nmda receptor antagonists for the treatment ... -...
TRANSCRIPT

NEUROPATHIC PAIN SECTION
Review ArticleNMDA Receptor Antagonists for the Treatmentof Neuropathic Painpme_981 1726..1742
Susan Collins, MSc,*†‡ Marnix J. Sigtermans, MD,†§
Albert Dahan, Prof, MD,†§ Wouter W. A. Zuurmond,Prof, MD,*† and Roberto S. G. M. Perez, PhD*†‡
*Department of Anesthesiology, VU University MedicalCenter, Amsterdam;
†Knowledge Consortium Trauma Related NeuronalDysfunction, Leiden;
‡EMGO+ Institute for Health and Care Research,Amsterdam, VU University Medical Center,Amsterdam;
§Department of Anesthesiology, Leiden UniversityMedical Center, Leiden, the Netherlands
Reprint requests to: Susan Collins, MSc, VU UniversityMedical Center, Department of Anesthesiology, DeBoelelaan 1117, 1081 HV Amsterdam, theNetherlands. Tel: 003-120-444-0293; Fax:003-120-444-4385; E-mail: [email protected].
This study is part of TREND (Trauma RElatedNeuronal Dysfunction), a knowledge consortium thatintegrates research on Complex Regional PainSyndrome type 1 (CRPS 1). This project is supportedby a Dutch Government grant (BSIK03016).
Abstract
Objective. The N-methyl-D-Aspartate (NMDA)receptor has been proposed as a primary target forthe treatment of neuropathic pain. The aim of thepresent study was to perform a meta-analysis evalu-ating the effects of (individual) NMDA receptorantagonists on neuropathic pain, and the response(sensitivity) of individual neuropathic pain disordersto NMDA receptor antagonist therapy.
Design. PubMed (including MEDLINE), EMBASEand CENTRAL were searched up to October 26, 2009for randomized placebo controlled trials (RCTs) onneuropathic pain. The methodological quality of theincluded trials was independently assessed by twoauthors using the Delphi list. Fixed or random
effects model were used to calculate the summaryeffect size using Hedges’ g.
Setting. NA.
Patients. The patients used for the study were neu-ropathic pain patients.
Interventions. The interventions used were NMDAreceptor antagonists.
Outcome measurements. The outcome of measure-ments was the reduction of spontaneous pain.
Results. Twenty-eight studies were included,meeting the inclusion criteria. Summary effect sizeswere calculated for subgroups of studies evaluatingketamine IV in complex regional pain syndrome(CRPS), oral memantine in postherptic neuralgia and,respectively, ketamine IV, and oral memantine in pos-tamputation pain. Treatment with ketamine signifi-cantly reduced pain in postamputation pain (pooledsummary effect size: -1.18 [confidence interval (CI)95% -1.98, -0.37], P = 0.004). No significant effect onpain reduction could be established for ketamine IVin CRPS (-0.65 [CI 95% -1.47, 0.16], P = 0.11) oralmemantine in postherptic neuralgia (0.03 [CI 95%-0.51, 0.56], P = 0.92) and for oral memantine in pos-tamputation pain (0.38 [CI 95% -0.21, 0.98], P = 0.21).
Conclusions. Based on this systematic review, noconclusions can yet be made about the efficacy ofNMDA receptor antagonists on neuropathic pain.Additional RCTs in homogenous groups of painpatients are needed to explore the therapeuticpotential of NMDA receptor antagonists in neuro-pathic pain.
Key Words. Meta-Analysis; NMDA ReceptorAntagonists; Neuropathic Pain
Introduction
Neuropathic pain is pain arising as a direct consequenceof a lesion or disease affecting the somatosensory sys-tem [1]. Neuropathic pain is manifested in disorders ofvarious etiologies such as post-herpetic neuralgia, dia-betic neuropathy, and complex regional pain syndrome
Pain Medicine 2010; 11: 1726–1742Wiley Periodicals, Inc.
1726

[2]. Symptoms associated with neuropathic pain are allo-dynia, hyperalgesia, and spontaneous pain. A number ofmechanisms have been described that may contribute tothe generation of neuropathic pain. Examples includenociceptor sensitization, ectopic excitability of sensoryneurons, alterations in ion channel expression on theperipheral level and spinal and/or cortical reorganizationand changes in inhibitory pathways and central sensitiza-tion on the central level [3–5].
Several therapies have been developed for the treatmentof neuropathic pain; however, these methods are notequally effective for all neuropathic pain patients [6]. TheN-methyl-D-Aspartate (NMDA) receptor has been pro-posed as a primary target for the treatment of neuropathicpain. Evidence suggests that the NMDA receptor withinthe dorsal horn plays an important role in both inflamma-tion and nerve injury-induced central sensitization [7]. Pro-longed pain stimuli of high intensity induce a cascade ofevents which activate the NMDA receptor. Activation ofthe NMDA receptor is associated with abnormalities in thesensory (peripheral and central) system, resulting in neu-ronal excitation and abnormal pain manifestations (spon-taneous pain, allodynia, hyperalgesia) [8–10]. Blocking ofthese receptors by antagonists may possibly impede orreverse the pain pathology, leading to a reduction of pain[11].
The effects of NMDA receptor antagonists on neuro-pathic pain patients of various etiologies have beeninvestigated in clinical trials in which positive as well asnegative outcomes on pain relief were found. Consider-ing the present ambiguity with respect to the generalefficacy of NMDA receptor antagonists, a research syn-thesis of literature is warranted. To date, no meta-analysis has been performed with respect to the efficacyof NMDA receptor antagonists for treatment of featuresof neuropathic pain.
Therefore, the aim of the present study was to perform ameta-analysis evaluating the effects of NMDA receptorantagonists on neuropathic pain.
Furthermore, subgroup analyses will be performed inassessing the effects of individual NMDA receptor antago-nists on neuropathic pain and their response on individualneuropathic pain disorders, testing the hypothesis thatNMDA receptor antagonists are effective in the treatmentof neuropathic pain.
Methods
Inclusion Criteria
Studies were sought that examined the effect of NMDAreceptor antagonists on spontaneous pain in acute andchronic neuropathic pain [1] patients of all ages. Studieshad to be blinded, randomized, placebo controlled, andthe outcome pain had to be recorded on a numericalrating scale.
Search Strategy
PubMed (including MEDLINE) (from 1966 to October 26,2009), EMBASE (Elsevier Embase.com) (from 1980 toOctober 26, 2009) and Cochrane Central Register ofControlled Trials (CENTRAL) databases were searchedfor studies written in the English, German or Dutchlanguage. In PubMed, MeSH terms (“Receptors, N-Methyl-D-Aspartate/antagonists and inhibitors,” “N-Methylaspartate/antagonists and inhibitors,” “Pain,” “Anal-gesia,” “Analgesia, Patient-Controlled,” “Analgesics,”“Hyperalgesia,” “Sensation,” “Proprioception”) were usedas well as free text terms (“nmda, N-Methyl-D-Aspartate,”“inhibit*,” “block*,” “antagoni*,” “pain,” “pains,” “analgesi*,”“hyperalgesi*,” “allodynia,” “hyperaesthesia,” “hyperes-thesi*,” “ache,” “aches,” “neuralgi*,” “neuropath*,” “sensi-tization,” “sensitization,” “arthralgi*,” “proprioception,”“sensation,” sciatica,” “metatarsalgia”). In addition, a ran-domized placebo controlled trials (RCTs) search filter rec-ommended by the Cochrane Collaboration was used [12].
EMBASE was searched with the EMtree terms: “n Methyld aspartic acid receptor blocking agent,” “Pain,” “Analge-sia,” and “Analgesic agent.”
CENTRAL was searched with the search terms: NMDAand “N Methyl D Aspartate” linked to inhibition*, inhibited,inhibit, block* and antagoni*, as well as the search termspain, pains, analgesi*, hyperalgesi*, allodynia, hyperaes-thesi*, hyperesthesi*, ache, aches, neuralgi*, neuropath*,sensitization, sensitization, arthralgi*, proprioception, sen-sation, sciatica, and metatarsalgia.
Quality Assessments
In order to determine the quality of the studies, identifiedstudies were independently scored by the authors SC andMS using the Delphi list [13]. The Delphi list consists ofnine items, with addition of two criteria (“Were theoutcome measurements described clearly” and “Wereadverse events described?”) to ascertain the method-ological and clinical accuracy of the trials. All criteria werescored with yes (= 1), no (= 0), or don’t know (0), withequal weights given to all criteria. The number of positivescores contributed to the quality scores, ranging from 0 to11. Disagreements were solved by consensus and if nec-essary by a third party (RP), studies with scores of 6 orhigher were considered as good quality studies [14].
Quantitative Analysis
The studies were analyzed using the effect size Hedges’ g(standardized mean difference) [15,16], which is calcu-lated by the difference between the experiment andcontrol treatment at the end of the treatment period,divided by the pooled standard deviation (SD) (see Appen-dix). A heterogeneity test statistics I2 [17,18] was deter-mined to assess whether a fixed or random effects modelwas appropriate to calculate the summary effect sizeusing Hedges’ g. A fixed effect model was used when the
1727
NMDA Receptor Antagonists for Neuropathic Pain
pooled effects of studies could be considered homog-enous (I2 statistics below 25%) [18].
The difference in pain relief between experimental andplacebo conditions as measured on a numerical ratingscale was taken as the primary outcome measure. In casedata for quantitative analysis were not present in thearticle, written permission for additional data wasrequested from the authors of these articles. If no addi-tional information was obtained from the author, the effectsize was estimated from significance levels, assumingconservative values (e.g., P = 0.5 if not significant;P = 0.05 if significant). For each study, a weighting factor(Wi) was estimated, assigning larger weights to effect sizesfrom studies with larger samples and, thus, smaller vari-ances. For studies evaluating different interventions ordifferent doses within the same study, the interventionswere regarded as independent treatments and thereforeeffect sizes were calculated separately for each interven-tion compared with placebo.
The summary effect size was then established by averag-ing the individual effect sizes. For each individual effectsize and for the summary effect size, a 95% confidenceinterval was obtained. The summary effect size was onlycalculated for comparable studies, evaluating the effectsof similar interventions in patients with the same painconditions. Furthermore, the summary effect size will onlybe reported for studies with a quality assessment score ofmore than 50% [13]. Cohen [19] has provided referencepoints to serve as guide in the interpretation of effect sizes:0.20 for “small” effects, 0.50 for “moderate” effects and0.80 for “large” effects. For all outcome variables, thesignificance level was set at 0.05.
Results
Quality of Studies
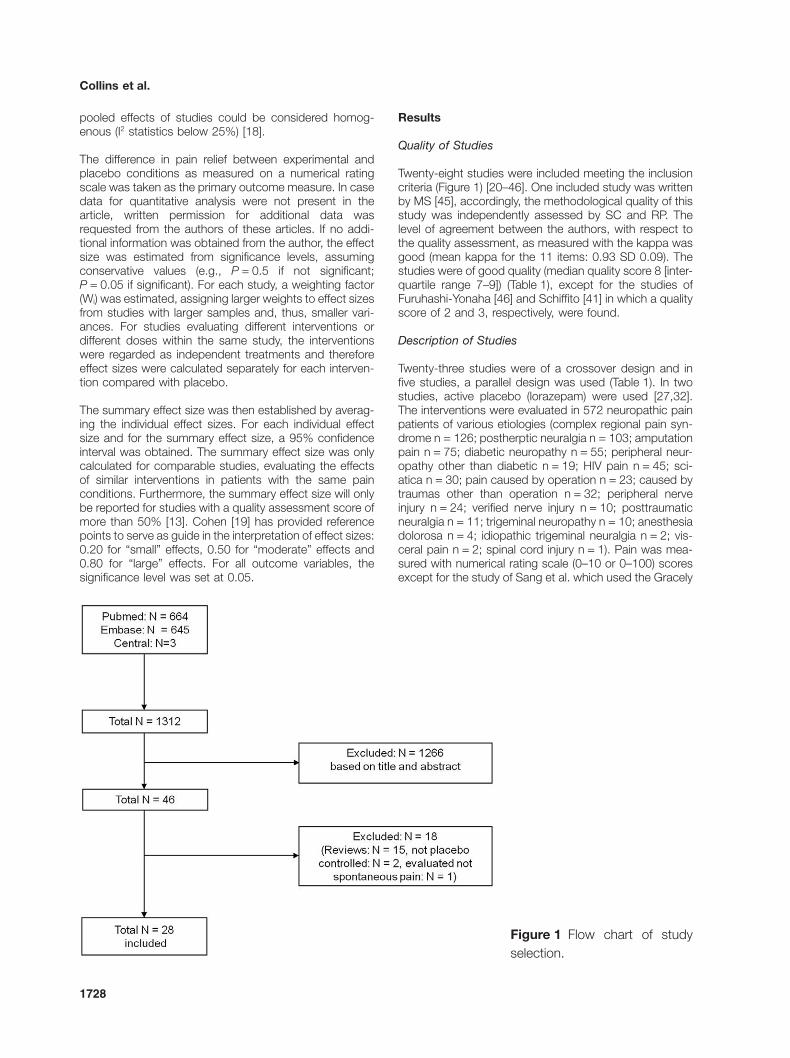
Twenty-eight studies were included meeting the inclusioncriteria (Figure 1) [20–46]. One included study was writtenby MS [45], accordingly, the methodological quality of thisstudy was independently assessed by SC and RP. Thelevel of agreement between the authors, with respect tothe quality assessment, as measured with the kappa wasgood (mean kappa for the 11 items: 0.93 SD 0.09). Thestudies were of good quality (median quality score 8 [inter-quartile range 7–9]) (Table 1), except for the studies ofFuruhashi-Yonaha [46] and Schiffito [41] in which a qualityscore of 2 and 3, respectively, were found.
Description of Studies
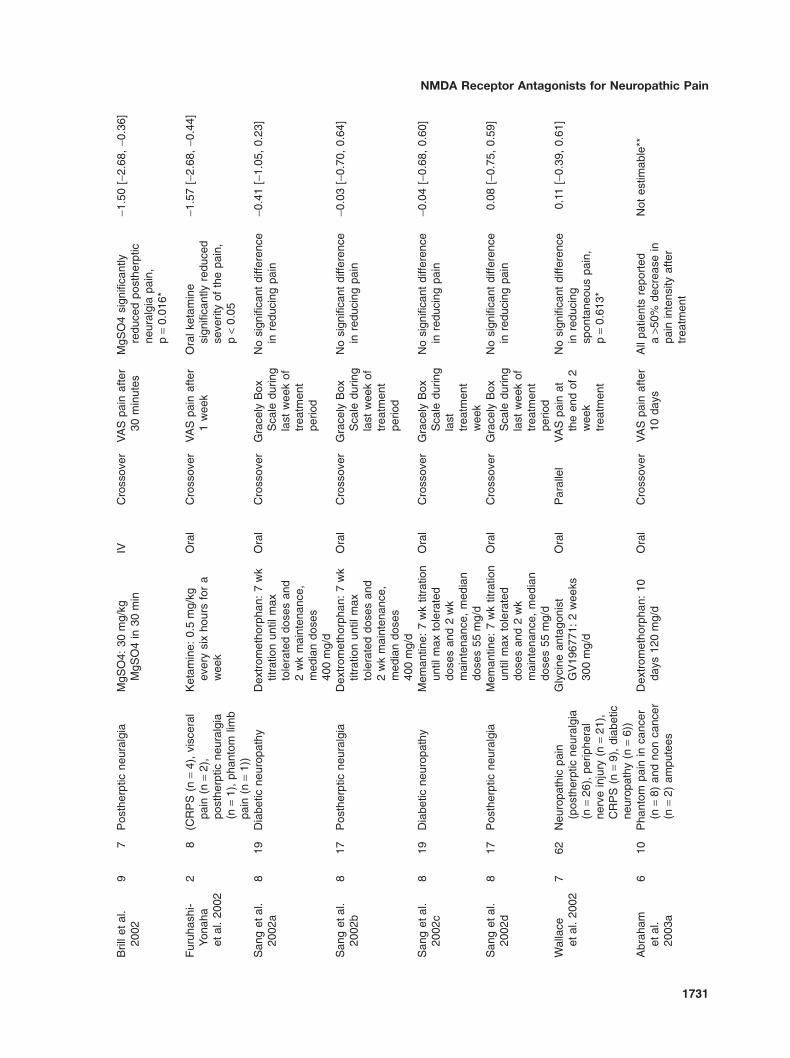
Twenty-three studies were of a crossover design and infive studies, a parallel design was used (Table 1). In twostudies, active placebo (lorazepam) were used [27,32].The interventions were evaluated in 572 neuropathic painpatients of various etiologies (complex regional pain syn-drome n = 126; postherptic neuralgia n = 103; amputationpain n = 75; diabetic neuropathy n = 55; peripheral neur-opathy other than diabetic n = 19; HIV pain n = 45; sci-atica n = 30; pain caused by operation n = 23; caused bytraumas other than operation n = 32; peripheral nerveinjury n = 24; verified nerve injury n = 10; posttraumaticneuralgia n = 11; trigeminal neuropathy n = 10; anesthesiadolorosa n = 4; idiopathic trigeminal neuralgia n = 2; vis-ceral pain n = 2; spinal cord injury n = 1). Pain was mea-sured with numerical rating scale (0–10 or 0–100) scoresexcept for the study of Sang et al. which used the Gracely
Figure 1 Flow chart of studyselection.
1728
Collins et al.

Tab
le1
Incl
uded
stud
ies
Aut
hors
QS
NP
atie
nts
Inte
rven
tions
App
lD
esig
nP
rimar
you
tcom
eR
esul
tsIn
divi
dual
effe
ctsi
ze(in
vers
eva
rianc
e)
Max
etal
.19
957
7P
osttr
aum
atic
pain
and
allo
dyni
aK
etam
ine:
2h,
0.75
mg/
kg/h
IVC
ross
over
VA
Spa
inaf
ter
2ho
urs
Ket
amin
esi
gnifi
cant
lyre
duce
dba
ckgr
ound
pain
,p
=0.
01
-0.8
8[-
1.98
,0.
22]
Fel
sby
etal
.19
95a
810
Chr
onic
neur
opat
hic
pain
(afte
ram
puta
tion
(n=
3),
afte
rop
erat
ion
(n=
5),
afte
rra
diat
ion
(n=
2))
Ket
amin
e:10
min
,0.
2m
g/kg
and
50m
in,
0.3
mg/
kg/h
IVC
ross
over
VA
Spa
in15
min
afte
rin
fusi
on
Ket
amin
esi
gnifi
cant
lyre
duce
dpa
inin
tens
ity,
p=
0.00
6
-0.4
2[-
1.41
,0.
45]
Fel
sby
etal
.19
95b
810
Chr
onic
neur
opat
hic
pain
(afte
ram
puta
tion
(n=
3),
afte
rop
erat
ion
(n=
5),
afte
rra
diat
ion
(n=
2))
MgC
l2:
10m
in,
0.16
mm
ol/k
gan
d50
min
0.16
mm
ol/k
g/h
IVC
ross
over
VA
Spa
in15
min
afte
rin
fusi
on
MgC
l2si
gnifi
cant
lyre
duce
dpa
inin
tens
ity,
p=
0.08
4
-0.2
9[-
1.22
,0.
64]
Nic
kola
jsen
etal
.19
96
811
Pos
tam
puta
tion
stum
pan
dph
anto
mlim
bpa
inK
etam
ine:
bolu
s0.
1m
g/kg
/5m
inan
d7
mgr/
kg/m
info
r40
min
IVC
ross
over
VA
Spa
inaf
ter
infu
sion
Ket
amin
esi
gnifi
cant
lyre
duce
dst
ump
and
phan
tom
pain
,p
<0.
05*
-0.8
9[-
1.78
,0.
01]
Eis
enbe
rget
al.
1998
1020
Pos
ther
ptic
neur
algi
aM
eman
tine:
wk
1:10
mg/
d,w
k2/
5:20
mg/
d
Ora
lP
aral
lel
VA
S(0
–10)
pain
afte
r5
wee
ks
No
stat
istic
ally
sign
ifica
ntdi
ffere
nce
inre
duct
ion
ofpa
in
0.23
[-0.
65,
1.11
]
Pud
etal
.19
987
13S
urgi
caln
euro
path
icpa
inin
canc
erpa
tient
sA
man
tadi
ne:
200
mg
in3
hour
sIV
Cro
ssov
erV
AS
pain
afte
r3
hin
fusi
ons
Am
anta
dine
sign
ifica
ntly
redu
ced
pain
,p
=0.
0001
-1.4
6[-
2.32
,-0
.60]
Med
rik-
Gol
dber
get
al.
1999
930
Sci
atic
aA
man
tadi
ne:
2.5
mg/
kgin
2ho
urs
IVC
ross
over
VA
Spa
inaf
ter
180
min
No
stat
istic
ally
sign
ifica
ntdi
ffere
nce
inre
duct
ion
ofsp
onta
neou
spa
in
0.04
[-0.
47,
0.55
]
Gal
eret
al.
2000
a9
22P
erip
hera
lneu
ropa
thic
pain
(pos
ther
ptic
neur
algi
a(n
=13
),di
abet
icpo
lyne
urop
athy
(n=
1),
perip
hera
lne
urop
athy
othe
rth
andi
abet
ic(n
=8)
)
Rilu
zole
:10
0m
g/d
for
2w
eeks
Ora
lC
ross
over
VA
Spa
inaf
ter
2w
eeks
No
stat
istic
ally
sign
ifica
ntdi
ffere
nce
inal
levi
atin
gpe
riphe
raln
euro
path
icpa
in,
p>
0.10
0.26
[-0.
34,
0.86
]
1729
NMDA Receptor Antagonists for Neuropathic Pain

Tab
le1
Con
tinue
d
Aut
hors
QS
NP
atie
nts
Inte
rven
tions
App
lD
esig
nP
rimar
you
tcom
eR
esul
tsIn
divi
dual
effe
ctsi
ze(in
vers
eva
rianc
e)
Gal
eret
al.
2000
b9
21P
erip
hera
lneu
ropa
thic
pain
(pos
ther
ptic
neur
algi
a(n
=9)
,di
abet
icpo
lyne
urop
athy
(n=
1),
perip
hera
lne
urop
athy
othe
rth
andi
abet
ic(n
=11
))
Rilu
zole
:20
0m
g/d
for
2w
eeks
Ora
lC
ross
over
VA
Spa
inaf
ter
2w
eeks
No
stat
istic
ally
sign
ifica
ntdi
ffere
nce
inin
alle
viat
ing
perip
hera
lne
urop
athi
cpa
in,
p>
0.10
-0.0
7[-
0.68
,0.
54]
Gilr
onet
al.
2000
816
Fac
ialn
eura
lgia
s(p
ossi
ble
trig
emin
alne
urop
athy
(n=
10),
anae
sthe
sia
dolo
rosa
(n=
4),
idio
path
ictr
igem
inal
neur
algi
a(n
=2)
)
Dex
trom
etho
rpha
n:12
0m
g/d,
titra
ted
tom
ax92
0m
g/d
for
6w
eeks
Ora
lC
ross
over
VA
Sov
eral
lda
ilypa
inaf
ter
6w
eeks
No
stat
istic
ally
sign
ifica
ntdi
ffere
nce
inre
duci
ngpa
in,
p=
0.81
0.05
[-0.
64,
0.74
]
Nic
kola
jsen
etal
.20
007
15N
euro
path
icpa
inaf
ter
ampu
tatio
n(n
=12
)or
oper
atio
n(n
=3)
Mem
antin
e:w
k1:
5m
g/d,
wk
2:10
mg/
d,w
k3:
15m
g/d,
wk4
/5:
20m
g/d
Ora
lC
ross
over
VA
S(0
–10)
pain
durin
gw
k4/5
No
sign
ifica
ntdi
ffere
nce
inre
duci
ngsp
onta
neou
spa
in
-0.4
1[-
1.14
,0.
32]
Leun
get
al.
2001
712
Neu
ropa
thic
pain
(pos
ther
ptic
neur
algi
a(n
=4)
,C
RP
S(n
=7)
,sp
inal
cord
inju
ry(n
=1)
)
Ket
amin
e:ta
rget
plas
ma
leve
lsof
50,
100
and
150
ng/m
l
IVC
ross
over
VA
Spa
inat
3pl
asm
ale
vels
No
sign
ifica
ntre
duct
ion
insp
onta
neou
spa
in*
0.28
[-0.
52,
1.08
]
Abr
aham
etal
.20
02a
83
Pha
ntom
pain
inca
ncer
ampu
tees
Dex
trom
etho
rpha
n:1
wk
120
mg/
dO
ral
Cro
ssov
erV
AS
pain
afte
r1
wee
kD
extr
omet
horp
han
sign
ifica
ntly
redu
ced
post
ampu
tatio
nph
anto
mlim
bpa
in,
p<
0.05
*
-2.2
7[-
4.42
,-0
.12]
Abr
aham
etal
.20
02b
83
Pha
ntom
pain
inca
ncer
ampu
tees
Dex
trom
etho
rpha
n:1
wk
180
mg/
dO
ral
Cro
ssov
erV
AS
pain
afte
r1
wee
kD
extr
omet
horp
han
sign
ifica
ntly
redu
ced
post
ampu
tatio
nph
anto
mlim
bpa
in,
p<
0.05
*
-2.2
7[-
4.42
,-0
.12]
1730
Collins et al.
Bril
leta
l.20
029
7P
osth
erpt
icne
ural
gia
MgS
O4:
30m
g/kg
MgS
O4
in30
min
IVC
ross
over
VA
Spa
inaf
ter
30m
inut
esM
gSO
4si
gnifi
cant
lyre
duce
dpo
sthe
rptic
neur
algi
apa
in,
p=
0.01
6*
-1.5
0[-
2.68
,-0
.36]
Fur
uhas
hi-
Yona
haet
al.
2002
28
(CR
PS
(n=
4),
visc
eral
pain
(n=
2),
post
herp
ticne
ural
gia
(n=
1),
phan
tom
limb
pain
(n=
1))
Ket
amin
e:0.
5m
g/kg
ever
ysi
xho
urs
for
aw
eek
Ora
lC
ross
over
VA
Spa
inaf
ter
1w
eek
Ora
lket
amin
esi
gnifi
cant
lyre
duce
dse
verit
yof
the
pain
,p
<0.
05
-1.5
7[-
2.68
,-0
.44]
San
get
al.
2002
a8
19D
iabe
ticne
urop
athy
Dex
trom
etho
rpha
n:7
wk
titra
tion
until
max
tole
rate
ddo
ses
and
2w
km
aint
enan
ce,
med
ian
dose
s40
0m
g/d
Ora
lC
ross
over
Gra
cely
Box
Sca
ledu
ring
last
wee
kof
trea
tmen
tpe
riod
No
sign
ifica
ntdi
ffere
nce
inre
duci
ngpa
in-0
.41
[-1.
05,
0.23
]
San
get
al.
2002
b8
17P
osth
erpt
icne
ural
gia
Dex
trom
etho
rpha
n:7
wk
titra
tion
until
max
tole
rate
ddo
ses
and
2w
km
aint
enan
ce,
med
ian
dose
s40
0m
g/d
Ora
lC
ross
over
Gra
cely
Box
Sca
ledu
ring
last
wee
kof
trea
tmen
tpe
riod
No
sign
ifica
ntdi
ffere
nce
inre
duci
ngpa
in-0
.03
[-0.
70,
0.64
]
San
get
al.
2002
c8
19D
iabe
ticne
urop
athy
Mem
antin
e:7
wk
titra
tion
until
max
tole
rate
ddo
ses
and
2w
km
aint
enan
ce,
med
ian
dose
s55
mg/
d
Ora
lC
ross
over
Gra
cely
Box
Sca
ledu
ring
last
trea
tmen
tw
eek
No
sign
ifica
ntdi
ffere
nce
inre
duci
ngpa
in-0
.04
[-0.
68,
0.60
]
San
get
al.
2002
d8
17P
osth
erpt
icne
ural
gia
Mem
antin
e:7
wk
titra
tion
until
max
tole
rate
ddo
ses
and
2w
km
aint
enan
ce,
med
ian
dose
s55
mg/
d
Ora
lC
ross
over
Gra
cely
Box
Sca
ledu
ring
last
wee
kof
trea
tmen
tpe
riod
No
sign
ifica
ntdi
ffere
nce
inre
duci
ngpa
in0.
08[-
0.75
,0.
59]
Wal
lace
etal
.20
027
62N
euro
path
icpa
in(p
osth
erpt
icne
ural
gia
(n=
26),
perip
hera
lne
rve
inju
ry(n
=21
),C
RP
S(n
=9)
,di
abet
icne
urop
athy
(n=
6))
Gly
cine
anta
goni
stG
V19
6771
:2
wee
ks30
0m
g/d
Ora
lP
aral
lel
VA
Spa
inat
the
end
of2
wee
ktr
eatm
ent
No
sign
ifica
ntdi
ffere
nce
inre
duci
ngsp
onta
neou
spa
in,
p=
0.61
3*
0.11
[-0.
39,
0.61
]
Abr
aham
etal
.20
03a
610
Pha
ntom
pain
inca
ncer
(n=
8)an
dno
nca
ncer
(n=
2)am
pute
es
Dex
trom
etho
rpha
n:10
days
120
mg/
dO
ral
Cro
ssov
erV
AS
pain
afte
r10
days
All
patie
nts
repo
rted
a>5
0%de
crea
sein
pain
inte
nsity
afte
rtr
eatm
ent
Not
estim
able
**
1731
NMDA Receptor Antagonists for Neuropathic Pain

Tab
le1
Con
tinue
d
Aut
hors
QS
NP
atie
nts
Inte
rven
tions
App
lD
esig
nP
rimar
you
tcom
eR
esul
tsIn
divi
dual
effe
ctsi
ze(in
vers
eva
rianc
e)
Abr
aham
etal
.20
03b
610
Pha
ntom
pain
inca
ncer
(n=
8)an
dno
nca
ncer
(n=
2)am
pute
es
Dex
trom
etho
rpha
n:10
days
180
mg/
dO
ral
Cro
ssov
erV
AS
pain
afte
r10
days
All
patie
nts
repo
rted
a>5
0%de
crea
sein
pain
inte
nsity
afte
rtr
eatm
ent
Not
estim
able
**
Am
inet
al.
2003
817
Dia
betic
perip
hera
lne
urop
athy
Am
anta
dine
:1
¥20
0m
gin
500
ml0
.9%
NaC
lIV
Cro
ssov
erV
AS
pain
afte
r1
wee
kA
man
tadi
nesi
gnifi
cant
lyre
duce
dpa
inin
tens
ityp
=0.
003
-0.9
8[-
1.71
,-0
.25]
Joru
met
al.
2003
712
Pos
ttr
aum
atic
neur
algi
a(n
=11
)an
dpo
sthe
rptic
neur
algi
a(n
=1)
Ket
amin
e:bo
lus
60mg
r/kg
and
6mg
r/kg
for
20m
in
IVC
ross
over
VA
Spa
inaf
ter
infu
sion
keta
min
esi
gnifi
cant
lyre
duce
dsp
onta
neou
spa
inp
=0.
015*
-1.0
8[-
1.94
,-0
.22]
Mai
eret
al.
2003
1116
Chr
onic
phan
tom
limb
pain
afte
ram
puta
tion
ofar
mor
leg
Mem
antin
e:w
eek
1tit
ratio
n30
mg/
d:5
mg/
d+
adde
d5
mg
daily
,w
2+3:
30m
g/d
Ora
lC
ross
over
VA
Spa
inaf
ter
3w
eeks
No
sign
ifica
ntdi
ffere
nce
inre
duci
ngph
anto
mlim
bpa
in*
0.24
[-0.
46,
0.94
]
Car
lsso
net
al.
2004
713
Neu
ropa
thic
pain
oftr
aum
atic
orig
inD
extr
omet
horp
han:
1¥27
0m
gO
ral
Cro
ssov
erV
AS
pain
afte
r0–
4ho
urs
Dex
trom
etho
rpha
nsi
gnifi
cant
lyre
duce
dpa
in,
p<
0.05
-0.8
1[-
1.61
,-0
.01]
Wie
chet
al.
2004
88
Chr
onic
phan
tom
limb
pain
Mem
antin
e:w
k1:
10m
g/d,
wk
2:20
mg/
d,w
k3/
4:30
mg/
d
Ora
lC
ross
over
VA
Spa
inaf
ter
4w
eeks
trea
tmen
t
No
sign
ifica
ntdi
ffere
nce
inre
duci
ngin
tens
ityof
chro
nic
limb
pain
,p
=0.
16*
0.74
[-0.
27,
1.05
]
Got
trup
etal
.20
068
19V
erifi
edne
rve
inju
rypa
inK
etam
ine:
bolu
s0.
1m
g/kg
in10
min
and
0.00
7m
g/kg
min
in20
min
IVC
ross
over
VA
Spa
indu
ring
infu
sion
Ket
amin
esi
gnifi
cant
lyre
duce
dsp
onta
neou
spa
in,
p<
0.01
-0.3
5[-
0.99
,0.
29]
Sch
ifitto
etal
.20
063
45H
IVas
soci
ated
sens
ory
neur
opat
hyM
eman
tine:
wk
1:10
mg/
d+
adde
dw
eekl
yfo
r4
wk
10m
g/d,
wk
4/16
:40
mg/
d
Ora
lP
aral
lel
VA
Spa
inaf
ter
16w
eeks
No
sign
ifica
ntdi
ffere
nce
inre
duci
ngH
IVas
soci
ated
sens
ory
neur
opat
hy,
p=
0.87
*
0.05
[-0.
54,
0.64
]
For
stet
al.
2007
a10
12N
euro
path
icpa
in(p
osth
erpt
icpa
in(n
=3)
,po
sttr
aum
atic
inju
ry(n
=6)
,C
RP
S(n
=3)
)
Nov
elgl
utam
ate
anta
goni
stC
NS
5161
HC
l:si
ngle
dose
of12
5mg
r
Ora
lC
ross
over
VA
Spa
inaf
ter
12ho
urs
No
sign
ifica
ntdi
ffere
nce
inre
duci
ngpa
in0.
16[-
0.64
,0.
96]
1732
Collins et al.

For
stet
al.
2007
b10
12N
euro
path
icpa
in(p
osth
erpt
icpa
in(n
=2)
,di
abet
icne
urop
athy
(n=
3),
post
trau
mat
icin
jury
(n=
6),
CR
PS
(n=
1))
Nov
elgl
utam
ate
anta
goni
stC
NS
5161
HC
l:si
ngle
dose
of25
0mg
r
Ora
lC
ross
over
VA
Spa
inaf
ter
12ho
urs
No
sign
ifica
ntdi
ffere
nce
inre
duci
ngpa
in0.
30[-
0.51
,1.
11]
For
stet
al.
2007
c10
14N
euro
path
icpa
in(d
iabe
ticne
urop
athy
(n=
8),
post
trau
mat
icin
jury
(n=
4),
CR
PS
(n=
2))
Nov
elgl
utam
ate
anta
goni
stC
NS
5161
HC
l:si
ngle
dose
of50
0mg
r
Ora
lC
ross
over
VA
Spa
inaf
ter
12ho
urs
No
sign
ifica
ntdi
ffere
nce
inre
duci
ngpa
in,
p=
0.11
-0.4
0[-
1.15
,0.
35]
Eic
henb
erge
ret
al.
2008
810
Chr
onic
phan
tom
limb
pain
afte
rtr
aum
a(n
=6)
and
surg
ery
(n=
4)
Ket
amin
e:0.
4m
g/kg
in1
hour
IVC
ross
over
VA
Spa
in60
min
afte
rin
fusi
on
Ket
amin
esi
gnifi
cant
lyre
duce
dph
anto
mlim
bpa
in,
p<
0.00
1*
-1.7
5[-
2.06
,-0
.72]
Sch
war
tzm
anet
al.
2009
919
CR
PS
Ket
amin
e:m
ax0.
35m
g/kg
/hin
4ho
urs
for
10da
ys
IVP
aral
lel
VA
Sov
eral
lpa
inaf
ter
2w
eeks
Ket
amin
esi
gnifi
cant
lyre
duce
dov
eral
lpai
n,p
<0.
05
-0.5
5[-
1.00
,0.
09]
Sig
term
ans
etal
.20
098
60C
RP
SK
etam
ine
(S+)
:22
.2�
2.0
mg/
h(m
ean
�S
D)
cont
inuo
usly
durin
g4.
2da
ys
IVP
aral
lel
VA
Spa
inaf
ter
1w
eek
Ket
amin
esi
gnifi
cant
lyre
duce
dsp
onta
neou
spa
in,
p<
0.00
1
-5.5
9[-
6.76
,-4
.47]
Fin
chet
al.
2009
720
CR
PS
Ket
amin
e10
%cr
eam
Topi
cal
Cro
ssov
erV
AS
pain
afte
r30
min
No
sign
ifica
ntdi
ffere
nce
inre
duci
ngpa
in0.
00[-
0.20
,0.
20]
QS
:qu
ality
scor
e.A
ppl:
appl
icat
ion.
IV:
intr
aven
ous.
CR
PS
:co
mpl
exre
gion
alpa
insy
ndro
me.
*:ef
fect
size
estim
ated
from
sign
ifica
nce
leve
ls,
ifp
valu
esw
ere
not
repo
rted
p=
0.5
ifno
tsi
gnifi
cant
and
p=
0.05
ifsi
gnifi
cant
wer
eas
sum
ed.
**:
effe
ctsi
zew
asno
tes
timab
lebe
caus
eno
info
rmat
ion
was
repo
rted
abou
tth
edi
rect
ion
(sig
nific
ant
orno
n-si
gnifi
cant
)of
sign
ifica
nce
leve
ls.
1733
NMDA Receptor Antagonists for Neuropathic Pain

Pain Box (0–20] scale for rating pain intensity, which wastransformed into a scale from 1 to 100. Positive resultsafter treatment with NMDA receptor antagonists werereported in 13 studies [22,24,30,31,34–36,38,40,43–46].
The effects of the NMDA receptor antagonist ketaminewas investigated in 11 studies [20–22,29,36,40,43–47], inwhich the effects of the S(+) enantiomer of ketamine wasevaluated by the study of Sigtermans et al. [45], while theother 10 studies investigated racemic (R/S) ketamine. Sixstudies evaluated memantine [23,28,32,37,39,41], fivestudied the effects of dextromethorphan [27,30,32,34,38],and three studies investigated amantadine [24,25,35].Furthermore, the effects of MgSO4 [31], MgCl2 [20], rilu-zole [26], GV196771 (a glycine antagonist) [33] and CNS5161 HCl (a novel NMDA receptor antagonist) [42] wereinvestigated. Adverse events after treatment with the dif-ferent interventions are presented in Table 2.
Quantitative Analysis
In 13 studies [22–27,32,35,40,42,44–46], data (mean andSD) was available for directly calculating hedges’ g statis-tical analysis. Authors of the remaining studies were con-tacted for additional data, of whom four [20,28,38,47]provided additional data. For the remaining studies[21,29–31,33,36,37,39,41], effect sizes were calculatedusing P-values and t statistics (see appendix). For thestudy by Abraham et al. [34], no information was providedabout the placebo group, therefore the individual effectsize could not be estimated for this study. Three studiesused different doses of NMDA receptor antagonists[26,30,42] and one evaluated more than one NMDAreceptor antagonist [32]. Effect sizes for the individualstudies and (different doses of) interventions are pre-sented in Table 1.
In order to calculate the summarize effect size in compa-rable studies with respect to used interventions, route ofadministration and evaluated pain patients, studiesassessing an intervention in one type of neuropathic painpatient and providing adequate data for analysis (a total of12 studies) were categorized according to pain disorder,resulting in four pain patients groups: CRPS, postherpticneuralgia, diabetic neuropathy and postamputation pain(Figure 2). Within these pain patient groups, the summaryeffect size was calculated for minimum two studies evalu-ating the same intervention.
Summary effect sizes were calculated for subgroups ofstudies evaluating intravenous ketamine in CRPS patients,oral memantine in postherptic neuralgia patients and,respectively, intravenous ketamine and oral memantine inpostamputation pain. The results of the two trials evaluat-ing dextromethorphan in postamputation pain were notsummarized, because the two trials (using different dosesof dextromethorphan) were performed and reported withinthe same study, and pooling of results would therefore bequestionable. Treatment with ketamine IV significantlyreduced postamputation pain (pooled summary effectsize: -1.18 [confidence interval (CI) 95% -1.98, -0.37],P = 0.004) (Figure 3). No significant effect on pain reduc-tion could be established for ketamine IV in CRPS (pooledsummary effect size -0.65 [CI 95% -1.47, 0.16], P = 0.11)oral memantine in postherptic neuralgia treatment (pooledsummary effect size 0.03 [CI 95% -0.51, 0.56], P = 0.92)and for oral memantine in postamputation pain (pooledsummary effect size 0.38 [CI 95% -0.21, 0.98], P = 0.21)(see Figures 4–6).
Discussion
Since the late 1980s, NMDA receptor antagonists havebeen known to decrease neuronal hyperexitability and
Table 2 Adverse events of interventions
Intervention Adverse events
Ketamine Sedation, dreams, hallucinations, dissociative reaction, nausea, headache, dizziness, fatigue,changes in mood, altered sight, feeling of unreality, dry mouth, light-headedness, paresthesia,changed taste, dysarthria, euphoria, tinnitus, drunkenness, itching, muteness, andhyperventilation.
Memantine Nausea, fatigue, dizziness, agitation, headache, sedation, dry mouth, gastrointestinal distress,anorexia, constipation, vertigo, restlessness, excitation, insomnia, blurred vision and tinnitus.
Amantadine Nausea.Dextromethorphan Cognitive impairment, dizziness, ataxia, light-headedness, drowsiness, vision disturbances,
euphoria, hot flushes, nausea, speaking difficulties, unpleasantness, numbness, concentrationproblems, shivers, vomiting, itching, dry mouth, tinnitus, rash, sedation, gastrointestinal distressand anorexia.
GV 196771 Dizziness.CNS 5161 HCl Headache, blurred vision, flatulence, dyspepsia, abdominal comfort and nausea.MgSO4 Mild feeling of warmth at the site of infusion.MgCl2 Heat sensations, injection pain and sedation.Riluzole Not mentioned.
1734
Collins et al.

reduce pain, and the efficacy of several NMDA receptorantagonists has been investigated in preclinical and clini-cal pain studies [48]. Despite the large number of studies,there is still no consensus on the efficacy of NMDA recep-tor antagonist on neuropathic pain therefore the presentsystematic review was performed.
We found several randomized placebo controlled studiesinvestigating the effects of a variety of interventions on adiversity of neuropathic pain patients. In order to pool orsummarize results to achieve an overall estimation of theeffectiveness of a therapeutic intervention, studies haveto be similar in the used intervention, route of adminis-tration and the investigated patients. Only half of the
found studies evaluated the intervention in one typeof neuropathic pain patient [21,23–25,28,30–32,35–37,39,41,43–45,47], of which only a few evaluated thesame NMDA receptor antagonists using same routes ofadministration in patients with similar neuropathic painetiologies. Consequently, we could only summarize theresults of two studies investigating ketamine IV in CRPS[44,45], two studies evaluating oral memantine in pos-therptic neuralgia [23,32] and, respectively, two studiesinvestigating ketamine IV [21,43] and two studies evalu-ating oral memantine in postamputation pain [37,39].Ketamine IV was shown to have a large effect [19] inreducing postamputation pain. Based on the smallnumber of pooled results and the lack of information
Figure 2 Included studiesdivided in four pain patientsgroups. *Summarize effect sizewas calculated for minimal twostudies evaluating the sameintervention and route of admin-istration in the same pain patientgroup. †Results of the trialswere not summarized, becausetrials were performed andreported within the same study.IV = intravenous; O = oral; T =topical.
1735
NMDA Receptor Antagonists for Neuropathic Pain

about the effects of other NMDA receptor antagonistsbesides ketamine and memantine on other pain condi-tions, we consider it speculative to draw definite conclu-sions about the efficacy of NMDA receptor antagonists
on neuropathic pain. Further, RCTs including well-definedneuropathic pain disease groups are needed to elucidatethe effects of NMDA receptor antagonists on neuro-pathic pain.
Figure 3 Intravenous ketamineversus placebo in postamputa-tion pain. I2 = 0%. Pooled sum-marized effect size, fixed effectmodel: -1.18 (confidence inter-val 95% -1.98, -0.37), P =0.004.
Figure 4 Intravenous and topi-cal ketamine versus placebo inCRPS. I2 = 55%. Pooled sum-marized effect size, randomeffect model: -0.65 (confidenceinterval 95% -1.47, 0.16),P = 0.11.
1736
Collins et al.

Besides increasing the ability to compare and/or poolindividual studies, examining just one type of pain patientalso increases the homogeneity of the investigated sampleand therefore reduces bias within a study. Neuropathic
pain consists of a very heterogeneous group of patientsregarding the type and degree of their complaints [49].This heterogeneity could also be expressed in the com-position of the NMDA receptor. The NMDA receptor is
Figure 5 Oral memantineversus placebo in postherpticneuralgia. I2 = 0%. Pooled sum-marized effect size, fixed effectmodel: 0.03 (confidence interval95% -0.51, 0.56), P = 0.92.
Figure 6 Oral memantineversus placebo in postamputa-tion pain. I2 = 0%. Pooled sum-marized effect size, fixed effectmodel: 0.38 (confidence interval95% -0.21, 0.98), P = 0.21.
1737
NMDA Receptor Antagonists for Neuropathic Pain

constructed of different subunits (NR1, NR2A-D andNR3A-C), which can be combined in different ways (NR1in combination with 2A–D or 3A–C) [48,50]. The differentsubtype combinations are known to have distinct bio-physical and pharmacological characteristics [51], whichmay influence binding of NMDA receptor antagonists. Inaddition, NMDA receptor antagonists are known to differin their NMDA subtype selectivity and affinity for specificcombinations of NMDA receptor subtypes. At present,little is known about the NMDA subtype pattern in dif-ferent neuropathic pain disorders. The expression of dif-ferent subunit combinations may result in differentselectivity and binding sensitivities for NMDA receptorantagonists, which may lead to differences in pain relief.Research in which the effects of NMDA receptor antago-nists are evaluated in homogenous groups of neuro-pathic pain patients is therefore required to assesspossible disease related differences in treatment effectsof NMDA receptor antagonists.
In this meta-analysis, we evaluated pain in neuropathicpain patients. Neuropathic pain has recently been rede-fined by the International Association for the Study ofPain as pain arising as a direct consequence of a lesionor disease affecting the somatosensory system [1]. Con-ditions without a clearly demonstrated lesion or diseaseaffecting the somatosensory nervous system, such asfibromyalgia, are not considered neuropathic pain. In thepast, there has been some discussion about CRPSbeing a neuropathic pain syndrome. We have includedstudies on CRPS patients, as recent findings of periph-eral pathological changes [52] and damage in the inner-vations of the skin in CRPS [53,54] support the conceptof CRPS being a peripheral neuropathic condition. Infibromyalgia patients, no physical or biological findingshave yet been made that relate directly to a lesion ordisease of the somatosensory system. However, abnor-mally enhanced temporal summation of second pain,expansion of receptive fields, hyperalgesia after electricalstimulation, and late evoked potentials have beendescribed in these patients [55–57]. These central hyper-sensitivities are indicative of the existence of central sen-sitization, suggestive of the presence of a neuropathiccomponent in fibromyalgia. NMDA receptor antagonistswere shown to reduce pain in fibromyalgia [58]. Furtherresearch is warranted to determine the effects of NMDAreceptor antagonists in fibromyalgia and other disorderswith features of neuropathic pain.
Ketamine is probably the most investigated NMDA recep-tor antagonists for the treatment of neuropathic pain [48],which explains the large number of trials using ketamine inour review. Ketamine is known to equally bind the NMDAsubtypes 2A to 2D and may therefore have a more favor-able effect in such a heterogenic disease as neuropathicpain, compared with NMDA receptor antagonists withmore discriminative NMDA subtype selectivity. In addition,ketamine is a high affinity NMDA receptor antagonist,resulting in long-term blocking of the receptor and stronginhibiting of the neuronal hyperexcitability occurring in neu-ropathic pain. A disadvantage of this undiscriminating and
strong binding property, however, is the higher proportionsof side effects due to binding of the antagonists to neuronalstructures not involved in pain.
The use of the S(+) eantiomer of ketamine in clinical trials[45], may be favorable regarding side effects. S(+) ket-amine is twice as potent in analgesic effect comparedwith racemic ketamine [59]; therefore, lower doses ofS(+) ketamine may reduce side effects, while providingpain reduction resembling racemic ketamine. In thepresent review, a statistically significant effect in reducingneuropathic pain for ketamine was only found for post-amputation pain. Evaluation of the individual effect sizes,however, revealed five large effect trials [19], in whichketamine was used in four trials (in patients with post-amputation pain [21,43], posttraumatic, postherptic neu-ralgia [36], and CRPS [45], respectively). Therefore, weargue that ketamine (and especially S(+) ketamine) maybe a promising intervention for pain relief in neuropathicpain. In this respect, a reservation has to be made withregard to the inclusion of an article by a member of ourgroup [45], therewith introducing possible interpretationbias. However, quality assessments for this article werenot performed by those directly involved in the study inquestion. Furthermore, omitting this article from theanalysis would not have lead to significantly differentconclusions.
Our methodology only considers spontaneous pain asoutcome measurement after treatment with NMDAreceptor antagonists. Many studies found in this reviewalso investigated the effects of NMDA receptor antago-nists on evoked pain (allodynia, hyperalgesia, winduppain) [22–27,30,35,40,42–44,47]. These studies usedvarious stimulus modalities of different strengths toevoke pain. In order to diminish the heterogeneity andmake comparison of different interventions possible, weonly used spontaneous pain as outcome measurement.Consequently, we have no information about the effectsof NMDA receptor antagonists on other aspects of sen-sitization. Possibly, some antagonists may affect spon-taneous pain, allodynia or hyperalgesia in a differentmanner. Further (meta-analytic) research may elucidatethe effects on NMDA receptor antagonists on otheraspect of sensitization.
Another methodological consideration in this study is thefact that only comparisons between NMDA receptorantagonists and placebo were taken into account. Com-parisons with active (real) interventions could possibly leadto lower effect sizes than those found in the present meta-analysis. On the other hand, one should bear in mind thateffect sizes in general will be negatively influenced by theheterogeneity of the included studies, thereby limiting theirmagnitude.
Conclusions
Based on the results found in this systematic review, noconclusions can yet be made about the efficacy of NMDA
1738
Collins et al.

receptor antagonists on neuropathic pain. However, evi-dence in favor of the effectiveness of NMDA receptorantagonists for the treatment of neuropathic pain, of whichketamine seems to be the most potent, is accumulating.Additional randomized placebo controlled studies inhomogenous groups of pain patients are needed to explorethe therapeutic potential of NMDA receptor antagonists inneuropathic pain.
Acknowledgments
We would like to express our gratitude to Ingrid Riphagen,MSc (Medical Library, VU University, Amsterdam, theNetherlands) for her expertise and support in searchingthe literature and to Prof Dr Riekie de Vet (EMGO+ Institutefor Health and Care Research, Amsterdam, VU UniversityMedical Center Amsterdam, the Netherlands) for heradvice with regard to the methodological assessment.This study is part of TREND (Trauma RElated NeuronalDysfunction), a knowledge consortium that integratesresearch on Complex Regional Pain Syndrome type 1(CRPS-1). This project is supported by a Dutch Govern-ment grant (BSIK03016).
Appendix [15,16,18,60–63]
Calculating Hedges’ g from the Mean, StandardDeviation and Number of Subjects
g M M SD pooledi e c= −( )
SD pooledSD n 1 +
SD n 1 n n 2e
2e
c2
c e c
=( ) −( )⎡⎣ ⎤⎦(
) −( )⎡⎣ ⎤⎦ +( ) − )Where, gi = hedges’ g for individual study i, M = mean,e = experimental group, c = control group, SD = standarddeviation, n = sample size in a particular group.
Calculating Hedges’ g from the t-Test
g tt
i e c e c e
c i
n n n n , and when n andn are equal g 2 N= +( ) ( )
=
Where, t = value of the t-test, N = total sample size.
Calculating Hedges’ gi from Significance Levels
When only P-values are reported, t-values can beobtained using a calculator or looked up in a table ofthe t distribution using P-levels and the degrees offreedom. From the t-test, hedges’ gi can be calculated(see above).
Calculating 95% Confidence Intervals (CI) forHedges’ gi
CI 1.96 two-tailed and a critical value at 0.05 Vi= ± ( ) ×
V N n n g 2Ni e c i2= ( ) + ( )
Where Vi = within-study variance of individual effect size i.
Calculating Summarized Effect Size Hedges’gAccording to Fixed Effect Model
g g W Ws i i/ i= ∑ ∑Wi 1 Vi=
Where, gs = summarized hedges’ g, Wi = estimatedweight for individual study i.
Calculating Homogeneity Statistics I2
I proportion of total variability explainedby heterogenei
2 =tty
I Q k 1 Q 100%, for Q k 12 = − −( )( ) × > −( )I 0, for Q k 12 = ≤ −( )
Q Wg Wg Wi i2
i i2
i= − ( )∑ ∑ ∑Q Q statistics=
A random effect model must be used when the pooledeffects of studies could be considered heterogeneous(I2 statistics � 25%).
Calculating Summarized Effect Size Hedges’gAccording to Random Effects Model
g g W Ws i i/ i= ∑ ∑Wi 1 V *i=
V * V,i2
i= +σθ
σθ2 Q k 1 c,= − −( )( )c W W Wi i
2i= − ( ) )( )∑ ∑ ∑
Where Vi* = total variance, sq2 = between study variance,
Q = Q statistics, k = number of studies in the meta-analysis.
Calculating 95% CI for gs
CI 1.96 two-tailed and a critical value at 0.05 Vs= ± ( ) ×
V 1 Ws i= ∑Where, Vs = variance of summarized effect size.
Calculating P-Values for gs
Z g Vs s=
Where, Z = Z-value.
P vales can be obtained using Z table.
References1 Loeser JD, Treede RD. The Kyoto protocol of IASP
Basic Pain Terminology. Pain 2008;137:473–7.
2 Baron R. Mechanisms of disease: Neuropathicpain—A clinical perspective. Nat Clin Pract Neurol2006;2:95–106.
1739
NMDA Receptor Antagonists for Neuropathic Pain

3 Bridges D, Thompson SWN, Rice ASC. Mechanismsof neuropathic pain. Br J Anaesth 2001;87:12–26.
4 Schaible HG, Richter F. Pathophysiology of pain. Lan-genbeck’s Arch Surg 2004;389:237–43.
5 Schwartzman RJ, Grothusen J, Kiefer TR, et al. Neu-ropathic central pain—Epidemiology, etiology, andtreatment options. Arch Neurol 2001;58:1547–50.
6 Finnerup NB, Otto M, McQuay HJ, et al. Algorithm forneuropathic pain treatment: An evidence-based pro-posal. Pain 2005;118:289–305.
7 Bleakman D, Alt A, Nisenbaum ES. Glutamate recep-tors and pain. Semin Cell Dev Biol 2006;17:592–604.
8 Bennett GJ. Update on the neurophysiology of paintransmission and modulation: Focus on the NMDA-receptor. J Pain Symptom Manage 2000;19:S2–S6.
9 Carlton SM, Hargett GL, Coggeshall RE. Localizationand activation of glutamate receptors in unmyelinatedaxons of rat glabrous skin. Neurosci Lett 1995;197:25–8.
10 Petrenko AB, Yamakura T, Baba H, et al. The role ofN-Methyl-D-Aspartate (NMDA) receptors in pain: Areview. Anesth Analg 2003;97:1108–16.
11 Carpenter KJ, Dickenson AH. NMDA receptors andpain—Hopes for novel analgesics. Reg Anesth PainMed 1999;24:506–8.
12 Glanville JM, Lefebvre C, Miles JN, et al. How to iden-tify randomized controlled trials in MEDLINE: Ten yearson. J Med Libr Assoc 2006;94:130–6.
13 Verhagen AP, de Vet HCW, de Bie RA, et al. TheDelphi list: A criteria list for quality assessment of ran-domized clinical trials for conducting systematicreviews developed by Delphi Consensus. J Clin Epi-demiol 1998;51:1235–41.
14 Verhagen AP, Karels C, Bierma-Zeinstra SMA, et al.Ergonomic and physiotherapeutic interventions fortreating work-related complaints of the arm, neck orshoulder in adults. Cochrane Database Syst Rev2006;19;3:CD003471.
15 Cooper H, Hedges V. The Handbook of ResearchSynthesis. New York: Russel Sage Foundation; 1994.
16 Durlak JA. How to select, calculate, and interpreteffect sizes. J Pediatr Psychol 2009;34:917–28.
17 Higgins JPT, Thompson SG. Quantifying heterogene-ity in a meta-analysis. Stat Med 2002;21:1539–58.
18 Higgins JPT, Thompson SG, Deeks JJ, et al. Measur-ing inconsistency in meta-analyses. BMJ 2003;327:557–60.
19 Cohen J. Statistical Power Analysis for the BehavioralStudies. New York: Academic Press; 1988.
20 Felsby S, Nielsen J, Rendt-Nielsen L, et al. NMDAreceptor blockade in chronic neuropathic pain: A com-parison of ketamine and magnesium chloride. Pain1996;64:283–91.
21 Nikolajsen L, Hansen CL, Nielsen J, et al. The effect ofketamine on phantom pain: A central neuropathic dis-order maintained by peripheral input. Pain 1996;67:69–77.
22 Max MB, Byassmith MG, Gracely RH, et al.Intravenous-infusion of the NMDA antagonist, ket-amine, in chronic posttraumatic pain with allodynia—Adouble-blind comparison to alfentanil and placebo.Clin Neuropharmacol 1995;18:360–8.
23 Eisenberg E, Kleiser A, Dortort A, et al. The NMDA(N-methyl-D-aspartate) receptor antagonist meman-tine in the treatment of postherpetic neuralgia: Adouble-blind, placebo-controlled study. Eur J Pain1998;2:321–7.
24 Pud D, Eisenberg E, Spitzer A, et al. The NMDAreceptor antagonist amantadine reduces surgicalneuropathic pain in cancer patients: A double-blind,randomized, placebo controlled trial. Pain 1998;75:349–54.
25 Medrik-Goldberg T, Lifschitz D, Pud D, et al. Intrave-nous lidocaine, amantadine, and placebo in the treat-ment of sciatica: A double-blind, randomized,controlled study. Reg Anesth Pain Med 1999;24:534–40.
26 Galer BS, Twilling LL, Harle J, et al. Lack of efficacy ofriluzole in the treatment of peripheral neuropathic painconditions. Neurology 2000;55:971–5.
27 Gilron I, Booher SL, Rowan JS, et al. A randomized,controlled trial of high-dose dextromethorphan in facialneuralgias. Neurology 2000;55:964–71.
28 Nikolajsen L, Gottrup H, Kristensen AGD, et al.Memantine (a N-methyl-D-aspartate receptor antago-nist) in the treatment of neuropathic pain after ampu-tation or surgery: A randomized, double-blinded,cross-over study. Anesth Analg 2000;91:960–6.
29 Leung A, Wallace MS, Ridgeway B, et al.Concentration-effect relationship of intravenous alfen-tanil and ketamine on peripheral neurosensory thresh-olds, allodynia and hyperalgesia of neuropathic pain.Pain 2001;91:177–87.
1740
Collins et al.

30 Abraham RB, Marouani N, Kollender Y, et al. Dex-tromethorphan for phantom pain attenuation in canceramputees: A double-blind crossover trial involvingthree patients. Clin J Pain 2002;18:282–5.
31 Brill S, Sedgwick PM, Hamann W, et al. Efficacy ofintravenous magnesium in neuropathic pain. Br JAnaesth 2002;89:711–4.
32 Sang CN, Booher S, Gilron I, et al. Dextromethorphanand memantine in painful diabetic neuropathy andpostherpetic neuralgia—Efficacy and dose-responsetrials. Anesthesiology 2002;96:1053–61.
33 Wallace MS, Rowbotham MC, Katz NP, et al. A ran-domized, double-blind, placebo-controlled trial of aglycine antagonist in neuropathic pain. Neurology2002;59:1694–700.
34 Abraham RB, Marouani N, Weinbroum AA. Dex-tromethorphan mitigates phantom pain in canceramputees. Ann Surg Oncol 2003;10:268–74.
35 Amin P, Sturrock NDC. A pilot study of the beneficialeffects of amantadine in the treatment of painful dia-betic peripheral neuropathy. Diabet Med 2003;20:114–8.
36 Jorum E, Warncke T, Stubhaug A. Cold allodynia andhyperalgesia in neuropathic pain: The effect ofN-methyl-D-aspartate (NMDA) receptor antagonistketamine—A double-blind, cross-over comparisonwith alfentanil and placebo. Pain 2003;101:229–35.
37 Maier C, Dertwinkel R, Mansourian N, et al. Efficacy ofthe NMDA-receptor antagonist memantine in patientswith chronic phantom limb pain—Results of a ran-domized double-blinded, placebo-controlled trial. Pain2003;103:277–83.
38 Carlsson KC, Hoem NO, Moberg ER, et al. Analgesiceffect of dextromethorphan in neuropathic pain. ActaAnaesthesiol Scand 2004;48:328–36.
39 Wiech K, Kiefer RT, Topfner S, et al. A placebo-controlled randomized crossover trial of the N-methyl-D-aspartic acid receptor antagonist, memantine, inpatients with chronic phantom limb pain. Anesth Analg2004;98:408–13.
40 Gottrup H, Bach FW, Juhl G, et al. Differential effect ofketamine and lidocaine on spontaneous and mechani-cal evoked pain in patients with nerve injury pain.Anesthesiology 2006;104:527–36.
41 Schifitto G, Yiannoutsos CT, Simpson DM, et al. Aplacebo-controlled study of memantine for the treat-ment of human immunodeficiency virus-associatedsensory neuropathy. J Neurovirol 2006;12:328–31.
42 Forst T, Smith T, Schutte K, et al. Dose escalatingsafety study of CNS5161HCl, a new neuronalglutamate receptor antagonist (NMDA) for the treat-ment of neuropathic pain. Br J Clin Pharmacol2007;64:75–82.
43 Eichenberger U, Neff F, Sveticic G, et al. Chronicphantom limb pain: The effects of calcitonin, ketamine,and their combination on pain and sensory thresholds.Anesth Analg 2008;106:1265–73. table.
44 Schwartzman RJ, Alexander GM, Grothusen JR, et al.Outpatient intravenous ketamine for the treatment ofcomplex regional pain syndrome: A double-blindplacebo controlled study. Pain 2009;147:107–15.
45 Sigtermans MJ, van Hilten JJ, Bauer MC, et al. Ket-amine produces effective and long-term pain relief inpatients with complex regional pain syndrome type 1.Pain 2009;145:304–11.
46 Furuhashi-Yonaha A, Iida H, Asano T, et al. Short- andlong-term efficacy of oral ketamine in eight chronic-pain patients. Can J Anaesth 2002;49:886–7.
47 Finch PM, Knudsen L, Drummond PD. Reduction ofallodynia in patients with complex regional pain syn-drome: A double-blind placebo-controlled trial oftopical ketamine. Pain 2009;146:18–25.
48 Childers WE, Baudy RB. N-Methyl-D-Aspartateantagonists and neuropathic pain: The search forrelief. J Med Chem 2007;50:2557–62.
49 Backonja MM, Galer BS. Pain assessment and evalu-ation of patients who have neuropathic pain. NeurolClin 1998;16:775–90.
50 Chen HSV, Lipton SA. The chemical biology of clini-cally tolerated NMDA receptor antagonists. J Neuro-chem 2006;97:1611–26.
51 Paoletti P, Neyton J. NMDA receptor subunits: Func-tion and pharmacology. Curr Opin Pharmacol2007;7:39–47.
52 Albrecht PJ, Hines S, Eisenberg E, et al. Pathologicalterations of cutaneous innervation and vasculature inaffected limbs from patients with complex regionalpain syndrome. Pain 2006;120:244–66.
53 Oaklander AL, Rissmiller JG, Gelman LB, et al. Evi-dence of focal small-fiber axonal degeneration incomplex regional pain syndrome-I (reflex sympatheticdystrophy). Pain 2006;120:235–43.
54 Chemali KR, Zhou L. Small fiber degeneration in post-stroke complex regional pain syndrome I. Neurology2007;69:316–7.
1741
NMDA Receptor Antagonists for Neuropathic Pain

55 Desmeules JA, Cedraschi C, Rapiti E, et al. Neuro-physiologic evidence for a central sensitization inpatients with fibromyalgia. Arthritis Rheum2003;48:1420–9.
56 Staud R, Cannon RC, Mauderli AP, et al. Temporalsummation of pain from mechanical stimulation ofmuscle tissue in normal controls and subjects withfibromyalgia syndrome. Pain 2003;102:87–95.
57 Granot M, Buskila D, Granovsky Y, et al. Simultaneousrecording of late and ultra-late pain evoked potentialsin fibromyalgia. Clinical. Neurophysiology 2001;112:1881–7.
58 Graven-Nielsen T, Kendall SA, Henriksson KG, et al.Ketamine reduces muscle pain, temporal summation,and referred pain in fibromyalgia patients. Pain2000;85:483–91.
59 Arendt-Nielsen L, Nielsen J, Petersen-Felix S, et al.Effect of racemic mixture and the (S+)-isomer of ket-
amine on temporal and spatial summation of pain. BrJ Anaesth 1996;77:625–31.
60 Sanchez-Meca J, Marin-Martinez F. Weighting byinverse variance or by sample size in meta-analysis: Asimulation study. Educ Psychol Meas 1998;58:211–20.
61 Huedo-Medina TB, Sanchez-Meca J, Marin-MartinezF, et al. Assessing heterogeneity in meta-analysis:Q statistic or I-2 index? Psychol Meth 2006;11:193–206.
62 Sanchez-Meca J, Marin-Martinez F. Confidence inter-vals for the overall effect size in random-effects meta-analysis. Psychol Meth 2008;13:31–48.
63 Marin-Martinez F, Sanchez-Meca J. Weighting byinverse variance or by sample size in random-effects meta-analysis. Educ Psychol Meas 2010;70:56–73.
1742
Collins et al.