt of this referral flags to the receiving organisation that there is a potential cancer case on its way.
A GP should not be encouraged to withhold a referral if a patient is unable to attend an appointment within 14 days. The operational standard takes account of such circumstances and this behaviour conflicts with the principles of awareness and early detection.
A patient should be given the information leaflet „Why Have I Been Given a „Two Week Wait‟ Hospital Appointment?‟ This explains why they are being referred urgently, the importance of being seen quickly and the importance for the NHS of patients keeping appointments.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 47
MAXIMUM 31 DAYS FROM URGENT GP REFERRAL TO FIRST TREATMENT FOR CHILDREN’S CANCER (31 DAY RTT)
31 DAY RTT PATHWAY - DEFINITIONS Overview For those patients who are referred under the urgent 2 week
standard and subsequently diagnosed with cancer there should be a maximum 31 day wait between the original GP referral and the first treatment commencing.
Start of wait The clock starts when the GP refers a patient for urgent investigation of symptoms, when a malignant diagnosis is suspected. See [clock starts] section below for the precise clock start point.
Clock starts A 31 Day RTT pathway starts when the Trust receives the referral (recorded as the CANCER REFERRAL TO TREATMENT PERIOD START DATE). This original referral can be received either:
Direct from the General Medical Practitioner/General Dental Practitioner (ORIGINAL REFERRAL REQUEST RECEIVED DATE)
Via Choose & Book, in which case the UBRN CONVERSION (the Unique Booking Reference Number conversion date for an appointment) would mark the start of the period.
Referrals from primary care to the following services start 31 Day RTT clocks:
Medical or surgical consultant-led services irrespective of setting
Straight to test – the GP refers the patient to a secondary care consultant and refers for the test at the same time.
Examples of referrals which may start an 2 week clock are:
Referrals from General Practitioners & General Dental Practitioners for suspected malignancy labelled as urgent, even if the two week wait is not mentioned specifically in the referral communication.
Referrals to National Screening programmes
Clock stops The period end is the first definitive treatment – this is recorded as the TREATMENT START DATE (CANCER). This start date may differ slightly for different treatments. For example, it would be:
the date the patient is admitted for an operation, for surgery – code 01
the date the first drug in an agreed course is given, for „anti-

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 48
31 DAY RTT PATHWAY - DEFINITIONS cancer drug regimen (cytotoxic chemotherapy)‟ – code 02;
the date the first fraction is given, for teletherapy (beam radiation excluding proton therapy) – code 05
Clock Pauses The pauses permissible in this pathway are the same as in the outpatient phase of the 18 week system i.e.: Pause for DNA of initial outpatient appointment
If a patient does not turn up (i.e. gives no notice) for the outpatient appointment/diagnostic clinic in the 2 week phase, that would have been recorded as DATE FIRST SEEN then the clock can be stopped from the date of the receipt of the referral (recorded as the CANCER REFERRAL TO TREATMENT PERIOD START DATE) to the date the patient rebooks their appointment as shown below
DNA is defined as a patient failing to attend an appointment/admission without prior notice.
Cancellations (defined as a patient giving any notice that they are unable to attend an appointment) do not pause the pathway.
Patient declines reasonable offer of admitted care
If the first treatment will involve admitted care, a patient has to be offered a „To Come In‟ (TCI) date for inpatient care (ordinary admission or day case) within the 31 or 62 day period. If the offer is declined the clock can be stopped from the date of the declined appointment to the point when the patient could make themselves available for an alternative admission.
This pause only applies to TCI offers for admitted care. As is the case with the 18 week pathway, no adjustments are permissible for non-admitted care.
Key Access Considerations
The 31 day count applies to children (under 16 years old), with cancer, and also those aged 16 or over who have acute leukaemia or testicular cancer. All other over 16s would be monitored against the adult RTT pathway of 62 days.
THIS STANDARD IS THE ONLY CANCER WAIT PATHWAY FOR WHICH RESPONSIBILITY FOR DELIVERY IS SHARED BETWEEN ACUTE TRUSTS – THERE IS THEREFORE THE RISK OF BIRMINGHAM CHILDREN’S HOSPITAL HAVING TO RECORD A BREACH ON A CASE THAT HAS BEEN REFERRED TO US LATE ON THE PATHWAY.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 49
31 DAYS FROM DECISION TO TREAT TO FIRST TREATMENT (31 DAY DTT)
31 DAY DTT PATHWAY – DEFNITIONS Overview This target applies to those patients who are diagnosed with cancer
who were not originally referred on the urgent two week pathway (e.g. they may have been referred routinely for non-specific symptoms). For these patients there should be a maximum wait of 31 days from when the treatment plan is decided upon, to the date the first treatment begins. It should noted that this pathway applies to a significant majority of the new cancer patients seen at Birmingham Children’s Hospital – relatively few are referred under the 2 week wait system/31 Day RTT pathway.
Start of wait The clock starts when the patient with a new cancer diagnosis who is not on the urgent pathway agrees their treatment plan with their consultant.
Clock starts A 31 Day DTT pathway starts when the patient agrees their treatment plan with the relevant consultant:
The starting point for this standard remains the date that a patient agrees a plan for their treatment. This is recorded as the CANCER TREATMENT PERIOD START DATE
Clock stops The period end is the first definitive treatment – this is recorded as the TREATMENT START DATE (CANCER). This start date may differ slightly for different treatments. For example, it would be:
the date the patient is admitted for an operation, for surgery – code 01
the date the first drug in an agreed course is given, for „anti-cancer drug regimen (cytotoxic chemotherapy)‟ – code 02;
the date the first fraction is given, for teletherapy (beam radiation excluding proton therapy) – code 05
Clock Pauses
The pauses permissible in this pathway are the same as in the outpatient phase of the 18 week system i.e.: Patient declines reasonable offer of admitted care
If the first treatment will involve admitted care, a patient has to be offered a To Come In (TCI) date for the inpatient care within the 31 day period. If the offer is declined the clock can be stopped from the date of the declined appointment to the point when the patient could make themselves available for an alternative admission.
This pause only applies to TCI offers for admitted care. As is the case with the 18 week pathway, no adjustments are permissible for non-admitted care.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 50
CONSULTANT UPGRADE ONTO 62 DAY UPGRADE TO TREATMENT PERIOD
CONSULTANT UPGRADE 62 DAY PATHWAY - DEFNITIONS Overview A consultant can choose to move the patient onto a 62 pathway
from the upgrade date to the date of first treatment:
An upgrade may occur for any case where a patient has not been referred as suspected two week wait (including breast symptoms), or has not been enrolled onto the 62 day pathway as a result of an abnormality identified by any one of the 3 cancer screening programmes. [The assumption is that by upgrading a patient they will be in the same position, or thereabouts, as if they had been originally referred as suspected two week or via the screening programmes.]
Start of wait The clock starts when a consultant decides to upgrade a patient.
Clock starts The starting point for this 62 day period is the date on which the consultant decides to upgrade the patient. This is recorded as the CONSULTANT UPGRADE DATE.
An upgrade may occur at any stage between receipt of referral and treatment decision making MDT. In practical terms an upgrade should occur at the earliest point in the pathway at which cancer is suspected and it is therefore it is expected that this decision would take place prior to the treatment decision making MDT. Upgrade is not permitted after this MDT
An upgrade can be made by the patient‟s identified consultant or, in the case of abnormal chest x-rays, can be made by a consultant radiologist. This will occur where, on the basis of information received (referral or test results) or contact with the patient, the consultant has a strong suspicion that the diagnosis is, or is likely to be, cancer. An upgrade should still occur where referral to another MDT is anticipated regardless of whether this is referral is within the same Trust or to another Trust.
An upgrade must be on or before a decision to treat a patient has been agreed (i.e. before the DECISION TO TREAT DATE recorded as the CANCER TREATMENT PERIOD START DATE (if recorded). It must also be on or before the multidisciplinary team meeting where the care plan that was subsequently agreed with the patient was discussed ie. the

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 51
CONSULTANT UPGRADE 62 DAY PATHWAY - DEFNITIONS MULTIDISCIPLINARY TEAM DISCUSSION DATE (CANCER) (if recorded).
Clock stops The period end is the first definitive treatment – this is recorded as the TREATMENT START DATE (CANCER). This start date may differ slightly for different treatments. For example, it would be:
the date the patient is admitted for an operation, for surgery – code 01
the date the first drug in an agreed course is given, for „anti-cancer drug regimen (cytotoxic chemotherapy)‟ – code 02;
the date the first fraction is given, for teletherapy (beam radiation excluding proton therapy) – code 05
Clock Pauses The pauses permissible in this pathway are the same as in the outpatient phase of the 18 week system i.e.: Patient declines reasonable offer of admitted care
A patient has to be offered a „To Come In‟ (TCI) date for inpatient care (ordinary admission or day case) within the 62 day period. If the offer is declined the clock can be stopped from the date of the declined appointment to the point when the patient could make themselves available for an alternative admission.
This pause only applies to TCI offers for admitted care. As is the case with the 18 week pathway, no adjustments are permissible for non-admitted care.
Key Access Considerations
Recurrences are not subject to 62 day target monitoring and are not expected to be upgraded as part of the implementation of the Cancer Reform Strategy targets.
Where within the 18 week period can an upgrade take place? Examples of when an upgrade might take place include: - on reading the referral letter; after seeing the patient for
the first time - after seeing test results (before or after seeing the patient) - after discussing the patient‟s case at a multidisciplinary
team meeting.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 52
31 DAYS FROM DECISION TO TREAT TO SUBSEQUENT TREATMENT (31 DAY SUBSEQUENT DTT)
31 DAY DTT SUBSEQUENT PATHWAY - DEFNITIONS Overview There should be a maximum 31 day wait from the decision to
treat/earliest clinically appropriate date to start of second or subsequent treatment(s) for all cancer patients including those diagnosed with a recurrence.
Start of wait The clock starts when the patient agrees to subsequent treatment with their consultant, or when they reach the earliest clinically appropriate date (ECAD) for a subsequent treatment which was agreed as part of the original treatment plan.
Clock starts The starting point for this 31 day period (recorded as the CANCER TREATMENT PERIOD START DATE) is either:
The DECISION TO TREAT DATE (DTT) – i.e. the date that a patient agrees a treatment plan for first or subsequent treatments within a Cancer Care Plan.
The EARLIEST CLINICALLY APPROPRIATE DATE (ECAD) - where there is no new DECISION TO TREAT DATE, but there has been a previously agreed and clinically appropriate period of delay before the next treatment can commence. In this case the subsequent activity may not be the start of the subsequent treatment itself, but could be the next appointment which deals with the planning of that subsequent treatment.
The ECAD is the earliest date that it is clinically appropriate for the next activity related to a treatment to take place. The activity may not always be the start of the treatment itself but could be the next appointment which deals with the planning of that treatment. When determining an ECAD only patient issues should be considered, and not local capacity constraints. Within the CWT-Db, ECAD is an option for the population of the field CANCER TREATMENT PERIOD START DATE which marks the start of a 31 day subsequent treatment period. Examples would be: - Patient with rectal cancer is to have radiotherapy
then surgery - after the radiotherapy the patient is not expected to be clinically fit for surgery for 6 weeks so the ECAD would be set for 6 weeks after radiotherapy
- Patient with breast cancer is to have surgery then radiotherapy – the patient would not be fit for planning radiotherapy until they are able to lift their arm over their

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 53
31 DAY DTT SUBSEQUENT PATHWAY - DEFNITIONS head – ECAD would be set for when the patient would be fit for radiotherapy planning to start.
ECAD decisions can be kept under review. For example, if an ECAD is set for 20 February 2009 but at a clinical review on 26 January it is clear that the patient has not recovered from an operation the ECAD could be put back to 2 March 2009. However, if 20 February has passed and the patient is unwell it would not be possible to reset the ECAD.
The ECAD can be set at a number of points including: at the clinical review with the patient following the preceding treatment. If it is not possible to make a decision at the review a further review could be arranged - at the start of the preceding treatment if the patient will
not be reviewed between treatments; - at the MDT meeting if it is possible to identify the likely
ECADs between treatments in an agreed package; - following receipt of test results and prior to seeing the
patient if this is quickest.
Clock stops The period end is the date on which the subsequent treatment starts – this is recorded as the TREATMENT START DATE (CANCER). This start date may differ slightly for different treatments. For example, it would be:
the date the patient is admitted for an operation, for surgery – code 01
the date the first drug in an agreed course is given, for „anti-cancer drug regimen (cytotoxic chemotherapy)‟ – code 02;
the date the first fraction is given, for teletherapy (beam radiation excluding proton therapy) – code 05
Clock Pauses
The pauses permissible in this pathway are the same as in the outpatient phase of the 18 week system i.e.: Patient declines reasonable offer of admitted care
A patient has to be offered a „To Come In‟ (TCI) date for inpatient care (ordinary admission or day case) within the 31 or 62 day period. If the offer is declined the clock can be stopped from the date of the declined appointment to the point when the patient could make themselves available for an alternative admission.
This pause only applies to TCI offers for admitted care. As is the case with the 18 week pathway, no adjustments are

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 54
31 DAY DTT SUBSEQUENT PATHWAY - DEFNITIONS permissible for non-admitted care.
Definition of Subsequent Treatment
A subsequent treatment could be: an anti-cancer treatment (curative or palliative) aimed at
shrinking (or delaying the growth/spread) of the tumour/cancer
the provision of palliation for the symptoms resulting from the tumour/cancer
active monitoring (where no active or palliative treatment is appropriate)
symptomatic support by non-specialist palliative care teams An individual patient may receive one, or a combination of many of these interventions.
a course of chemotherapy is counted as a subsequent treatment not each cycle within that course. A change in drug type within chemotherapy would be classed as a subsequent treatment if it was a second treatment course.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 55
CANCER WAITING TIMES REFERRAL STANDARDS
CANCER WAIT STANDARDS The current set of Cancer Waiting Times Targets was originally set out in the „Cancer Reform Strategy‟ (2008). More detailed guidance was subsequently provided by the DH in 2009 in the following documents:
„Going Further on Cancer Waits‟ version 6.5 „Going Further on Cancer Waits Guidance: Dataset Chapter‟
They apply to every English NHS patient treated for cancer in the English NHS.
General The specific standards for each stage of treatment (outpatient, diagnostic, inpatient or day case) must all be followed. This includes:
Recording and grading a referral – identifying whether they are urgent referrals requiring an appointment within 2 weeks.
2 week wait from GP/GDP referral to date first seen For children referred on the 2 week pathway, a 31
day maximum wait from the original GP/GDP referral to 1st treatment
For those not referred on the urgent 2 week route, a 31 day wait from decision to treat to first treatment.
Option for consultants to upgrade patients referred routinely onto 62 day pathway from upgrade to first treatment.
31 day wait for subsequent anti-cancer treatments.
Data Standards The full title of the Cancer Waits dataset is the „National Cancer Waiting Times Monitoring Dataset‟. This dataset is more complex than that required for the 18 weeks pathway. Appendix 4 lists the data items and provides an indication of whether these are mandatory or optional. Full definitions of each of the terms are available on the Connecting for Health Data Dictionary website, in the „clinical datasets‟ section.
Measurement
It is not possible to measure the Trust‟s compliance with the Cancer Waits standards unless the relevant patient pathway details are recorded. As indicated, Appendix 8 outlines the mandatory data requirements that the Trust must collect for each patient to monitor the cancer pathways:
Once collected the information is entered on the Somerset Cancer Register (SCR) system. This

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 56
CANCER WAIT STANDARDS database is used to run cancer-specific PTLs to monitor the status of cancer patients in relation to the cancer waiting times targets.
At the end of each month the waiting times data for the month is uploaded from the SCR to the DH Open Exeter website via csv file.
Inter-Provider Transfers When a patient is transferred from one acute sector- provider to another a minimum amount of cancer waits data must accompany them, so that the management at the receiving provider can monitor the patient accurately. When a patient is transferred a „tertiary alert form‟ is filled in by the transferring trust. This must then be faxed to the dedicated oncology referral fax in the receiving trust (this is in addition to the clinical referral letter). The Pan Birmingham Cancer Network has produced a tertiary alert form for use by all Trusts in the Network (Appendix 5). This must be obtained for:
Referrals or transfers from other hospitals This must be provided for:
Patients transferred or referred to another provider.
Patients transferred back to their local hospital for post-operative care.
Adjustments/suspensions to the Cancer pathways
The adjustments permissible on the cancer pathways are the same as on the 18 week pathway, with the exception of how a 1st DNA of outpatient appointment is dealt with Pause for DNA of initial outpatient appointment
If a patient does not turn up (i.e. gives no notice) for the outpatient appointment/diagnostic clinic in the 2 week phase, that would have been recorded as DATE FIRST SEEN then the clock can be stopped from the date of the receipt of the referral (recorded as the CANCER REFERRAL TO TREATMENT PERIOD START DATE) to the date the patient rebooks their appointment as shown below
DNA is defined as a patient failing to attend an appointment/admission without prior notice.
Cancellations (defined as a patient giving notice that they are unable to attend an appointment) do

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 57
CANCER WAIT STANDARDS not pause the pathway.
Patient declines reasonable offer of admitted care
A patient has to be offered a To Come In (TCI) date for inpatient care (ordinary admission or day case) within the 31 or 62 day period. If the offer is declined the clock can be stopped from the date of the declined appointment to the point when the patient could make themselves available for an alternative admission.
This pause only applies to TCI offers for admitted care. As is the case with the 18 week pathway, no adjustments are permissible for non-admitted care.
DNA at 1st appointment on 2 week urgent pathway
If a patient has been referred as a 2 week wait and DNAs their first appointment the clock can be suspended, but the patient should automatically be contacted and offered another appointment (unlike on the standard 18 week route). Only after the 2nd DNA can steps be taken to return the referral.
DNA at inpatient admission
If a cancer or suspected cancer patient DNAs an admission, they should be offered another date.
DNA & patient initiated cancellation - protection for patients on urgent 2 week pathway (outpatient)
A patient cannot be referred back to the GP: - if they are unable to accept an appointment
within 2 weeks. Once a referral has been received by secondary care it should not be returned due to patient unavailability.
- after a DNA of their first appointment. - after a single appointment cancellation . - after multiple (2 or more) cancellations, unless
this has been agreed with the patient (by cancelling an appointment a patient has shown a willingness to engage with the NHS).
- if they are not immediately fit for diagnostics/ treatments needed.
- if they have not made contact after a first DNA within a given time period.
- if they have been referred under the 2ww by a GP inappropriately (the GP should be asked to withdraw an inappropriate referral in this scenario).
A patient can be referred back to their GP if: - a consultant thinks the two week wait‟ referral is
inappropriate and this has been discussed with

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 58
CANCER WAIT STANDARDS the GP and the GP has agreed to withdraw the two week wait referral status
- after multiple (2 or more) DNAs but not after 2 non attendances where one non attendance is due to a cancellation.
Patient-initiated cancellation Outpatients Diagnostic Inpatient Day Case Pre-operative assessment
If the patient has:
Agreed a date and then cancelled it an agreed second date will be arranged in liaison with the patients. If the patient cancels again the patient should be informed that the referral will be reviewed by the clinician.
Note: If the patient is cancelled by the hospital, then the process for agreeing a date begins again.
Cancellations by the hospital Outpatients Diagnostic Inpatient Day Case Pre-operative assessment
These must be kept to a minimum. The patient‟s clock does not stop for a hospital-initiated cancellation. The patient must be rebooked and treated within the cancer waiting times standards.
Patient Choice Outpatients Diagnostic Inpatient Day Case Pre-operative assessment
Patients can choose to rearrange an initial outpatient appointment on a 2 week wait
For treatment patients have the right to refuse a reasonable offer date for admitted care
Only one reasonable offer date needs to be supplied to the patient for admitted treatment – the 18 week method of offering 2 dates with 3 weeks notice does not apply to cancer waits.
Patient is unfit Outpatient Diagnostic Inpatient Day Cases
If a patient becomes unfit once they have started a pathway then no suspensions or adjustments are permitted on the cancer pathways – the clock continues. This will potentially result in breaches but this is reflected in the current national operational standards that indicate the performance levels Trusts should reach.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 59
CANCER WAIT STANDARDS Performance Management
Cancer Wait National Operational Standards Trusts should aim to deal with the following percentage of pathways in time:
62-Day (Urgent GP Referral To Treatment) Wait For First Treatment: All Cancers – 85%
62-Day Wait For First Treatment From Consultant Screening Service Referral: All Cancers – 90%
31-Day (Decision To Treatment) Wait For First Treatment: All Cancers 96%
31-Day Wait For Second Or Subsequent Treatment: Anti Cancer Drug Treatments (chemotherapy) – 98%
31-Day Wait For Second Or Subsequent Treatment: Surgery – 94%
31-Day Wait For Second Or Subsequent Treatment: Radiotherapy Treatments - 94%
All Cancer Two Week Wait - 93% Two Week Wait for Symptomatic Breast Patients
(Cancer Not initially Suspected) - 93%
Data Quality There are established information sharing links between oncology/haematology and other specialties who may deal with cancer pathways (e.g. dermatology, ophthalmology.
The Somerset Cancer Register has standard data management & audit tools that ensure the waiting times data collected is consistent and adheres to the requirements of the National Cancer Waiting Times Monitoring Dataset, in preparation for upload to Open Exeter.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 60
PERFORMANCE MANAGEMENT The Trusts are required to ensure that 95% of patients on a non-admitted and 90% of patients on an admitted pathway are treated within 18 weeks.
Weekly
A weekly report of all patients on a RTT pathway and inpatient and outpatient waiting times for those not on a pathway is sent to the Directorate Management Team and Patient Access Team by the Information Department.
The Directorate Management Teams reconcile the PTL [patient tracking list] and forward exception reports to the Patient Access Manager for patients: Non-Admitted:
Waiting for 1st appointment without a date at 6 weeks.
Waiting 10 weeks or more with no further appointment [follow up or TCI.
Admitted:
Waiting 10 weeks or more with no TCI. With a TCI date greater than 18 weeks.
Diagnostics:
Patients who are or will be waiting 6 weeks or more without a date for a diagnostic procedure (see appendix 6)
The Associate Services Director reviews the summary PTL and signs off with the Patient Access Team Manager. Note: The Directorate Management Teams will be required to meet with the Deputy Chief Operating Officer to agree actions to address variances where plans do not exist. If a patient will not be seen in 18 weeks, and it is not a legitimate wait, then an 18 Week Breach Exception Report (Appendix 7) should be submitted to the Deputy Chief Operating Officer. Legitimate Waits (See Appendix 8 for details of Legitimate Waits and Unnecessary Waits):
Patient chose to wait longer than 18 weeks for their first definitive treatment.
Patient non-cooperation (DNA‟s). The provider must ascertain communications with the patient were effective and received in good time.
Not in the patient‟s best clinical interest (waiting longer than 18 weeks is clinically appropriate).
The Medical Secretaries ensure all out-patient appointments are outcomed and waiting list entries actioned.
Weekly open referral report for patients who are not on the waiting

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 61
list to be reviewed and updated accordingly.
The Chief Operating Officer, Director of Performance and Associate Director of IM&T sign off the Trust level 18 week PTL.
Monthly Outpatients: Total number of referrals
Total number on waiting list OP stage of treatment Outpatient cancellations DNA‟s
Inpatients:
% patients clinically graded as urgent seen within appropriate time
Total number on waiting list IP stage of treatment % Planned Admissions without admit by date
Suspensions Short notice cancellations Cancelled by hospital
18 weeks RTT
Incomplete pathways % against admitted targets % of non admitted
Stage of treatment or Care Quality Commission
EMT/Board reports received
% Admitted patients seen within 18 weeks at the end of the month and data completeness
% Non Admitted patients seen within 18 weeks at the end of the month and data completeness
Summary report of 18 week breaches
Number of out-patients that will breach waiting time standards by the end of the month
Number of in-patients that will breach waiting time standards by the end of the month
Number of patients waiting for a diagnostic that will breach waiting time standards by the end of the month.
Operations cancelled on the day by hospital and those not readmitted within 28 days
All cancers, % seen within:
One month urgent referral to treatment One month diagnosis to treatment Two weeks of initial referral
Choose and Book:
% services directly bookable % slot availability
Performance Directorate performance is actively managed by the Deputy Chief Operating Officer through monthly review with exceptions reported to EMT by the Chief Operating Officer

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 62
GOVERNANCE
Governance The Users of this policy need to provide assurance that it is being implemented according to the guidelines and definitions and that any proposed changes are agreed and risk assessed before being implemented.
Weekly/Monthly On a weekly basis data quality reporting against each standard will be produced by the Associate Director of Information and Technology. The Patient Access Team will investigate specific issues and support the Directorate Management Teams in addressing these.
Key trends or issues will be identified by the Patient Access Team, reported to the Deputy Chief Operating Officer and presented to the Clinical Access Group to develop corrective action plans. Significant variances will be reported through the Chief Operating Officer to the Executive Management Team. The Chief Operating Officer and the Director of Performance and Planning will formally receive the data quality reports at the point of monthly sign off of external returns and will not sign off any return until the associated data quality report is available.
Annually An annual audit plan will be submitted to the Audit Committee to be undertaken by both Internal Audits and locally through the Patient Access Team and Information and Technology. Specific areas for focus will be identified based on risk assessment of policy adherence and trends identified in data quality reports and presented at the Clinical Access meeting.
Changes to Policy Any changes to this policy should be agreed through the Clinical Access Group which will include representatives from Directorate Management Teams, the Patient Access Team, Nursing, IM&T and Clinical and which reports through the Chief Operating Officer to the Executive Management Team.
Data set change notices [DSCN’s]
Prior to processing any data set change notices within the Trust, these must be signed off and agreed through the Clinical Access Group which will include representatives from Directorate Management, Patient Access Team, Nursing, IM&T and Clinical and which reports through the Chief Operating Officer to the Executive Management Team.
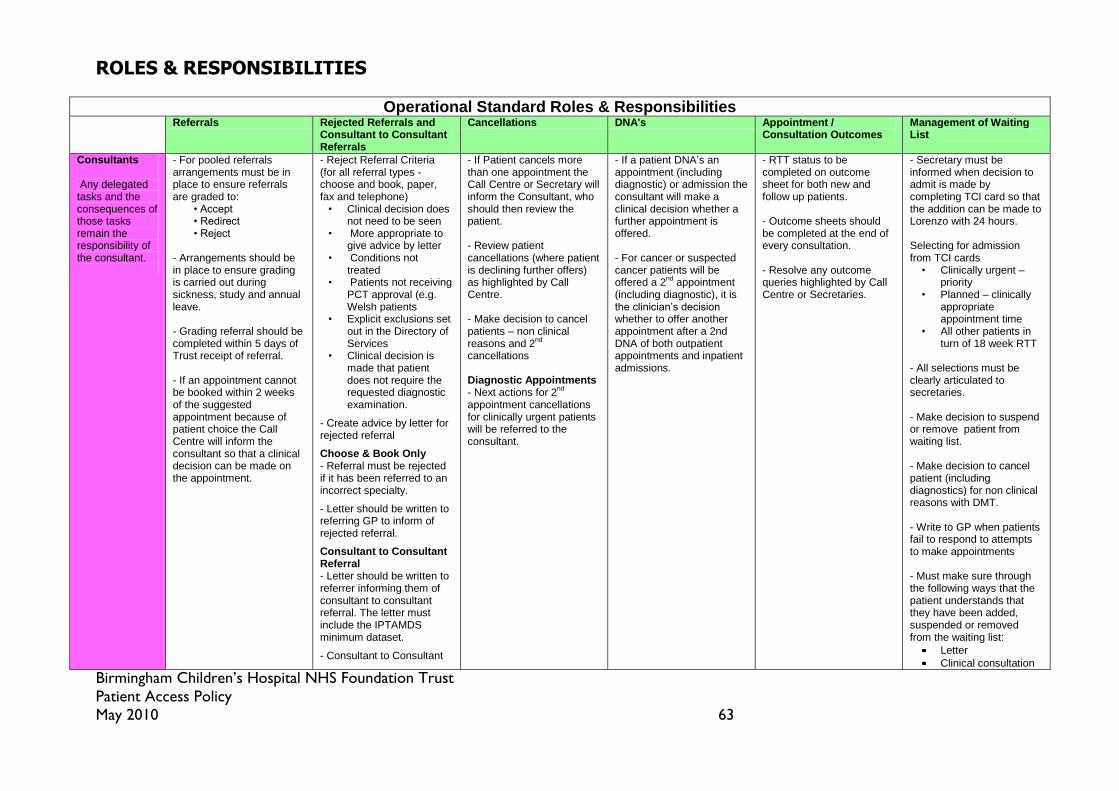
Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 63
ROLES & RESPONSIBILITIES
Operational Standard Roles & Responsibilities Referrals Rejected Referrals and
Consultant to Consultant Referrals
Cancellations DNA's Appointment / Consultation Outcomes
Management of Waiting List
Consultants Any delegated tasks and the consequences of those tasks remain the responsibility of the consultant.
- For pooled referrals arrangements must be in place to ensure referrals are graded to: • Accept • Redirect • Reject - Arrangements should be in place to ensure grading is carried out during sickness, study and annual leave. - Grading referral should be completed within 5 days of Trust receipt of referral. - If an appointment cannot be booked within 2 weeks of the suggested appointment because of patient choice the Call Centre will inform the consultant so that a clinical decision can be made on the appointment.
- Reject Referral Criteria (for all referral types - choose and book, paper, fax and telephone)
• Clinical decision does not need to be seen
• More appropriate to give advice by letter
• Conditions not treated
• Patients not receiving PCT approval (e.g. Welsh patients
• Explicit exclusions set out in the Directory of Services
• Clinical decision is made that patient does not require the requested diagnostic examination.
- Create advice by letter for rejected referral
Choose & Book Only - Referral must be rejected if it has been referred to an incorrect specialty.
- Letter should be written to referring GP to inform of rejected referral.
Consultant to Consultant Referral - Letter should be written to referrer informing them of consultant to consultant referral. The letter must include the IPTAMDS minimum dataset.
- Consultant to Consultant
- If Patient cancels more than one appointment the Call Centre or Secretary will inform the Consultant, who should then review the patient. - Review patient cancellations (where patient is declining further offers) as highlighted by Call Centre. - Make decision to cancel patients – non clinical reasons and 2
nd
cancellations Diagnostic Appointments - Next actions for 2
nd
appointment cancellations for clinically urgent patients will be referred to the consultant.
- If a patient DNA’s an appointment (including diagnostic) or admission the consultant will make a clinical decision whether a further appointment is offered. - For cancer or suspected cancer patients will be offered a 2
nd appointment
(including diagnostic), it is the clinician’s decision whether to offer another appointment after a 2nd DNA of both outpatient appointments and inpatient admissions.
- RTT status to be completed on outcome sheet for both new and follow up patients. - Outcome sheets should be completed at the end of every consultation. - Resolve any outcome queries highlighted by Call Centre or Secretaries.
- Secretary must be informed when decision to admit is made by completing TCI card so that the addition can be made to Lorenzo with 24 hours. Selecting for admission from TCI cards
• Clinically urgent – priority
• Planned – clinically appropriate appointment time
• All other patients in turn of 18 week RTT
- All selections must be clearly articulated to secretaries. - Make decision to suspend or remove patient from waiting list. - Make decision to cancel patient (including diagnostics) for non clinical reasons with DMT. - Write to GP when patients fail to respond to attempts to make appointments - Must make sure through the following ways that the patient understands that they have been added, suspended or removed from the waiting list:
Letter
Clinical consultation

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 64
Operational Standard Roles & Responsibilities Referrals Rejected Referrals and
Consultant to Consultant Referrals
Cancellations DNA's Appointment / Consultation Outcomes
Management of Waiting List
referrals should be given the same priority as GP referrals.
Diagnostic Referrals - When advised by the Radiology Receptionist that a referral has been rejected it is the responsibility of the referring clinician to inform the patient.
Telephone confirmation
Call Centre - Referral (including diagnostic referrals) will be added to Lorenzo within 1 working day of receipt by Trust, this includes recording the clock start for the RTT status, Registered GP, NHS number, Ethnic coding, overseas status, contact number and school.
- Agree all offers of appointments with patient.
- All appointment dates offered must be reasonable, this is two different dates at least 3 weeks in advance.
- Where patient cannot be reached to negotiate appointment (there should be at least 2 attempts on 2 different occasions to contact patient).an appointment should be allocated and a confirmation letter sent by post. For routine appointments the patient should be given the option to cancel and rebook For urgent appointments the patient should be asked to call and confirm that the
- Lorenzo must be updated when booking or changing a referral, including misdirected referrals being changed to the correct consultant and specialty. - Ensure IPTAMDS form is obtained for inter provider transfers. Choose & Book Only - Reject Referral if referral letter is not available within 7 days - A full explanation for rejection should be input onto C&B system. - Check for rejections - Print relevant rejection letters
- If Patient cancels more than one appointment the consultant should be informed to review the patient. - If a patient cancels and does not want to an appointment the referral should be returned to the consultant.
- Discuss not true DNA’s with DMT & reinstate if required. - Ensure clear verbal and written communication about appointment or admission that patients will be returned to the care of the GP if the patient DNA’s
- Collect clinic outcome forms - Input information from outcome sheets onto Lorenzo within one working day of appointment where there are no clinical queries. - Take outcome queries & inpatient instructions to secretaries

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 65
Operational Standard Roles & Responsibilities Referrals Rejected Referrals and
Consultant to Consultant Referrals
Cancellations DNA's Appointment / Consultation Outcomes
Management of Waiting List
appointment is acceptable.
- If through patient choice an appointment cannot be booked within 2 weeks of the suggested appointment time the consultant must be informed.
Choose & Book Only - Check system for incoming referrals
- Contact secretary with relevant referrals
- Check referral letter is attached to referral request (through work list)
Med Sec - All referrals should be sent to the Call Centre upon receipt to allow them to be added to Lorenzo within one working day of receipt by the Trust. - Agree all offers of appointments with patient. - All appointment dates offered must be reasonable, this is two different dates at least 3 weeks in advance.
- Rejected referral must go to Call Centre to alter Lorenzo if the patient is moved to a more appropriate Consultant. - All misdirected referrals should be returned to the Call Centre. Consultant to Consultant Referral - IPTAMDS minimum dataset should be included with referral letter.
- If Patient cancels more than one appointment the consultant should be informed to review the patient.
- Cancer DNA’s are offered a 2
nd appointment.
- Discuss not true DNA’s with DMT and reinstate if required. - Ensure clear verbal and written communication about appointment or admission that patients will be returned to the care of the GP if the patient DNA’s
- Resolve outcome queries highlighted by Call Centre within 24 hours. - Validate clinic lists to ensure all outcomes have been entered onto Lorenzo.
- Once decision has been made to admit patient it is added to Lorenzo waiting list within 24 hours. - TCI card with appointment time & date is sent to Central Admission Team when patient is selected for admission. - All diagnostic codes or part-diagnostic must be clearly identified on the inpatient or day case waiting list using clinical coding. - Inform CAT of suspension or removals (including diagnostics) by email, including patient demographic details, name of consultant, the date of planned admission and reason for removal. - Telephone call should be

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 66
Operational Standard Roles & Responsibilities Referrals Rejected Referrals and
Consultant to Consultant Referrals
Cancellations DNA's Appointment / Consultation Outcomes
Management of Waiting List
made informing patient when they are selected for admission. - When patients do not respond to telephone calls or letter demographics should be checked with GP or referrer. - When patient does not respond and demographics are correct the Central Admission Team should be instructed (by e-mail) to remove patient from waiting list. Instructions should include the reason for removal.
Central Admission Team
Diagnostic Appointments - After a 2
nd patient
cancellation for a routine appointment the patient will be removed from the waiting list and a letter will be sent to the requesting clinician advising of the outcome. A copy will also be filed in the case notes. - Next actions for 2
nd
appointment cancellations for clinically urgent patients will be referred to the consultant.
- TCI patient on Lorenzo and send a patient letter when patient is selected for admission. - Suspend or remove patient from waiting list on Lorenzo when instructed in writing by secretary, DMT or Radiology Receptionist.
Radiology Department / Radiology Receptionist
- Referral (including diagnostic referrals) will be added to Lorenzo within 1 working day of receipt by Trust, this includes recording the clock start for the RTT status, Registered
- Must advise the requesting clinician that referral has been rejected (including rejection by patient).
Diagnostic Appointments - After a 2
nd patient
cancellation for a routine appointment the patient will be removed from the waiting list and a letter will be sent to the requesting
- Inform CAT of suspension or removals from waiting list for diagnostics by email, including patient demographic details, name of consultant, the date of planned admission and

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 67
Operational Standard Roles & Responsibilities Referrals Rejected Referrals and
Consultant to Consultant Referrals
Cancellations DNA's Appointment / Consultation Outcomes
Management of Waiting List
GP, NHS number, Ethnic coding, overseas status, contact number and school.
clinician advising of the outcome. A copy will also be filed in the case notes. - Next actions for 2
nd
appointment cancellations for clinically urgent patients will be referred to the consultant.
reason for removal. - Suspend or remove patient from waiting list on RMS when instructed in writing.
Clinical Co-ordinator
- Patients cancelled for anything other than clinical reasons are escalated to DMT and Consultant - Potential cancellations for the 2
nd time must be
escalated to the DMT before cancellation.
Clinical Coding Department
- Aid specialties to maintain an appropriate set of codes to identify diagnostic procedures carried out.
Directorate Management Team
- Ensure that there is a process in place for all consultants and secretaries to continue grading referrals (paper and electronic) during sickness & annual leave. - Grading referral should be completed within 5 days of Trust receipt of referral. Choose & Book Only- Open new slots when contacted by Patient Access Team because of no capacity.
- Patients must be advised that referral (including diagnostic referrals) has been returned. The DMT is responsible for making sure this happens within their specialties.
For cancellations initiated by the hospital: Outpatients Ensure a new date is negotiated with patient Inpatients/Day Cases - If patient is already at the hospital the date should be negotiated before the patient goes home. - If patient is cancelled on the day of admission a new date must be negotiated by telephone. - Make decision to cancel patients – non clinical reasons and 2
nd
cancellations with Consultant
- Discuss not true DNA’s with Call Centre or Medical Secretary and advise whether patient should be reinstated.
- Ensure clinical specialties maintain an appropriate set of codes to identify diagnostic procedures carried out. - Inform CAT of suspension or removals by email, including patient demographic details, name of consultant, the date of planned admission and reason for removal. - Make decision to cancel patient (including diagnostics) for non clinical reasons with Consultant.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 68
Operational Standard Roles & Responsibilities Referrals Rejected Referrals and
Consultant to Consultant Referrals
Cancellations DNA's Appointment / Consultation Outcomes
Management of Waiting List
- Ensure patients cancelled by the hospital are seen within 28 calendar days (inpatients) of the original date or a date prior to the end of the 18-week pathway, whichever is the earliest.
Patient Access Manager
Choose & Book – Patient Referrals not Booked - Check patients not being booked due to capacity and contact Directorate to open new slots. - Contact patient within 48 hours of their attempt to convert their UBRN and negotiate appointment. - All appointment dates offered must be reasonable, this is 2 different dates at least 3 weeks in advance. - Escalate no capacity to DCOO.
Deputy Chief Operating Officer
- Discuss no capacity with DMT to resolve.
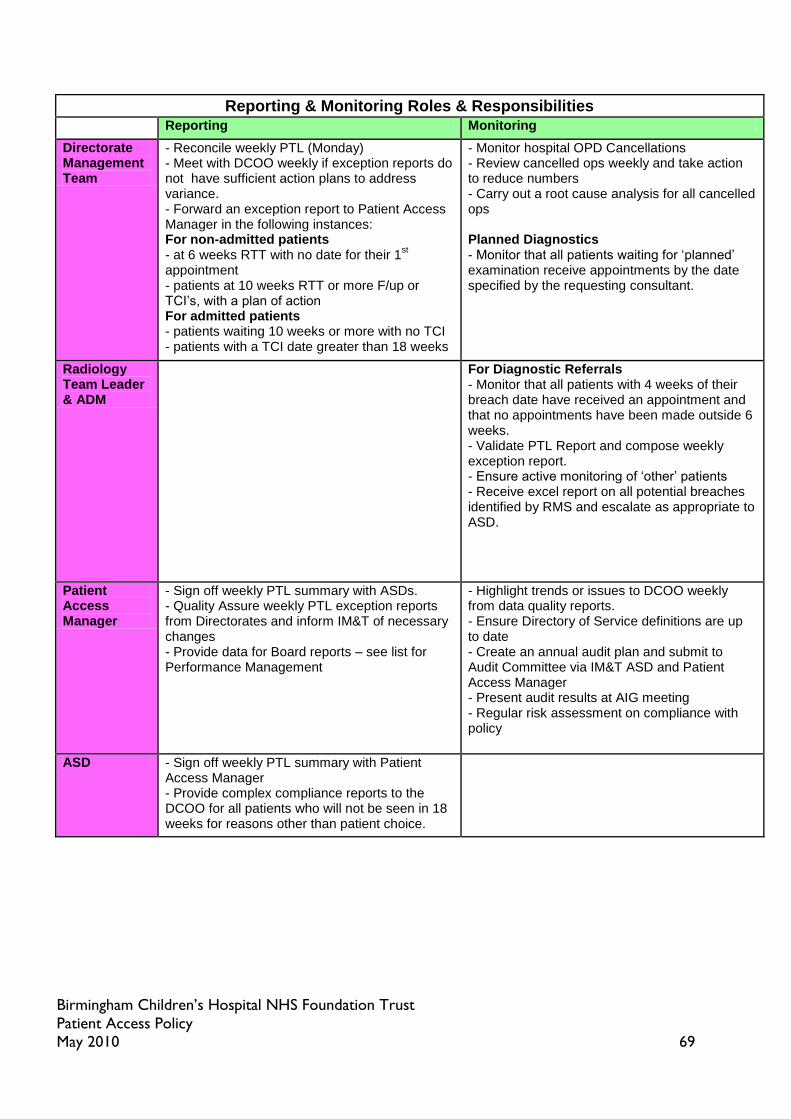
Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 69
Reporting & Monitoring Roles & Responsibilities Reporting Monitoring
Directorate Management Team
- Reconcile weekly PTL (Monday) - Meet with DCOO weekly if exception reports do not have sufficient action plans to address variance. - Forward an exception report to Patient Access Manager in the following instances: For non-admitted patients - at 6 weeks RTT with no date for their 1
st
appointment - patients at 10 weeks RTT or more F/up or TCI’s, with a plan of action For admitted patients - patients waiting 10 weeks or more with no TCI - patients with a TCI date greater than 18 weeks
- Monitor hospital OPD Cancellations - Review cancelled ops weekly and take action to reduce numbers - Carry out a root cause analysis for all cancelled ops Planned Diagnostics - Monitor that all patients waiting for ‘planned’ examination receive appointments by the date specified by the requesting consultant.
Radiology Team Leader & ADM
For Diagnostic Referrals - Monitor that all patients with 4 weeks of their breach date have received an appointment and that no appointments have been made outside 6 weeks. - Validate PTL Report and compose weekly exception report. - Ensure active monitoring of ‘other’ patients - Receive excel report on all potential breaches identified by RMS and escalate as appropriate to ASD.
Patient Access Manager
- Sign off weekly PTL summary with ASDs. - Quality Assure weekly PTL exception reports from Directorates and inform IM&T of necessary changes - Provide data for Board reports – see list for Performance Management
- Highlight trends or issues to DCOO weekly from data quality reports. - Ensure Directory of Service definitions are up to date - Create an annual audit plan and submit to Audit Committee via IM&T ASD and Patient Access Manager - Present audit results at AIG meeting - Regular risk assessment on compliance with policy
ASD - Sign off weekly PTL summary with Patient Access Manager - Provide complex compliance reports to the DCOO for all patients who will not be seen in 18 weeks for reasons other than patient choice.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 70
Reporting & Monitoring Roles & Responsibilities Reporting Monitoring
IM&T ASD - Provide weekly PTL report (Monday) via V drive. - Email availability of PTL to DMT's and Patient Access Team - Provide a summary PTL by Directorate following changes as Directed by Patient Access Manager. - Provide Data quality Reports weekly to Patient Access Team. - Sign off trust 18 week PTL weekly (Wednesday) - Provide data for Board reports – see list for Performance Management - Provide weekly report to DMT’s on cancellations
- Provide weekly report to DMT's on cancellations.
Performance Manager
- Prepare Board Report
Director of Performance
- Sign off Trust 18 week PTL weekly (Wednesday) - Agree Board report & provide to COO
- Monitor Directorate performance at weekly & monthly reviews
Deputy Chief Operating Officer
- Report variance to COO from weekly reports on data quality and monthly access improvement action plans - Meet with DMT weekly if exception reports do not have sufficient action plans. - Review complex compliance reports from ASD's - Sign off trust 18 week PTL weekly (Wednesday)
- Takes highlighted trends and issues to Access Improvement Group monthly to develop action plans - Monthly review of cancelled ops RCA’s - Monitor Directorate performance at weekly & monthly reviews
Chief Operating Officer
- Present compliance report on Access Targets to EMT - Receive Data Quality Variance report prior to external sign off of PTL - Reports variance & actions for data quality to EMT - Sign off trust 18 week PTL weekly (Wednesday)
Access Improvement Group / Clinical Access Group
- Receive audit results & develop action plans - Agree changes to policy - Agree data set change notices
Audit Committee
- Receive audit plan
EMT - Receive compliance reports for data quality and target compliance.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 71
EDUCATION, TRAINING & SUPPORT There will be staged training for this policy. The training will be separated into 6 sections.
Policy launch for all staff. Policy training for relevant core trainers and leads. Lorenzo and process training for all current users. Ongoing regular refresher training. Changes in process. Training of policy, Lorenzo and process for all new staff.
Policy launch: By External Team and Deputy Chief Operating Officer.
A week of events to raise the awareness of the policy and individual roles and responsibilities.
Policy training: By Patient Access Manager and External Team.
A two week period of policy training aimed at all core trainers in readiness for the cascade training.
Lorenzo and process training for all current users: By the Lorenzo Training Team.
A four week period to update all current users in the use of the waiting list and 18 week pathway on Lorenzo. This training should also include process and link into the patient access policy.
Ongoing and refresher training: By The Patient Access Manager.
Refresher training will be ongoing on an annual basis. Areas of staff requiring refresher training will be identified via the data quality reports reviewed by the Patient Access Team. Refresher training is to be completed on line through a question and answer assessment and scores for individual staff will be made available for their line managers /team leaders. The results are to be used to assess competence and individuals understanding of the policy and process. From this any further training requirements are to be identified and addressed.
Changes in process: By The Patient Access Manager.
Any changes in process will be made available to all current users via their line managers‟ team leaders and training will be through a cascade process. Followed by on line question and answer assessment.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 72
Training of policy, Lorenzo and process for all new staff: As part of Trust Induction
All new staff into the Trust must receive policy training as part of their Trust induction. Local induction policy training will be given by the core trainers. ( Line managers /team leaders) Lorenzo and process training must be given prior to the Lorenzo card being issued. The Lorenzo and process training has to be carried out by the experienced Lorenzo training team.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 73
ABOUT THIS APPOINTMENT:
NEW APPOINTMENTS FOLLOW UP APPOINTMENTS
Seen & Managed – Discharged
(30)
Seen & Managed family to call if
another appointment required
(suspended)
(30)
Seen & Managed needs a Future
Appointment
(30)
Start of active monitoring
initiated by clinician (suspended)
(32)
Discharge
(90)
Open Appointment family to
call if required (suspended)
(90)
Follow Up Appointment
(90)
Start of active monitoring
initiated by clinician (suspended)
(90)
Add to In Patient Waiting List
(20)
Add to Day Case Waiting List
(20)
Further Investigations / Test
required
(20)
Seen, needs to be referred to
another clinician for the same
condition
(21)
Seen in follow up clinic now
needs definitive treatment;
Add to In Patient Waiting List
(11)
Seen in follow up now needs
definitive treatment;
Add to Day Case Waiting List
(11)
Seen in follow up now needs to
be referred to another Clinician
(21)
ABOUT THE NEXT APPOINTMENT:
Which Clinic (Clinic ID):
In (number): _____________
Weeks Months
Years
Interpreter Required
Language: __________________
Follow up appointment made
Outcome set: further action required
Comments:
OUTPATIENT APPOINTMENT
OUTCOME FORM
Birmingham Children’s Hospital NHS Foundation Trust
Affix Patient Label here
18 week pathway
stopped
18 week pathway
complete
Continued 18 week
pathway
Start a New 18 week
pathway
APPENDIX 1: 18 WEEK RTT OUTCOME SHEET

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 74
APPENDIX 2: 18 WEEK RTT CODE OPTIONS
RTT Options - The first activity in a Referral to Treatment period where the first treatment that is intended to manage a patient's disease, condition or injury will stop the clock.
Clock Status RTT Code
Description
Clock Start 10 1st Activity after Referral in RTT
First activity in a RTT period
Clock Start
11 1st Activity after WW end
Active monitoring end - first activity at the start of a new RTT period following active monitoring
Clock Start
12 1st Activity after cons ref in RTT
First activity at the start of a new RTT period following a decision to refer directly to the Cons for a separate condition
SUBSEQUENT ACTIVITY DURING A REFERRAL TO TREATMENT PERIOD
During 20 Further Activity in RTT Subsequent activity during a RTT period - further activities anticipated
21 Tertiary referral
Transfer to another Health Care Provider - subsequent activity during a RTT period anticipated by another HCP
ACTIVITY THAT ENDS THE REFERRAL TO TREATMENT PERIOD – CLOCK STOPS
Clock Stop 30 Start 1st Treatment
First treatment - the start of the first treatment that is intended to manage a patient's disease, condition or injury in a RTT period
Clock Stop 31 Start WW by pt Start of active monitoring initiated by the patient
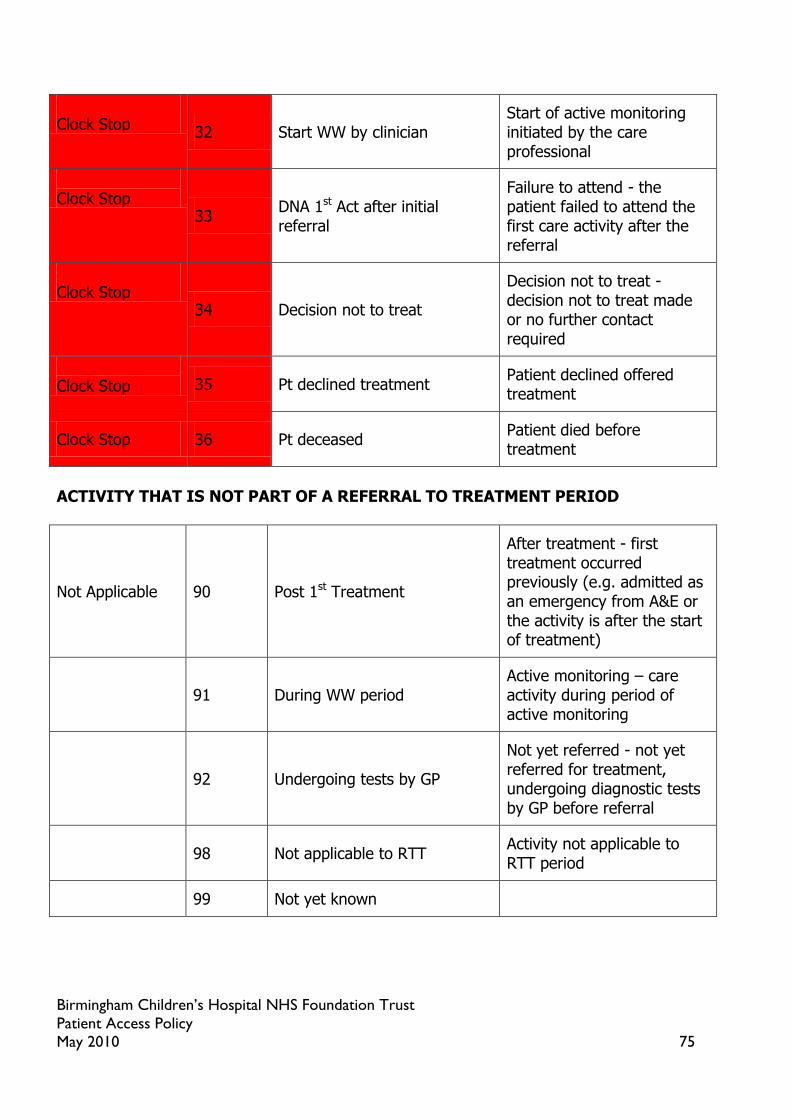
Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 75
Clock Stop
32 Start WW by clinician Start of active monitoring initiated by the care professional
Clock Stop
33 DNA 1st Act after initial referral
Failure to attend - the patient failed to attend the first care activity after the referral
Clock Stop
34 Decision not to treat
Decision not to treat - decision not to treat made or no further contact required
Clock Stop 35 Pt declined treatment
Patient declined offered treatment
Clock Stop 36 Pt deceased Patient died before treatment
ACTIVITY THAT IS NOT PART OF A REFERRAL TO TREATMENT PERIOD
Not Applicable 90 Post 1st Treatment
After treatment - first treatment occurred previously (e.g. admitted as an emergency from A&E or the activity is after the start of treatment)
91 During WW period Active monitoring – care activity during period of active monitoring
92 Undergoing tests by GP
Not yet referred - not yet referred for treatment, undergoing diagnostic tests by GP before referral
98 Not applicable to RTT Activity not applicable to RTT period
99 Not yet known

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 76
APPENDIX 3: IPTAMDS FORM - Inter Provider Transfer Administrative Minimum Dataset (IPTAMDS)
PrinterDateTime
Referring Organisation Name: Birmingham Children‟s Hospital
Referring Organisation Code: RQ3
Referring Clinician
Patient Family Name PatientSurname
Patient Forename PatientForename
Date of Birth PatientDateOfBirth
NHS Number PatientNHSNumber
Patient Unit ID PatientFACILNumber
Patient Address PatientAddressLine1 PatientAddressLine2 PatientAddressLine4
Patient Post Code PatientPostCode
Patient / Family contact details PatientTelNumber
GP Practice Details GPHealthOrgDesc GPAddressLine1 GPAddressLine2 GPPostCode
Patient Pathway ID RQ3 Section 1: Has the patient had treatment for the condition they are being referred on for? If yes proceed to section 3 If no proceed to section 2
Yes No
Section 2: If no, the patient is still on an active 18 week pathway so please enter the original referral date:
Section 3: Is the patient being referred on for a different condition?
Yes No If yes this starts a new 18 week pathway from the date this IPTAMDS is received
Referred to:
Consultant Specialty Hospital

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 77
APPENDIX 4
DATA ITEMS IN NATIONAL CANCER WAITING TIMES MONITORING DATASET: INCLUDES INDICATION OF WHETHER THESE ARE MANDATORY OR OPTIONAL The following table lists the 40 data items in the waiting times subset of the national cancer dataset and sets out whether their collection is mandatory or optional for different service providers. Data Item Health Care
Provider where patient is first seen following a referral request with priority type 3 'two week wait', or urgent referral from cancer screening service
Health Care Provider where patient receives first definitive treatment for cancer following a referral request with priority type 3 'two week wait', or urgent referral from cancer screening service
Health Care Provider where patient receives second or subsequent treatment for cancer following a referral request with priority type 3 'two week wait', or an urgent referral from cancer screening service
Health Care Provider where patient receives first definitive treatment for cancer following a consultant upgrade onto a 62 day patient pathway
Health Care Provider where patient receives second or subsequent treatment for cancer following a consultant upgrade onto a 62 day patient pathway
Health Care Provider where patient receives first definitive treatment for cancer following a referral request from another source of referral for out-patients or a different priority type
Health Care Provider where patient receives second or subsequent treatment for cancer following a referral request from another source of referral for out-patients or a different priority type
NHS Number M M M M M M M
Patient Pathway Identifier
M M* M* M* M* M* M*
Organisation Code (Patient Pathway Identifier Issuer)
M M* M* M* M* M* M*
Decision to Refer Date (Cancer or Breast Symptoms)
M* N/A N/A N/A N/A O N/A
Source of Referral for Out-Patients
M N/A N/A M N/A O N/A
Priority Type M N/A N/A M N/A O N/A
Cancer Referral to Treatment Period Start Date
M M M O N/A O N/A
Cancer Referral to Treatment Period Start Date
M M M O N/A O N/A
Two Week Wait Cancer or Symptomatic Breast Referral Type
M N/A M N/A N/A O N/A
Consultant Upgrade Date
N/A N/A N/A M N/A O N/A

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 78
Data Item Health Care Provider where patient is first seen following a referral request with priority type 3 'two week wait', or urgent referral from cancer screening service
Health Care Provider where patient receives first definitive treatment for cancer following a referral request with priority type 3 'two week wait', or urgent referral from cancer screening service
Health Care Provider where patient receives second or subsequent treatment for cancer following a referral request with priority type 3 'two week wait', or an urgent referral from cancer screening service
Health Care Provider where patient receives first definitive treatment for cancer following a consultant upgrade onto a 62 day patient pathway
Health Care Provider where patient receives second or subsequent treatment for cancer following a consultant upgrade onto a 62 day patient pathway
Health Care Provider where patient receives first definitive treatment for cancer following a referral request from another source of referral for out-patients or a different priority type
Health Care Provider where patient receives second or subsequent treatment for cancer following a referral request from another source of referral for out-patients or a different priority type
Organisation Code (Provider Consultant Upgrade)
N/A N/A N/A M N/A O N/A
Date First Seen
M N/A N/A M N/A O N/A
Organisation Code (Provider First Seen)
M N/A N/A N/A N/A N/A N/A
Waiting Time Adjustment (First Seen)
M* N/A N/A N/A N/A N/A N/A
Waiting Time Adjustment Reason (First Seen)
M*
Delay Reason Comment (First Seen)
M* N/A N/A M* N/A N/A N/A
Delay Reason Referral to First Seen (Cancer or Breast Symptoms)
M* N/A N/A N/A N/A N/A N/A
Multidisciplinary Team Discussion Indicator
M* M* M* M* M* M* M*
Multidisciplinary Team Discussion Date (Cancer)
M* M* M* M* M* M* M*
Multidisciplinary Team Discussion Indicator
M* M* M* M* M* M* M*
Multidisciplinary Team Discussion Date (Cancer)
M* M* M* M* M* M* M*
Cancer or Symptomatic Breast Referral Patient Status
M M M M M M M

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 79
Data Item Health Care Provider where patient is first seen following a referral request with priority type 3 'two week wait', or urgent referral from cancer screening service
Health Care Provider where patient receives first definitive treatment for cancer following a referral request with priority type 3 'two week wait', or urgent referral from cancer screening service
Health Care Provider where patient receives second or subsequent treatment for cancer following a referral request with priority type 3 'two week wait', or an urgent referral from cancer screening service
Health Care Provider where patient receives first definitive treatment for cancer following a consultant upgrade onto a 62 day patient pathway
Health Care Provider where patient receives second or subsequent treatment for cancer following a consultant upgrade onto a 62 day patient pathway
Health Care Provider where patient receives first definitive treatment for cancer following a referral request from another source of referral for out-patients or a different priority type
Health Care Provider where patient receives second or subsequent treatment for cancer following a referral request from another source of referral for out-patients or a different priority type
Primary Diagnosis (ICD)
N/A M M M M M M
Tumour Laterality
N/A M M M M M M
Cancer Treatment Event Type
N/A M M M M M M
Metastatic Site N/A M* M* M* M* M* M*
Organisation Code (Provider Decision to Treat (Cancer))
M* M M M M M M
Cancer Treatment Period Start Date
N/A M M M M M M
Treatment Start Date (Cancer)
N/A M M M M M M
Cancer Treatment Modality
N/A M M M M M M
Cancer Care Setting (Treatment)
N/A M M M M M M
Clinical Trial Indicator
N/A M M M M M M
Organisation Code (Provider Treatment Start Date (Cancer))
N/A M M M M M M
Radiotherapy Priority
N/A M* M* M* M* M* M*
Radiotherapy Intent
N/A M* M* M* M* M* M*
Delay Reason Comment (Decision to Treatment)
N/A M* M* M* M* M* M*
Delay Reason (Decision to Treatment)
N/A M* M* M* M* M* M*
Waiting Time Adjustment
N/A M* M* M* M* M* M*

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 80
Data Item Health Care Provider where patient is first seen following a referral request with priority type 3 'two week wait', or urgent referral from cancer screening service
Health Care Provider where patient receives first definitive treatment for cancer following a referral request with priority type 3 'two week wait', or urgent referral from cancer screening service
Health Care Provider where patient receives second or subsequent treatment for cancer following a referral request with priority type 3 'two week wait', or an urgent referral from cancer screening service
Health Care Provider where patient receives first definitive treatment for cancer following a consultant upgrade onto a 62 day patient pathway
Health Care Provider where patient receives second or subsequent treatment for cancer following a consultant upgrade onto a 62 day patient pathway
Health Care Provider where patient receives first definitive treatment for cancer following a referral request from another source of referral for out-patients or a different priority type
Health Care Provider where patient receives second or subsequent treatment for cancer following a referral request from another source of referral for out-patients or a different priority type
(Treatment)
Waiting Time Adjustment Reason (Treatment)
N/A M* M* M* M* M* M*
Delay Reason Comment (Referral to Treatment)
N/A M* N/A M* N/A O* N/A
Delay Reason Referral to Treatment (Cancer)
N/A M* N/A M* N/A O* N/A
Delay Reason Comment (Consultant Upgrade)
N/A M* N/A M* N/A O* N/A
Delay Reason (Consultant Upgrade)
N/A M* N/A M* N/A O* N/A
Key: M = Mandatory - the Standard Contract Schedule 5 requires NHS provider organisations to submit this information on a monthly basis.
The Department of Health require the data to be submitted 25 working days after the end of each month or quarter. M* = Mandatory if applicable - the Standard Contract Schedule 5 requires NHS provider organisations to submit this information on a
monthly basis, where collection of the item was applicable to them. The Department of Health require the data to be submitted 25 working days after the end of each month or quarter.
O = Optional O* = Optional if applicable N/A = Not Applicable

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 81
APPENDIX 5 – MDT ALERT TO INCOMING PATIENTS
Select ONE of the following:
First treatment □ MDT ALERT TO INCOMING PATIENT
Subsequent treatment □
Recurrence □ To be sent to: Insert Trust
Was this a: Tertiary cancer alert fax no: Insert Fax Number
Consultant upgrade □ From: (person sending this fax)
Upgrade date / / Trust:
PPI Tel:
Patient Details
Forename Surname DOB / /
NHS Number Hospital Number (Referring Trust)
Address
Is the patient aware of the diagnosis? Yes/ No/ Not known
Patient tel. no.
Referral Details
GP 2 week referral (suspected cancer or breast symptoms)
Y / N Date of receipt of GP 2 week referral (suspected cancer or breast symptoms)
/ /
NEW! Screening referral Y / N NEW! 62 day screening pathway start date
/ /
GP name (Referring)
GP Phone
GP Practice name Trust First Seen
Date First Seen / / Date discussed at MDT meeting
/ /
Decision to Treat Date (date discussed and agreed with patient)
/ / Earliest Clinically Appropriate Date (ECAD)
/ /
Clinician (Referring) Speciality
Clinician Referred to at Insert Trust Speciality
Has a referral letter together with imaging/histology reports been sent to clinician at Insert Trust ? If No please arrange.
Yes / No
NEW! Please list all tests that are booked for this patient:
Type of test:
Date of test: / / / / / / / /
Referred for Treatment Yes / No Planned Treatment Type
Surgery/ Chemotherapy/ Radiotherapy/ Palliative Care/ Brachytherapy Referred for Diagnosis Yes / No
Diagnosis Confirmed Yes / No Tumour Type (diagnosis)
Date of clinical intervention which confirmed cancer (date of diagnosis)
/ /
Reasons for Delay in meeting target(s)
Pause(s)(no. of days)
Reasons for pause(s)
Target Treatment Date
This document is not intended to replace the clinical referral letter.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 82
Birmingham Children’s Hospital NHS Trust Primary Contact: James Borland Tertiary Referral Centre for: Lead Cancer Manager Lead Cancer Manager Oncology Fax: 0121 333 8241 Haematology Fax: 0121 333 9841 Tel: 0121 333 9999 Neuro-oncology Fax: 0121 333 8151 Email: [email protected]
Retinoblastoma Fax: 0121 333 9461
Dudley Group of Hospitals NHS Trust Primary Contact: Hannah Coyle Hannah Coyle Tertiary Referral Centre for:
Lead Cancer Manager Lead Cancer Manager Upper Gastrointestinal (Specialist Surgery)
Tel: 01384 456111 Email: [email protected] Fax: 01384 244082
Heart of England NHS Foundation Trust Primary Contact Gaynor Hill Tertiary Referral Centre for: Lead Cancer Manager Lung (Surgery) Haematology Upper Gastrointestinal (Specialist Surgery) Urology (Prostate & Bladder) Fax: 0121 424 1549 Tel: 0121 424 1164 Penile Fax: 0121 424 7814 Email: [email protected]
The Royal Orthopaedic Hospital NHS Trust Primary Contact: Lin Russell Tertiary Referral Centre for: Consultant Nurse Sarcoma / Bone cancer Tel: 0121 684 4057 Email: [email protected] Fax: 0121 685 4146
Royal Wolverhampton Hospitals NHS Trust Primary Contact: Kate Jenks Tertiary Referral Centre for: Lead Cancer Manager Lead Cancer Manager Lung
(Surgery) Urology (Specialist Surgery)
Radiotherapy Gynaecology (Specialist Surgery)
Tel: 01902 307 999 Email: [email protected] Fax: 01902 695 609
Sandwell and West Birmingham Hospitals NHS Trust Primary Contact: Jenny Donovan Tertiary Referral Centre for: Lead Cancer Manager Gynaecology (Specialist Surgery) – City
Hospital Tel: 0121 553 1831 Fax: 0121 5075343 Ophthalmology – City Hospital

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 83
Email: [email protected] Fax: 0121 5073322 (Sandwell Hospital) Fax: 0121 5074737 (City Hospital)
University Hospital Birmingham NHS Foundation Trust Primary Contact: Lynne Dodson Tertiary Referral Centre for:
Lead Cancer Manager Brain/CNS Urology (Prostate & Bladder) Hepatobiliary
Head & Neck Upper Gastrointestinal (Specialist Surgery)
Haematology Chemotherapy Skin (Lymphoma) Radiotherapy Testicular cancer Tel: 0121 627 1627 ext 52237 Email: [email protected] Fax: 0121 460 5820

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 84
Appendix 6: Diagnostics Performance Management Process
Performance Management
All patients referred for a diagnostic examination must be seen within 6 weeks (excluding pauses). In order to ensure adherence to this standard the waiting list must be monitored by Team Leader and Assistant Directorate Manager on a weekly basis using the following process:
Note the 4/5/6 week breach dates ensuring that all patients within 4 weeks of their breach date have received an appointment and that no appointments have been made outside of the 6 week breach date.
Use this information to validate the weekly PTL and compose the weekly exception report.
Ensure all patients recorded as „other‟ (i.e. under a suspension) are actively being monitored or have an end date for the suspension and a new appointment date.
[Radiology - Extract all patients waiting for a diagnostic examination (appointments and pending) from RMS into excel] All potential breaches must be escalated as follows:
Team Leader/Assistant Directorate Manager
Assistant Directorate Manager
Associate Service Director The Directorate Management Team are responsible for monitoring the list of patients waiting for a „planned‟ examination ensuring that they receive an appointment by the date specified by the requesting Consultant. [In Radiology the Administration Team Leader is responsible for the above and if there is no available capacity for the patient to be seen during normal working hours, the examination will be performed „on call‟].

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 85
Data Quality
A TCI patient on as “planned” without an
admit by date recorded on Lorenzo. A TCI patient on as “planned” without notes
recorded on RMS.
Patients with no admission type. Patients whose waiting list type has been
changed. % of patients by waiting list type by speciality
– reviewed monthly against agreed tolerance levels.
Patients whose waiting list specialty does not match the specialty of the linked referral.
Patients who are paused but the comments field is blank.

Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 86
APPENDIX 7: 18 WEEK BREACH REPORT TEMPLATE - a report must be completed for all unnecessary waits 18 Week Breach Exception Report –to be completed for every patient identified as an 18 week breach due to an unnecessary wait. The completed form should be returned to the Patient Access Team.
Directorate Speciality Patient Hospital Number Patient’s first name Patient’s surname Referral date Date of outpatient appointment Number of weeks since
referral
Date added to waiting list Reason for TCI
First definitive treatment date Weeks waited from referral to first definitive treatment date
Why did this patient breach and what escalation process took place to avoid the 18 week breach? This section must give a comprehensive account of all actions taken to avoid the 18 week breach.
Could this patient have been seen by an alternative provider (other than BCH)?
What plans have been put in place to avoid 18 week breaches in the future?
Was the Associate Service Director aware that this patient was going to breach the 18 week target?
Name of staff member completing this form
Date form completed ASD signature
The 18 week commitment is a universal pledge, as set out in the NHS Constitution and NHS Operating Framework. This commitment should be delivered for every patient, in every speciality unless the patient
chooses otherwise or it is not in their best clinical interest. All specialities need to understand and act
upon the reasons for any unnecessary waits.
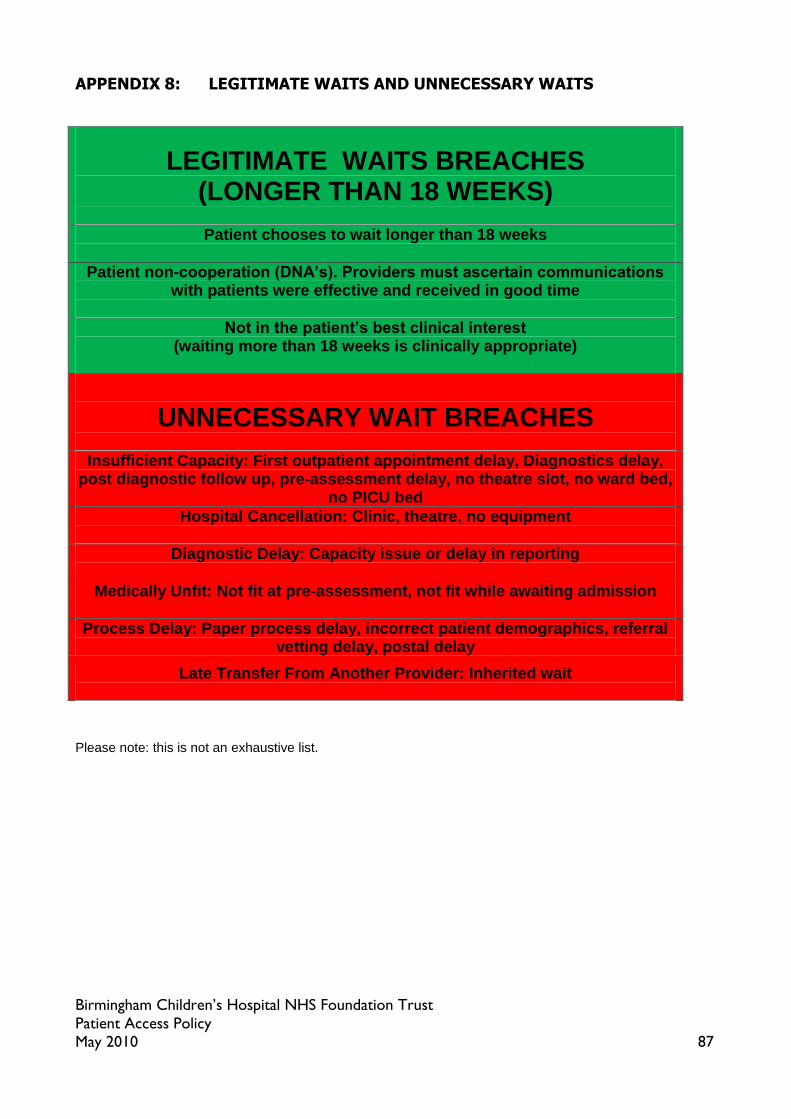
Birmingham Children’s Hospital NHS Foundation Trust
Patient Access Policy May 2010 87
APPENDIX 8: LEGITIMATE WAITS AND UNNECESSARY WAITS
Please note: this is not an exhaustive list.
LEGITIMATE WAITS BREACHES (LONGER THAN 18 WEEKS)
Patient chooses to wait longer than 18 weeks
Patient non-cooperation (DNA’s). Providers must ascertain communications with patients were effective and received in good time
Not in the patient’s best clinical interest (waiting more than 18 weeks is clinically appropriate)
UNNECESSARY WAIT BREACHES
Insufficient Capacity: First outpatient appointment delay, Diagnostics delay, post diagnostic follow up, pre-assessment delay, no theatre slot, no ward bed,
no PICU bed
Hospital Cancellation: Clinic, theatre, no equipment
Diagnostic Delay: Capacity issue or delay in reporting
Medically Unfit: Not fit at pre-assessment, not fit while awaiting admission
Process Delay: Paper process delay, incorrect patient demographics, referral vetting delay, postal delay
Late Transfer From Another Provider: Inherited wait