olivier dauwalder françois delahaye, ali...
TRANSCRIPT

Olivier DAUWALDER1,2,3
François Delahaye, Ali M’Hammedi, Brice Guerpillon, Guy de Gevigney, André Boibieux, Olivier Dauwalder, Coralie Bouchiat, François Vandenesch,
1- Institut des Agents Infectieux (IAI) Hospices Civils de Lyon 2- Laboratoire de Bactériologie, Centre de Biologie et de Pathologie Est, Hospices Civils de Lyon; - 3- CIRI Centre International de Recherche en Infectiologie; INSERM U111; CNRS UMR5308; Université de Lyon; Ecole Normale Supérieure de Lyon; Lyon, France
[email protected] - #BioDAO

Projets R&D mixte HCL/bioMérieux : bioMérieux
Evaluation réactifs SANS financement BD
BioMérieux
Luminex
R-Biopharm

Endocardite
• Maladie grave : mortalité 20%
• 5 à 10% des patients feront une seconde endocardite
Faut-il rechercher la porte d’entrée de l’EI ?
• Selon les recommandations européennes : pas d’indications
• Selon les recommandations américaines : pas d’indications
Est il important…
• …de rechercher et de traiter la porte d’entrée de l’endocardite ?
• …de rechercher et de traiter la ou les portes d’entrée potentielle des futures EI ?
Selton-Suty C, Célard M, Le Moing V, et al.; AEPEI Study Group. Preeminence of Staphylococcus aureus in infective endocarditis: a 1-year population-based survey. Clin Infect Dis 2012;54:1230-9. Alagna L, Park LP,Nicholson BP, et al. Repeat endocarditis: analysis of risk factors based on the International Collaboration on Endocarditis - Prospective Cohort Study. Clin Microbiol Infect 2014;20:566-75.- Habib G, Hoen B, Tornos P, etal. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): the Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society ofCardiology (ESC). Endorsed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and the International Society of Chemotherapy (ISC) for Infection and Cancer. Eur Heart J 2009;30:2369-413. - Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association TaskForce on Practice Guidelines. J Am Coll Cardiol 2014;63:e57-185.

Evaluer les performances de la recherche de la porte
d’entrée de l’endocardite infectieuse active
Evaluer les performances des recherches de la ou les
porte(s) d’entrée potentielle(s) à une seconde
endocardite infectieuse

Critères de sélection◦ Patient hospitalisé à l’hôpital Louis PRADEL
(Hospices Civils de Lyon)
◦ Entre janvier 2005 et 2011
◦ Diagnostic d’endocardite infectieuse CERTAINE selon les critères de DUKE-LI
Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis 2000;30:633-8

Systématique pour tous les patients• Scanner thoraco abdomino pelvien,
• Consultation stomatologique avec réalisation d’un orthopantogramme,
• Consultation ORL,
• Consultation urologique
Systématique chez les femmes• Consultation
gynécologique
Si lésions cutanées ou périorificielles lors de l’examen clinique initial• Consultation
dermatologique
Si EI due à un microorganisme provenant du tube digestif• Colonoscopie
• Gastroscopie
Si patient ≥ 50 ans avec antécédents familiaux de polype(s) colique (s):• Colonoscopie
• Gastroscopie

Systémati-quement
réalisé
Fonction du micro-organisme identifié
Pendant la période
d’hospitalisation
Sous couverture
antibiotique adaptée au
micro-organisme impliqué

Entre 2005 et 2011 : 444 patients éligibles
Exclusion de 82 patients décédés
durant l’hospitalisation
Exclusion de 44 patients pour dossier clinique
incomplet ou manquant
Inclusion de 318 patients
(320 EI)

Age médian; 61 +/- 2 ans
75% d’hommes
Maladie de valve native pré existante: 29%
Au moins 1 valve prothétique: 22%
Dispositif implantable (pacemaker, stimulateur, défibrillateur) : 11%

Identification chez 74% des patients inclus (238/318)
Porte d’entrée identifiée Nombre de
patients
Pourcentage
Cutanée 96 40%
Orale / dentaire 68 29%
Gastro-intestinale 56 23%
Uro-génitale 10 4%
ORL 5 2%
Respiratoire 3 1%
Total 238 100%

Nosocomiale: 41%Communautaire :
34%
Toxicomanie IV : 22%
Maladie d’inoculation
• Morsure de pou: Bartonella quintana
• Griffade: Bartonella henselae

Importance des causes nosocomiales
Porte d’entrée cutanée N (%)
Causes nosocomiales n=39
Dispositifs intra-vasculaires (VVC
n=8; VVP n=5; chambre
implantable n=4)
17 (44%)
Infection d’un dispositif cardiaque
implantable (pacemaker,
défibrillateur)
11 (28%)
Infection du site opératoire
(remplacement valvulaire: n=6;
chirurgie vasculaire: n=3;
chirurgie orthopédique: n=2)
11 (28%)
Porte d’entrée cutanée N (%)
Causes communautaires n=33
Plaie cutanée par un objet
domestique
6 (19%)
Erysipèle 5 (15%)
Mal performant plantaire 5 (15%)
Traumatisme cutanée au cours
d’un accident du travail
4 (12%)
Abcès cutané et furoncle 4 (12%)
Ulcère veineux des MI 3 (9%)
Escarre 2 (6%)
Piqûre (oursin, écharde) 2 (6%)
Morsure d’insecte 1 (3%)
Prurigo 1 (3%)

Prédominance des staphylocoques
◦ EI nosocomiales : 87%
◦ EI communautaires : 82%
◦ EI chez les toxicomanes: 52%
Microorganisme EI nosocomiale EI communautaire Toxicomanie IV
Staphylococcus aureus 15 (SARM: 3) 27 (SARM: 1) 11 (SARM: 1)
Staphylococcus non aureus 19 (SNA-RM: 8) 3
Enterococcus faecalis 3
Streptococcus du groupe G 1
Streptococcus agalactiae 1
Streptococcus dysgalactiae 1
Streptococcus pyogenes 1
Klebsiella 1 (K. pneumoniae) 2 (K. oxytoca)
Propionibacterium 1 (P. spp) 1 (P. acnes)
Serratia marcescens 1
Champignons 3
Pas de microorganisme isolé 2
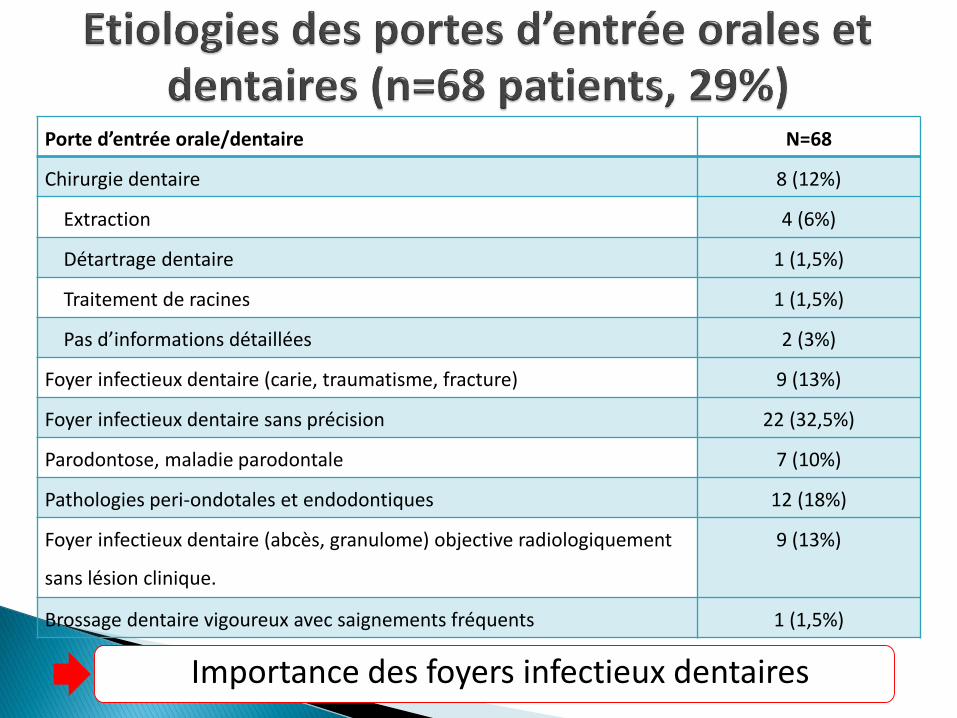
Importance des foyers infectieux dentaires
Porte d’entrée orale/dentaire N=68
Chirurgie dentaire 8 (12%)
Extraction 4 (6%)
Détartrage dentaire 1 (1,5%)
Traitement de racines 1 (1,5%)
Pas d’informations détaillées 2 (3%)
Foyer infectieux dentaire (carie, traumatisme, fracture) 9 (13%)
Foyer infectieux dentaire sans précision 22 (32,5%)
Parodontose, maladie parodontale 7 (10%)
Pathologies peri-ondotales et endodontiques 12 (18%)
Foyer infectieux dentaire (abcès, granulome) objective radiologiquement
sans lésion clinique.
9 (13%)
Brossage dentaire vigoureux avec saignements fréquents 1 (1,5%)

Prédominance des streptocoques « oraux »
Microorganismes n=68
Streptococcus viridans (oraux) 47 (69%)
HACCEK 7 (10%)
Streptococcus pyogenes 1 (1,5%)
Streptococcus pneumoniae 1 (1,5%)
Streptococcus dysgalactiae 1 (1,5%)
Gemella morbillorum 2 (3%)
Abiotrophia defectiva 1 (1,5%)
Bulleidia extructa 1 (1,5%)
Peptostretococcus anaerobius 1 (1,5%)
Neisseria sicca 1 (1,5%)
Acinetobacter spp 1 (1,5%)
Propionibacterium acnes 1 (1,5%)
Pas de microorganisme isolé 3 (4,5%)
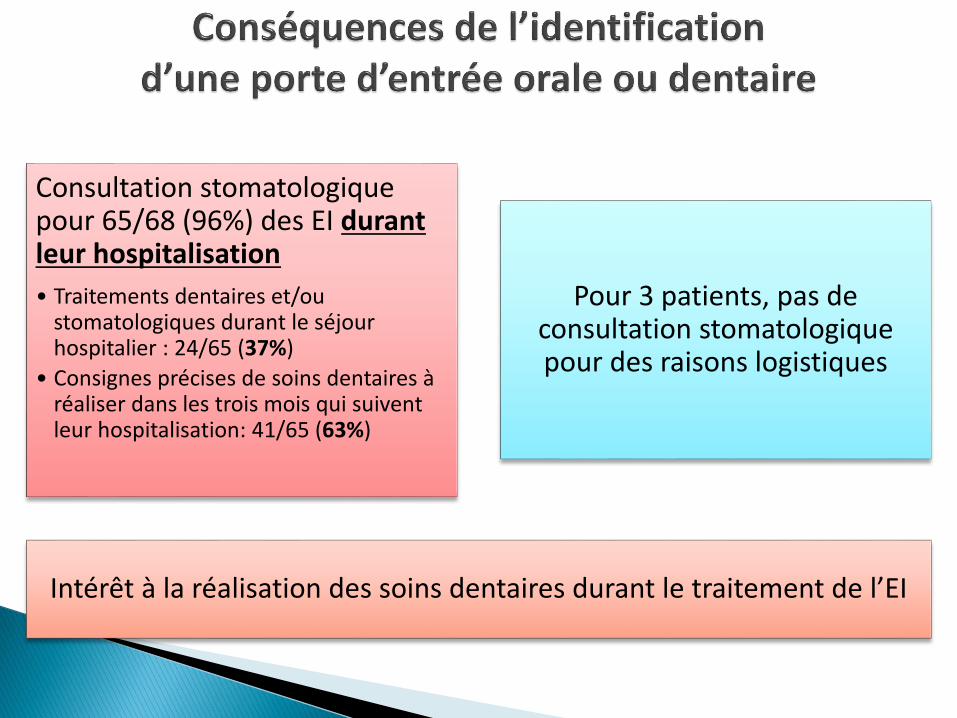
Consultation stomatologique pour 65/68 (96%) des EI durant leur hospitalisation
• Traitements dentaires et/ou stomatologiques durant le séjour hospitalier : 24/65 (37%)
• Consignes précises de soins dentaires à réaliser dans les trois mois qui suivent leur hospitalisation: 41/65 (63%)
Pour 3 patients, pas de consultation stomatologiquepour des raisons logistiques
Intérêt à la réalisation des soins dentaires durant le traitement de l’EI

Présence de polypes chez 46% des patients
Diagnostic d’ADK colique dans 14% des patients
Porte d’entrée n=56
Tractus gastro intestinal supérieur 5 (9%)
Ulcère de l’oesophage 2
Atrophie de l’antrum et du fundus 1
Varices œsophagiques et ulcère du bulbe 1
Gastrostomie 1
Tractus gastro intestinal inférieur 51 (91%)
Polypes 22
Unique, ≥ 1 cm 7
Multiple, ≥ 1 cm 5
Multiple, < 1 cm 4
Multiple, de taille inconnue 6
Adénocarcinome colorectal 8
Diverticulose du sigmoïde 11
Diverticulose du sigmoïde + polypes multiples ≥ 1 cm 4
Angiodysplasie diffuse 2
Iléite active 1
Colostomie terminale due à un cancer rectal 2
Colonoscopie avec résection de plusieurs polypes 1

Prédominance de Streptococcus gallolyticus et d’Enterococcus faecalis
Microorganismes n=56
Streptococcus bovis (S. gallolyticus) 28 (50%)
Streptococcus agalactiae (Streptocoque du groupe B) 3 (6%)
Streptococcus dysgalactiae 1 (2%)
Streptococcus salivarius 1 (2%)
Enterococcus faecalis 16 (27%)
Enterococcus faecium 3 (3%)
Staphylococcus aureus 1 (2%)
Pas de microorganisme isolé 3 (3%)

Portes d’entrée urinaires
• Pyélonéphrite aigue (n=4)
• Hypertrophie bénigne de la prostate avec rétention urinaire (n=1)
• Biopsie prostatique (n=1)
• Résection prostatique (n=1)
• Résection d’un cancer de la vessie (n=1)
• Sténose urétrale (n=1)
• Micro organismes isolés: S. bovis(n=2); Enterococcus (n=1); S. agalactiae (n=1); Escherichia coli(n=1)
Portes d’entrée génitales
• Infection à S. agalactiae sur nécrose d’un fibrome intra utérin (n=1)

Causes
• Pan-sinusite avec abcès cérébral (n=2)
• Phlegmon des amygdales
• Rechute d’un carcinome laryngé
• Epistaxis récidivantes, cautérisation d’un polype nasal
Documentation microbiologique
• Streptococcus pneumoniae (n=3)
• Pas de documentation (n=2)

Isolement d’un microorganisme dont l'habitat est :◦ cutané : 49%
◦ oral ou dentaire : 22%
◦ gastro intestinal : 22%
Microorganisms n=
Microorganismes à habitat cutanéo-muqueux 40
Staphylococcus aureus 23 (SARM: 3)
Staphylococcus non aureus 10
Propionibacterium (acnes, granulosum) 4
Corynebacterium 3
Microorganismes à habitat oral ou dentaire 22
Streptocoques oraux 15
HACCEK 3
Gemella 2
Streptococcus pyogenes 1
Abiotrophia adiacens 1
Microorganismes à habitat digestif 18
Streptocoques gastro-intestinaux 7
Streptococcus agalactiae 5
Tropheryma whipplei 3
Entérocoques 2
Polymicrobien: (Streptocoque du groupe G et Staphylococcus
epidermidis)
1
EI à hémocultures négatives 1
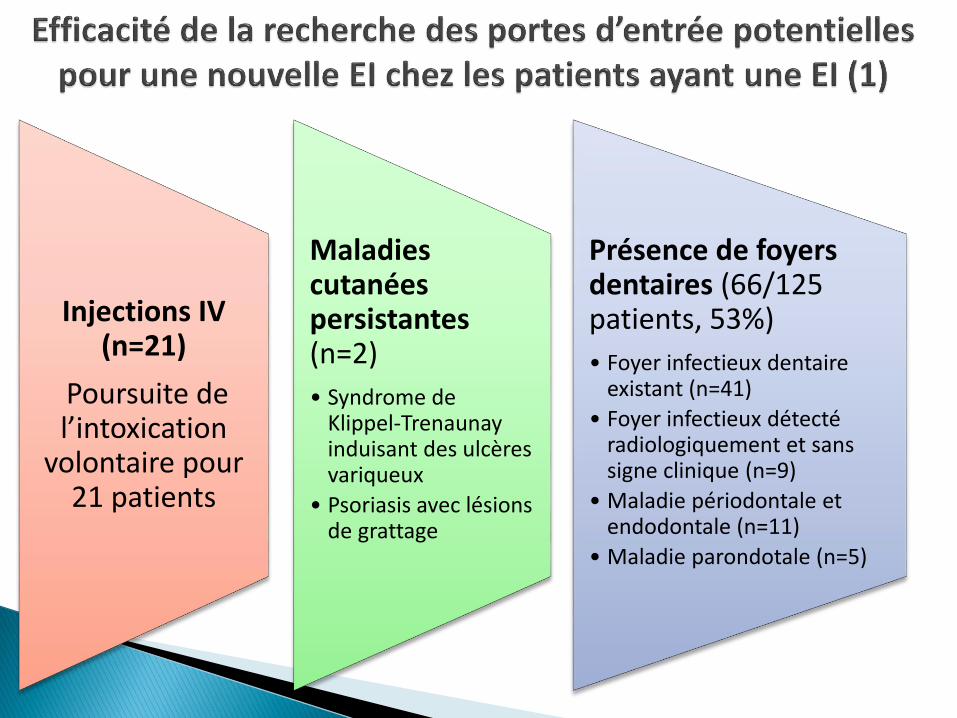
Injections IV (n=21)
Poursuite de l’intoxication
volontaire pour 21 patients
Maladies cutanées persistantes (n=2)
• Syndrome de Klippel-Trenaunay induisant des ulcères variqueux
• Psoriasis avec lésions de grattage
Présence de foyers dentaires (66/125 patients, 53%)
• Foyer infectieux dentaire existant (n=41)
• Foyer infectieux détecté radiologiquement et sans signe clinique (n=9)
• Maladie périodontale et endodontale (n=11)
• Maladie parondotale (n=5)

Présence de foyers gastro-intestinaux (polypes, diverticules, adénocarcinomes) chez 32/80 (40%) patients ayant un coloscopie car
• Age ≥50 ans
• Antécédents familiaux de polypes coliques
Présence de foyers génito-urinaires chez 11/52 patients (21%)
• Cancer de la prostate, hypertrophie bénigne de la prostate avec rétention, sténose urétrale,
• Pyélonéphrite, lithiase chronique
• Cancer de la vessie, etc.
Présence de lésions ORL chez 6/180
patients (3%)

Son identification est possible dans ¾ des cas de notre série
Prédominance des
• Portes d’entrée cutanées
• Nosocomiales
• Toxicomanes IV
• S. aureus puis les S. non aureus
• Porte d’entrée orale et dentaire: No 2
• Porte d’entrée gastro intestinale: No 3
Lorsqu’elle n’est pas détectée, le
microorganisme responsable peut
aider à la trouver…

Microorganismes Habitat Porte d’entrée potentielle de l’EI
Group mitis/salivarius (e.g., S. sanguis, sanguinis,
parasanguinis, gordonii, mitis, oralis, mutans, salivarius)
Plaque dentaire, langue, muqueuse orale,
oropharynx
Pathologies dentaires et parodontales
Streptococcus du Groupe milleri (S. constellatus,
intermedius, anginosus)
Oropharynx, plaque sous gingivale, tractus gastro intestinal, vagin
(S. anginosus)
Pathologies dentaires et parodontales
Pathologies digestivesInfections vaginales
Aagard K, Luna RA, Versalovic J. The Human Microbiome of Local Body sites and Their Unique Biology. In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences, 2014:11–18. Sinner SW. ViridansStreptococci, Nutritionally Variant Streptococci, Groups C and G Streptococci, and Other Related Organisms. In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences, 2014:2349–2361. HumanMicrobiome Project Consortium. Structure, function and diversity of the healthy human microbiome. Nature 2012;486:207–214. Paster BJ, Olsen I, Aas JA, Dewhirst FE. The breadth of bacterial diversity in the human periodontal pocket and otheroral sites. Periodontol. 2000 2006;42:80–87. - Curtis MA, Zenobia C, Darveau RP. The relationship of the oral microbiotia to periodontal health and disease. Cell Host Microbe 2011;10:302–306. Frandsen EV, Pedrazzoli V, Kilian M. Ecology of viridansstreptococci in the oral cavity and pharynx. Oral Microbiol. Immunol. 1991;6:129–133. Fowler VG, Scheld MW, Bayer AS. Endocarditis and Intravscular Infections. In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases.Elsevier Health Sciences, 2014:990–1028. Corredoira J, Alonso MP, Coira A, et al. Characteristics of Streptococcus bovis endocarditis and its differences with Streptococcus viridans endocarditis. Eur. J. Clin. Microbiol. Infect. Dis. 2008;27:285–291.Tomás Carmona I, Diz Dios P, Limeres Posse J, González Quintela A, Martínez Vázquez C, Castro Iglesias A. An update on infective endocarditis of dental origin. J Dent 2002;30:37–40. . Petti CA, Straton CW. Streptococcus anginosus Group. In:Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences, 2014:2362–2365. Gossling J. Occurrence and pathogenicity of the Streptococcus milleri group. Rev. Infect. Dis. 1988;10:257–285. CoykendallAL. Classification and identification of the viridans streptococci. Clin. Microbiol. Rev. 1989;2:315–328. . Belko J, Goldmann DA, Macone A, Zaidi AK. Clinically significant infections with organisms of the Streptococcus milleri group. Pediatr. Infect. Dis.J. 2002;21:715–723. Cunha BA, D'Elia AA, Pawar N, Schoch P. Viridans streptococcal (Streptococcus intermedius) mitral valve subacute bacterial endocarditis (SBE) in a patient with mitral valve prolapse after a dental procedure: the importance ofantibiotic prophylaxis. Heart Lung 2010;39:64–72.

Corredoira J, Alonso MP, Coira A, et al. Characteristics of Streptococcus bovis endocarditis and its differences with Streptococcus viridans endocarditis. Eur. J. Clin. Microbiol. Infect. Dis. 2008;27:285–291. Boleij A, Tjalsma H. The itinerary of Streptococcus gallolyticus infection in patients with colonic malignant disease. Lancet Infect Dis 2013;13:719–724. Boleij A, van Gelder MMHJ, Swinkels DW, Tjalsma H. Clinical Importance of Streptococcus gallolyticus infection among colorectal cancer patients: systematic review and meta-analysis. Clin. Infect. Dis. 2011;53:870–878. Bennett JE, Dolin R, Blaser MJ. Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences; 2014. Schlegel L, Grimont F, Ageron E, Grimont PAD, Bouvet A. Reappraisal of the taxonomy of the Streptococcus bovis/Streptococcus equinus complex and related species: description of Streptococcus gallolyticus subsp. gallolyticus subsp. nov., S. gallolyticus subsp. macedonicus subsp. nov. and S. gallolyticus subsp. pasteurianus subsp. nov. International Journal of Systematic and Evolutionary Microbiology 2003;53:631–645. Corredoira-Sánchez J, García-Garrote F, Rabuñal R, et al. Association between bacteremia due to Streptococcus gallolyticus subsp. gallolyticus (Streptococcus bovis I) and colorectal neoplasia: a case-control study. Clin. Infect. Dis. 2012;55:491–496.
Microorganismes Habitat Porte d’entrée potentielle de l’EI
S. bovis group (y compris S. gallolyticus subsp gallolyticus)
Tractus gastro intestinal Adénome et adénocarcinome
colorectaux, voies biliaires, tractus gastro-intestinal
Enteroccocus faecalis, Enterococcus faecium
Tractus gastro-intestinalTractus génito-urinaire
Geste invasif du tractus génito-urinaire (cytoscopie, lithotripsie, prostatectomie,
césarienne, curetage)

Microorganismes Habitat Porte d’entrée potentielle de l’EI
Streptocoque du groupe A :S. pyogenes
Oropharynx, peau, tractus génito-urinaire
Infections de la peau et des tissus mous, pharyngite, endométrite
Streptocoque du groupe B :S. agalactiae
Muqueuse orale, tractus gastro
intestinal, vagin, urètre antérieur
Tumeur colique (bénigne, maligne), translocation bactérienne du tractus digestif, infection de la peau et des tissus mous, infection du tractus génito-urinaire
Streptocoque du groupe C : S. dysgalactiae, S. equi, S. equisimilis, S. zooepidemicus
Nasopharynx, peau, tractus génito-urinaire
Infections cutanées et du tractus respiratoire, toxicomanes
Streptocoque du groupe G : S. dysgalactiae, S. anginosus
Nasopharynx, peau, tractus génito-urinaire
Infections génito-urinaires
Aagard K, Luna RA, Versalovic J. The Human Microbiome of Local Body sites and Their Unique Biology. In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences, 2014:11–18. - Sinner SW. Viridans Streptococci, Nutritionally VariantStreptococci, Groups C and G Streptococci, and Other Related Organisms. In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences, 2014:2349–2361. Human Microbiome Project Consortium. Structure, function and diversity of the healthyhuman microbiome. Nature 2012;486:207–214. - Paster BJ, Olsen I, Aas JA, Dewhirst FE. The breadth of bacterial diversity in the human periodontal pocket and other oral sites. Periodontol. 2000 2006;42:80–87. Curtis MA, Zenobia C, Darveau RP. The relationship of the oral microbiotia toperiodontal health and disease. Cell Host Microbe 2011;10:302–306. Frandsen EV, Pedrazzoli V, Kilian M. Ecology of viridans streptococci in the oral cavity and pharynx. Oral Microbiol. Immunol. 1991;6:129–133. Fowler VG, Scheld MW, Bayer AS. Endocarditis and Intravscular Infections. In:Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences, 2014:990–1028. Corredoira J, Alonso MP, Coira A, et al. Characteristics of Streptococcus bovis endocarditis and its differences with Streptococcus viridans endocarditis. Eur. J. Clin.Microbiol. Infect. Dis. 2008;27:285–291. Tomás Carmona I, Diz Dios P, Limeres Posse J, González Quintela A, Martínez Vázquez C, Castro Iglesias A. An update on infective endocarditis of dental origin. J Dent 2002;30:37–40

Microorganismes Habitat Porte d’entrée potentielle de l’EI
Streptococcus pneumoniae NasopharynxPneumopathie, otite moyenne
aiguë
Streptocoques déficients : Granulicatella (Abiotrophia) defectiva
Microbiote oral, plaque dentaire
Parodontose, Toxicomanie
Sinner SW. Viridans Streptococci, Nutritionally Variant Streptococci, Groups C and G Streptococci, and Other Related Organisms. In: Mandell, Douglas, and Bennett's principles and practice of infectiousdiseases. Elsevier Health Sciences, 2014:2349–2361. Bryant AE, Stevens DL. Streptococcus pyogenes. In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier HealthSciences, 2014:2285–2299. Ramirez CA, Naraqi S, McCulley DJ. Group A beta-hemolytic streptococcus endocarditis. Am. Heart J. 1984;108:1383–1386. Janoff EN, Musher DM. Streptococcus pneumoniae.In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences, 2014:2310–2327. Bruyn GA, Thompson J, Van der Meer JW. Pneumococcal endocarditis in adultpatients. A report of five cases and review of the literature. Q. J. Med. 1990;74:33–40. Takeshita T, Yasui M, Shibata Y, et al. Dental plaque development on a hydroxyapatite disk in young adults observedby using a barcoded pyrosequencing approach. Sci Rep 2015;5:8136. Ramos JN, Santos dos LS, Vidal LMR, et al. A case report and literature overview: Abiotrophia defectiva aortic valve endocarditis indeveloping countries. Infection 2014;42:579–584. Adam EL, Siciliano RF, Gualandro DM, et al. Case series of infective endocarditis caused by Granulicatella species. Int. J. Infect. Dis. 2015;31:56–58.Centers for Disease Control and Prevention (CDC). Fatal rat-bite fever--Florida and Washington, 2003. MMWR Morb. Mortal. Wkly. Rep. 2005;53:1198–1202. Kimura M, Tanikawa T, Suzuki M, et al. Detectionof Streptobacillus spp. in feral rats by specific polymerase chain reaction. Microbiol. Immunol. 2008;52:9–15. Madhubashini M, George S, Chandrasekaran S. Streptobacillus moniliformis endocarditis: casereport and review of literature. Indian Heart J 2013;65:442–446. Rupp ME. Streptobacillus moniliformis endocarditis: case report and review. Clin. Infect. Dis. 1992;14:769–772.

Aagard K, Luna RA, Versalovic J. The Human Microbiome of Local Body sites and Their Unique Biology. In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences, 2014:11–18. Wertheim H FL, Melles DC, Vos MC, van Leeuwen W, van Belkum A, Verbrugh HA, et al. The role of nasal carriage in Staphylococcus aureus infections. Lancet Infect Dis 2005;12:751-762. Que Y-A, Moreillon P. Staphylococcus aureus (Including Staphylococcal Toxic Shock Syndrome). In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences, 2014:2237–2271. Saginur R, Suh KN. Staphylococcus aureus bacteraemia of unknown primary source: where do we stand? Int. J. Antimicrob. Agents 2008;32 Suppl 1:S21–5. Bahrain M, Vasiliades M, Wolff M, Younus F. Five cases of bacterial endocarditis after furunculosis and the ongoing saga of community-acquired methicillin-resistant Staphylococcus aureus infections. Scand. J. Infect. Dis. 2006;38:702–707. Murray RJ. Staphylococcus aureus infective endocarditis: diagnosis and management guidelines. Intern Med J 2005;35 Suppl 2:S25–44. Rupp ME, Soper DE, Archer GL. Colonization of the female genital tract with Staphylococcus saprophyticus. J Clin Microbiol 1992;30:2975–2979.
Microorganismes Habitat Porte d’entrée potentielle de l’EI
Staphylococcus aureus Nez, pharynx, périnée, peau,
intestin
Infections liées aux soins, toxicomanie, infection de la peau
et des tissus mous
Staphylococcus saprophyticus Périnée Infection du tractus génito-urinaire
S. epidermidis, capitis, haemolyticus, hominis, schleiferi, lugdunensis, etc.
Peau Infections cutanées, Infections liées aux soins

Fowler VG, Scheld MW, Bayer AS. Endocarditis and Intravscular Infections. In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences, 2014:990–1028. Rupp ME, Fey PD. Staphylococcus epidermidisand Other Coagulase-Negative Staphylococci. In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences, 2014:2Z72–2282. Henderson B, Wilson M, Sharp L, Ward JM. Actinobacillusactinomycetemcomitans. J. Med. Microbiol. 2002;51:1013–1020. Steinberg JP, Burd EM. Other Gram-Negative and Gram-Variable Bacilli. In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences,2014:2666–2683. Patrick WD, Brown WD, Ian Bowmer M, Sinave CP. Infective endocarditis due to Eikenella corrodens: Case report and review of the literature. Can J Infect Dis 1990;1:139–142. Sheng WS, Hsueh PR, Hung CC, Teng LJ, Chen YC, LuhKT. Clinical features of patients with invasive Eikenella corrodens infections and microbiological characteristics of the causative isolates. Eur. J. Clin. Microbiol. Infect. Dis. 2001;20:231–236. Nwaohiri N, Urban C, Gluck J, Ahluwalia M, Wehbeh W.Tricuspid valve endocarditis caused by Haemophilus parainfluenzae: a case report and review of the literature. Diagn. Microbiol. Infect. Dis. 2009;64:216–219. Feder HM, Roberts JC, Salazar JC, Leopold HB, Toro-Salazar O. HACEK endocarditis ininfants and children: two cases and a literature review. Pediatr. Infect. Dis. J. 2003;22:557–562.
Microorganismes Habitat Porte d’entrée potentielle de l’EI
HACCEKHaemophilus spp., Aggregatibacter
(Actinobacillus) actinomycetemcommitans, Capnocytophaga spp., Cardiobacterium hominis, Eikenella corrodens, Kingella
kingae
OropharynxParodontite, infections
dentaires et buccales, soins dentaires, toxicomanie IV
E. coli, Salmonella spp.,Enterobacter spp., etc.
Périnée, tractus génito-urinaire
Infections liées aux soins, translocation digestive,
toxicomanie IV, infections génito-urinaires
Pseudomonas spp. EauToxicomanie IV
Infections liées aux soins
Streptobacillus moniliformis Cavité orale des rats, gerbilles, souris, cochons
d’inde
Morsure de rat ou lésions cutanées

Fowler VG, Scheld MW, Bayer AS. Endocarditis and Intravscular Infections. In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences, 2014:990–1028. Raoult D, Marrie T. Q fever. Clin. Infect. Dis.1995;20:489–95– quiz 496. Gandhi TN, Welch DF, Koehler JE. Bartonella, Including Cat-Scratch Disease. In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences, 2014:2649–2643 Mosbacher ME,Klotz S, Klotz J, Pinnas JL. Bartonella henselae and the potential for arthropod vector-borne transmission. Vector Borne Zoonotic Dis. 2011;11:471–477. Desenclos JC, Laporte A, Brouqui P. [Louse-borne infections in humans]. Med Mal Infect2011;41:295–300. Marth T, Schneider T. Whipple's Disease. In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences, 2014:2418–2424. Fenollar F, Lagier J-C, Raoult D. Tropheryma whipplei andWhipple's disease. J. Infect. 2014;69:103–112. Fenollar F, Celard M, Lagier J-C, Lepidi H, Fournier P-E, Raoult D. Tropheryma whipplei endocarditis. Emerging Infect. Dis. 2013;19:1721–1730. Edelstein PH, Roy CR. Legionnaires' disease and PontiacFever. In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences, 2014:2633–2644. Gul CH, Erdem H. Brucellosis (Brucella Species). In: Mandell, Douglas, and Bennett's principles and practice ofinfectious diseases. Elsevier Health Sciences, 2014:2584–2589.
Microorganismes Habitat Porte d’entrée potentielle de l’EI
Coxiella burnetiiRuminants (femelles
parturientes), oiseaux, tiques
Inhalation ou contact avec des liquides biologiques contaminés, ingestion de
lait cru, morsures de tiques
Bartonella henselae Chats Griffades de chats
Bartonella quintana ? Pediculus humanus corporis
Tropheryma whippleiTractus gastro
intestinal humainInconnue
LegionellaEau, notamment eau
chaudeInhalation
Brucella (B. melitensis, B. abortus, B. suis)
Ruminants (mouton, chèvre, veau, bœuf)
Ingestion de lait cru, contact cutané ou inhalation de liquides biologiques
contaminés

Fowler VG, Scheld MW, Bayer AS. Endocarditis and Intravscular Infections. In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences, 2014:990–1028. Kim R, Reboli AC. Other Coryneform Bacteria andRhodococci. In: Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Elsevier Health Sciences, 2014:2373–2382 D'Agata E. Pseudomonas aeruginosa and Other Pseudomonas Species. In: Mandell, Douglas, and Bennett'sprinciples and practice of infectious diseases. Elsevier Health Sciences, 2014:2518–2531. Dawson NL, Brumble LM, Pritt BS, Yao JD, Echols JD, Alvarez S. Left-sided Pseudomonas aeruginosa endocarditis in patients without injection drug use.Medicine 2011;90:250–255. Minces LR, Shields RK, Sheridan K, Ho KS, Silveira FP. Peptostreptococcus infective endocarditis and bacteremia. Analysis of cases at a tertiary medical center and review of the literature. Anaerobe 2010;16:327–330.Marín A, Lustig N, Cruz R, Córdova S. [Infective endocarditis caused by Listeria monocytogenes: review of the literature and a case report]. Rev Chilena Infectol 2013;30:436–440. Sohail MR, Gray AL, Baddour LM, Tleyjeh IM, Virk A. Infectiveendocarditis due to Propionibacterium species. Clin. Microbiol. Infect. 2009;15:387–394. Kurz M, Kaufmann BA, Baddour LM, Widmer AF. Propionibacterium acnes prosthetic valve endocarditis with abscess formation: a case report. BMC Infect.Dis. 2014;14:105. Kalokhe AS, Rouphael N, Chami El MF, Workowski KA, Ganesh G, Jacob JT. Aspergillus endocarditis: a review of the literature. Int. J. Infect. Dis. 2010;14:e1040–7. Bush LM, Paturi A, Chaparro-Rojas F, Perez MT. Mycobacterialprosthetic valve endocarditis. Curr Infect Dis Rep 2010;12:257–265. Bouchiat C, Saison J, Boisset S, et al. Nontuberculous Mycobacteria: An Underestimated Cause of Bioprosthetic Valve Infective Endocarditis. Open Forum Infect Dis 2015;2:ofv047.Yuan S-M. Mycobacterial endocarditis: a comprehensive review. Rev Bras Cir Cardiovasc 2015;30:93–103. Sax H, Bloemberg G, Hasse B, et al. Prolonged Outbreak of Mycobacterium chimaera Infection After Open-Chest Heart Surgery. CLIN INFECTDIS 2015;61:67–75.
Microorganismes Habitat Porte d’entrée potentielle de l’EI
Corynebacterium jeikeium, C. striatum
Environnement, commensaux de la peau et
des muqueuses
Infections liées aux soins (KT; chirurgie, etc.), toxicomanie IV
Peptostreptococcus spp.
Oropharynx, lésions cutanées chroniques, tractus
gastro-intestinal, tractus génito-urinaire
Gingivite, parodontite, pied diabétique,
Listeria spp Environnement Ingestion d’aliments contaminés
Propionibacterium spp. Oropharynx, peauInfections liées aux soins, gestes
invasifs

Kalokhe AS, Rouphael N, Chami El MF, Workowski KA, Ganesh G, Jacob JT. Aspergillus endocarditis: a review of the literature. Int. J. Infect. Dis. 2010;14:e1040–7. - Bush LM, Paturi A, Chaparro-Rojas F, Perez MT. Mycobacterial prosthetic valve endocarditis. Curr Infect Dis Rep 2010;12:257–265. - Bouchiat C, Saison J, Boisset S, et al. Nontuberculous Mycobacteria: An Underestimated Cause of Bioprosthetic Valve Infective Endocarditis. Open Forum Infect Dis 2015;2:ofv047. - Yuan S-M. Mycobacterial endocarditis: a comprehensive review. Rev Bras Cir Cardiovasc 2015;30:93–103. Sax H, Bloemberg G, Hasse B, et al. Prolonged Outbreak of Mycobacterium chimaera Infection After Open-Chest Heart Surgery. CLIN INFECT DIS 2015;61:67–75. - Lefort A, Chartier L, Sendid B, et al. Diagnosis, management and outcome of Candida endocarditis. Clin. Microbiol. Infect. 2012;18:E99–E109.
Microorganismes Habitat Porte d’entrée potentielle de l’EI
Mycobactéries atypiques (M. chelonae, M. fortuitum,
M. chimaera, etc.)
Environnement (eau, sol, animaux,
surfaces inertes, etc.)
Infections associées aux soins, gestes invasifs, valves bioprothétiques
contaminées
Aspergillus Environnement Inhalation, chirurgie cardio-thoracique
Candida Peau, tractus digestifInfections associées aux soins, gestes
invasifs, toxicomanie IV, mycose cutanée

Toxicomanes, patients atteints de
pathologies cutanées chroniques : prévention impossible
Porte d’entrée ORL: faibles performances,
peu d’anomalies détectées
Porte d’entrée génito-urinaire:
faibles performances, peu d’anomalies
détectées
Porte d’entrée orale/dentaire:
lésion(s) détectée(s) dans 53% des cas
Porte d’entrée gastro-intestinale: •Lésion(s) détectée(s) dans 40% des cas dues aux
limites de réalisation de la coloscopie systématique
•Patient > 50 ans (incidence élevée des adénocarcinomes coliques),
•ATCD de polypes coliques.
Chirouze C, Patry I, Duval X, et al. Streptococcus bovis/Streptococcus equinus complex fecal carriage, colorectal carcinoma, and infective endocarditis: a new appraisal of acomplex connection. Eur J Clin Microbiol Infect Dis 2013;32:1171-6.

Patient atteint d’une EI selon Duke-Li
Age ≥ 50 ans ou antécédents personnels et/ou familiaux de polypes coliques
Oui Non
Consultations•Stomatologique (♀♂)•ORL (♀♂)•Urologique (♀♂)•Dermatologique (♀♂)•Gynécologique (♀)Réalisation d’une•Coloscopie•Gastroscopie
Si un microorganisme a été identifié, utiliser l’habitat naturel ou le site de colonisation de ce microorganisme pour rechercher la porte d’entrée
Micro-organisme à habitat digestif
Micro-organisme à habitat oral/dentaire
Micro-organisme à habitat cutané
Pas de micro-organisme identifié
Consultations•Stomatologique (♀♂)•ORL (♀♂)•Urologique (♀♂)•Gynécologique (♀)•Dermatologique (♀♂) si présence de lésions cutanées ou cutanéo-muqueuses
• Traitement de la porte d’entrée de l’EI active (durant le traitement de l’EI)• Traitement de la porte d’entrée potentielle durant le traitement de l’EI active ou peu de temps après

François DELAHAYE, Ali M’HAMMEDI, Brice GUERPILLON, Guy de GEVIGNEY, André BOIBIEUX, Coralie BOUCHIAT, François VANDENESCH
Tous les cardiologues, infectiologues, chirurgiens, pathologistes, pharmaciens, microbiologistes membres et participants à la RCP EI du mercredi et qui se lèvent tôt !