outcomes in different residential settings for people … · heller (2002), and beadle-brown ......
TRANSCRIPT

Outcomes in Different Residential Settings for PeopleWith Intellectual Disability: A Systematic Review
Agnes Kozma, Jim Mansell, and Julie Beadle-BrownUniversity of Kent, Tizard Centre (Canterbury, Kent, United Kingdom)
AbstractLarge-scale reviews of research in deinstitutionalization and community living were lastconducted about 10 years ago. Here we surveyed research from 1997 to 2007. Articles wereincluded if the researchers based the study on original research, provided information onthe participants and methodology, compared residential arrangements for adults withintellectual disability, and were published in English-language peer-reviewed journals. Sixty-eight articles were found. In 7 of 10 domains, the majority of studies show that community-based services are superior to congregate arrangements. These studies provide moreevidence of the benefits of deinstitutionalization and community living and continue toindicate variability in results, suggesting that factors other than the basic model of care areimportant in determining outcomes.
DOI: 10.1352/1944-7558-114.3.193
The replacement of large residential institu-tions by local, smaller services supporting peoplewith intellectual disabilities in the community hasbeen one of the most important shifts in adult socialservices in some Western countries in the past 30years (Bigby & Fyffe, 2006; Mansell & Ericsson,1996). Most progress has been made in Scandinavia,North America, Australasia, and the United King-dom (Mansell, 2006). Elsewhere, deinstitutionaliza-tion has only just started or is not yet taking place.For example, in recent research investigatorsestimated that there are over one million peoplewith disabilities in institutions in the EuropeanUnion (Freyhoff, Parker, Coue, & Greig, 2004;Mansell, Beadle-Brown, & Clegg, 2004; Mansell,Knapp, Beadle-Brown, & Beecham, 2007).
The impact of different forms of residentialsupports on the quality of life of people withintellectual disabilities has attracted considerableattention. Emerson and Hatton (1994) reviewed71 articles published in 1980–1994 in the UnitedKingdom. Young, Sigafoos, Suttie, Ashman, andGrevell (1998) reviewed 13 Australian studies
published between 1980 and 1998. Kim (2001)reviewed the behavioral outcomes of deinstitu-tionalization for people with intellectual disabil-ities in studies published in the United Statesbetween 1980 and 1999. McConkey (2000),Heller (2002), and Beadle-Brown, Mansell, andKozma (2007) reviewed papers reporting on anyaspect of deinstitutionalization or communityservices for people with intellectual disabilitiesduring periods of one year. A number of reviewershave focused on specific aspects of deinstitution-alization, such as engagement in activity andresident–staff interactions (Felce, 1998), commu-nity integration (Myers, Agers, Kerr, & Myles,1998), and costs (Walsh, Kastner, & Green, 2003).These reviews suggest that the weight of researchfavored community-based services in most do-mains considered, although there were exceptions,and reviewers also frequently drew attention tothe variability of results found in service modelsof the same type.
In the present study we provide a compre-hensive review of more recent research on
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
E American Association on Intellectual and Developmental Disabilities 193

outcomes in residential settings for people withintellectual disabilities, including both deinstitu-tionalization and postdeinstitutionalization stud-ies. All research published in English fromdifferent countries since 1997 were considered.There are four main reasons why a new review ofthe literature is needed: (a) exploration of whethermore recent experiences in different countriescontinues to provide evidence on the benefits ofcommunity living for people with intellectualdisabilities; (b) deinstitutionalization, the expan-sion of community-based services, and thecontraction of institutions are still underway inmany countries, and research evidence remainsuseful to policymakers for deciding about theallocation of resources to different types of livingarrangements; (c) it is very likely that the lastdecade included the move of more people withmore severe disabilities to community servicesthan occurred in earlier stages of the process,making more recent studies of interest; (d) thesystem of community-based services in somecountries is now relatively well-established andnew forms of residential arrangements (e.g.,supported and independent living) are increasing-ly common, which challenge and provide alter-natives to more traditional models of communityliving. The outcomes of these arrangements arealso worth reviewing.
Method
Selection of StudiesWe used three methods to identify studies for
this review: (a) electronic search with a combina-tion of key terms (deinstitutionalisation/deinsti-tutionalization, learning/intellectual disabilities,mental retardation, living arrangements, commu-nity services, resettlement, transition to commu-nity care, relocation, hospital/institution closure,residential care institution) on academic searchengines (Web of Science, PsycINFO, and GoogleScholar); (b) search of selected journals (e.g.,Mental Retardation, American Journal on MentalRetardation, Journal of Applied Research in Intellec-tual Disabilities, Journal of Intellectual DisabilityResearch, British Journal of Learning Disabilities);and (c) follow-up of references in relevant papersand publications. We found 107 that werepotentially relevant and screened them morethoroughly using the following criteria: (a)published either in print or electronically between
1997 and 2007, (b) appeared in a peer-reviewedEnglish-language journal, (c) based on originalqualitative or quantitative research and containedinformation on the participants and methodolo-gy, and (d) compared two or more residentialarrangements for adults with an intellectual and/or developmental disability in terms of clearlydefined user outcomes.
For the final review, we selected 68 studiesthat met all the above criteria. These articles werealso checked with a recent unpublished review(Noonan Walsh et al., 2007). Investigators report-ing on the Hissom closure in Oklahoma (Conroy,Spreat, Yuskauskas, & Elks, 2003; Spreat &Conroy, 2002; Spreat, Conroy, & Fullerton,2005) that met all the inclusion criteria wereexcluded in the light of recent controversy (Walsh& Kastner, 2006).
Review ProcedureWe reviewed the 68 studies and coded them
according to country, research design, instru-ments, number of participants, settings, outcomedomains, and results. Studies mainly came fromEnglish-speaking countries, and only 9 articlesreported on experiences elsewhere (the Nether-lands, Finland, Taiwan, Norway). In the majorityof studies (49), researchers evaluated the impact ofdeinstitutionalization and compared institutionswith a variety of community-based settings. Inpostdeinstitutionalization studies (19) (Stancliffe,Emerson, & Lakin, 2004), researchers comparedoutcomes of different community-based residen-tial supports.
Definitions of institution and community-basedservices varied country by country. Commonfeatures of institutions typically included largesize, atypical architectural design, segregationfrom the local community, and highly regulatedrestrictive environments. Community-based set-tings included a variety of arrangements, such asdispersed or clustered, ordinary or purpose-builtgroup homes, and supported living. Researchersreported the size (range) of settings, but structuralor functional characteristics were rarely discussed(Stancliffe, Emerson, & Lakin, 2004).
Twenty-seven studies had a cross-sectionaldesign with matched samples and 23, a longitu-dinal design. In 18 studies investigators combinedboth and either compared ‘‘movers’’ and ‘‘stayers’’or people moving to different types of residentialarrangements.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
194 E American Association on Intellectual and Developmental Disabilities

Researchers used different methods to controlfor the impact of participant characteristics on theindividual outcomes of residential arrangements.In longitudinal studies investigators relied on pre–post designs with or without comparison groups.For cross-sectional studies they used matchedgroups or statistical procedures.
The majority of studies (42 of 68) had asample size of 100 or more participants; however,in 11 studies researchers used a small sample withless than 50 participants. These studies might lackstatistical power and, therefore, their resultsshould be viewed with caution. Investigators didnot commonly report sampling strategies. Con-venience samples were relatively widespread. In afew, more recent studies (e.g., Emerson, 2004b),researchers used representative sampling tech-niques (Noonan Walsh et al., 2007).
In most studies (66 of 68) investigators took aquantitative approach, using a variety of instru-ments. People with intellectual disabilities hadvirtually no input into the design of studies.Researchers in only two papers (Emerson, 2004b;Emerson & McVilly, 2004) from the same studyreported some participation of people withintellectual disabilities, although there are goodexamples in recent research (Miller, Cooper,Cook, & Petch, 2008).
The outcome domains reported by theseresearchers were coded into 10 categories: (a)community presence and participation, (b) socialnetworks and friendships, (c) family contact, (d)self-determination and choice, (e) quality of life,(f) adaptive behavior, and (g) user and familyviews and satisfaction. Authors of 29 studiesreported on more than one domain.
We briefly summarized the results of eachstudy; the overall direction of change and magni-tude of outcomes are indicated in the summarytables (e.g., better, more, declined). For quantita-tive studies we used statistical significance and forqualitative studies employed the strength ofopinion as an arbiter in reporting outcomes. Unlessotherwise stated results reported in the summarytables are significant; we noted nonsignificant orinconclusive results. We also highlighted internalvariations of outcomes and the factors associatedwith internal variation.
The results are presented below by domain. Ineach section we provide a brief summary of thegeneral results, highlight the factors associatedwith variation, and present a summary table of thestudies.
Results
Community Presence and ParticipationThe presence of people with intellectual
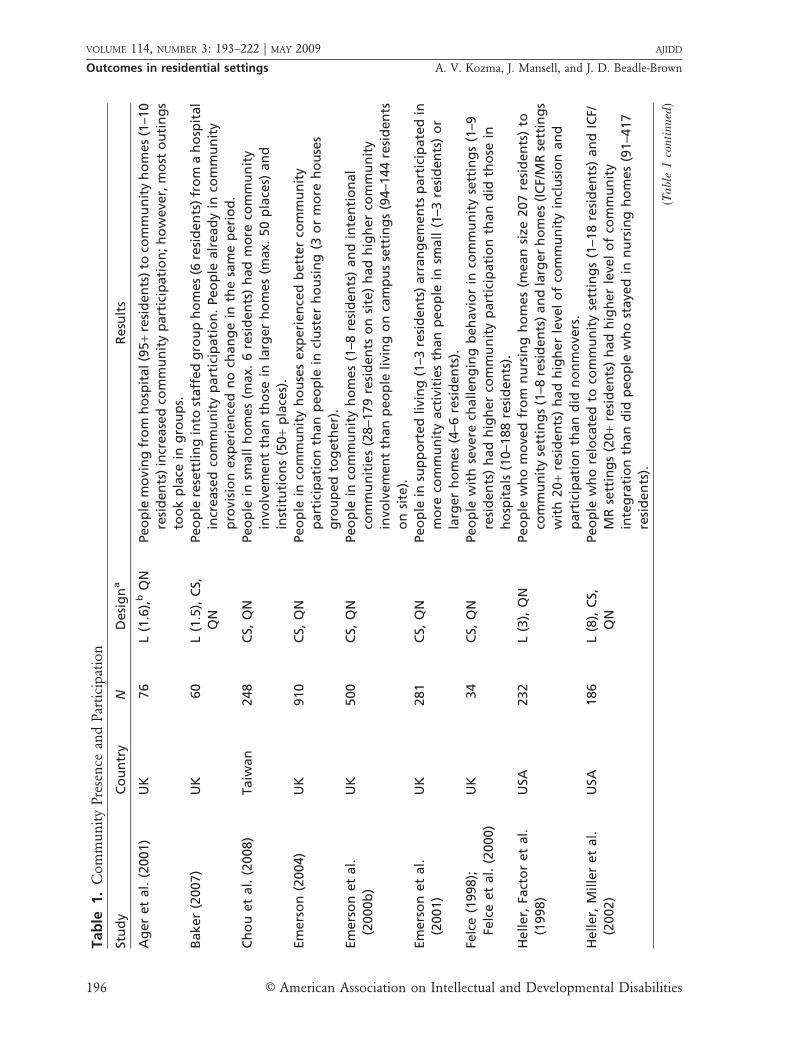
disabilities in the community, their participationin community-based activities, and use of com-munity facilities are often seen as one of the coreindicators of their social integration (Emerson &Hatton, 1994). Authors of 14 publications report-ed on some aspect of community integration,most often measured as the use of mainstreamcommunity facilities (e.g., services, leisure) andparticipation in activities outside the home(Table 1).
Small-scale community arrangements werefound to offer more community involvement tousers than were larger settings (Ager, Myers, Kerr,Myles, & Green, 2001; Chou, Lin, Pu, Lee, &Chang, 2008; Felce et al., 1998). Researchersfound that semi-independent or supported livingarrangements provided more community integra-tion than did traditional residential services(Emerson et al., 2001; Howe, Horner, & Newton,1998; Stancliffe & Keane, 2000). Community-based services did not, however, guarantee betteroutcomes. Community participation was alsofound to be associated with adaptive behavior(Baker, 2007), level and complexity of needs(McConkey, Walsh-Gallagher, & Sinclair, 2005),and the individual’s social competence. It wasassociated with service factors, including thequality of supports. Results also suggest that thecommunity presence and participation of peoplewith intellectual disabilities was very limitedacross all settings. People with more severedisabilities in particular are at risk of havinglimited community experiences (Baker, 2007).
Social Networks and FriendshipsMeaningful friendships and social relation-
ships are important determinants of emotionaland physical well-being (Emerson & McVilly,2004). In 9 studies investigators reported on someaspects of social networks and friendships (Ta-ble 2). Researchers typically focused on the sizeand density of networks and friendships, findingthat friendships and social networks of peoplewith intellectual disabilities were associated withliving arrangements as well as personal character-istics. In terms of number of friends, people insmall settings with low staff turnover had morefriends. Those in supported living arrangementshad more friends outside the home, were more
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
E American Association on Intellectual and Developmental Disabilities 195
Tab
le1.
Co
mm
un
ity
Pre
sen
cean
dPar
tici
pat
ion
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Ag
er
et
al.
(2001)
UK
76
L(1
.6),
bQ
NPeo
ple
mo
vin
gfr
om
ho
spit
al(9
5+
resi
den
ts)
toco
mm
un
ity
ho
mes
(1–1
0
resi
den
ts)
incr
ease
dco
mm
un
ity
part
icip
ati
on
;h
ow
eve
r,m
ost
ou
tin
gs
too
kp
lace
ing
rou
ps.
Baker
(2007)
UK
60
L(1
.5),
CS,
QN
Peo
ple
rese
ttlin
gin
tost
aff
ed
gro
up
ho
mes
(6re
sid
en
ts)
fro
ma
ho
spit
al
incr
ease
dco
mm
un
ity
part
icip
ati
on
.Peo
ple
alr
ead
yin
com
mu
nit
y
pro
visi
on
exp
eri
en
ced
no
chan
ge
inth
esa
me
peri
od
.
Ch
ou
et
al.
(2008)
Taiw
an
248
CS,
QN
Peo
ple
insm
all
ho
mes
(max.
6re
sid
en
ts)
had
mo
reco
mm
un
ity
invo
lvem
en
tth
an
tho
sein
larg
er
ho
mes
(max.
50
pla
ces)
an
d
inst
itu
tio
ns
(50
+p
lace
s).
Em
ers
on
(2004)
UK
910
CS,
QN
Peo
ple
inco
mm
un
ity
ho
use
sexp
eri
en
ced
bett
er
com
mu
nit
y
part
icip
ati
on
than
peo
ple
incl
ust
er
ho
usi
ng
(3o
rm
ore
ho
use
s
gro
up
ed
tog
eth
er)
.
Em
ers
on
et
al.
(2000b
)
UK
500
CS,
QN
Peo
ple
inco
mm
un
ity
ho
mes
(1–8
resi
den
ts)
an
din
ten
tio
nal
com
mu
nit
ies
(28–1
79
resi
den
tso
nsi
te)
had
hig
her
com
mu
nit
y
invo
lvem
en
tth
an
peo
ple
livi
ng
on
cam
pu
sse
ttin
gs
(94–1
44
resi
den
ts
on
site
).
Em
ers
on
et
al.
(2001)
UK
281
CS,
QN
Peo
ple
insu
pp
ort
ed
livi
ng
(1–3
resi
den
ts)
arr
an
gem
en
tsp
art
icip
ate
din
mo
reco
mm
un
ity
act
ivit
ies
than
peo
ple
insm
all
(1–3
resi
den
ts)
or
larg
er
ho
mes
(4–6
resi
den
ts).
Felc
e(1
998);
Felc
eet
al.
(2000)
UK
34
CS,
QN
Peo
ple
wit
hse
vere
challen
gin
gb
eh
avi
or
inco
mm
un
ity
sett
ing
s(1
–9
resi
den
ts)
had
hig
her
com
mu
nit
yp
art
icip
ati
on
than
did
tho
sein
ho
spit
als
(10–1
88
resi
den
ts).
Heller,
Fact
or
et
al.
(1998)
USA
232
L(3
),Q
NPeo
ple
wh
om
ove
dfr
om
nu
rsin
gh
om
es
(mean
size
207
resi
den
ts)
to
com
mu
nit
yse
ttin
gs
(1–8
resi
den
ts)
an
dla
rger
ho
mes
(IC
F/M
Rse
ttin
gs
wit
h20
+re
sid
en
ts)
had
hig
her
leve
lo
fco
mm
un
ity
incl
usi
on
an
d
part
icip
ati
on
than
did
no
nm
ove
rs.
Heller,
Mille
ret
al.
(2002)
USA
186
L(8
),C
S,
QN
Peo
ple
wh
ore
loca
ted
toco
mm
un
ity
sett
ing
s(1
–18
resi
den
ts)
an
dIC
F/
MR
sett
ing
s(2
0+
resi
den
ts)
had
hig
her
leve
lo
fco
mm
un
ity
inte
gra
tio
nth
an
did
peo
ple
wh
ost
aye
din
nu
rsin
gh
om
es
(91–4
17
resi
den
ts).
(Ta
ble
1co
nti
nu
ed)
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
196 E American Association on Intellectual and Developmental Disabilities

likely to be known by their neighbors, and havevisitors (Emerson & McVilly, 2004; Forrester-Jones et al., 2006; McConkey, 2007). Servicecharacteristics, such as the implementation ofactive support (Stancliffe, Jones, Mansell, & Lowe,2008), may moderate the effect of setting size andare associated with larger social networks (Robert-son, Emerson, Gregory et al., 2001). Friendshipand social network were also associated withindividual characteristics, such as adaptive skillsand (lack of) severe challenging behavior (Emer-son & McVilly, 2004).
Although more able people in dispersedsupported living were at relatively higher risk ofbeing isolated (McConkey, 2007), there was nostrong evidence of a relationship between loneli-ness and small setting size, including supportedliving. Loneliness was found to be associated withincompatibility between residents, which is morelikely to happen in larger settings, and feelingunsafe in the local community (Stancliffe et al.,2007). Friendship activities with other people whohave intellectual disabilities typically took place inthe public domain. These relationships werecharacterized by high stability and reciprocityand were highly valued by people themselves(Emerson & McVilly, 2004; Forrester-Jones et al.,2006; Robertson, Emerson, Gregory et al., 2001).
Family ContactFamily contact has been associated with social
and psychological well-being and social inclusionof people with intellectual disabilities (Robertson,Emerson, Gregory et al., 2001; Stancliffe & Lakin,2006). Investigators in 8 studies in the currentreview reported on some aspect of family contact,most often frequency and form (Table 3).
Resettlement in the community was shown tobe an opportunity to re-establish family contact,which tended to remain stable over time (Spreat,Conroy, & Rice, 1998; Stancliffe & Lakin, 2006).Very large size was associated with less familycontact (Chou et al., 2008); but, overall, form andfrequency of family contact were not related totype and size of living arrangement; rather theywere correlated to distance to the family homeand personal characteristics, such as ability andresident and parent age.
Self-Determination/ChoiceSelf-determination and choice are highly
valued in Western cultures and are importantTab
le1.
Co
nti
nu
ed
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Ho
we
et
al.
(1998)
USA
34
CS,
QN
Peo
ple
insu
pp
ort
ed
livi
ng
arr
an
gem
en
ts(1
–3re
sid
en
ts)
had
hig
her
com
mu
nit
yp
art
icip
ati
on
than
did
peo
ple
inla
rger
ho
mes
(2–2
0
resi
den
ts).
McC
on
key
(2007)
Irela
nd
,
UK
620
CS,
QN
Peo
ple
insm
all
ho
mes
(max.
6re
sid
en
ts),
an
dd
isp
ers
ed
an
dcl
ust
ere
d
sup
po
rted
livi
ng
use
dm
ore
com
mu
nit
yam
en
itie
sth
an
did
peo
ple
in
larg
eh
om
es
(avg
.20
resi
den
ts)
or
inca
mp
us
sett
ing
s(1
00
+re
sid
en
ts
on
site
).
Stan
clif
fe&
Kean
e
(2000)
Au
stra
lia
54
CS,
QN
Peo
ple
inse
mi-
ind
ep
en
den
tlivi
ng
arr
an
gem
en
ts(1
–4p
eo
ple
livi
ng
tog
eth
er)
use
dm
ore
com
mu
nit
yfa
ciliti
es
than
did
peo
ple
wh
olive
d
ing
rou
ph
om
es
(3–7
resi
den
ts).
Stan
clif
fe&
Lakin
(1998)
USA
187
CS,
QN
Peo
ple
inco
mm
un
ity
sett
ing
s(2
–15
resi
den
ts)
en
joye
dg
reate
r
com
mu
nit
yp
art
icip
ati
on
than
resi
den
tsin
inst
itu
tio
ns
(16
+re
sid
en
ts).
aC
S5
cro
ss–s
ecti
on
al;
L5
lon
gitu
din
al;
QN
5q
uan
tita
tive
;Q
L5
qu
alit
ativ
e.bT
he
nu
mb
erin
par
enth
eses
ind
icat
esth
ele
ngt
ho
fth
est
ud
yin
year
s.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
E American Association on Intellectual and Developmental Disabilities 197

Tab
le2.
So
cial
Net
wo
rks
and
Fri
end
ship
s
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Em
ers
on
et
al.
(2000b
)
UK
500
CS,
QN
Peo
ple
inco
mm
un
ity
ho
mes
(1–8
resi
den
ts)
an
din
ten
tio
nal
com
mu
nit
ies
(28–1
79
resi
den
tso
nsi
te)
had
larg
er
soci
al
netw
ork
s
than
did
peo
ple
livi
ng
on
cam
pu
sse
ttin
gs
(94–1
44
resi
den
tso
nsi
te).
Em
ers
on
,
Ro
bert
son
,
Gre
go
ry,
Kess
isso
glo
u
et
al.
(2000)
UK
40
CS,
QN
Peo
ple
inco
mm
un
ity
ho
mes
(1–8
resi
den
ts)
had
larg
er
soci
aln
etw
ork
s
than
did
peo
ple
livi
ng
on
cam
pu
sse
ttin
gs
(94–1
44
resi
den
tso
nsi
te).
Em
ers
on
&M
cVilly
(2004)
UK
1,5
42
CS,
QN
Peo
ple
insm
aller
com
mu
nit
y-b
ase
dse
ttin
gs
(1–4
resi
den
ts)
an
d
sup
po
rted
livi
ng
arr
an
gem
en
ts(1
–3p
eo
ple
livi
ng
tog
eth
er)
part
icip
ate
din
mo
refr
ien
dsh
ipact
ivit
ies
than
did
peo
ple
inla
rger
sett
ing
s.O
ther
sett
ing
chara
cteri
stic
s(t
ype
of
pro
visi
on
,st
aff
ing
)
were
als
oim
po
rtan
tp
red
icto
rso
ffr
ien
dsh
ipact
ivit
ies.
Forr
est
er–
Jon
es
et
al.
(2006)
UK
213
CS,
QN
,Q
LPeo
ple
insm
all
com
mu
nit
yh
om
es
(2–5
pla
ces)
,su
pp
ort
ed
an
d
ind
ep
en
den
tlivi
ng
arr
an
gem
en
tsan
dh
ost
els
(6+
resi
den
ts,va
riab
le
staff
sup
po
rt)
had
mo
rere
cip
roca
lre
lati
on
ship
sth
an
did
peo
ple
in
resi
den
tialan
dn
urs
ing
ho
mes
(6+
pla
ces,
con
tin
uo
us
staff
sup
po
rt).
Sup
po
rted
livi
ng
an
dh
ost
el
resi
den
tsre
po
rted
mo
rere
cip
roca
l
rela
tio
nsh
ips.
Heller,
Fact
or
et
al.
(1998)
USA
232
L(3
)b,
QN
Peo
ple
wh
om
ove
dfr
om
nu
rsin
gh
om
es
(mean
size
207
resi
den
ts)
to
com
mu
nit
yse
ttin
gs
(1–8
resi
den
ts)
an
dla
rger
ho
mes
(IC
F/M
R
sett
ing
sw
ith
20
+re
sid
en
ts)
visi
ted
mo
refr
ien
ds
an
dre
ceiv
ed
mo
re
visi
tsth
an
did
no
nm
ove
rs.
McC
on
key
(2007)
Irela
nd
,U
K620
CS,
QN
Peo
ple
incl
ust
ere
dan
dd
isp
ers
ed
sup
po
rted
livi
ng
(1–3
peo
ple
livi
ng
tog
eth
er)
were
mo
relikely
toh
ave
frie
nd
san
dvi
sito
rsfr
om
ou
tsid
e
the
ho
me
than
peo
ple
insm
all
ho
mes
(max.
6p
lace
s),
larg
eh
om
es
(avg
.20
resi
den
ts)
or
inca
mp
us
sett
ing
s(1
00
+re
sid
en
tso
nsi
te).
Ro
bert
son
,
Em
ers
on
,
Gre
go
ryet
al.
(2001)
UK
500
CS,
QN
,Q
LPeo
ple
livi
ng
insm
aller
com
mu
nit
y-b
ase
dse
ttin
gs
(1–8
resi
den
ts)
an
d
inte
nti
on
al
com
mu
nit
ies
(28–1
79
resi
den
tso
nsi
te)
had
larg
er
soci
al
netw
ork
sth
an
did
peo
ple
livi
ng
on
cam
pu
sse
ttin
gs
(94–1
44
resi
den
tso
nsi
te).
(Ta
ble
2co
nti
nu
ed)
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
198 E American Association on Intellectual and Developmental Disabilities
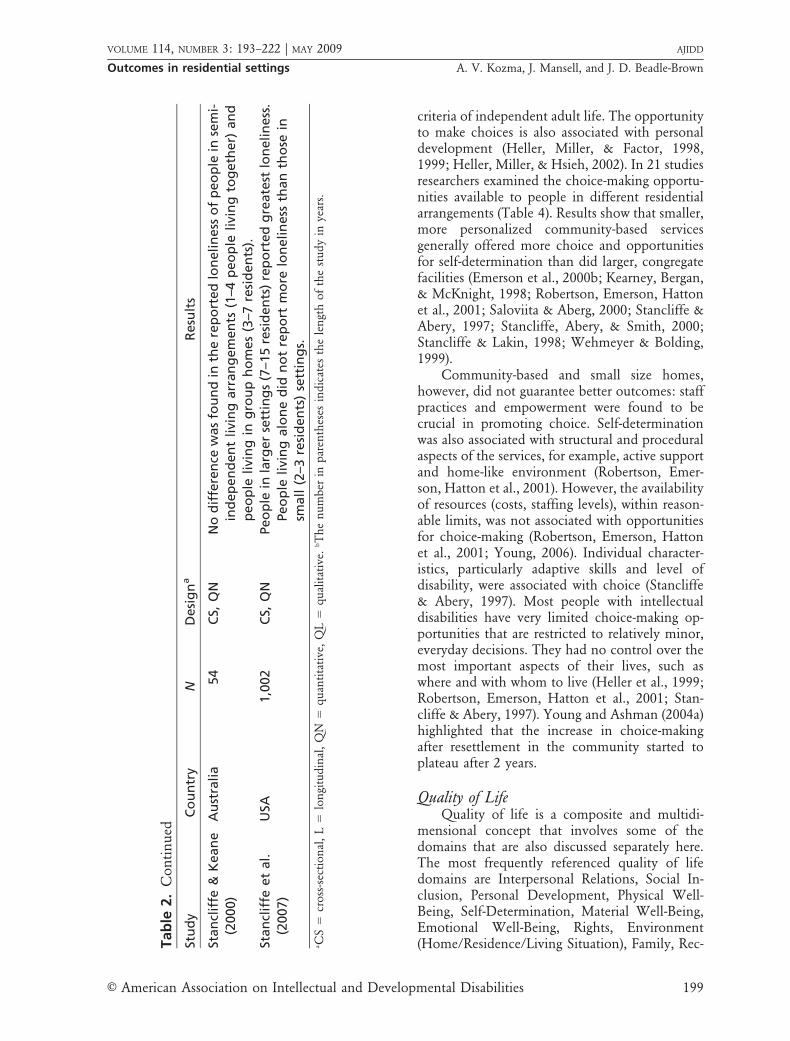
criteria of independent adult life. The opportunityto make choices is also associated with personaldevelopment (Heller, Miller, & Factor, 1998,1999; Heller, Miller, & Hsieh, 2002). In 21 studiesresearchers examined the choice-making opportu-nities available to people in different residentialarrangements (Table 4). Results show that smaller,more personalized community-based servicesgenerally offered more choice and opportunitiesfor self-determination than did larger, congregatefacilities (Emerson et al., 2000b; Kearney, Bergan,& McKnight, 1998; Robertson, Emerson, Hattonet al., 2001; Saloviita & Aberg, 2000; Stancliffe &Abery, 1997; Stancliffe, Abery, & Smith, 2000;Stancliffe & Lakin, 1998; Wehmeyer & Bolding,1999).
Community-based and small size homes,however, did not guarantee better outcomes: staffpractices and empowerment were found to becrucial in promoting choice. Self-determinationwas also associated with structural and proceduralaspects of the services, for example, active supportand home-like environment (Robertson, Emer-son, Hatton et al., 2001). However, the availabilityof resources (costs, staffing levels), within reason-able limits, was not associated with opportunitiesfor choice-making (Robertson, Emerson, Hattonet al., 2001; Young, 2006). Individual character-istics, particularly adaptive skills and level ofdisability, were associated with choice (Stancliffe& Abery, 1997). Most people with intellectualdisabilities have very limited choice-making op-portunities that are restricted to relatively minor,everyday decisions. They had no control over themost important aspects of their lives, such aswhere and with whom to live (Heller et al., 1999;Robertson, Emerson, Hatton et al., 2001; Stan-cliffe & Abery, 1997). Young and Ashman (2004a)highlighted that the increase in choice-makingafter resettlement in the community started toplateau after 2 years.
Quality of LifeQuality of life is a composite and multidi-
mensional concept that involves some of thedomains that are also discussed separately here.The most frequently referenced quality of lifedomains are Interpersonal Relations, Social In-clusion, Personal Development, Physical Well-Being, Self-Determination, Material Well-Being,Emotional Well-Being, Rights, Environment(Home/Residence/Living Situation), Family, Rec-T
ab
le2.
Co
nti
nu
ed
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Stan
clif
fe&
Kean
e
(2000)
Au
stra
lia
54
CS,
QN
No
dif
fere
nce
was
fou
nd
inth
ere
po
rted
lon
elin
ess
of
peo
ple
inse
mi-
ind
ep
en
den
tlivi
ng
arr
an
gem
en
ts(1
–4p
eo
ple
livi
ng
tog
eth
er)
an
d
peo
ple
livi
ng
ing
rou
ph
om
es
(3–7
resi
den
ts).
Stan
clif
feet
al.
(2007)
USA
1,0
02
CS,
QN
Peo
ple
inla
rger
sett
ing
s(7
–15
resi
den
ts)
rep
ort
ed
gre
ate
stlo
nelin
ess
.
Peo
ple
livi
ng
alo
ne
did
no
tre
po
rtm
ore
lon
elin
ess
than
tho
sein
small
(2–3
resi
den
ts)
sett
ing
s.aC
S5
cro
ss-s
ecti
on
al,
L5
lon
gitu
din
al,
QN
5q
uan
tita
tive
,Q
L5
qu
alit
ativ
e.bT
he
nu
mb
erin
par
enth
eses
ind
icat
esth
ele
ngt
ho
fth
est
ud
yin
year
s.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
E American Association on Intellectual and Developmental Disabilities 199

Tab
le3.
Fam
ily
Co
nta
ct
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Ch
ou
et
al.
(2008)
Taiw
an
248
CS,
QN
Peo
ple
insm
all
ho
mes
(max.
6re
sid
en
ts)
rece
ived
mo
refa
mily
visi
ts
than
did
tho
sein
gro
up
ho
mes
(max.
50
resi
den
ts)
an
din
stit
uti
on
s
(50
+re
sid
en
ts).
Em
ers
on
et
al.
(2000b
)
UK
500
CS,
QN
No
sig
nif
ican
td
iffe
ren
cew
as
fou
nd
inth
ele
vel
of
fam
ily
con
tact
in
com
mu
nit
yh
om
es
(1–8
resi
den
ts),
inte
nti
on
al
com
mu
nit
ies
(28–1
79
resi
den
tso
nsi
te)
an
dca
mp
us
sett
ing
s(9
4–1
44
resi
den
tso
nsi
te).
Em
ers
on
,
Ro
bert
son
,
Gre
go
ry,
Kess
isso
glo
uet
al.
(2000)
UK
40
CS,
QN
No
sig
nif
ican
td
iffe
ren
cew
as
fou
nd
betw
een
the
leve
lo
ffa
mily
visi
tsin
com
mu
nit
yh
om
es
(1–8
resi
den
ts)
an
din
cam
pu
sse
ttin
gs
(94–1
44
resi
den
tso
nsi
te).
Heller,
Fact
or
et
al.
(1998)
USA
232
L(3
)b,
QN
No
dif
fere
nce
was
fou
nd
inth
efr
eq
uen
cyan
dp
att
ern
of
fam
ily
con
tact
betw
een
peo
ple
wh
om
ove
dfr
om
nu
rsin
gh
om
es
(mean
size
207
resi
den
ts)
toco
mm
un
ity
sett
ing
s(1
–8re
sid
en
ts)
an
dla
rger
ho
mes
(IC
F/M
Rse
ttin
gs
wit
h20
or
mo
rere
sid
en
ts)
an
dth
ose
wh
ost
aye
d.
McC
on
key
et
al.
(2005)
Irela
nd
106
CS,
QN
No
dir
ect
an
dsi
gn
ific
an
tre
lati
on
ship
was
fou
nd
betw
een
typ
eo
f
acc
om
mo
dati
on
(cam
pu
sw
ith
55
resi
den
tso
nsi
tean
dh
om
es
wit
h5
resi
den
ts)
an
dfa
mily
con
tact
.
Spre
at
et
al.
(1998)
USA
80
L(5
),C
S,Q
NPeo
ple
wh
ore
loca
ted
fro
mn
urs
ing
ho
mes
(avg
.50
resi
den
ts)
to
com
mu
nit
y-b
ase
dsu
pp
ort
ed
livi
ng
arr
an
gem
en
ts(2
–3p
eo
ple
livi
ng
tog
eth
er)
had
incr
ease
dco
nta
ctw
ith
their
fam
ilie
s.Peo
ple
wh
o
rem
ain
ed
inn
urs
ing
ho
mes
exp
eri
en
ced
no
chan
ge.
Stan
clif
fe&
Lakin
(1998)
USA
187
CS,
QN
Peo
ple
inco
mm
un
ity
sett
ing
s(2
–15
resi
den
ts)
had
mo
reco
nta
ctw
ith
their
fam
ilie
sth
an
did
resi
den
tsin
inst
itu
tio
ns
(16
+re
sid
en
ts).
Stan
clif
fe&
Lakin
(2006)
USA
155
L(4
),C
S,Q
NPeo
ple
wh
om
ove
dfr
om
inst
itu
tio
ns
(16
+re
sid
en
ts)
toco
mm
un
ity
sett
ing
s(2
–15
resi
den
ts)
incr
ease
dfa
mily
con
tact
that
rem
ain
ed
stab
le.
Peo
ple
rem
ain
ing
inin
stit
uti
on
sexp
eri
en
ced
gre
ate
rlo
sso
f
con
tact
ove
rti
me.
aC
S5
cro
ss-s
ecti
on
al,
L5
lon
gitu
din
al,
QN
5q
uan
tita
tive
,Q
L5
qu
alit
ativ
e.bT
he
nu
mb
erin
par
enth
eses
ind
icat
esth
ele
ngt
ho
fth
est
ud
yin
year
s.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
200 E American Association on Intellectual and Developmental Disabilities

Tab
le4.
Sel
f-D
eter
min
atio
n/C
ho
ice
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Ch
ou
et
al.
(2008)
Taiw
an
248
CS,
QN
Peo
ple
insm
all
ho
mes
(max.
6re
sid
en
ts)
an
dco
mm
un
ity
ho
mes
(max.
50
resi
den
ts)
had
mo
reo
pp
ort
un
ity
tom
ake
cho
ices
than
did
tho
sew
ho
live
din
inst
itu
tio
ns
(50
+re
sid
en
ts).
Em
ers
on
et
al.
(2000b
)U
K500
CS,
QN
Peo
ple
inco
mm
un
ity
ho
mes
(1–8
resi
den
ts)
had
gre
ate
rch
oic
e
than
peo
ple
inin
ten
tio
nal
com
mu
nit
ies
(28–1
79
resi
den
tso
n
site
)an
dp
eo
ple
inca
mp
us
sett
ing
s(9
4–1
44
resi
den
tso
nsi
te).
Em
ers
on
,R
ob
ert
son
,
Gre
go
ry,
Kess
isso
glo
u
et
al.
(2000)
UK
40
CS,
QN
Peo
ple
inco
mm
un
ity
ho
usi
ng
(1–8
resi
den
ts)
had
gre
ate
rch
oic
e
than
peo
ple
inca
mp
us
sett
ing
s(9
4–1
44
resi
den
tso
nsi
te).
Em
ers
on
et
al.
(2001)
UK
281
CS,
QN
Peo
ple
insu
pp
ort
ed
livi
ng
(1–3
peo
ple
livi
ng
tog
eth
er)
had
gre
ate
ro
vera
llch
oic
ean
dm
ore
cho
ice
ove
rw
ith
wh
om
an
d
wh
ere
they
live
dth
an
did
peo
ple
insm
all
gro
up
ho
mes
(1–3
resi
den
ts)
an
dla
rge
gro
up
ho
mes
(4–6
resi
den
ts).
Felc
e(1
998);
Felc
eet
al.
(2000)
UK
34,
34
CS,
QN
Peo
ple
wit
hse
vere
challen
gin
gb
eh
avi
or
inco
mm
un
ity
sett
ing
s
(1–9
resi
den
ts)
had
hig
her
au
ton
om
yth
an
peo
ple
inh
osp
itals
(10–1
88
resi
den
ts).
Heller,
Mille
ret
al.
(1999)
USA
58
L(3
)b,
QN
Peo
ple
wh
ore
loca
ted
fro
mn
urs
ing
ho
mes
(91–4
17
resi
den
ts)
to
com
mu
nit
y-b
ase
dse
ttin
gs
(1–9
2re
sid
en
ts,
mean
size
58)
incr
ease
dth
eir
au
ton
om
yan
dch
oic
e-m
akin
go
pp
ort
un
itie
s.
Heller
et
al.
(2002)
USA
186
L(8
),C
S,Q
NPeo
ple
wh
om
ove
dto
small
an
dm
ore
att
ract
ive
com
mu
nit
y
sett
ing
s(1
–18
resi
den
ts)
had
mo
reo
pp
ort
un
ity
for
cho
ice-
makin
g,th
an
did
peo
ple
wh
ore
main
ed
inn
urs
ing
ho
mes
(91–
417
resi
den
ts)
or
larg
er,
less
att
ract
ive
sett
ing
s(I
CF/
MR
ho
mes
wit
h20
+re
sid
en
ts).
Kearn
ey
et
al.
(1998)
USA
122,
67
CS,
L(1
.25),
QN
Peo
ple
wh
om
ove
dto
small
com
mu
nit
y-b
ase
dfa
ciliti
es
(6o
r
few
er
resi
den
ts)
fro
mla
rge
inst
itu
tio
ns
(99–2
70
resi
den
ts)
exp
eri
en
ced
an
incr
ease
inch
oic
e.
ava
ilab
ilit
y.
Ro
bert
son
,Em
ers
on
,
Hatt
on
et
al.
(2001)
UK
281
CS,
QN
Peo
ple
insm
aller
com
mu
nit
y-b
ase
dh
om
es
or
sup
po
rted
livi
ng
arr
an
gem
en
ts(1
–3p
eo
ple
livi
ng
tog
eth
er)
an
dw
ith
mo
re
ho
me-l
ike
arc
hit
ect
ura
ld
esi
gn
had
mo
reo
pp
ort
un
itie
sfo
r
self
-dete
rmin
ati
on
than
did
peo
ple
livi
ng
inla
rger
com
mu
nit
y
ho
mes
(4–8
resi
den
ts).
(Ta
ble
4co
nti
nu
ed)
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
E American Association on Intellectual and Developmental Disabilities 201

Tab
le4.
Co
nti
nu
ed
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Salo
viit
a&
Ab
erg
(2000)
Fin
lan
d54
CS,
QN
Peo
ple
ing
rou
ph
om
es
(5–1
2re
sid
en
ts)
had
mo
rese
lf-
dete
rmin
ati
on
than
did
peo
ple
inin
stit
uti
on
s(9
9re
sid
en
ts).
Stan
clif
fe&
Ab
ery
(1997)
USA
127
L(3
),C
S,Q
NPeo
ple
wh
om
ove
dfr
om
an
inst
itu
tio
n(1
6+
resi
den
tso
nsi
te)
to
com
mu
nit
yse
ttin
gs
(2–1
6re
sid
en
ts)
had
gre
ate
rch
oic
e-
makin
go
pp
ort
un
itie
sth
an
did
tho
sew
ho
staye
din
the
inst
itu
tio
ns.
Stan
clif
fe&
Kean
e(2
000)
Au
stra
lia
54
CS,
QN
Peo
ple
inse
mi-
ind
ep
en
den
tlivi
ng
arr
an
gem
en
ts(1
–4p
eo
ple
livi
ng
tog
eth
er)
had
mo
rech
oic
eth
an
peo
ple
wh
olive
din
gro
up
ho
mes
(3–7
resi
den
ts).
Stan
clif
fe&
Lakin
(1998)
USA
187
CS,
QN
Peo
ple
insm
aller
com
mu
nit
yh
om
es
(2–4
an
d5–6
resi
den
ts)
had
mo
rech
oic
eth
an
did
resi
den
tsin
inst
itu
tio
ns
(16
+re
sid
en
ts)
an
dla
rger
com
mu
nit
yse
ttin
gs
(7–1
5re
sid
en
ts).
Stan
clif
fe,
Ab
ery
,&
Smit
h
(2000)
USA
74
CS,
QN
Peo
ple
inse
mi-
ind
ep
en
den
tlivi
ng
arr
an
gem
en
ts(u
pto
3p
eo
ple
livi
ng
tog
eth
er)
had
mo
rep
ers
on
al
con
tro
lan
dse
lf-
dete
rmin
ati
on
than
did
tho
sein
HC
BS
Waiv
er
ho
mes
(2–6
peo
ple
ino
ne
bu
ild
ing
)an
dIC
F/M
Rse
ttin
gs
(4–4
4re
sid
en
tsin
on
eb
uild
ing
).
Weh
meye
r&
Bo
ldin
g
(1999)
USA
273
CS,
QN
Peo
ple
wh
olive
din
no
nco
ng
reg
ate
(1–3
peo
ple
livi
ng
tog
eth
er)
an
dco
ng
reg
ate
(4–6
resi
den
ts)
com
mu
nit
yse
ttin
gs
had
gre
ate
ro
pp
ort
un
itie
sfo
rse
lf-d
ete
rmin
ati
on
than
did
peo
ple
inco
ng
reg
ate
no
nco
mm
un
ity
sett
ing
s(1
2o
rm
ore
resi
den
ts).
Yo
un
g(2
000,
2001);
Yo
un
g&
Ash
man
(2004a)
Au
stra
lia
32,
95,
104
L(1
.5;
1.5
;2.5
),
QN
Peo
ple
had
gre
ate
rch
oic
e-m
akin
go
pp
ort
un
itie
saft
er
relo
cati
on
fro
man
inst
itu
tio
n(1
60
resi
den
ts)
toco
mm
un
ity
sett
ing
s(2
–4re
sid
en
ts).
Yo
un
g(2
006)
Au
stra
lia
60
L(2
.5),
QN
Peo
ple
had
gre
ate
rch
oic
e-m
akin
go
pp
ort
un
itie
saft
er
relo
cati
on
fro
man
inst
itu
tio
n(1
60
resi
den
ts)
toco
mm
un
ity
sett
ing
s(2
–4re
sid
en
ts).
Peo
ple
wh
olive
din
dis
pers
ed
sett
ing
s
had
mo
rech
oic
e-m
akin
go
pp
ort
un
itie
sth
an
did
peo
ple
in
clu
stere
dg
rou
ph
om
es
(up
to20–2
5p
eo
ple
on
on
ep
urp
ose
-
bu
ilt
site
).
Yo
un
g&
Ash
man
(2004b
)A
ust
ralia
104
L(2
.5),
QN
Peo
ple
inall
ag
eg
rou
ps
had
gre
ate
rch
oic
e-m
akin
g
op
po
rtu
nit
ies
aft
er
relo
cati
on
fro
man
inst
itu
tio
n(1
60
resi
den
ts)
toco
mm
un
ity
ho
mes
(2–4
resi
den
ts).
aC
S5
cro
ss-s
ecti
on
al,
L5
lon
gitu
din
al,
QN
5q
uan
tita
tive
,Q
L5
qu
alit
ativ
e.bT
he
nu
mb
erin
par
enth
eses
ind
icat
esth
ele
ngt
ho
fth
est
ud
yin
year
s.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
202 E American Association on Intellectual and Developmental Disabilities
Tab
le5.
Qu
alit
yo
fL
ife
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Ag
er
et
al
(2001)
UK
76
L(1
.6)b
,Q
NPeo
ple
exp
eri
en
ced
bett
er
qu
ality
of
life
aft
er
mo
vin
gfr
om
a
lon
g–s
tay
ho
spit
al
(95
+re
sid
en
ts)
toco
mm
un
ity
ho
mes
(1–
10
resi
den
ts).
Go
ldin
get
al.
(2005)
UK
12
L(1
),C
S,Q
NPeo
ple
had
bett
er
qu
ality
of
life
follo
win
gre
loca
tio
nfr
om
a
ho
spit
al
tosp
eci
alist
challen
gin
gb
eh
avi
or
com
mu
nit
y
sett
ing
s(6
resi
den
ts).
Jan
ssen
,V
reeke
et
al.
(1999)
Ho
llan
d199
CS,
QN
Peo
ple
livi
ng
ind
isp
ers
ed
com
mu
nit
yh
om
es
(1–1
8re
sid
en
ts,
mean
9)
an
din
gro
up
ho
mes
clu
stere
do
nth
esi
teo
fth
e
inst
itu
tio
n(1
–18
resi
den
ts,
mean
9)
had
sim
ilar
qu
ality
of
life
.
Yo
un
g(2
000,
2001)
Au
stra
lia
32,
95
L(1
.5;
1.5
),
QN
Peo
ple
had
bett
er
life
circ
um
stan
ces
aft
er
relo
cati
on
fro
man
inst
itu
tio
n(1
60
resi
den
ts)
toco
mm
un
ity
sett
ing
s(2
–4
resi
den
ts).
Yo
un
g(2
006)
Au
stra
lia
60
L(2
.5),
QN
Peo
ple
had
bett
er
life
circ
um
stan
ces
aft
er
relo
cati
on
fro
man
inst
itu
tio
n(1
60
resi
den
ts)
tod
isp
ers
ed
(2–4
resi
den
ts)
an
d
clu
stere
dco
mm
un
ity
sett
ing
s(2
–4re
sid
en
ts/s
ett
ing
,u
pto
20–2
5p
eo
ple
on
on
ep
urp
ose
-bu
ilt
site
).Peo
ple
in
dis
pers
ed
sett
ing
sh
ad
bett
er
qu
ality
of
life
than
tho
sein
clu
stere
dse
ttin
gs.
Yo
un
g&
Ash
man
(2004a,
2004b
)
Au
stra
lia
104,
104
L(2
.5;
2.5
),
QN
Peo
ple
had
bett
er
life
circ
um
stan
ces
aft
er
relo
cati
on
fro
man
inst
itu
tio
n(1
60
resi
den
ts)
toco
mm
un
ity
ho
mes
(2–4
resi
den
ts),
bu
tth
ere
are
con
sid
era
ble
vari
ati
on
sam
on
g
ind
ivid
uals
an
dse
ttin
gs.
aC
S5
cro
ss-s
ecti
on
al,
L5
lon
gitu
din
al,
QN
5q
uan
tita
tive
,Q
L5
qu
alit
ativ
e.bT
he
nu
mb
erin
par
enth
eses
ind
icat
esth
ele
ngt
ho
fth
est
ud
yin
year
s.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
E American Association on Intellectual and Developmental Disabilities 203

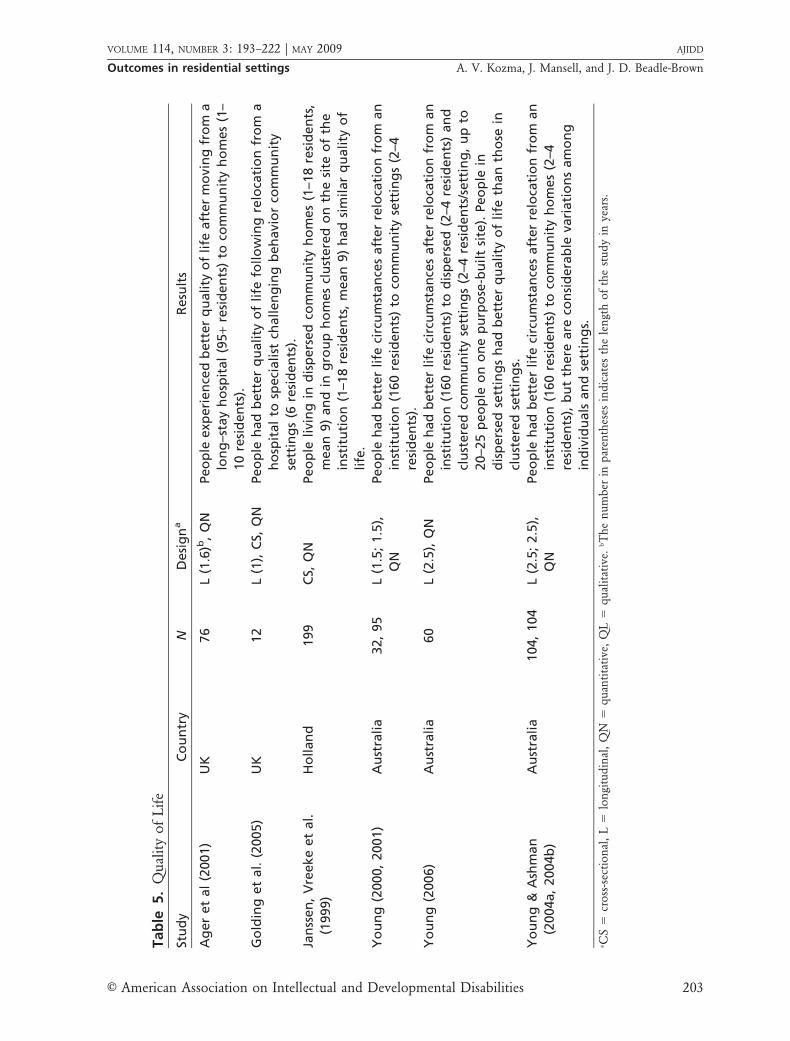
reation and Leisure, and Safety/Security (Ver-dugo, Schalock, Keith, & Stancliffe, 2005).Quality of life measures to evaluate residentialarrangements were used in 8 studies (Table 5).
Relocation to the community was generallyassociated with better quality of life (Ager et al.,2001; Young, 2000, 2001, 2006; Young & Ash-man, 2004a), but there were considerable varia-tions among people and settings in terms of gainsassociated with individual characteristics, staffpractices, and service procedures (Young & Ash-man, 2004b).
Adaptive BehaviorImproving the adaptive skills, abilities, and
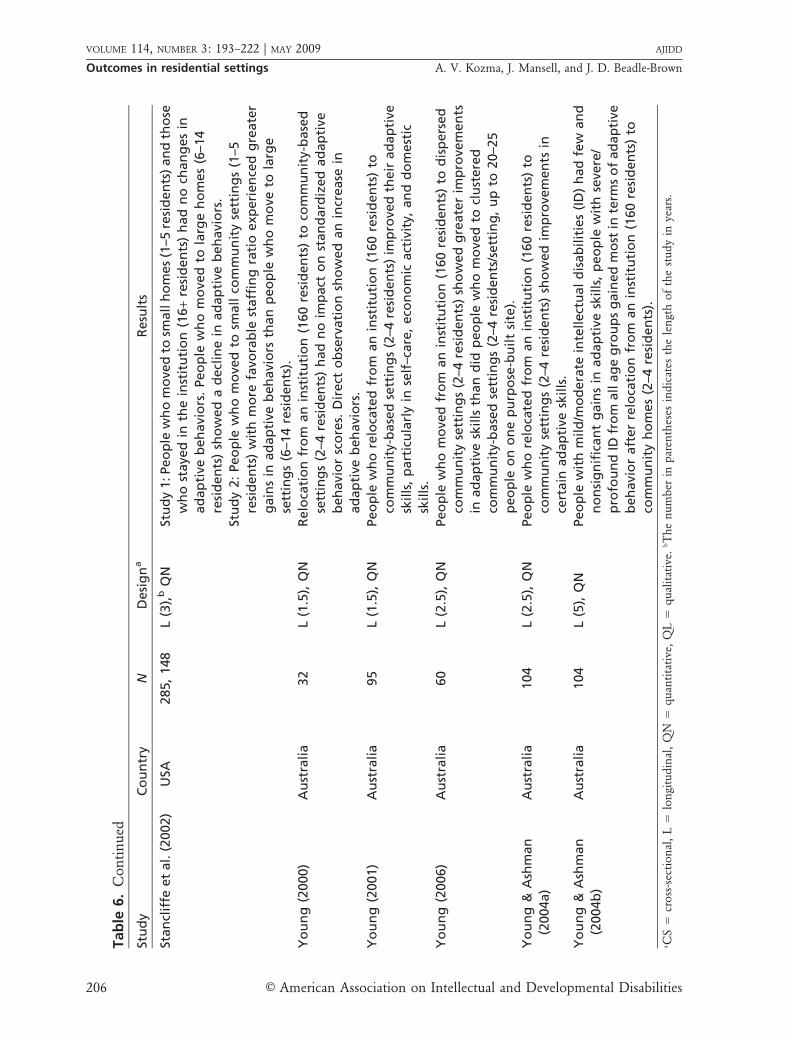
competence of people with intellectual disabilitieswas one of the most important rationales duringthe early stages of deinstitutionalization (Emerson& Hatton, 1994). Level of adaptive behavior is animportant determinant of quality of life. Re-searchers in 15 studies used adaptive behavior asan outcome indicator using standardized mea-sures (Table 6).
Some investigators found no evidence ofincreases in adaptive behavior upon relocationto community housing. Others found improve-ments in certain areas but not in other domains(Heller, Factor, Hsieh, & Hahn, 1998; Macleod,Morrison, Swanston, & Lindsay, 2002; Young,2000, 2001). People who remained in institutionsor other congregate settings were more likely toexperience a decline, whereas movers maintainedor improved their abilities. Some evidence alsosuggests that as a result of resettlement peoplewith more severe and profound disabilities gainedmore in adaptive skills than did people with mild/moderate intellectual disability (Young & Ash-man, 2004b). Some researchers found thatgains in adaptive skills were associated withenvironmental and service factors, includingsmall size, attractiveness and stimulation of thephysical environment, opportunities for choice-making (Heller, Miller et al., 1998; Spreatet al., 1998; Stancliffe, Hayden, Larson, & Lakin,2002), teaching of skills and autonomy (Lerman,Apgar, & Jordan, 2005), and implementation ofactive support (Young, 2006; Young & Ashman,2004a).
Challenging BehaviorEmerson and Hatton (1994) noted that
challenging behaviors are
culturally unusual or unacceptable behaviors, such as self-injury or aggression, that place the health or safety of theperson or others in jeopardy or are likely to lead to the personbeing excluded or denied access to ordinary communitysettings. (p. 17)
Challenging behaviors are, therefore, an impor-tant determinant of quality of life. In 13 studiesresearchers looked at individual challengingbehavior and in 4 others compared responses tochallenging behavior in different residential ar-rangements (Tables 7 and 8).
Most investigators reported no significantchanges in challenging behaviors upon resettle-ment to different forms of community residences(Heller, Factor et al., 1998; Hundert, Walton-Allen, Vasdev, Cope, & Summers, 2003; Spreat etal., 1998; Stancliffe et al., 2002; Young &Ashman, 2004b); others, however, found adeterioration in certain behaviors, such as disrup-tive behavior and passivity (Nøttestad & Linaker,1999, 2002). Others noted that although the levelof challenging behavior as measured by standard-ized instruments remained the same, observationrevealed changes in the nature of challengingbehaviors and the reduction of certain problembehaviors after relocation (Golding, Emerson, &Thornton, 2005; Young, 2006; Young & Ashman,2004a).
The ecobehavioral relationship between staffattention and challenging behavior was found tobe similar in institutions and in the community:Problem behavior was associated with lack of staffattention, and staff tended to respond more tochallenging behavior than to appropriate behavioracross all setting-types (Hundert et al., 2003).
Treatment and management of challengingbehavior were found to be associated withcharacteristics of the residence: institution per-sonnel used more restrictive practices (Saloviita,2002), and workers in community-based serviceswere more likely to use sedation (Emerson et al.,2000a). People in community-based settingsreceived more informal interventions, whereasthose in institutions had more formal interven-tions and access to professional behavioralsupport (Stancliffe, Hayden, & Lakin, 1999).
Psychotropic MedicationPsychotropic medication is widely used to
manage and reduce challenging behaviors, al-though their efficacy is questionable (Matson etal., 2000). The use of psychotropic drugs isreceiving increased attention; researchers in 4
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
204 E American Association on Intellectual and Developmental Disabilities

Tab
le6.
Ad
apti
veB
ehav
ior
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Go
ldin
get
al.
(2005)
UK
12
L(1
)bC
S,Q
NPeo
ple
wh
ore
loca
ted
fro
ma
ho
spit
al
tosp
eci
alist
challen
gin
g
beh
avi
or
com
mu
nit
yse
ttin
gs
(6re
sid
en
ts)
gain
ed
do
mest
icsk
ills
.
Peo
ple
alr
ead
ylivi
ng
inco
mm
un
ity
ho
mes
(6re
sid
en
ts)
als
o
sho
wed
imp
rove
men
tsin
ad
ap
tive
skills
.
Heller,
Fact
or
et
al.
(1998)
USA
232
L(3
),Q
NPeo
ple
wh
om
ove
dfr
om
nu
rsin
gh
om
es
(mean
size
207
resi
den
ts)
to
com
mu
nit
yse
ttin
gs
(1–8
resi
den
ts)
an
dla
rger
ho
mes
(IC
F/M
R
sett
ing
sw
ith
20
or
mo
rere
sid
en
ts)
imp
rove
dad
ap
tive
beh
avi
ors
,
wh
ere
as
no
nm
ove
rsd
ecl
ined
.
Heller,
Mille
ret
al.
(2002)
USA
186
L(8
),C
S,Q
NPeo
ple
wh
om
ove
dto
com
mu
nit
yse
ttin
gs
(1–1
8re
sid
en
ts)
an
dIC
F/
MR
sett
ing
s(2
0o
rm
ore
resi
den
ts)
main
tain
ed
their
ad
ap
tive
skills
,
wh
ere
as
peo
ple
wh
ost
aye
din
nu
rsin
gh
om
es
(91–4
17
resi
den
ts)
decl
ined
.
Heller,
Mille
ret
al.
(1998)
USA
268
L(3
),Q
NPeo
ple
wh
ore
loca
ted
fro
mn
urs
ing
ho
mes
(82–4
85
resi
den
ts,
mean
285)
toco
mm
un
ity-b
ase
dse
ttin
gs
(2–4
8re
sid
en
ts,
mean
8)
sho
wed
gain
sin
ad
ap
tive
skills
,p
art
icu
larl
yth
ose
wh
om
ove
dto
smaller
ho
mes.
Kearn
ey
et
al.
(1998)
USA
67
L(1
.25),
QN
Peo
ple
wh
om
ove
dfr
om
ala
rge
inst
itu
tio
n(9
9–2
70
resi
den
ts)
to
com
mu
nit
y-b
ase
dh
om
es
(6o
rfe
wer
resi
den
ts)
exp
eri
en
ced
po
siti
vech
an
ges
inad
ap
tive
skills
.
Lerm
an
et
al.
(2005)
USA
220
(160)
L(7
),Q
NPeo
ple
wh
om
ove
dfr
om
an
inst
itu
tio
n(1
,190
resi
den
ts)
to
com
mu
nit
y-b
ase
dse
ttin
gs
exp
eri
en
ced
an
ove
rall
imp
rove
men
tin
ad
ap
tive
skills
wh
ile
staye
rsm
ain
tain
ed
or
decl
ined
their
ad
ap
tive
beh
avi
ors
.
Macl
eo
det
al.
(2002)
UK
4L
(3),
QN
Peo
ple
wh
om
ove
dfr
om
alo
ng
–sta
yh
osp
ital
toa
com
mu
nit
yh
om
e
sho
wed
an
incr
ease
inco
mm
un
icati
on
beh
avi
ors
an
dan
imp
rove
men
tin
daily
livi
ng
skills
as
measu
red
by
stan
dard
ized
inst
rum
en
ts.
Ho
weve
r,d
irect
ob
serv
ati
on
sho
wed
ad
ecr
ease
in
ad
ap
tive
beh
avi
ors
.
Spre
at
et
al.
(1998)
USA
80
L(5
),Q
NPeo
ple
wh
ore
loca
ted
fro
mn
urs
ing
ho
mes
(avg
.50
resi
den
ts)
to
com
mu
nit
y-b
ase
dsu
pp
ort
ed
livi
ng
arr
an
gem
en
ts(2
–3p
eo
ple
livi
ng
tog
eth
er)
sho
wed
no
chan
ges
inad
ap
tive
skills
,b
ut
tho
se
wh
ost
aye
din
nu
rsin
gh
om
es
exp
eri
en
ced
ad
ecl
ine.
(Ta
ble
6co
nti
nu
ed)
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
E American Association on Intellectual and Developmental Disabilities 205
Tab
le6.
Co
nti
nu
ed
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Stan
clif
feet
al.
(2002)
USA
285,
148
L(3
),b
QN
Stu
dy
1:Peo
ple
wh
om
ove
dto
small
ho
mes
(1–5
resi
den
ts)
an
dth
ose
wh
ost
aye
din
the
inst
itu
tio
n(1
6+
resi
den
ts)
had
no
chan
ges
in
ad
ap
tive
beh
avi
ors
.Peo
ple
wh
om
ove
dto
larg
eh
om
es
(6–1
4
resi
den
ts)
sho
wed
ad
ecl
ine
inad
ap
tive
beh
avi
ors
.
Stu
dy
2:
Peo
ple
wh
om
ove
dto
small
com
mu
nit
yse
ttin
gs
(1–5
resi
den
ts)
wit
hm
ore
favo
rab
lest
aff
ing
rati
oexp
eri
en
ced
gre
ate
r
gain
sin
ad
ap
tive
beh
avi
ors
than
peo
ple
wh
om
ove
tola
rge
sett
ing
s(6
–14
resi
den
ts).
Yo
un
g(2
000)
Au
stra
lia
32
L(1
.5),
QN
Relo
cati
on
fro
man
inst
itu
tio
n(1
60
resi
den
ts)
toco
mm
un
ity-b
ase
d
sett
ing
s(2
–4re
sid
en
ts)
had
no
imp
act
on
stan
dard
ized
ad
ap
tive
beh
avi
or
sco
res.
Dir
ect
ob
serv
ati
on
sho
wed
an
incr
ease
in
ad
ap
tive
beh
avi
ors
.
Yo
un
g(2
001)
Au
stra
lia
95
L(1
.5),
QN
Peo
ple
wh
ore
loca
ted
fro
man
inst
itu
tio
n(1
60
resi
den
ts)
to
com
mu
nit
y-b
ase
dse
ttin
gs
(2–4
resi
den
ts)
imp
rove
dth
eir
ad
ap
tive
skills
,p
art
icu
larl
yin
self
–care
,eco
no
mic
act
ivit
y,an
dd
om
est
ic
skills
.
Yo
un
g(2
006)
Au
stra
lia
60
L(2
.5),
QN
Peo
ple
wh
om
ove
dfr
om
an
inst
itu
tio
n(1
60
resi
den
ts)
tod
isp
ers
ed
com
mu
nit
yse
ttin
gs
(2–4
resi
den
ts)
sho
wed
gre
ate
rim
pro
vem
en
ts
inad
ap
tive
skills
than
did
peo
ple
wh
om
ove
dto
clu
stere
d
com
mu
nit
y-b
ase
dse
ttin
gs
(2–4
resi
den
ts/s
ett
ing
,u
pto
20–2
5
peo
ple
on
on
ep
urp
ose
-bu
ilt
site
).
Yo
un
g&
Ash
man
(2004a)
Au
stra
lia
104
L(2
.5),
QN
Peo
ple
wh
ore
loca
ted
fro
man
inst
itu
tio
n(1
60
resi
den
ts)
to
com
mu
nit
yse
ttin
gs
(2–4
resi
den
ts)
sho
wed
imp
rove
men
tsin
cert
ain
ad
ap
tive
skills
.
Yo
un
g&
Ash
man
(2004b
)
Au
stra
lia
104
L(5
),Q
NPeo
ple
wit
hm
ild
/mo
de
rate
inte
llect
ual
dis
ab
ilit
ies
(ID
)h
ad
few
an
d
no
nsi
gn
ific
an
tg
ain
sin
ad
ap
tive
skills
,p
eo
ple
wit
hse
vere
/
pro
fou
nd
IDfr
om
all
ag
eg
rou
ps
gain
ed
mo
stin
term
so
fad
ap
tive
beh
avi
or
aft
er
relo
cati
on
fro
man
inst
itu
tio
n(1
60
resi
den
ts)
to
com
mu
nit
yh
om
es
(2–4
resi
den
ts).
aC
S5
cro
ss-s
ecti
on
al,
L5
lon
gitu
din
al,
QN
5q
uan
tita
tive
,Q
L5
qu
alit
ativ
e.bT
he
nu
mb
erin
par
enth
eses
ind
icat
esth
ele
ngt
ho
fth
est
ud
yin
year
s.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
206 E American Association on Intellectual and Developmental Disabilities

Tab
le7.
Ch
alle
ngi
ng
Beh
avio
r
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Go
ldin
get
al.
(2005)
UK
12
L(1
),b
CS,
QN
Peo
ple
wh
ore
loca
ted
fro
ma
ho
spit
al
tosp
eci
alist
challen
gin
g
beh
avi
or
com
mu
nit
yse
ttin
gs
(6re
sid
en
ts)
decr
ease
do
bse
rved
challen
gin
gb
eh
avi
ors
bu
th
ad
no
chan
ges
inst
an
dard
ize
dsc
ore
s.
Peo
ple
alr
ead
ylivi
ng
inco
mm
un
ity
sett
ing
s(6
resi
den
ts)
sho
wed
no
chan
ges.
Hu
nd
ert
et
al.
(2003)
Can
ad
a17
L(1
.3),
QN
Peo
ple
wh
ore
loca
ted
fro
man
inst
itu
tio
n(7
0re
sid
en
ts)
tod
isp
ers
ed
com
mu
nit
y-b
ase
dse
ttin
gs
(5re
sid
en
ts)
main
tain
ed
challen
gin
g
beh
avi
or
at
sim
ilar
leve
ls.
Macl
eo
det
al.
(2002)
UK
4L
(3),
QN
Peo
ple
wh
om
ove
dfr
om
ala
rge
ho
spit
al
toa
com
mu
nit
yh
om
e
sho
wed
an
incr
ease
inch
allen
gin
gb
eh
avi
or
alo
ng
wit
h
imp
rove
men
tin
ad
ap
tive
an
dco
mm
un
icati
on
skills
.
Nø
ttest
ad
&Li
naker
(1999)
No
rway
109
L(8
),Q
NPeo
ple
wh
ore
loca
ted
fro
man
inst
itu
tio
n(1
28
resi
den
ts)
to
com
mu
nit
yse
ttin
gs
sho
wed
incr
ease
dag
gre
ssio
nto
ward
so
thers
,
dis
rup
tive
beh
avi
or,
an
dp
ass
ivit
y,b
ut
no
chan
ges
inse
lf-i
nju
ry
an
dd
est
ruct
ion
of
ob
ject
s.
Nø
ttest
ad
&Li
naker
(2001)
No
rway
68
L(8
),Q
ND
eve
lop
men
to
fse
lf-i
nju
ryaft
er
rese
ttle
men
tfr
om
an
inst
itu
tio
n
(128
resi
den
ts)
toco
mm
un
ity-
base
dse
ttin
gs
was
no
tass
oci
ate
d
wit
hse
ttin
gsi
zean
dty
pe.
Nø
ttest
ad
&Li
naker
(2002)
No
rway
64
L(8
),C
S,Q
ND
eve
lop
men
to
fag
gre
ssiv
eb
eh
avi
or
aft
er
relo
cati
on
fro
man
inst
itu
tio
n(1
28
resi
den
ts)
toco
mm
un
ity-b
ase
dse
ttin
gs
was
no
t
ass
oci
ate
dw
ith
sett
ing
size
an
dty
pe.
Spre
at
et
al.
(1998)
USA
80
L(5
),C
S,Q
NPeo
ple
wh
ore
loca
ted
fro
mn
urs
ing
ho
mes
(avg
.50
resi
den
ts)
to
com
mu
nit
y-b
ase
dsu
pp
ort
ed
livi
ng
arr
an
gem
en
ts(2
–3p
eo
ple
livi
ng
tog
eth
er)
an
dp
eo
ple
wh
ost
aye
din
nu
rsin
gh
om
es
sho
wed
no
chan
ges
inch
allen
gin
gb
eh
avi
ors
.
Stan
clif
feet
al.
(2002)
USA
285,
148
L(3
),C
S,Q
NSt
ud
y1:In
itia
ld
ete
rio
rati
on
inch
allen
gin
gb
eh
avi
or
aft
er
relo
cati
on
fro
man
inst
itu
tio
n(1
6+
resi
den
ts)
toco
mm
un
ity
sett
ing
s(1
–14
resi
den
ts)
was
fou
nd
.O
nth
elo
ng
er
term
,n
od
iffe
ren
cefr
om
inst
itu
tio
nal
leve
lso
fp
rob
lem
beh
avi
or
occ
urr
ed
.
Stu
dy
2:
Ch
an
ges
inch
allen
gin
gb
eh
avi
or
were
no
tre
late
dto
com
mu
nit
yse
ttin
gty
pe
(IC
F/M
Ro
rH
CB
SW
aiv
er)
. (Ta
ble
7co
nti
nu
ed)
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
E American Association on Intellectual and Developmental Disabilities 207
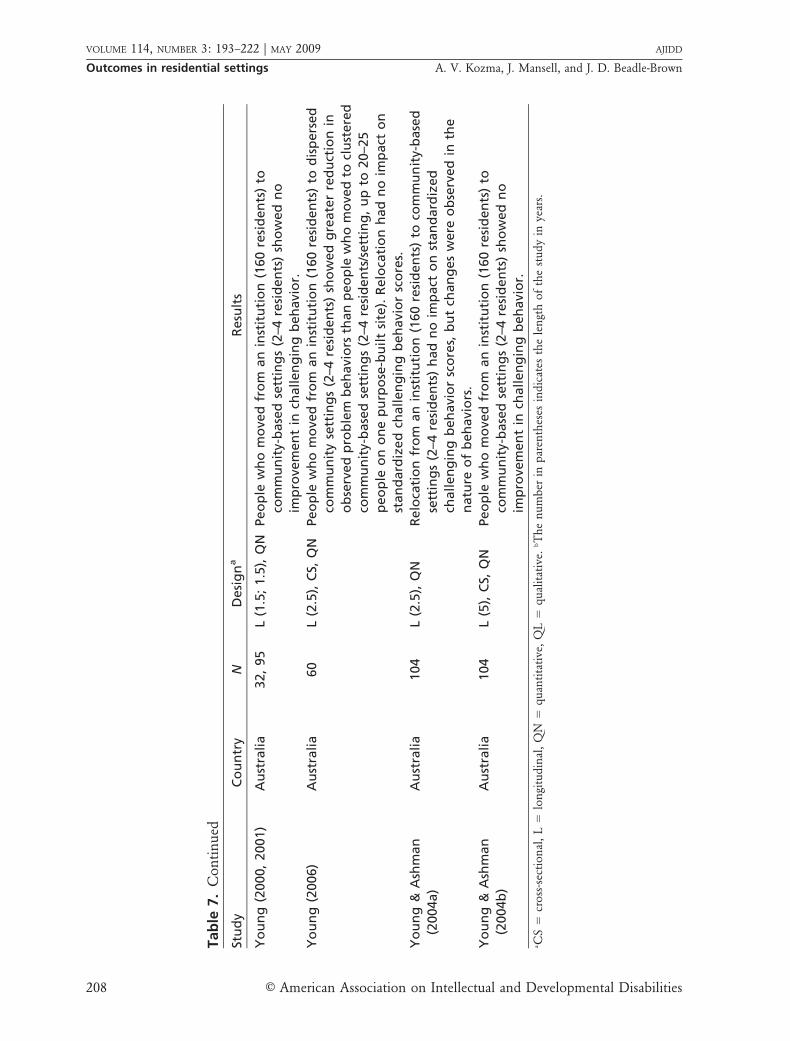
Tab
le7.
Co
nti
nu
ed
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Yo
un
g(2
000,
2001)
Au
stra
lia
32,
95
L(1
.5;
1.5
),Q
NPeo
ple
wh
om
ove
dfr
om
an
inst
itu
tio
n(1
60
resi
den
ts)
to
com
mu
nit
y-b
ase
dse
ttin
gs
(2–4
resi
den
ts)
sho
wed
no
imp
rove
men
tin
challen
gin
gb
eh
avi
or.
Yo
un
g(2
006)
Au
stra
lia
60
L(2
.5),
CS,
QN
Peo
ple
wh
om
ove
dfr
om
an
inst
itu
tio
n(1
60
resi
den
ts)
tod
isp
ers
ed
com
mu
nit
yse
ttin
gs
(2–4
resi
den
ts)
sho
wed
gre
ate
rre
du
ctio
nin
ob
serv
ed
pro
ble
mb
eh
avi
ors
than
peo
ple
wh
om
ove
dto
clu
stere
d
com
mu
nit
y-b
ase
dse
ttin
gs
(2–4
resi
den
ts/s
ett
ing
,u
pto
20–2
5
peo
ple
on
on
ep
urp
ose
-bu
ilt
site
).R
elo
cati
on
had
no
imp
act
on
stan
dard
ize
dch
allen
gin
gb
eh
avi
or
sco
res.
Yo
un
g&
Ash
man
(2004a)
Au
stra
lia
104
L(2
.5),
QN
Relo
cati
on
fro
man
inst
itu
tio
n(1
60
resi
den
ts)
toco
mm
un
ity-
base
d
sett
ing
s(2
–4re
sid
en
ts)
had
no
imp
act
on
stan
dard
ized
challen
gin
gb
eh
avi
or
sco
res,
bu
tch
an
ges
were
ob
serv
ed
inth
e
natu
reo
fb
eh
avi
ors
.
Yo
un
g&
Ash
man
(2004b
)
Au
stra
lia
104
L(5
),C
S,Q
NPeo
ple
wh
om
ove
dfr
om
an
inst
itu
tio
n(1
60
resi
den
ts)
to
com
mu
nit
y-b
ase
dse
ttin
gs
(2–4
resi
den
ts)
sho
wed
no
imp
rove
men
tin
challen
gin
gb
eh
avi
or.
aC
S5
cro
ss-s
ecti
on
al,
L5
lon
gitu
din
al,
QN
5q
uan
tita
tive
,Q
L5
qu
alit
ativ
e.bT
he
nu
mb
erin
par
enth
eses
ind
icat
esth
ele
ngt
ho
fth
est
ud
yin
year
s.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
208 E American Association on Intellectual and Developmental Disabilities

studies addressed this issue (Table 9). Some founda decrease in the medication of people withintellectual disabilities moving to communitysettings (Spreat et al., 1998), others reportednonsignificant changes in the number of peopleon medication, dosage, and frequency (Nøttestad& Linaker, 2003).
McGillvray and McCabe (2005) showed asignificant increase in psychotropic medicationuse in Australian community settings in the1990s; the authors reported a similar percentageof people receiving drugs in the community andin institutions in 2000. However, polypharmacywas still more widespread in institutions (McGil-livray & McCabe, 2005; Robertson, Emerson,Gregory, Hatton, Kessissoglou, & Hallam, 2000).
Health, Risk Factors, and MortalityImproving health and reducing lifestyle-relat-
ed risks have been important in most countries.Not only are they central to the well-being ofindividuals, but poor health imposes significantcosts on health and social services. Despite itsrelevance, relatively little is known about thehealth-related outcomes of different residentialarrangements. Researchers in 6 studies surveyedhealth and lifestyle-related risk factors (Table 10).
Most researchers found no evidence oftransfer trauma or transition shock nor of anincrease in mental health problems among peoplemoving to community settings (Heller, Factor etal., 1998; Nøttestad & Linaker, 1999; Read, 2004);however in some mortality studies (e.g., Strauss,Shavelle, Baumeister, & Anderson, 1998), re-searchers claimed that the higher rate of mortalityshortly after relocation could possibly be attribut-ed to a relocation syndrome.
The prevalence of certain health risk factors,particularly inactivity and obesity among peoplewith intellectual disability, was high. Less restric-tive living arrangements decreased the likelihoodof inactivity but increased the probability ofsmoking, poor diet, and obesity. There weresignificant differences between men and women(Bryan, Allan, & Russell, 2000; Robertson et al.,2000).
A special aspect of community living is theexposure to crime and abuse, which has receivedlimited attention in the literature (see Table 11).Higher perceived exposure to crime and verbalabuse were thought to be associated with sup-ported, semi-independent, or independent living
arrangements (Emerson et al., 2001). People livingin intentional communities or other clusteredresidences were perceived to be at less risk(Emerson, Robertson, Gregory, Kessissoglou etal., 2000).
The issue of mortality in community settingshas received considerable attention mainly in theliterature in the United States. Ten studies on thisissue are included in the review (see Table 12).Some researchers found improvements (Conroy& Adler, 1998); others, no difference (O’Brien &Zaharia, 1998) or higher risk of mortality in thecommunity (Shavelle & Strauss, 1999; Shavelle,Strauss, & Day, 2005; Strauss, Anderson, Shavelle,Sheridan, & Trenkle, 1998; Strauss, Kastner, &Shavelle, 1998; Strauss, Shavelle, Anderson, &Baumeister, 1998; Strauss et al., 1998). Higher riskwas hypothesized to be the outcome of inade-quate access to health care. Some results suggestthat higher mortality was not related to relocationbut rather to the presence of specific risk variablesin the people selected for moving (Lerman, Apgar,& Jordan, 2003; Read, 2004).
User and Family Views and SatisfactionAn important aspect of service provision is
the satisfaction of its users. The utilization ofsubjective measures in evaluation has beencontested (Hatton, 1998; Perry & Felce, 2005;Verdugo et al., 2005), and it is not verywidespread. In 6 studies researchers surveyed theviews of service users and their families byemploying mainly quantitative techniques (Ta-ble 13).
Investigators found high satisfaction withcommunity-based arrangements among both ser-vice users and their families. Movers were criticalabout institutions and did not want to return—even if they missed certain things, such as peopleand some activities (Gregory, Robertson, Kessis-soglou, Emerson, & Hatton, 2001). Although ahigher number of parents and family membershad been critical of deinstitutionalization and theprospect of resettlement initially, the majoritywere positive once it happened (McConkey,McConaghie, Mezza, & Wilson, 2003; NoonanWalsh et al., 2001; O’Brien, 2001), and satisfac-tion remained stable over a period of 10 years(Tøssebro & Lundeby, 2006).
A limitation of these results should be kept inmind, however; researchers often used retrospec-tive methods that are likely to distort opinion in
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
E American Association on Intellectual and Developmental Disabilities 209

favor of current arrangements. Most parentsreported high satisfaction with institutions (Lar-son & Lakin, 1991).
Discussion
In this review we have presented the out-comes of deinstitutionalization and a comparisonof different residential arrangements for peoplewith intellectual disabilities using studies pub-lished between 1997 and 2007. In these studiesresearchers have predominantly reported onmature service models from countries wheredeinstitutionalization has been unfolding fordecades and has made considerable progress. Fivemain conclusions emerge from this literature: (a)the overall picture is comparable to previousreviews, namely, small-scale arrangements aresuperior to large, congregate options in mostdomains; (b) there is considerable variability inindividual outcomes based on individual andservice characteristics; (c) there are three areaswhere community-based services do not providebetter outcomes; (d) experiences are similar indifferent countries; and (e) despite significantimprovements, people with intellectual disabili-ties are still one of the most disadvantaged groupsof society. Finally, some implications for futureresearch are highlighted.
Similar outcomes to earlier studies. In theevaluation literature, researchers have largelyfocused on objective components of quality oflife measurements (Verdugo et al., 2005) usingstandardized instruments. Community participa-tion, choice, and adaptive and challengingbehaviors are the most often used outcomemeasures, but new issues have also receivedattention, such as psychotropic drug use, risks,and lifestyle-related risk factors.
Results have confirmed the picture that hademerged from previous research: People in small-scale community-based residences or in semi-independent or supported living arrangementshave a better objective quality of life than dopeople in large, congregate settings. Particularly,they have more choice-making opportunities;larger social networks and more friends; accessmore mainstream facilities, and participate morein community life; have more chances to acquirenew skills and develop or maintain existing skills;and are more satisfied with their living arrange-ments. In a recent unpublished review, NoonanWalsh et al. (2007) found similar results.T
ab
le8.
Tre
atm
ent
of
Ch
alle
ngi
ng
Beh
avio
r
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Em
ers
on
et
al.
(2000a)
UK
500
CS,
QN
Co
mm
un
ity-
base
dh
om
es
(1–8
resi
den
ts)
were
mo
relikely
tou
sese
dati
on
;
cam
pu
sse
ttin
gs
(94–1
44
resi
den
tso
nsi
te)
use
dm
ore
ph
ysic
al
rest
rain
t.
Feld
man
et
al.
(2004)
Can
ad
a625
CS,
QN
Inst
itu
tio
ns
(300–7
00
resi
den
ts),
gro
up
ho
mes,
an
din
dep
en
den
t/se
mi-
ind
ep
en
den
tlivi
ng
arr
an
gem
en
tsare
no
td
iffe
ren
tin
term
so
ffo
rmality
of
inte
rven
tio
ns
tom
an
ag
ech
allen
gin
gb
eh
avi
ors
.
Salo
viit
a(2
002)
Fin
lan
d261
CS,
QN
Peo
ple
wh
olive
din
inst
itu
tio
ns
(159
resi
den
ts)
were
sub
ject
ed
tom
ore
rest
rict
ive
an
dn
eg
ati
vep
ract
ices
tom
an
ag
ech
allen
gin
gb
eh
avi
or
than
were
tho
sein
clu
stere
dco
mm
un
ity
ho
mes
(5re
sid
en
ts/s
ett
ing
,3
sett
ing
scl
ust
ere
d
tog
eth
er
inth
eco
mm
un
ity)
an
dg
rou
ph
om
es
(5–1
0re
sid
en
ts).
Stan
clif
fe,
Hayd
en
et
al.
(1999)
USA
151
L(3
)b,
QN
Peo
ple
wh
om
ove
dto
com
mu
nit
y-b
ase
dse
ttin
gs
(2–1
5re
sid
en
ts,m
ean
6.6
)h
ad
mo
rein
form
al
inte
rven
tio
ns
tom
an
ag
ech
allen
gin
gb
eh
avi
ors
.Part
icip
an
ts
wh
ost
aye
din
inst
itu
tio
ns
(16
+re
sid
en
ts)
were
mo
relikely
tore
ceiv
efo
rmal
inte
rven
tio
ns
an
dp
rofe
ssio
nal
beh
avi
or
sup
po
rtse
rvic
es.
aC
S5
cro
ss-s
ecti
on
al,
L5
lon
gitu
din
al,
QN
5q
uan
tita
tive
,Q
L5
qu
alit
ativ
e.bT
he
nu
mb
erin
par
enth
eses
ind
icat
esth
ele
ngt
ho
fth
est
ud
yin
year
s.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
210 E American Association on Intellectual and Developmental Disabilities

Tab
le9.
Psy
cho
tro
pic
Med
icat
ion
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Spre
at
Co
nro
yet
al.
(1998)
USA
80
L(5
)b,
CS,
QN
Peo
ple
rece
ived
less
med
icati
on
aft
er
relo
cati
on
fro
mn
urs
ing
ho
mes
(avg
.50
resi
den
ts)
tosu
pp
ort
ed
livi
ng
arr
an
gem
en
ts(2
–3p
eo
ple
livi
ng
tog
eth
er)
than
tho
sew
ho
staye
din
nu
rsin
gh
om
es.
Nø
ttest
ad
&Li
naker
(2003)
No
rway
109
L(8
),Q
NN
um
be
ro
fp
eo
ple
rece
ivin
gm
ed
icati
on
befo
rean
daft
er
relo
cati
on
fro
man
inst
itu
tio
n(1
28
resi
den
ts)
toco
mm
un
ity
sett
ing
sd
ecl
ined
no
nsi
gn
ific
an
tly.
McG
illv
ray
&
McC
ab
e(2
005)
Au
stra
lia
762,
873
L(8
),C
S,Q
NN
od
iffe
ren
ceb
etw
een
pro
po
rtio
no
fp
eo
ple
inco
mm
un
ity
sett
ing
s
an
din
stit
uti
on
sw
ho
rece
ived
med
icati
on
tom
an
ag
ech
allen
gin
g
beh
avi
ors
.In
itia
ld
iffe
ren
ces
inle
vel
of
dru
gu
seb
etw
een
inst
itu
tio
ns
an
dco
mm
un
ity
sett
ing
sw
ere
red
uce
d.
Ro
bert
son
,
Em
ers
on
,
Gre
go
ry,
Hatt
on
,
Kess
isso
glo
u,
&
Hallam
(2000)
UK
500
CS,
QN
Peo
ple
wh
olive
din
cam
pu
sse
ttin
gs
(94–1
44
resi
den
tso
nsi
te)
were
mo
relikely
tore
ceiv
ep
sych
otr
op
icm
ed
icati
on
an
dm
ore
than
on
e
typ
eo
fp
sych
otr
op
icm
ed
icati
on
than
were
peo
ple
inin
ten
tio
nal
com
mu
nit
ies
(28–1
79
resi
den
tso
nsi
te)
an
dco
mm
un
ity
sett
ing
s(1
–
8re
sid
en
ts).
aC
S5
cro
ss-s
ecti
on
al,
L5
lon
gitu
din
al,
QN
5q
uan
tita
tive
,Q
L5
qu
alit
ativ
e.bT
he
nu
mb
erin
par
enth
eses
ind
icat
esth
ele
ngt
ho
fth
est
ud
yin
year
s.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
E American Association on Intellectual and Developmental Disabilities 211
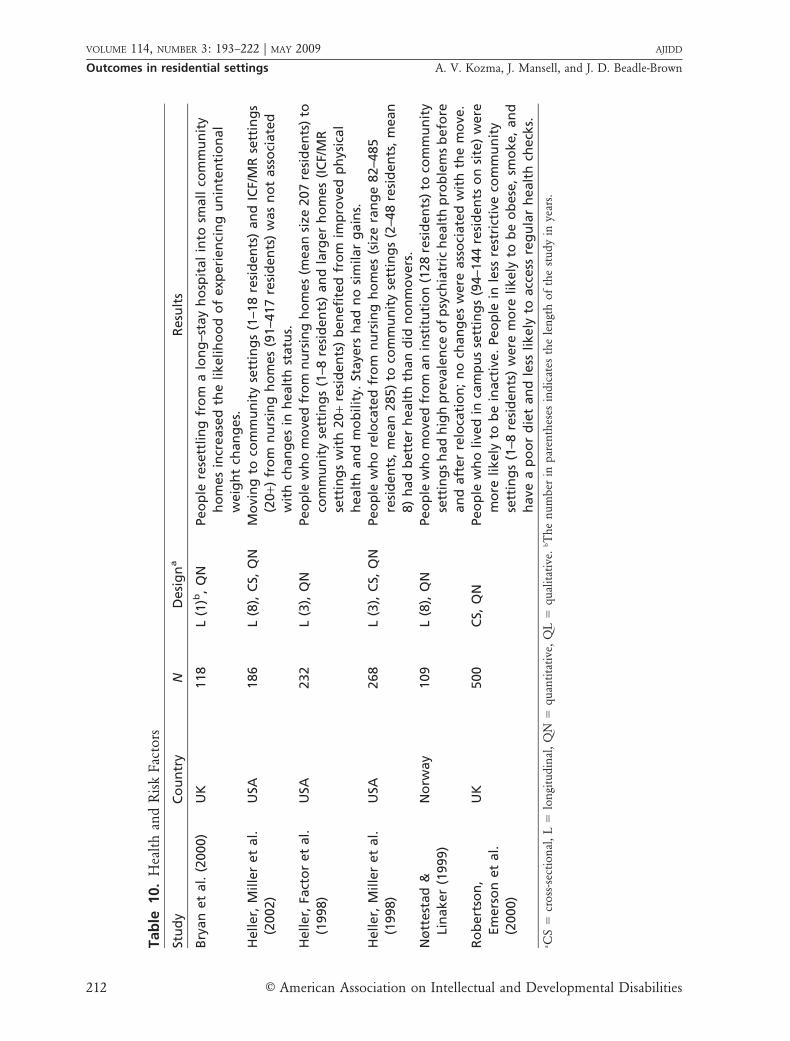
Tab
le10.
Hea
lth
and
Ris
kFac
tors
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Bry
an
et
al.
(2000)
UK
118
L(1
)b,
QN
Peo
ple
rese
ttlin
gfr
om
alo
ng
–sta
yh
osp
ital
into
small
com
mu
nit
y
ho
mes
incr
ease
dth
elikelih
oo
do
fexp
eri
en
cin
gu
nin
ten
tio
nal
weig
ht
chan
ges.
Heller,
Mille
ret
al.
(2002)
USA
186
L(8
),C
S,Q
NM
ovi
ng
toco
mm
un
ity
sett
ing
s(1
–18
resi
den
ts)
an
dIC
F/M
Rse
ttin
gs
(20
+)fr
om
nu
rsin
gh
om
es
(91–4
17
resi
den
ts)
was
no
tass
oci
ate
d
wit
hch
an
ges
inh
ealt
hst
atu
s.
Heller,
Fact
or
et
al.
(1998)
USA
232
L(3
),Q
NPeo
ple
wh
om
ove
dfr
om
nu
rsin
gh
om
es
(mean
size
207
resi
den
ts)
to
com
mu
nit
yse
ttin
gs
(1–8
resi
den
ts)
an
dla
rger
ho
mes
(IC
F/M
R
sett
ing
sw
ith
20
+re
sid
en
ts)
ben
efi
ted
fro
mim
pro
ved
ph
ysic
al
healt
han
dm
ob
ilit
y.St
aye
rsh
ad
no
sim
ilar
gain
s.
Heller,
Mille
ret
al.
(1998)
USA
268
L(3
),C
S,Q
NPeo
ple
wh
ore
loca
ted
fro
mn
urs
ing
ho
mes
(siz
era
ng
e82–4
85
resi
den
ts,
mean
285)
toco
mm
un
ity
sett
ing
s(2
–48
resi
den
ts,
mean
8)
had
bett
er
healt
hth
an
did
no
nm
ove
rs.
Nø
ttest
ad
&
Lin
aker
(1999)
No
rway
109
L(8
),Q
NPeo
ple
wh
om
ove
dfr
om
an
inst
itu
tio
n(1
28
resi
den
ts)
toco
mm
un
ity
sett
ing
sh
ad
hig
hp
reva
len
ceo
fp
sych
iatr
ich
ealt
hp
rob
lem
sb
efo
re
an
daft
er
relo
cati
on
;n
och
an
ges
were
ass
oci
ate
dw
ith
the
mo
ve.
Ro
bert
son
,
Em
ers
on
et
al.
(2000)
UK
500
CS,
QN
Peo
ple
wh
olive
din
cam
pu
sse
ttin
gs
(94–1
44
resi
den
tso
nsi
te)
were
mo
relikely
tob
ein
act
ive.
Peo
ple
inle
ssre
stri
ctiv
eco
mm
un
ity
sett
ing
s(1
–8re
sid
en
ts)
were
mo
relikely
tob
eo
bese
,sm
oke,
an
d
have
ap
oo
rd
iet
an
dle
sslikely
toacc
ess
reg
ula
rh
ealt
hch
eck
s.aC
S5
cro
ss-s
ecti
on
al,
L5
lon
gitu
din
al,
QN
5q
uan
tita
tive
,Q
L5
qu
alit
ativ
e.bT
he
nu
mb
erin
par
enth
eses
ind
icat
esth
ele
ngt
ho
fth
est
ud
yin
year
s.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
212 E American Association on Intellectual and Developmental Disabilities

Variability of outcomes. Although people gen-erally have a better life in the community,research continues to highlight disparities withinthe same type of living arrangement. These areparticularly salient in the domains of CommunityParticipation, Social Networks, and Self-Determi-nation. There are two main patterns of variability:variations in the outcomes associated with thecharacteristics of service users, and those associ-ated with the characteristics of the services.
Positive outcomes are generally associatedwith better adaptive skills and abilities, and peoplewith high or complex support needs, includingchallenging behaviors, are at greater risk ofexperiencing poorer outcomes in communityservices. The provision of ordinary environmentsis not enough to achieve quality and positiveoutcomes in community services (Mansell, Felce,Jenkins, de Kock, & Toogood, 1987). Felce (1998)argued that three factors are necessary to createreal opportunities for people with more severedisabilities in community settings: available activ-ity, available personal support, and effective assis-tance. Mansell et al. (2003) found that, among arange of organizational and staff variables, adap-tive behavior and care practices were the onlyfactors predictive of engagement in meaningfulactivities in community settings.
The variability of outcomes in communityservices might threaten the consensus supportingdeinstitutionalization and community living pol-icies by removing the evidence that communityservices are better for everyone (Mansell, 2006).Recent debates on the worth of clustered arrange-ments seem to be evidence of this (Bigby, 2004;Cummins & Lau, 2004; Emerson, 2004a).
Countries that implemented deinstitutional-ization now face the challenge of strengtheningthe implementation of community living. Thisrequires more than the adoption of certainresidential arrangements (Bigby, 2004). Evaluationresearch in these countries can be used to identifyfactors associated with positive outcomes andgood practices in community living.
Three domains where community services do notperform better. Results also show that there arethree outcome domains where community servic-es might not do better than institutions: Chal-lenging Behavior, Psychotropic Medication, andMortality. Challenging behavior has long beenshown not to be directly linked to communityliving (Emerson & Hatton, 1994; Kim, 2001).Many challenging behaviors are a response toT
ab
le11.
Ris
ksin
the
Com
mun
ity
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Em
ers
on
et
al.
(2000b
)
UK
500
CS,
QN
Peo
ple
inin
ten
tio
nalco
mm
un
itie
s(2
8–1
79
resi
den
tso
nsi
te)
were
rela
tive
lyle
ss
exp
ose
dto
crim
ean
d(v
erb
al)
ab
use
than
were
peo
ple
inco
mm
un
ity
(1–8
resi
den
ts)
or
cam
pu
sse
ttin
gs
(94–1
44
resi
den
tso
nsi
te).
Co
mm
un
ity
sett
ing
s
were
safe
rin
term
so
facc
iden
ts.
Em
ers
on
et
al.
(2001)
UK
281
CS,
QN
Peo
ple
insu
pp
ort
ed
livi
ng
(1–3
resi
den
ts)
arr
an
gem
en
tsw
ere
perc
eiv
ed
tob
eat
hig
her
risk
of
ab
use
than
were
peo
ple
insm
all
gro
up
ho
mes
(1–3
resi
den
ts)
or
larg
er
gro
up
ho
mes
(4–6
resi
den
ts).
Stan
clif
fe&
Kean
e(2
000)
Au
stra
lia
54
CS,
QN
No
dif
fere
nce
inth
ep
erc
eiv
ed
safe
tyo
fp
eo
ple
inse
mi-
ind
ep
en
den
tlivi
ng
arr
an
gem
en
ts(1
–4p
eo
ple
livi
ng
tog
eth
er)
an
dp
eo
ple
livi
ng
ing
rou
ph
om
es
(3–7
resi
den
ts).
aC
S5
cro
ss–s
ecti
on
al,
L5
lon
gitu
din
al,
QN
5q
uan
tita
tive
,Q
L5
qu
alit
ativ
e.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
E American Association on Intellectual and Developmental Disabilities 213

Tab
le12.
Mo
rtal
ity
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Co
nro
y&
Ad
ler
(1998)
USA
1,1
54
L(8
)b,
QN
Decr
ease
dm
ort
ality
was
ass
oci
ate
dw
ith
the
rese
ttle
men
to
fth
e
resi
den
ts(1
,154)
of
an
inst
itu
tio
n(1
,154
resi
den
ts)
inco
mm
un
ity
sett
ing
s.
Lerm
an
et
al.
(2003)
USA
300
L(7
),Q
NR
ese
ttle
men
tfr
om
inst
itu
tio
ns
toco
mm
un
ity
sett
ing
sw
as
no
t
ass
oci
ate
dw
ith
incr
ease
dri
sko
fm
ort
ality
.
O’B
rien
&Zah
ari
a
(1998)
USA
6,8
10
L(5
),C
S,Q
NR
ese
ttle
men
tfr
om
inst
itu
tio
ns
toco
mm
un
ity
sett
ing
sw
as
no
t
ass
oci
ate
dw
ith
incr
ease
dri
sko
fm
ort
ality
.M
ort
ality
rate
sin
com
mu
nit
yfa
ciliti
es
were
decl
inin
g.
Read
(2004)
UK
111
L(1
.5),
QN
Hig
her
mo
rtali
tyaft
er
relo
cati
on
fro
mh
osp
ital
toco
mm
un
ity
sett
ing
s
was
no
tass
oci
ate
dw
ith
serv
ice
fact
ors
.
Shave
lle
&St
rau
ss
(1999)
USA
1,8
12
L(1
),C
S,Q
NU
pd
ate
of
the
1998
stu
dy
by
Stra
uss
,Sh
ave
lle
et
al.
Ag
ain
fou
nd
gre
ate
r
risk
of
mo
rtality
for
tho
sem
ovi
ng
toco
mm
un
ity
sett
ing
sfr
om
an
inst
itu
tio
nth
an
tho
sest
ayi
ng
.
Shave
lle,
Stra
uss
&
Day
(2005)
USA
1,7
76
L(3
),C
S,Q
NG
reate
rri
sko
fm
ort
ality
was
fou
nd
inco
mm
un
ity
sett
ing
sth
an
in
inst
itu
tio
ns.
Stra
uss
,A
nd
ers
on
et
al.
(1998)
USA
48
CS,
QN
Sim
ilar
cau
ses
of
death
am
on
gin
stit
uti
on
al
an
dco
mm
un
ity
resi
den
ts.
Stra
uss
,K
ast
ner
et
al.
(1998)
USA
22,5
76
L(1
0),
CS,
QN
Ris
k–f
act
or
ad
just
ed
mo
rtality
was
fou
nd
tob
eh
igh
er
inco
mm
un
ity
sett
ing
sth
an
inin
stit
uti
on
s.
Stra
uss
,Sh
ave
lle,
Bau
meis
ter
&
An
ders
on
(1998)
USA
1,8
78
L(3
),C
S,Q
NG
reate
rri
sko
fm
ort
ality
was
ass
oci
ate
dw
ith
rese
ttle
men
tfr
om
inst
itu
tio
ns
inco
mm
un
ity
sett
ing
s.Th
eri
skw
as
hig
her
sho
rtly
aft
er
the
mo
ve.
Stra
uss
,Sh
ave
lle,
An
ders
on
&
Bau
meis
ter
(1998)
USA
520
L(1
4),
CS,
QN
Cert
ain
ext
ern
al
cau
ses
of
death
are
mo
reco
mm
on
inco
mm
un
ity
sett
ing
sth
an
inin
stit
uti
on
san
dvi
ceve
rsa.
aC
S5
cro
ss-s
ecti
on
al,
L5
lon
gitu
din
al,
QN
5q
uan
tita
tive
,Q
L5
qu
alit
ativ
e.bT
he
nu
mb
erin
par
enth
eses
ind
icat
esth
ele
ngt
ho
fth
est
ud
yin
year
s.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
214 E American Association on Intellectual and Developmental Disabilities

Tab
le13.
Use
ran
dFam
ily
Sat
isfa
ctio
n
Stu
dy
Co
un
try
ND
esi
gn
aR
esu
lts
Gre
go
ryet
al.
(2001)
UK
96
CS,
QL
Serv
ice
use
rsexp
ress
ed
hig
ho
vera
llsa
tisf
act
ion
inco
mm
un
ity
ho
mes
(1–8
resi
den
ts),
inte
nti
on
alco
mm
un
itie
s(2
8–1
79
resi
den
ts
on
site
),an
dca
mp
us
sett
ing
s(9
4–1
44
resi
den
tso
nsi
te).
Resi
den
ts
of
inte
nti
on
al
com
mu
nit
ies
were
mo
resa
tisf
ied
wit
hce
rtain
asp
ect
so
fth
eir
live
s.
Heller,
Fact
or
et
al.
(1998)
USA
232
L(3
)b,
QN
Peo
ple
wh
om
ove
dfr
om
nu
rsin
gh
om
es
(mean
size
207
resi
den
ts)
toco
mm
un
ity
sett
ing
s(1
–8re
sid
en
ts)
an
dla
rger
ho
mes
(IC
F/M
R
sett
ing
sw
ith
20
+re
sid
en
ts)
were
mo
resa
tisf
ied
wit
hth
eir
livi
ng
arr
an
gem
en
tan
dlife
styl
eth
an
were
no
nm
ove
rs.
McC
on
key
et
al
(2003)
UK
39,
34
L(5
),Q
L,Q
NSe
rvic
eu
sers
an
dth
eir
fam
ilie
sw
ere
mo
resa
tisf
ied
wit
hco
mm
un
ity
sett
ing
s(2
–36
resi
den
ts)
than
wit
hh
osp
ita
ls.
O’B
rien
(2001)
New
Zeala
nd
46
staff
,22
pare
nts
,9
serv
ice
use
rs
L(9
),Q
LSe
rvic
eu
sers
,fa
milie
s,an
dst
aff
view
ed
relo
cati
on
fro
man
inst
itu
tio
n(6
1re
sid
en
ts)
toco
mm
un
ity
sett
ing
s(5
resi
den
ts)
as
clearl
yp
osi
tive
.
Tø
sseb
ro&
Lun
deb
y(2
006)
No
rway
222,
176
L(1
2),
QN
Fam
ilie
sexp
ress
ed
mo
resa
tisf
act
ion
wit
hco
mm
un
ity
care
than
wit
hin
stit
uti
on
s.Po
siti
veo
pin
ion
rem
ain
ed
stab
le
lon
git
ud
inall
y.
Wals
h,
Lin
eh
an
et
al.
(2001)
UK
,Ir
ela
nd
291
CS,
QN
Fam
ilie
sw
ere
mo
resa
tisf
ied
wit
hcu
rren
tlivi
ng
arr
an
gem
en
ts,
com
mu
nit
yh
om
es
(1–8
resi
den
ts),
inte
nti
on
al
com
mu
nit
ies
(28–
179
resi
den
tso
nsi
te),
an
dca
mp
us
sett
ing
s(9
4–1
44
resi
den
tso
n
site
)th
an
wit
hp
revi
ou
slivi
ng
arr
an
gem
en
ts,
incl
ud
ing
ho
spit
al
pro
visi
on
.aC
S5
cro
ss-s
ecti
on
al,
L5
lon
gitu
din
al,
QN
5q
uan
tita
tive
,Q
L5
qu
alit
ativ
e.bT
he
nu
mb
erin
par
enth
eses
ind
icat
esth
ele
ngt
ho
fth
est
ud
yin
year
s.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
E American Association on Intellectual and Developmental Disabilities 215

demands in the environment. Although institu-tions often are a low-demand environment,community services provide more stimulationand demands. Certain challenging behaviors area predictable response to these environments.There is a wealth of research on interventions forchallenging behavior, but now priority should begiven to put this into practice in services(Emerson, 2001).
Psychotropic medication is closely related tochallenging behaviors. The most common reasonfor the use of such drugs for people withintellectual disabilities is the management ofchallenging behaviors, even though effectivenessis questionable (Matson et al., 2000). Investigatorshave suggested that community service providersare not well equipped to deal with individualswho have challenging behaviors that then leads tothe overuse of medication. Research has alsoshown that medication can be substantiallyreduced if adequate clinical and environmentalconditions are put in place in services (Ahmed etal., 2000).
Mortality is generally considered to be anobjective, quantifiable, and comparable measure ofhealth status. Institutions had very high mortalityrates (see, e.g., Rothman & Rothman, 2005). In thelate 1990s, an extensive debate developed in theUnited States as to whether community placementwas associated with higher mortality. Evidence isinconclusive because a large number of studieswere focused on one geographical area (California)and on the same period (1993–1999). This issue hasreceived less attention elsewhere, and in thosestudies that were conducted, researchers founddifferent results. Sutherland et al. suggested thatincreased mortality might be confounded byparticipant characteristics and is not, therefore,necessarily the outcome of the residential setting(Sutherland, Couch, & Iacono, 2002).
Similar experiences across countries. Similarresults were reported from countries with differentwelfare arrangements, socioeconomic context,and service structures, suggesting that the modelof community living for adults with intellectualdisabilities is not bound to certain countries andcan successfully be implemented in differentsituations. The fact that studies come from onlya handful of countries, however, suggests thatthere is a gap in our understanding of residentialsupports for people with intellectual disabilities inother geographical areas and sociocultural, polit-ical, and economic contexts.
Many countries still rely on large institutionsin the provision of services for people withdisabilities (Freyhoff et al., 2004; Mansell et al.,2007). There is resistance towards deinstitutional-ization and community living; policies andpractices change slowly (Freyhoff et al., 2004;Vann & Siska, 2006). The recent ratification of theUnited Nations Convention on the Rights ofPersons With Disabilities by many of thesecountries (for details see http://www.un.org/disabilities/default.asp?id5257), however, mightbring about a new wave of deinstitutionalization.The Convention declares the right of people withdisabilities to live in the community.
For countries that consider implementingdeinstitutionalization and community-living pol-icies, published research provides a strong foun-dation for small-scale community-based arrange-ments. However, there is a need for more researchon the living conditions, including the outcomesof different residential supports in other parts ofthe world.
The importance of normative evaluations. Betteroutcomes found in community services in com-parison to congregate settings are not necessarily‘‘good enough.’’ The evidence suggests that manypeople with intellectual disabilities have poorerlife experiences compared with individuals in thegeneral population. They have limited communi-ty experience, social networks, and choice-makingopportunities. This should encourage researchersto make comparisons with the general population,including gender differences, and uncover thedisadvantages and discrimination people withintellectual disabilities face in our societies.
The process of deinstitutionalization is farfrom complete; institutions still exist in manycountries, and community-based alternatives faceserious challenges of implementation in thecontext of societal and economic changes (Bigby,2004; Emerson, 2004a; Fujiura & Parish, 2007;Mansell, 2006). Continued evidence of therelative merits of small, local services is likely tocontinue to be important. However, In this reviewwe also identify how research is moving beyondsimple structural characteristics of services and isturning to exploration of variations in outcomes,understanding the organizational determinants ofquality services. As large institutions disappear,the policy problem will become one of sustaininggood outcomes for everyone in the community,which will require understanding of the relativecontribution of different factors in different
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
216 E American Association on Intellectual and Developmental Disabilities
circumstances. A further trend is the shift fromcomparison with the past to comparison with thelife experience of individuals in the generalpopulation, including the impact of recent trendsin our societies upon the lives of people withintellectual disabilities. Increasingly, researchersneed to focus on issues and use methods thatapply to the whole population, including peoplewith intellectual disabilities.
References
Ager, A., Myers, F., Kerr, P., Myles, S., & Green,A. (2001). Moving home: Social integrationfor adults with intellectual disabilities reset-tling into community provision. Journal ofApplied Research in Intellectual Disabilities, 14,392–400.
Ahmed, Z., Fraser, W., Kerr, M. P., Kiernan, C.,Emerson, E., Robertson, J., et al. (2000).Reducing antipsychotic medication in peoplewith a learning disability. British Journal ofPsychiatry, 176, 42–46.
Baker, P. A. (2007). Individual and service factorsaffecting deinstitutionalization and commu-nity use of people with intellectual disabili-ties. Journal of Applied Research in IntellectualDisabilities, 20, 105–109.
Beadle-Brown, J., Mansell, J., & Kozma, A. (2007).Deinstitutionalization in intellectual disabili-ties. Current Opinion in Psychiatry, 20, 437–442.
Bigby, C. (2004). But why are these questionsbeing asked? A commentary on Emerson(2004). Journal of Intellectual and DevelopmentalDisability, 29, 202–205.
Bigby, C., & Fyffe, C. (2006). Tensions betweeninstitutional closure and deinstitutionalisa-tion: What can be learned from Victoria’sinstitutional redevelopment? Disability &Society, 21, 567–581.
Bryan, F., Allan, T., & Russell, L. (2000). Themove from a long-stay learning disabilitieshospital to community homes: A com-parison of clients’ nutritional status. Journalof Human Nutrition and Dietetics, 13, 265–270.
Chou, Y. C., Lin, L., Pu, C., Lee, W., & Chang, C.(2008). Outcomes and costs of residentialservices for adults with intellectual disabilitiesin Taiwan: A comparative evaluation. Journalof Applied Research in Intellectual Disabilities, 21,114–125.
Conroy, J., & Adler, M. (1998). Mortality amongPennhurst class members, 1978 to 1989: Abrief report. Mental Retardation, 36, 380–385.
Conroy, J., Spreat, S., Yuskauskas, A., & Elks, M.(2003). The Hissom closure outcomes study:A report on six years of movement tosupported living. Mental Retardation, 41,263–275.
Cummins, R., & Lau, A. (2004). Cluster housingand the freedom of choice: A response toEmerson 2004. Journal of Intellectual &Developmental Disability, 29, 198–201.
Emerson, E. (2001). Challenging behaviour: Analysisand intervention in people with severe learningdisabilities (2nd ed.). Cambridge: CambridgeUniversity Press.
Emerson, E. (2004a). Cluster housing and free-dom of choice: A response to Cummins andLau’s and Bigby’s commentaries. Journal ofIntellectual & Developmental Disability, 29,206–210.
Emerson, E. (2004b). Cluster housing for adultswith intellectual disabilities. Journal of Intellec-tual & Developmental Disability, 29, 187–197.
Emerson, E., & Hatton, C. (1994). Moving out:Relocation from hospital to community. London:Her Majesty’s Stationery Office.
Emerson, E., & McVilly, K. (2004). Friendshipactivities of adults with intellectual disabilitiesin supported accommodation in NorthernEngland. Journal of Applied Research in Intellec-tual Disabilities, 17, 191–197.
Emerson, E., Robertson, J., Gregory, N., Hatton,C., Kessissoglou, S., Hallam, A., et al. (2000a).Treatment and management of challengingbehaviours in residential settings. Journal ofApplied Research in Intellectual Disabilities, 13,197–215.
Emerson, E., Robertson, J., Gregory, N., Hatton,C., Kessissoglou, S., Hallam, A., et al.(2000b). Quality and costs of community-based residential supports, village communi-ties, and residential campuses in the UnitedKingdom. American Journal on Mental Retar-dation, 105, 81–102.
Emerson, E., Robertson, J., Gregory, N., Hatton,C., Kessissoglou, S., Hallam, A., et al. (2001).Quality and costs of supported living resi-dences and group homes in the UnitedKingdom. American Journal on Mental Retar-dation, 106, 401–415.
Emerson, E., Robertson, J., Gregory, N., Kessis-soglou, S., Hatton, C., Hallam, A., et al.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
E American Association on Intellectual and Developmental Disabilities 217

(2000). The quality and costs of community-based residential supports and residentialcampuses for people with severe and complexdisabilities. Journal of Intellectual & Develop-mental Disability, 25, 263–279.
Felce, D. (1998). The determinants of staff andresident activity in residential services forpeople with severe intellectual disability:Moving beyond size, building design, loca-tion and number of staff 1. Journal ofIntellectual & Developmental Disability, 23,103–119.
Felce, D., Lowe, K., Beecham, J., & Hallam, A.(2000). Exploring the relationships betweencosts and quality of services for adults withsevere intellectual disabilities and the mostsevere challenging behaviours in Wales: Amultivariate regression analysis. Journal ofIntellectual & Developmental Disability, 25,307–326.
Felce, D., Lowe, K., Perry, J., Baxter, H., Jones, E.,Hallam, A., et al. (1998). Service support topeople in Wales with severe intellectualdisability and the most severe challengingbehaviours: Processes, outcomes and costs.Journal of Intellectual Disability Research, 42,390–408.
Forrester-Jones, R., Carpenter, J., Coolen-Schrij-ner, P., Cambridge, P., Tate, A., Beecham, J.,et al. (2006). The social networks of peoplewith intellectual disability living in thecommunity 12 years after resettlement fromlong-stay hospitals. Journal of Applied Researchin Intellectual Disabilities, 19, 285–295.
Freyhoff, G., Parker, C., Coue, M., & Greig, N.(Eds.). (2004). Included in society: Resultsand recommendations of the European researchinitiative on community-based residential alter-natives to disabled people. Brussels: InclusionEurope.
Fujiura, G., & Parish, S. (2007). Emerging policychallenges in intellectual disabilities. MentalRetardation and Developmental Disabilities Re-search Reviews, 13, 188–194.
Golding, L., Emerson, E., & Thornton, A. (2005).An evaluation of specialized community-based residential supports for people withchallenging behaviour. Journal of IntellectualDisabilities, 9, 145–154.
Gregory, N., Robertson, J., Kessissoglou, S.,Emerson, E., & Hatton, C. (2001). Factorsassociated with expressed satisfaction amongpeople with intellectual disability receiving
residential supports. Journal of IntellectualDisability Research, 45, 279–291.
Hatton, C. (1998). Whose quality of life is itanyway? Some problems with the emergingquality of life consensus. Mental Retardation,36, 104–115.
Heller, T. (2002). Residential settings and out-comes for individuals with intellectual dis-abilities. Current Opinion in Psychiatry, 15,503–508.
Heller, T., Factor, A. R., Hsieh, K., & Hahn, J. E.(1998). Impact of age and transitions out ofnursing homes for adults with developmentaldisabilities. American Journal on Mental Retar-dation, 103, 236–248.
Heller, T., Miller, A. B., & Factor, A. (1998).Environmental characteristics of nursinghomes and community-based settings, andthe well-being of adults with intellectualdisability. Journal of Intellectual DisabilityResearch, 42, 418–428.
Heller, T., Miller, A. B., & Factor, A. (1999).Autonomy in residential facilities and com-munity functioning of adults with mentalretardation. Mental Retardation, 37, 449–457.
Heller, T., Miller, A. B., & Hsieh, K. (2002). Eight-year follow-up of the impact of environmen-tal characteristics on well-being of adults withdevelopmental disabilities. Mental Retarda-tion, 40, 366–378.
Howe, J., Horner, R. H., & Newton, J. S. (1998).Comparison of supported living and tradi-tional residential services in the state ofOregon. Mental Retardation, 36, 1–11.
Hundert, J., Walton-Allen, N., Vasdev, S., Cope,K., & Summers, J. (2003). A comparison ofstaff–resident interactions with adults withdevelopmental disabilities moving from insti-tutional to community living. Journal onDevelopmental Disabilities, 10, 93–112.
Kearney, C. A., Bergan, K. P., & McKnight, T. J.(1998). Choice availability and persons withmental retardation: A longitudinal and re-gression analysis. Journal of Developmental andPhysical Disabilities, 10, 291–305.
Kim, S. (2001). Behavioural outcomes of dein-stitutionalisation for people with intellectualdisability: A review of US studies conductedbetween 1980 and 1999. Journal of Intellectual& Developmental Disability, 26, 35–50.
Larson, S. A., & Lakin, K. C. (1991). Parentattitudes about residential placement before
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
218 E American Association on Intellectual and Developmental Disabilities

and after deinstitutionalization: A researchsynthesis. Journal of the Association for Personswith Severe Handicaps, 16, 25–38.
Lerman, P., Apgar, D. H., & Jordan, T. (2003).Deinstitutionalization and mortality: Find-ings of a controlled research design in NewJersey. Mental Retardation, 41, 225–236.
Lerman, P., Apgar, D. H., & Jordan, T. (2005).Longitudinal changes in adaptive behaviors ofmovers and stayers: Findings from a con-trolled research design. Mental Retardation, 43,25–42.
Macleod, F. J., Morrison, F., Swanston, M., &Lindsay, W. (2002). Effects of relocation onthe communication and challenging behav-iours of four people with severe learningdisabilities. British Journal of Learning Disabil-ities, 30, 32–37.
Mansell, J. (2006). Deinstitutionalisation andcommunity living: Progress, problems andpriorities. Journal of Intellectual and Develop-mental Disability, 31, 65–76.
Mansell, J., Beadle-Brown, J., & Clegg, S. (2004).The situation of large residential institutionsin Europe. In G. Freyhoff, C. Parker, M.Coue, & N. Greig (Eds.), Included in society:Results and recommendations of the EuropeanResearch Initiative on Community-Based Resi-dential Alternatives to Disabled People. Brussels:Inclusion Europe.
Mansell, J., Beadle-Brown, J., MacDonald, S., &Ashman, B. (2003). Resident involvement inactivity in small community homes forpeople with learning disabilities. Journal ofApplied Research in Intellectual Disabilities, 16,63–74.
Mansell, J., & Ericsson, K. (Eds.). (1996). Deinsti-tutionalization and community living. Intellectualdisability services in Britain, Scandinavia and theUSA. London: Chapman & Hall.
Mansell, J., Felce, D., Jenkins, J., de Kock, U., &Toogood, A. (1987). Developing staffed housingfor people with mental handicaps. TunbridgeWells, Kent, UK: Costello.
Mansell, J., Knapp, M., Beadle-Brown, J., &Beecham, J. (2007). Deinstitutionalisation andcommunity living—Outcomes and costs: Report ofa European study (Vol. 2: main report).Canterbury: Tizard Centre, University ofKent.
Matson, J., Bamburg, J., Mayville, E., Pinkston, J.,Bielecki, J., Kuhn, D., et al. (2000). Psycho-pharmacology and mental retardation: A 10
year review (1990–1999). Research in Develop-mental Disabilities, 21, 263–296.
McConkey, R. (2000). Community care andresettlement. Current Opinion in Psychiatry,13, 491–495.
McConkey, R. (2007). Variations in the socialinclusion of people with intellectual disabil-ities in supported living schemes and residen-tial settings. Journal of Intellectual DisabilityResearch, 51, 207–217.
McConkey, R., McConaghie, J., Mezza, F., &Wilson, J. (2003). Moving from long-stayhospitals: The views of Northern Irish pa-tients and relatives. Journal of IntellectualDisabilities, 7, 78–93.
McConkey, R., Walsh-Gallagher, D., & Sinclair,M. (2005). Social inclusion of people withintellectual disabilities: The impact of placeof residence. Irish Journal of PsychologicalMedicine, 22, 10–14.
McGillvray, J., & McCabe, M. P. (2005). Therelationship between residence and the phar-macological management of challenging be-havior in individuals with intellectual disabil-ity. Journal of Developmental and PhysicalDisabilities, 17, 311–325.
Miller, E., Cooper, S. A., Cook, A., & Petch, A.(2008). Outcomes important to people withintellectual disabilities. Journal of Policy andPractice in Intellectual Disabilities, 5, 150–158.
Myers, F., Agers, A., Kerr, P., & Myles, S. (1998).Outside looking in? Studies of the commu-nity integration of people with learningdisabilities. Disability & Society, 13, 389–413.
Noonan Walsh, P., Emerson, E., Lobb, C.,Hatton, C., Bradley, V., Schalock, R., et al.(2007). Supported accommodation services forpeople with intellectual disabilities: A review ofmodels and instruments used to measure quality oflife in different various settings. Dublin, Ireland:National Disability Authority.
Noonan Walsh, P., Linehan, C., Hillery, J.,Durkan, J., Emerson, E., Hatton, C., et al.(2001). Family views of the quality ofresidential supports. Journal of Applied Researchin Intellectual Disabilities, 14, 292–309.
Nøttestad, J., & Linaker, O. (1999). Psychiatrichealth needs and services before and aftercomplete deinstitutionalisation of peoplewith intellectual disability. Journal of Intellec-tual Disability Research, 43, 523–530.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
E American Association on Intellectual and Developmental Disabilities 219

Nøttestad, J., & Linaker, O. (2002). Predictors forattacks on people after deinstitutionalization.Journal of Intellectual Disability Research, 46,493–502.
Nøttestad, J., & Linaker, O. (2003). Psychotropicdrug use among people with intellectualdisability before and after deinstitutionaliza-tion. Journal of Intellectual Disability Research,47, 464–471.
O’Brien, K. F., & Zaharia, E. S. (1998). Recentmortality patterns in California. Mental Retar-dation, 36, 408–411.
O’Brien, P. (2001). Perceptions of change, advan-tage and quality of life for people withintellectual disability who left a long stayinstitution to live in the community. Journalof Intellectual & Developmental Disability, 26,67–82.
Perry, J., & Felce, D. (2005). Correlation bet-ween subjective and objective measures ofoutcome in staffed community housing.Journal of Intellectual Disability Research, 49,278–287.
Read, S. (2004). Mortality of people with learningdisability following relocation from long-stayhospital to social care. Journal of IntellectualDisabilities, 8, 299–314.
Robertson, J., Emerson, E., Gregory, N., Hatton,C., Kessissoglou, S., & Hallam, A. (2000).Receipt of psychotropic medication by peo-ple with intellectual disability in residentialsettings. Journal of Intellectual Disability Re-search, 44, 666–676.
Robertson, J., Emerson, E., Gregory, N., Hatton,C., Kessissoglou, S., Hallam, A., et al. (2001).Social networks of people with mentalretardation in residential settings. MentalRetardation, 39, 201–214.
Robertson, J., Emerson, E., Gregory, N., Hatton,C., Turner, S., Kessissoglou, S., et al. (2000).Lifestyle related risk factors for poor health inresidential settings for people with intellectualdisabilities. Research in Developmental Disabil-ities, 21, 469–486.
Robertson, J., Emerson, E., Hatton, C., Gregory,N., Kessissoglou, S., Hallam, A., et al. (2001).Environmental opportunities and supportsfor exercising self-determination in commu-nity-based residential settings. Research inDevelopmental Disabilities, 22, 487–502.
Rothman, D. J., & Rothman, S. M. (2005). TheWillowbrook wars. Bringing the mentally disabled
into the community. Somerset, NJ: TransactionPublishers.
Saloviita, T. (2002). Challenging behaviour, andstaff responses to it, in residential environ-ments for people with intellectual disability inFinland. Journal of Intellectual & DevelopmentalDisability, 27, 21–30.
Saloviita, T., & Aberg, M. (2000). Self-determina-tion in hospital, community group homes,and apartments. British Journal of Developmen-tal Disabilities, 46, 23–29.
Shavelle, R., & Strauss, D. (1999). Mortality ofpersons with developmental disabilities aftertransfer into community care: A 1996 update.American Journal on Mental Retardation, 104,143–147.
Shavelle, R., Strauss, D., & Day, S. (2005).Deinstitutionalization in California: Mor-tality of persons with developmental dis-abilities after transfer into community care,1997–1999. Journal of Data Science, 3, 371–380.
Spreat, S., & Conroy, J. (2002). The impact ofdeinstitutionalization on family contact. Re-search in Developmental Disabilities, 23, 202–210.
Spreat, S., Conroy, J., & Fullerton, A. (2005). Acost-benefit analysis of community and insti-tutional placements for persons with mentalretardation in Oklahoma. Research in Develop-mental Disabilities, 26, 17–31.
Spreat, S., Conroy, J., & Rice, D. (1998). Improvequality in nursing homes or institute com-munity placement? Implementation ofOBRA for individuals with mental retarda-tion. Research in Developmental Disabilities, 19,507–518.
Stancliffe, R., & Abery, B. (1997). Longitudinalstudy of deinstitutionalization and the exer-cise of choice. Mental Retardation, 35, 159–169.
Stancliffe, R., Abery, B., & Smith, J. (2000).Personal control and the ecology of commu-nity living settings: Beyond living-unit sizeand type. American Journal on Mental Retar-dation, 105, 431–454.
Stancliffe, R., Emerson, E., & Lakin, C. (2004).Residential supports. In E. Emerson, C.Hatton, T. Thompson, & T. Parmenter(Eds.), Applied research in intellectual disabilities(pp. 459–478). Chichester, W. Sussex, Eng-land: Wiley.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
220 E American Association on Intellectual and Developmental Disabilities

Stancliffe, R., Hayden, M., & Lakin, K. (1999).Interventions for challenging behavior inresidential settings. American Journal on Men-tal Retardation, 104, 364–375.
Stancliffe, R., Hayden, M., Larson, S., & Lakin, K.(2002). Longitudinal study on the adaptiveand challenging behaviors of deinstitutional-ized adults with mental retardation. AmericanJournal on Mental Retardation, 107, 302–320.
Stancliffe, R., Jones, E., Mansell, J., & Lowe, K.(2008). Active support: A critical review andcommentary. Journal of Intellectual & Develop-mental Disability, 33, 196–214.
Stancliffe, R., & Keane, S. (2000). Outcomes andcosts of community living: A matchedcomparison of group homes and semi-inde-pendent living. Journal of Intellectual &Developmental Disability, 25, 281–305.
Stancliffe, R., & Lakin, K. (1998). Analysis ofexpenditures and outcomes of residentialalternatives for persons with developmentaldisabilities. American Journal on Mental Retar-dation, 102, 552–568.
Stancliffe, R., & Lakin, K. (2006). Longitudinalfrequency and stability of family contact ininstitutional and community living. MentalRetardation, 44, 418–429.
Stancliffe, R., Lakin, K., Doljanac, R., Byun, S.,Taub, S., & Chiri, G. (2007). Loneliness andliving arrangements. Intellectual and Develop-mental Disabilities, 45, 380–390.
Strauss, D., Anderson, T. W., Shavelle, R.,Sheridan, F., & Trenkle, S. (1998). Causes ofdeath of persons with developmental disabil-ities: Comparison of institutional and com-munity residents. Mental Retardation, 36, 386–391.
Strauss, D., Kastner, T. A., & Shavelle, R. (1998).Mortality of adults with developmental dis-abilities living in California institutions andcommunity care, 1985–1994. Mental Retarda-tion, 36, 360–371.
Strauss, D., Shavelle, R., Anderson, T. W., &Baumeister, A. (1998). External causes ofdeath among persons with developmentaldisability: The effect of residential placement.American Journal of Epidemiology, 147, 855–862.
Strauss, D., Shavelle, R., Baumeister, A., &Anderson, T. W. (1998). Mortality in personswith developmental disabilities after transferinto community care. American Journal onMental Retardation, 102, 569–581.
Sutherland, G., Couch, M. A., & Iacono, T.(2002). Health issues for adults with develop-mental disability. Research in DevelopmentalDisabilities, 23, 422–445.
Tøssebro, J., & Lundeby, H. (2006). Familyattitudes to deinstitutionalisation: Changesduring and after reform years in a Scandina-vian country. Journal of Intellectual & Develop-mental Disability, 31, 115–119.
Vann, B. H., & Siska, J. (2006). From ‘cage beds’to inclusion: The long road for individualswith intellectual disability in the CzechRepublic. Disability & Society, 21, 425–439.
Verdugo, M., Schalock, R., Keith, K., & Stancliffe,R. (2005). Quality of life and its measure-ment: Important principles and guidelines.Journal of Intellectual Disability Research, 49,707–717.
Walsh, K., & Kastner, T. (2006). The Hissomclosure in Oklahoma: Errors and interpreta-tion problems in Conroy et al. (2003). MentalRetardation, 44, 353–369.
Walsh, K., Kastner, T., & Green, R. (2003). Costcomparisons of community and institutionalresidential settings: Historical review of se-lected research. Mental Retardation, 41, 103–122.
Wehmeyer, M. L., & Bolding, N. (1999). Self-determination across living and workingenvironments: A matched-samples study ofadults with mental retardation. Mental Retar-dation, 37, 353–363.
Young, L. (2000). A preliminary report on theclosure of the Challinor Centre. Journal ofIntellectual & Developmental Disability, 25,119–126.
Young, L. (2001). Closure of the Challinor CentreII: An extended report on 95 individuals after12 months of community living. Journal ofIntellectual & Developmental Disability, 26, 51–66.
Young, L. (2006). Community and cluster centreresidential services for adults with intellectualdisability: Long-term results from an Austra-lian-matched sample. Journal of IntellectualDisability Research, 50, 419–431.
Young, L., & Ashman, A. F. (2004a). Deinstitu-tionalisation in Australia Part II: Results froma long-term study. British Journal of Develop-mental Disabilities, 50, 29–45.
Young, L., & Ashman, A. F. (2004b). Deinstitu-tionalization for older adults with severemental retardation: Results from Australia.
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
E American Association on Intellectual and Developmental Disabilities 221

American Journal on Mental Retardation, 109,397–412.
Young, L., Sigafoos, J., Suttie, J., Ashman, A., &Grevell, P. (1998). Deinstitutionalisation ofpersons with intellectual disabilities: A reviewof Australian studies. Journal of Intellectual &Developmental Disability, 23, 155–170.
Received 11/21/2008, accepted 12/8/2008.Editor-in-charge: Eric Emerson
Correspondence regarding this article should besent to Agnes Kozma, University of Kent, TizardCentre, Canterbury, Kent CT2 7LZ, UnitedKingdom. E-mail: [email protected]
VOLUME 114, NUMBER 3: 193–222 | MAY 2009 AJIDD
Outcomes in residential settings A. V. Kozma, J. Mansell, and J. D. Beadle-Brown
222 E American Association on Intellectual and Developmental Disabilities