on selected gi infections - ucsf cme · updates on selected gi infections joanne engel, m.d., ph.d....
TRANSCRIPT

2/14/2017
1
Updates on selected GI infections
Joanne Engel, M.D., Ph.D.Professor
Depts of Medicine and Microbiology/ImmunologyUCSF
Disclosures
None
Updates on:
• Food‐borne GI illnesses with a focus on infectious diarrhea
– Traveler’s diarrhea will be covered on Friday (Brian Schwartz)
– C. diff was covered yesterday(Sarah Doernberg)
• Abdominal infections
• H. pylori (person‐person)
Diarrhea: a global cause of disease
• 2nd leading cause of morbidity/mortality worldwide
• In the US
– 200‐375 million episodes/year
– 73 million physician visits
– 1.8 million hospitalizations
– 5000 deaths
– Each person has 1‐2 diarrheal illnesses/yr

2/14/2017
2
Case
• 32 yo female calls your office c/o diarrhea x 2
days. She notes 8 loose stools in the past 24
hrs. She has a low grade temp, mild nausea,
and has vomited x 2. She denies bloody
stools, recent travel, ingestion of unsual foods.
No sick contacts.
Differential Dx
• Infectious
• Ischemic
• IBD
• Iatrogenic/Osmotic
• Malabsorption
The players aka “The dirty laundry list”Viral Bacterial ProtozoalCalicivirus (Norwalk,
Norovirus, Sapovirus)Salmonella 16.4 Giardia
RotavirusCampylobacter
14.3E. histolytica
Adenovirus Shigella 2.3 Cryptosporidium 1.4
CMV Yersinia 0.3 Microsporidium
AstrovirusE. Coli (shiga toxin)
1.1Cyclospora
Small round virus C. difficile
Corona virus C. perfringens
HSV S. aureus
Bacillus
Vibrio 0.4
Listeria
Chlamydia, GC *cases per 100,000 in US
Some enteric pathogens are very infectious
Organism Inoculum
Shigella 10‐100
Giardia 30‐100
Cryptosporidium parvum 30‐100
Shigatoxin‐producing E. coli 10‐100
Norovirus 10‐100
Salmonella 103‐105
Campylobacter 103‐106
Cholera 106
ETEC 108
A little goes a long way…

2/14/2017
3
Symptoms: not really specific• Bloody diarrhea
– In USA: Shigella, Campy, Salmonella, Shigatoxin‐producing E. coli
– Consider also: Amoebiasis, Vibrio, Aeromonas, Yersinia, Plesiomonas
• Watery diarrhea
– ETEC, enteric viruses, Crytposporidium parvum, Cyclospora cayetanensis
• Fever: Implies inflammation, consider:– Invasive bacteria (Salmonella, Shigella, Campy)
– C. diff
– Noro/rotavirus
• Vomiting– Viral gastroenteritis
– Preformed toxin (incubation 2‐7 hours): B. cereus, Staph aureus
– Anisakiasis
• Non‐GI syndromes– Fish and mushroom toxins, botulism, listeria, typhoid, HAV, toxoplasma,
brucella Talan D et al., Clin Infect Dis. 2001 Feb 15;32(4):573‐80
Take a good history
• When & how illness began
• Stool characteristics
• Frequency & quantity
• Presence of dysenteric symptoms
• Symptoms of volume depletion
• Associated symptoms
• Epidemiologic clues
Be a Sherlock Holmes• Travel to developing area
• Food‐handler or caregiver
• Day‐care center attendance or employment– “a veneer of feces”
• Consumption of raw meats, eggs, unpasteurized milk/cheese, swimming in or drinking from untreated fresh water
• Farm or zoo animals, reptiles
• Exposure to other ill persons
• Medications, esp antibiotics
• Underlying medical conditions, HIV, IC
• Receptive anal intercourse or oral/anal contact
Etiology of severe acute gastroenteritis in adults in ER
• Prospective multicenter ER‐based study)
• Pathogens found in ~50%
• Norovirus comprises 50% of identified pathogens; 25% of all cases
0
5
10
15
20
25
30
Iden
tified
pathogens in ER
visits
Bresee et al, JID, 2012

2/14/2017
4
When should you do a work‐up?
• Duration >3‐7 days; > 24 hours if associated with blood; “mod‐severe disease”
• Hospital admission
• Outbreak settings
– Even if not useful for rx, can have public health benefit
• Immunocompromised patients
• Risky patients: HCW, food handlers, daycare
• Persistent diarrhea
Guerrant RL et al. Clinical Infectious Diseases ; 2001 ; 32 : 331 ‐35Riddle et al, AJG, 2016
What’s the work‐up• Stool cx for Salmonella, Shigella, Campy, E. coli 0157:H7
(sorbitol‐negative)– Non‐0157:H7 STEC are sorbitol +, need to also order Shiga‐toxin by EIA
– Shellfish‐assoc or cholera suspectedsalt‐containing media is needed for Vibrio
• C. diff toxin
• Rotavirus Ag (esp in kids)
• Yersinia culture (if compatible travel hx)
• Parasites (if persistent or host factors):– Stool O+P
– Giardia Ag
– Coccidia exam (cyclospora, isospora, cryptosporidium)
– Modified trichrome stainMicrosporidia
• STI risks: RPR; GC and chlamydia (incl LGV work‐up if positive)
Guerrant RL et al. Clinical Infectious Diseases ; 2001 ; 32 : 331 ‐350
FDA approved Multiplex PCR
Riddle et al, AJG, 2016
Infectious causes of persistent diarrhea• Definition
– Persistent diarrhea > 14 days
– Chronic diarrhea > 4‐6 weeks, not usually infectious in etiology
• 3% of returning travelers
• Enteric parasites
– Giardia: Freshwater, daycare centers
– E. histolytica
– Cryptosporidium: Human and animal reservoir, drinking water, low inoculum
– Cyclospora: Nepal, Haiti, Peru, Guatemalan rasperries, seasonal
– Isospora
– In HIV, consider Microsporidia, MAC
• Bacteria: Shigella, enteroaggregative E. coli
• Post‐infectious IBS– ~10‐15% vs. 2% in the general population
• Brainerd diarrhea Dupont, HL. JAMA. 2016

2/14/2017
5
Case
• 25 attendees of the ID holiday party become ill, and you are suspicious for a foodborne disease
• Median incubation period = 28h
• 90% with vomiting
• 50% with diarrhea
• 30% with fever
• Recovery occurred in 12‐60 hours
What is the etiology?
A. Norovirus
B. Shigella sonnei
C. Staphylococcus aureus enterotoxin
D. C. perfringens
E. B. cereus
Foodborne disease by incubation period
• < 2 hours: Chemical agent – scrombroid, ciguatera, mushroom toxins, etc
• 2‐7 hours: Preformed toxin (except C. perfringens)– Staph aureus, B cereus
• 8‐14 hours: Increased inoculum and C. perfringens– Not necessarily more severe
• > 14 hours: Most viruses and bacteriaNorwalkRotavirus
Viral diarrhea vs bacterial diarrhea
• Viral diarrhea usually resolves ≤ 3 days
Norovirus

2/14/2017
6
What is the etiology?
A. NorovirusB. Shigella sonnei
– Diarrhea predominates
C. Staphylococcus aureus enterotoxin– Too long an incubation– No fever
D. C. perfringens– Too long incubation– Vomiting is unusual
E. B. cereus– Too long incubation
Kaplan criteria
• Used to determine if outbreak likely 2/2 Norovirus
• 99% sp, 68% sn if all criteria met
1. Mean/median illness duration of 12‐60 hrs
2. Mean/median incubation period of 24‐48 hrs
3. > 50% of people with vomiting
4. No bacterial agent found
Turcios RM et al., Clin Infect Dis. 2006 Apr 1;42(7):964‐9
Just a little stomach flu… Holy sh**

2/14/2017
7
• Single (+) stranded, noneveloped RNA virus
• Caliciviridae family
• Genogroups‐>genotypes‐>strains
• Replicates only in GI tract
• Persists in environment
• Humans are the only reservoir
Glass et al, NEJM, 2009Sx
• Inc 12‐48 hrs (mean 33 hrs)
• Sudden onset diarrhea, vomiting, abd pain, malaise, low grade fever
– Profuse and projectile
• Usually self‐limited, resolves ≤ 3 d
– Prolonged and severe sx in elderly, very young, IC pts
– Prolonged asymptomatic shedding
• Up to 8 wks in healthy pts
• Up to 1 yr in severely IC pts
Larry the vomiting robot
Dx
• Not culturable
• Older techniques: EM, stool ELISA
• Gold standard: RT‐PCR (since early 1990’s)
– 68% sensitive
– 99% specific
– Available at public health depts, state & national labs, sendouts
Evolving epidemiology
• Most common cause of gastroenteritis• Leading cause of diarrhea
• Leading cause of foodborne‐associated illnesses
• Responsible for 50% of gastroenteritis outbreaks worldwide
• Greatly under‐reported– Only 1/1562 cases identified
– ~21 million cases/yr US
– ~2.1 million ambulatory visits/yr
– ~71,000 norovirus‐associated hospitalizations costing $493 million/yr (CID 2011: 52, 466)
– ~800 deaths/yr US
– 200,000 deaths annually children <5 developing
nations
CDCGastanaduy et al, JID, 2013

2/14/2017
8
Norovirus is a moving target• Antigenic shift and drift (like influenza)
– Change in viral capsid affects binding to GI tract oligosaccharides
– New variant‐>new epidemic wave
– New pandemic strain every 2‐4 yrs
• GI, GII, GIV genotypes cause most human infxns
– GII.4 strains predominant since 1990’s
– GII.4 Sydney strain, GII.p17, GII.17
– Continue to evolve q 2‐3 yrs
Why is norovirus so difficult to contain?
• Highly transmissable: a little goes a long way…– ID50: 10‐100 virions– Facile 2˚ spread
• Viral shedding precedes clinical illness in >30% of pts • Prolonged shedding
– Up to 8 wks in healthy hosts– Up to 1 yr in IC hosts
• Asymptomatic shedders
– Withstands wide range of temps and persists in environment
– Immunity is short‐lived and not cross‐protective against antigenic variants
Why is norovirus so difficult to contain?• Multiple modes of transmission
– Food• Globalization of food distribution• Increased # of people who handle the food we eat• Increased consumption of food at risk of contamination (fresh vegetables and fruit)
– Water– Airborne via vomitus
• Susceptibility correlates w/distance from vomiting event
– Contact w/contaminated surfaces– Fomites– Person‐person contact– Resistant to many disinfectants
Interrupting transmission
• Disinfection– Wipe surface w/detergent to remove particle debris followed by hypochlorite bleach (5000 ppm) as disinfectant
– Other disinfectants less efficient: (quanternary ammonium compounds, alcohols)
– Alcohol‐based disinfectants are insufficient
• Wash hands for 1 min w/soap & water, rinse for 20 sec, dry w/disposable towels

2/14/2017
9
Interrupting transmission
• Institutional settings– Cohort pts and staff
– Minimize transport, visitors
– Isolation, contact precautions for sick pts (48 hrsafter sx resolve)
– Sick staff stay home until 48 hrs after sx resolve
– Alcohol in, soap& water out
Vaccine?
• Challenging due to rapid evolution of antigenic variants and short‐lived immunity
• Ligocyte (acquired by Takeda): in phase II clinical trials
• Vaxart: VP1 protein‐based norovirus oral tablet vaccine in phase I trials
Norovirus: The perfect pathogen?
• Highly contagious
• Rapidly & prolifically shed
• Constantly evolving
• Evokes limited immunity
• Only moderately virulent—doesn’t kill host
Planning your next cruise….Cdc vessel sanitation site
2016
2/14/2017
10
CID 2010; 50:133‐164
IDSA guidelines 2009 A few definitions
• Complicated intra‐abdominal infection: “extends beyond hollow viscus of origin into peritoneal space and is associated w/abscess formation or peritonitis”
More definitions
• Mild‐moderate severity community acquired (CA) infection
• Severe CA infection: – age >70
– medical comorbidities
– poor nutritional status
– major peritoneal soilage or multiple abscesses
– patient hemodynamically unstable
– source control delayed or not feasible
• HA associated
– invasive device
– h/o MRSA infxn or colonization
– h/o surgery, hospitalization, dialysis, or LTHCF in previous 12 mos
Case
• 44F with no prior medical history presents to ED with several hrs of diffuse abdominal pain and chills.
• Tc 37.8C, HR 85, BP 140/80, SaO2 100% RA.
• WBC 16K, other labs normal. UA and pregnancy test negative.
• Empiric Abx?
• If so, which ones

2/14/2017
11
Source control
• Diffuse peritonitis due to perforated viscous is a surgical urgency
• If possible, percutaneous drainage of abscesses is preferred– But not if there is a perforated viscous
• Not enough data to support specific approaches
– E.g. extent of resection/debridement, anastamosis vs. ostomy, what tissue is debrided, wound management technique
• Highly selected patients who are clinically stable with a well‐circumscribed focus of infection may be treated with antibiotics alone, provided that very close follow‐up is possible
Solomkin JS et al., Clin Infect Dis ; 2010 ; 501 : 133 ‐164
Abx selection
• Empiric rx according to predicted flora and likelihood of abx resistance– Narrower spectrum for mild‐mod CA infxns
– Broader coverage (MDR GNR, enterococcus, yeast) for severe HCA infxns
Oral flora
Miami beach for bacteria
Microbiology
• Organisms identified in 3 randomized prospective studies (N=1237)
• Bacteremia is uncommon– 0‐5%, more likely
in critical illness
Solomkin JS et al., Clin Infect Dis ; 2010 ; 501 : 133 ‐164
Organism % of pts
Escherichia coli 71
Klebsiella species 14
Pseudomonas aeruginosa 14
Proteus mirabilis 5
Enterobacter species 5
Bacteroides fragilis 35
Other Bacteroides species 71
Clostridium species 29
Prevotella species 12
Peptostreptococcus species 17
Fusobacterium species 9
Eubacterium species 17
Streptococcus species 38
Enterococcus species 23
Staphylococcus aureus 4
Does she need antibiotics now?
• Cholangitis – decreased rates of complication
• Cholecystitis – lack of data, but usually done
• Diverticulitis – no longer routinely recommended in mild uncomplicated disease (but lowest level of evidence)
• Appendicitis – generally yes.
– Select cases: abx preferred over surgery, but this approach still not widely recommended)
IDSA guidelines: Antibiotics indicated as soon as Dx of hollow viscus infection/rupture is made or suspected – within 1 hr for septic patients, within 8 hrs for hemodynamically stable pts
Gastroenterology 2015;149:1944 – 1949.

2/14/2017
12
Case continued…
• CT scan ‐> cholecystitis.
• Surgery planned for tomorrow.
• NKDA.
• Which antibiotics?
Empiric therapy for mild to mod CA infections at UCSF
Severity Drug(s) of First Choice Severe PCN allergy
Mild‐ModerateCA
Ertapenem 1g IV dailyOR
Piperacillin/tazobactam3.375 g IV ‐ 4.5g IV q6h
VancomycinPLUS
Aztreonam 2 g IV q8hPLUS
Metronidazole 500 mg IV q8h
Severe CA
VancomycinPLUS
Piperacillin/tazobactam4.5 g IV q6h
VancomycinPLUS
Aztreonam 2 g IV q8hPLUS
Metronidazole 500 mg IV q8h
UCSF IDMP website.Do not need to cover Pseudomonas, Enterococcus, yeast
Case continued…
• Ertapenam started
• Successful cholecystectomy
• Doing well POD2, ready for d/c
• How long to continue abx?
Duration of therapy
• If no perforation or evidence of abscess, d/c abx 24 hrsafter surgery –
• No evidence to use abx prophylaxis for the drain!

2/14/2017
13
Case continued…
• Pt dc’d home
• Next day, surgeon calls. Intraoperative tissues sent for culture growing Enterococcus species (among other things)
• Pt is clinically stable
• Were cultures appropriate?
• Do you need to restart abx?
• Does enterococcus need to be covered?
Role of intra‐operative cultures
• Cultures optional in low risk CA infection, but “may be of value in detecting epidemiological changes in resistance patterns”
• Anaerobic cultures not necessary if abx regimen covers anaerobes
• Gram stain generally NOT useful in CA infections, but may be useful in HA infections if yeast is shown
• For low risk CA infections, uncovered organisms do not need to be covered unless pt fails to improve
• For severe or HA infections, consider on case‐by‐case basis
How should micro data guide treatment?
• If good response to source control and initial abx, no need to change even if untreated organisms are found
• Use micro to guide therapy if not responding well to empirical abx
• For severe or HCA infections, pathogenic potential and density of organisms should be considered
Solomkin JS et al., Clin Infect Dis ; 2010 ; 501 : 133 ‐164
Role of Enterococcus
• Unclear role as pathogen, no good studies
• Found in 20% of intra‐abdominal infections
• Regimens that don’t cover enterococcus work for community acquired infections
2/14/2017
14
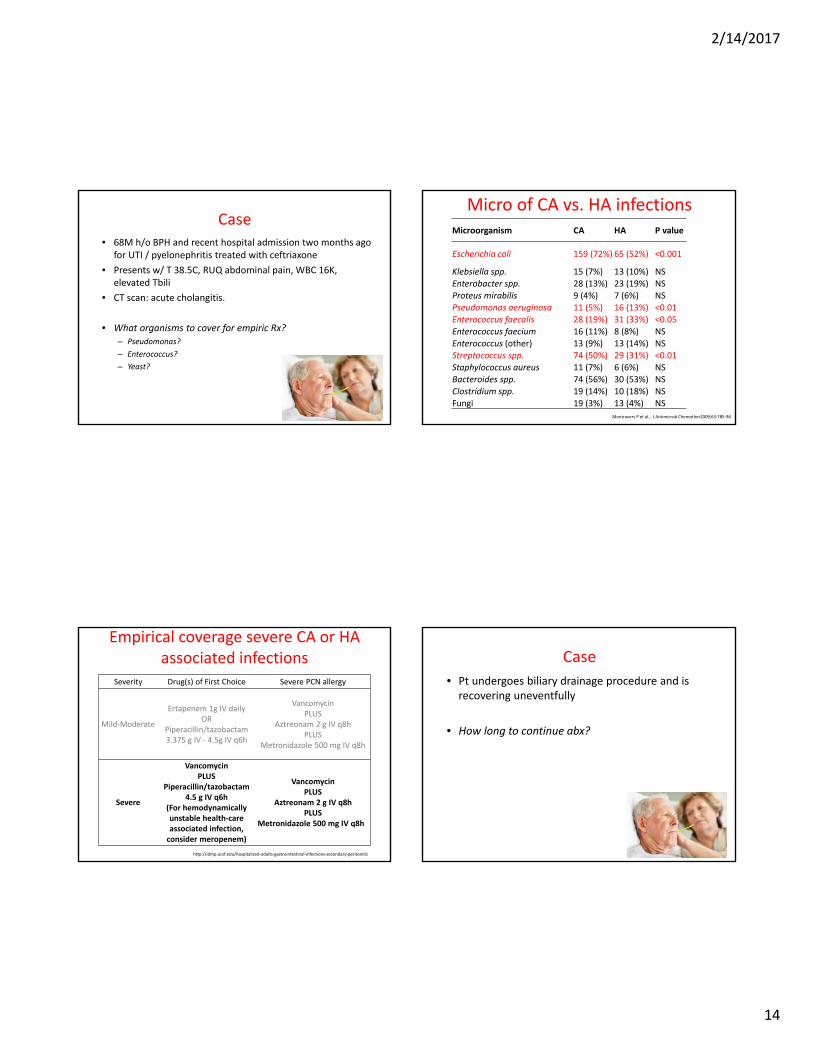
Case• 68M h/o BPH and recent hospital admission two months ago
for UTI / pyelonephritis treated with ceftriaxone
• Presents w/ T 38.5C, RUQ abdominal pain, WBC 16K, elevated Tbili
• CT scan: acute cholangitis.
• What organisms to cover for empiric Rx?– Pseudomonas?
– Enterococcus?
– Yeast?
Micro of CA vs. HA infectionsMicroorganism CA HA P value
Escherichia coli 159 (72%) 65 (52%) <0.001
Klebsiella spp. 15 (7%) 13 (10%) NSEnterobacter spp. 28 (13%) 23 (19%) NSProteus mirabilis 9 (4%) 7 (6%) NSPseudomonas aeruginosa 11 (5%) 16 (13%) <0.01Enterococcus faecalis 28 (19%) 31 (33%) <0.05Enterococcus faecium 16 (11%) 8 (8%) NSEnterococcus (other) 13 (9%) 13 (14%) NSStreptococcus spp. 74 (50%) 29 (31%) <0.01Staphylococcus aureus 11 (7%) 6 (6%) NSBacteroides spp. 74 (56%) 30 (53%) NSClostridium spp. 19 (14%) 10 (18%) NSFungi 19 (3%) 13 (4%) NS
Montravers P et al., J Antimicrob Chemother2009;63:785‐94
Empirical coverage severe CA or HA associated infections
Severity Drug(s) of First Choice Severe PCN allergy
Mild‐Moderate
Ertapenem 1g IV dailyOR
Piperacillin/tazobactam3.375 g IV ‐ 4.5g IV q6h
VancomycinPLUS
Aztreonam 2 g IV q8hPLUS
Metronidazole 500 mg IV q8h
Severe
VancomycinPLUS
Piperacillin/tazobactam4.5 g IV q6h
(For hemodynamically unstable health‐care associated infection, consider meropenem)
VancomycinPLUS
Aztreonam 2 g IV q8hPLUS
Metronidazole 500 mg IV q8h
http://idmp.ucsf.edu/hospitalized‐adults‐gastrointestinal‐infections‐secondary‐peritonitis
Case
• Pt undergoes biliary drainage procedure and is recovering uneventfully
• How long to continue abx?

2/14/2017
15
Abx duration
• If complicated infection (perforation, phlegmon),abx for 4 – 7 d “unless unable to achieve adequate source control” – How short can you go?
• Consider longer duration + reimaging / cultures + change abxif poor clinical response, or in more complex hosts (immunocompromised, etc)
STOP‐IT: Study To Optimize Peritoneal Infection Therapy
• Open‐label multicenter randomized trial of 518 patients with complicated intra‐abdominal infection
• Source control intervention was carried out (surgery or drainage)
– Not well specified in study
• Control group: Abx until 2 d post resolution of fever, WBC < 11K, resumption of PO diet.
• Experimental group: 4 d Abx after source control procedures
• Primary outcome: composite of surgical site infection, recurrent intra‐abdominal infection, or death
• Secondary outcome: Duration of antibiotic therapy
STOP‐IT trial. Sawyer, et al. N Engl J Med. 2015;372(21):1996
STOP‐IT Results
• No difference in composite primary endpoint – 21.8% of experimental group vs. 22.3% control (p = 0.92)
• Duration of abx 4 d vs 8 d (p = <0.001)
• Adherence to protocol 82% experimental vs 73% control
Conclusion: For patients who achieve source control procedure, 4 days of abx adequate
STOP‐IT trial. Sawyer, et al. N Engl J Med. 2015;372(21):1996
Enterococcus – when to cover
• Definitely: positive blood cultures
• Maybe: Enterococcus recovered in abd fluid cultures in HA infxn
• Per IDSA, strongly consider in:
‐ Immunocompromised patients
‐ Health care‐associated postoperative peritonitis
‐ Severe sepsis who have previously received cephalosporinsand other broad‐spectrum antibiotics selecting for Enterococcus species
‐ Valvular heart disease or prosthetic intravascular material (risk of endocarditis)
• Do NOT need to empirically cover VRE unless high index of suspicion

2/14/2017
16
Role of MRSA
• Quite rare in CA intra‐abd infections – guidelines do NOT recommend empiric coverage
• Per IDSA: “Empiric antimicrobial coverage directed against MRSA should be provided to patients with health care–associated intra‐abdominal infection who are known to be colonized with the organism or who are at risk of having an infection due to this organism because of prior treatment failure and significant antibiotic exposure”
• Would consider adding anti‐MRSA coverage in HD unstable patients (treat as per sepsis guidelines)
Role of Yeast
• C. albicans found in ∼20% of patients with acute perforations of GI tract
• Does not always need to be treated
• Definitely treat:
‐ Positive blood cultures
‐ Immunocompromised patients
‐ GI perforation on PPI
‐ Postoperative infection
‐ Recurrent intra‐abdominal infection
• Consider in:
– Pancreatitis surgery (empirically)
– Heavy growth from intra‐op cultures
Anti‐fungal Rx
• C. albicans: fluconazole
• Rising rates of non‐albicans Candida (C. glabrata, C. krusei, etc) for HD unstable patients, use echinocandins until yeast ID is known
• C. parapsilosis, C. lusitaniae, C. guilliermondii, C. orthopsilosis have decreased susceptibility to echinocandins!
Case
• 26M prev healthy
• high‐speed MVA with blunt trauma, intra‐abdominal perforation.
• Started on empiric antibiotics and undergoes urgent surgical repair.
• Now clinically stable.
• Abx for how long?

2/14/2017
17
Indications for <24 hours of abx Rx
• Traumatic injuries repaired within 12 hrs
• Intra‐op contamination
• Acute upper GI perforations (stomach, duodenum, proximal jejeunem) in absence of antacid therapy or malignancy
• Uncomplicated acute appendicitis with repair
A word on pancreatitis
• 80% of pancreatitis recover within 1 wk – Abx are NOT recommended for acute pancreatitis (mild or severe)
• 20% develop necrotizing pancreatitis ‐ roughly one‐third of these will develop superinfection (high mortality)
• Dx: Clinical deterioration or lack of improvement after ~10 days of supportive care. FNA for dx/micro recommended.
• Rx: controversial – empiric antibiotics vs targeted therapy via FNA/drainage vs necrosectomy
• Often involves multiple procedures
• Length of Rx by clinical improvement
Consistent principles
• Prophylactic abx (< 24 hrs duration)
– Traumatic injuries repaired within 12 hrs
– Intra‐op contamination
– Acute perfs of stomach, duodenum, proximal jejeunem in absence of antacid therapy or malignancy
– Uncomplicated acute appendicitis
• Treatment abx (>24 hrs):until resolution of clinical signs of infxn
– STOP‐IT study: or 4 days, if adequate source control
• W/u if no response after 5‐7 d of rx
• enterococcus, yeast only need to be treated in specific situations
Intra‐abdominal Infections take‐home
• Source control is crucial
• Cover aerobic and anaerobic GPCs and GNRs
– Enterococcus if HA post‐surgical, immunocompromised, prosthetic material, severe infection, prior cephalosporins
– MRSA if hospital‐acquired or known carrier
– Yeast if HA post‐operative, pancreatitis associated, perf on PPI, immunosuppressed
• Shorter courses of antibiotics may be possible if source control is achieved and symptoms of infection resolve

2/14/2017
18
Updated treatment recs H. pylori
• Increasing therapy failure for H. pylori
• Recommended 1st line Rx is quadruple therapy x 14 D
– Unless known low clarithro resistance or known local efficacy of 3 drug regimens
• Rifabutin regimens restricted to pts who failed to respond to 3 prior options
Fallone et al, Gastroenterology, 2016
Recommended regimens
Dosing