pancreatic tuberculosis: look at the kidney!
TRANSCRIPT
Y
I
P
VD
waaoctlmciswg
1
R
h1
ARTICLE IN PRESSG ModelDLD-2717; No. of Pages 1
Digestive and Liver Disease xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Digestive and Liver Disease
jou rna l h om epage: www.elsev ier .com/ locate /d ld
mage of the Month
ancreatic tuberculosis: Look at the kidney!
ishal Sharma, Puneet Chhabra, Surinder Singh Rana ∗, Deepak Kumar Bhasinepartment of Gastroenterology, Post Graduate Institute of Medical Education and Research (PGIMER), Sector 12, Chandigarh, India
Reference
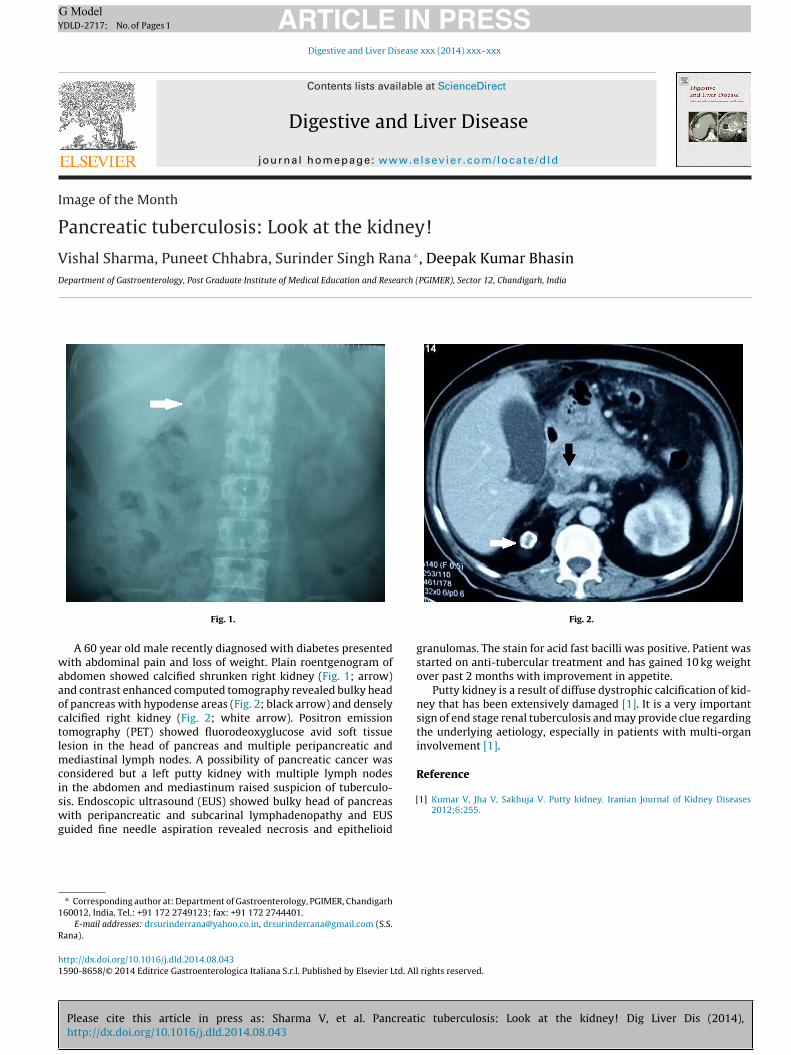
Fig. 1.
A 60 year old male recently diagnosed with diabetes presentedith abdominal pain and loss of weight. Plain roentgenogram of
bdomen showed calcified shrunken right kidney (Fig. 1; arrow)nd contrast enhanced computed tomography revealed bulky headf pancreas with hypodense areas (Fig. 2; black arrow) and denselyalcified right kidney (Fig. 2; white arrow). Positron emissionomography (PET) showed fluorodeoxyglucose avid soft tissueesion in the head of pancreas and multiple peripancreatic and
ediastinal lymph nodes. A possibility of pancreatic cancer wasonsidered but a left putty kidney with multiple lymph nodes
Please cite this article in press as: Sharma V, et al. Pancreathttp://dx.doi.org/10.1016/j.dld.2014.08.043
n the abdomen and mediastinum raised suspicion of tuberculo-is. Endoscopic ultrasound (EUS) showed bulky head of pancreasith peripancreatic and subcarinal lymphadenopathy and EUS
uided fine needle aspiration revealed necrosis and epithelioid
∗ Corresponding author at: Department of Gastroenterology, PGIMER, Chandigarh60012, India. Tel.: +91 172 2749123; fax: +91 172 2744401.
E-mail addresses: [email protected], [email protected] (S.S.ana).
[
ttp://dx.doi.org/10.1016/j.dld.2014.08.043590-8658/© 2014 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd. All
Fig. 2.
granulomas. The stain for acid fast bacilli was positive. Patient wasstarted on anti-tubercular treatment and has gained 10 kg weightover past 2 months with improvement in appetite.
Putty kidney is a result of diffuse dystrophic calcification of kid-ney that has been extensively damaged [1]. It is a very importantsign of end stage renal tuberculosis and may provide clue regardingthe underlying aetiology, especially in patients with multi-organinvolvement [1].
ic tuberculosis: Look at the kidney! Dig Liver Dis (2014),
1] Kumar V, Jha V, Sakhuja V. Putty kidney. Iranian Journal of Kidney Diseases2012;6:255.
rights reserved.