novel advances in the management of squamous cell ... · novel advances in the management of...
TRANSCRIPT
01
Novel Advances in the Management of Squamous Cell Carcinoma of the Head and NeckRobert Haddad, MDDisease Center Leader, Head and Neck Oncology Program, Dana-Farber Cancer Institute, Harvard Medical SchoolBoston, MA
02
Disclosures
• Research Funding: BMS, Merck, VentiRx, Boehringer Ingelheim, Celgene, Bayer
• Consultant: Merck, Eisai, Bayer, BI
• NCCN: Member—Head and Neck Committee
• NCCN: Chair—Thyroid Committee

03
Head and Neck Cancer
• Introduction– Epidemiology, HPV, Clinical Features, Prevention,
Treatment Modalities, Clinical Trials
• Concurrent Chemoradiotherapy
• Sequential Chemoradiotherapy
• Recurrent/Metastatic Disease
• Conclusion
04
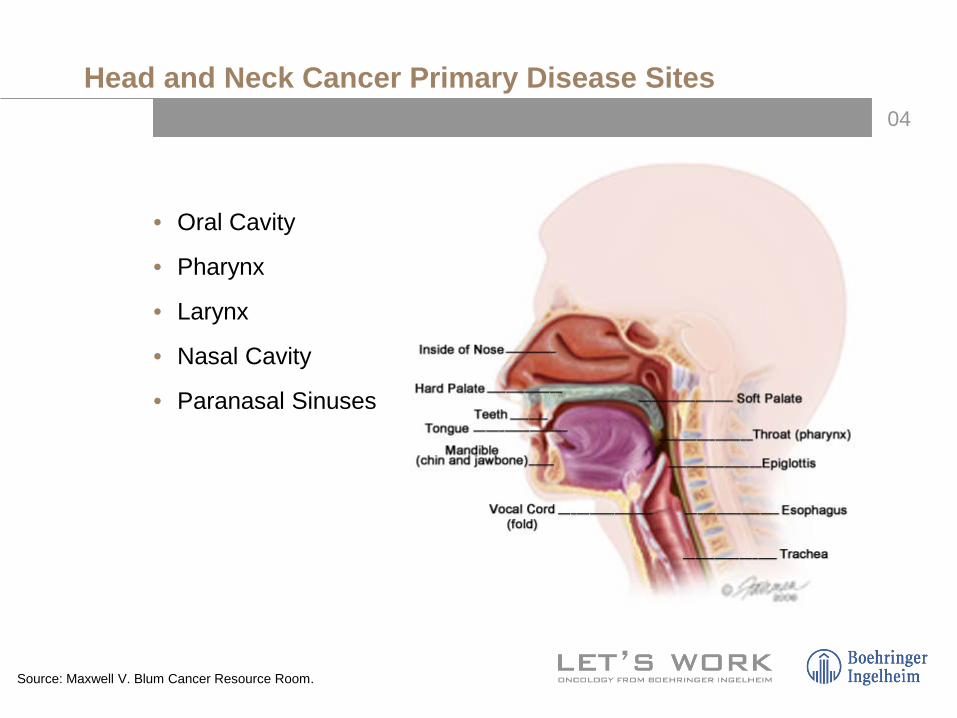
Head and Neck Cancer Primary Disease Sites
• Oral Cavity
• Pharynx
• Larynx
• Nasal Cavity
• Paranasal Sinuses
Source: Maxwell V. Blum Cancer Resource Room.
05
Epidemiology
• Incidence:– US: 48,000 new cases per year– Central and South America: ≈43,000 per year
• Median age of diagnosis: ≈60 years
• Male>Female
• Strongly associated with tobacco and alcohol
• Epstein-Barr virus risk factor for nasopharynx cancers
• Human papillomavirus increasingly appreciated as a risk factor
06
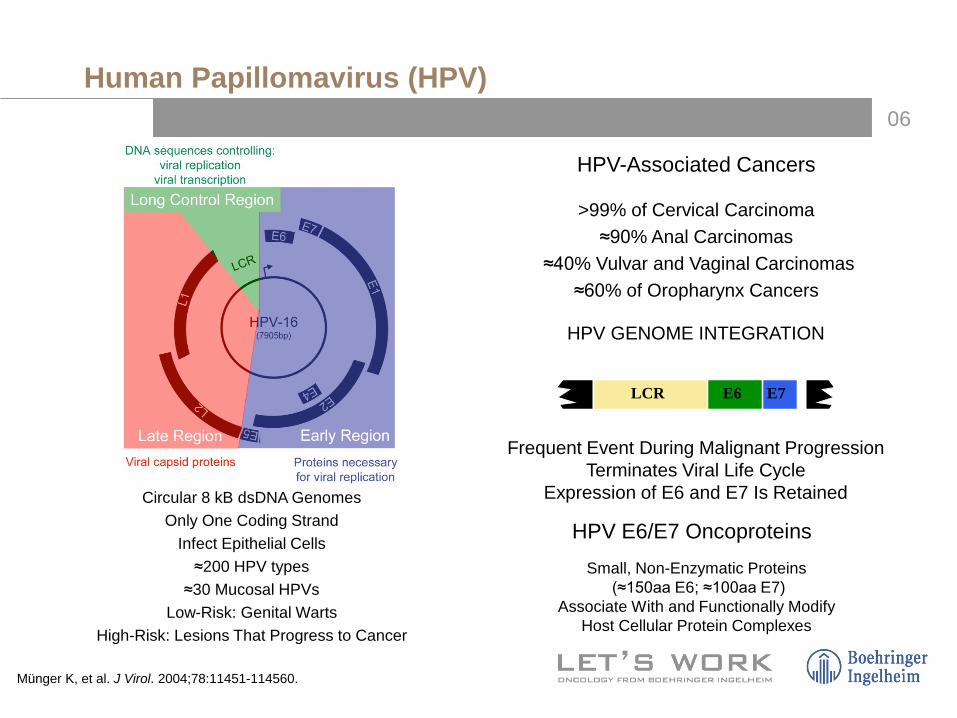
Circular 8 kB dsDNA GenomesOnly One Coding Strand
Infect Epithelial Cells≈200 HPV types
≈30 Mucosal HPVsLow-Risk: Genital Warts
High-Risk: Lesions That Progress to Cancer
HPV E6/E7 OncoproteinsSmall, Non-Enzymatic Proteins
(≈150aa E6; ≈100aa E7)Associate With and Functionally Modify
Host Cellular Protein Complexes
HPV GENOME INTEGRATION
LCR E6 E7
Frequent Event During Malignant Progression Terminates Viral Life Cycle
Expression of E6 and E7 Is Retained
HPV-Associated Cancers
>99% of Cervical Carcinoma≈90% Anal Carcinomas
≈40% Vulvar and Vaginal Carcinomas≈60% of Oropharynx Cancers
Münger K, et al. J Virol. 2004;78:11451-114560.
Human Papillomavirus (HPV)
07
Human Papillomavirus (HPV)-PositiveHead and Neck Cancer
• HPV 16 is the viral subtype in the vast majority of patients
• Half of oropharynx cancers will have HPV 16 DNA
• Often occurs in nonsmokers, nondrinkers
• Median age younger than HPV-negative patients; incidence increasing
• Men and women at more similar risk
• Associated with ↑ number of sexual partners and high-risk sexual practices
• Favourable prognosis
Fakhry C, et al. J Clin Oncol. 2006;24:2606-2617. Chaturvedi AK, et al. J Clin Oncol. 2008;26:612-619.

08
HPV Testing in Tumours
• In situ hybridisation
• p16 immunohistochemistry
• PCR
09
PFS in overall population
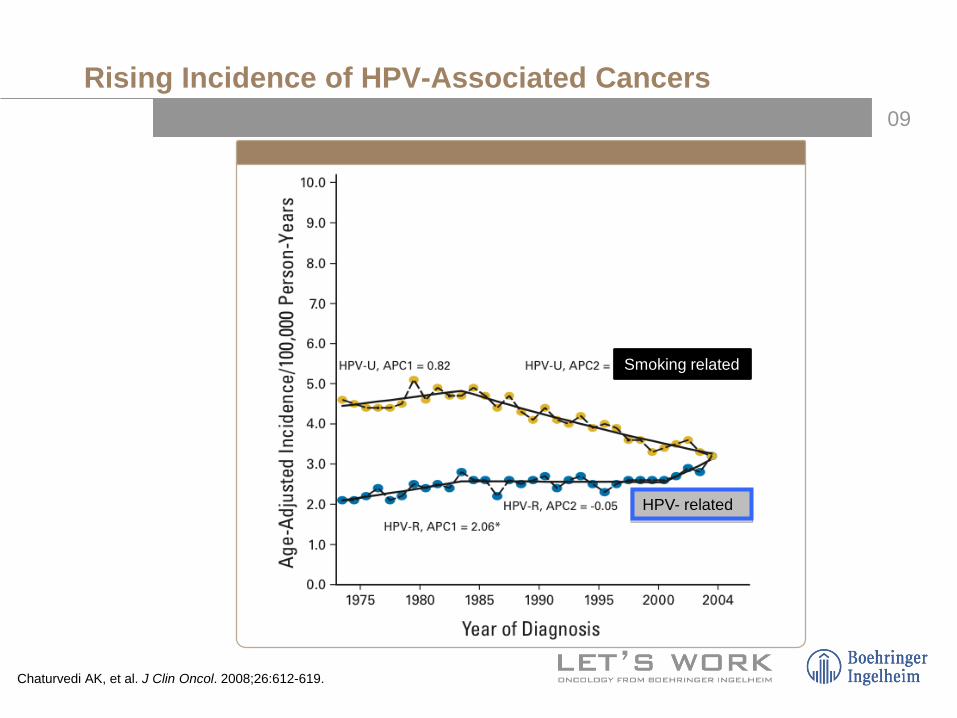
Rising Incidence of HPV-Associated Cancers
Chaturvedi AK, et al. J Clin Oncol. 2008;26:612-619.
Smoking related
HPV- related

010
Survival Outcomes by HPV Status in Oropharyngeal Cancer in RTOG 0129Ang et al. N Engl J Med. 2010.
011
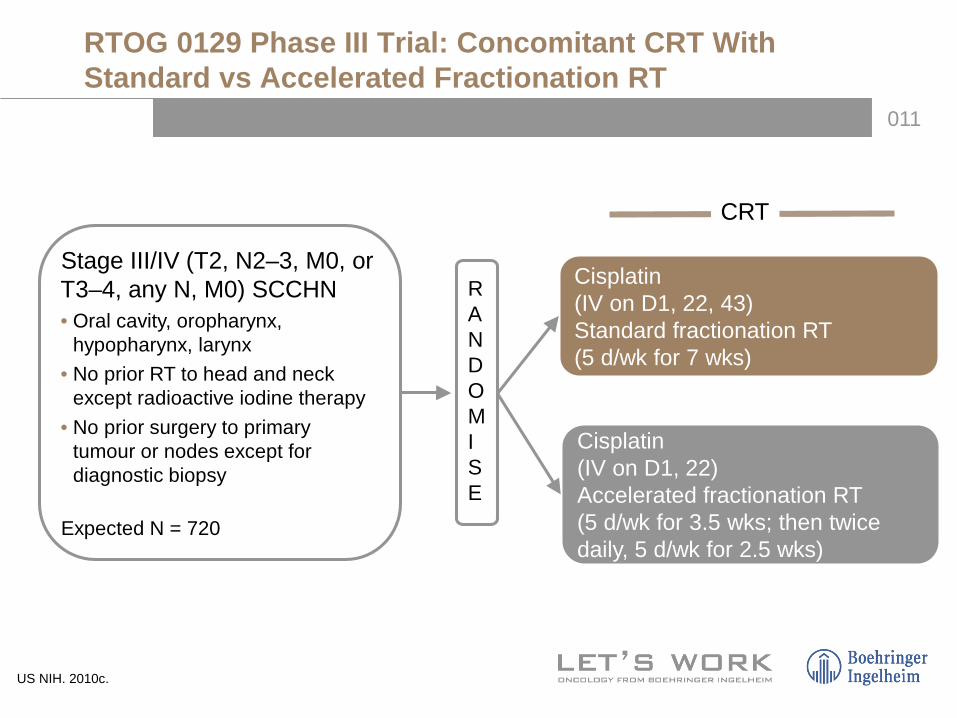
RTOG 0129 Phase III Trial: Concomitant CRT With Standard vs Accelerated Fractionation RT
Stage III/IV (T2, N2–3, M0, or T3–4, any N, M0) SCCHN• Oral cavity, oropharynx,
hypopharynx, larynx• No prior RT to head and neck
except radioactive iodine therapy• No prior surgery to primary
tumour or nodes except for diagnostic biopsy
Expected N = 720
Cisplatin(IV on D1, 22, 43)Standard fractionation RT(5 d/wk for 7 wks)
CRT
RANDOMISE
Cisplatin(IV on D1, 22)Accelerated fractionation RT(5 d/wk for 3.5 wks; then twice daily, 5 d/wk for 2.5 wks)
US NIH. 2010c.
012PFS in overall population
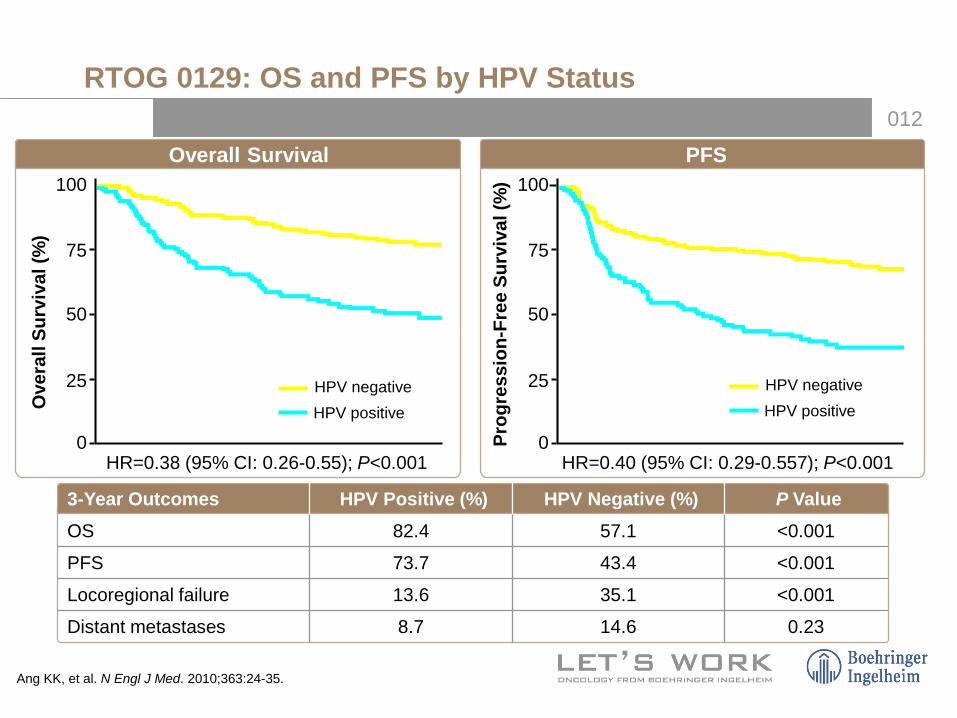
RTOG 0129: OS and PFS by HPV Status
Ang KK, et al. N Engl J Med. 2010;363:24-35.
3-Year Outcomes HPV Positive (%) HPV Negative (%) P ValueOS 82.4 57.1 <0.001
PFS 73.7 43.4 <0.001
Locoregional failure 13.6 35.1 <0.001
Distant metastases 8.7 14.6 0.23
HR=0.38 (95% CI: 0.26-0.55); P<0.001 HR=0.40 (95% CI: 0.29-0.557); P<0.001
Ove
rall
Surv
ival
(%)
HPV negativeHPV positive
75
50
25
0
75
50
25
0Prog
ress
ion-
Free
Sur
viva
l (%
)
Overall Survival100
HPV negativeHPV positive
100PFS
013
PFS in overall population
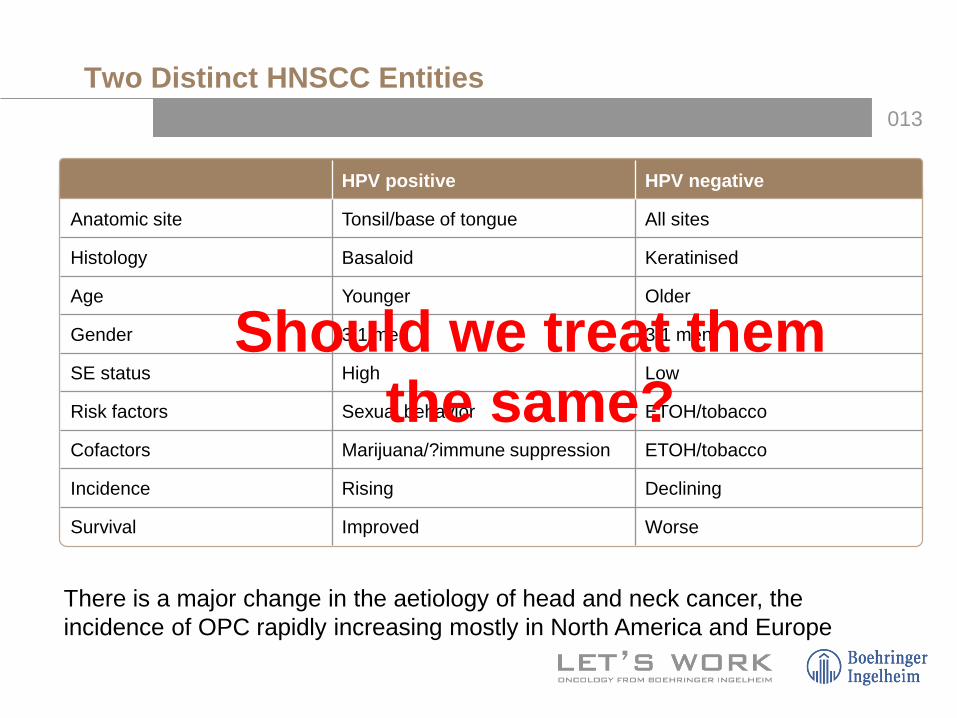
Two Distinct HNSCC Entities
HPV positive HPV negative
Anatomic site Tonsil/base of tongue All sites
Histology Basaloid Keratinised
Age Younger Older
Gender 3:1 men 3:1 men
SE status High Low
Risk factors Sexual behavior ETOH/tobacco
Cofactors Marijuana/?immune suppression ETOH/tobacco
Incidence Rising Declining
Survival Improved Worse
There is a major change in the aetiology of head and neck cancer, the incidence of OPC rapidly increasing mostly in North America and Europe
Should we treat them the same?

014
E1308: A Phase II Trial of Induction Chemotherapy Followed by Cetuximab With Low Dose vs Standard Dose IMRT in Patients With HPV-Associated Resectable Squamous Cell Carcinoma of the OropharynxCmelak et al. ASCO 2014.
015
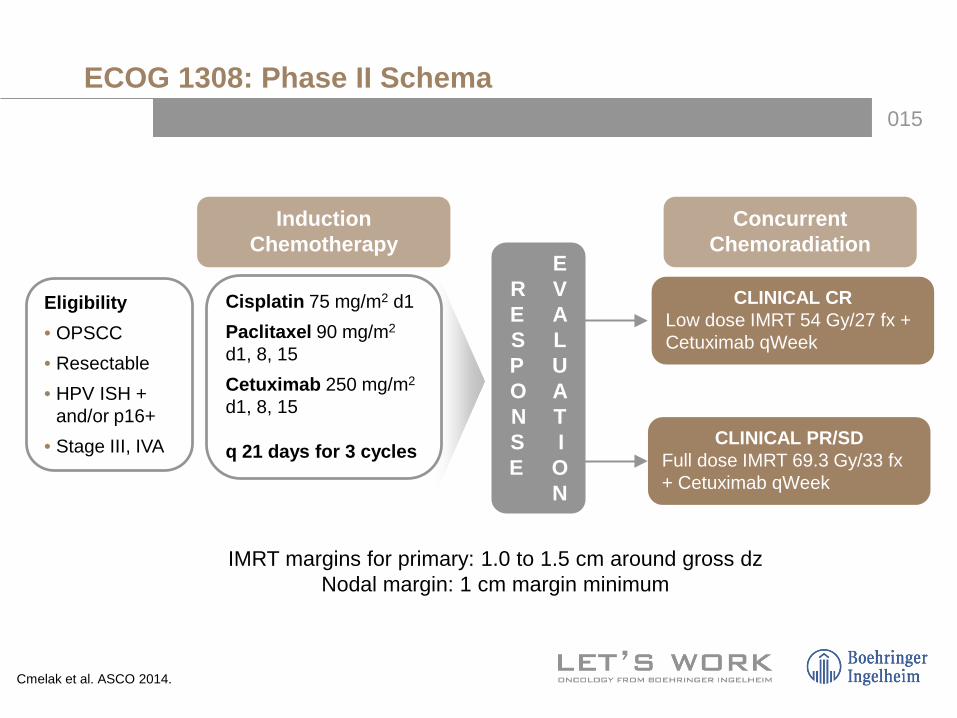
ECOG 1308: Phase II Schema
Cisplatin 75 mg/m2 d1Paclitaxel 90 mg/m2
d1, 8, 15Cetuximab 250 mg/m2
d1, 8, 15
q 21 days for 3 cycles
ER VE AS LP UO AN TS I E O
N
CLINICAL CR Low dose IMRT 54 Gy/27 fx + Cetuximab qWeek
CLINICAL PR/SDFull dose IMRT 69.3 Gy/33 fx+ Cetuximab qWeek
Induction Chemotherapy
Concurrent Chemoradiation
IMRT margins for primary: 1.0 to 1.5 cm around gross dzNodal margin: 1 cm margin minimum
Eligibility• OPSCC• Resectable• HPV ISH +
and/or p16+• Stage III, IVA
Cmelak et al. ASCO 2014.
016
PFS in overall population
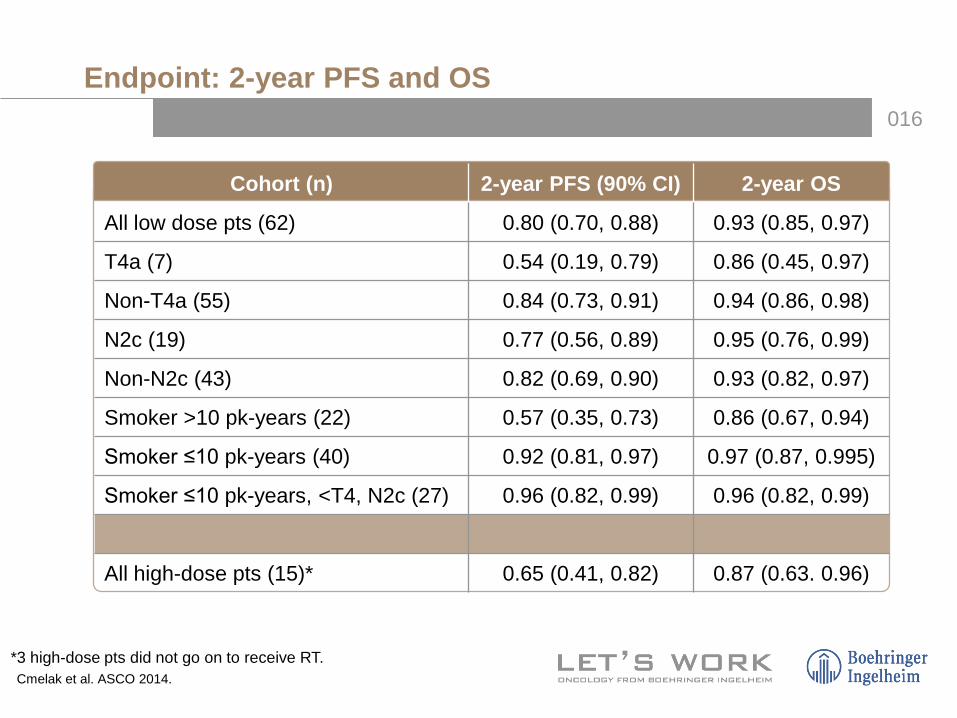
Endpoint: 2-year PFS and OS
Cohort (n) 2-year PFS (90% CI) 2-year OS
All low dose pts (62) 0.80 (0.70, 0.88) 0.93 (0.85, 0.97)
T4a (7) 0.54 (0.19, 0.79) 0.86 (0.45, 0.97)
Non-T4a (55) 0.84 (0.73, 0.91) 0.94 (0.86, 0.98)
N2c (19) 0.77 (0.56, 0.89) 0.95 (0.76, 0.99)
Non-N2c (43) 0.82 (0.69, 0.90) 0.93 (0.82, 0.97)
Smoker >10 pk-years (22) 0.57 (0.35, 0.73) 0.86 (0.67, 0.94)
Smoker ≤10 pk-years (40) 0.92 (0.81, 0.97) 0.97 (0.87, 0.995)
Smoker ≤10 pk-years, <T4, N2c (27) 0.96 (0.82, 0.99) 0.96 (0.82, 0.99)
All high-dose pts (15)* 0.65 (0.41, 0.82) 0.87 (0.63. 0.96)
*3 high-dose pts did not go on to receive RT.Cmelak et al. ASCO 2014.

017
PFS in overall population
Overall survival by RT dose
PFS in overall population
Progression-free survival by RT dose
PFS and Survival: Dose
2-year = 80%
2-year = 65%
2-year = 87%
2-year = 93%
Cmelak et al. ASCO 2014.

018
Summary E1308
• Induction chemo followed by reduced-dose IMRT/cetuximab was feasible in a Cooperative Group setting
• CCR to induction was noted in 71% (52/80) and was well tolerated
• The 2-year PFS in 54 Gy IMRT patients was 80% (95% CI: 0.70, 0.88), and 2-year survival was 93%
• Best predictor of outcome: smoking history
• Best results of 54 Gy were in smokers <10 pk-years, non T-4 and non-N2c: 2-year PFS and 2-year survival of 96% (90% CI: 0.82, 0.99) (n=27)
• This approach remains investigational. Further studies are planned
019
RANDOMISE
A
Bolus cisplatin
XRT
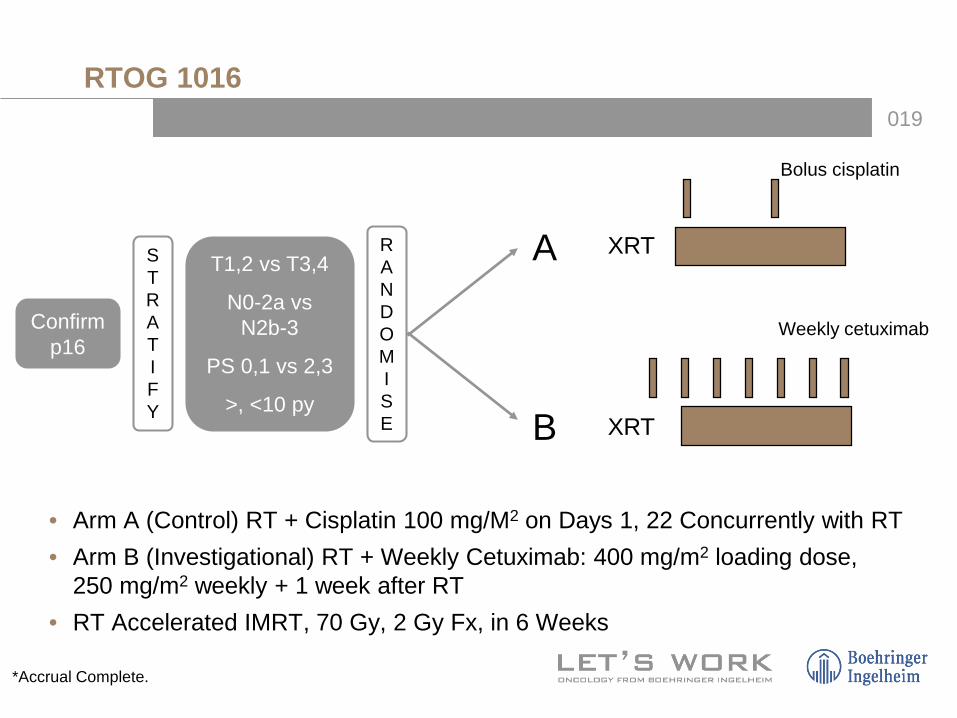
RTOG 1016
STRATIFY
Weekly cetuximab
XRTB
Confirm p16
T1,2 vs T3,4
N0-2a vs N2b-3
PS 0,1 vs 2,3
>, <10 py
*Accrual Complete.
• Arm A (Control) RT + Cisplatin 100 mg/M2 on Days 1, 22 Concurrently with RT• Arm B (Investigational) RT + Weekly Cetuximab: 400 mg/m2 loading dose,
250 mg/m2 weekly + 1 week after RT• RT Accelerated IMRT, 70 Gy, 2 Gy Fx, in 6 Weeks
020
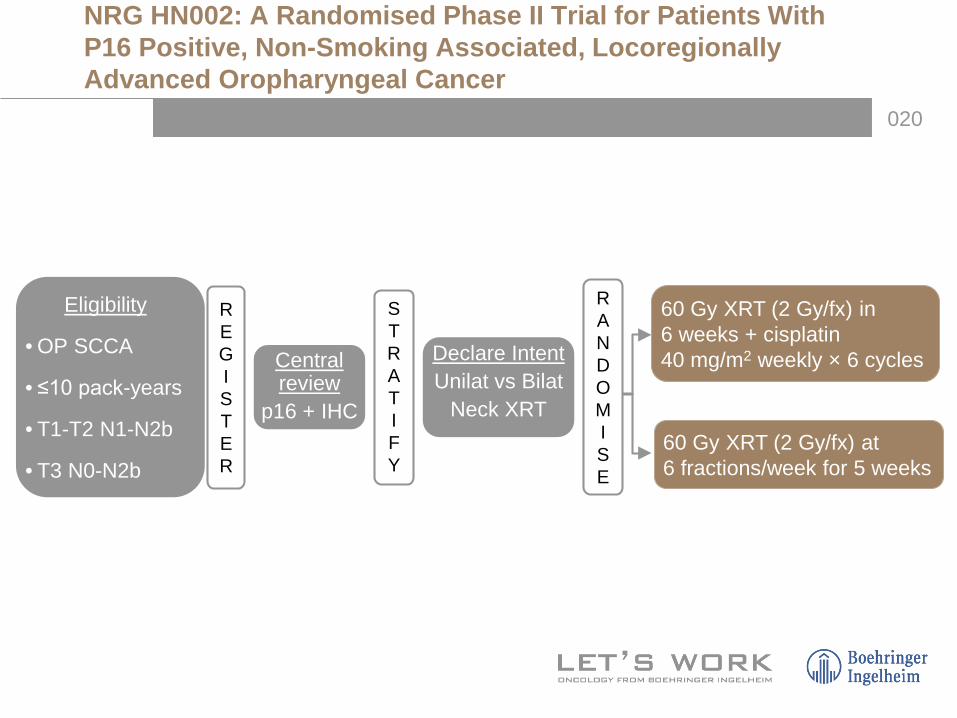
NRG HN002: A Randomised Phase II Trial for Patients With P16 Positive, Non-Smoking Associated, LocoregionallyAdvanced Oropharyngeal Cancer
Eligibility
• OP SCCA
• ≤10 pack-years
• T1-T2 N1-N2b
• T3 N0-N2b
60 Gy XRT (2 Gy/fx) in 6 weeks + cisplatin 40 mg/m2 weekly × 6 cycles
60 Gy XRT (2 Gy/fx) at 6 fractions/week for 5 weeks
R E G IS T E R
Central review
p16 + IHC
Declare IntentUnilat vs Bilat
Neck XRT
RANDOMISE
STRATIFY

021
Surgery: TORS, TLM, Other

022
ECOG-3311: HPV Positive
023
Evaluation and Staging
• Clinical exam of the head and neck• Endoscopy
– Fiberoptic flexible laryngopharyngoscopy– Exam under anaesthesia: laryngoscopy, oesophagoscopy,
bronchoscopy
• Biopsy – Fine needle aspiration of a neck node– Punch/core biopsy– Excisional biopsy
• Computed axial tomography/magnetic resonance imaging of primary site and neck
• Chest imaging• Positron emission tomography• Tumour-Node-Metastasis system applied

024
Treatment Approach
Disease Extent Treatment Options
T1N0-1 or T2N0 Surgery or RT
T2N1 or T3-4 or N2-3 Combined modality
Recurrent or M1
Surgery and/or RTCombined modalityChemotherapy
NCCN Clinical Practice Guidelines in Oncology. Head and Neck Cancers. V.2.2010. http://www.nccn.org/professionals/physician_gls/f_guidelines.asp.

025
Treatment Approach
Disease Extent Treatment Options
T1N0-1 or T2N0 Surgery or RT
T2N1 or T3-4 or N2-3 Combined modality
Recurrent or M1
Surgery and/or RTCombined modalityChemotherapy
026
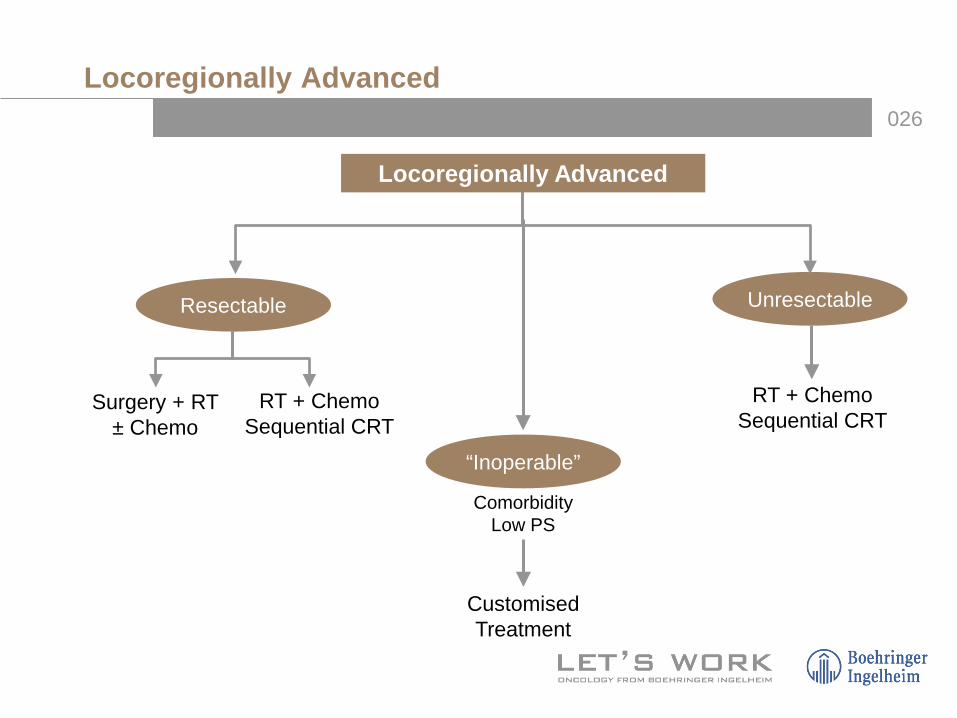
Locoregionally Advanced
Surgery + RT ± Chemo
RT + ChemoSequential CRT
RT + ChemoSequential CRT
ComorbidityLow PS
CustomisedTreatment
Resectable
“Inoperable”
Unresectable
Locoregionally Advanced

027
Concurrent Chemoradiotherapy
028
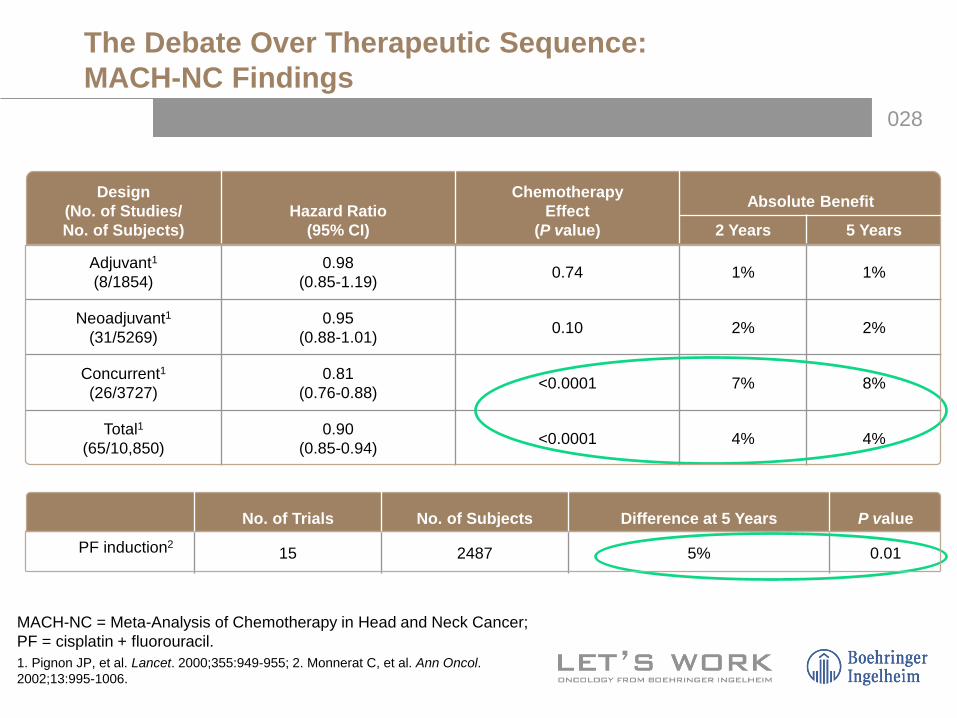
The Debate Over Therapeutic Sequence: MACH-NC Findings
MACH-NC = Meta-Analysis of Chemotherapy in Head and Neck Cancer; PF = cisplatin + fluorouracil.1. Pignon JP, et al. Lancet. 2000;355:949-955; 2. Monnerat C, et al. Ann Oncol. 2002;13:995-1006.
Design(No. of Studies/No. of Subjects)
Hazard Ratio(95% CI)
ChemotherapyEffect
(P value)
Absolute Benefit
2 Years 5 Years
Adjuvant1(8/1854)
0.98(0.85-1.19) 0.74 1% 1%
Neoadjuvant1(31/5269)
0.95(0.88-1.01) 0.10 2% 2%
Concurrent1(26/3727)
0.81(0.76-0.88) <0.0001 7% 8%
Total1(65/10,850)
0.90(0.85-0.94) <0.0001 4% 4%
No. of Trials No. of Subjects Difference at 5 Years P value
PF induction215 2487 5% 0.01
029
Concurrent Therapy: Standard of Care
• Cisplatin 100 mg/m2 days 1, 22, and 43 of RT
• RT standard fractionation, 70 Gy over 7 weeks (2-Gy fractions)
• Potential approaches to improve on CRT:– Addition of induction chemotherapy– Accelerated fractionation of RT

030
RTOG 91-11 Induction Cisplatin/5-FU vs Concomitant Cisplatin vs RT Alone in Resectable SCC
Resectable stage III/IV SCC
• Glottic or supraglotticcancer
• Previously untreated
N=515
RANDOMISE
Cisplatin (100 mg/m2, d1)5-FU (1000 mg/m2/day, d1-5 C-I)
every 3 wks, 2 cycles
ICTRT (N=173)
CRT (N=171)
Cisplatin (100 mg/m2, every 3 wks, 3 cycles)
RT (2 Gy/fr, 35 fr, total 70 Gy)
RT (2 Gy/fr, 35 fr, total 70 Gy)
RT (N=171)
RT(2 Gy/fr, 35 fr, total 70 Gy)
LFS = laryngectomy-free survival.Forastiere AA, et al. N Engl J Med. 2003;349:2091-2098.
• Primary end point: larynx preservation
• Secondary end point: LFS
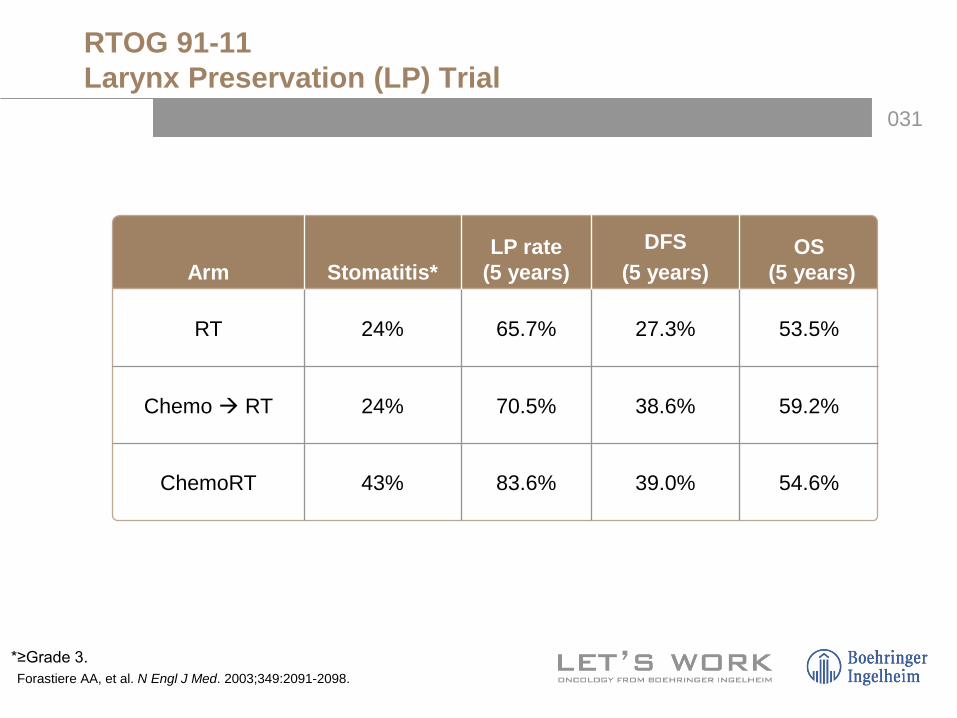
031
RTOG 91-11Larynx Preservation (LP) Trial
Arm Stomatitis*LP rate
(5 years)DFS
(5 years)OS
(5 years)
RT 24% 65.7% 27.3% 53.5%
Chemo RT 24% 70.5% 38.6% 59.2%
ChemoRT 43% 83.6% 39.0% 54.6%
*≥Grade 3.Forastiere AA, et al. N Engl J Med. 2003;349:2091-2098.

032
Forastiere AA, et al. J Clin Oncol. 2013;31:845-852.©2013 by American Society of Clinical Oncology.
38.8%
27.5%
Primary Endpoint LFS
os
Ten-year Update on RTOG-91-11
033PFS in overall population
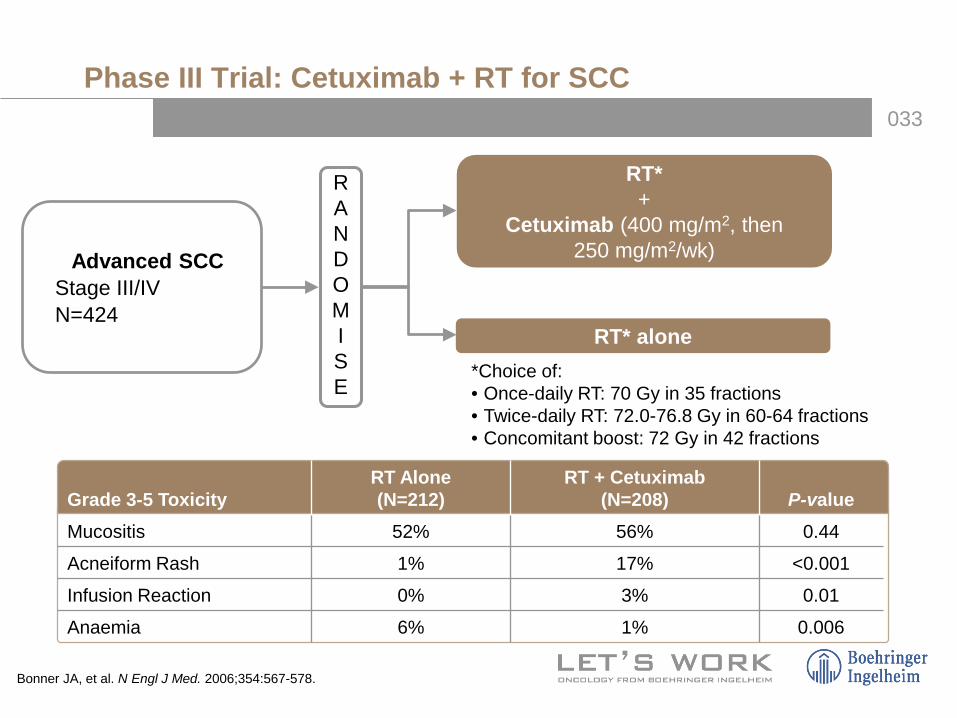
Phase III Trial: Cetuximab + RT for SCC
Grade 3-5 ToxicityRT Alone (N=212)
RT + Cetuximab (N=208) P-value
Mucositis 52% 56% 0.44
Acneiform Rash 1% 17% <0.001
Infusion Reaction 0% 3% 0.01
Anaemia 6% 1% 0.006
Bonner JA, et al. N Engl J Med. 2006;354:567-578.
Advanced SCC• Stage III/IV• N=424
RT*+
Cetuximab (400 mg/m2, then 250 mg/m2/wk)
RT* alone*Choice of: • Once-daily RT: 70 Gy in 35 fractions• Twice-daily RT: 72.0-76.8 Gy in 60-64 fractions• Concomitant boost: 72 Gy in 42 fractions
RANDOMISE

034
PFS in overall populationPFS in overall population
Phase III: Cetuximab + RT for SCC: Results
47% vs 34% at 3 yearsP<0.01 at 3 years
55% vs 45% at 3 yearsP=0.05 at 3 years
Locoregional Control OS
Bonner JA, et al. N Engl J Med. 2006;354:567-578.

035
Sequential Chemoradiotherapy
036
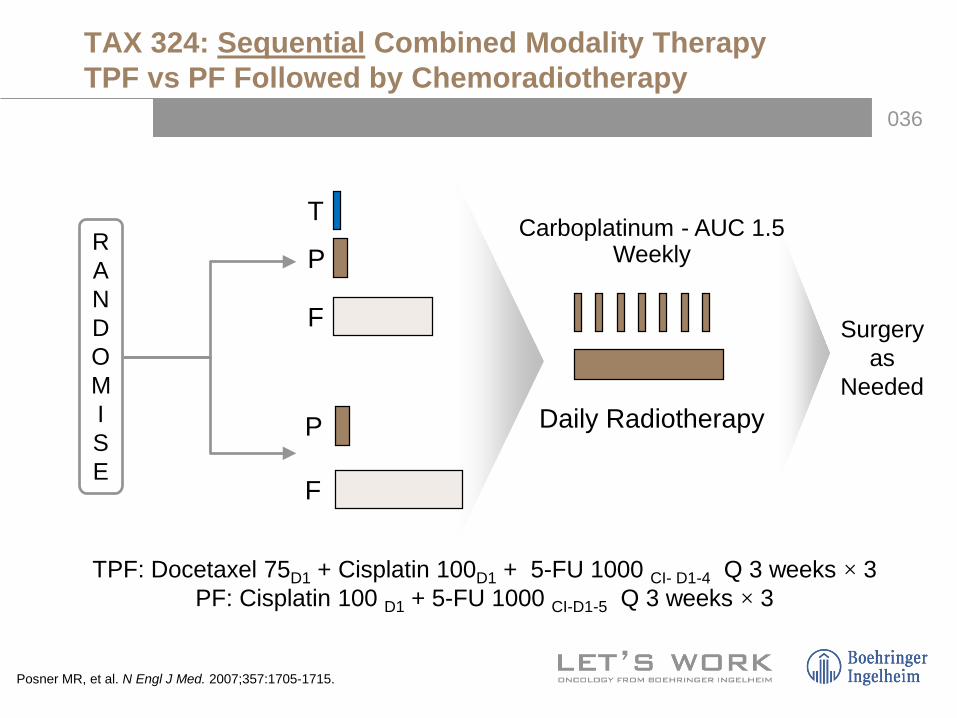
TAX 324: Sequential Combined Modality TherapyTPF vs PF Followed by Chemoradiotherapy
RANDOMISE
P
P
F
F
Carboplatinum - AUC 1.5 Weekly
Daily Radiotherapy
T
TPF: Docetaxel 75D1 + Cisplatin 100D1 + 5-FU 1000 CI- D1-4 Q 3 weeks × 3 PF: Cisplatin 100 D1 + 5-FU 1000 CI-D1-5 Q 3 weeks × 3
Surgery as
Needed
Posner MR, et al. N Engl J Med. 2007;357:1705-1715.
037
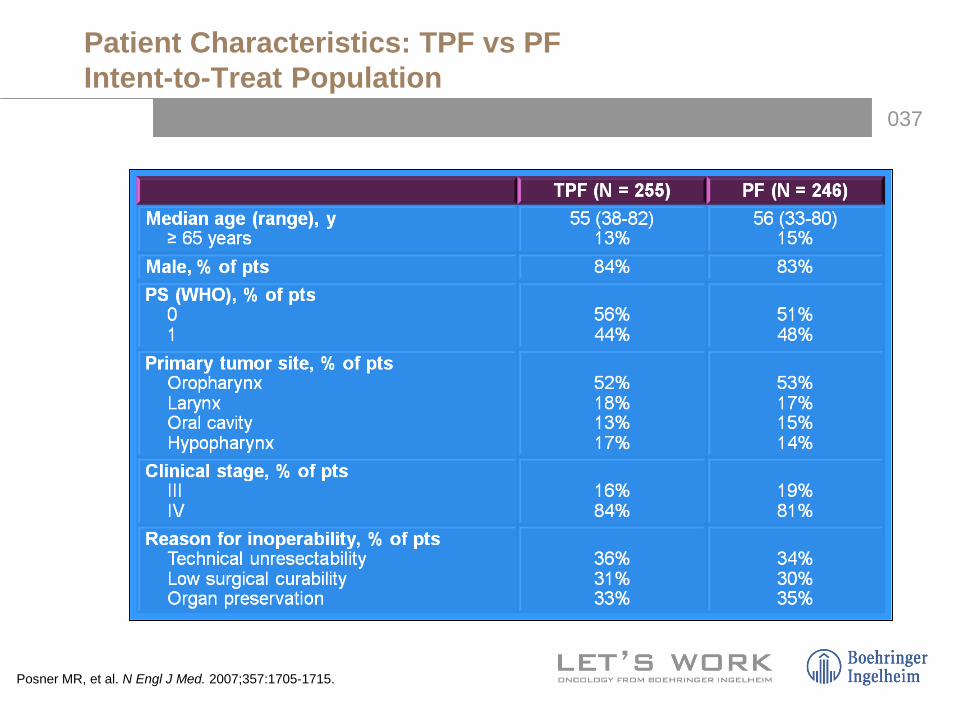
Patient Characteristics: TPF vs PFIntent-to-Treat Population
Posner MR, et al. N Engl J Med. 2007;357:1705-1715.
038
PFS in overall populationPFS in overall population
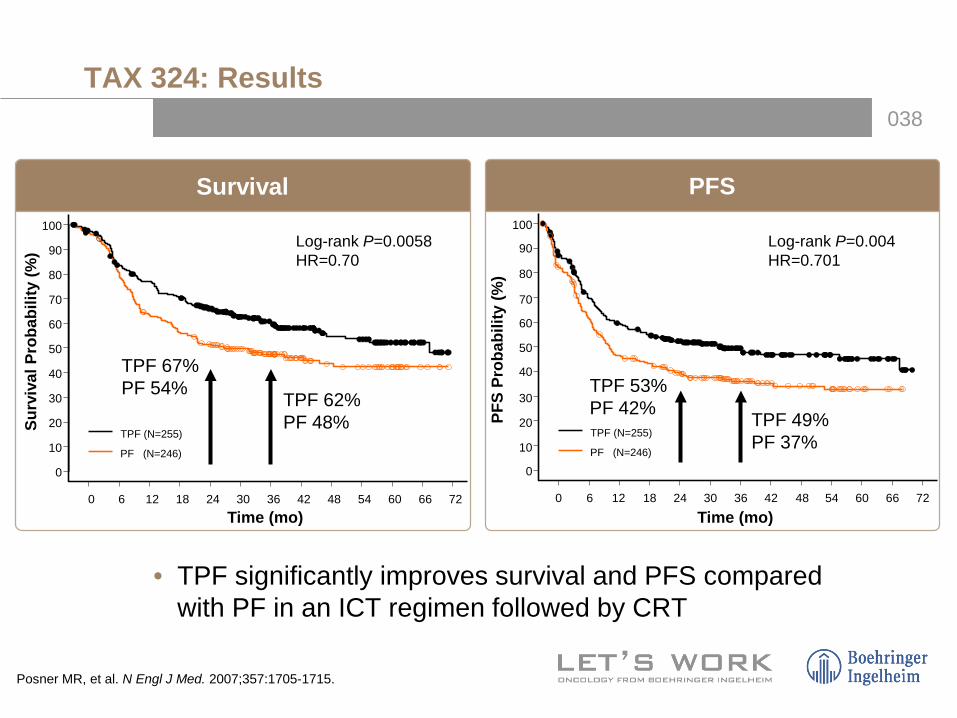
TAX 324: Results
• TPF significantly improves survival and PFS compared with PF in an ICT regimen followed by CRT
TPF 62%PF 48%
TPF 67%PF 54%
Log-rank P=0.0058HR=0.70
TPF 53%PF 42% TPF 49%
PF 37%
Log-rank P=0.004HR=0.701
Survival PFS
Time (mo)
Surv
ival
Pro
babi
lity
(%)
0 6 12 18 24 30 36 42 48 54 60 66 72
0
10
20
30
40
50
60
70
80
90
100
TPF (N=255)
PF (N=246)
Time (mo)PF
S Pr
obab
ility
(%)
0 6 12 18 24 30 36 42 48 54 60 66 72
0
10
20
30
40
50
60
70
80
90
100
TPF (N=255)
PF (N=246)
Posner MR, et al. N Engl J Med. 2007;357:1705-1715.

039
PFS in overall population
TAX 324 Phase III Trial: Docetaxel/Cisplatin/5-FU vs Cisplatin/ 5-FU Sequential Therapy in Advanced SCCHN—Toxicity
Grade 3/4 Toxicity TPF PFStomatitis 21% 27%
Nausea 14% 14%
Lethargy 5% 10%
Vomiting 8% 10%
Diarrhoea 7% 3%
Anorexia 12% 12%
Neutropaenia 83% 56%
Febrile neutropaenia 12% 7%
Neutropaenic infection 12% 8%Stomatitis 37% 38%
Dysphagia 23% 24%
Mouth, nose dryness 5% 4%
Nausea 6% 6%
Rash/itch 5% 2%
During ICTN=251 TPF,
243 PF
During CRTN=203 TPF,
184 PF
Posner MR, et al. N Engl J Med. 2007;357:1705-1715.

040
PFS in overall population
Taxane + PF Phase III Trials
Vermorken (2007)1 Hitt (2005)2
Chemo PF DPF PF PaPF
Subjects 181 177 193 189
Med PFS* 8.2 mo 11.0 mo 12 mo 20 mo
Med OS* 14.5 mo 18.8 mo 37 mo 43 mo
RR* 54% 68% 68% 80%
P<0.05 for all outcomes except P=0.06 for OS in Hitt study.1. Vermorken JB, et al. N Engl J Med. 2007;357:1695-1704.2. Hitt R, et al. J Clin Oncol. 2005;23:8636-8645.

041
Conclusions
• Overall survival advantage >3 years with TPF sequential therapy
– 40.5-month improvement in median overall survival at 3 years– 30% reduction in the risk of mortality (P=0.0058)
Consistent with prior phase III trial (TAX 323)
• Patients received a median of 3 cycles of induction chemotherapy in the TPF and PF arms
• In the TPF arm, 81% of patients went on to receive CRT
• Grade 3/4 treatment-emergent adverse events– Less stomatitis, thrombocytopaenia, and lethargy in the
TPF arm– More neutropaenia and febrile neutropaenia (any grade) in the
TPF arm
042
Impact of Induction Chemotherapy (CT):Opposing Views and Ongoing Controversy
• Pro: Allows time to optimise patient medical status; Possible customisation of RT dosing based on response to treatment; provides early treatment of distant micrometastatic disease
• Con: Induction CT may affect adversely compliance to subsequent concurrent CT/RT or choice of CT/RT regimen; adds 2-4 months to treatment

043
Clinical Scenarios to Consider Induction Therapy
1. Potential distant metastasis
2. Delay in radiation simulation
3. Impending local issue (eg, airway)
4. Markedly advanced disease (eg, bulky, N2c, N2b, N3, low neck, dermal infiltration)
5. Organ preservation strategy in patients with markedly advanced disease
044
Neck Dissection (ND)After Chemoradiotherapy
• Indicated for gross residual disease
• Not indicated for pretreatment N1 disease that has achieved clinical complete response
• For pretreatment N2-3 disease, opinions vary: – When pretreatment neck disease is N2-3, some centres
choose routine ND regardless of response to chemoradiotherapy
– However, others will observe if a clinical complete response on PET scan 12 weeks post-therapy is achieved with chemoradiotherapy
Pellitteri PK, et al. Head Neck. 2006;28:166-175.Ong SC, et al. J Nucl Med. 2008;49:532-540.
045
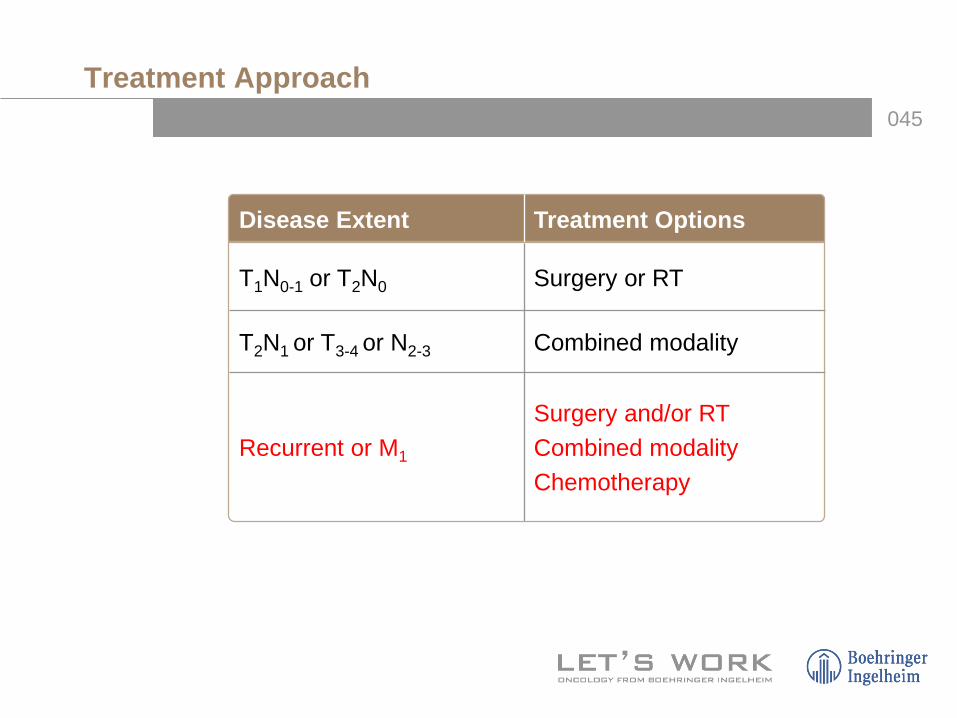
Treatment Approach
Disease Extent Treatment Options
T1N0-1 or T2N0 Surgery or RT
T2N1 or T3-4 or N2-3 Combined modality
Recurrent or M1
Surgery and/or RTCombined modalityChemotherapy
046
Palliative Chemotherapy
047
Palliative Chemotherapy
• Treatment for recurrent disease without surgical or radiotherapy option
• 1st line therapy: – Historically platinum-based doublet – Overall RR 30%-40% – Median survival 6-9 months regardless of treatment– Randomised controlled trials fail to demonstrate clear
improvement in OS compared to RX with single agents
• Active agents: cisplatin, carboplatin, 5-FU, taxanes, methotrexate, cetuximab, ifosfamide, gemcitabine (for nasopharynx cancer) and others
DeVita VT, et al. Cancer: Principles & Practice of Oncology. 8th ed. Lippincott Williams & Wilkins; 2008.
048
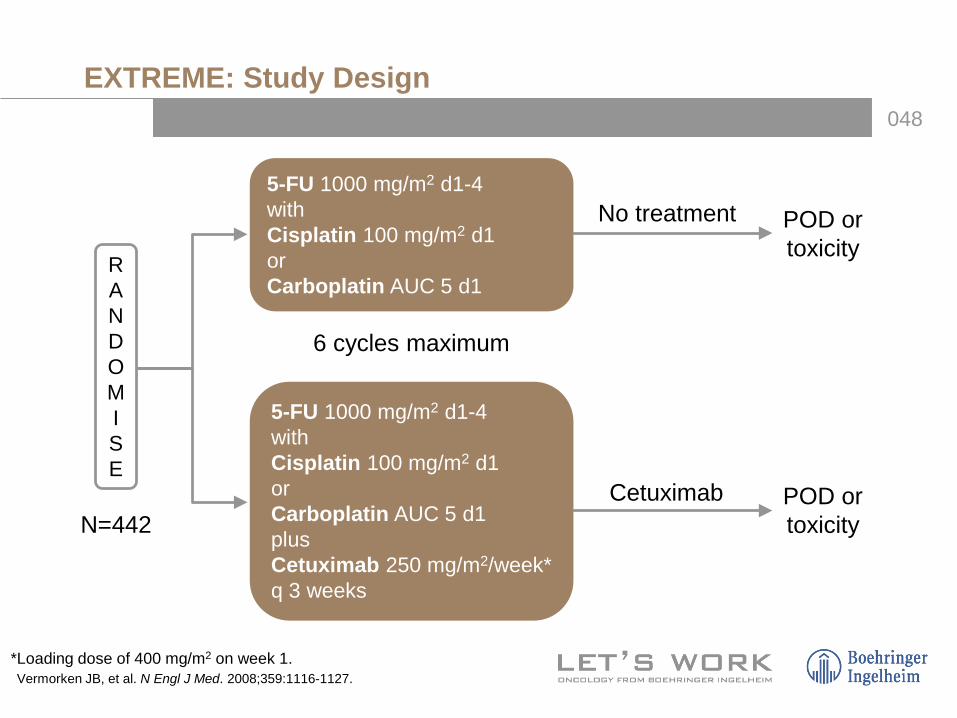
EXTREME: Study Design
5-FU 1000 mg/m2 d1-4withCisplatin 100 mg/m2 d1orCarboplatin AUC 5 d1plusCetuximab 250 mg/m2/week*q 3 weeks
*Loading dose of 400 mg/m2 on week 1.Vermorken JB, et al. N Engl J Med. 2008;359:1116-1127.
RANDOMISE
N=442
5-FU 1000 mg/m2 d1-4withCisplatin 100 mg/m2 d1orCarboplatin AUC 5 d1
No treatment
6 cycles maximum
POD ortoxicity
Cetuximab POD ortoxicity

049
PFS in overall population
EXTREME: First-Line Platinum/5-FU ± Cetuximab in Recurrent/Metastatic SCC: Survival
10.1 mos7.4 mos
Survival Time (months)Patients at Risk:
Platinum/5-FUCetuximab + Platinum/5-FU
220 173 127 83 65 47 19 8 1222 184 153 118 82 57 30 15 3
HR (95% CI)=0.797 (0.644-0.986)Strat. log-rank test: 0.0362
Platinum/5-FUCetuximab + Platinum/5-FU
Surv
ival
Pro
babi
lity
0.00.10.20.30.40.50.60.70.80.91.0
0 3 6 9 12 15 18 21 24
OSRR
18%35%
Vermorken JB, et al. N Engl J Med. 2008;359:1116-1127.
050
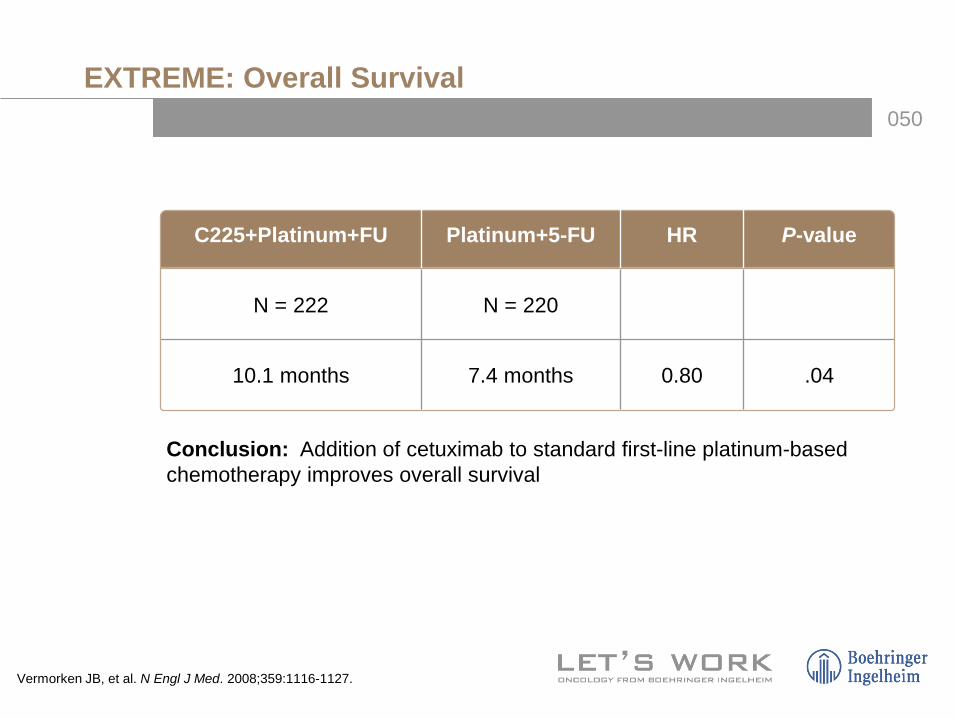
EXTREME: Overall Survival
C225+Platinum+FU Platinum+5-FU HR P-value
N = 222 N = 220
10.1 months 7.4 months 0.80 .04
Conclusion: Addition of cetuximab to standard first-line platinum-based chemotherapy improves overall survival
Vermorken JB, et al. N Engl J Med. 2008;359:1116-1127.

051
Phase II Trial: Cetuximab Monotherapy in Platinum-Refractory Recurrent/Metastatic SCC
Platinum-refractory SCC• Stage III/IV recurrent and/or
metastatic SCC not suitable for local therapy
• Documented PD within 30 days of cisplatin- or carboplatin-based chemotherapy (≥2 and ≤6 cycles)
• Tumour tissue available for IHC of EGFR expression
• No nasopharyngeal carcinoma• No nonplatinum chemotherapy
or RT within past 3 wks• No prior/concomitant surgery
within 30 days of enrollment
N=103
CR, PR, or SDContinue cetuximab until PD
PDOptional: cisplatin or
carboplatin + cetuximab N = 53
Monotherapy (continued if CR, PR, SD)
Vermorken JB, et al. N Engl J Med. 2008;359:1116-1127.Trigo J, et al. Presented at: American Society of Clinical Oncology 2004 Annual Meeting. Abstract 5502. Published as Trigo J, et al. J Clin Oncol. 2004;22:5502.
Cetuximab(400 mg/m2 then by
250 mg/m2/wk)≥6 wks
052
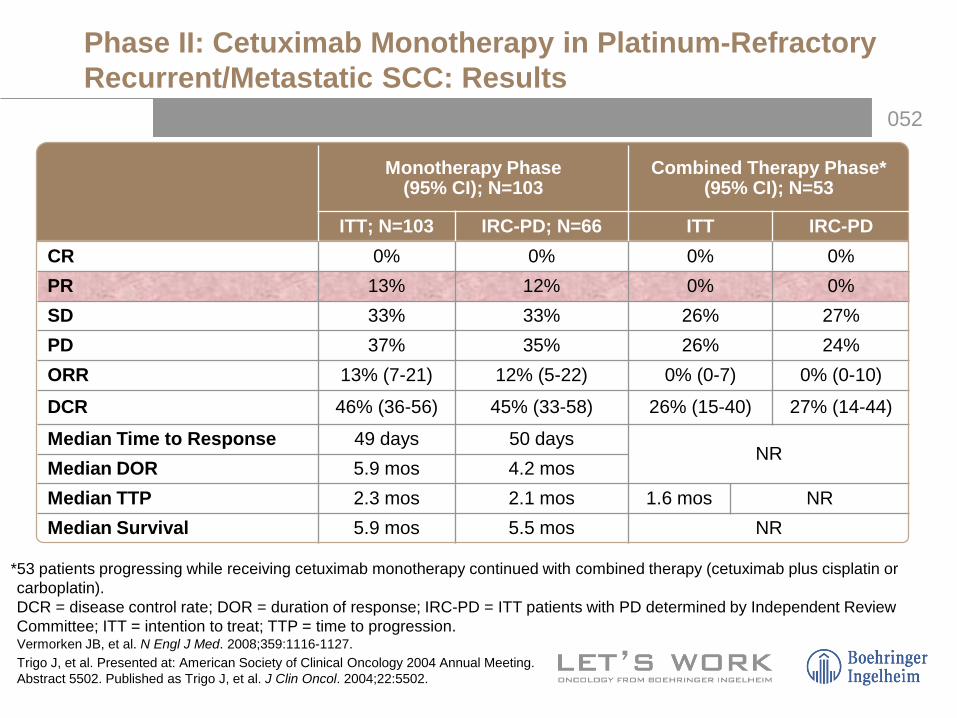
Phase II: Cetuximab Monotherapy in Platinum-Refractory Recurrent/Metastatic SCC: Results
Monotherapy Phase (95% CI); N=103
Combined Therapy Phase* (95% CI); N=53
ITT; N=103 IRC-PD; N=66 ITT IRC-PDCR 0% 0% 0% 0%PR 13% 12% 0% 0%SD 33% 33% 26% 27%PD 37% 35% 26% 24%ORR 13% (7-21) 12% (5-22) 0% (0-7) 0% (0-10)
DCR 46% (36-56) 45% (33-58) 26% (15-40) 27% (14-44)
Median Time to Response 49 days 50 daysNR
Median DOR 5.9 mos 4.2 mosMedian TTP 2.3 mos 2.1 mos 1.6 mos NRMedian Survival 5.9 mos 5.5 mos NR
*53 patients progressing while receiving cetuximab monotherapy continued with combined therapy (cetuximab plus cisplatin or carboplatin).DCR = disease control rate; DOR = duration of response; IRC-PD = ITT patients with PD determined by Independent Review Committee; ITT = intention to treat; TTP = time to progression.Vermorken JB, et al. N Engl J Med. 2008;359:1116-1127.Trigo J, et al. Presented at: American Society of Clinical Oncology 2004 Annual Meeting. Abstract 5502. Published as Trigo J, et al. J Clin Oncol. 2004;22:5502.
053
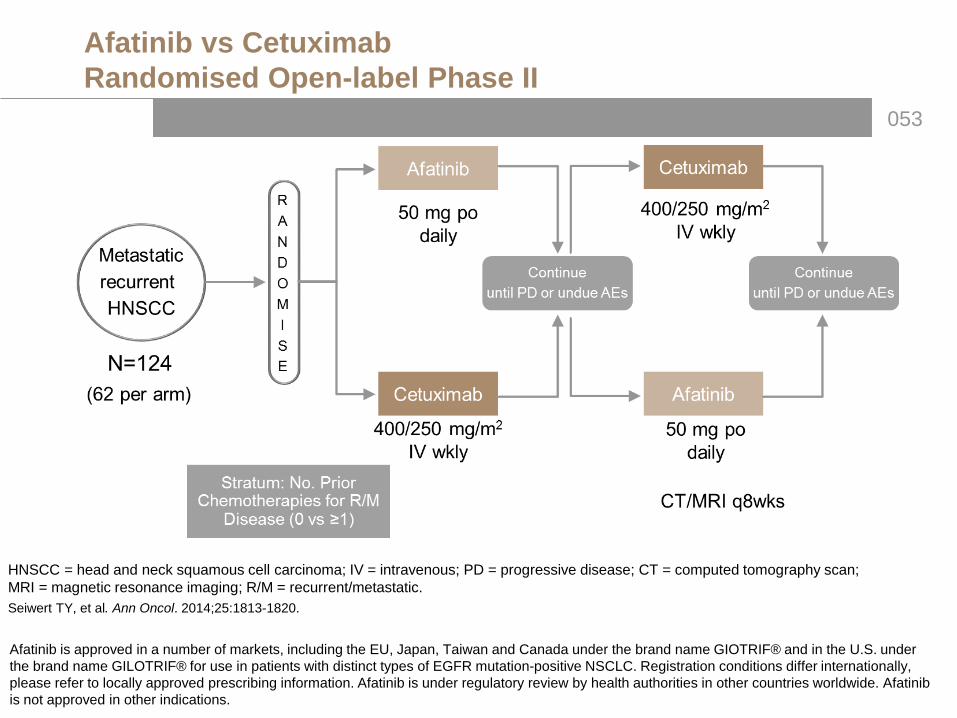
Afatinib vs CetuximabRandomised Open-label Phase II
HNSCC = head and neck squamous cell carcinoma; IV = intravenous; PD = progressive disease; CT = computed tomography scan; MRI = magnetic resonance imaging; R/M = recurrent/metastatic.Seiwert TY, et al. Ann Oncol. 2014;25:1813-1820.
Afatinib is approved in a number of markets, including the EU, Japan, Taiwan and Canada under the brand name GIOTRIF® and in the U.S. under the brand name GILOTRIF® for use in patients with distinct types of EGFR mutation-positive NSCLC. Registration conditions differ internationally, please refer to locally approved prescribing information. Afatinib is under regulatory review by health authorities in other countries worldwide. Afatinibis not approved in other indications.

054
Response to Therapy (Randomised Set) Stage 1Afatinib vs Cetuximab Open-label Phase II
Stage 1 TreatmentAfatinib
n=62Cetuximab
n=62P value
Disease control (CR, PR, SD)
50.0% 56.5% 0.48
Objective response (CR, PR) 16.1% 6.5% 0.09
Confirmation was made per protocol after 8 wks.Evaluable patients are those with at least 1 post-baseline image (afatinib = 52 and cetuximab = 57).
Per investigator assessment
Seiwert TY, et al. Ann Oncol. 2014;25:1813-1820.

055
Stage 2 Disease Control Rate: Afatinib vs Cetuximab
Seiwert TY, et al. Ann Oncol. 2014;25:1813-1820.
Cetuximab (after prior Afatinib) n=3219%
Afatinib (after prior Cetuximab) n=3633%
056
0
10
20
30
40
50
60
70
80
90
Patie
nts
(%)
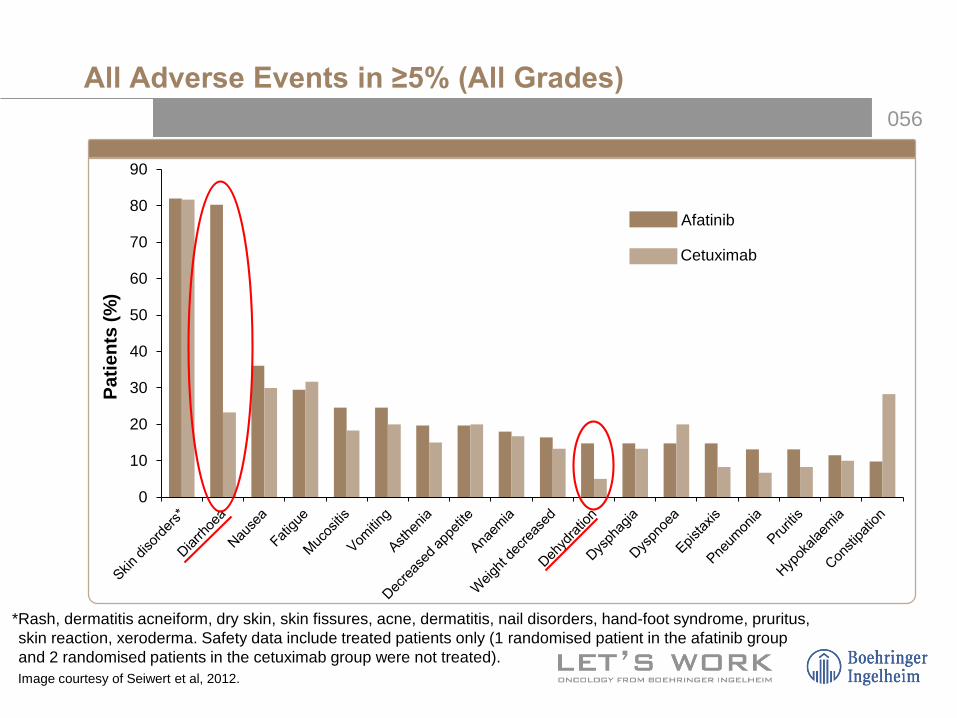
All Adverse Events in ≥5% (All Grades)
Afatinib
Cetuximab
*Rash, dermatitis acneiform, dry skin, skin fissures, acne, dermatitis, nail disorders, hand-foot syndrome, pruritus, skin reaction, xeroderma. Safety data include treated patients only (1 randomised patient in the afatinib group and 2 randomised patients in the cetuximab group were not treated).Image courtesy of Seiwert et al, 2012.

057
Trial Design End Points Study Sites
Phase III, Randomised, Open-Label
Primary: PFS Key Secondary: OS; HR 0.73
Global
R/M HNSCC • Failing Platinum-Based CT for R/M HNSCC
• Documented PD• PS = 0–1• Max 1 CT Regimen for R/M HNSCC
• No Prior EGFR TKIs
RANDOMISE
2:1
Afatinib 40 mg qdp.o.
N=316
MTX 40 mg/m2 qw i.v.
N=158
LUX: HNC 1 (1200.43) Afatinib vs MTX in Second-Line R/M HNSCC
Treatment Until PD
N=483
Stratified by: ECOG PS, previous EGFR-targeted mAb for recurrent or metastatic disease
Machiels JP, et al. Lancet Oncol. 2015;16:583-594.
058
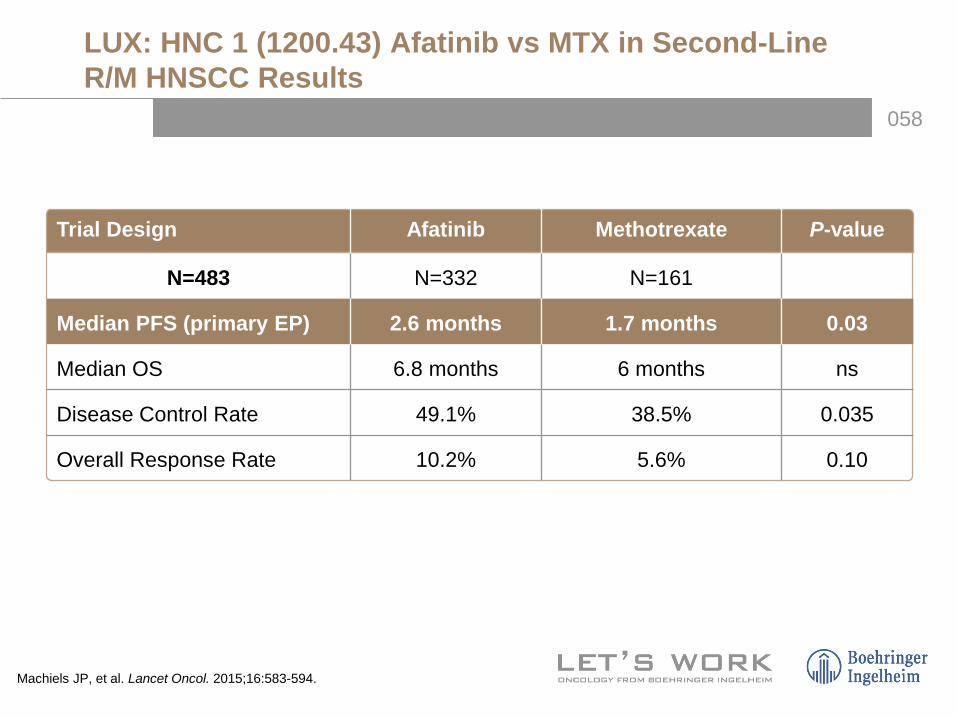
Trial Design Afatinib Methotrexate P-value
N=483 N=332 N=161
Median PFS (primary EP) 2.6 months 1.7 months 0.03
Median OS 6.8 months 6 months ns
Disease Control Rate 49.1% 38.5% 0.035
Overall Response Rate 10.2% 5.6% 0.10
LUX: HNC 1 (1200.43) Afatinib vs MTX in Second-Line R/M HNSCC Results
Machiels JP, et al. Lancet Oncol. 2015;16:583-594.

059
Afatinib vs Methotrexate as 2nd-Line Treatment (LUX-H/N1)
Time (months)
0
0.2
0.4
0.6
0.8
1.0
0 3 6 9 12
Estim
ated
PFS
Pro
babi
lity
15 18
No. of patientsAfatinib 322 93 26 9 3 1 0MTX 161 28 6 2 0 0 0
Afatinib(n=322)
MTX(n=161)
PFS event, n (%) 275 (85.4) 135 (83.9)
Median PFS (months) 2.6 1.7
HR (95% CI) 0.80 (0.65–0.98)
Log-rank test p-value 0.03042.8%
30.5%
Machiels JP, et al. Lancet Oncol. 2015;16:583-594.

060Factors Number of
patients HR (95% CI)
Total 483 0.80 (0.65–0.98)
Baseline ECOG PS 01
131352
0.730.77
(0.49–1.10)(0.60–0.98)
Prior use of EGFR-targeted antibody for R/M HNSCC
NoYes
196287
0.630.91
(0.45–0.88)(0.70–1.19)
Gender MaleFemale
41271
0.740.95
(0.59–0.92)(0.55–1.64)
Age <65 years≥65 years
355128
0.790.68
(0.62–1.01)(0.45–1.03)
RegionAsiaEuropeNorth/Latin American
4336960
0.620.820.41
(0.32–1.20)(0.64–1.04)(0.21–0.79)
Smoking pack-years <10 pack years≥10 pack years
87381
1.050.71
(0.66–1.70)(0.56–0.90)
Alcohol consumption ≤7 units/week>7 units/week
37491
0.790.73
(0.62–1.00)(0.46–1.14)
Primary tumour site
Oral cavityOropharynxHypopharynxLarynx
13615393
101
0.690.990.780.59
(0.46–1.04)(0.68–1.44)(0.48–1.25)(0.38–0.92)
Recurrence or metastasesRecurrentMetastaticBoth
16764
241
0.591.180.81
(0.42–0.84)(0.65–2.14)(0.60–1.10)
p16 PositiveNegative
49208
0.950.69
(0.51–1.75)(0.50–0.96)
Response to prior platinum therapy for R/M HNSCC
CR/PR/SDPD
261146
0.820.66
(0.62–1.09)(0.45–0.96)
PFS Subgroup Analysis
Favours Afatinib1/4 11/16 4 16
Favours Methotrexate Machiels JP, et al. Lancet Oncol. 2015;16:583-594.

061
FactorsNumber of
patientsAdjusted mean
difference (95% CI)
Pain HN35 (Q1–Q4 from QLQ-HN35) 382 –4.4 (–8.3, –0.4)
Pain in mouth (Q1) 380 –3.7 (–9.2, 1.7)
Pain in jaw (Q2) 380 –7.5 (–12.5, –2.5)
Soreness in mouth (Q3) 380 –2.5 (–8.0, 2.9)
Painful throat (Q4) 382 –4.3 (–9.2, 0.6)
Swallowing scale (Q5–Q8 from QLQ-HN35) 369 –0.1 (–4.3, 4.2)
Problem swallowing liquid (Q5) 373 –2.5 (–8.3, 3.2)
Problem swallowing pureed food (Q6) 365 –1.1 (–6.6, 4.4)
Problem swallowing solid food (Q7) 364 0.0 (–5.8, 5.8)
Choked when swallowing (Q8) 361 2.5 (–2.9, 7.9)
Global health status (Q8–Q9 from QLQ-C30) 384 –0.6 (–4.4, 3.3)
Overall health rate (Q29) 384 –0.5 (–4.5, 3.5)
Quality of life rate (Q30) 378 –0.3 (–4.5, 3.9)
Changes in Patient-reported Outcomes Over Time
– 10 0–20 2010Favours Afatinib Favours Methotrexate Machiels JP, et al. Lancet Oncol. 2015;16:583-594.

062
Afatinib Clinical Programme in HNSCC
LUX-Head & Neck 12nd line R/MPublished2
LUX-Head & Neck 2 Adjuvant, LA
Recruiting
Afatinib vs CetuximabPhase II PoC
Published1
LUX-Head & Neck 32nd line R/MRecruiting
LUX-Head & Neck 4Adjuvant, LA
Recruiting
Asian Bridging Trials (Ph III)
1. Seiwert TY, et al. Ann Oncol. 2014;25:1813-1820; 2. Machiels JP, et al. Lancet Oncol. 2015;16:583-594; 3. ClinicalTrials.gov Identifiers: NCT01345669 (LHN2), NCT 01856478 (LHN3), NCT 02131155 (LHN4), NCT 01427478 (BIBW2992ORL).
Pivotal Phase III Trials
Recurrent/Metastatic
Locally advanced
BIBW2992ORL
Maintenance, LARecruiting

063
Conclusions
• Afatinib significantly improved PFS vs methotrexate
• Tumour shrinkage was greater, response rate higher and DCR significantly higher compared to methotrexate
• Patient-reported outcomes favoured afatinib over methotrexate
• OS was not significantly different between afatinib and methotrexate
• Overall AE profiles were as expected– Fewer treatment-related dose reductions, discontinuations and fatal
events with afatinib compared to methotrexate
• Afatinib has shown efficacy and improved patient-reported outcomes in a Phase III trial in this setting
• Investigations with adjuvant afatinib in LA HNSCC following CRT are ongoing
064
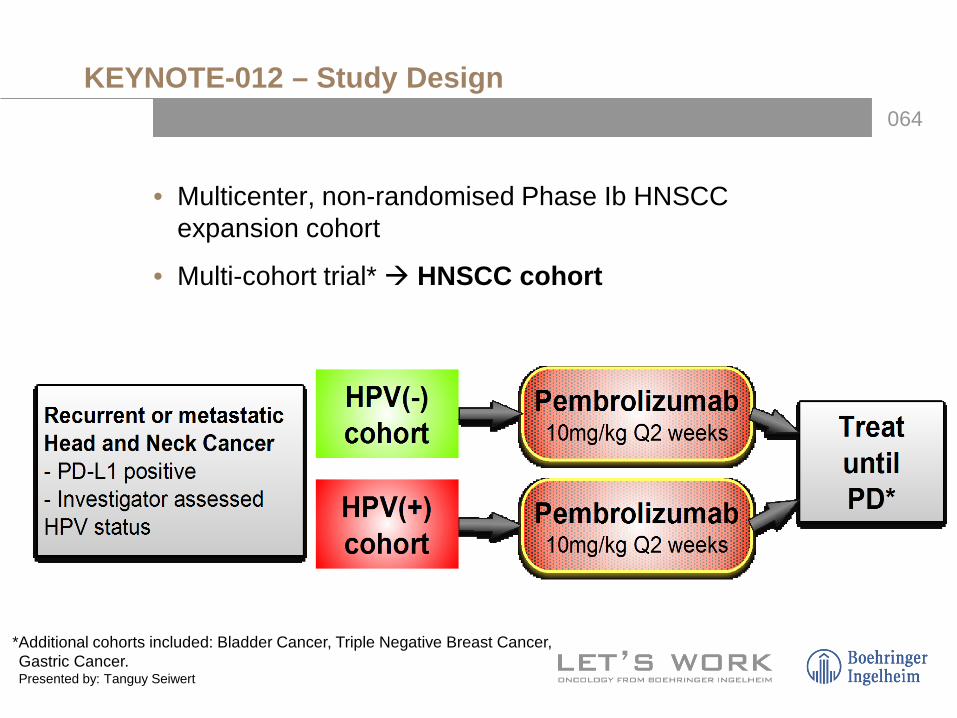
KEYNOTE-012 – Study Design
• Multicenter, non-randomised Phase Ib HNSCC expansion cohort
• Multi-cohort trial* HNSCC cohort
*Additional cohorts included: Bladder Cancer, Triple Negative Breast Cancer, Gastric Cancer.Presented by: Tanguy Seiwert

065
Phase Ib Study of Pembrolizumab (MK-3475) in Patients With HPV-negative and HPV-positive HNSCC: Efficacy Waterfall Plot
Seiwert T, et al. ASCO 2014. Abstract 6011.
51% (26/51) of patients had decreased tumour burden
HPV (+)HPV (-)
Subjects–100
–80
–60
–40
–20
0
20
40
60
80
100
Cha
nge
From
Bas
elin
e, %
56 pts evaluable for response Total Head/Neck N=56†
HPV (+)N=20
HPV (-)N=36§
Response Evaluation n (%) n (%) n (%) Best Overall Response
(Complete + Partial)‡ 11 (19.6) 4 (20.0) 7 (19.4)

066
Best Overall Response
• PD-L1 expression correlates with Response
• Using a Youden-Index derived, preliminary PD-L1 cut point:– Above cutpoint: 45.5% (5/11) RR– Below cutpoint: 11.4% (5/44) RR
56 pts evaluable for response
Total Head/neck N=56*
HPV (+)N=20
HPV (-)N=36§
Response Evaluation n (%) 95% CI† n (%) 95% CI† n (%) 95% CI†
Complete Response 1 (1.8) (0.0, 9.6) 1 (5.0) (0.1, 24.9) 0 (0.0) (0.0, 9.7)
Partial Response 10 (17.9) (8.9, 30.4) 3 (15.0) (3.2, 37.9) 7 (19.4) (8.2, 36.0)
Best Overall Response (Complete + Partial)‡ 11 (19.6) (10.2, 32.4) 4 (20.0) (5.7, 43.7) 7 (19.4) (8.2, 36.0)
Stable Disease 16 (28.6) (17.3, 42.2) 8 (40.0) (19.1, 63.9) 8 (22.2) (10.1, 39.2)
Progressive Disease 25 (44.6) (31.3, 58.5) 7 (35.0) (15.4, 59.2) 18 (50.0) (32.9, 67.1)
No Assessment 4 (7.1) (2.0, 17.3) 1 (5.0) (0.1, 24.9) 3 (8.3) (1.8, 22.5)
Based on RECIST 1.1 Per site assessment; includes confirmed and unconfirmed responses.*61 patients eligible for treatment; 60 patients dosed; 56 patients eligible for pre-defined full analysis set. †Based on binomial exact confidence interval method.‡A single patient with PD followed by PR on treatment was classified as PR.§Includes 2 patients for whom HPV data were unavailable.Slide courtesy of Tanguy Seiwert.

067
Presente
068
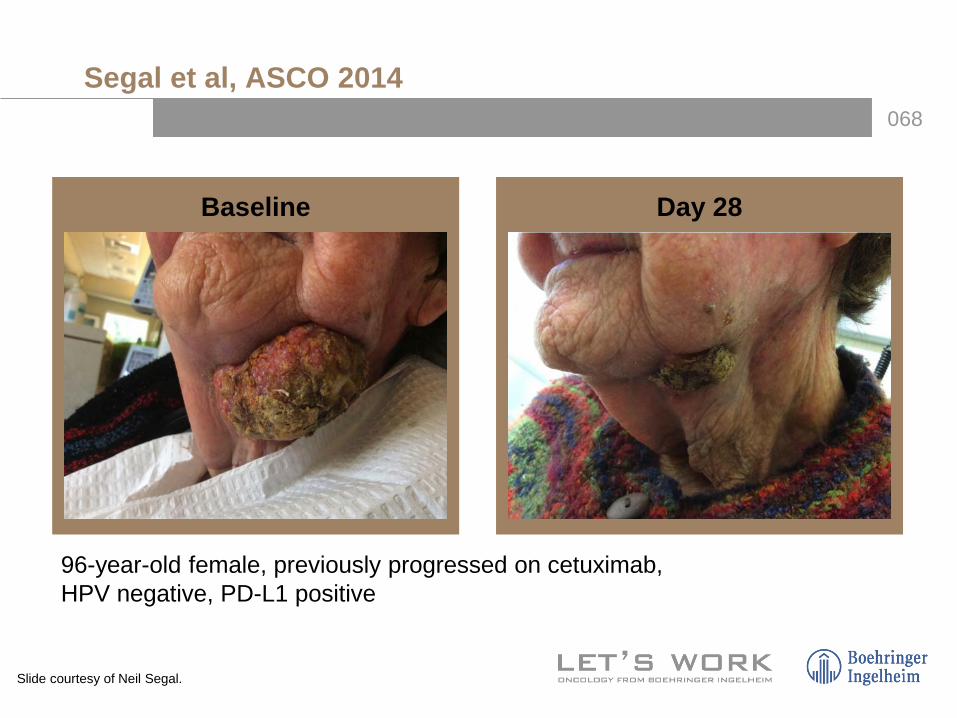
Segal et al, ASCO 2014
Baseline Day 28
Slide courtesy of Neil Segal.
96-year-old female, previously progressed on cetuximab, HPV negative, PD-L1 positive
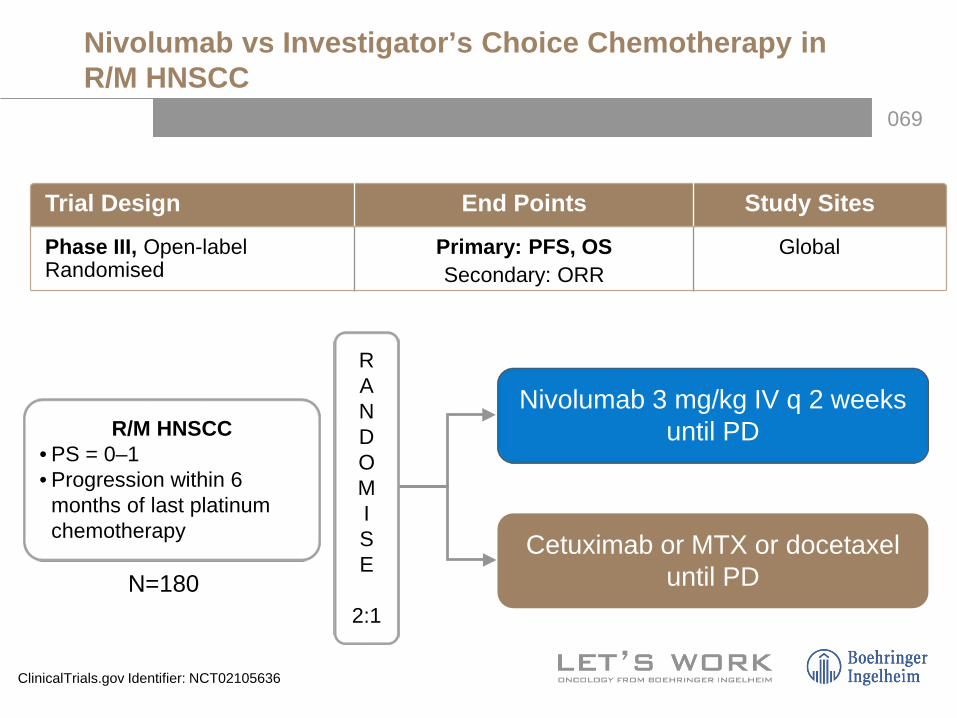
069
Trial Design End Points Study Sites
Phase III, Open-label Randomised
Primary: PFS, OS Secondary: ORR
Global
R/M HNSCC • PS = 0–1• Progression within 6 months of last platinum chemotherapy
RANDOMISE
2:1
Nivolumab 3 mg/kg IV q 2 weeks until PD
Cetuximab or MTX or docetaxeluntil PD
Nivolumab vs Investigator’s Choice Chemotherapy in R/M HNSCC
N=180
ClinicalTrials.gov Identifier: NCT02105636
070
Comprehensive Genomic Characterisation of Squamous Cell Carcinoma of the Head and Neck
January 2015

071
The Genetic Wiring of HNSCCs
TCGA Network. Nature. 2015.
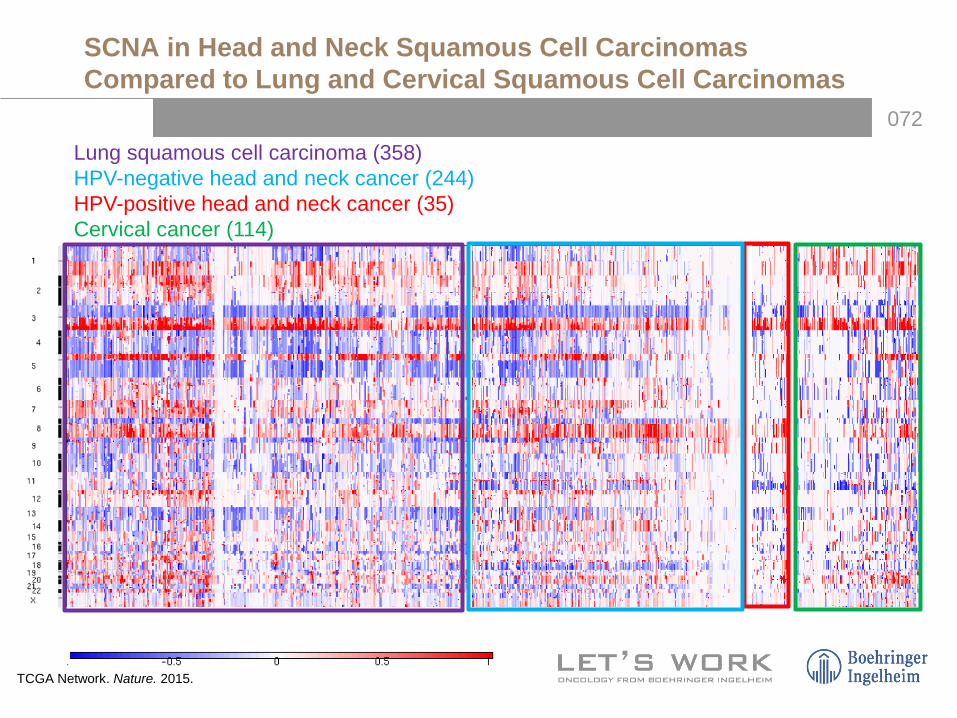
072Lung squamous cell carcinoma (358)HPV-negative head and neck cancer (244)HPV-positive head and neck cancer (35)Cervical cancer (114)
SCNA in Head and Neck Squamous Cell Carcinomas Compared to Lung and Cervical Squamous Cell Carcinomas
TCGA Network. Nature. 2015.

073
Candidate Therapeutic Targets
TCGA. Nature. 2015.

074
Response to Pazopanib in a Patient With a FGFR2 Mutation
2 weeks pazopanib
FGFR2 P253R
Liao et al. 2013.

075ABL1 AKT1 AKT2 AKT3 ALK ALOX12B APC AR ARAF ARID1A ASXL1 ATM ATRX AURKA AURKB AXL B2M BAP1 BCL2 BCL2L12 BCL6 BCOR BCORL1 BLM BMPR1A BRAF BRCA1 BRCA2 BRD4 BRIP1
BUB1B CARD11 CBL CBLB CCND1 CCND2 CCND3 CCNE1 CD274 CD58 CD79B CDC73 CDH1 CDK1 CDK2 CDK4 CDK5 CDK6 CDK9 CDKN2A CDKN2B CDKN2C CEBPA CHEK2 CIITA CREBBP CRKL CRLF2 CRTC1 CRTC2
CTNNB1 CUX1 CYLD DDB2 DDR2 DICER1 DIS3 DMD DNMT3A EED EGFR EP300 EPHA3 EPHA5 EPHA7 ERBB2 ERBB3 ERBB4 ERCC2 ERCC3 ERCC4 ERCC5 ESR1 ETV1 ETV4 ETV5 ETV6 EWSR1 EXT1 EXT2
EZH2 FAM46C FANCA FANCC FANCD2 FANCE FANCF FANCG FAS FBXW7 FGFR1 FGFR2 FGFR3 FGFR4 FH FKBP9 FLCN FLT1 FLT3 FLT4 FUS GATA3 GATA4 GATA6 GLI1 GLI2 GLI3 GNA11 GNAQ GNAS
GPC3 GSTM5 H3F3A HNF1A HRAS ID3 IDH1 IDH2 IGF1R IGH@ IgK@ IgL@ IKZF1 IKZF3 JAK2 JAK3 KDM6B KDR KIT KRAS LMO1 MAP2K1 MCL1 MDM2 MDM4 MECOM MEF2B MEN1 MET MITF
MLH1 MLL MLL2 MPL MSH2 MSH6 MTOR MUTYH MYB MYBL1 MYC MYCL1 MYCN MYD88 NBN NF1 NF2 NFE2L2 NFKBIA NFKBIZ NKX2-1 NOTCH1 NOTCH2 NPM1 NRAS NTRK3 PALB2 PARK2 PAX5 PDCD1LG2
PDGFRA PDGFRB PHF6 PHOX2B PIK3C2B PIK3CA PIK3R1 PIM1 PMS1 PMS2 PNRC1 PRAME PRDM1 PRF1 PRKAR1A PRKCI PRKDC PRPF40B PRPF8 PSMD13 PTCH1 PTEN PTK2 PTPN11 RAD21 RAF1 RARA RB1 RBL2 RECQL4
REL RET RFWD2 RHPN2 ROS1 RPL26 RUNX1 SBDS SDHAF2 SDHB SDHC SDHD SETBP1 SF1 SF3B1 SH2B3 SMAD2 SMAD4 SMARCA4 SMARCB1 SMC1A SMC3 SMO SOCS1 SOX2 SRC SRSF2 STAG1 STAG2 STAT3
STK11 SUFU SUZ12 SYK TCF3 TERC TERT TET2 TNFAIP3 TP53 TRA@ TRB@ TRG@ TSC1 TSC2 U2AF1 VHL WRN WT1 XPA XPC XPO1 ZNF708 ZRSR2
Illumina HiSeq
Neal Lindeman – Director; Center for Advanced Molecular Diagnostics
Oncopanel – DFCI/BWH Targeted Next Generation Sequencing – Launched Summer 2013
076
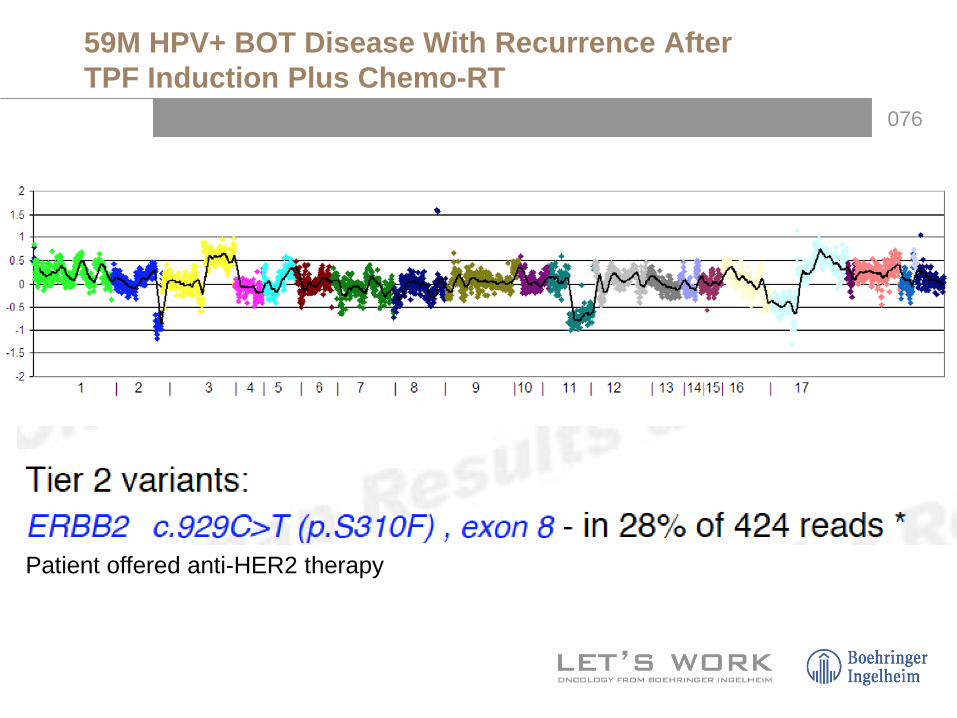
Patient offered anti-HER2 therapy
59M HPV+ BOT Disease With Recurrence After TPF Induction Plus Chemo-RT
077
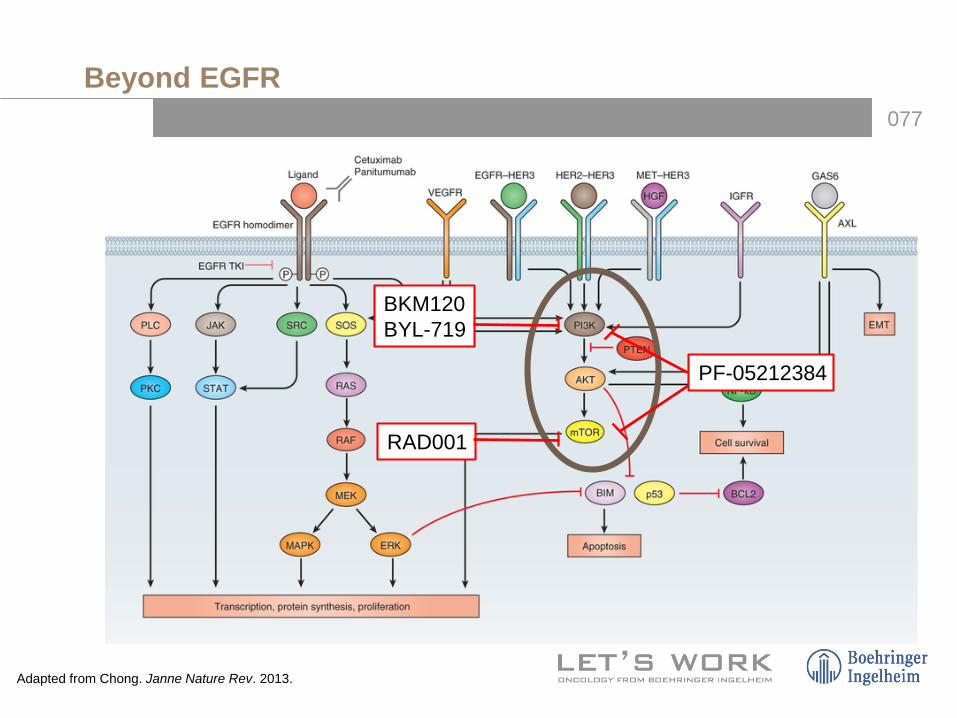
Beyond EGFR
Adapted from Chong. Janne Nature Rev. 2013.
BKM120BYL-719
PF-05212384
RAD001

078
Genomic Alterations in the Clinic
Commercial NGS DFHCC/BWH Profile NGS
079
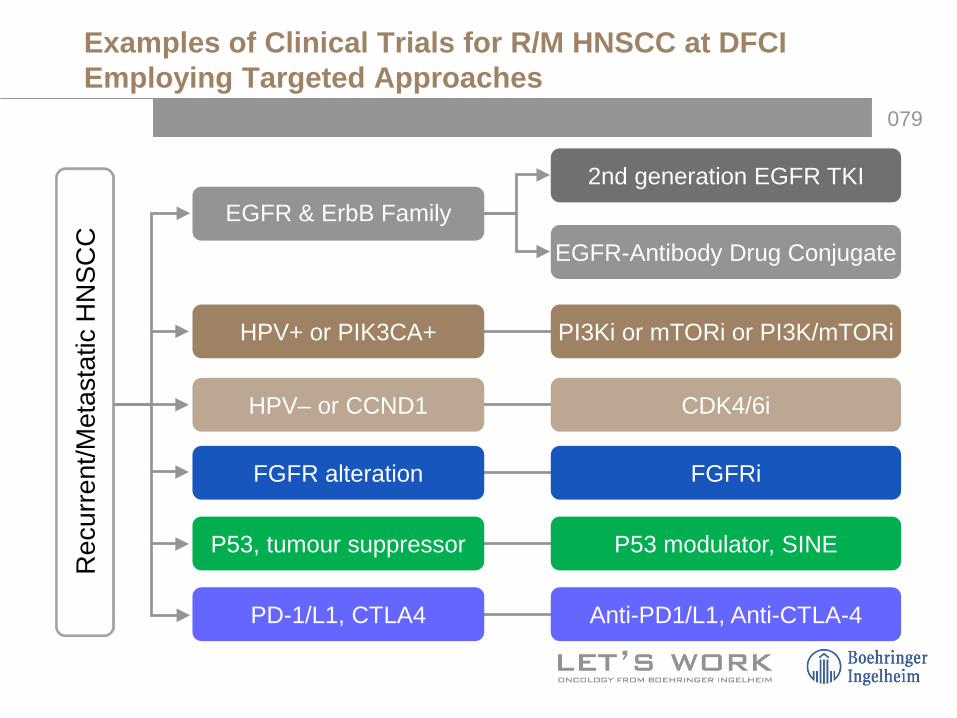
Examples of Clinical Trials for R/M HNSCC at DFCI Employing Targeted Approaches
EGFR & ErbB Family2nd generation EGFR TKI
EGFR-Antibody Drug Conjugate
HPV– or CCND1 CDK4/6i
FGFR alteration FGFRi
P53, tumour suppressor P53 modulator, SINE
PD-1/L1, CTLA4 Anti-PD1/L1, Anti-CTLA-4
Rec
urre
nt/M
etas
tatic
HN
SCC
PI3Ki or mTORi or PI3K/mTORiHPV+ or PIK3CA+

080
Conclusions: Treatment of SCCHN in 2015
• Multiple options available – Concurrent chemoRT– Sequential therapy: TPF is the standard induction
regimen – Targeted therapy: Cetuximab/RT
• Patient selection is important– Stage, patient characteristics, PS, and primary site
• HPV-related oropharynx disease is a major public health problem– HPV-positive and HPV-negative disease are distinct
entities Pts with HPV-positive disease demonstrate improved
responses to therapy and better survival De-intensification is a relevant research question