“palliative care” dr david plume mbbs drcog mrcgp macmillan gpf, gp advisor and primary care...
TRANSCRIPT

“Palliative Care”
Dr David Plume MBBS DRCOG MRCGPMacmillan GPF, GP Advisor and Primary
Care Network Lead.

“Palliative Care”
• “talk about medicine” or “talk about air”• Enormous subject!• Feedback regarding questionnaires and PPoC• Choice of Topic Areas:
– Symptom Control inc Breathlessness and Nausea/Vomiting, setting up a syringe driver.
– Current initiatives/developments inc improved drug charts for EOL, transferable DNACPR forms, end of treatment letters etc.
– Q and A

Local Feedback-Questionnaires• In late 2007 and again in late 2008 I sent out questionnaires
looking at twenty nine criteria for palliative care provision in 1’ care.
• These included;– Nominated lead?– Keeping a list?– Information getting to 1’ care rapidly enough?– Support for patients on the cancer journey– Frequency of palliative care meetings– Who goes?– H/O forms used and updated?– Are you recording PPoC, concerns etc and using LCP?– Do you have educational input from specialist team?

Local Feedback-Questionnaires• Regionally there had been significant improvements between 2007
and 2008.• Increased numbers with a nominated lead, cancer dx list, who were
getting better info from 2’ care, palliative care list. • Meetings were now monthly for majority with only small minority
having < or > frequency• Meetings continued to predominantly be GPs/DNs and SPCN but
17% of surgeries also have SW• Better recording of attendance/use of h/o forms/provision of
benefits advice.• Many more surgeries were making sure they were updating the h/o
forms and also patients concerns/expectations and needs.• 98% of surgeries use the LCP

Local Feedback-PPoC Pilot• Many thanks for your involvement.• Regionally 58% wanted to remain at home, 34%
wanted a nursing home/care home and the other 8% wanted to go to hospital.
• 83% of patient initiated on the document died in their PPoC
• Usual reason for not achieving this were care/carer issues or unexpected decline.
• Very +ve feedback• With PCT, with costings, for regional rollout.

Symptom Control
• Nausea and Vomiting.• Breathlessness.• Setting up a syringe driver.

Nausea and Vomiting

DEFINITIONS
• Nausea “an unpleasant feeling of the need to vomit, often accompanied by autonomic symptoms”
• Retching “rhythmic, laboured, spasmodic movements of the diaphragm and abdominal muscles”
• Vomiting “forceful expulsion of gastric contents through the mouth” – complex reflex process
Nausea is worse than vomiting.Occurs in 60% of people with advanced cancer.

ESTABLISHING the probable diagnosis in NAUSEA & VOMITING
• History
– Is there any relationship with food or pain – peptic ulcer?– Is it projectile or faeculant – high obstruction?– Did it start with certain medication (eg morphine, digoxin,
NSAIDS)?– Do certain events or situations trigger it? (eg hospital,
anxiety, chemotherapy)– ? Large volume vomit – gastric stasis– Distinguish between vomiting/expectoration/regurgitation– Psychological assessment

PATTERN• Nausea relieved by vomiting – gastric stasis / bowel
obstruction.
• Vomiting shortly after eating or drinking, with little nausea – oesophageal / mediastinal disease
• Sudden unpredictable vomit, possibly worse on waking – raised intracranial pressure
• Persistent nausea with little relief from vomiting – chemical / metabolic cause
EXAMINATION• Eyes - Possible jaundice
- Examine fundi for papilloedema
• Abdomen - Masses- Hepatomegaly- Distension / ascites- Presence or absence of bowel sounds
• PR - If constipation suspected
• Bloods - Renal & Liver function- Calcium- Specific drug levels if indicated

MANAGEMENT of NAUSEA and VOMITING
• Review of drug regime• Cough = Antitussive• Gastritis = Reduction of gastric acid =
? Stop gastric irritant drugs• Constipation = Laxative• Raised intracranial pressure = Corticosteroid• Hypercalcaemia = IV Saline / Bisphophonate (correction is
not always appropriate in a dying patient)• Ascites = ?Paracentesis
R. Twycross 1997

MANAGING NAUSEA & VOMITINGANTI-EMETICS
1. Dopamine receptor antagonists D2- Metoclopramide- Haloperidol
2. Histamine & muscarinic receptor antagonists H1- Cyclizine
3. Prokinetic- Metoclopramide- Domperidone (does not cross BBB)
4. 5HT3 antagonists 5HT3- Granisetron- Tropesitron- Ondansetron

MANAGING NAUSEA & VOMITINGANTI-EMETICS
5. Dexamethasone- ? Reduces permeability of BBB to emetogenic
substances6. Benzodiazepines
- Amnesic, anxiolytic & sedative7. Cannabinoids
- AIDS / chemotherapy- Brainstem cannabinoid receptor
8. Octreotide- Anti-secretory properties

DRUG ADMINISTRATION
• Oral route suitable for mild nausea.
• Syringe driver or rectal route for moderate to severe nausea and / or vomiting.
• Anti-emetics should be given regularly rather than PRN.
• Optimise dose of anti-emetic every 24 hours.
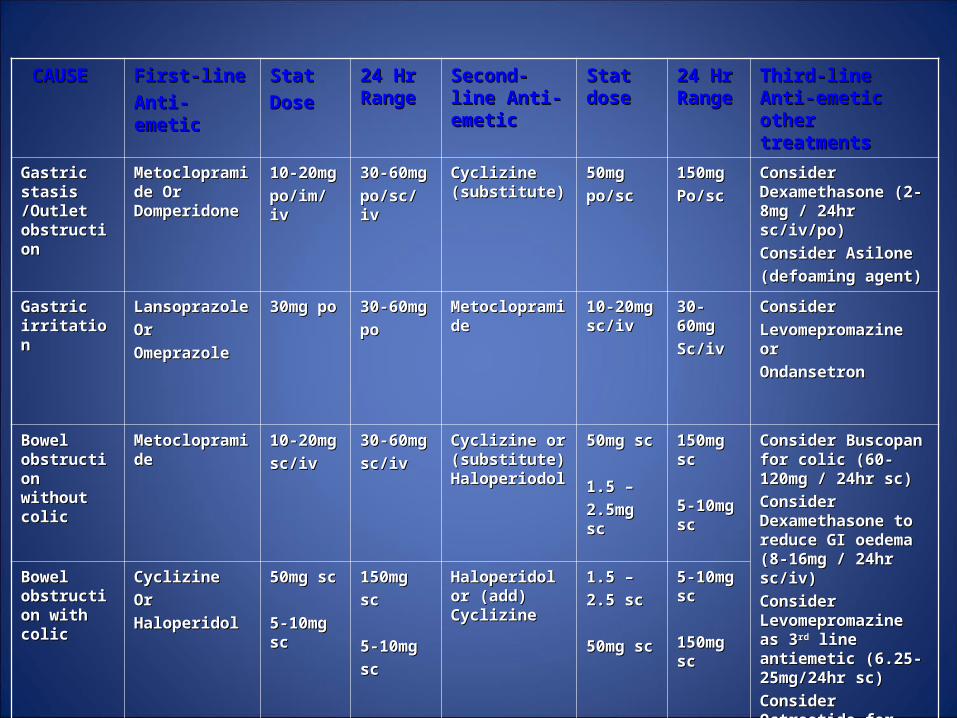
CAUSECAUSE First-line First-line
Anti-emeticAnti-emetic
StatStat
DoseDose
24 Hr 24 Hr RangeRange
Second-line Second-line Anti-emeticAnti-emetic
Stat Stat dosedose
24 Hr 24 Hr RangeRange
Third-line Anti-Third-line Anti-emetic other emetic other treatmentstreatments
Gastric stasis Gastric stasis /Outlet /Outlet obstruction obstruction
Metoclopramide Metoclopramide Or Domperidone Or Domperidone
10-20mg10-20mg
po/im/ivpo/im/iv
30-60mg30-60mg
po/sc/ivpo/sc/iv
Cyclizine Cyclizine (substitute)(substitute)
50mg50mg
po/scpo/sc
150mg150mg
Po/scPo/sc
Consider Consider Dexamethasone (2-8mg / Dexamethasone (2-8mg / 24hr sc/iv/po)24hr sc/iv/po)
Consider AsiloneConsider Asilone
(defoaming agent)(defoaming agent)
Gastric Gastric irritationirritation
LansoprazoleLansoprazole
Or Or
Omeprazole Omeprazole
30mg po30mg po 30-60mg30-60mg
popo
MetoclopramideMetoclopramide 10-20mg 10-20mg sc/ivsc/iv
30-60mg30-60mg
Sc/ivSc/iv
Consider Consider
Levomepromazine or Levomepromazine or
OndansetronOndansetron
Bowel Bowel obstruction obstruction without colicwithout colic
MetoclopramideMetoclopramide 10-20mg10-20mg
sc/ivsc/iv
30-60mg30-60mg
sc/ivsc/iv
Cyclizine or Cyclizine or (substitute) (substitute) HaloperiodolHaloperiodol
50mg sc50mg sc
1.5 – 1.5 –
2.5mg sc2.5mg sc
150mg sc150mg sc
5-10mg 5-10mg scsc
Consider Buscopan for Consider Buscopan for colic (60-120mg / 24hr colic (60-120mg / 24hr sc)sc)
Consider Consider Dexamethasone to Dexamethasone to reduce GI oedema (8-reduce GI oedema (8-16mg / 24hr sc/iv) 16mg / 24hr sc/iv)
Consider Consider Levomepromazine as 3Levomepromazine as 3rdrd line antiemetic (6.25-line antiemetic (6.25-25mg/24hr sc) 25mg/24hr sc)
Consider Octreotide for Consider Octreotide for large volume vomiting large volume vomiting (300-100mcg/24hr)(300-100mcg/24hr)
Bowel Bowel obstruction obstruction with colicwith colic
Cyclizine Cyclizine
OrOr
HaloperidolHaloperidol
50mg sc50mg sc
5-10mg sc5-10mg sc
150mg150mg
scsc
5-10mg5-10mg
scsc
Haloperidol or Haloperidol or (add) Cyclizine(add) Cyclizine
1.5 – 1.5 –
2.5 sc2.5 sc
50mg sc50mg sc
5-10mg 5-10mg scsc
150mg sc150mg sc

CAUSECAUSE First-line First-line
Anti-emeticAnti-emetic
StatStat
DoseDose
24 Hr 24 Hr RangeRange
Second-line Second-line Anti-emeticAnti-emetic
Stat Stat dosedose
24 Hr 24 Hr RangeRange
Third-line Anti-Third-line Anti-emetic other emetic other treatmentstreatments
Chemical / Chemical / Metabolic Metabolic Drugs eg Drugs eg Morphine, Morphine, Uraemia Uraemia Hypercal-Hypercal-caemia caemia
HaloperidolHaloperidol 1.5-2.5mg1.5-2.5mg
sc/posc/po
1.5-10mg1.5-10mg
po/scpo/sc
Cyclizine (add)Cyclizine (add) 50mg50mg
ScSc
150mg150mg
ScSc
Consider Consider Levomepromazine (6.25-Levomepromazine (6.25-25mg/24hr sc)25mg/24hr sc)
Ondansetron Ondansetron (8-16mg/24hr po/iv/sc) (8-16mg/24hr po/iv/sc) may help sickness due to may help sickness due to uraemiauraemia
Raised Raised intracranial intracranial pressurepressure
Cyclizine Cyclizine
and and
DexamethasoneDexamethasone
50mg sc50mg sc
8-16mg8-16mg
po/sc/ivpo/sc/iv
150mg150mg
ScSc
8-16mg 8-16mg po/sc/ivpo/sc/iv
Consider Consider Levomepromazine (6.25-Levomepromazine (6.25-25mg / 24hr sc)25mg / 24hr sc)
Motion Motion sicknesssickness
CyclizineCyclizine 50mg50mg
sc/posc/po
150mg150mg
sc/posc/po
Consider Consider Levomepromazine (6.25-Levomepromazine (6.25-25mg / 24hr sc)25mg / 24hr sc)
Consider Consider Prochlorperazine (25mg Prochlorperazine (25mg pr or 3.6mg buccal)pr or 3.6mg buccal)
Cause Cause unknownunknown
CyclizineCyclizine
And / orAnd / or
HaloperidolHaloperidol
50mg 50mg po/scpo/sc
1.5-2.5mg 1.5-2.5mg
150mg150mg
Po/scPo/sc
1.5-10mg1.5-10mg
Po/ScPo/Sc
Metoclopramide Metoclopramide (substitute)(substitute)
10 – 20mg10 – 20mg
Po/im/ivPo/im/iv
30-60mg 30-60mg po/sc/ivpo/sc/iv
Consider Consider Levomepromazine Levomepromazine (6.25–25mg / 245hr sc)(6.25–25mg / 245hr sc)
Consider Consider Prochlorperazine (25mg Prochlorperazine (25mg pr or 3-6mg buccal)pr or 3-6mg buccal)
Consider Consider Dexamethasone Dexamethasone 2-8mg/24hrs Consider 2-8mg/24hrs Consider BenzodiazepineBenzodiazepine

DRUG ADMINISTRATIONSummary of Guidelines
1. After clinical evaluation, document the most likely cause(s).2. Monitor the severity of nausea and vomiting.3. Treat reversible causes.4. Assess psychological aspects, eg anxiety.5. Prescribe first-line anti-emetic for most likely cause both
regularly and prn.6. Optimize does of anti-emetic every 24 hours.7. Reassess and change drugs by adding or substituting the
second-line anti-emetic.- If little benefit, reassess the cause and change to appropriate first-line anti-emetic.- ?converting to oral route after > 3 days.- Continue indefinitely unless the cause is self-limiting.

Breathlessness
Dyspnoea
• Unpleasant awareness of difficulty in breathing
• Pathological when ADLs affected and associated with disabling anxiety
• Resulting in :physiological
behavioural responses

Dyspnoea• Breathlessness experienced by 70% cancer patients
in last few weeks of life
• Severe breathlessness affects 25% cancer patients in last week of life

Causes of breathlessness-Cancer
– Pleural effusion– Large airway obstruction– Replacement of lung by cancer– Lymphangitis carcinomatosa– Tumour cell microemboli– Pericardial Effusion– Phrenic nerve palsy– SVC obstruction– Massive ascites– Abdominal distension– Cachexia-anorexia syndrome respiratory muscle weakness.– Chest infection

Causes of Breathlessness-Treatment
– Pneumonectomy– Radiation induced fibrosis– Chemotherapy induced
• Pneumonitis• Fibrositis• Cardiomyopathy
– Progestogens• Stimulates ventilation• Increased sensitivity to carbon dioxide.

Causes of Breathlessness- Debility
– Atelectasis– Anaemia– PE– Pneumonia– Empyema– Muscle weakness

Causes of Breathlessness-Concurrent
o COPDo Asthmao HFo Acidosiso Fevero Pneumothoraxo Panic disorder, anxiety, depression

Reversible causes of breathlessness!
• Resp. Infection• COPD/Asthma• Hypoxia• Obstructed Bronchus/SVC• Lymphangitis Carcinomatosa• Pleural Effusion• Ascites• Pericardial Effusion• Anaemia• Cardiac Failure• PE

Breathlessness Cycle
PANIC
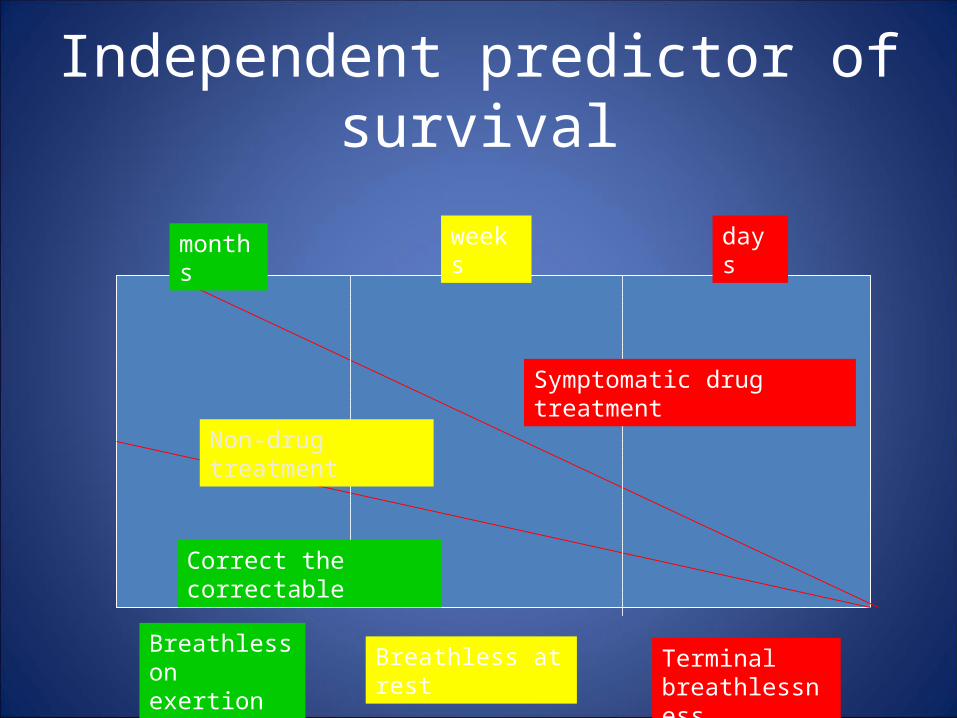
Independent predictor of survival
Breathless on exertion
Breathless at rest Terminal breathlessness
Correct the correctable
Non-drug treatment
Symptomatic drug treatment
months weeks days

Is this Terminal Breathlessness?
Are there appropriate treatments that couldor should be tried at home?
Does this patient want and need transfer for investigations and treatment?
Consider transfer to hospital for investigation & treatment if:
Pre-SOB condition good
Acute onset SOB
Patient receiving ongoing disease modifying treatment
Manage at home if:
Burden of transfer for investigation & treatment too great
Consider Oral antibioticsNebulisersSteroidsOxygen

Non-Drug Therapies
• Explore perception of patient and carers• Maximise the feeling of control over the
breathing• Maximise functional ability• Reduce feelings of personal and social
isolation.
Patient and Carer Perception
• Meaning to patient and carer• Explore anxiety esp. fear of sudden death• Inform that not life threatening• State what is likely to/not to happen• Realistic goal setting• Help patient and carer adjust to loss of
roles/abilities.

Maximize control
• Breathing control advice– Diaphragmatic breathing– Pursed lips breathing
• Relaxation techniques• Plan of action for acute episodes
– Written instructions step by step– Increased confidence coping
• Electric fan• Complementary therapies

Maximize function
• Encourage exertion to breathlessness to improve tolerance/desensitise to breathlessness
• Evaluation by physios/OT’s/SW to target support to need.
Reduce feelings of isolation
• Meet others in similar situation• Day centre• Respite admissions

Breathlessness Clinic
• Nurse lead• NNUH-Monday Afternoon• Lung cancer and Mesothelioma• Referral by GP/SPCN/Palliative Medicine
team/Generalist Consultants• PBL Day Unit-Wednesday, link with NNUH.
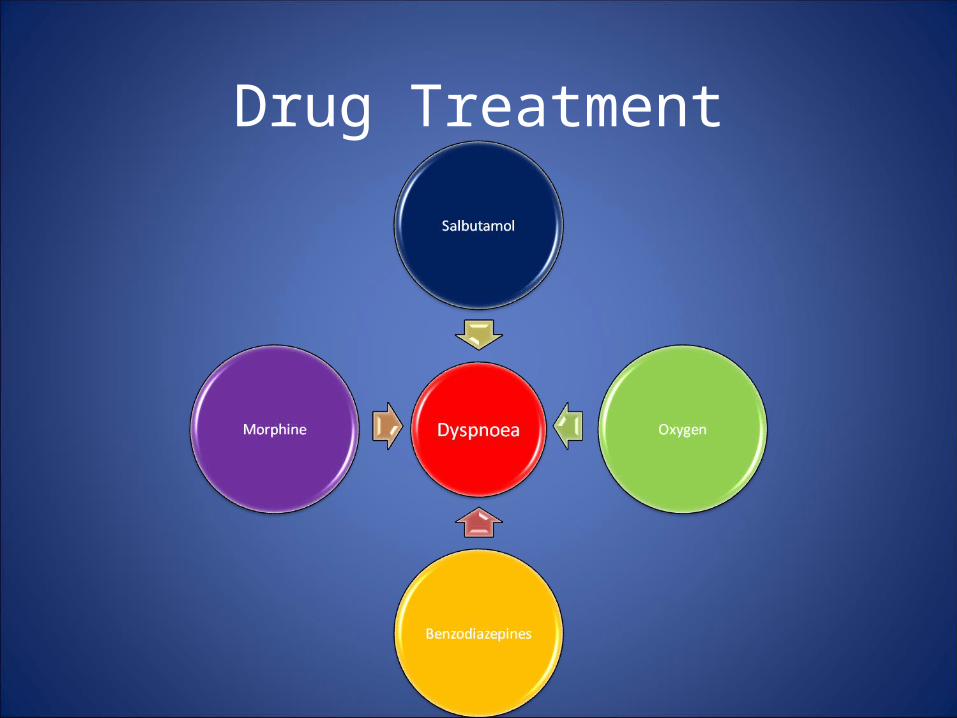
Drug Treatment

What do I give?• Bronchodilators work well in COPD and Asthma even if nil known sensitivity.
• O2 increases alveolar oxygen tension and decreases the work of breathing to maintain an arterial tension.
– Usual rules regarding COPD/Hypercapnic Resp. failure apply.
• Opioids reduce the vent.response to inc. CO2, dec O2 and exercise hence dec resp effort and breathlessness.
– If morphine naïve-Start with stat dose of Oramorph 2.5-5mg or Diamorphine 2.5-5mg sc and titrate Repeated 4hrly as needed.
– If on morphine already for pain a dose 100% or > of q4h dose may be needed, if less severe 25% q4h may be given
• Benzodiazipines stat dose of Lorazepam 0.5mg SL, Diazepam 2-5mg or Midazolam 2.5-5mg scRepeated 4hrly as needed

Ongoing treatment
A syringe driver should be commenced if a 2nd stat dose is needed within 24hrs
• Diamorphine 10-20mg CSCI / 24hrs
• Midazolam 5-20mg CSCI / 24hrs
Remember to prescribe statsReview & adjust dose daily if needed

Terminal Breathlessness
• Great fear of patients and relatives• Treat appropriately- Opioid and sedative/anxiolytic-
Diamorphine and midazolam-PRN and CSCI• If agitation or confusion -haloperidol or Nozinan• Some patients may brighten.• Sedation not the aim but likely due to drugs and
disease.

Respiratory Secretions (death rattle)
• Rattling noise due to secretions in hypopharynx moving with breathing
• Usually occurs within days-hours of death• Occurs in ~40% cancer patients (highest risk if existing lung
pathology or brain metastases)
• Patient rarely distressed• Family commonly are distressed
• Treat early• Position patient semi-prone
• Suction rarely helpful

Respiratory Secretions• If secretions are present, two options.
• A) Hyoscine Butylbromide (Buscopan)– Stat-20mg 1hrly– CSCI-80-120mg/24 hrs
• B) Glycopyrronium– Stat-0.4mg 4hrly– CSCI-0.6-1.2mg /24 hrs
Remember Stats at appropriate doses Review & adjust dose daily


Current Initiatives• EOL Drug Charts
– At piloting stage– Aim to clarify and simplify prescribing at the EOL
• DNACPR– “Allow a natural and dignified death”– Development of transferable DNACPR form from 1’2’3’ and
visa versa– Piloting later in year
• EOT Letters– Much more info, especially on late effects, anticipated
problems, points of re-referral etc.– Meet next week with Tom Roques– Integrate with electronic records

Q and A
• I am not a palliative care physician and you have an excellent resource in Gail!
• Happy to answer questions.