bph / luts - prostate cancer uk · bph / luts dr jonny coxon ma md mrcs mrcgp drcog fecsm...
TRANSCRIPT

05/12/2016
1
LUTS 1
BPH / LUTS
Dr Jonny Coxon
MA MD MRCS MRCGP DRCOG FECSM
Beaconsfield Medical Practice, Brighton
&
Brighton & Sussex Universities NHS Trust
LUTS 2
“As man draws near the common goal
Can anything be sadder
Than he who, master of his soul
Is servant to his bladder‟
LUTS 3
Prevalence of BPH
LUTS 4
Prevalence
It is abnormal NOT to have benign growth of the prostate with
increasing age
LUTS 5
Prevalence
TZ
PZ
LUTS 6
Prevalence

05/12/2016
2
LUTS 7
Prevalence • 2007 study: enlarged prostate = 4th most
common diagnosis in men over 50.
• Approximately 1/3 of men over 50 have moderate to severe LUTS
• i.e. ~ 3 million men in UK
LUTS 8
• Huge issue = men reporting symptoms at all
• Some can be rather stoical: “just part of growing old”
Presentation: what do patients say?
LUTS 9
• “I’m worried about me prostrate”
• “While I’m here doc…”
Presentation: what do patients say?
Lack of
physical
intimacy
Anger or
conflict
Avoidance
or withdrawal
A feeling of
distance or
isolation
Lack of
communication
Re
po
rti
ng
sp
ec
ific
re
lati
on
sh
ip
co
nc
ern
s
Men with mild symptoms (n=216)
Men with moderate-to-severe symptoms (n=203)
Spouses of men with enlarged prostate (n=77)
Roehrborn CG et al. Prostate Cancer Prostatic Dis 2006;9:30–34.
Presentation
LUTS 11
• “I’m here because the wife sent me in.”
Presentation: what do patients say?
LUTS 13
• GPs worry about missing prostate cancer – only 11% confident distinguishing between BPH & PCa
• ~ ½ refer before maximising medical therapy
• GPs seek specialist advice in 1/3 men with LUTS
Presentation: what do we say?

05/12/2016
3
LUTS 14
• Urologists feel ~40% of BPH referrals could be managed in primary care
• ~ 2/3 of urologists agree that interpreting PSA is difficult for GPs
Presentation: what do we say?
LUTS 15
What are LUTS?
• What happened to “prostatism”?
• Or at least “BPH”?
LUTS 16
What are LUTS?
BPH
CNS Renal
Cardiac Pituitary
BPE BOO
LUTS 17
LUTS: Storage symptoms
• Urgency
+/- Urge Incontinence
• Frequency
• Nocturia
• (Nocturnal enuresis)
(OAB)
LUTS 19
LUTS: Voiding symptoms
• Hesitancy
• Straining
• Poor flow
• Intermittency
• Terminal dribble

05/12/2016
4
LUTS 20
LUTS: Post-micturition
1) Post micturition dribble
2) Incomplete emptying
LUTS 21
LUTS: Assessment
June 2015
LUTS 22
LUTS: Assessment
4 pages of interest:
• Initial assessment
• Referral
• Conservative management
• Drug treatment
LUTS 23
LUTS: Assessment Consider as minimum 2-part consultation:
• Part 1
– Initial Hx & Ex
– Provide info
– Tests & forms to fill in
• Part 2
– Review & discuss management
LUTS 24
LUTS Assessment: History • Storage symptoms
• Voiding symptoms
• How much bother from symptoms?
• What’s the patient’s worry?
LUTS 25
LUTS Assessment: History
• Other elements of PMH, e.g.
– Diabetes
– Heart failure
– Kidney failure
– Liver failure
– OSA
– Oedema, chronic venous stasis
– Neurological conditions
05/12/2016
5
LUTS 26
LUTS Assessment: History
• Medications, e.g.:
– Diuretics
– Ca channel blockers
– SSRIs
– Bronchodilators (anti-cholinergics)
– Antihistamines
LUTS 27
LUTS Assessment: History
• Medications, e.g.:
– Lithium
– Benzodiazepines
– NSAIDs
– Pioglitazone
– Gabapentin
– Pregabalin
LUTS 28
LUTS Assessment: Examination
• Abdomen
• External genitalia
• PR / DRE
LUTS 29
LUTS Assessment: Examination
PR / DRE:
• Is it smooth?
• Is it big?
LUTS 30
LUTS Assessment: Examination
LUTS 31
LUTS Assessment: Examination

05/12/2016
6
LUTS 32
LUTS Assessment: Investigations
• Urine dipstick test
• Bloods:
– “Offer a serum creatinine test only if you suspect renal impairment”
– PSA?
LUTS 34
LUTS Assessment: Investigations
• “Ask men with bothersome LUTS to complete a urinary frequency volume chart.”
• “Offer men considering treatment an assessment of baseline symptoms with a validated symptom score (e.g. IPSS).”
LUTS 35 LUTS 36
LUTS Assessment: Investigations
• What’s normal?
• Void: ~300-500ml
• Fluid in: ~1.5-2L / 24 hrs
• Urine out: ~1.5-2L / 24 hrs
– 30ml/kg / 24hrs
• Frequency: > 8 voids/ 24hrs
• Nocturia: as > 1 void at night
• (Nocturnal polyuria: >⅓ volume at night)
LUTS 37
LUTS Assessment: Investigations
• Small volume voids with variation in voided volume – characteristic of OAB
• Small volume voids without significant variation in voided volume:
LUTS 38

05/12/2016
7
LUTS 39 LUTS 40
• Ask re ED
• Measure BP
• Might add to bloods:
– Lipids
– Glucose
LUTS Assessment: Not NICE
LUTS & Erectile Dysfunction
Inc
ide
nc
e ,
%
2
12
2
25
5
45
17
53
7
33
6
43
12
53
19
64
16
41
20
50
31
52
44 45
0
10
20
30
40
50
60
70 No, I cannot get an erection
Net reduction in stiffness
Rosen et al. Eur Urol 2003;44(6):637-49.
LUTS Severity
Age 50 – 59 years
LUTS Severity
Age 60 – 69 years
LUTS Severity
Age 70 – 79 years
LUTS 42
• Interest in sex declines with worsening LUTS
• Many studies shown association of LUTS with ED
• Prostate disease 2nd only to DM as ED risk factor:
– more than PVD, hyperlipidaemia, HT, depression, IHD
LUTS & ED
LUTS 43
• Unclear how much association is physiological, or related to sleep disturbance/anxiety
LUTS & ED
LUTS 44
LUTS & Metabolic Syndrome
Gacci et al, Eur Urol 2011; 60: 809-825

05/12/2016
8
LUTS 45
Link with Metabolic Syndrome
N=409, men presenting with moderate/severe LUTS Lee et al BJUI 2012; 110:540-5
LUTS 46
Link with Metabolic Syndrome
N=409, men presenting with moderate/severe LUTS Lee et al BJUI 2012; 110:540-5
LUTS 47
LUTS & Metabolic Syndrome
Kellogg Parsons J et al Eur Urol 2011
LUTS 48
LUTS & Metabolic Syndrome
LUTS 49
LUTS & Metabolic Syndrome
• Primary Care = ideal setting for holistic management of male LUTS
• The prostate as the “gateway to men’s health”
LUTS 50
LUTS Management
Uncomplicated LUTS Complicated LUTS
• Gradual onset
• Impalpable bladder
• Normal external genitalia
• Benign feeling prostate
• Normal PSA
• No infection / haematuria
• Raised PSA / Abnormal DRE
• Pelvic / Urogenital pain
• Recurrent UTI / Dysuria
• Palpable bladder
• Incontinence
• Haematuria
• Severe symptoms
• Bladder stones!

05/12/2016
9
LUTS 51
LUTS Management • If LUTS not bothersome or complicated, reassure
Cancer worry:
• For most cases, NO strong link between onset of LUTS & onset of prostate cancer
LUTS 52
LUTS Management
• Think possible causes (PMH/Meds)
• Offer:
–advice on lifestyle interventions (e.g. fluid intake, caffeine, smoking, time of diuretics)
–information on the condition
LUTS 53 LUTS 54
LUTS Management - Conservative
• If you suspect OAB, offer:
– supervised bladder training
– if needed, containment products.
LUTS 55
LUTS Management - Conservative
• If you suspect OAB, offer:
– supervised bladder training
– if needed, containment products.
• Do not offer penile clamps
LUTS 56
LUTS Management - Conservative
• For men with post-micturition dribble, advise how to perform urethral milking:

05/12/2016
10
LUTS 57
LUTS Management – Drug Rx
• Offer only if bothersome LUTS, & conservative management unsuccessful or not appropriate.
• Do not offer homeopathy, phytotherapy or acupuncture.
LUTS 58
LUTS Management – Drug Rx
• Overactive bladder:
–Offer an anticholinergic
LUTS 59
LUTS Management – Drug Rx
• Overactive bladder:
–Mirabegron (Betmiga), 50mg od
–β3-adrenoceptor agonist
• NICE: only if anticholinergic is ineffective, contraindicated or not tolerated
LUTS 60
LUTS Management – Drug Rx 1. Moderate to severe LUTS (not OAB predominant):
–Offer an α-blocker
2. LUTS with PSA >1.4, prostate >30g:
- high risk of progression:
–Offer a 5-α reductase inhibitor (5-ARI)
If 1 and 2:
–Offer combination treatment
LUTS 61
• Progression =
– Worsening symptoms
– Acute retention
– BPH-related surgery
Risk factors:
– Age over 70
– Moderate to severe bothersome symptoms
– PSA > 1.4 ng/ml, Prostate volume >30ml
LUTS Management – Drug Rx
LUTS 62
Adapted from Marberger MJ et al Eur Urol 2000;38:563-568.
Risk of Acute Retention by Baseline PSA
% o
f m
en
wit
h A
UR
(2
ye
ars
)
Serum PSA level <1.4 ng/ml
(n=705)
Serum PSA level ≥1.4 ng/ml
(n=1394)
9-fold increase in risk (p<0.001)
0.4
3.9
5
4
3
2
1
0
(2 years)

05/12/2016
11
LUTS 63
LUTS Management: α-blockers
• Reduce tone of bladder neck / prostate
• Ideal first line in primary care for ‘mixed LUTS’
• Rapid onset 4-6 weeks
• No effect on PSA level or prostate size
LUTS 64
LUTS Management: α-blockers
• BUT: do not prevent progression
• S/E include: dizzy, faint, weak, bowel effects, headache, ejaculatory dysfunction …
LUTS 65
LUTS Management: 5-ARIs
• Inhibit conversion of T to DHT
• ↓prostate volume
• Most effective in larger prostates
LUTS 66
LUTS Management: 5-ARIs
• Beneficial effects start at 6-9 months, fully develop over years
• ↓symptoms & ↓rate of retention / surgery
• S/E include: fatigue, ED, ↓ libido, gynaecomastia
LUTS 67
LUTS Management: 5-ARIs & PSA
• Any confirmed increase from lowest PSA level may signal non-compliance to therapy, or prostate cancer (particularly high-grade)
– should be carefully evaluated
• Can still use PSA to help risk assessment of PCa, after a new baseline established
LUTS 68
LUTS Management: Combination

05/12/2016
12
LUTS 69
LUTS Management: Combination
• Studies show combination Rx:
–Most effective for controlling symptoms
–Most effective for reducing progression
• e.g. At 4 years, combination vs tamsulosin alone: ↓ risk of acute retention / surgery by 70%
• 7.7% actual risk reduction (NNT=13)
Roehrborn CG et al. J Urol 2008;179:616–21;
Siami P et al. Contemp Clin Trials 2007;28:770–9
McConnell JD et al. NEJM 2003;349:2387–98
LUTS 70
LUTS 71 LUTS 72
LUTS 73
LUTS Management – Drug Rx
2012:
Cialis (tadalafil) 5 mg od: Licensed for treating the “signs & symptoms of BPH”
SLS restrictions amended, so can prescribe for condition other than ED
LUTS 74
LUTS Management – Drug Rx
Tadalafil for LUTS:
• IPSS scores do improve
• NICE 2015: Do not offer solely for LUTS, unless part of a trial
05/12/2016
13
LUTS Management – Drug Rx
Add muscarinic receptor antagonist
+ continue with
Edu/Lifestyle
Edu/Lifestyle with or without
5-ARI ± α1-blocker/
PDE5-I
Male LUTS EAU Guidelines 2015
(without indications for surgery)
Watchful waiting
with or without
Edu/Lifestyle
Edu/Lifestyle with or without Anti cholinergic
Edu/Lifestyle with or without
Vasopressin Analogue
Bothersome symptoms?
Storage symptoms predominant?
Edu/Lifestyle with or without
α1-blocker/PDE5-I
- + Nocturnal polyuria
predominant?
Prostate volume >40 ml?
Long-term treatment?
Residual storage symptoms
-
-
-
-
+
+
+
+
Gratzke C et al. Eur Urol 2015;67:1099-1109
LUTS Management – Drug Rx
LUTS 78
LUTS Management – Drug Rx Back to NICE:
• Consider adding an anticholinergic if storage symptoms after α–blocker for LUTS
• LOW risk of retention
LUTS 79
LUTS Management – Drug Rx Back to NICE:
• Nocturnal polyuria (>1/3 urine at night):
– Consider late-afternoon loop diuretic
– Consider desmopressin, if other medical causes have been excluded
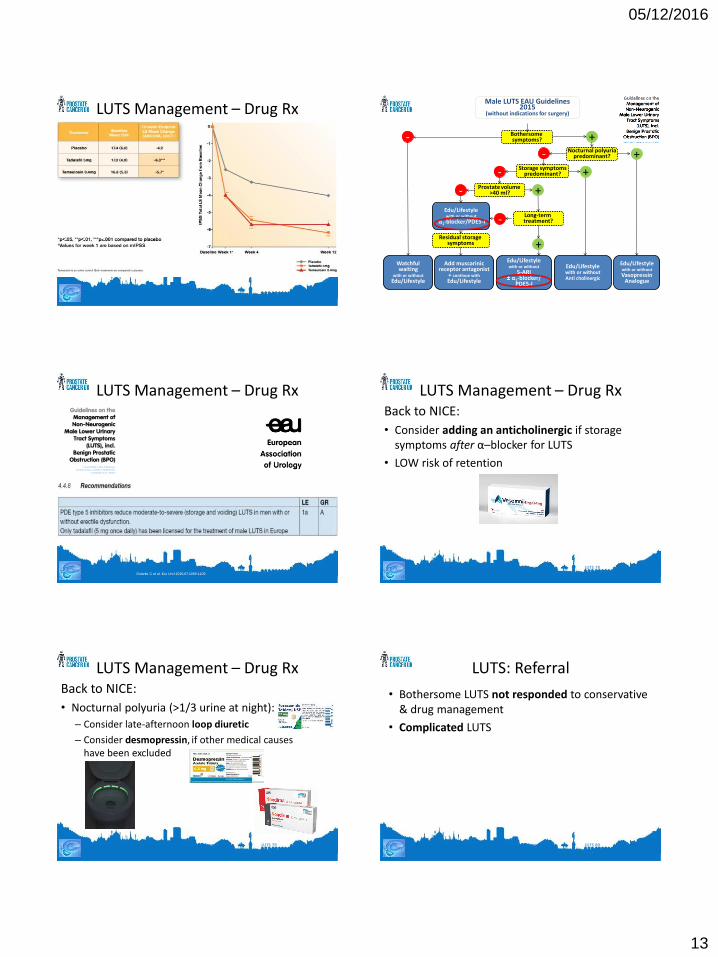
LUTS 80
LUTS: Referral
• Bothersome LUTS not responded to conservative & drug management
• Complicated LUTS

05/12/2016
14
LUTS 81
LUTS: Secondary Care
• Flow-rate
• Post-void residual
LUTS 82
LUTS: Secondary Care
• Flow-rate
• Post-void residual
• Possibly:
– Cystoscopy
– Upper tract imaging
LUTS 83
LUTS: Secondary Care
• Flow-rate
• Post-void residual
• Possibly:
– Cystoscopy
– Upper tract imaging
– Urodynamics (if considering surgery)
LUTS 84
LUTS: Surgery Voiding:
• TURP
• TUVP
• HoLEP (laser)
• TUIP / BNI (often smaller prostates, young men)
• Urethrotomy
LUTS 85
LUTS: Surgery Voiding:
• ‘Urolift’ for some
– Relieves LUTS while avoiding risk to sexual function
– Day case, with cost savings
LUTS 86
LUTS: Surgery
Storage:
• Botox injections
• Sacral / tibial nerve stimulation
• Cystoplasty

05/12/2016
15
LUTS 87
LUTS: SUMMARY
• Common, under-reported
• Ask: what is bothering the patient?
• Strong link with ED / Metabolic Syndrome
• Holistic assessment
• Think: balls
LUTS 88
LUTS: SUMMARY
• Lifestyle intervention especially fluid intake
• Medical therapy according to symptoms
• Find & treat nocturnal polyuria
• Remember: a progressive condition
• Refer if not responding / atypical / complicated