operational tolerance: past lessons and future prospects
TRANSCRIPT

REVIEW
Operational Tolerance: Past Lessons and FutureProspectsJosh LevitskyDivision of Hepatology and Comprehensive Transplant Center, Northwestern University FeinbergSchool of Medicine, Chicago, IL
Every liver transplant (LT) center has had patients who either self-discontinue immunosuppressive (IS) therapy or are delib-erately withdrawn due to a research protocol or clinical concern (ie, lymphoproliferative disorder [LPD], overwhelming infec-tion). This is understandable because maintenance IS therapy, particularly calcineurin inhibitors (CNI), is associated withsignificant cost, side effects, and considerable long-term morbidity and mortality. Detrimental effects of IS therapy includeincreased risk of cardiovascular disease, metabolic syndrome, bone loss, opportunistic and community-acquired infections,and malignancy. In fact, LT recipients have among the highest rates of chronic kidney disease and associated mortalityamong all nonkidney solid organ recipients. This mortality is only ameliorated by undergoing a curative kidney transplant,usurping costs and valuable organ resources. The search for improved treatment algorithms includes trial and error CNIdose minimization, the use of alternative IS agents (antimetabolites, mammalian target of rapamycin [mTOR] inhibitors), oreven complete CNI withdrawal. Yet those who are successful in achieving such operational tolerance (no immunosuppres-sion and normal allograft function) are considered lucky. The vast majority of recipients will fail this approach, develop acuterejection or immune-mediated hepatitis, and require resumption of IS therapy. As such, withdrawal of IS following LT is notstandard-of-care, leaving clinicians to currently maintain transplant patients on IS therapy for life. Nonetheless, the long-term complications of all IS therapies highlight the need for strategies to promote immunologic or operational tolerance.Clinically applicable biomarker assays signifying the potential for tolerance as well as tolerogenic IS conditioning are invaria-bly needed if systematic, controlled rather than ‘‘hit or miss’’ approaches to withdrawal are considered. This review will pro-vide an overview of the basic mechanisms of tolerance, particularly in relation to LT, data from previous IS withdrawalprotocols and biomarker studies in tolerant recipients, and a discussion on the prospect of increasing the clinical feasibilityand success of withdrawal. Liver Transpl 17:222-232, 2011. VC 2011 AASLD.
Received October 26, 2010; accepted December 23, 2010.
BASIC MECHANISMS OF TRANSPLANTTOLERANCE
Experimental support for transplant tolerance wasdemonstrated in the early 1950s, when Billinghamand Medawar induced tolerance to skin allografts inmice by injection of allogeneic cells in the neonatal pe-
riod.1-3 Key discoveries from that era led to under-standing the role of the thymus in immune system de-velopment and self-immune and alloimmunetolerance (central tolerance). They also led to the dem-onstration of immunoregulation or deletion/anergy ofautoreactive/alloreactive cells in the circulation (pe-ripheral tolerance). Figure 1 displays the proposed
Abbreviations: APC, antigen-presenting cell; AZA, azathioprine; CD, clusters of differentiation; CNI, calcineurin inhibitor; CyA,cyclosporine A; DDLT, deceased donor liver transplant; FOXP3, forkhead/winged helix transcription factor 3; HCV, hepatitis Cvirus; HLA, human leukocyte antigen; IFN, interferon; IL, interleukin; IS, immunosuppression; LDLT, live donor liver transplant;LPD, lymphoproliferative disorder; LT, liver transplant; MHC, major histocompatibility complex; mTOR, mammalian target ofrapamycin; NK, natural killer; NKT, natural killer T cells; PCD, programmed cell death; PD-1, programmed cell death-1; pDC,plasmacytoid dendritic cell; TAC, tacrolimus; TCR, T cell receptor; TGF-b, transforming growth factor-beta; Th2, T helper 2; Tr1,type 1 T regulatory cell; Treg, T regulatory cell.
Address reprint requests to Josh Levitsky, M.D., M.S., Assistant Professor of Medicine and Surgery, Division of Hepatology and ComprehensiveTransplant Center, Northwestern University Feinberg School of Medicine, 676 North St. Clair Street, Suite 1900, Chicago, IL 60611. Telephone:312-695-9286; FAX: 312-695-0036; E-mail: [email protected]
DOI 10.1002/lt.22265View this article online at wileyonlinelibrary.com.LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
VC 2011 American Association for the Study of Liver Diseases.
LIVER TRANSPLANTATION 17:222-232, 2011
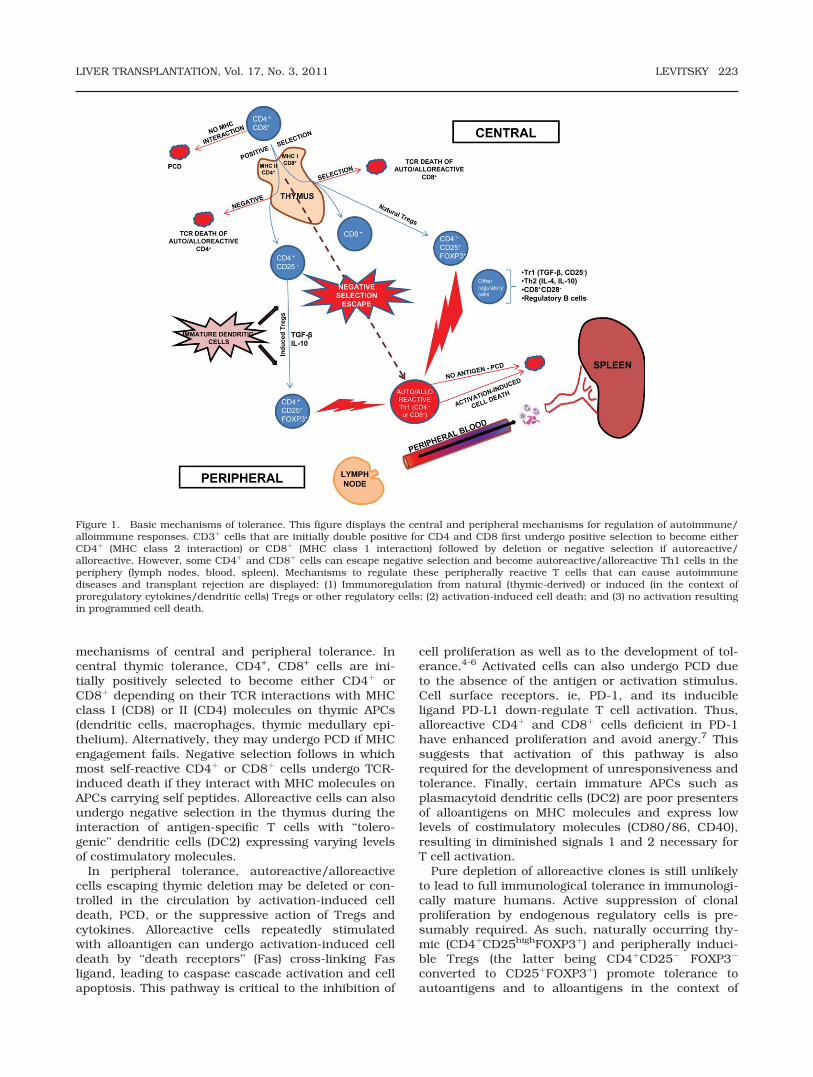
mechanisms of central and peripheral tolerance. Incentral thymic tolerance, CD4+, CD8+ cells are ini-tially positively selected to become either CD4þ orCD8þ depending on their TCR interactions with MHCclass I (CD8) or II (CD4) molecules on thymic APCs(dendritic cells, macrophages, thymic medullary epi-thelium). Alternatively, they may undergo PCD if MHCengagement fails. Negative selection follows in whichmost self-reactive CD4þ or CD8þ cells undergo TCR-induced death if they interact with MHC molecules onAPCs carrying self peptides. Alloreactive cells can alsoundergo negative selection in the thymus during theinteraction of antigen-specific T cells with ‘‘tolero-genic’’ dendritic cells (DC2) expressing varying levelsof costimulatory molecules.
In peripheral tolerance, autoreactive/alloreactivecells escaping thymic deletion may be deleted or con-trolled in the circulation by activation-induced celldeath, PCD, or the suppressive action of Tregs andcytokines. Alloreactive cells repeatedly stimulatedwith alloantigen can undergo activation-induced celldeath by ‘‘death receptors’’ (Fas) cross-linking Fasligand, leading to caspase cascade activation and cellapoptosis. This pathway is critical to the inhibition of
cell proliferation as well as to the development of tol-erance.4-6 Activated cells can also undergo PCD dueto the absence of the antigen or activation stimulus.Cell surface receptors, ie, PD-1, and its inducibleligand PD-L1 down-regulate T cell activation. Thus,alloreactive CD4þ and CD8þ cells deficient in PD-1have enhanced proliferation and avoid anergy.7 Thissuggests that activation of this pathway is alsorequired for the development of unresponsiveness andtolerance. Finally, certain immature APCs such asplasmacytoid dendritic cells (DC2) are poor presentersof alloantigens on MHC molecules and express lowlevels of costimulatory molecules (CD80/86, CD40),resulting in diminished signals 1 and 2 necessary forT cell activation.
Pure depletion of alloreactive clones is still unlikelyto lead to full immunological tolerance in immunologi-cally mature humans. Active suppression of clonalproliferation by endogenous regulatory cells is pre-sumably required. As such, naturally occurring thy-mic (CD4þCD25highFOXP3þ) and peripherally induci-ble Tregs (the latter being CD4þCD25� FOXP3�
converted to CD25þFOXP3þ) promote tolerance toautoantigens and to alloantigens in the context of
Figure 1. Basic mechanisms of tolerance. This figure displays the central and peripheral mechanisms for regulation of autoimmune/alloimmune responses. CD3þ cells that are initially double positive for CD4 and CD8 first undergo positive selection to become eitherCD4þ (MHC class 2 interaction) or CD8þ (MHC class 1 interaction) followed by deletion or negative selection if autoreactive/alloreactive. However, some CD4þ and CD8þ cells can escape negative selection and become autoreactive/alloreactive Th1 cells in theperiphery (lymph nodes, blood, spleen). Mechanisms to regulate these peripherally reactive T cells that can cause autoimmunediseases and transplant rejection are displayed: (1) Immunoregulation from natural (thymic-derived) or induced (in the context ofproregulatory cytokines/dendritic cells) Tregs or other regulatory cells; (2) activation-induced cell death; and (3) no activation resultingin programmed cell death.
LIVER TRANSPLANTATION, Vol. 17, No. 3, 2011 LEVITSKY 223

transplantation.8-10 After TCR engagement,CD4þCD25high Tregs characteristically express an in-tracellular protein FOXP3,11,12 which is critical for themaintenance and function of the major Treg subpopu-lation (CD4þCD25highFOXP3þ). The absence of FOXP3leads to severe autoimmune disease in mice andhumans.13-15 FOXP3 blocks the transcription of T cellactivation molecules such as IL-2 and the expressionof the IL-7 receptor (CD127), the absence of whichcan distinguish Treg cells (CD127low) from effectorand memory T cells (CD127high).16 Following activa-tion, Treg cells are also less sensitive to apoptosisthan cytotoxic effector subsets.17 As alluded to above,the CD4þCD25highFOXP3þ cells are not the only puta-tive Tregs, because other populations (CD25� TGF-b–producing Tr1 cells, IL-10–expressing cells,CD8þCD28� suppressors, ‘‘regulatory’’ B cells) haveall been characterized as immunoregulatory. Thesemechanisms involve a number of cellular interactions,regulatory (IL-4, IL-10, TGF-b) cytokines, specializedchemokine receptors, autocrine/paracrine recruit-ment of more Tregs (‘‘infectious tolerance’’), andimmature dendritic cells (DC2) promoting alloreactivecell anergy and Treg generation.12,18
Although having complexity in cell make-up, trans-plant tolerance is perhaps more simply defined asallospecific immunologic unresponsiveness, eitherdue to deletion of alloreactive T cells (occurring natu-rally or with immunosuppressive therapy) or by activesuppression from allospecific regulatory cells. Table 1lists the immunological criteria of which some or allappear to be important in transplant tolerance.19,20
Immunosuppression appears to play an importantrole in the initial induction and maintenance of tolero-genic mechanisms, particularly early after transplan-tation when alloreactive and inflammatory signals areat their peak. A notable example of this is the poten-tial association of tolerance with lymphodepletionalinduction therapy,21-24 either by depletion of alloreac-tive clones or augmentation of Tregs. This is in con-trast with antitolerogenic mechanisms seen with is-chemia/reperfusion injury and subsequent Toll-likereceptor activation of APCs.25-29 Donor/recipient he-matopoietic microchimerism has been demonstratedin long-term liver and kidney transplant survivorsand postulated to result in reciprocal donor/recipientcell exhaustion (ie, absence of both rejection andgraft-versus-host disease).19,30-34 Controversial, how-
ever, is the actual requirement of chimerism for toler-ance because this may only be a transient phenom-enon.35,36 Also contentious is the role of FOXP3þ
expression in human organ transplant recipients,because FOXP3þ cells are found with rejecting organtransplants. More evidence is needed on the actualfunction of donor-specific and nonspecific FOXP3þ
Tregs coming from and migrating to various tissuecompartments (blood, lymphoid organs, bone marrow,and allograft).
THE LIVER AS A TOLEROGENICORGAN
The liver itself represents a unique ‘‘window’’ to theimmune system and is the most immunoregulatorysolid organ that is transplanted (Fig. 2). It contains ahigh number of extramedullary hematopoietic cells, alarge mass of nonhematopoietic cells (hepatocytes,stellate cells, endothelial cells), and secretes a varietyof proteins (ie, HLA-G) and cytokines with immunore-gulatory effects.37-39 The abundance of residentimmunocytes and APCs appear to be regulatory in
TABLE 1. Immunological Criteria for Transplant Tolerance
Early immune quiescence (ablation of alloreactive effector T cells and inflammatory signals) induced by potentimmunosuppressive therapy and minimization of ischemia/reperfusion injury
Inactivation of immunoreactive clones by an ‘‘exhaustion’’ process using reduced dose maintenance or tolerogenicimmunosuppression
State of regulatory (IL-10, TGF-b) versus inflammatory (IL-6, IFN-c) cytokine production and gene/protein expressionThe establishment of a myeloid and lymphoid chimeric state by donor-derived, blood-forming elementsExpansion of regulatory T cells (CD4þCD25high FOXP3þ) and immature dendritic cells to favor immunoregulation overreactivity
Immunogenetic similarity
Figure 2. Putative components of liver immunoregulation. Thisfigure illustrates clinical and immunologic evidence supportingliver transplant immunoregulation. The significant contributionfrom resident regulatory cells and cytokines is likely a majorfactor leading to low rejection rates and IS requirements.
224 LEVITSKY LIVER TRANSPLANTATION, March 2011

nature and protective of graft injury and rejection,although in some cases can lead to early graft-versus-host disease.37 These cells might even engulf (‘‘suici-dal emperipolesis’’) recipient allospecific cytotoxic Tcells as one of the pathways of liver immunoregula-tion.40 Donor-specific immunoregulatory effects, clo-nal deletion of alloreactive immunocytes, dilution orinhibition of alloantibody, and mixed donor-recipienthematopoietic microchimerism are also putative com-ponents of liver immunoregulation.41-48 Moreover, theliver graft itself may itself be considered a source ofpersistent tolerogen in contrast to being a target ofimmune destruction.
Consistent with these mechanisms and distinctfrom other solid organ recipients, LT recipients dem-onstrate a greater ability to withstand lower IS dosesand have a propensity toward tolerance over alloreac-tivity. This is evident clinically by the insignificance ofHLA matching, minimal relevance of a single rejectionepisode (except in HCV-positive recipients), the lowincidence of acute/chronic rejection, the reduceddegree of induction/maintenance IS required, and theimmunological protection conferred by the liver onother organs in combined transplants (liver–kidney,liver–intestine). That being said, these basic mecha-nisms and clinical phenomena cannot be generalizedto all LT recipients, and the reasons why minimizedor no IS is achievable in only some recipients havenot been sufficiently elucidated.
IMMUNOSUPPRESSION WITHDRAWAL:LEARNING FROM THE PAST
Although immunological and clinical evidence exist forthe development of LT tolerance, complete withdrawalof IS (mainly CNI) maintenance therapy is only suc-cessful in �20% of recipients in prospective studies todate (Table 2; �5 patients/study).35,49-61 This low per-centage is likely due to known CNI mechanisms inhib-
iting immunoregulation and the lack of available, well-defined immune monitoring to detect immunoregula-tion or unresponsive states. This inability to immuno-logically predict or achieve successful withdrawal hascompelled clinicians to maintain long-term CNIs andother IS at recommended doses, despite the toxicitiesand morbidity. However, the failures and successesfrom the previous studies present useful lessons onspecific patient characteristics (primary liver disease,time from transplant, type of transplant) to guidemore effective approaches to withdrawal.
The vast majority of withdrawal studies have onlyfocused on the nonimmune, non–viral infected popu-lation. Most studies excluded patients with a historyof immune-mediated diseases, ie, autoimmune hepati-tis, primary biliary cirrhosis, and primary sclerosingcholangitis, or with a more significant or recent his-tory of rejection. Yet, the negative impact of chronic IStherapy in this population may be higher, becausemany are empirically treated with long-term double ortriple therapy to avoid rejection. Although it makesclinical sense to not include these ‘‘immunoreactive’’patients in tolerance trials, it might be beneficial todetermine clinical phenotypes, graft histology, or bio-markers associated with a greater success of IS mini-mization (proper tolerance) rather than complete with-drawal. Approaches involving more aggressiveimmune manipulation (myeloablation plus stem celltherapy) have not been studied in this population butwarrant consideration.
Only one study has examined the effect of IS with-drawal in HCV-positive recipients, an important groupto consider given the known negative impact of IS onHCV recurrence and fibrosis progression.57 This studydemonstrated improvement in fibrosis after with-drawal, similar to that seen with successful post-LTIFN therapy.62,63 However, this preliminary study hasnot been replicated, and a follow-up study almost 3years later did not show histological differences
TABLE 2. Elective Withdrawal Studies
Center (No. of Patients)
Adult or
Pediatric
DDLT
or LDLT Baseline IS
Years from LT
to Tapering Tolerant Failure*
Pittsburgh (n ¼ 95) Both DDLT TAC or CyA þ AZA Mean, 8.4 6 4.7 18 (18.9%) 40 (42.1%)London (n ¼ 18) Adult DDLT CyA, AZA, prednisolone Median, 7 (5-11) 5 (27.7%) 13 (72.2%)Kyoto (n ¼ 115) Pediatric LDLT TAC >2 49 (42.6%) 20 (17.4%)Murcia (n¼ 9) Adult DDLT CyA Median, 5.1 (2-9) 3 (33.3%) 6 (66.6%)Rome (n ¼ 34, only HCV) Adult DDLT CyA Mean, 5.3 6 1.7 8 (23.5%) 26 (76.5%)New Orleans (n ¼ 18) Adult DDLT TAC >0.5 1 (5.6%) 17 (94.4%)Winnipeg (n ¼ 26)† Adult DDLT CyA þ AZA or
prednisoloneMean, 4.3 6 1.1 8 (30.8%) 18 (69.2%)
Miami (n ¼ 104)‡ Adult DDLT TAC or CyA Median, 4 (3.6-4.6) 23 (22.1%) 81 (61.5%)Barcelona (n ¼ 102) Adult DDLT TAC or CyA Median, 7.9 40 (77.9%) 62 (60.0%)
*Either due to rejection, immune-mediated hepatitis, noncompliance, resumption of immunosuppression, diseaserecurrence, or other. The remaining patients were deemed ‘‘weaning in progress’’ in all studies.
†Randomized controlled trial of ursodeoxycholic acid given at 15 mg/kg/day versus placebo in withdrawing patients; 3patients developed autoimmune hepatitis recurrence after withdrawal.
‡45 received donor bone marrow cell infusions; 59 did not.
LIVER TRANSPLANTATION, Vol. 17, No. 3, 2011 LEVITSKY 225

between HCV-positive transplant recipients in whomIS was withdrawn and those in whom it was main-tained.64 In addition, the development of graft rejec-tion associated with withdrawal of IS in HCV-positivepatients may have an opposite effect on HCV recur-rence, fibrosis progression, and long-term graft sur-vival. To address these concerns, larger prospectivestudies including HCV recipients in withdrawal inconjunction with specific immunological monitoringare currently being conducted.65,66
The length of time between transplantation and ISwithdrawal might also affect the success and clinicalbenefit of withdrawal. Many of the studies in Table 2excluded patients who were within 3 years of LT, so itis difficult to compare the pros and cons of early ver-sus late withdrawal. Newer trials in IS withdrawalhave enrolled stable LT recipients for withdrawal asearly as one year post-LT with or without inductiontherapy,65,67 with one study showing high rates ofrejection following a protocol of antithymocyte globu-lin induction and early TAC weaning.67 A more recentstudy, not yet formally published, demonstratedgreater success when patients were withdrawn late(>5 years) after LT.49 Although IS withdrawal may beintuitively more successful when done later after LT,the potential for IS adverse effects is greater the lon-ger patients are maintained on IS. Overall, at thisjuncture, there does not seem to be clear linear corre-lation between withdrawal success and time fromtransplantation. Thus, strategies designed to ‘‘tolerize’’patients and withdraw IS earlier after LT may havemore beneficial impact on IS-related morbidity.
In regard to type of transplant, ie, LDLT versusDDLT or pediatric versus adult, the Kyoto group dem-onstrated a high IS withdrawal success rate (42.6%)fairly early after pediatric LDLT.55,56 Other case serieshave reported IS withdrawal in recipients of simulta-neous or staggered donor hematopoietic cell trans-plantation and LDLT.51,68-71 The success of theseapproaches may be in part due to greater HLA similar-ities between the related donor/recipient pairs or theavoidance of significant ischemia/reperfusion injuryby the nature of the procedure. However, other thanthe Kyoto report, no firm clinical data are available tosuggest that LDLT recipients require less IS or can bewithdrawn more easily compared to DDLT. In addi-tion, no head-to-head trials comparing IS withdrawalin LDLT versus DDLT, with or without stem cell ther-apy, have been or are currently being performed, butcertainly are of great interest and potential.
Finally, the issue of IS withdrawal in children is im-portant given the negative, life-long impact of IS ther-apy in this population. Only the Pittsburgh and Kyotogroups have a large enough prospective experience inchildren, succeeding in achieving tolerance in 22(34%) and 49 (43%) recipients, respectively.54,55
Favorable factors for success include longer time fromtransplantation, achievement of monotherapy, trans-plantation for nonimmune diseases, the presence ofLPD, and younger age.72,73 Of unclear importance isthe presence of fibrosis and decreased bile duct size
on postwithdrawal protocol biopsies of ‘‘operationallytolerant’’ pediatric recipients.60 More data on long-term histology of withdrawn patients will be availablesoon to clarify the incidence, etiology, and significanceof such graft abnormalities as well as other clinicaloutcomes.74
SPONTANEOUSLY TOLERANTRECIPIENTS: WHAT HAVE THESE‘‘LUCKY’’ PATIENTS TAUGHT US?
There have been reports of successful IS discontinua-tion in the setting of LPD53,75 or by self-withdrawalwithout the knowledge of the center. Other than inresearch protocols or life-threatening infections, LPDis perhaps the only situation in which there is generalclinical consensus to intentionally taper or withdrawIS, usually on a temporary basis until the completionof chemotherapy. The self-withdrawal group, althoughfew and far between, represents fortunate patientswho ‘‘escaped’’ rejection. In turn, transplant research-ers in some cases have obtained samples from thesespontaneously or research protocol tolerant patientsand their ‘‘tolerant phenotype’’ has allowed testing ofin vitro bioassays as putative in vivo markers of toler-ance. The major candidates are blood immunopheno-typic assays (CD4þCD25highFOXP3þ cells, and dendri-tic and Vd1/Vd2 cell ratios), cytokine gene profiles(NK, cd T cell, CD8þ receptor genes) and genomicmicroarrays, although donor-specific assessmentsand immune characterization of allograft tissue needto be more robustly developed as specific identifiers oftolerance (Table 3).
Operationally tolerant recipients appear to have dif-ferent cellular immunophenotypic profiles comparedto healthy volunteers and recipients maintaining IS orexperiencing rejection. Studies have shown thatoperationally tolerant pediatric and adult LT recipi-ents have significantly higher peripheral bloodCD4þCD25high T cells and cd T cells (Vd1/Vd2 ratio)compared to nontolerant recipients or healthy individ-uals.61,76 In a subset, the suppressive properties ofthe isolated CD4þCD25þ cells were donor-antigenspecific.60 Blood FOXP3 transcripts in conjunctionwith CD4þCD25high T cells were observed in higherfrequency in LT recipients who underwent successfulwithdrawal versus those who developed rejection.77
Other cell populations observed to be higher in with-drawing and fully tolerant recipients include plasma-cytoid ‘‘regulatory’’ dendritic cells (DC2 orCD11c�CD123high), particularly the ratio of DC2:DC1(DC1 or CD11cþCD123�/loþ) and B (CD19þ) cells, thelatter also seen in tolerant kidney transplant recipi-ents.61,78-80 Interestingly, in the allograft specifically,FOXP3 expression and CD4þCD25high T cells increasein both tolerant and rejecting liver81,83 and otherorgan recipients.84,85 The presence of graft FOXP3þ
cells in rejection likely represents either activatedalloreactive T cells or regulatory T cells homing to thegraft to control immune responses. Thus, even with
226 LEVITSKY LIVER TRANSPLANTATION, March 2011

available histological analysis and a ‘‘window’’ to thegraft itself, immunohistochemical characterization ofgraft immunocytes may be less useful and predictivethan peripheral blood analyses that have shown moreconsistent results.
There have also been reports of cytokine, genomic,and HLA signatures present in tolerant patients thatmight predict the ability to achieve tolerance prior toweaning.49,76,86-92 An early study demonstrated thatpediatric patients on minimal or no IS had low tumornecrosis factor-a and high IL-10 gene polymorphismprofiles compared to control patients on maintenanceIS.93 More recently, gene expression profiling of opera-tionally tolerant liver recipients demonstrated aunique signature involving receptors for cd T cells andNK cells, as well as proteins involved in cell prolifera-tion arrest.76 This correlated with increased numbersof circulating putative Tregs (CD4þCD25þ) and cd Tcells (mainly the Vd1þ subset). The same group foundsimilar gene (NK, cd, and CD8þ cells) and immuno-phenotypic (CD4þCD25þ, cd T cells of the Vd1þ sub-set) signatures in LT recipients who were successfullywithdrawn from IS in an actual weaning protocol com-pared to healthy controls and recipients who rejectedwith weaning.86 This signature appears to be specificto tolerant LT recipients because a different B cell–related signature has been demonstrated in tolerantkidney recipients.94,80 Whether microchimerism playsan active role in immune quiescence may depend onthe characterization of the chimeric immunocyte sub-sets and perhaps such genomic and transcriptional
predilections. Finally, levels of soluble HLA-G havebeen shown to be significantly higher in tolerant pedi-atric recipients compared to those with rejection orstable on IS therapy.95 Although prospective studiesare currently ongoing,49 sequential data are not yetpublished to directly support the ability of these‘‘tolerance’’ assays to predict successful withdrawal,nor are they yet commercially available in clinicalsettings.
HOW AND WHEN WILL WITHDRAWALBECOME A REALISTIC OPTION?
Currently, few if any transplant clinicians would con-sider IS withdrawal a feasible option. Without predic-tive tools or clinical guidance, the risks currently out-weigh the small potential for success. The key for thefuture is determining which clinical and immunologi-cal characteristics identify the population most likelyto succeed, such that withdrawal would only be con-sidered in such a suitable group. Conversely, thosewith unfavorable characteristics and bioassays wouldnot be considered for IS withdrawal and thus avoidthe accompanying risk of rejection and graft loss. For-tunately, we are closer to having predictive immuno-logical and genetic assays (Table 3) that might be clin-ically serviceable. In addition, the tolerogenic profilesof IS agents, well described in vitro, need to be clari-fied in vivo to determine optimal IS protocols thatfacilitate tolerance. Although controversial, the tolero-genic potential may be greatest with certain induction(thymoglobulin, alemtuzumab) and maintenance(mTOR inhibitors) agents and the least with CNIs andIL-2 receptor (anti-CD25) agents. The next section willfocus on how different IS therapies and bioassaysmight allow for expansion of the number of tolerantrecipients.
Induction Immunosuppression Selection
A more aggressive approach would be to use up-frontlymphodepleting induction therapy to eliminate earlydetrimental immune signals and promote clonal dele-tion of effector cells. Ischemia/reperfusion injuryelaborates proinflammatory innate cytokines (tumornecrosis factor-a) that activate Toll-like receptors, pro-motes alloantigen presentation by APCs, and inhibitsimmunoregulation. Reduction in ischemia/reperfu-sion injury (ie, LDLT) in combination with inductiontherapy might putatively alter the balance towardimmunoregulation over alloreactivity. Studies havedemonstrated the possible regulatory effects of anti-thymocyte globulin and the anti-CD52 antibody alem-tuzumab in deleting alloreactive effector cells whilepreserving regulatory cells and their components.96
However, the limited existing data suggest thatinduction approaches may not increase the success ofIS withdrawal and perhaps rather favor a state inwhich minimized IS doses can be achieved.20,58 Morerecently, an induction approach (antithymocyte globu-lin; ATG-Fresenius) in conjunction with early IS (TAC)
TABLE 3. Candidate Liver Transplant Tolerance Assays
More Definitive
� Peripheral blood immunophenotyping– CD4þCD25highFOXP3þ cells– DC2:DC1 ratio– cd T cells (Vd1/Vd2 ratio)
� Genomic signatures– NK cell, cd T cell, CD8þ cell receptors– Cytokine gene polymorphisms (TNF-a, IL-10)
� Soluble HLA-GLess Definitive
� Allograft immunophenotyping– Immunohistochemical staining and in vitroculture for Treg:Teff ratio
– FOXP3 mRNA� Donor-specific approaches
– Mixed lymphocyte reaction (proliferation,CFSE labeling, Treg MLR)
– Cell-mediated lymphotoxicity– ELISPOT (Th1 and Th2 cytokines)– Delayed type hypersensitivity (Trans-vivo)– Donor-specific antibodies and HLA typing
� Detection of hematopoietic chimerism
The more definitive assays have been validated inoperationally tolerant liver transplant recipients. The lessdefinitive assays are either inconclusive or inadequatelystudied in clinical tolerance protocols.
LIVER TRANSPLANTATION, Vol. 17, No. 3, 2011 LEVITSKY 227

withdrawal was associated with a high rate of rejec-tion and actually did not allow for significant minimi-zation of TAC.67 Also of concern is the presence ofmemory effector cells that are more resistant to lym-phodepletional therapy. If possible, elimination of do-nor-specific memory cells and preservation of nonspe-cific memory responses might promote tolerance andmaintain important immune surveillance againstpathogens and tumor cells, respectively. It is alsouncertain if costimulatory blockade molecules (cyto-toxic T lymphocyte antigen 4 [CTLA-4] immunoglobu-lin) or IL-2 receptor inhibitors being developed or al-ready in practice have pro- or antitolerogenic effects,although negative effects are more likely becauseTregs express CTLA-4 and respond to IL-2 for prolifer-ation. In summary, the putative immunoregulatoryproperties of lymphodepletional or other inductionapproaches do not, as of yet, appear to translate clini-cally in facilitating IS withdrawal in LT recipients.Randomized trials comparing induction versus nonin-duction tolerance protocols in LT recipients areneeded to clarify the overall risks and benefits of theseapproaches.
Maintenance Immunosuppression Selection
Previous nonclinical studies have demonstrated dif-ferences in immunoregulatory properties of mainte-nance IS agents. The CNI agents inhibit the calci-neurin-driven pathways of IL-2 and IFN-ctranscription resulting in inhibition of T cell activa-tion. However, these same CNI mechanisms are coun-ter-regulatory, because IL-2 is critical for FOXP3expression and the survival and proliferation ofCD4þCD25highFOXP3þ Tregs.97-99 In addition, CNIsdo not affect the maturation of dendritic cells, whichpresent alloantigen and produce costimulatory mole-cules that activate effectors and inhibit Treg genera-tion.97,98 Conversely, whereas not yet clinically estab-lished, the mTOR inhibitors (rapamycin, everolimus)and possibly the antimetabolites (mycophenolic acid)suppress alloreactive T cells but also enhance Treggeneration in vitro. Unlike CNIs, these agents do notinhibit initial IL-2 transcription that is important forthe maintenance and function of Tregs. When admin-istered alone or with costimulatory blockade/IL-10 invitro, they inhibit the maturation and function of IFN-c–producing T helper 1 (Th1) cells and dendritic cells,and increase the percentage of CD4þCD25high FOXP3þ
Tregs and CD8þCD28� suppressor cells.100-102 Rapa-mycin also appears to promote regulatory costimulatorymolecules.103
In the clinical setting, limited data have shown thatliver and kidney transplant recipients treated withmTOR agents have higher percentages of phenotypicTregs versus those recipients on CNI therapy.104-107
As such, one of the possible reasons for the low suc-cess rates in prior weaning studies could be that themajority of patients were withdrawn directly from CNItherapy that may have inhibited regulatory mecha-nisms. If conversion from CNI to putative ‘‘tolerogenic’’
IS therapies such as rapamycin is found to enhancethe generation of Tregs and other tolerance bio-markers, this might be an interventional step to facili-tate the ability to increase the number of tolerantpatients. However, without supportive clinical with-drawal data, this approach is purely theoretical andshould be rigorously tested in prospective fashionagainst the standard agents. In addition, it is notknown if these IS-influenced Tregs are functionallyregulatory in vivo or regulate donor-specific allores-ponses in the peripheral blood as well as the forma-tive (bone marrow) and target (liver) organs.
Use of Biomarkers
The ultimate goal would be to demonstrate persistentrecipient hyporesponsiveness or unresponsiveness tothe donor. This may now be more feasible with donor-specific immune monitoring assays90,91 to moreclearly detect states favoring alloimmune quiescenceover reactivity, ie, whether they are due to partial clo-nal deletion/exhaustion19,20 or an active regulatoryprocess.108 These functional assays (mixed lympho-cyte reactions, ELISPOT, Trans-vivo delayed-typehypersensitivity, cell-mediated lympholysis) mightthen be used to monitor patients before, during, andafter IS minimization and withdrawal, allowing contin-uation of withdrawal in those with favorable donor-specific responses and avoiding such interventions inthose with immunoreactivity. In the absence of donor-specific assays, nonspecific genomic (NK, cd T cellgenes), immunophenotypic (CD4þCD25highFOXP3þ, cd[Vd1þ] T cells), and HLA (soluble HLA-G) signaturesdescribed previously in this review (Table 3) appear tobe ready for testing as tolerance predictors in pro-spective studies. Ideally, along with standard liver his-tology, they could be used to determine suitable andunsuitable candidates for weaning. For example, outof 100 patients, 30 might speculatively have thegenomic and immunophenotypic tolerance signaturesprior to weaning, of which perhaps 20 will wean suc-cessfully. This still results in the same 20% successrate seen in prior studies, although the rate of rejec-tion has been reduced from 80% to 10% by onlyweaning the 30 patients with the signature. In addi-tion, the use of tolerogenic IS approaches in combina-tion with predictive signatures to guide decision-mak-ing could eventually alter the balance enough to makeweaning feasible and successful on an even greaterpercentage of LT recipients.
Stem Cell Transplantation
A riskier approach would be to use partially or non-myeloablative therapies (chemotherapeutic agents,total lymphoid irradiation) followed by donor CD34þ
or mesenchymal stem cell infusions to induce toler-ance.51,68 The concept here is that the induction ofmixed donor/recipient chimerism might provide anew T cell repertoire tolerant to both recipient and do-nor and facilitate earlier removal of IS therapy.
228 LEVITSKY LIVER TRANSPLANTATION, March 2011

However, precursor alloreactive T cells would need tobe aggressively depleted for tolerance induction, par-ticularly in MHC-mismatched allografts.109 Suchhigher intensity conditioning protocols geared towardprofound T cell elimination would carry high risks ofinfectious and malignant (LPD) complications andmay only be suitable in less sick recipients (thosewith low MELD scores) or LDLT pairs with better HLAmatching. Whether these strategies are ultimatelyrequired for donor-specific tolerance to develop inliver recipients is not known, although given the toxic-ity, they may be more intuitive for organ transplants(kidney, pancreas, cardiac) with a higher barrier totolerance.36
CONCLUSION
The limitations of past experiences have indeed pro-vided valuable lessons in considering futureapproaches to withdrawal. First, it is likely too restric-tive to only consider patients without viral or immunediseases for withdrawal, because these populationsmay arguably derive even greater clinical benefits.Hence, carefully designed, disease-specific withdrawalapproaches incorporating clinical, immunological, andhistological monitoring should support inclusion ofthese patients in such trials. Second, the ‘‘require-ment’’ for a prolonged quiescent time from transplanta-tion to withdrawal is contentious. Comparative trials ofearly versus late withdrawal that incorporate not onlyoverall success rates but also clinical risks and bene-fits are needed. Similarly, comparative LDLT versusDDLT withdrawal trials are required to better establishthe most optimal approaches and patient selection.Third, trials need to not only include patients at high-est risk of IS complications (those with HCC, HCV,chronic kidney disease), but also children and youngadults who are subject to longer lifetime IS exposures.
Finally, the true benefit of IS withdrawal on healthoutcomes, physical and mental quality of life, andcosts has not been fully characterized, likely due tothe low percentages who have actually reached thisendpoint or followed in withdrawal studies.52 Somestudies have preliminarily suggested that IS with-drawal may improve CNI side effects, such as kidneyfunction, hyperlipidemia, hypertension, and diabetes,and quality of life.64,110 Yet, a limitation of all with-drawal studies is the absence of prospectively fol-lowed, IS-maintained patients as control cohorts. Inaddition, IS minimization strategies such as oncedaily or more intermittent dosing might speculativelybe more beneficial to the LT population than full with-drawal and provide the most optimal approach. Assuch, long-term outcomes and IS-related effects, bothspecific (HCV/HCC recurrence) and general (renal,metabolic, infection, malignancy, cardiovascular),need to be prospectively compared in those patientswho are successfully withdrawn versus those who aremaintained (no attempt at withdrawal; standard orminimized doses) to better characterize the risk/bene-fit pendulum. These approaches are likely to be more
useful in understanding the true clinical benefits ofwithdrawal rather than comparing such outcomes intolerant versus intolerant (failed withdrawal; higherrisk) recipients.64,110
In conclusion, rather than identifying such ‘‘lucky’’tolerant patients ex post facto, prospectiveapproaches incorporating patient characteristics, dis-ease states, tolerogenic IS selection, and immunemonitoring should increase the feasibility of achievingtolerance and establish it as a legitimate option forselect patients. The era of ‘‘lifetime IS therapy for all’’needs to and can move into a new era of ‘‘personalizedIS strategies’’, with a significant percentage of recipi-ents undergoing weaning and others being main-tained, all based on precisely determined immunologi-cal traits, therapies, and biomarkers.
REFERENCES
1. Billingham RE, Brent L, Medawar PB. Actively acquiredtolerance of foreign cells. Nature 1953;172:603-606.
2. Billingham RE, Brent L, Medawar PB. Acquired toler-ance of skin homografts. Ann N Y Acad Sci 1955;59:409-416.
3. Medawar PB, Woodruff MF. The induction of toleranceby skin homografts on newborn rats. Immunology1958;1:27-35.
4. Pan TL, Goto S, Lin YC, Lord R, Chiang KC, Lai CY,et al. The fas and fas ligand pathways in liver allografttolerance. Clin Exp Immunol 1999;118:180-187.
5. Desbarats J, Duke RC, Newell MK. Newly discoveredrole for Fas ligand in the cell-cycle arrest of CD4þ Tcells. Nat Med 1998;4:1377-1382.
6. Desbarats J, Freed JH, Campbell PA, Newell MK. Fas(CD95) expression and death-mediating function areinduced by CD4 cross-linking on CD4þ T cells. ProcNatl Acad Sci U S A 1996;93:11014-11018.
7. Wang L, Han R, Hancock WW. Programmed cell death 1(PD-1) and its ligand PD-L1 are required for allografttolerance. Eur J Immunol 2007;37:2983-2990.
8. Gao Q, Rouse TM, Kazmerzak K, Field EH.CD4þCD25þ cells regulate CD8 cell anergy in neonataltolerant mice. Transplantation 1999;68:1891-1897.
9. Sakaguchi S, Sakaguchi N, Asano M, Itoh M, Toda M.Immunologic self-tolerance maintained by activated Tcells expressing IL-2 receptor alpha-chains (CD25).Breakdown of a single mechanism of self-tolerancecauses various autoimmune diseases. J Immunol 1995;155:1151-1164.
10. Baecher-Allan C, Brown JA, Freeman GJ, Hafler DA.CD4þCD25high regulatory cells in human peripheralblood. J Immunol 2001;167:1245-1253.
11. Hori S, Nomura T, Sakaguchi S. Control of regulatory Tcell development by the transcription factor Foxp3. Sci-ence 2003;299:1057-1061.
12. Tang Q, Bluestone JA. The Foxp3þ regulatory T cell: ajack of all trades, master of regulation. Nat Immunol2008;9:239-244.
13. Brunkow ME, Jeffery EW, Hjerrild KA, Paeper B, ClarkLB, Yasayko SA, et al. Disruption of a new forkhead/winged-helix protein, scurfin, results in the fatal lym-phoproliferative disorder of the scurfy mouse. NatGenet 2001;27:68-73.
14. Bennett CL, Christie J, Ramsdell F, Brunkow ME, Fer-guson PJ, Whitesell L, et al. The immune dysregulation,polyendocrinopathy, enteropathy, X-linked syndrome
LIVER TRANSPLANTATION, Vol. 17, No. 3, 2011 LEVITSKY 229

(IPEX) is caused by mutations of FOXP3. Nat Genet2001;27:20-21.
15. Lin W, Haribhai D, Relland LM, Truong N, Carlson MR,Williams CB, Chatila TA. Regulatory T cell developmentin the absence of functional Foxp3. Nat Immunol 2007;8:359-368.
16. Liu W, Putnam AL, Xu-Yu Z, Szot GL, Lee MR, Zhu S,et al. CD127 expression inversely correlates with FoxP3and suppressive function of human CD4þ T reg cells. JExp Med 2006;203:1701-1711.
17. Yolcu ES, Ash S, Kaminitz A, Sagiv Y, Askenasy N, Yar-koni S. Apoptosis as a mechanism of T-regulatory cellhomeostasis and suppression. Immunol Cell Biol 2008;86:650-658.
18. Mays LE, Chen YH. Maintaining immunological toler-ance with Foxp3. Cell Res 2007;17:904-918.
19. Starzl TE, Demetris AJ, Murase N, Ildstad S, Ricordi C,Trucco M. Cell migration, chimerism, and graft accep-tance. Lancet 1992;339:1579-1582.
20. Starzl TE, Murase N, Abu-Elmagd K, Gray EA, ShapiroR, Eghtesad B, et al. Tolerogenic immunosuppressionfor organ transplantation. Lancet 2003;361:1502-1510.
21. Neujahr D, Turka LA. Lymphocyte depletion as a bar-rier to immunological tolerance. Contrib Nephrol 2005;146:65-72.
22. Shapiro R, Jordan ML, Basu A, Scantlebury V, PotdarS, Tan HP, et al. Kidney transplantation under a tolero-genic regimen of recipient pretreatment and low-dosepostoperative immunosuppression with subsequentweaning. Ann Surg 2003;238:520-525.
23. Shapiro R, Basu A, Tan H, Gray E, Kahn A, RandhawaP, et al. Kidney transplantation under minimal immu-nosuppression after pretransplant lymphoid depletionwith Thymoglobulin or Campath. J Am Coll Surg 2005;200:505-515.
24. D’Addio F, Yuan X, Habicht A, Williams J, Ruzek M,Iacomini J, et al. A novel clinically relevant approach totip the balance toward regulation in stringent trans-plant model. Transplantation 2010;90:260-269.
25. Kim IK, Bedi DS, Denecke C, Ge X, Tullius SG. Impactof innate and adaptive immunity on rejection and toler-ance. Transplantation 2008;86:889-894.
26. Hutchings A, Wu J, Asiedu C, Hubbard W, Eckhoff D,Contreras J, et al. The immune decision toward allo-graft tolerance in non-human primates requires earlyinhibition of innate immunity and induction of immuneregulation. Transpl Immunol 2003;11:335-344.
27. LaRosa DF, Rahman AH, Turka LA. The innate immunesystem in allograft rejection and tolerance. J Immunol2007;178:7503-7509.
28. Pasare C, Medzhitov R. Toll pathway-dependent block-ade of CD4þCD25þ T cell-mediated suppression bydendritic cells. Science 2003;299:1033-1036.
29. Zhai Y, Meng L, Gao F, Wang Y, Busuttil RW, Kupiec-Weglinski JW. CD4þ T regulatory cell inductionand function in transplant recipients after CD154blockade is TLR4 independent. J Immunol 2006;176:5988-5994.
30. Starzl TE, Demetris AJ, Trucco M, Zeevi A, Ramos H,Terasaki P, et al. Chimerism and donor-specific non-reactivity 27 to 29 years after kidney allotransplanta-tion. Transplantation 1993;55:1272-1277.
31. Starzl TE, Demetris AJ, Trucco M, Murase N, Ricordi C,Ildstad S, et al. Cell migration and chimerism afterwhole-organ transplantation: the basis of graft accep-tance. HEPATOLOGY 1993;17:1127-1152.
32. Starzl TE, Demetris AJ, Trucco M, Ricordi C, Ildstad S,Terasaki PI, et al. Chimerism after liver transplantationfor type IV glycogen storage disease and type 1 Gauch-er’s disease. N Engl J Med 1993;328:745-749.
33. Hove WR, van Hoek B, Bajema IM, Ringers J, vanKrieken JH, Lagaaij EL. Extensive chimerism in livertransplants: vascular endothelium, bile duct epithe-lium, and hepatocytes. Liver Transpl 2003;9:552-556.
34. Ayala R, Grande S, Albizua E, Crooke A, Meneu JC,Moreno A, et al. Long-term follow-up of donor chimer-ism and tolerance after human liver transplantation.Liver Transpl 2009;15:581-591.
35. Pons JA, Yelamos J, Ramırez P, Oliver-Bonet M, San-chez A, Rodrıguez-Gago M, et al. Endothelial cell chi-merism does not influence allograft tolerance in livertransplant patients after withdrawal of immunosup-pression. Transplantation 2003;75:1045-1047.
36. Kawai T, Cosimi AB, Spitzer TR, Tolkoff-Rubin N,Suthanthiran M, Saidman SL, et al. HLA-mismatchedrenal transplantation without maintenance immuno-suppression. N Engl J Med 2008;358:353-361.
37. Starzl TE. The ‘‘privileged’’ liver and hepatic tolerogenic-ity. Liver Transpl 2001;7:918-920.
38. Calne RY, Sells RA, Pena JR, Davis DR, Millard PR,Herbertson BM, et al. Induction of immunological toler-ance by porcine liver allografts. Nature 1969;223:472-476.
39. Calne RY, White HJ, Yoffa DE, Binns RM, Maginn RR,Herbertson RM, et al. Prolonged survival of liver trans-plants in the pig. Br Med J 1967;4:645-648.
40. Benseler V, McCaughan GW, Schlitt HJ, Bishop GA,Bowen DG, Bertolino P. The liver: a special case intransplantation tolerance. Semin Liver Dis 2007;27:194-213.
41. Balan V, Ruppert K, Demetris AJ, Ledneva T, Duques-noy RJ, Detre KM, et al. Long-term outcome of humanleukocyte antigen mismatching in liver transplantation:results of the National Institute of Diabetes and Diges-tive and Kidney Diseases Liver Transplantation Data-base. HEPATOLOGY 2008;48:878-888.
42. Kamada N, Davies HS, Roser B. Reversal of transplan-tation immunity by liver grafting. Nature 1981;292:840-842.
43. Kamada N, Shinomiya T. Clonal deletion as the mecha-nism of abrogation of immunological memory followingliver grafting in rats. Immunology 1985;55:85-90.
44. Kamada N, Wight DG. Antigen-specific immunosup-pression induced by liver transplantation in the rat.Transplantation 1984;38:217-221.
45. Markus BH, Fung JJ, Gordon RD, Vanek M, Starzl TE,Duquesnoy RJ. HLA histocompatibility and liver trans-plant survival. Transplant Proc 1987;19:63-65.
46. Opelz G, Mytilineos J, Scherer S, Dunckley H, TrejautJ, Chapman J, et al. Survival of DNA HLA-DR typedand matched cadaver kidney transplants. The Collabo-rative Transplant Study. Lancet 1991;338:461-463.
47. Starzl TE, Demetris AJ, Trucco M, Ramos H, Zeevi A,Rudert WA, et al. Systemic chimerism in human femalerecipients of male livers. Lancet 1992;340:876-877.
48. Thomson AW, Lu L, Wan Y, Qian S, Larsen CP, Starzl TE.Identification of donor-derived dendritic cell progenitorsin bone marrow of spontaneously tolerant liver allograftrecipients. Transplantation 1995;60:1555-1559.
49. Benitez C, Lozano JJ, Martinez-Llordella M, Puig-Pey I,Lopez M, Tisone G, et al. Use of transcriptional bio-markers to identify liver transplant recipients who cansuccessfully discontinue immunosuppressive therapy.Am J Transplant 2010;10 (Suppl 4):A517.
50. Tryphonopoulos P, Tzakis AG, Weppler D, Garcia-Morales R, Kato T, Madariaga JR, et al. The role of do-nor bone marrow infusions in withdrawal of immuno-suppression in adult liver allotransplantation. Am JTransplant 2005;5:608-613.
230 LEVITSKY LIVER TRANSPLANTATION, March 2011
51. Donckier V, Troisi R, Le Moine A, Toungouz M, RicciardiS, Colle I, et al. Early immunosuppression withdrawal af-ter living donor liver transplantation and donor stem cellinfusion. Liver Transpl 2006;12:1523-1528.
52. Girlanda R, Rela M, Williams R, O’Grady JG, HeatonND. Long-term outcome of immunosuppression with-drawal after liver transplantation. Transplant Proc2005;37:1708-1709.
53. Hurwitz M, Desai DM, Cox KL, Berquist WE, EsquivelCO, Millan MT. Complete immunosuppressive with-drawal as a uniform approach to post-transplant lym-phoproliferative disease in pediatric livertransplantation. Pediatr Transplant 2004;8:267-272.
54. Mazariegos GV, Reyes J, Marino I, Flynn B, Fung JJ,Starzl TE. Risks and benefits of weaning immunosup-pression in liver transplant recipients: long-term follow-up. Transplant Proc 1997;29:1174-1177.
55. Oike F, Yokoi A, Nishimura E, Ogura Y, Fujimoto Y,Kasahara M, et al. Complete withdrawal of immunosup-pression in living donor liver transplantation. Trans-plant Proc 2002;34:1521.
56. Takatsuki M, Uemoto S, Inomata Y, Egawa H, Kiuchi T,Fujita S, et al. Weaning of immunosuppression in livingdonor liver transplant recipients. Transplantation2001;72:449-454.
57. Tisone G, Orlando G, Cardillo A, Palmieri G, ManziaTM, Baiocchi L, et al. Complete weaning off immuno-suppression in HCV liver transplant recipients is feasi-ble and favourably impacts on the progression ofdisease recurrence. J Hepatol 2006;44:702-709.
58. Eason JD, Cohen AJ, Nair S, Alcantera T, Loss GE. Tol-erance: is it worth the risk? Transplantation 2005;79:1157-1159.
59. Tryphonopoulos P, Ruiz P, Weppler D, Nishida S, LeviDM, Moon J, et al. Long-term follow-up of 23 opera-tional tolerant liver transplant recipients. Transplanta-tion 2010;90:1556-1561.
60. Koshiba T, Li Y, Takemura M, Wu Y, Sakaguchi S, Min-ato N, et al. Clinical, immunological, and pathologicalaspects of operational tolerance after pediatric living-donor liver transplantation. Transpl Immunol 2007;17:94-97.
61. Li Y, Koshiba T, Yoshizawa A, Yonekawa Y, Masuda K,Ito A, et al. Analyses of peripheral blood mononuclearcells in operational tolerance after pediatric living donorliver transplantation. Am J Transplant 2004;4:2118-2125.
62. Abdelmalek MF, Firpi RJ, Soldevila-Pico C, Reed AI,Hemming AW, Liu C, et al. Sustained viral response tointerferon and ribavirin in liver transplant recipientswith recurrent hepatitis C. Liver Transpl 2004;10:199-207.
63. Berenguer M, Palau A, Aguilera V, Rayon JM, Juan FS,Prieto M. Clinical benefits of antiviral therapy inpatients with recurrent hepatitis C following liver trans-plantation. Am J Transplant 2008;8:679-687.
64. Orlando G, Manzia T, Baiocchi L, Sanchez-Fueyo A,Angelico M, Tisone G. The Tor Vergata weaning offimmunosuppression protocol in stable HCV liver trans-plant patients: the updated follow up at 78 months.Transpl Immunol 2008;20:43-47.
65. Shaked A, Feng S, Punch J, Reyes G, Levitsky J, Klint-malm G, Zimmerman M, et al. Gradual withdrawal ofimmune system suppressing drugs in patients receivinga liver transplant (AWISH). National Institute of Allergyand Infectious Diseases, Immune Tolerance Network,NCT00135694. http://clinicaltrials.gov.
66. Sanchez-Fueyo A, Tisone G, Berenguer M. Effect ofImmunosuppression Drug Weaning on Hepatitis C Vi-rus (HCV)-Induced Liver Damage After Liver Transplan-tation. NCT00668369. http://clinicaltrials.gov.
67. Benıtez CE, Puig-Pey I, Lopez M, Martınez-Llordella M,Lozano JJ, Bohne F, et al. ATG-Fresenius treatmentand low-dose tacrolimus: results of a randomized con-trolled trial in liver transplantation. Am J Transplant2010;10:2296-2304.
68. Donckier V, Troisi R, Toungouz M, Colle I, Van Vlier-berghe H, Jacquy C, et al. Donor stem cell infusion af-ter non-myeloablative conditioning for toleranceinduction to HLA mismatched adult living-donor livergraft. Transpl Immunol 2004;13:139-146.
69. Granot E, Loewenthal R, Jakobovich E, Gazit E, Sokal E,Reding R. Living related liver transplant following bonemarrow transplantation from same donor: long-termsurvival without immunosuppression. Pediatr Trans-plant 2010; doi:10.1111/j.1399-3046.2010.01378.x.
70. Kim SY, Kim DW, Choi JY, Kim DG, Min WS, Lee JW,Kim CC. Full donor chimerism using stem-cell trans-plantation for tolerance induction in the human leuko-cyte antigen-matched liver transplant setting.Transplantation 2009;88:601-603.
71. Matthes-Martin S, Peters C, Konigsrainer A, Fritsch G,Lion T, Heitger A, et al. Successful stem cell transplan-tation following orthotopic liver transplantation fromthe same haploidentical family donor in a girl withhemophagocytic lymphohistiocytosis. Blood 2000;96:3997-3999.
72. Seyfert-Margolis V, Feng S. Tolerance: is it achievablein pediatric solid organ transplantation? Pediatr ClinNorth Am 2010;57:523-538.
73. Talisetti A, Hurwitz M, Sarwal M, Berquist W, CastilloR, Bass D, et al. Analysis of clinical variables associ-ated with tolerance in pediatric liver transplant recipi-ents. Pediatr Transplant 2010;14:976-979.
74. Feng S, Ekong U. Withdrawal of Immunosuppression inPediatric Liver Transplant Recipients (WISP-R). ImmuneTolerance Network, National Institute of Allergy and In-fectious Diseases (NIAID), NCT00320606. http://clinicaltrials.gov.
75. Birkeland SA, Hamilton-Dutoit S, Bendtzen K. Long-term follow-up of kidney transplant patients with post-transplant lymphoproliferative disorder: duration ofposttransplant lymphoproliferative disorder-inducedoperational graft tolerance, interleukin-18 course, andresults of retransplantation. Transplantation 2003;76:153-158.
76. Martınez-Llordella M, Puig-Pey I, Orlando G, Ramoni M,Tisone G, Rimola A, et al. Multiparameter immuneprofiling of operational tolerance in liver transplanta-tion. Am J Transplant 2007;7:309-319.
77. Pons JA, Revilla-Nuin B, Baroja-Mazo A, Ramırez P,Martınez-Alarcon L, Sanchez-Bueno F, et al. FoxP3 inperipheral blood is associated with operational tolerancein liver transplant patients during immunosuppressionwithdrawal. Transplantation 2008;86:1370-1378.
78. Mazariegos GV, Zahorchak AF, Reyes J, Ostrowski L,Flynn B, Zeevi A, Thomson AW. Dendritic cell subsetratio in peripheral blood correlates with successfulwithdrawal of immunosuppression in liver transplantpatients. Am J Transplant 2003;3:689-696.
79. Newell KA, Asare A, Kirk AD, Gisler TD, Bourcier K,Suthanthiran M, et al. Identification of a B cell signa-ture associated with renal transplant tolerance inhumans. J Clin Invest 2010;120:1836-1847.
80. Sagoo P, Perucha E, Sawitzki B, Tomiuk S, StephensDA, Miqueu P, et al. Development of a cross-platformbiomarker signature to detect renal transplant tolerancein humans. J Clin Invest 2010;120:1848-1861.
81. Naka EL, Ponciano VC, Rangel EB, Cenedeze MA,Pacheco-Silva A, Camara NO. FOXP3-positive regula-tory cells inside the allograft and the correlation withrejection. Transplant Proc 2006;38:3202-3204.
LIVER TRANSPLANTATION, Vol. 17, No. 3, 2011 LEVITSKY 231
82. Stenard F, Nguyen C, Cox K, Kambham N, Umetsu DT,Krams SM, et al. Decreases in circulatingCD4þCD25hiFOXP3þ cells and increases in intragraftFOXP3þ cells accompany allograft rejection in pediatricliver allograft recipients. Pediatr Transplant 2009;13:70-80.
83. Li Y, Zhao X, Cheng D, Haga H, Tsuruyama T, Wood K,et al. The presence of Foxp3 expressing T cells withingrafts of tolerant human liver transplant recipients.Transplantation 2008;86:1837-1843.
84. Veronese F, Rotman S, Smith RN, Pelle TD, Farrell ML,Kawai T, et al. Pathological and clinical correlates ofFOXP3þ cells in renal allografts during acute rejection.Am J Transplant 2007;7:914-922.
85. Dijke IE, Caliskan K, Korevaar SS, Maat AP, ZondervanPE, Balk AH, et al. FOXP3 mRNA expression analysisin the peripheral blood and allograft of heart transplantpatients. Transpl Immunol 2008;18:250-254.
86. Martınez-Llordella M, Lozano JJ, Puig-Pey I, Orlando G,Tisone G, Lerut J, et al. Using transcriptional profilingto develop a diagnostic test of operational tolerance inliver transplant recipients. J Clin Invest 2008;118:2845-2857.
87. Carreno MR, Esquenazi V, Gomez C, Garcia-Morales R,Mathew J, Cirocco R, et al. Immunophenotyping andcellular immune responses of cadaveric donor bonemarrow cells. Transplant Proc 1998;30:727-728.
88. Cookson S, Doherty DG, Todryk S, Gibbs P, PortmannB, O’Grady J, et al. Hepatic expression of IL-15 mRNAis associated with liver graft acceptance. TransplImmunol 2003;11:39-48.
89. Lau AH, Thomson AW. Dendritic cells and immune reg-ulation in the liver. Gut 2003;52:307-314.
90. Mathew JM, Garcia-Morales R, Fuller L, Rosen A, Cian-cio G, Burke GW, et al. Donor bone marrow-derivedchimeric cells present in renal transplant recipientsinfused with donor marrow. I. Potent regulators of re-cipient antidonor immune responses. Transplantation2000;70:1675-1682.
91. Mathew JM, Garcia-Morales RO, Carreno M, Jin Y,Fuller L, Blomberg B, et al. Immune responses and theirregulation by donor bone marrow cells in clinical organtransplantation. Transpl Immunol 2003;11:307-321.
92. Miller J, Mathew J, Garcia-Morales R, Zucker KE, Car-reno M, Jin Y, et al. The human bone marrow as animmunoregulatory organ. Transplantation 1999;68:1079-1090.
93. Mazariegos GV, Reyes J, Marino IR, Demetris AJ, FlynnB, Irish W, et al. Weaning of immunosuppression inliver transplant recipients. Transplantation 1997;63:243-249.
94. Newell KA, Asare A, Kirk AD, Gisler TD, Bourcier K,Suthanthiran M, et al. Identification of a B cell signa-ture associated with renal transplant tolerance inhumans. J Clin Invest 2010;120:1836-1847.
95. Zarkhin V, Talisetti A, Li L, Wozniak LJ, McDiarmid SV,Cox K, et al. Expression of soluble HLA-G identifiesfavorable outcomes in liver transplant recipients.Transplantation 2010;90:1000-1005.
96. Lopez M, Clarkson MR, Albin M, Sayegh MH, NajafianN. A novel mechanism of action for anti-thymocyteglobulin: induction of CD4þCD25þFoxp3þ regulatory Tcells. J Am Soc Nephrol 2006;17:2844-2853.
97. Woltman AM, de Fijter JW, Kamerling SW, Paul LC,Daha MR, van Kooten C. The effect of calcineurin inhib-itors and corticosteroids on the differentiation ofhuman dendritic cells. Eur J Immunol 2000;30:1807-1812.
98. Szabo G, Gavala C, Mandrekar P. Tacrolimus and cy-closporine A inhibit allostimulatory capacity and cyto-kine production of human myeloid dendritic cells. JInvestig Med 2001;49:442-449.
99. Gao W, Lu Y, El Essawy B, Oukka M, Kuchroo VK,Strom TB. Contrasting effects of cyclosporine andrapamycin in de novo generation of alloantigen-specificregulatory T cells. Am J Transplant 2007;7:1722-1732.
100. Battaglia M, Stabilini A, Draghici E, Gregori S, Moc-chetti C, Bonifacio E, Roncarolo MG et al. Rapamycinand interleukin-10 treatment induces T regulatory type1 cells that mediate antigen-specific transplantationtolerance. Diabetes 2006;55:40-49.
101. Battaglia M, Stabilini A, Roncarolo MG. Rapamycinselectively expands CD4þCD25þFoxP3þ regulatory Tcells. Blood 2005;105:4743-4748.
102. Nikolaeva N, Bemelman FJ, Yong SL, van Lier RA, tenBerge IJ. Rapamycin does not induce anergy but inhib-its expansion and differentiation of alloreactive humanT cells. Transplantation 2006;81:445-454.
103. Sho M, Sandner SE, Najafian N, Salama AD, Dong V,Yamada A, et al. New insights into the interactionsbetween T-cell costimulatory blockade and conventionalimmunosuppressive drugs. Ann Surg 2002;236:667-675.
104. Segundo DS, Ruiz JC, Izquierdo M, Fernandez-Fres-nedo G, Gomez-Alamillo C, Merino R, et al. Calcineurininhibitors, but not rapamycin, reduce percentages ofCD4þCD25þFOXP3þ regulatory T cells in renal trans-plant recipients. Transplantation 2006;82:550-557.
105. Levitsky J, Miller J, Wang E, Rosen A, Flaa C, Abecas-sis M, et al. Immunoregulatory profiles in liver trans-plant recipients on different immunosuppressiveagents. Hum Immunol 2009;70:146-150.
106. Levitsky J, Mathew JM, Flaa CW, Rosen A, Tambur AR,Miller J. Immunoregulatory effects of conversion fromtacrolimus to sirolimus in liver transplant recipients[Abstract]. HEPATOLOGY 2009;50:568A.
107. Hendrikx TK, Velthuis JH, Klepper M, van Gurp E, GeelA, Schoordijk W, et al. Monotherapy rapamycin allowsan increase of CD4 CD25 FoxP3 T cells in renal recipi-ents. Transpl Int 2009;22:884-891.
108. Levitsky J, Miller J, Leventhal J, Huang X, Flaa C,Wang E, Tambur A, Burt RK, Gallon L, Mathew JM.The human ‘‘Treg MLR’’: immune monitoring forFOXP3þ T regulatory cell generation. Transplantation2009;88:1303-1311.
109. Wells AD, Li XC, Li Y, Walsh MC, Zheng XX, Wu Z,et al. Requirement for T-cell apoptosis in the inductionof peripheral transplantation tolerance. Nat Med 1999;5:1303-1307.
110. Pons JA, Ramırez P, Revilla-Nuin B, Pascual D, Bar-oja-Mazo A, Robles R, et al. Immunosuppression with-drawal improves long-term metabolic parameters,cardiovascular risk factors and renal function inliver transplant patients. Clin Transplant 2009;23:329-336.
232 LEVITSKY LIVER TRANSPLANTATION, March 2011