hiv-related infections, co-infections and …hivarchive.com/hiv11/uploads/hiv-related infections...
TRANSCRIPT
P154 High acceptability of cognitive screening in HIV-infected patients: a pilot studyFasel, D; Kunze, U; Monsch, A; Battegay, M* (Basel, Switzerland)
P156 Syphilis in HIV-infected patients: predictors for serological failure and serofast statePalacios, R*; Navarro, F; Moreno, T; Ruiz, J; Nuño, E; Márquez, M; Santos, J (Málaga, Spain)
P157 Role and interpretation of FDG-PET/CT in HIV patients with fever of unknown origin: a prospective studyMartin, C*; Castaigne, C; Tondeur, M; Flamen, P; De Wit, S (Brussels, Belgium)
P158 Kidney transplantation in HIV-positive patients: a report of 14 casesCasari, S*; Bossini, N; Albini, L; Setti, G; Valerio, F; Izzo, I; Costarelli, S; Sandrini, S; Cancarini, G; Castelli, F (Brescia, Italy)
P159 STI screening in people living with HIV: are we getting the whole story?Perez, K*; Bassett, D; Schembri, G; Lee, V (Manchester, UK)
P161 Infections and cancer after ARV: a Portuguese cohortPereira, N*; Caldas, C; Azevedo, C; Andrade, P; Serrão, R; Sarmento, A (Porto, Portugal)
P162 Hospitalisation causes of HIV-infected patients in 2011 in an HIV reference center in the Paris region, FranceRapp, C*; Reggad, A; Aoun, A; Ficko, C; Andriamanantena, D; Flateau, C (Saint Mandé, France)
P163 Aspergillosis in HIV patients: a case seriesLaurent, F; Martin, C*; De Wit, S (Brussels, Belgium)
HIV-RELATED INFECTIONS, CO-INFECTIONS AND
CANCERS – OTHER
*Indicates presenting author.
High Acceptability of a Cognitive Screening Test Batteryin HIV-infected Patients, a Pilot Study
Dominique Fasel 1, Ursula Kunze 2, Andreas U. Monsch 2, Manuel Battegay 1
1 Div. of Infectious Diseases & Hospital Epidemiology and 2 Memory Clinic, University Hospital Basel, Switzerland
Background• Identifying neurocognitive deficits in ageing HIV-infected
individuals is important.• This study aimed to evaluate the acceptability of screening
neurocognitive deficits in HIV-infected patients evaluating ashort screening test battery validated with an in depth neuro-psychological examination.
Methods• 30 patients (26 men, 4 women) from the HIV clinic were
examined with a new screening test battery and a neuro-psychological examination.
• The screening tests consisted of questions and exami-nations on cognition in everyday situations, mood andselected cognitive functions:- word list memory, grooved pegboard, psychomotor
speed, trail making test, psychomotor speed and exe-cutive functions, digit symbol test.
• The screening was defined as pathological if patients hadmore than one pathological domain in the test.
• The neuropsychological examination covered the following tasks:- MMS, clock time, BVLT; 5 point test, Corsi blocks, Ra-
venʼs matrices, Wisconsin Card Sorting Test, Rey figure,verbal fluency (semantic and phonematic), BostonNaming Test, repeating numbers, Colour Trails, apraxiatest and Stroop.
• Patients (a) and nurses (b) received a questionnaire toevaluate test acceptance:
(a) Is the test too difficult?, are the instructions under-standable?, too much privacy?, is the screening rea-sonable?, is the test burdening?, are you interested inthe results?, is the test duration too long?
(b) Is the test too difficult for patients?, is the screening rea-sonable?, is the test burdening for the study nurse?, isthe test duration too long?
• The screening test was performed by the assistance of anurse and lasted 26 minutes in average (mean, range 19-33).
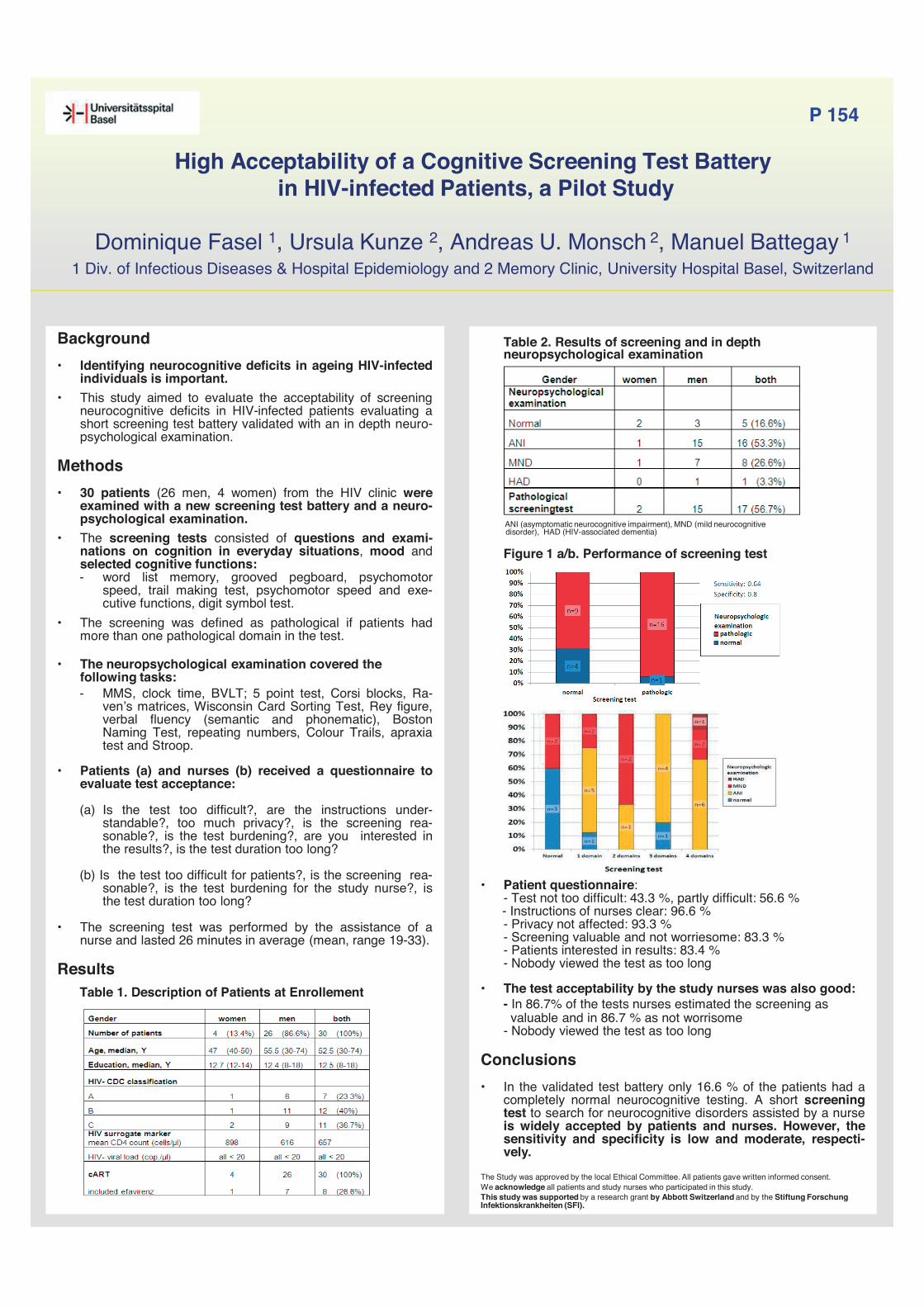
ResultsTable 1. Description of Patients at Enrollement
Table 2. Results of screening and in depth neuropsychological examination
ANI (asymptomatic neurocognitive impairment), MND (mild neurocognitivedisorder), HAD (HIV-associated dementia)
Figure 1 a/b. Performance of screening test
• Patient questionnaire:- Test not too difficult: 43.3 %, partly difficult: 56.6 %- Instructions of nurses clear: 96.6 %- Privacy not affected: 93.3 %- Screening valuable and not worriesome: 83.3 %- Patients interested in results: 83.4 %- Nobody viewed the test as too long
• The test acceptability by the study nurses was also good:- In 86.7% of the tests nurses estimated the screening asvaluable and in 86.7 % as not worrisome
- Nobody viewed the test as too long
Conclusions• In the validated test battery only 16.6 % of the patients had a
completely normal neurocognitive testing. A short screeningtest to search for neurocognitive disorders assisted by a nurseis widely accepted by patients and nurses. However, thesensitivity and specificity is low and moderate, respecti-vely.
The Study was approved by the local Ethical Committee. All patients gave written informed consent.We acknowledge all patients and study nurses who participated in this study. This study was supported by a research grant by Abbott Switzerland and by the Stiftung ForschungInfektionskrankheiten (SFI).
P 154

RESULTS
Episodes of syphilis 141 • Early 104 (73.7%) • Late or indeterminate latent 37 (26.2%)
Epidemiological and clinical data of the 141 cases
Male sex 139 (98.5)
Homosexual men 123 (87.2)
Age (years) 36.3 (29.7-46.1)
HBV/HCV coinfection 23 (16.3)
Coincident diagnosis with HIV infection 46 (32.6)
CD4/mm3 at the time of syphilis 476 (252-621)
On ART at the time of syphilis 67 (70.5)*
HIV VL prior to syphilis < 50 cop/mL 50 (74.6)**
First episode 109 (77.3)
Clinical presentation • Asymptomatic • Chancre • Secondarism • Others
55 (39.0) 17 (12.1) 61 (43.3)
8 (5.7)
RPR > 1/64 61 (43.3)
Lumbar punction • Abnormal CSF
39 (27.7) 10 (25.6)
*Of the 95 patients with prior diagnose of HIV infection. **Of the 67 patients on ART. Quantitative variables are expresed as mean (IQR) and qualitative data as n (%)
Table 1. Comparison between patients with and without serological failure
Failure 21 (18.1)
Response 95 (81.8)
p
Age (years) 36.9 (29.0-47.0) 36.3 (29.5-45.6) 0.7 HBV/HCV coinfection 3 (14.8) 13 (13.6) 1.0
Coincident 6 (28.5) 33 (34.7) 0.7 First episode 18 (85.7) 75 (78.9) 0.7 Syphilis stage • Early • Late/indeterminate
16 (76.1) 5 (23.8)
73 (76.8) 22 (22.9)
1.0
Asymptomatic 6 (28.5) 39 (41.0) 0.3
RPR > 1/64 9 (42.8) 42 (44.2) 1.0 First line tratment 17 (80.9) 79 (83.1) 0.4 CD4/mm3 412 (212-545) 480 (296-661) 0.09 On ART* 9 (60.0) 46 (74.1) 0.8 HIV VL < 50 cop/mL** 8 (88.8) 32 (69.5) 1.0
Table 2. Comparison between patients with and without serofast state
In this series of HIV-infected patients, with many patients on ART and with good immunological and virological parameters, serological failure and serofast state were frequent.
Immunological status, and age could influence on serological response to syphilis treatment in HIV-infected patients.
CONCLUSIONS
References: 1. Palacios R, et al. Serological response to syphilis treatment in HIV-infected patients. Factors related to serological failure. EACS 2007 (P13.4/02). 2. Kim JH, et al. Factors influencing syphilis treatment failure and/or re-infection in HIV co-infected patients: immunosuppression or behaviors. Chinese Medical Journal 2011. 3. Seña AC, et al. Predictors of serological cure and serofast state after treatment in HIV-negative persons with early syphilis. Clin Infect Dis 2011.
Syphilis in HIV-infected patients: predictors for serological failure and serofast state
R. Palacios, F. Navarro, T. Moreno, J. Ruiz, E. Nuño, M. Márquez, J. Santos. UGC Enfermedades Infecciosas and IBIMA. Hospital Virgen de la Victoria. Málaga (Spain)
INTRODUCTION Because syphilis and HIV infections are both sexually transmitted infections (STI), coinfection is not rare. HIV-infected patients treated for syphilis may be at increased risk for serological failure and serofast state. The aim of this is study was to analyse serological response to treatment in HIV-infected patients diagnosed with syphilis, and factors associated with serological cure and serofast state.
PATIENTS AND METHODS Design of the study: open-label, no controlled, observational study. Study population: all HIV-patients who have been diagnosed with syphilis in our
hospital during 2004-2011. Definitions:
• Serological response: 4-fold decrease in RPR by 12 or 24 months after treatment of early or late syphilis.
• Serofast: success with persistently stable reactive RPR. • Failure/re-infection: failure to decrease 4 folds in RPR by 12 or 24 months
after treatment or sustained 4-fold increase in RPR after treatment response Statistic analysis (SPSS program)
• Comparison between patients with and without treatment serological failure • Comparison between patients with and without serofast state
P 156
Treatment and serological evolution*
First line treatment (penicillin) • Early • Late/indeterminate latent
111 (89.5) 93 (89.2) 34 (91.7)
Months of serological follow up 14.4 (12.0-18.9)
Serological response 95 (81.8)
Serological failures • Early • Late/indeterminate latent
21 (18.1) 16 (18.0) 5 (18.5)
Serofast state 36 (31.0)
*116 patients satisfied criteria for serological response analysis. Qualitative variables are expresed as n (%)
*Of the patients with prior diagnose of HIV infection. **Of the patients on ART. Quantitative variables are expresed as mean (IQR) and qualitative data as n (%)
Serofast 36 (31.0)
No serofast 80 (68.9)
p
Age (years) 40.9 (32.8-47.6) 33.8 (27.5-45.5) 0.02 HBV/HCV coinfection 5 (13.8) 7 (8.7) 0.7
Coincident 11 (30.5) 23 (28.7) 0.5 First episode 28 (77.7) 49 (61.2) 0.5 Syphilis stage • Early • Late/indeterminate
28 (77.7) 8 (22.2)
46 (57.5) 13 (16.2)
1.0
Asymptomatic 14 (38.8) 22 (27.5) 1.0
RPR > 1/64 17 (47.2) 24 (30.0) 0.6 First line tratment 28 (77.7) 52 (65.0) 0.09 CD4/mm3 389 (193-535) 535 (314-691) 0.02 On ART* 19 (76.0) 27 (47.3) 0.5 HIV VL < 50 cop/mL** 12 (63.1) 21 (77.7) 0.2
*Of the patients with prior diagnose of HIV infection. **Of the patients on ART. Quantitative variables are expresed as mean (IQR) and qualitative data as n (%)

P157: Role and interpretation of FDG-PET/CT in HIV patients with Fever of Unknown Origin: a prospective study
Ch. Martin1, C. Castaigne2-3, M. Tondeur2, P. Flamen3, S. De Wit1
Saint-Pierre University Hospital, Department of Infectious Diseases1, Nuclear Medicine2
Iris-Bordet PET-scan Unit3, Brussels, BelgiumE-mail : [email protected]
Purpose of the study
Fever of unknown origin (FUO) is a challenging clinicalentity in HIV patients. FDG-PET/CT is well validated inthe work-up of FUO in HIV negative patients.Metabolism of HIV reactive lymph nodes can decreasespecificity of FDG-PET/CT in viremic patients.The aim of this study is to evaluate prospectivelyusefulness of FDG-PET/CT in investigation of FUO inHIV positive patients and whether HIV viremia impactson FDG-PET/CT performance.
Methods
Analyze of FDG-PET/CT of 20 HIV positive patients withFUO and comparison with FDG-PET/CT of 10 HIVviremic patients without FUO. Final diagnosis for FUOwas based on histopathology, microbiologic assays, orclinical and imaging follow-up. Mode of diagnosis,accordance of FDG-PET/CT with final diagnosis,localization of invasive diagnosis procedures wasrecorded in order to assess usefulness of FDG-PET/CT.
Summary of results
FDG-PET/CT of asymptomatic patients showed adifferent pattern from FUO patients. Reactive HIVlymph nodes in asymptomatic patients were mostlyperipheral (mean SUVmax 6.5). In patients with FUOand underlying focal pathologies, we observed centralhypermetabolic lymph nodes with mean SUVmaxof 11.6.Presence of high FDG uptake in central lymph nodehas 100% specificity for focal pathology, even inviremic patients and absence of these has 100%negative predictive value.When possible, lymph node biopsy in centralhypermetabolic areas allowed identifying underlyingdisease in all FUO patients.For peripheral lymph nodes, a ROC curve was built inorder to define the best cut off of SUVmax for biopsy:SUVmax of 6-8 showed a sensitivity of 62.5% andspecificity of 75%.
DIAGNOSIS (n)Peripheralmean SUVmax
Centralmean SUVmax
ConclusionsFDG-PET/CT excluded or led directly to focal etiology of the febrile state in 80% of HIV p. with FUO.Although number of patients was small, we could highlight several features to help interpretingFDG-PET/CT in HIV patients with FUO. As in HIV negative p., FDG-PET/CT is highly performant inFUO in HIV p. even if they are viremic.
A) FUO patient: infection with atypical mycobacteria. FDG-PET/CT shows intense FGD uptake in central (abdominal) and peripheral (one subclavicular) lymph nodes
B) Viremic patient without FUO: moderate FDG uptake is observed in cervical (SUVmax 5.1), axillary (2.8) and mediastinal lymph nodes (3.8)
A) B)
n/10 MeanSUVmax
Peripheral LN Cervical 9 5.5 (3.6- 8.8)
Axillary 8 5.1 (2.3- 11.2)
Iliac 5 4.7 (3.3- 7.2)
Inguinal 7 3.6 (2.2- 5.1)
Central LN Mediastinal 1 3.80
Group 1 FUO patients
Group 2 asymptomatic patients
DIAGNOSIS (n) mean SUVmax mean SUVmax
Tuberculosis (8) 9.3 13,1
Non tuberculous mycobact. (3) 14.7 (n=1) 15,4
Non focal pathol. (4) 4,7 3.1 (n=1)
Non Hodgkin Lymphomas (2) 7,4 4,8
Hodgkin Lymphomas (1) 22 (n=1) 18 (n=1)

Presented at HIV11th 2012 – Glasgow, UK
Materials and methods We reported the results of kidney Tx in HIV positive patients from deceased donors from June 2007 to March 2012 at our Institution.
All the patients had to have CD4+ T-cell counts ≥200/mm3 and, if on cART, undetectable plasma HIV-RNA. The induction immunosuppressive therapy consisted of metilprednisolone and basilixmab; tacrolimus and/or mycofenolic acid were used for maintenance therapy. The therapeutic drug monitoring (TDM) has been performed for the adjustment of both their doses [1].
Introduction Although the combined antiretroviral therapy (cART) reduced the risk of HIV-associated nephropaty, the incidence of end-stage renal disease (ESRD) remains elevated. Therefore, efficacy and safety of renal transplantation (Tx) is an important resource in the HIV-infected population.
Results A total of 14 patients underwent kidney Tx. They have been on dialysis (haemo- = 13, peritoneal- = 1) for 5 3 years and they have been included on the Tx waiting list for 10 8 months. The baseline characteristic are showed in Table 1.
At the last available point of follow-up (median=42.8 months, IQR=8.5-55.2), 8 out of the 13 patients (61.6%) without steroid had at least one acute rejection episode, but only 1 patient lost the graft after 43 months, due to chronic rejection associated with infectious and vascular complications. After the Tx the median CD4+ T-cell count increased from 382.5 (IQR=233-415) to 434 (IQR=282-605) cells/mm3 (p=0.055). In figure 1 are reported the CD4+ trends of 9 patients with a follow-up of at least 6 months.
Spedali Civili of Brescia
Kidney Transplantation in HIV-positive patients: a report of 14 cases
Salvatore Casari1, Nicola Bossini2, Laura Albini1, Gisella Setti2, Francesca Valerio2,
Ilaria Izzo1, Silvia Costarelli1, Silvio Sandrini2, Giovanni Cancarini2, Francesco Castelli1
1Clinic of Infectious and Tropical Diseases, Spedali Civili General Hospital, Brescia, Italy
2Unit of Nefrology, Spedali Civili General Hospital, Brescia, Italy
Conclusions Kidney Tx appears to be safe in HIV-positive
patients undergoing cART.
The viro-immunological parameters remained well
controlled with no increases in infectious
complications or cancers and with a satisfactory
control of HIV infection.
However, the high rejection rate is a serious
concern and suggests to consider a steroid-
containing immunosuppressive regimen also in HIV-
infected subjects.
HIV infection was well controlled, with only 2 (14.3%) cases of virological failure which were promptly resolved after cART regimen modification. Table 2 shows the observed infectious complications. The skin Kaposi Sarcoma has been resolved by switching to immunosuppresive therapy with sirolimus [2].
1. Trullas JC, et al. Kidney Int. 2011; 79:825-842 2. Gheith O, et al. Clin Exp Nephrol. 2007; 11:251-254

Sexual health screening in people living with HIV – Are we getting the whole story?
K Perez, D Bassett, G Schembri, V LeeManchester Centre for Sexual Health, Central Manchester University Hospitals NHS Foundation Trust, UK
• PeoplelivingwithHIVareabletoenjoymeaningfulsexualrelationships.Thereremainshoweverthekeyresponsibilityofreducingtransmissiontoothersandwithinthisthepreventionandmanagementofsexuallytransmittedinfections(STIs).
• NewcasesofSTIsthataredetectedinknownHIVinfectedpeopleareindicativeofongoingriskysexual
behaviourandpotentialHIVtransmission.AmongHIV-diagnosedmenwhohavesexwithmen(MSM),7.6%presentedwithanacuteSTIwithinayearoftheirdiagnosis.(1)
• In2008and2011BHIVApublishedguidanceonSTItesting,recommendingannualSTIscreeningregardlessoftheirreportedhistory.(2,3)
• Weconductedaretrospectivecasenotereviewof385HIVpositivepatientspresentingforroutineHIVcareinalargecityteachinghospitalHIVclinicduring2010.
• Informationincludingdemographics,HIVparameters,sexualhistoryandSTIscreeningwascollected.
Table1.Patientdemographiccharacteristics.
Patient Characteristics Male 296 (77%) MSM 245 Female 89 (23%) Median age (range) years 37 (17-75) Median year of diagnosis(range) 2005 (1998-2010) Median CD4 (range) cells/mm3 467 (1-1848) HIV viral load <40 copies /ml 248 (64%) On HAART 296 (77%) HBV co-infection 18 (4.7%) HCV co-infection 17 (4.1%)
Figure1Patientethnicity-58%whiteBritish,27%BlackAfricanand 7% other white.
Figure 2. HIV risk factors - 63% were MSM, 34% heterosexual, 2% bisexual and 1% IVDU.
• 249(65%)patientshadatleast1STIscreeninthepast12months.56(14%)declinedtestingand77(21%)werenotofferedastheywereinaregularrelationshipornotsexuallyactive.
Figure 3 STI screen offered in the last 12 months
Figure 4 Asymptomatic STI screens performed in the past 12 months
Figure 5 Symptomatic STI screens performed in the past 12 months.
Figure 6 Number of patients with regular partner(s)
Figure 7 HIV status of the regular partner - 44% known HIV positive & 49% HIV negative.
Figure 8 Serosorting occurred in only 3% of patients.
Figure9
• Figure9Self-reportedcondomuse.69%reportedalwaysusedcondomsforvaginalsex,68%foranaland11%fororalsex.
Figure10STIdiagnosedinMSM
• TherewerenoSTIsdiagnosedinheterosexualmalesandfemales.Figure10showedthenumberofepisodesofSTIsdiagnosedinMSM.Rectalinfections(Chlamydia,LGV,andGC)indicatedunsafesex.
Figure 11 Infections in MSM reporting consistent condom use for anal sex.
• 160reportedconsistentcondomuseforanalsex,ofthese15%hadrectalSTIsdiagnosed(Figure11).45%ofpatientsreportedmonogamousrelationshipover12months.6.4%ofthesehadSTIs.
Figure 12. Other STIs diagnosed Figure 13 shows the number of patients in
a regular relationship that also reported casual partners.
• RoutineSTIscreeningisofferedannuallyinthemajorityofourcohortwithreasonableuptakerates.
• STIsarestillbeingdiagnosedinpeoplelivingwithHIVdespiteourrepeatedsafersexmessagesandsignificantlyinthosewithconsistentself-reportedcondomuse.InourcohortthiswasalmostexclusivelyinMSM.
• 23%ofthosewithregularpartnersalsoreportconcurrentcasualpartner(s)makingitimportanttotakeafullsexualhistoryandemphasisesafersexmessagesateachvisit.
• STIscreeningshouldbeofferedannuallyeveninthosereportingmonogamousrelationshipsassignificantnumbers(6.4%)werediagnosedwithanSTI.Morefrequentscreeningshouldstillbeoffereddependantonsexualhistory.
• NewHCVco-infectionarebeingdiagnosedinHIVpositiveMSM.HCVantibodyserologyshouldbedocumentedatbaselineandthenyearly.InindividualsorgroupsatincreasedriskofHCV(MSM),HCVserologyshouldbeconsideredwitheachroutineHIVfollow-up(4).
1. PetersL,HughesG,BrownA,etal.IncidenceofacuteSTIsinHIV-infectedpersonsreceivingHIVcare–preventionfailure?OralpresentationatthesecondjointconferenceofBHIVAandBASHH20-23April2010,ManchesterCentralConventionComplex.
2. FakoyaA,LambaH,MackieNetal.BritishHIVAssociation,BASHHandFSRHguidelinesforthemanagementofthesexualandreproductivehealthofpeoplelivingwithHIVinfection2008.HIVMed2008;9:681–720.
3. AsboeD,AitkenC,BoffitoMetal.BritishHIVAssociationguidelinesfortheroutineinvestigationandmonitoringofadultHIV-1-infectedindividuals2011.HIVMedicine(2012),13,1–44.
4. HealthProtectionAgency.SexuallytransmittedinfectionsinmenwhohavesexwithmenintheUK:2011Report.
Background
Discussion
Results
Method
References
0
50
100
150
200
250
160
40 36
13 13
215
92
1424
always
occasional
neveralways
occasional
neveralways
occasional
never
0
5
10
15
20
25
30
5
15
25
4
13
18
27
Chlamydia
Pharyngeal
UrethralRectal
Pharyngeal
UrethralRectal
LGV GC
STI’s Diagnosed in MSM
Infec'ons and Cancer a.er An'retroviral Therapy
Nuno Rocha Pereira, Carlos Azevedo, Paulo Andrade, Cá'a Caldas, Rosário Serrão, António Sarmento Infec'ous Diseases Service. Centro Hospitalar S. João & Oporto Medical School
Background The advent of an,retroviral therapy (ARV) resulted in a significant decrease in opportunis,c infec,ons; however these diseases s,ll represent an important cause of morbidity and mortality. ARV also changed the spectrum of cancers of HIV pa,ents as a result of immune recovery and increased life expectancy.
Methods Assessment and registry of the events (infec,ons and neoplas,c condi,ons) occurring aDer ini,a,on of ARV in a cohort of HIV-‐infected pa,ents who started ARV between January/2007 and December/2011. We included records of these events un,l March/2012. Epidemiological , c l inical and laboratorial data were analyzed and compared with a control group of HIV-‐infected pa,ents that started ARV in the same period but didn’t experienced those comorbidi,es. Pa,ents lost to follow-‐up were excluded. Sta,s,cal significance of the differences found was evaluated with T-‐student test and Chi-‐square test; differences were considered sta,s,cally significant when p<0,05.
Results
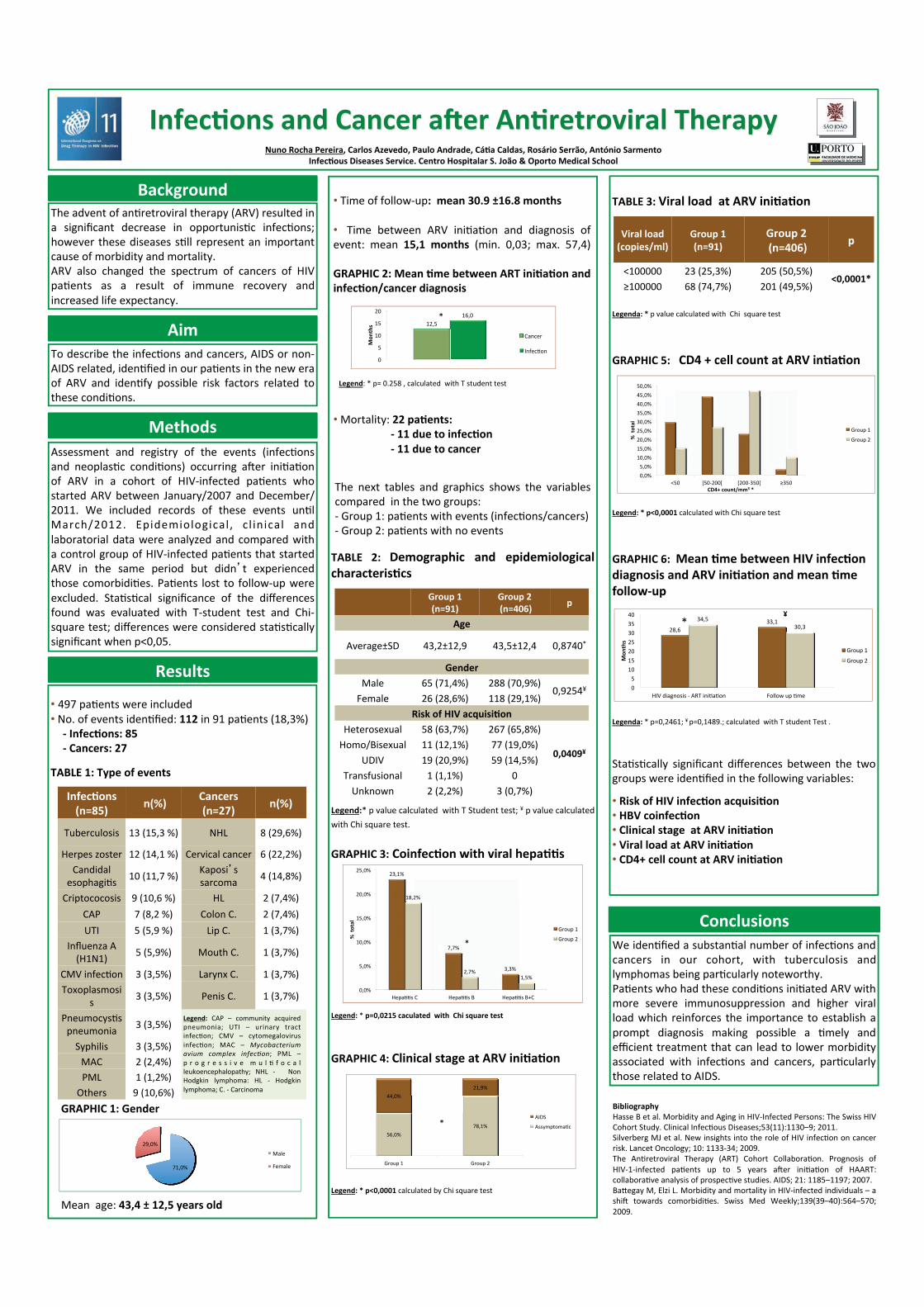
• 497 pa,ents were included • No. of events iden,fied: 112 in 91 pa,ents (18,3%)
-‐ Infec'ons: 85 -‐ Cancers: 27
TABLE 1: Type of events
TABLE 2: Demographic and epidemiological characteris'cs Legend:* p value calculated with T Student test; ¥ p value calculated with Chi square test. GRAPHIC 3: Coinfec'on with viral hepa''s Legend: * p=0,0215 caculated with Chi square test
GRAPHIC 4: Clinical stage at ARV ini'a'on Legend: * p<0,0001 calculated by Chi square test
Group 1 (n=91)
Group 2 (n=406) p
Age
Average±SD 43,2±12,9 43,5±12,4 0,8740*
Gender Male 65 (71,4%) 288 (70,9%)
0,9254¥ Female 26 (28,6%) 118 (29,1%)
Risk of HIV acquisi'on Heterosexual 58 (63,7%) 267 (65,8%)
0,0409¥
Homo/Bisexual 11 (12,1%) 77 (19,0%) UDIV 19 (20,9%) 59 (14,5%)
Transfusional 1 (1,1%) 0 Unknown 2 (2,2%) 3 (0,7%)
56,0% 78,1%
44,0% 21,9%
Group 1 Group 2
AIDS
Assymptoma,c
TABLE 3: Viral load at ARV ini'a'on Legenda: * p value calculated with Chi square test
GRAPHIC 5: CD4 + cell count at ARV in'a'on
Legend: * p<0,0001 calculated with Chi square test
GRAPHIC 6: Mean 'me between HIV infec'on diagnosis and ARV ini'a'on and mean 'me follow-‐up
Legenda: * p=0,2461; ¥ p=0,1489.; calculated with T student Test .
Sta,s,cally significant differences between the two groups were iden,fied in the following variables:
• Risk of HIV infec'on acquisi'on • HBV coinfec'on • Clinical stage at ARV ini'a'on • Viral load at ARV ini'a'on • CD4+ cell count at ARV ini'a'on
Viral load (copies/ml)
Group 1 (n=91)
Group 2 (n=406) p
<100000 23 (25,3%) 205 (50,5%) <0,0001*
≥100000 68 (74,7%) 201 (49,5%)
0,0% 5,0% 10,0% 15,0% 20,0% 25,0% 30,0% 35,0% 40,0% 45,0% 50,0%
<50 [50-‐200[ [200-‐350[ ≥350
% total
CD4+ count/mm3 *
Group 1
Group 2
28,6 33,1 34,5
30,3
0 5 10 15 20 25 30 35 40
HIV diagnosis -‐ ART ini,a,on Follow up ,me
Mon
ths
Group 1
Group 2
*
Conclusions We iden,fied a substan,al number of infec,ons and cancers in our cohort, with tuberculosis and lymphomas being par,cularly noteworthy. Pa,ents who had these condi,ons ini,ated ARV with more severe immunosuppression and higher viral load which reinforces the importance to establish a prompt diagnosis making possible a ,mely and efficient treatment that can lead to lower morbidity associated with infec,ons and cancers, par,cularly those related to AIDS.
¥
Aim To describe the infec,ons and cancers, AIDS or non-‐AIDS related, iden,fied in our pa,ents in the new era of ARV and iden,fy possible risk factors related to these condi,ons.
*
Bibliography Hasse B et al. Morbidity and Aging in HIV-‐Infected Persons: The Swiss HIV Cohort Study. Clinical Infec,ous Diseases;53(11):1130–9; 2011. Silverberg MJ et al. New insights into the role of HIV infec,on on cancer risk. Lancet Oncology; 10: 1133-‐34; 2009. The An,retroviral Therapy (ART) Cohort Collabora,on. Prognosis of HIV-‐1-‐infected pa,ents up to 5 years aDer ini,a,on of HAART: collabora,ve analysis of prospec,ve studies. AIDS; 21: 1185–1197; 2007. Bapegay M, Elzi L. Morbidity and mortality in HIV-‐infected individuals – a shiD towards comorbidi,es. Swiss Med Weekly;139(39–40):564–570; 2009.
Infec'ons (n=85) n(%) Cancers
(n=27) n(%)
Tuberculosis 13 (15,3 %) NHL 8 (29,6%)
Herpes zoster 12 (14,1 %) Cervical cancer 6 (22,2%) Candidal esophagi,s 10 (11,7 %)
Kaposi’s sarcoma 4 (14,8%)
Criptococosis 9 (10,6 %) HL 2 (7,4%) CAP 7 (8,2 %) Colon C. 2 (7,4%) UTI 5 (5,9 %) Lip C. 1 (3,7%)
Influenza A (H1N1) 5 (5,9%) Mouth C. 1 (3,7%)
CMV infec,on 3 (3,5%) Larynx C. 1 (3,7%) Toxoplasmosi
s 3 (3,5%) Penis C. 1 (3,7%)
Pneumocys,s pneumonia 3 (3,5%)
Syphilis 3 (3,5%) MAC 2 (2,4%) PML 1 (1,2%) Others 9 (10,6%)
Legend: CAP – community acquired pneumonia; UTI – urinary tract infec,on; CMV – cytomegalovirus infec,on; MAC – Mycobacterium avium complex infec4on; PML – p r o g r e s s i v e m u l , f o c a l leukoencephalopathy; NHL -‐ Non Hodgkin lymphoma: HL -‐ Hodgkin lymphoma; C. -‐ Carcinoma
• Time of follow-‐up: mean 30.9 ±16.8 months • Time between ARV ini,a,on and diagnosis of event: mean 15,1 months (min. 0,03; max. 57,4) GRAPHIC 2: Mean 'me between ART ini'a'on and infec'on/cancer diagnosis • Mortality: 22 pa'ents:
-‐ 11 due to infec'on -‐ 11 due to cancer
71,0%
29,0% Male
Female
GRAPHIC 1: Gender
Mean age: 43,4 ± 12,5 years old
The next tables and graphics shows the variables compared in the two groups: -‐ Group 1: pa,ents with events (infec,ons/cancers) -‐ Group 2: pa,ents with no events
*
Legend: * p= 0.258 , calculated with T student test
23,1%
7,7%
3,3%
18,2%
2,7% 1,5%
0,0%
5,0%
10,0%
15,0%
20,0%
25,0%
Hepa,,s C Hepa,,s B Hepa,,s B+C
% total
Group 1
Group 2 *
12,5 16,0
0
5
10
15
20
Mon
ths
Cancer
Infec,on
Hospitalization causes of HIV-infected patients in 2011 in an HIV reference center in the Paris region, France
C. RAPP, A. REGGAD, O. AOUN, C. FICKO, D. ANDRIAMANANTENA, C. FLATEAU
Infectious and tropical diseases department
Bégin military Hospital, 94163 Saint-Mandé, France
BACKGROUND
CONCLUSION
References
1. Rapport Yeni 2010 Prise en charge médicale des personnes infectées par le VIH, www.sante.gouv.fr
2. Berry SA, Fleishman JA, Moore RD et al. Trends in reasons for hospitalization in a multisite United States cohort of persons living with HIV, 2000-2008. J Acquir Immune Defic Syndr. 2012; 59:368-75.
3. Buchacz K, Baker RK, Moorman AC et al. Rates of hospitalizations and associated diagnoses in a large multisite cohort of HIV patients in the United States, 1994-2005. AIDS 2008;22:1345-54.
4. Betz ME, Gebo KA, Barber E et al. Pattern of diagnoses in hospital admissions in a multistate cohort of HIV-positive adults in 2001. Med Care 2005;43:113-14.
Aknowledgement : COREVIH Sud Paris, France (Pr D. Salmon, Cochin Hospital, Paris, France)
OBJECTIVES
Hospitalisation of HIV-infected patients remains significant and the causes are diversifying. Infections, in particular in patients screened at a late stage, cancers and management of comorbidities justify a coordinated referral to the different specialists.
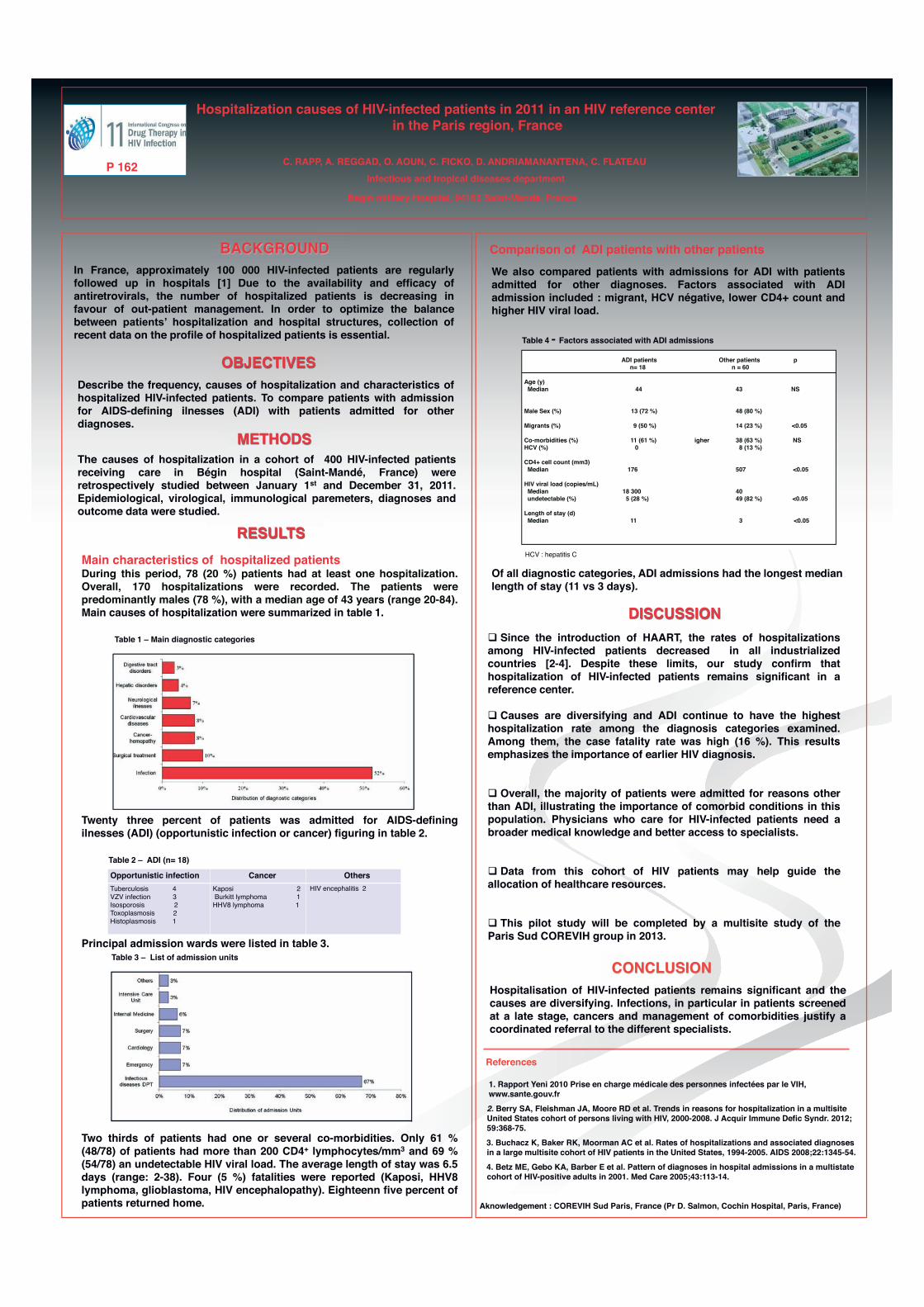
METHODS The causes of hospitalization in a cohort of 400 HIV-infected patients receiving care in Bégin hospital (Saint-Mandé, France) were retrospectively studied between January 1st and December 31, 2011. Epidemiological, virological, immunological paremeters, diagnoses and outcome data were studied. RESULTS Main characteristics of hospitalized patients During this period, 78 (20 %) patients had at least one hospitalization. Overall, 170 hospitalizations were recorded. The patients were predominantly males (78 %), with a median age of 43 years (range 20-84). Main causes of hospitalization were summarized in table 1. Table 1 – Main diagnostic categories Twenty three percent of patients was admitted for AIDS-defining ilnesses (ADI) (opportunistic infection or cancer) figuring in table 2. Table 2 – ADI (n= 18) Principal admission wards were listed in table 3. Table 3 – List of admission units Two thirds of patients had one or several co-morbidities. Only 61 % (48/78) of patients had more than 200 CD4+ lymphocytes/mm3 and 69 % (54/78) an undetectable HIV viral load. The average length of stay was 6.5 days (range: 2-38). Four (5 %) fatalities were reported (Kaposi, HHV8 lymphoma, glioblastoma, HIV encephalopathy). Eighteenn five percent of patients returned home.
DISCUSSION Since the introduction of HAART, the rates of hospitalizations among HIV-infected patients decreased in all industrialized countries [2-4]. Despite these limits, our study confirm that hospitalization of HIV-infected patients remains significant in a reference center.
Causes are diversifying and ADI continue to have the highest hospitalization rate among the diagnosis categories examined. Among them, the case fatality rate was high (16 %). This results emphasizes the importance of earlier HIV diagnosis.
Overall, the majority of patients were admitted for reasons other than ADI, illustrating the importance of comorbid conditions in this population. Physicians who care for HIV-infected patients need a broader medical knowledge and better access to specialists. Data from this cohort of HIV patients may help guide the allocation of healthcare resources.
This pilot study will be completed by a multisite study of the Paris Sud COREVIH group in 2013.
P 162
In France, approximately 100 000 HIV-infected patients are regularly followed up in hospitals [1] Due to the availability and efficacy of antiretrovirals, the number of hospitalized patients is decreasing in favour of out-patient management. In order to optimize the balance between patients’ hospitalization and hospital structures, collection of recent data on the profile of hospitalized patients is essential.
Describe the frequency, causes of hospitalization and characteristics of hospitalized HIV-infected patients. To compare patients with admission for AIDS-defining ilnesses (ADI) with patients admitted for other diagnoses.
ADI patients Other patients p n= 18 n = 60 Age (y) Median 44 43 NS Male Sex (%) 13 (72 %) 48 (80 %) Migrants (%) 9 (50 %) 14 (23 %) <0.05 Co-morbidities (%) 11 (61 %) igher 38 (63 %) NS HCV (%) 0 8 (13 %) CD4+ cell count (mm3) Median 176 507 <0.05 HIV viral load (copies/mL) Median 18 300 40 undetectable (%) 5 (28 %) 49 (82 %) <0.05 Length of stay (d) Median 11 3 <0.05
Comparison of ADI patients with other patients
Opportunistic infection Cancer Others Tuberculosis 4 VZV infection 3 Isosporosis 2 Toxoplasmosis 2 Histoplasmosis 1
Kaposi 2 Burkitt lymphoma 1 HHV8 lymphoma 1
HIV encephalitis 2
We also compared patients with admissions for ADI with patients admitted for other diagnoses. Factors associated with ADI admission included : migrant, HCV négative, lower CD4+ count and higher HIV viral load. Table 4 - Factors associated with ADI admissions
HCV : hepatitis C Of all diagnostic categories, ADI admissions had the longest median length of stay (11 vs 3 days).

P163: Aspergillosis in HIV patients (p): a case seriesF. Laurent1, Ch. Martin1, S. De Wit1
Saint-Pierre University Hospital, Division of Infectious Diseases1, Brussels, BelgiumE-mail : [email protected]
Purpose of the study
Aspergillosis is uncommon in HIV p. and has beenmostly reported in HIV p. with CD4<50/µL. Data on riskfactors and prognosis are scarce.We reviewed 19 cases of aspergillosis diagnosed in ourHIV cohort.
Methods
In Brussels Saint-Pierre HIV cohort, 19 patients werediagnosed with aspergillosis between 1998 and 2012(8.7/10 000 patient/year of follow-up). We analyzedretrospectively and described localization andinvasiveness of aspergillosis, risk factors, mode ofdiagnosis, treatment and outcome of these patients.
Summary of results
Demographic features of patients, clinical dataʼs of aspergillosis and risk factors are presented respectively in Table 1, 2 and 3.
Mean Range
Age (years old) 40 22-60
CD4 count (/µl) 355 1-1463
African Caucasian
Ethnic group (%) 74 26
Incidence of aspergillosis rose recently, probably due tobetter diagnosis (Figure 1).Mode of diagnosis of IA and aspergilloma is presented in Table 4.
The global mortality was 42%.Seven p. out of 10 with invasive aspergillosis diedincluding 3 p. before antifungal therapy. Three p. weretreated with voriconazole, 1 with liposomal
CT GM serum GM BAL culture pathology no data
IA 6 7 5 8 3 1
aspergilloma 5 1 3 1 1 1Table 4 Mode of diagnosis (CT computerized tomography, GM galactomannan)
0
1
2
3
4
5
6
7
8
0
50
100
150
200
250
300
350
400
450
"n cases
n galactomannan
Figure 1
ConclusionsIncidence of aspergillosis in HIV p. remains low but in accordance to previous reports, mortality of IA is high(70%). Wide use of Galactomannan has a role in recent increasing incidence. CD4 <100 was a risk factor in only37% (50% for IA) and 80% of p. who died had other risk factors, mostly corticotherapy. IA is concomitant in 50%with other severe infectious diseases which can potentially occult aspergillosis emergence and worsenprognosis. Prognosis of pulmonary aspergilloma and sinus fungal ball is better.
A) Cerebral aspergillosis
B) Pulmonary aspergilloma
C) Pulmonary invasive aspergillosis
A) B)
n (%) Mortality (%)
Invasive aspergillosis (IA) total 10 (53%) 70
Proven* 3 66
Probable* 5 80
Possible* 2 50
Pulmonary aspergilloma 6 (31%) 16.6
Sinus Fungal Ball 3 (16%) 0
Table1 Demographic dataʼs
Table 2 Clinical dataʼs of aspergillosis
*IDSA definitions
Heterosexual Other
Mode of HIV infection 12 7
%
CD4<100/µl 37
Corticotherapy 50
Tbc sequelae 80
Neutropenia 20
Cirrhosis 20
IVDUse 20
Concomitant Infection 50% for IA
Table 3 Risk factors for aspergillosis
C)
treated with voriconazole, 1 with liposomalamphotericine and 3 with bitherapy.Among p. with aspergilloma (n=6), the major associatedrisk factor was tuberculosis sequelae (80%). Two p.were successfully treated with surgery andvoriconazole, 3 failed with itraconazole. One died frommassive hemoptysis, 2 were lost to follow-up, 1 iscurrently asymptomatic without treatment.Among p. with sinus fungal ball (n=3), all recoveredwithout relapse with surgical treatment associated withvoriconazole for one.
Invasive aspergillosis arose in the time course of septic shock in 30% and opportunistic infections occurred concomitantly in 40%.