oxigenacion tisular
TRANSCRIPT

KATHERYNE CHAPARRO M.RESIDENTE ANESTESIOLOGÍA
Objetivo global de manejo del paciente crítico:
2.Mantener oxigenación tisular3.Sostener metabolismo
aeróbico4.Evitar disfunción de órganos

Inadecuada perfusión tisularCompromiso entrega de oxígenoMetas de reanimación
Measurement of acid–base resuscitation endpoints: lactate, base deficit, bicarbonate or what?. Curr Opin Crit Care 12:569–574. 2006
SOBRE REANIMACION
DEFICITREANIMACION

Revisión de fenómenos fisiopatológicos Identificación de métodos de mediciónDescripción de intervenciones médicas

1. Fenómenos fisiopatológicos

CONVECCION
DIFUSION
DIFUSION
CONVECCION
Diagnostic Measures o Evaluate Oxygenation in Critically Ill Adults. AACN Clinical Issues. 2004: Volume 15, Vumber 4, pp. 506–524

Estado de inadecuada oxigenación tisular, donde los niveles de O2 son tan bajos que no se
puede mantener la respiración mitocondrial
Assessment of tissue oxygenation in the critically-ill. European Journal of Anaesthesiology 2000, 17, 221±229

Assessment of tissue oxygenation in the critically-ill. European Journal of Anaesthesiology 2000, 17, 221±229
38 ATP

Measurement of acid–base resuscitation endpoints: lactate, base deficit, bicarbonate or what? Curr Opin Crit Care . 2006: 12:569–574.
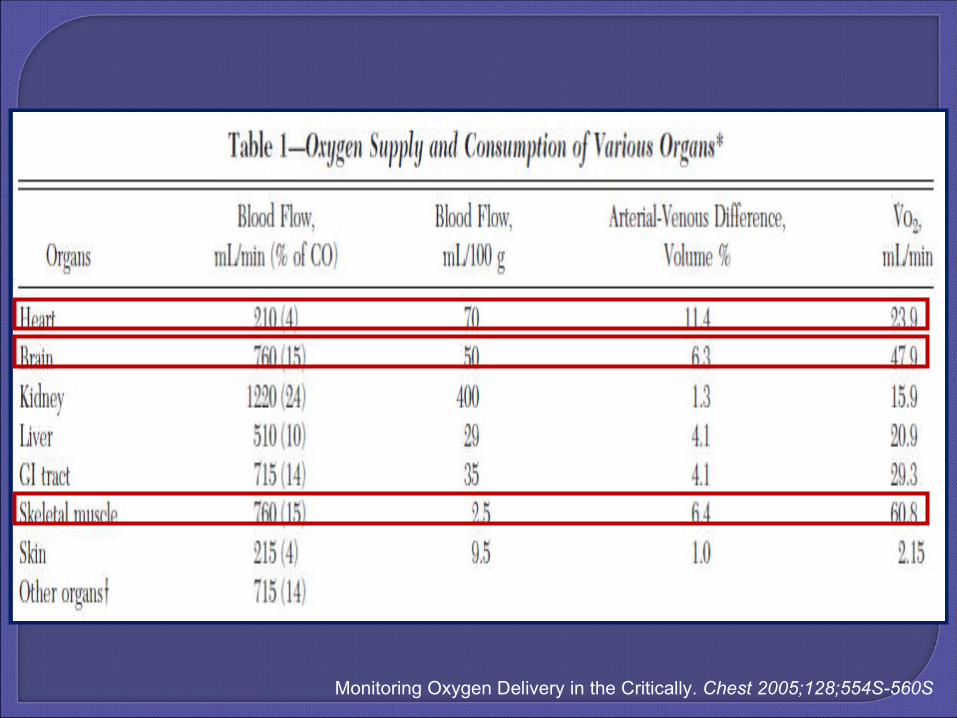
Monitoring Oxygen Delivery in the Critically. Chest 2005;128;554S-560S

DO2: Entrega de O2
DO2 = GC x CaO2CaO2 = 1,34 x Hb x SaO2 + 0.003 PaO2
• VO2: utilización de O2
VO2 = GC x (CaO2 – CvO2)CvO2 = 1,34 x Hb x SvO2 + 0.003 PvO2

CaO2 = 1,34 x Hb x SaO2 + 0.003 PaO2
GASTO CARDIACO
ANEMIA
DESATURACIÓN DE O2
Diagnostic Measures o Evaluate Oxygenation in Critically Ill Adults. AACN Clinical Issues. 2004: Volume 15, Vumber 4, pp. 506–524

Normal 1000 ml/min600 ml/min/m2
Sensibilidad variable de tejidos a DO2
Más sensibles, cardiomiocitos, neuronas, cel renales.
Tolerancia 15 a 20 min hipoxia riñón e hígado60 a 90 musculo esquelético
Musculo liso vascular 24 a 72 hPelo y uñas pueden seguir creciendo
Endpoints of Resuscitation What Should We Be Monitoring? AACN Advanced Critical Care 2006: Volume 17, Number 3, pp.306–316
The pulmonary physician in critical care c 2: Oxygen delivery and consumption in the critically ill Thorax 2002;57;170-177

Estado de concienciaLlenado capilar (sensibilidad 6%, especificidad
93%)Frialdad de pielFrecuencia cardiacaGasto urinario
Diagnostic Measures o Evaluate Oxygenation in Critically Ill Adults. AACN Clinical Issues. 2004: Volume 15, Vumber 4, pp. 506–524

VO2 normal 250 ml/min130 ml/min/m2No hay parámetros clínicos para su valoraciónMedición en relación al DO2
Endpoints of Resuscitation What Should We Be Monitoring? AACN Advanced Critical Care 2006: Volume 17, Number 3, pp.306–316
Diagnostic Measures o Evaluate Oxygenation in Critically Ill Adults. AACN Clinical Issues. 2004: Volume 15, Vumber 4, pp. 506–524

Calorimetría indirectaFormula inversa de FickSubestima el valorDiferencia con calorimetría 8 – 27%
Diagnostic Measures o Evaluate Oxygenation in Critically Ill Adults. AACN Clinical Issues. 2004: Volume 15, Vumber 4, pp. 506–524

TASA METABÓLICAActividad físicaEscalofrio, hipertermiaActividad simpática elevadaMedicamentos: adrenalinaRégimen alimentario rico en
glucosaDistres respiratorio
The pulmonary physician in critical care c 2: Oxygen delivery and consumption in the critically ill Thorax 2002;57;170-177


DO2 1000 ml/minVO2 250 ml/minExtracción 25%TEO2 crítico 60 – 70%
Tasa de extracción es la cantidad O2 consumido en relación a la fracción de O2 entregado
TASA DE EXTRACCIÓN = VO2 / DO2
Diagnostic Measures o Evaluate Oxygenation in Critically Ill Adults. AACN Clinical Issues. 2004: Volume 15, Vumber 4, pp. 506–524

180 a 330 mL/min
The pulmonary physician in critical care c 2: Oxygen delivery and consumption in the critically ill Thorax 2002;57;170-177
Matching total body oxygen consumption and delivery: a crucial objective? Intensive Care Med (2004) 30:2170–2179

VO2 = DO2 x EO2
VO2o/ VO2n = DO2o/DO2n x EO2o/EO2N
INDICES:VO2o/VO2n = Función global, < 1 disoxia, shock
DO2o/DO2n = función circulatoria, < 1 fallaEO2o/EO2N = función tisular, < 1 falla tisular
Oxygen uptake-to-delivery relationship: a way to assess adequate flow. Critical Care 2006, 10(Suppl 3):S4

Reposo EO2: 25%
Monitoring Oxygen Delivery in the Critically. Chest 2005;128;554S-560S
Bajo CvO2
Alta CvO2
Monitoring Oxygen Delivery in the Critically. Chest 2005;128;554S-560S

Matching total body oxygen consumption and delivery: a crucial objective? Intensive Care Med (2004) 30:2170–2179

Incremento de VO2, desacople o aumento de TM
Deterioro de la difusión de O2: alt microvascular o
edema tisular
Matching total body oxygen consumption and delivery: a crucial objective? Intensive Care Med (2004) 30:2170–2179

HIPOXIA
ANEMIA
ISQUEMIA
HIPOXIA HISTOTOXICA
HIPOXIA TISULAR
Tissue Hypoxia. How to detect, how to correct, how to prevent. Am J. Respir Crit Care Med. Vol 154. pp 1573-1578. 1996.
VO2 = CO x Hb x 1.39 x SaO2 x ERO2
Assessment of tissue oxygenation in the critically-ill. European Journal of Anaesthesiology 2000, 17, 221±229

Caída del DO2 primariamente por caída
del GC
Problema de distribución de DO2 entre y dentro de los
órganos
Defecto de uptake y consumo de O2
The pulmonary physician in critical care c 2: Oxygen delivery and consumption in the critically ill Thorax 2002;57;170-177

B. Vallet, E. Wiel, and G. Lebuffe. Resuscitation from circulatory shock: an approach based on oxygen –derived parameters. Yearbook of intensive Care and Emergency Medicine. 2005

Trastorno global de DO2
Trastornos de flujo regional entre y dentro de los órganos
Endotelio órgano activo
The pulmonary physician in critical care c 2: Oxygen delivery and consumption in the critically ill Thorax 2002;57;170-177

The pulmonary physician in critical care c 2: Oxygen delivery and consumption in the critically ill Thorax 2002;57;170-177

1. SIMPLES: monitoria clínica y lactato2. INTERMEDIOS: Variables relacionadas con
VO23. COMPLEJOS: valoración VO2 y relación
VO2/DO2
Matching total body oxygen consumption and delivery: a crucial objective?. Intensive Care Med (2004) 30:2170–2179


1. Restauración de una adecuada entrega de O2
2. Resolución de la deuda de oxígeno
3. Eliminación de los metabolitos anaeróbicos
Endpoints of Resuscitation What Should We Be Monitoring? AACN Advanced Critical Care 2006: Volume 17, Number 3, pp.306–316

Endpoints of Resuscitation What Should We Be Monitoring? AACN Advanced Critical Care 2006: Volume 17, Number 3, pp.306–316
1. Adecuado aporte de O2
2.Resolver la deuda de O2
3.Eliminar metabolismo anaerobio
1. Puede haber isquemia regional
2. Retraso3. No disponible para medición continua


Cantidad de base (mMol) requerida para titular 1 L de sangre arterial a un pH 7,4, con la muestra completamente saturada de O2, T 37 oC y pCO2 40 mmHg
BD = - (HCO3 – 24,8 + (16,2 x (pH - 7,4))
Normal -3 a 3>3 alcalosis < -3 acidosis
Diagnostic Measures o Evaluate Oxygenation in Critically Ill Adults. AACN Clinical Issues. 2004: Volume 15, Vumber 4, pp. 506–524

Sensible con grado y duración de DO2 inadecuado en pacientes con tx
Mortalidad alta > -15 en < 55 años
Leve -2 a -5 mMol Moderado -6 a -14 mMol
Severo > - 15 mMol
Diagnostic Measures o Evaluate Oxygenation in Critically Ill Adults. AACN Clinical Issues. 2004: Volume 15, Vumber 4, pp. 506–524
Measurement of acid–base resuscitation endpoints: lactate, base deficit, bicarbonate or what? Curr Opin Crit Care . 2006: 12:569–574.

Se puede alterar con hipocapnia, bicarbonato y hipotermia
Otras condiciones diferentes al VO2/DO2 lo pueden alterar: enf renal, ac. Hiperclorémica, intoxicaciones, cetoacidosis, enfisema
Endpoints of Resuscitation What Should We Be Monitoring? AACN Advanced Critical Care 2006: Volume 17, Number 3, pp.306–316
Déficit de base no asociado a aumento de Ac láctico no se relaciona con mortalidad
Measurement of acid–base resuscitation endpoints: lactate, base deficit, bicarbonate or what? Curr Opin Crit Care . 2006: 12:569–574.

Marcador de inadecuada oxigenación tisularNormal < 2 mMol/LDuración y magnitud de la elevación marcador
de mortalidadSen 87% y Esp 80% predictor de mortalidad
Endpoints of Resuscitation What Should We Be Monitoring? AACN Advanced Critical Care 2006: Volume 17, Number 3, pp.306–316Measurement of acid–base resuscitation endpoints: lactate, base deficit, bicarbonate or what? Curr Opin Crit Care . 2006: 12:569–574.
Don’t take vitals, take a lactate. Intensive Care Med (2007) 33:1863–1865Lactate as a marker of energy failure in critically ill patients: hypothesis. Critical Care December 2005 Vol 9 No 6

Componente del metabolismo normalNiveles = producción / depuración INFLUENCIA: glicolisis, metabolismo
proteico, disfunción hepáticaTemprana depuración en shock: buen
pronóstico


Monitoring oxygen transport and tissue oxygenation. Curr Opin Anaesthesiol 17:107–117. 2004

Cambio de relación por cambio en perfusión tisular
Menor SvO2 en V. cava sup
Menor SvO2 en V. cava inferior

Se mide por extracción de sangre del puerto distal del catéter SG o medición continua por fibroóptico
Mide SvO2: sangre cava sup, inf y seno coronario
Representa balance VO2/DO2
Normal 60 – 75%
Endpoints of Resuscitation What Should We Be Monitoring? AACN Advanced Critical Care 2006: Volume 17, Number 3, pp.306–316

SvO2 : VO2 aumentado o DO2 disminuido
Baja SvO2 siempre representa incompleta resucitación
Alta SvO2 no utilización de O2 o mal distribución sanguínea
Medición sin retraso
Endpoints of Resuscitation What Should We Be Monitoring? AACN Advanced Critical Care 2006: Volume 17, Number 3, pp.306–316
MAL PRONÓSTICO SvO2 BAJA:• Enfermedad cardiopulmonar• Choque séptico• Choque cardiogénico• Postoperatorio de cirugía cardiovascular
The value of venous oximetry. Curr Opin Crit Care. 2005 11:259—263.

SvO2: V. cava sup, inferior y seno coronario
SvcO2: V cava superiorMuestra tendencia de
SvO2Menor riesgo que SGCorrelación con SvO2 es
7 ± 4%
Mixed vs Central Venous Oxygen Saturation May Be Not Numerically Equal, But Both Are Still Clinically Useful. CHEST / 129 / 3 / MARCH, 2006

AnestesiaTrauma cráneo
encefálicoShock (5-18%)Shunt de
microcirculación
Mas que valores precisos de SvO2, cuales cambios de SvO2 reflejan alteración hemodinámica y como el
tratamiento se refleja en la SvcO2cThe value of venous oximetry. Curr Opin Crit Care. 2005 11:259—263.

Tonometría salinaAnalizador de gases
Tonometría aireinfrarojo
Gastric Tonometry The Hemodynamic Monitor of Choice (Pro). CHEST / 123 / 5 / MAY, 2003

Predictor de severidad y resultado de estados de Shock
Hipoperfusión gástrica H+, lactato, CO2
Diferencia CO2 gástrico y arterial < 10 mmHg
Gap amplio indica hipoperfusión esplácnica
Endpoints of Resuscitation What Should We Be Monitoring? AACN Advanced Critical Care 2006: Volume 17, Number 3, pp.306–316
Gastric Tonometry The Hemodynamic Monitor of Choice (Pro). CHEST / 123 / 5 / MAY, 2003

Monitoring oxygen transport and tissue oxygenation. Curr Opin Anaest. 2004: 17:107–117.

El PCO2 se aumenta con acides gástrica y reflujo duodenal
Se afecta por anti H2, sonda de alimentación, secreción gastrica endógena
Variabilidad de pCO2 entre individuos
Measurement of acid–base resuscitation endpoints: lactate, base deficit, bicarbonate or what? Curr Opin Crit Care . 2006: 12:569–574.
Valor diagnóstico de hipoperfusión, valor pronóstico. No cambio en el resultado de pacientes como herramienta
terapéutica
Gastric Tonometry The Hemodynamic Monitor of Choice (Pro). CHEST / 123 / 5 / MAY, 2003

Dispositivo sublingual Mide tensión de CO2 pCO2 >70 mmHg correlaciona
con hipoperfusión sublingual Correlación con tonometría
gástrica y marcadores séricos Requiere colaboración del
paciente Medición intermitente
Endpoints of Resuscitation What Should We Be Monitoring? AACN Advanced Critical Care 2006: Volume 17, Number 3, pp.306–316

Mide diferencia de absorción de cromóferos (Hb)
Monitoriza consumo de O2 mitocondrial via citocromo aa3
Falla en mostrar sobrevida
Saturación de O2 tisularUtilización de O2 celularFlujo sanguíneo tisular
Endpoints of Resuscitation What Should We Be Monitoring? AACN Advanced Critical Care 2006: Volume 17, Number 3, pp.306–316Measurement of acid–base resuscitation endpoints: lactate, base deficit, bicarbonate or what? Curr Opin Crit Care . 2006: 12:569–574.


762 pacientes Control IC: 2,5 a 3,5ml/min/1,73 m2 Supramáximo IC: > 4,5 ml/min/1,73 m2 SvO2 ≥ 70%



Efecto de la anemia: compensación mantener DO2
2.Aumento GC, menor viscosidad, aumento simpático
3.Poca interacción inflamatoria
Oxygen delivery. Crit Care Med 2003 Vol. 31, No. 12 (Suppl.)

838 pacientesRestrictivo < 7 gr/dl, Hb 7 – 9Liberal < 10 gr/dl, Hb 10 -12

Disminución de la mortalidadTerapia tempranaAntes de inicio de falla orgánica

Disminución de mortalidad 30 v.s 46.5%Menor disfunción multiorgánicaMayor logro de metas

No hay un marcador universalmente aplicable Ninguno ha mostrado independientemente
mejorar la sobrevidaCual end point es usado para guiar la
resucitación es menos importante que como se interpretan y como cambian la terapia

GRACIAS