open vs laparoscopic vs robotic radical prostatectomy
DESCRIPTION
Open vs laparoscopic vs robotic radical prostatectomy. Oliver Hakenberg Department of Urology, Rostock University Rostock, Germany. NEWSWEEK, December 5, 2005. Alaska. 2001. 2002. 2003. 2004. 2005. daVinci systems in the USA 2005. Über 16000 Roboter-assistierte RPEs in den USA 2005. - PowerPoint PPT PresentationTRANSCRIPT
Oliver HakenbergDepartment of Urology, Rostock University
Rostock, Germany
Open vs laparoscopic vs roboticradical prostatectomy
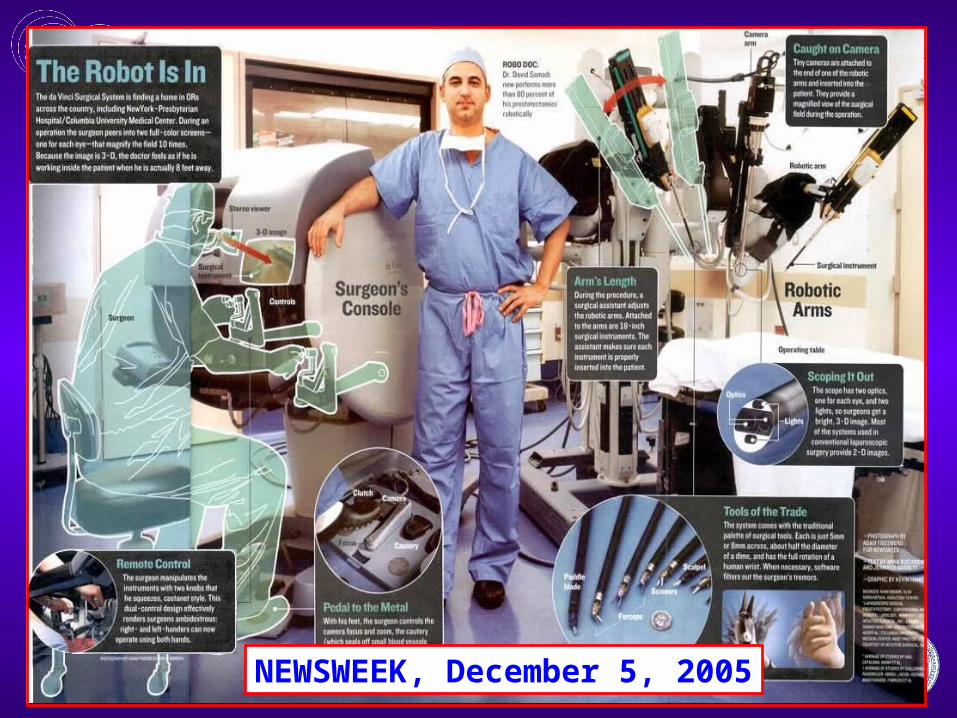
NEWSWEEK, December 5, 2005
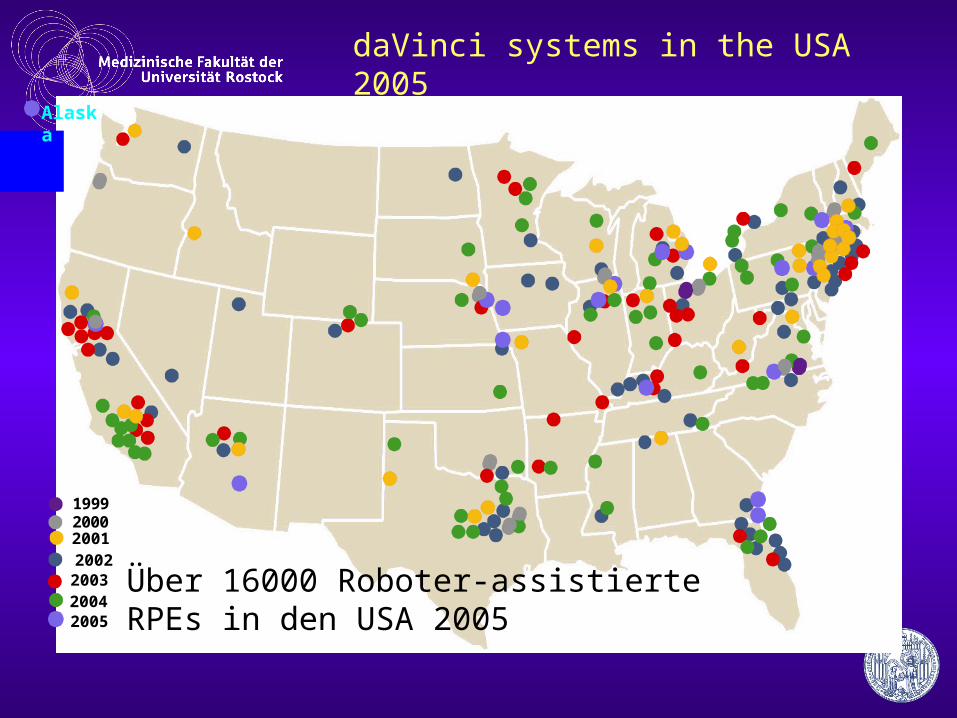
19992000
200220032004
Alaska
2005
2001
daVinci systems in the USA 2005
Über 16000 Roboter-assistierte RPEs in den USA 2005
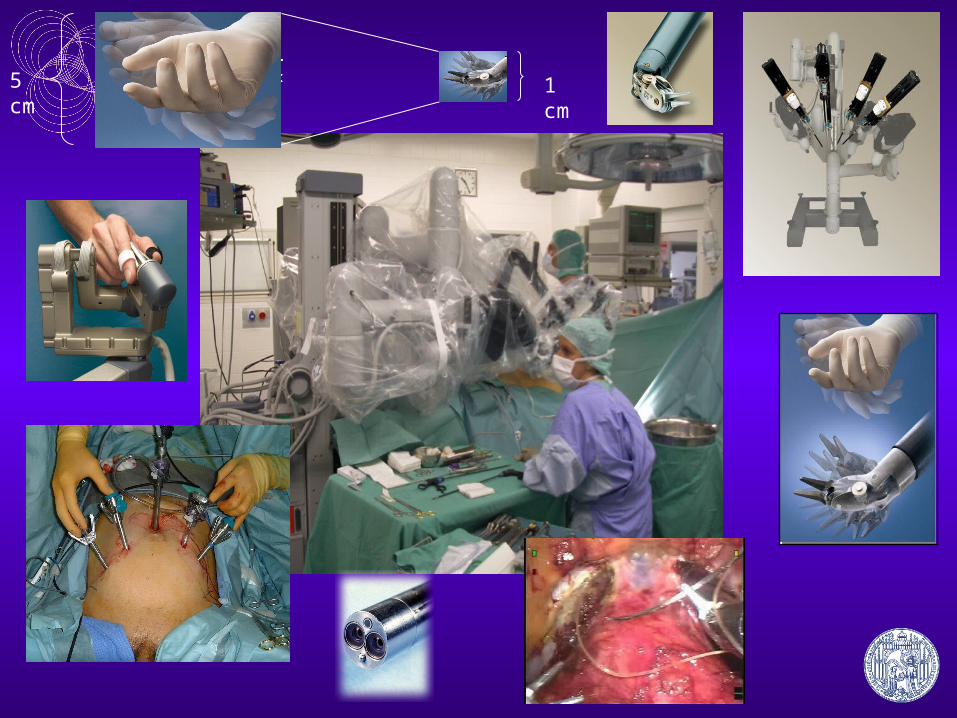
5 cm
1 cm
What are the criteria?
• oncological outcome• functional results• complications• increasing case numbers• costs and revenues from surgery
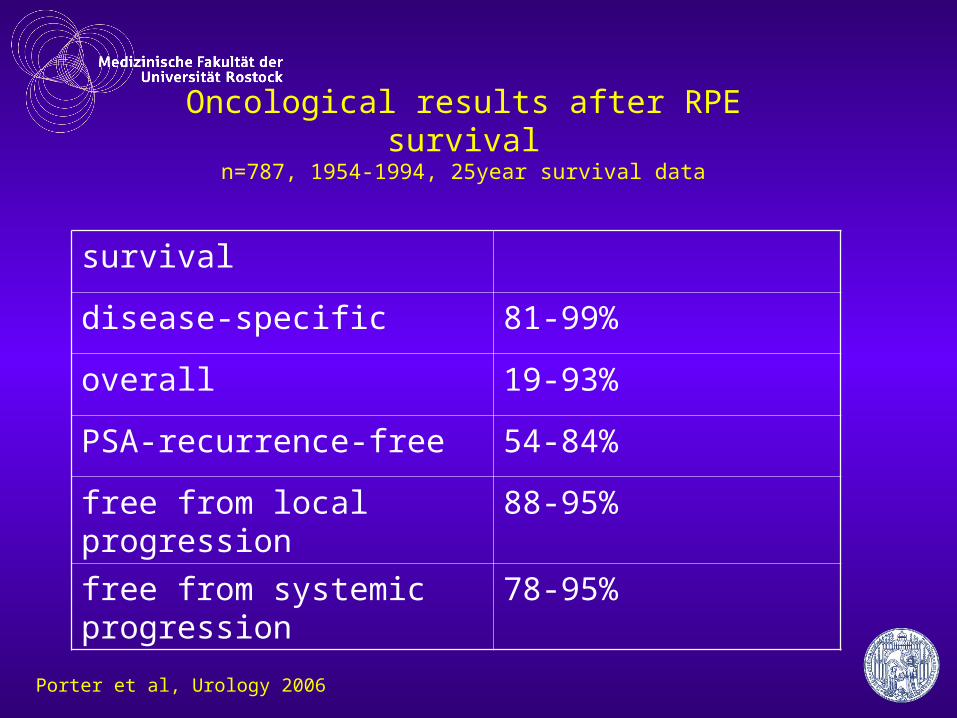
Oncological results after RPEsurvival
n=787, 1954-1994, 25year survival data
survival
disease-specific 81-99%
overall 19-93%
PSA-recurrence-free 54-84%
free from local progression 88-95%
free from systemic progression 78-95%
Porter et al, Urology 2006
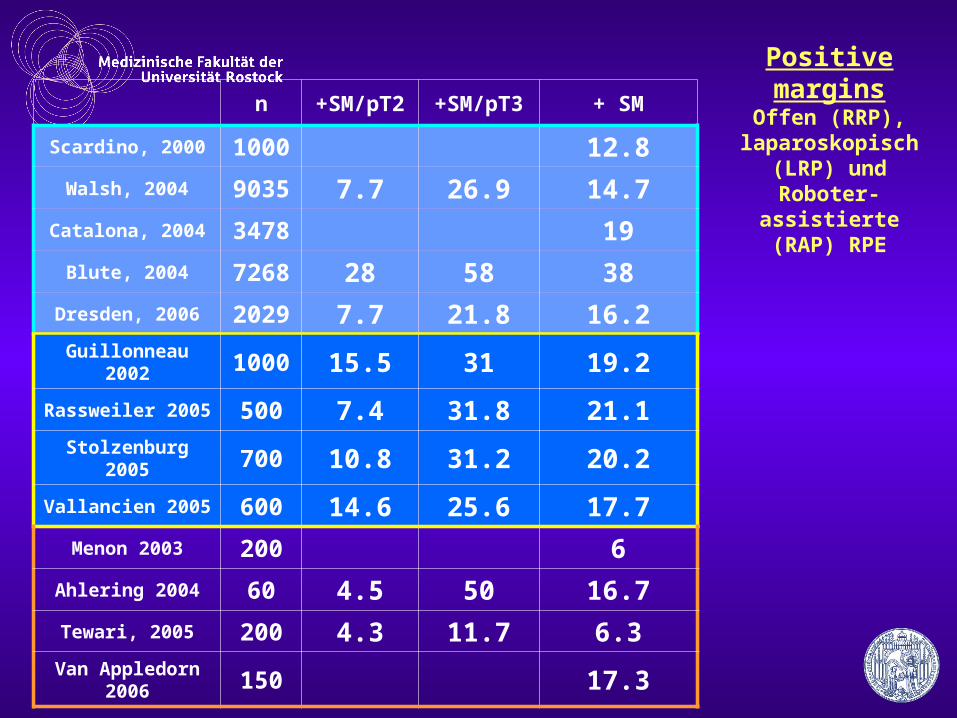
Positive marginsOffen (RRP),
laparoskopisch (LRP) und Roboter-assistierte
(RAP) RPE
n +SM/pT2 +SM/pT3 + SM
Scardino, 2000 1000 12.8
Walsh, 2004 9035 7.7 26.9 14.7
Catalona, 2004 3478 19
Blute, 2004 7268 28 58 38
Dresden, 2006 2029 7.7 21.8 16.2
Guillonneau 2002 1000 15.5 31 19.2
Rassweiler 2005 500 7.4 31.8 21.1
Stolzenburg 2005 700 10.8 31.2 20.2
Vallancien 2005 600 14.6 25.6 17.7
Menon 2003 200 6
Ahlering 2004 60 4.5 50 16.7
Tewari, 2005 200 4.3 11.7 6.3
Van Appledorn 2006 150 17.3
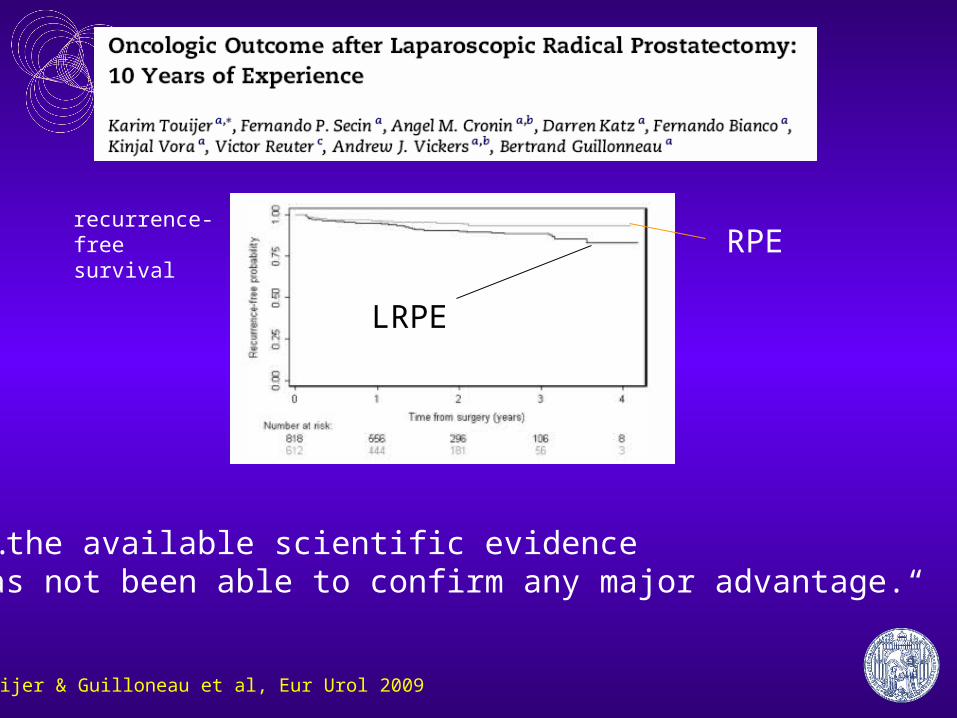
„…the available scientific evidence has not been able to confirm any major advantage.“
Touijer & Guilloneau et al, Eur Urol 2009
RPE
LRPE
recurrence-free survival
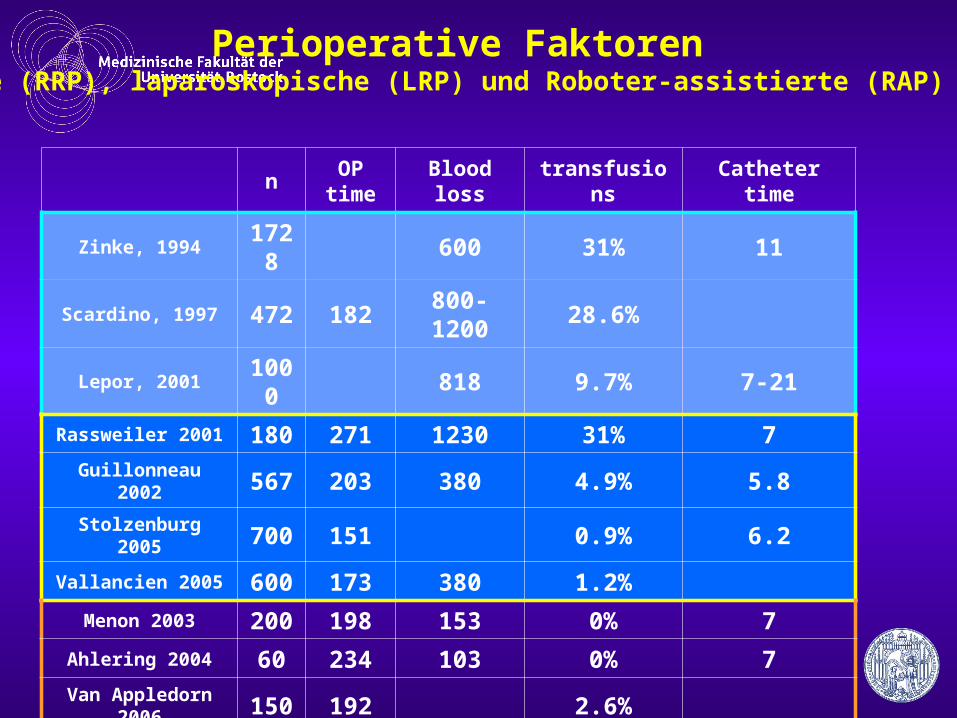
Perioperative Faktorenoffene (RRP), laparoskopische (LRP) und Roboter-assistierte (RAP) RPE
nOP
timeBlood loss transfusions Catheter time
Zinke, 1994 1728 600 31% 11
Scardino, 1997 472 182 800-1200 28.6%
Lepor, 2001 1000 818 9.7% 7-21
Rassweiler 2001 180 271 1230 31% 7
Guillonneau 2002 567 203 380 4.9% 5.8
Stolzenburg 2005 700 151 0.9% 6.2
Vallancien 2005 600 173 380 1.2%
Menon 2003 200 198 153 0% 7
Ahlering 2004 60 234 103 0% 7
Van Appledorn 2006 150 192 2.6%
functional results• continence• potency• cosmesis• duration of hospital stay • time out of work• complications
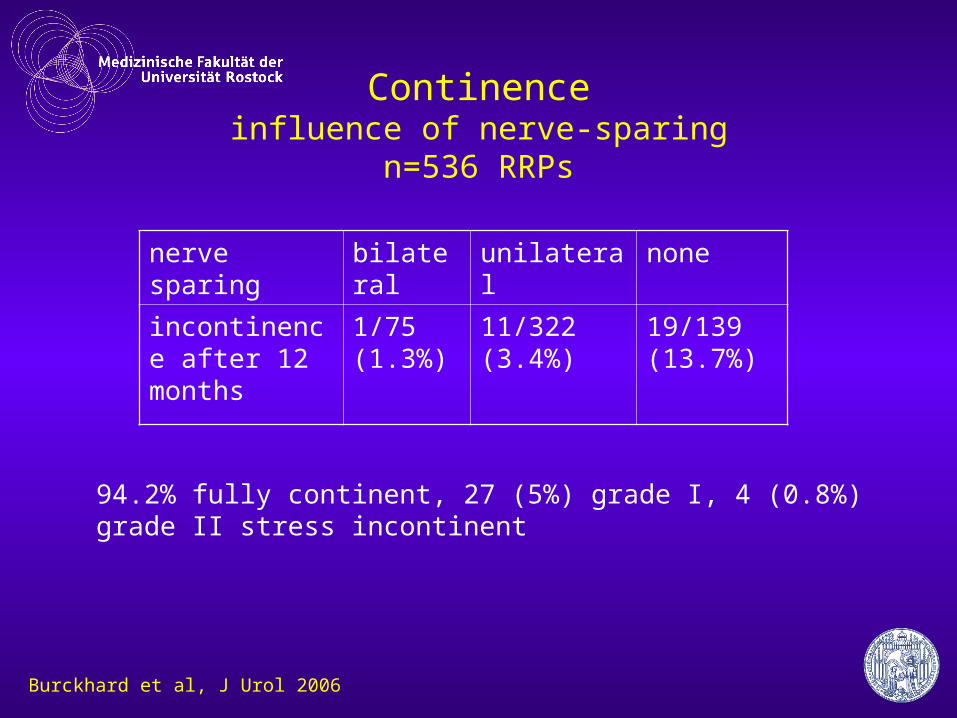
Continenceinfluence of nerve-sparing
n=536 RRPs
nerve sparing bilateral unilateral none
incontinence after 12 months
1/75 (1.3%)
11/322 (3.4%)
19/139 (13.7%)
94.2% fully continent, 27 (5%) grade I, 4 (0.8%) grade II stress incontinent
Burckhard et al, J Urol 2006
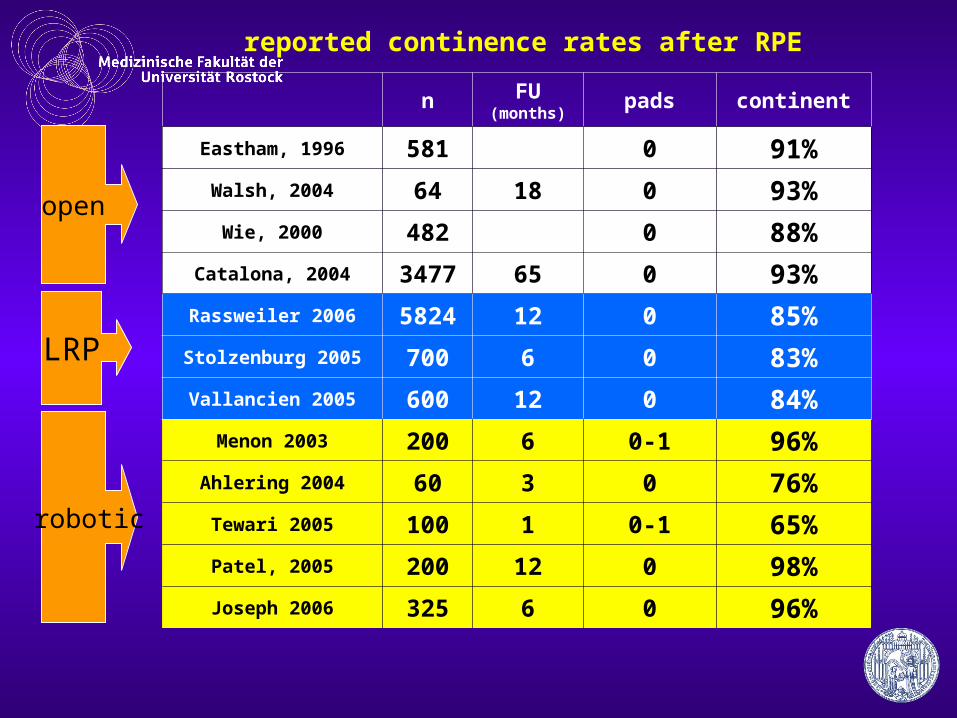
reported continence rates after RPE
n FU (months)
pads continent
Eastham, 1996 581 0 91%
Walsh, 2004 64 18 0 93%
Wie, 2000 482 0 88%
Catalona, 2004 3477 65 0 93%
Rassweiler 2006 5824 12 0 85%
Stolzenburg 2005 700 6 0 83%
Vallancien 2005 600 12 0 84%
Menon 2003 200 6 0-1 96%
Ahlering 2004 60 3 0 76%
Tewari 2005 100 1 0-1 65%
Patel, 2005 200 12 0 98%
Joseph 2006 325 6 0 96%
open
LRP
robotic
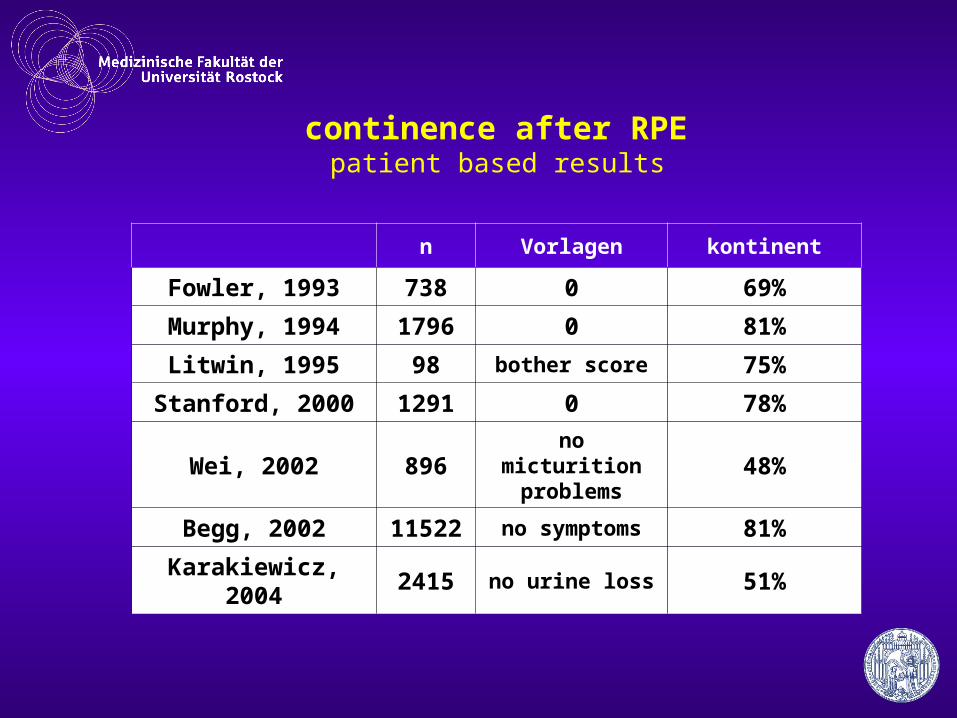
continence after RPE patient based results
n Vorlagen kontinent
Fowler, 1993 738 0 69%
Murphy, 1994 1796 0 81%
Litwin, 1995 98 bother score 75%
Stanford, 2000 1291 0 78%
Wei, 2002 896no micturition
problems 48%
Begg, 2002 11522 no symptoms 81%
Karakiewicz, 2004 2415 no urine loss 51%
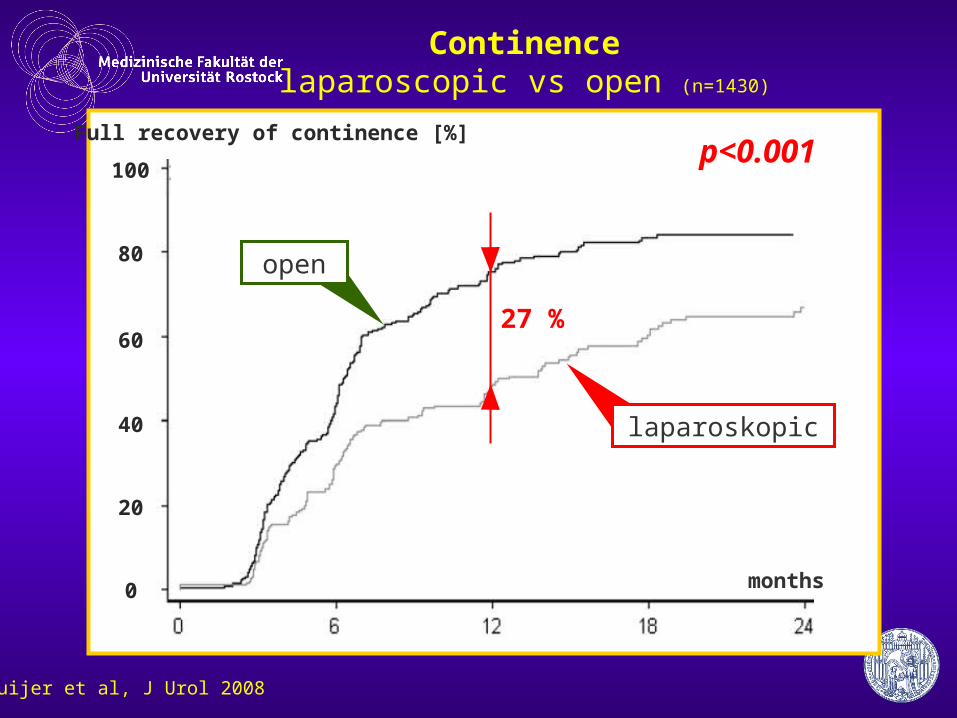
Continencelaparoscopic vs open (n=1430)
Touijer et al, J Urol 2008
100
80
60
40
20
0
Full recovery of continence [%]
months
open
laparoskopic
p<0.001
27 %
3 6 12 18 0
20
40
60
80
100
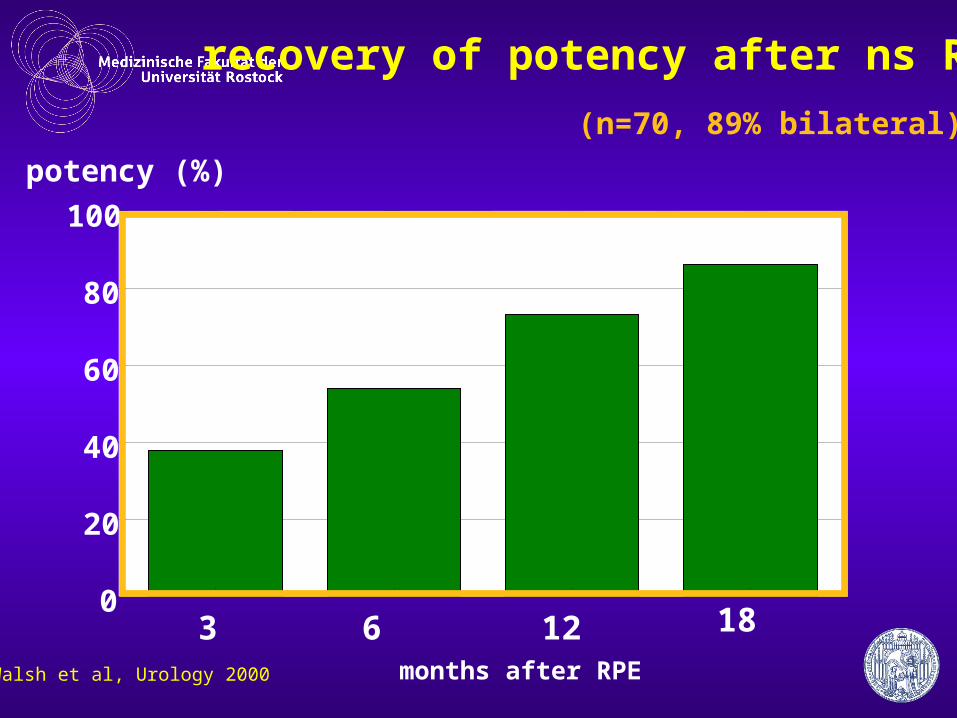
potency (%)
recovery of potency after ns RPE
(n=70, 89% bilateral)
Walsh et al, Urology 2000 months after RPE
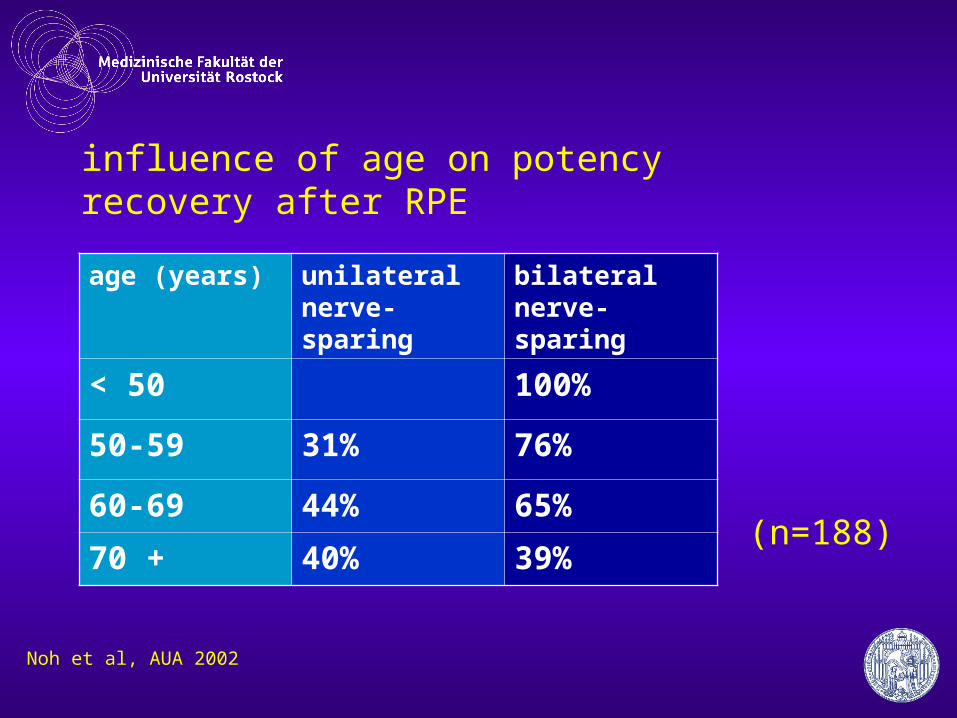
influence of age on potency recovery after RPE
age (years) unilateral nerve- sparing
bilateral nerve- sparing
< 50 100%
50-59 31% 76%
60-69 44% 65%
70 + 40% 39%
Noh et al, AUA 2002
(n=188)
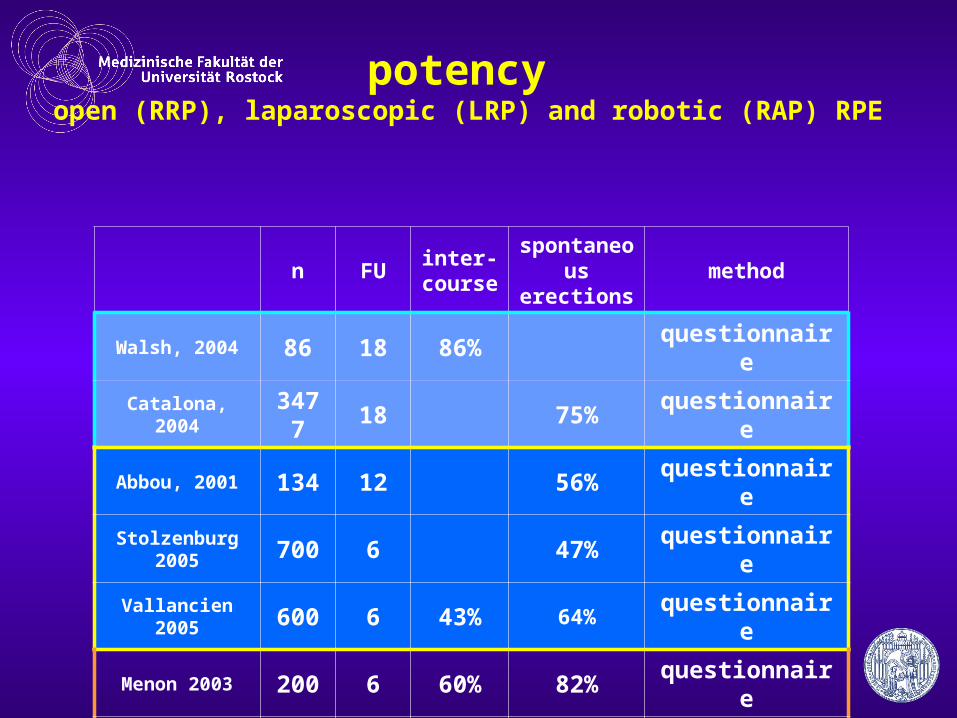
potency open (RRP), laparoscopic (LRP) and robotic (RAP) RPE
n FUinter-course
spontaneous erections
method
Walsh, 2004 86 18 86% questionnaire
Catalona, 2004 3477 18 75% questionnaire
Abbou, 2001 134 12 56% questionnaire
Stolzenburg 2005 700 6 47% questionnaire
Vallancien 2005 600 6 43% 64% questionnaire
Menon 2003 200 6 60% 82% questionnaire
Ahlering 2004 45 6 33% questionnaire
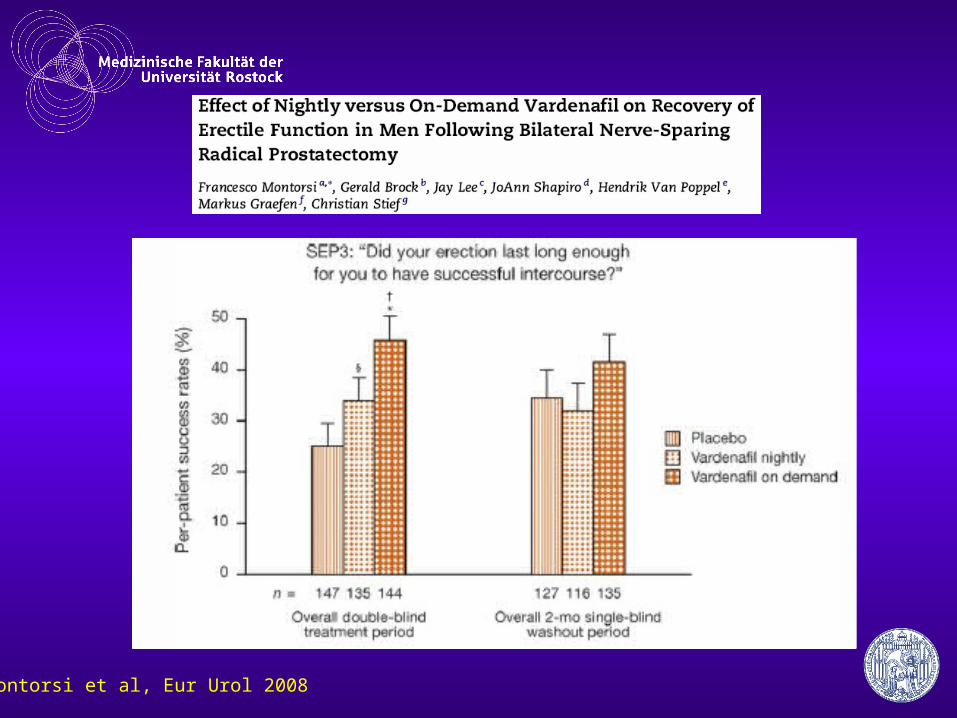
Montorsi et al, Eur Urol 2008
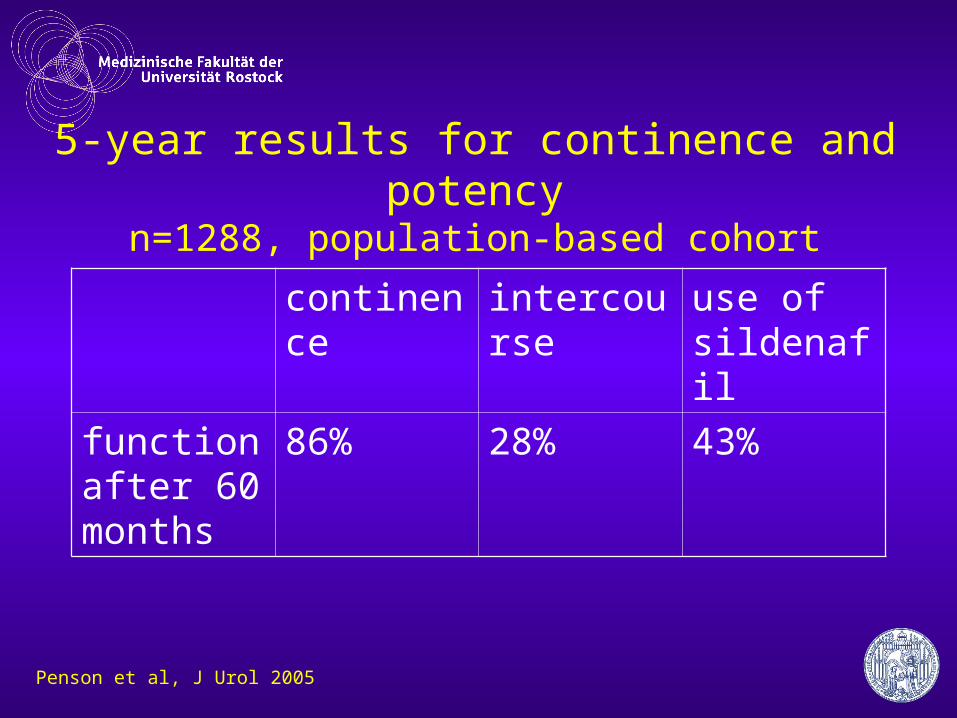
5-year results for continence and potencyn=1288, population-based cohort
continence intercourse use of sildenafil
function after 60 months
86% 28% 43%
Penson et al, J Urol 2005

cosmesisOpen prostatectomy: mini laparotomy
day 12 at 6 months
8 cm
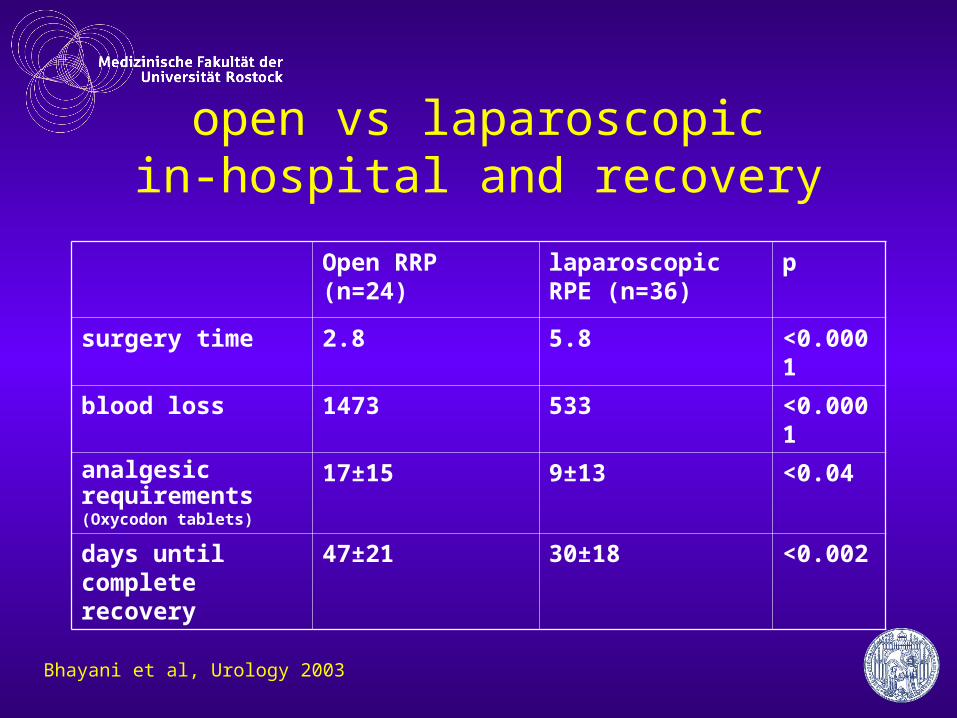
open vs laparoscopicin-hospital and recovery
Open RRP (n=24) laparoscopic RPE (n=36)
p
surgery time 2.8 5.8 <0.0001
blood loss 1473 533 <0.0001
analgesic requirements(Oxycodon tablets)
17±15 9±13 <0.04
days until complete recovery
47±21 30±18 <0.002
Bhayani et al, Urology 2003
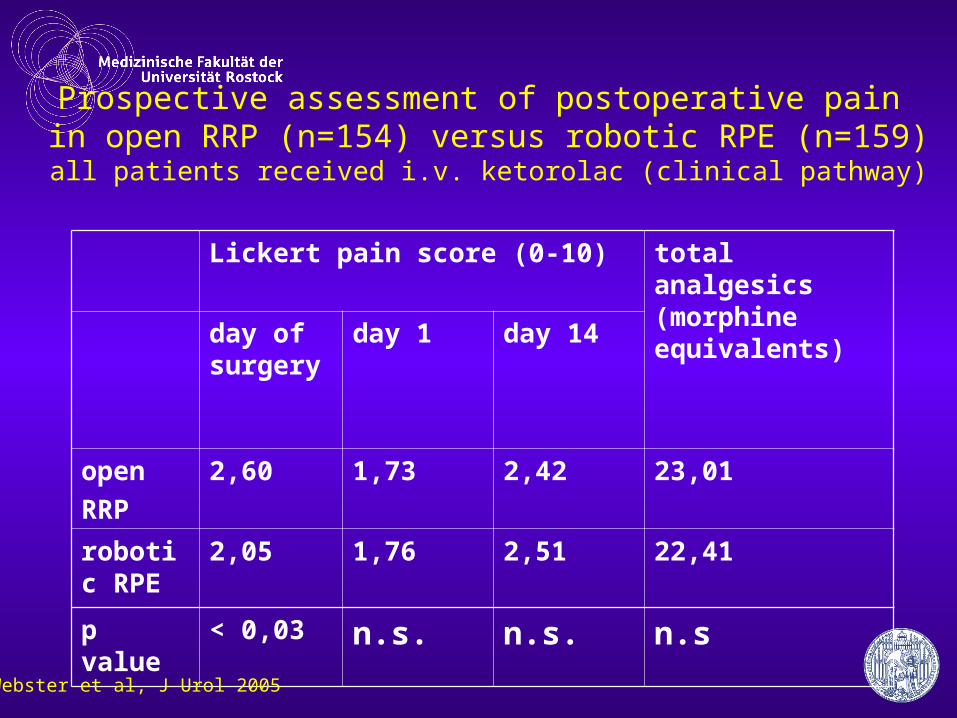
Prospective assessment of postoperative pain in open RRP (n=154) versus robotic RPE (n=159)
all patients received i.v. ketorolac (clinical pathway)
Lickert pain score (0-10) total analgesics (morphine equivalents)
day of surgery
day 1 day 14
open
RRP
2,60 1,73 2,42 23,01
robotic RPE
2,05 1,76 2,51 22,41
p value < 0,03 n.s. n.s. n.s
Webster et al, J Urol 2005
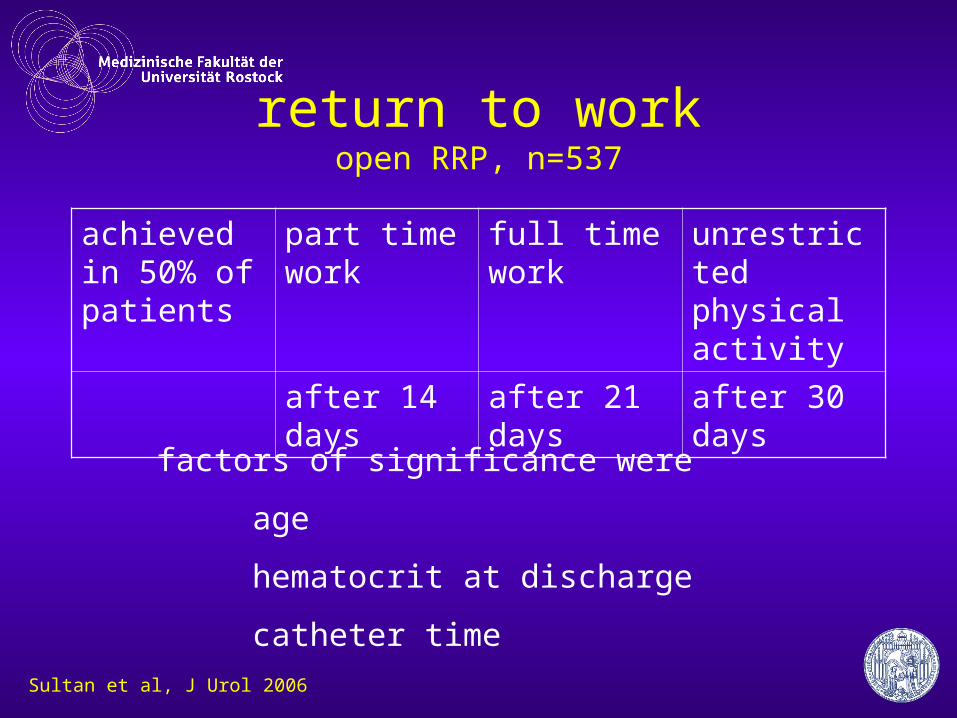
return to workopen RRP, n=537
achieved in 50% of patients
part time work
full time work unrestricted physical activity
after 14 days after 21 days after 30 days
factors of significance were
age
hematocrit at discharge
catheter time
Sultan et al, J Urol 2006
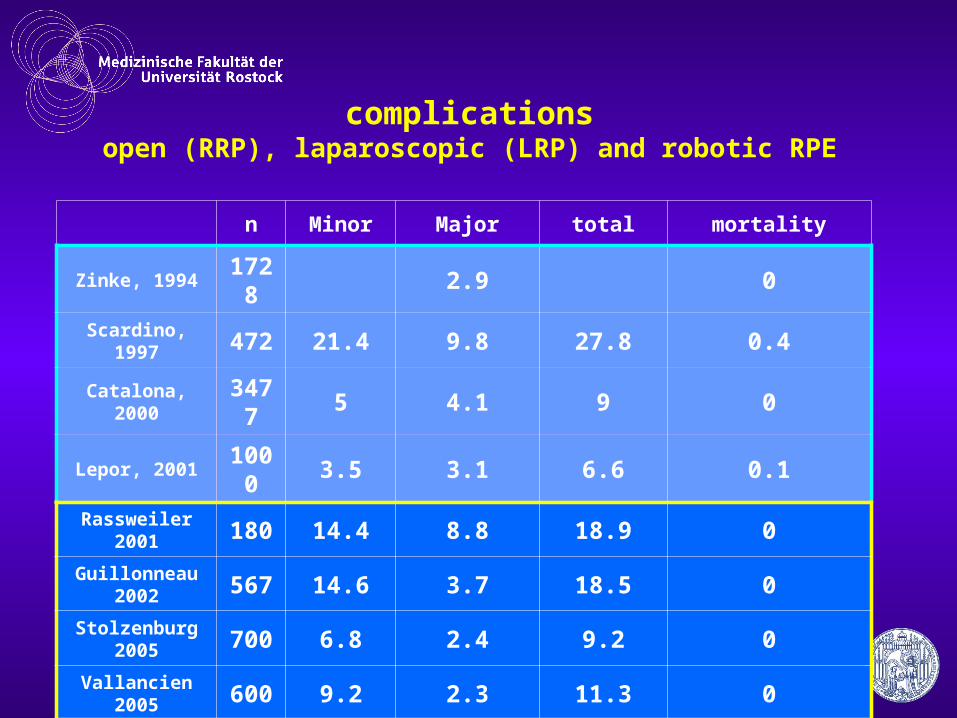
complicationsopen (RRP), laparoscopic (LRP) and robotic RPE
n Minor Major total mortality
Zinke, 1994 1728 2.9 0
Scardino, 1997 472 21.4 9.8 27.8 0.4
Catalona, 2000 3477 5 4.1 9 0
Lepor, 2001 1000 3.5 3.1 6.6 0.1
Rassweiler 2001 180 14.4 8.8 18.9 0
Guillonneau 2002 567 14.6 3.7 18.5 0
Stolzenburg 2005 700 6.8 2.4 9.2 0
Vallancien 2005 600 9.2 2.3 11.3 0
Menon 2003 200 1.5 2 3.5 0
Ahlering 2004 60 3.3 3.3 6.7 0
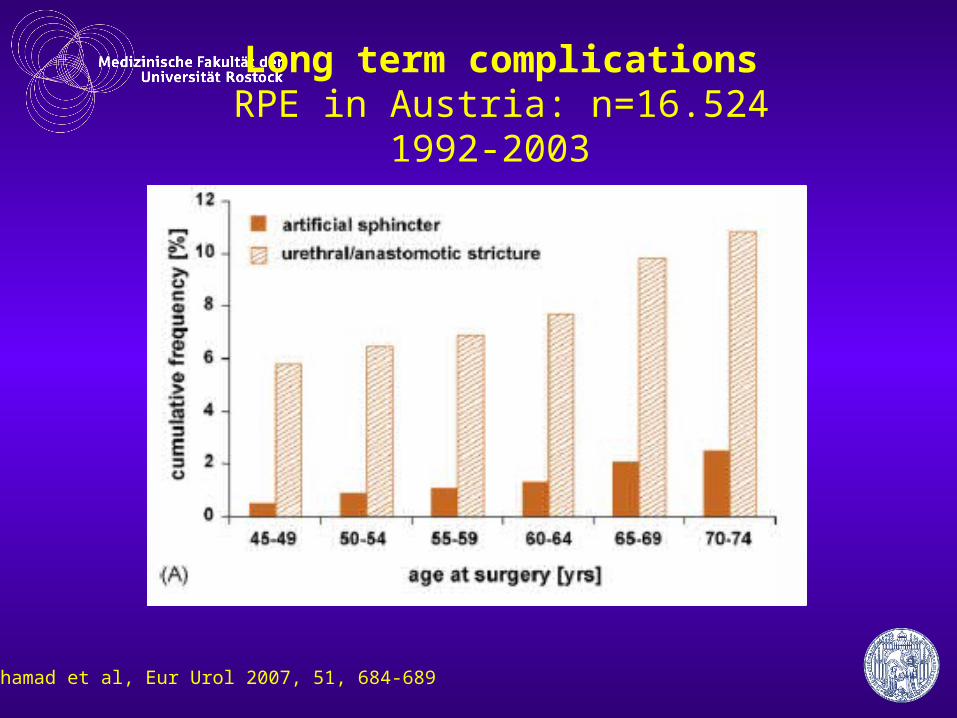
Long term complicationsRPE in Austria: n=16.524
1992-2003
Mohamad et al, Eur Urol 2007, 51, 684-689
increasing case numbers
• OR time and capacity• surgical volume• complications• costs & revenues
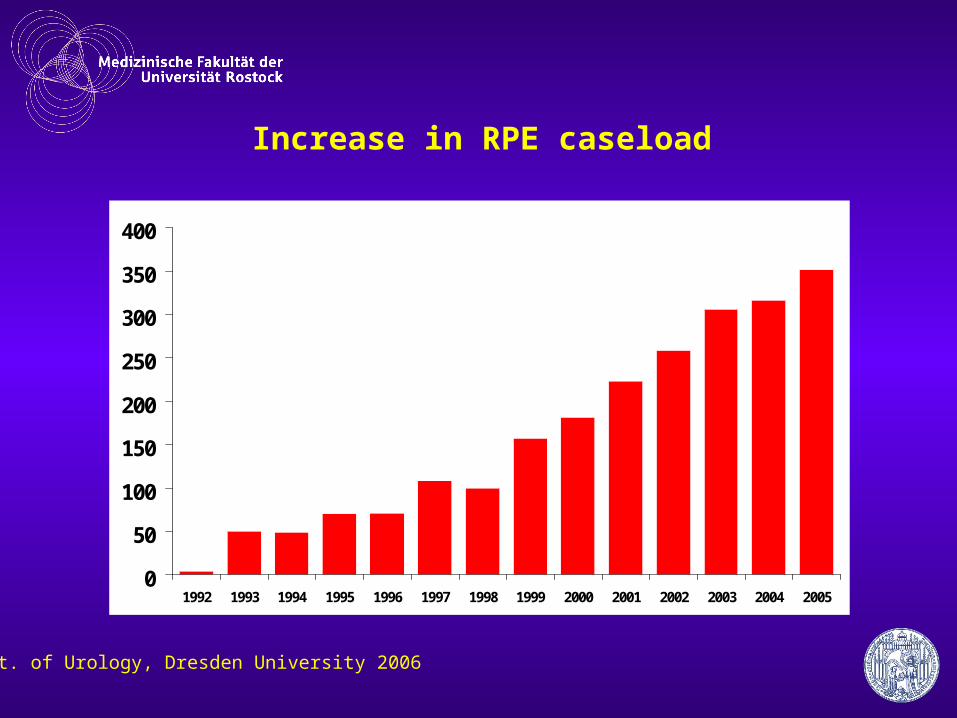
Increase in RPE caseload
0
50
100
150
200
250
300
350
400
1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
Dept. of Urology, Dresden University 2006
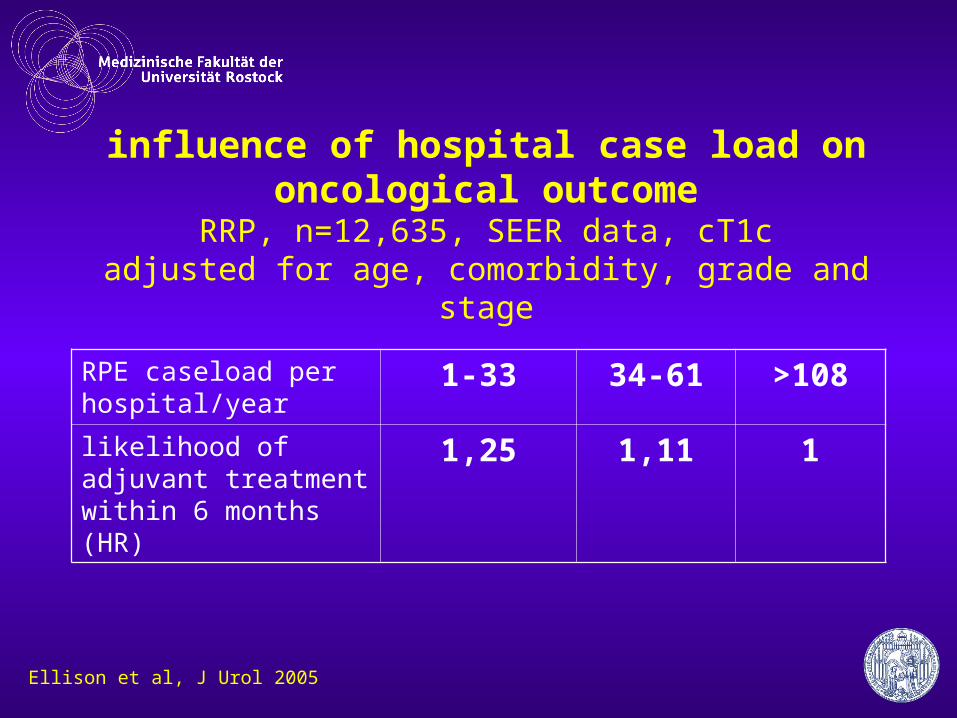
influence of hospital case load on oncological outcome
RRP, n=12,635, SEER data, cT1cadjusted for age, comorbidity, grade and stage
RPE caseload per hospital/year
1-33 34-61 >108
likelihood of adjuvant treatment within 6 months (HR)
1,25 1,11 1
Ellison et al, J Urol 2005
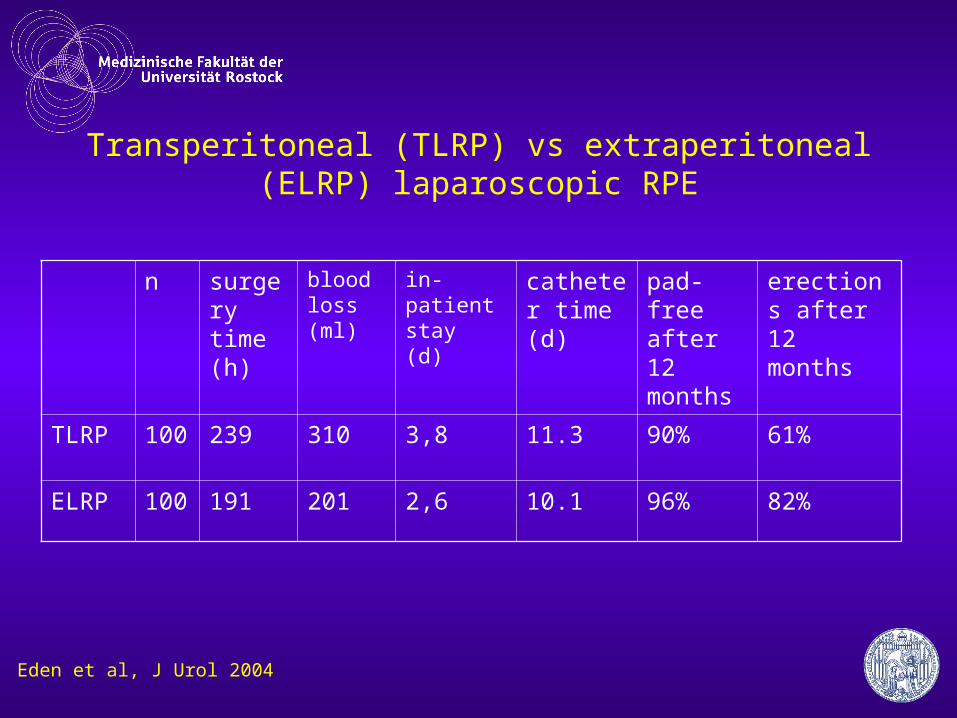
Transperitoneal (TLRP) vs extraperitoneal (ELRP) laparoscopic RPE
n surgery time (h)
blood loss (ml)
in-patient stay (d)
catheter time (d)
pad-free after 12 months
erections after 12 months
TLRP 100 239 310 3,8 11.3 90% 61%
ELRP 100 191 201 2,6 10.1 96% 82%
Eden et al, J Urol 2004
costs depend on surgery time LRP vs RRP, cost analysis
• LRP increases costs by 17.5%• factors for cost increase (in this order)
– surgery time– in-hospital stay– use of disposables
• cost equivalence– if surgery time for LRP < 160 minutes– or if LRP is outpatient surgery!!
Link et al, J Urol 2004
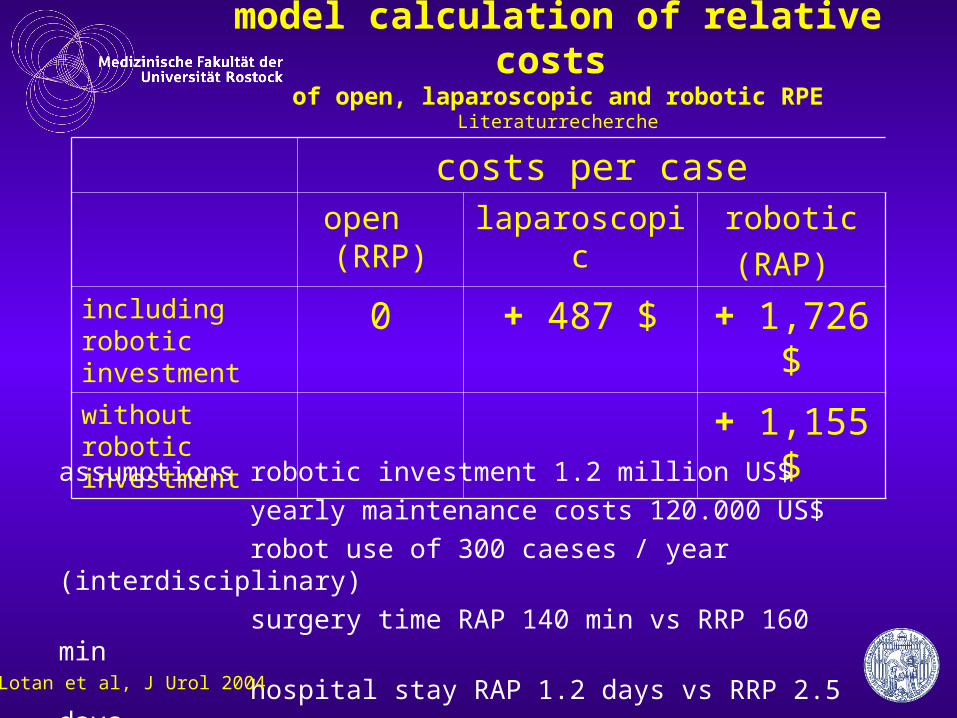
model calculation of relative costs of open, laparoscopic and robotic RPE
Literaturrecherche
costs per caseopen (RRP)
laparoscopic robotic
(RAP) including robotic investment
0 + 487 $ + 1,726 $
without robotic investment
+ 1,155 $
assumptions robotic investment 1.2 million US$
yearly maintenance costs 120.000 US$
robot use of 300 caeses / year (interdisciplinary)
surgery time RAP 140 min vs RRP 160 min
hospital stay RAP 1.2 days vs RRP 2.5 days
Lotan et al, J Urol 2004
costs depend on case numbers and local structuresmodel calculation
• extra costs of RAP vs RRP of 783 $/case
• cost effective with 10 cases/week
• with 14 cases/week or more RAP becomes cheaper if in-patient stay is < 1.5 days
Scales et al, J Urol 2005
Ficarra et al, Eur Urol, 2009
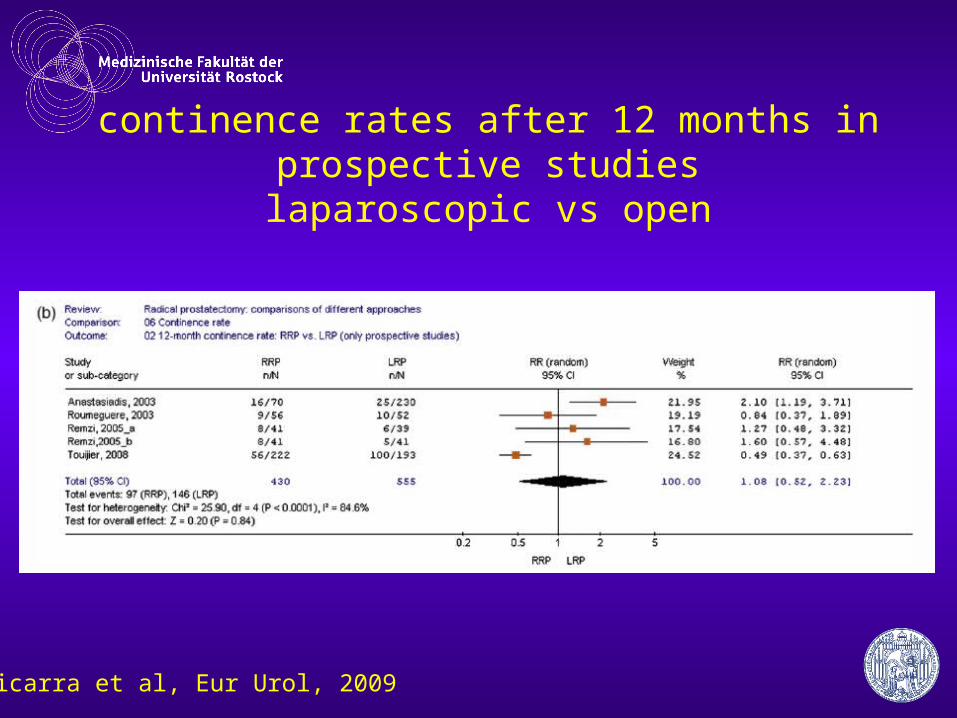
continence rates after 12 months in prospective studieslaparoscopic vs open
Ficarra et al, Eur Urol, 2009
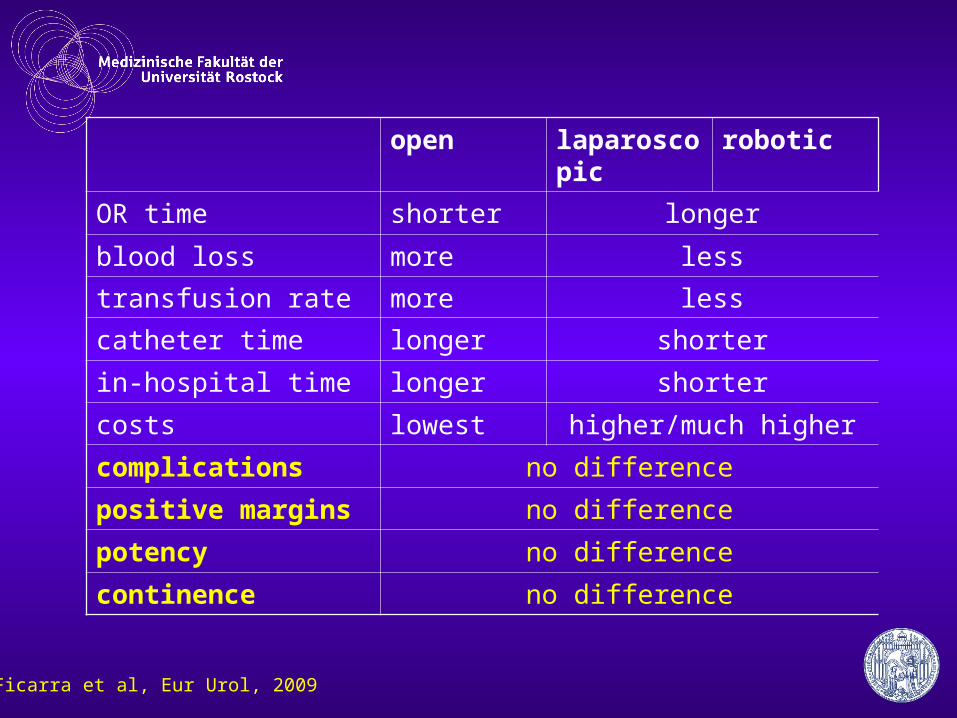
open laparoscopic robotic
OR time shorter longer
blood loss more less
transfusion rate more less
catheter time longer shorter
in-hospital time longer shorter
costs lowest higher/much higher
complications no difference
positive margins no difference
potency no difference
continence no difference
Ficarra et al, Eur Urol, 2009
Comparing robotic, laparoscopic and open retropubic prostatectomy… the available data were not sufficient to prove the superiority of any surgical approach in terms of functional and oncologic outcome.
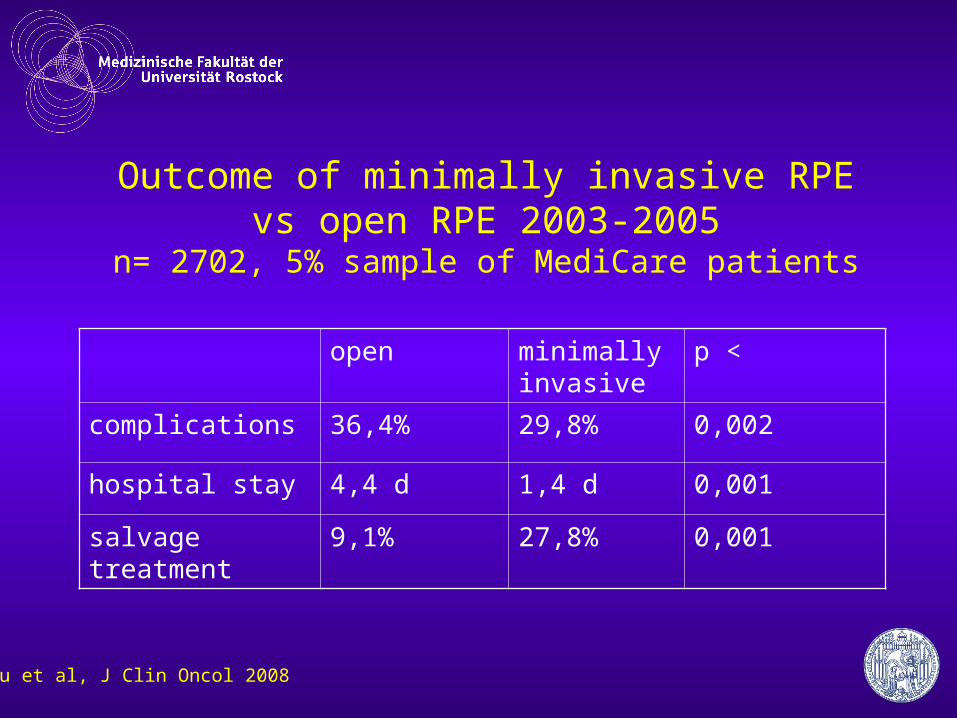
Outcome of minimally invasive RPE vs open RPE 2003-2005
n= 2702, 5% sample of MediCare patients
open minimally invasive
p <
complications 36,4% 29,8% 0,002
hospital stay 4,4 d 1,4 d 0,001
salvage treatment 9,1% 27,8% 0,001
Hu et al, J Clin Oncol 2008
„Minimally invasive“„modern“
„high tech“„no blood loss“„fully continent“
„fully potent“
„…wide acceptance of new techniques based on hypothetical benefits or extrapolated proven advantages from other surgical operations such as cholecystectomy…“
„This study is more of a comparison of surgeons and their techniques than a pure comparison of surgical technique.“
Touijer et al, J Urol 2008