obstetric early warning system sepsis - 1000 lives plus · obstetric early warning system learning...
TRANSCRIPT

Obstetric Early
Warning System
Learning
session 4
29th May 2012
Recognising & responding
to acute illness
Sepsis
• Agree and understand the language • Agree the normal/abnormal physiological
parameters for obstetrics in order to devise an effective trigger system.
• Agree effective accompanying escalation guidance.
• Work with the National Early Warning System
(NEWS) and explore its alignment for the use in obstetrics.
• What would be the best name – ONEWS, NEOWS or any other suggestions?
AIM of Paper – Obs EWS
Obstetric Early warning system
PREVIOUSLY……..

Modified Obstetric Early Warning System (MEOWS)
•Recommended by CMACE in the
absence of a validated tool
•Colour coded
•Mostly in use across Wales
•Associated ‘trigger’ (escalation)
criteria not always clear
•Doesn’t provide clear recognition of
improvement or deterioration
•Usage varies across Wales – e.g. all
women or just high risk women
PREVIOUSLY……..

Agreeing the Physiological Parameters in obstetrics -
What is normal/abnormal?
• MEOWS
• Existing numerical obstetric early warning systems
• NEWS
• Work undertaken with maternity clinicians (Nov 11)
• Specific physiological differences in pregnancy
• Report: Providing equity of critical and maternity care for the critically ill pregnant or recently pregnant woman (Royal College of Anaesthetists, 2011)
What has informed this work?

Attempting to adapt NEWS to Obstetrics
Feedback – Obs EWS
• OVERWHELMING FEEDBACK THAT THE SERVICE
DOES NOT CURRENTLY REQUIRE A ‘NEW’
OBSTETRIC EARLY WARNING SERVICE – would need
validating so wouldn’t be available immediately.
• Singh et al (2012) A validation study of the CEMACH
recommended modified early obstetric warning system
(MEOWS) - provided further validation.
Where next?
• Need to remind ourselves: ‘what are we trying to achieve?’ improve the recognition of and response to acutely ill women
• What EWS are you currently using? 5/6 using MEOWS
• Process compliance measured via bundles.
• Can you demonstrate that tool is effective?
• Outcome measures that demonstrate the effectiveness of the early warning tool you use.
• Robust escalation guidance is key appropriate, timely
response

Outcome Measures
Reviewing cases will also highlight issues with your Early
Warning System.
Multi-disciplinary Review
Denominator: all women triggered as having severe sepsis requiring a response in one month.
Numerator: the number of women within above set that
were transferred to high dependency unit, delivery
suite or critical care within that month.
Calculate as a percentage by dividing the numerator by
the denominator and multiplying the result by 100.
This needs to include women transferred to Labour
Ward for one to one care, High dependency unit
or ICU.
Number of women escalated to
higher level of care
Monthly number of calls for a response to women who
have been assessed as being of medium or high risk of acute deterioration.
Number of calls for rapid response
to medium and high risk acute illness
(depending on local guidance and
which track and trigger system
is used)
Operational DefinitionMeasure Name

You will need to ensure that you
have robust escalation systems
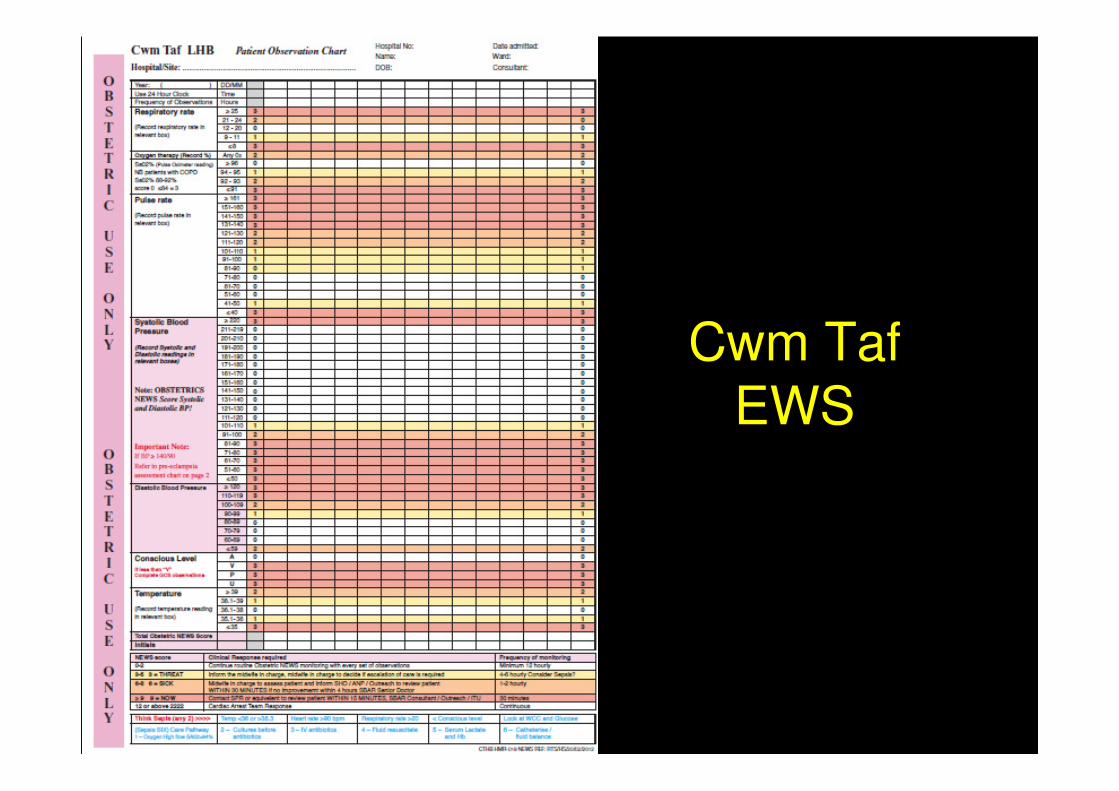
Cwm Taf
EWS
Recommendations
• Maternity Units to continue using their existing observation tracking charts/EWS eg. MEOWS.
• To locally agree escalation guidance that is explicit (RCA / RCOG).
• Demonstrate effectiveness of tool.
• How to guide will be updated to reflect this.

SEPSIS Previously………
The questions
• How do we define sepsis in pregnancy?
• Is sepsis defined the same at all stages of pregnancy and the puerperium?
• Is there a simple screening tool for sepsis in pregnancy?
• Can general advice be given on the management of sepsis in pregnancy? In other words, is the general ‘sepsis six’ care bundle appropriate for use in pregnancy or are modifications necessary?

How have we answered these
questions?
•Reviewed the current evidence
•Explored what is already happening
•Confidential enquiry
•Consultation with the service
•New RCOG Guidance

How do we define sepsis
in pregnancy?
• Sepsis: infection plus systemic manifestations of infection.
• Severe sepsis: sepsis plus sepsis-induced organ dysfunction or tissue hypoperfusion.
• Septic shock: the persistence of hypoperfusion despite adequate fluid replacement therapy.
RCOG (2012)
• Do we know the answer to this question?
Is sepsis defined the same at all stages of pregnancy and the puerperium?

Is there a simple screening tool for sepsis in pregnancy?
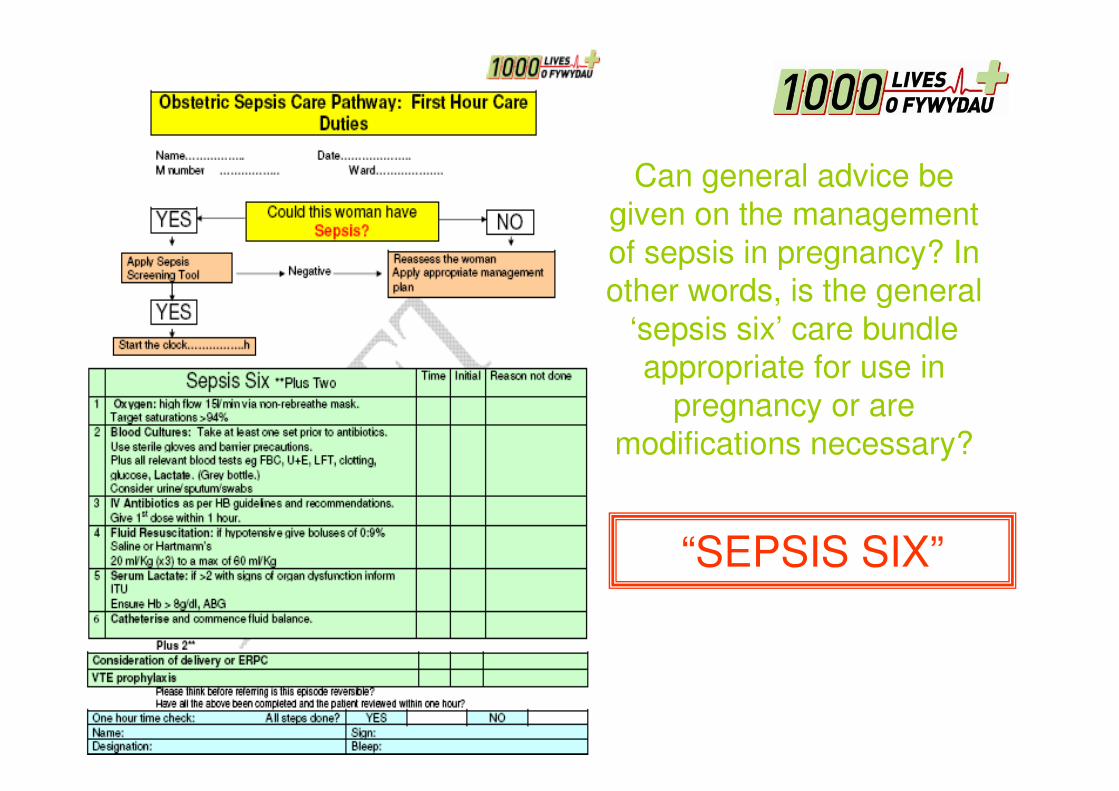
Can general advice be
given on the management
of sepsis in pregnancy? In other words, is the general
‘sepsis six’ care bundle appropriate for use in
pregnancy or are
modifications necessary?
“SEPSIS SIX”

Can general advice be
given on the management
of sepsis in pregnancy? In other words, is the general
‘sepsis six’ care bundle appropriate for use in
pregnancy or are
modifications necessary?
“SEPSIS SIX”
PLUS TWO
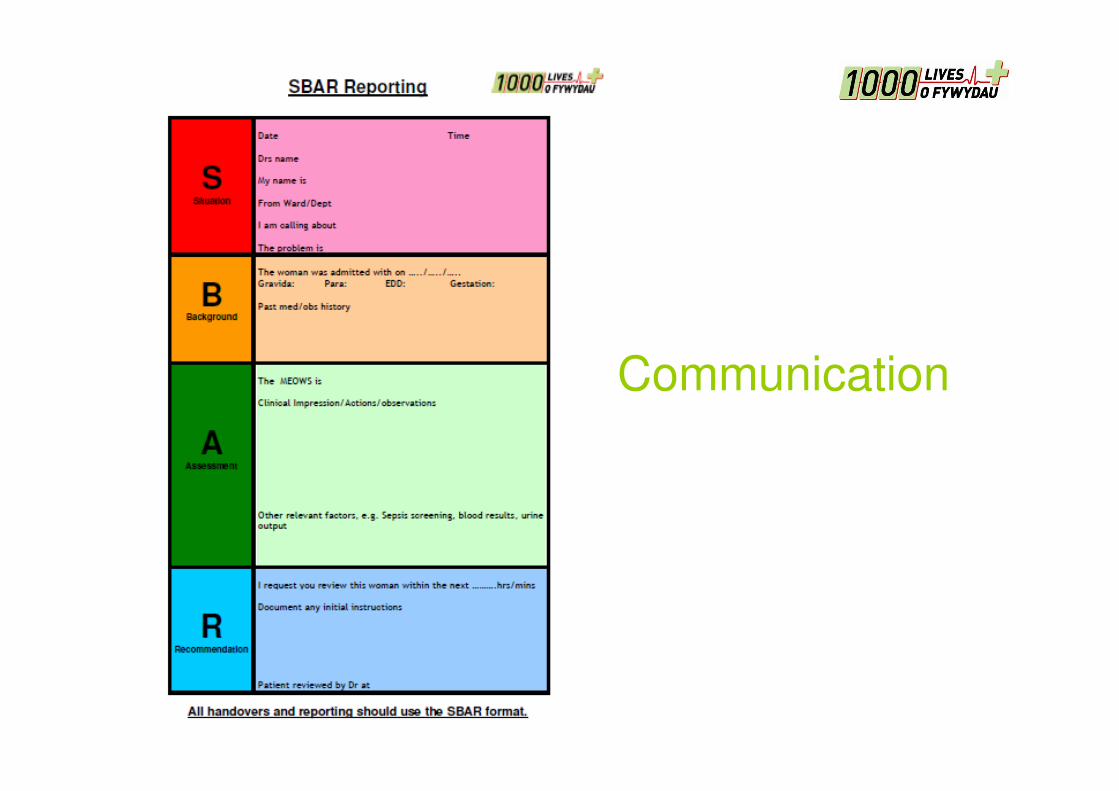
Communication
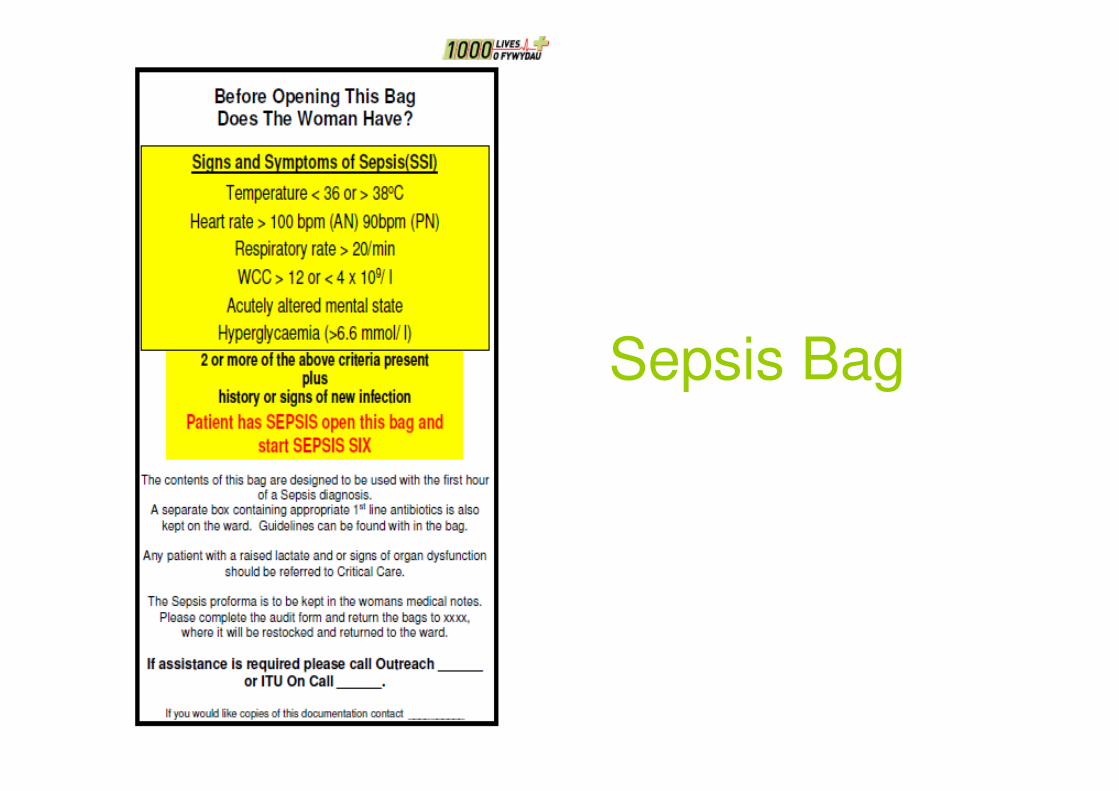
Sepsis Bag

Antibiotic Therapy

Measuring Effectiveness
Process
% compliance to Sepsis Six Bundle
Outcome Measures
Multidisciplinary reviews – learning from cases of sepsis that occur
Number of calls for rapid response to medium and high risk acute illness (depending on local guidance and which track and trigger system is used)
Monthly number of calls for a response to women who have been assessed as being of medium or high risk of acute deterioration
Number of women escalated to higher level of care - needs to include women transferred to Labour Ward for one to one care, High dependency unit or ICU
Sepsis Mortality

Outputs
• Updated How to
Guide June 2012
• PEG: Recognition of
the deteriorating pregnant woman and
escalation to
appropriate care
• PEG: Sepsis in
pregnancy