nitric oxide inhalation and nitric oxide synthase inhibitor supplement for endotoxin-induced...
TRANSCRIPT
The principal objective in treating persistent pulmonaryhypertension of the newborn (PPHN) is to selectively lowerpulmonary arterial pressure. Treatments used to date haveincluded hyperventilation alkali-therapy and drug therapy.1–3
However, these carry the risk of inducing dilatation of thesystemic arteries rather than just pulmonary arteries, in turnlowering the systemic arterial pressure. In 1992, Robertset al. and Kinsella et al. introduced NO inhalation therapyfor the treatment of PPHN, and its use spread almostinstantaneously around the world.4,5 In NO therapy, NO gas,which dilates blood vessels, is inhaled directly through thetrachea. As the NO gas enters the lungs and is deactivatedby binding with hemoglobin in the pulmonary circulation,the vessel dilatory action of the NO does not reachperipheral locations outside of the lungs.
The selective dilatory action of NO on the pulmonaryvessels is what currently makes NO inhalation the leadingtreatment for PPHN.6,7 However, it has become a commonexperience to find that NO inhalation is not as effectiveagainst PPHN complicated with sepsis as it is against PPHNwith meconium aspiration syndrome (MAS).8 One reasonfor this is thought to be the hypotension produced by sepsis.When the patient is in a state of endotoxin shock, NOtherapy is ineffective and there is no response to theadministration of vasopressors such as catecholamines;therefore the prognosis is poor. The primary factors in thiscondition are thought to be blood vessel dilation and thereduced contraction of cardiac muscles as a result of theexcessive production of endogenous NO.9
Some studies on circulatory dynamics during experi-mental endotoxin shock have been reported. In particular,there have been occasional reports over the past severalyears on the use of NOS inhibitors against low bloodpressure as a result of the excessive production of NO totreat circulatory failure caused by endotoxins.10 Initially,
Pediatrics International (2001) 43, 343–349
Original Article
Nitric oxide inhalation and nitric oxide synthase inhibitorsupplement for endotoxin-induced hypotension
SATOSHI SUZUKI,1 HAJIME TOGARI,2 NOBUYUKI YAMAGUCHI2 AND KELLY MULLINSHAAS2
1Department of Pediatrics, Nagoya City Johoku Hospital and 2Department of Pediatrics, Nagoya CityUniversity Medical School, Nagoya, Japan
Abstract BBaacckkggrroouunndd: This study was performed to determine whether a combined therapy of nitric oxide (NO)inhalation and nitric oxide synthase (NOS) inhibitor is effective in experimental animals with endotoxin-induced refractive hypotension accompanied by pulmonary hypertension.MMeetthhooddss: Escherichia coli lipopolysaccharide (1 mg/kg) was administered to 10 newborn piglets to induceendotoxemia. The experiment then began 60 min later, when the systemic arterial pressure dropped. Theinhalation of 20 p.p.m. NO at 60 and 120 min of endotoxemia created a control group. Another group wasalso administered N w-nitro-L-arginine (L-NNA; 5 mg) after the first NO inhalation at 60 min of endo-toxemia (the L-NNA group). Pulmonary arterial pressure, systemic arterial pressure and cardiac output weremeasured and compared among the groups.RReessuullttss: Three of the 5 piglets in the control group died of hypotensive shock, while in the L-NNA group thesystemic arterial pressure recovered to pre-endotoxin administration levels. The L-NNA group produced afurther increase in pulmonary arterial pressure against which NO inhalation was effective.CCoonncclluussiioonn: Nitric oxide inhalation alone carries a potential risk of further lowering systemic arterialpressure in a piglet with hypotension induced by endotoxin, whereas the combined therapy resulted in therecovery of the blood pressure to pre-endotoxin levels. The combined therapy was simultaneously effectiveagainst pulmonary hypertension.
Key words endotoxin-induced hypotension, newborn infant, nitric oxide inhalation, nitric oxide synthase inhibitor.
Correspondence: Satoshi Suzuki, Division of Neonatology,Department of Pediatrics, Nagoya City Johoku Hospital, 2-15Kita Nagoya, 462-0033 Japan. Email: [email protected]
Received 4 August 2000; revised 5 February 2001; accepted16 February 2001.

good results were reported in animal experiments using NOSinhibitors only.11–13 However, it was later found that adminis-tration of NOS inhibitors carries a great risk of decreasingcardiac output and tissue blood flow, or ischemia of thecardiac muscles.14 Thus, this has recently been considered aninappropriate treatment.15–20 However, most of these experi-ments used mature animals, with investigations using new-born animals rarely encountered. Furthermore, in actualclinical practice, this pathological condition is seen morefrequently in infants soon after birth, as well as in neonateswith residual physiological pulmonary hypertension. How-ever, most current data is for older infants. The presentexperiment was therefore conducted to provide more data onthe postnatal period.
In the present study, we prepared a model of pulmonaryhypertension accompanying endotoxin-induced hypotensionin piglets immediately after birth, and investigated theeffects of NO inhalation and NOS inhibitors on the circula-tory system. The aim of this study was to investigatewhether a combined treatment using NO inhalation and thetotal NOS inhibitor Nω-nitro-L-arginine (L-NNA) is effectiveagainst early phase hypotension and pulmonary hypertensionfollowing the administration of endotoxins. Endotoxin shockmay be considered to have an early stage beginning whenthe systemic arterial pressure drops about 1 h after adminis-tration and a subsequent late stage. As the late stage involvesthe risk of multiple organ failure it was excluded from thepresent investigation.
Methods
This experimental protocol was approved by the EthicsCommittee of the Nagoya City University Medical School.After anesthetizing 10 newborn piglets (day 0) with theinhalation of ether and an intramuscular injection of 20 mg/kgpentobarbital sodium, an incision was made in the tracheaand a Portex tube (3.5 mm) was inserted. The piglets wereparalyzed with 0.2 mg/kg of pancuronium bromide andventilated with a Sechrist Infant Ventilator (model IV-100;Sechrist, Anaheim, CA, USA). The pressure was initially setat inspiration pressure/expiration pressure of 10/1 cmH2O,inspiratory time of 0.5 s, and was then adjusted to maintainPaO2 between 60 and 80 mmHg and PaCO2 between 35 and45 mmHg. A 5 Fr Swan-Ganz catheter (Thermodilutioncatheter, Baxter Healthcare Corporation, Edwards Division,Deerfieldf, IL, USA) or a 5 Fr Berman angiographic catheter(Balloon catheter, Arrow, USA) was inserted using fluoro-scopy via the external carotid vein, and placed in the mainpulmonary artery to measure the pulmonary arterial pressure(PAP) and cardiac output. Systemic arterial pressure (SAP)was monitored in the descending aorta via the umbilicalartery.
Escherichia coli (O-111, k-58) was incubated overnightand lipopolysaccharides (LPS) were extracted by the phenol-water method. They were then purified by centrifugation anddialysis.
After stabilizing the piglets in the supine position, LPSwere administered through the umbilical vein to create theendotoxin model. The ventilator setting was then adjusted tomaintain PaO2 and PaCO2 within the range mentioned above.The early phase of endotoxin shock (60 min endotoxemia)was taken to be the point about 60 min after the adminis-tration of LPS when the blood pressure had dropped to lessthan 75% of the pre-experiment level. The experiment wasbegun at this point.
The first 20 p.p.m. NO inhalation (1st iNO) was dispensedat 60 min endotoxemia. Changes in the pulmonary arterialpressure and blood pressure were observed. Then, 1 mL ofsaline was given to the control group and 5 mg of L-NNA(3 mg in a bolus followed by infusion of 2 mg for 20 min) tothe L-NNA group via the umbilical vein. Sixty minutes later(120 min endotoxemia) the second 20 p.p.m. NO inhalation(2nd iNO) was dispensed. The pulmonary arterial pressure,blood pressure, and cardiac output were compared betweenthe two groups.
A MacLab/8 s (ADI Instruments, Mountain View, CA,USA) was used for data collection, and a Ciba-CorningBlood Gas Analyzer model 248 (CIBA Corning, Medfield,MA, USA) for monitoring blood gases. The pulmonary andsystemic arterial pressures were measured with a HewlettPackard model 78801 B Neonatal Monitor (Hewlett Packard,Andover, MA, USA). Cardiac output was measured with aCardiac Output Computer, model 9520 A (American EdwardsLaboratories, Irvine, CA, USA). Concentrations of NO, nitricdioxide (NO2), and nitric oxides (NOX), within the NOinhalation circuit were continuously measured with aChemiluminescence NO-NO2-NOX Analyzer, model 42H(Thermo Electron Corporation, Franklin, MA, USA).
All results were analyzed using the matched paired t-test,and P<0.05 was considered statistically significant.
Results
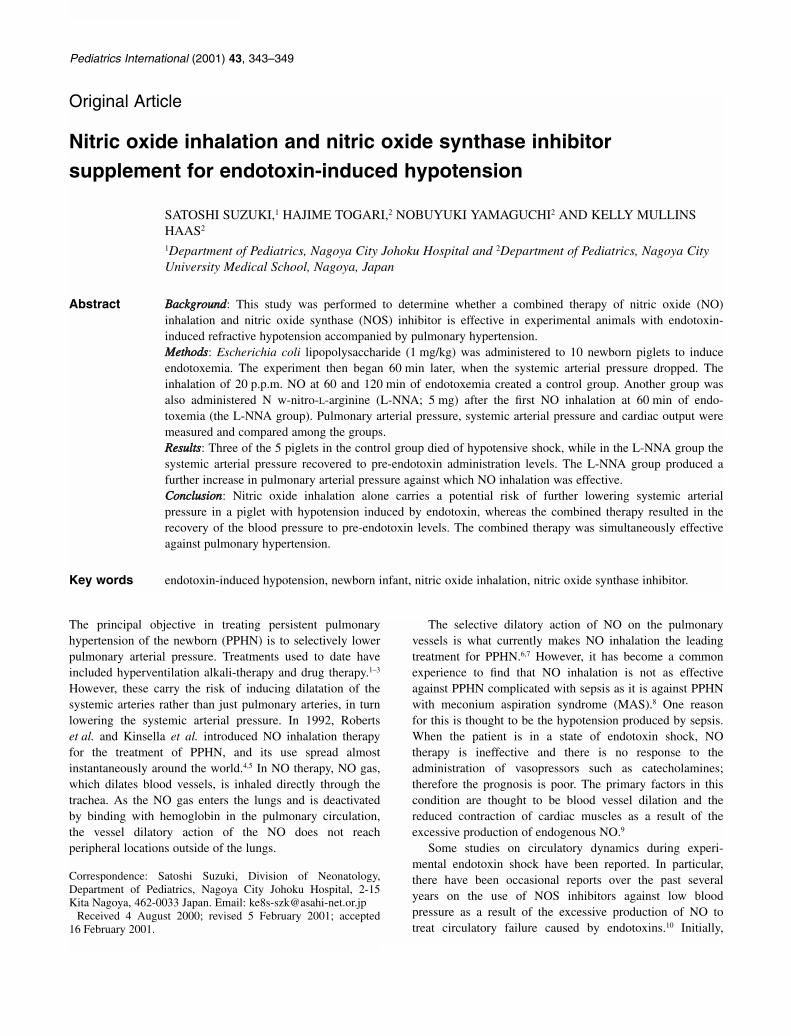
There were no significant differences between the twogroups in bodyweight or pre-experimental systemic arterialpressure, pulmonary arterial pressure, cardiac output, pH,PaO2, or PaCO2 (Table 1). There was a temporary rise inboth systemic and pulmonary arterial pressures following theadministration of 1 mg/kg of the endotoxin. After 60 min,the systemic arterial pressure had dropped to 57~6.7 mmHg(71% of pre-endotoxin level) in the control group and54~25.3 mmHg (68%) in the L-NNA group, both signifi-cantly lower than pre-experimental values. In contrast,pulmonary arterial pressure was 31.6~3.8 mmHg (168%)
344 S Suzuki et al.
in the control group and 24.8~4.0 mmHg (141%) in the L-NNA group, both being states of pulmonary hypertension.Cardiac output following the administration of the endotoxindecreased from 0.36~0.04–0.25~0.05 L/min (69%) in thecontrol group, and from 0.36~0.05–0.27~0.04 L/min(75%) in the L-NNA group (Fig. 1a,b,c)
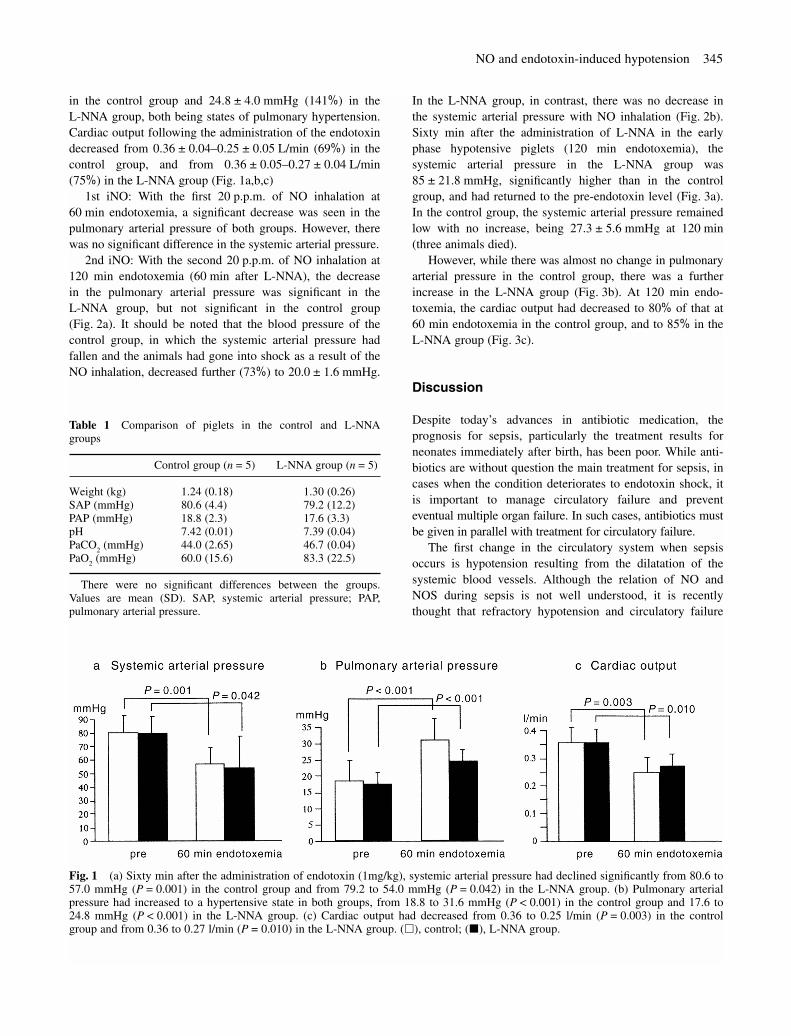
1st iNO: With the first 20 p.p.m. of NO inhalation at60 min endotoxemia, a significant decrease was seen in thepulmonary arterial pressure of both groups. However, therewas no significant difference in the systemic arterial pressure.
2nd iNO: With the second 20 p.p.m. of NO inhalation at120 min endotoxemia (60 min after L-NNA), the decrease in the pulmonary arterial pressure was significant in the L-NNA group, but not significant in the control group(Fig. 2a). It should be noted that the blood pressure of thecontrol group, in which the systemic arterial pressure hadfallen and the animals had gone into shock as a result of theNO inhalation, decreased further (73%) to 20.0~1.6 mmHg.
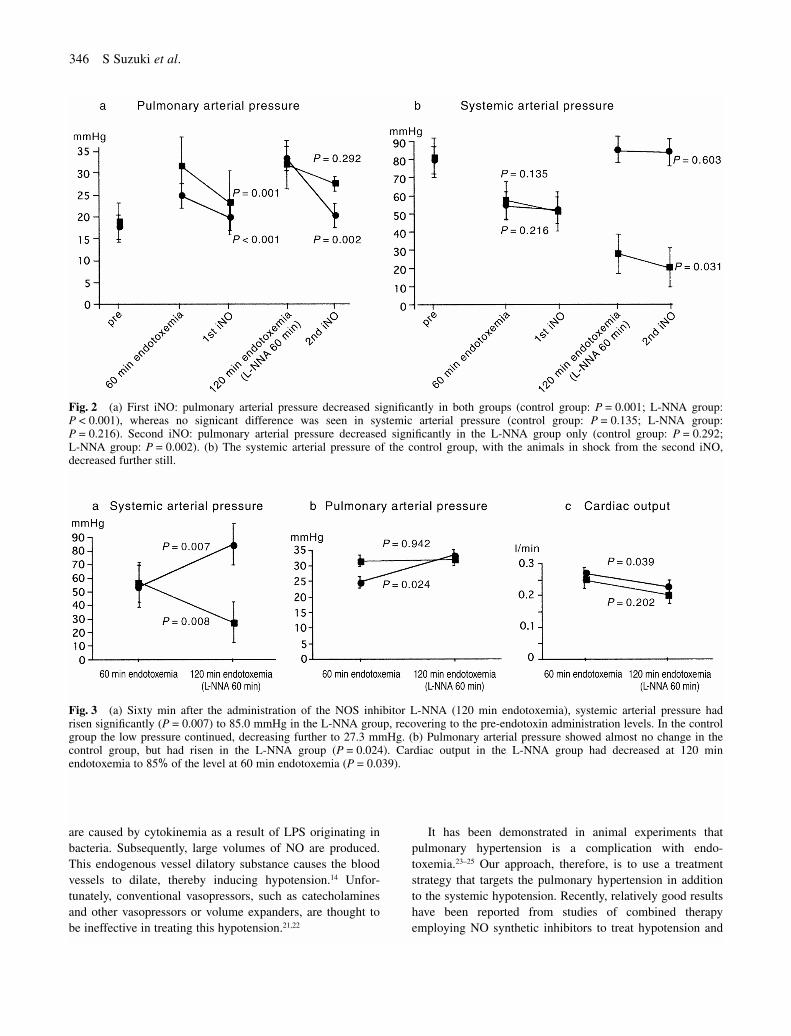
In the L-NNA group, in contrast, there was no decrease inthe systemic arterial pressure with NO inhalation (Fig. 2b).Sixty min after the administration of L-NNA in the earlyphase hypotensive piglets (120 min endotoxemia), thesystemic arterial pressure in the L-NNA group was85~21.8 mmHg, significantly higher than in the controlgroup, and had returned to the pre-endotoxin level (Fig. 3a).In the control group, the systemic arterial pressure remainedlow with no increase, being 27.3~5.6 mmHg at 120 min(three animals died).
However, while there was almost no change in pulmonaryarterial pressure in the control group, there was a furtherincrease in the L-NNA group (Fig. 3b). At 120 min endo-toxemia, the cardiac output had decreased to 80% of that at60 min endotoxemia in the control group, and to 85% in theL-NNA group (Fig. 3c).
Discussion
Despite today’s advances in antibiotic medication, theprognosis for sepsis, particularly the treatment results forneonates immediately after birth, has been poor. While anti-biotics are without question the main treatment for sepsis, incases when the condition deteriorates to endotoxin shock, itis important to manage circulatory failure and preventeventual multiple organ failure. In such cases, antibiotics mustbe given in parallel with treatment for circulatory failure.
The first change in the circulatory system when sepsisoccurs is hypotension resulting from the dilatation of thesystemic blood vessels. Although the relation of NO andNOS during sepsis is not well understood, it is recentlythought that refractory hypotension and circulatory failure
NO and endotoxin-induced hypotension 345
Table 1 Comparison of piglets in the control and L-NNAgroups
Control group (n=5) L-NNA group (n=5)
Weight (kg) 1.24 (0.18) 1.30 (0.26)SAP (mmHg) 80.6 (4.4) 79.2 (12.2)PAP (mmHg) 18.8 (2.3) 17.6 (3.3)pH 7.42 (0.01) 7.39 (0.04)PaCO2 (mmHg) 44.0 (2.65) 46.7 (0.04)PaO2 (mmHg) 60.0 (15.6) 83.3 (22.5)
There were no significant differences between the groups.Values are mean (SD). SAP, systemic arterial pressure; PAP,pulmonary arterial pressure.
Fig. 1 (a) Sixty min after the administration of endotoxin (1mg/kg), systemic arterial pressure had declined significantly from 80.6 to57.0 mmHg (P=0.001) in the control group and from 79.2 to 54.0 mmHg (P=0.042) in the L-NNA group. (b) Pulmonary arterialpressure had increased to a hypertensive state in both groups, from 18.8 to 31.6 mmHg (P<0.001) in the control group and 17.6 to24.8 mmHg (P<0.001) in the L-NNA group. (c) Cardiac output had decreased from 0.36 to 0.25 l/min (P=0.003) in the controlgroup and from 0.36 to 0.27 l/min (P=0.010) in the L-NNA group. (�), control; (�), L-NNA group.
are caused by cytokinemia as a result of LPS originating inbacteria. Subsequently, large volumes of NO are produced.This endogenous vessel dilatory substance causes the bloodvessels to dilate, thereby inducing hypotension.14 Unfor-tunately, conventional vasopressors, such as catecholaminesand other vasopressors or volume expanders, are thought tobe ineffective in treating this hypotension.21,22
It has been demonstrated in animal experiments thatpulmonary hypertension is a complication with endo-toxemia.23–25 Our approach, therefore, is to use a treatmentstrategy that targets the pulmonary hypertension in additionto the systemic hypotension. Recently, relatively good resultshave been reported from studies of combined therapyemploying NO synthetic inhibitors to treat hypotension and
346 S Suzuki et al.
Fig. 2 (a) First iNO: pulmonary arterial pressure decreased significantly in both groups (control group: P=0.001; L-NNA group:P<0.001), whereas no signicant difference was seen in systemic arterial pressure (control group: P=0.135; L-NNA group:P=0.216). Second iNO: pulmonary arterial pressure decreased significantly in the L-NNA group only (control group: P=0.292; L-NNA group: P=0.002). (b) The systemic arterial pressure of the control group, with the animals in shock from the second iNO,decreased further still.
Fig. 3 (a) Sixty min after the administration of the NOS inhibitor L-NNA (120 min endotoxemia), systemic arterial pressure hadrisen significantly (P=0.007) to 85.0 mmHg in the L-NNA group, recovering to the pre-endotoxin administration levels. In the controlgroup the low pressure continued, decreasing further to 27.3 mmHg. (b) Pulmonary arterial pressure showed almost no change in thecontrol group, but had risen in the L-NNA group (P=0.024). Cardiac output in the L-NNA group had decreased at 120 minendotoxemia to 85% of the level at 60 min endotoxemia (P=0.039).

NO inhalation for pulmonary hypertension.23,25,26 However,most cases of sepsis treated by neonatologists occur within72 h of birth, when respiratory and circulatory dynamics areadapting to the extra-uterine environment. However, each ofthe studies cited above used young pigs or adult animals assubjects. Obviously, the respiratory and circulatory dynamicsof neonates are immature compared to those of adults andthe sensitivity to endotoxins is likely to be different. Data onneonates immediately after birth are necessary, and thus thepresent experiment was conducted using day 0 neonatalpigs. In actual clinical practice most patients sent to neo-natologists have already fallen into endotoxin shock andhave gone into a hypotensive state. To simulate this, thepresent experiment began at the point where the systemicarterial pressure had fallen below 75% of the standard value.A comparison was then made between the control group(endotoxin only) and the NOS inhibitor treatment group (L-NNA).
In the present study, the experiment began in both groups60 min after the administration of the endotoxin, at a timewhen significant hypotension and pulmonary hypertensionhad been achieved compared to the beginning of the experi-ment. Unfortunately, three of the five animals in the controlgroup died of this hypotension. This is similar to the resultsobtained by Henderson et al. using dogs, in which the hypo-tension started 40 min after the administration of endotoxinsand the animals died at 90 min.19 As the expression of theNOS in the blood vessel endothelium and nitrite (NO2–) andnitrate (NO3–) concentrations in the serum were not directlyobserved, it is unknown whether inducible NOS (iNOS) orconstitutive NOS (cNOS) contributed to the hypotension;however, if one considers that endotoxin shock is dividedinto early and late phases, it seems clear considering thetime-course that this is early phase endotoxin shock with theparticipation of cNOS.21,22 In early phase endotoxin shock,the blood vessels are dilated as a result of the excessiveproduction of NO, peripheral blood resistance declines, andhypotension results.
The cause of the pulmonary hypertension in endotoxinshock is probably multifactorial.25 It possibly includesthromboxane, perivascular edema, intravascular obstruction,and hypoxic vasoconstriction.27,28 At present the role of NOin septic pulmonary hypertension is not clearly understood.However, as only the pulmonary arteries are constricted, therelease of some type of vasoconstrictor is not likely; rather,there appears to be some secondary effect from the hypoxiaas a result of the degrading condition. As small neonatalpigs weighing about 1.5 kg were used in the present experi-ment, wedge pressure and central venous pressure could notbe measured, so neither pulmonary vascular resistance(PVR) nor systemic vascular resistance (SVR) could bedirectly evaluated. Considering the changes in pulmonaryand systemic arterial pressure, however, it is suggested that
the endotoxin shock is expressed as an elevation in the PVRand a decrease in the SVR.
It has been reported both that cardiac output increases14
and decreases26,29 due to endotoxins. In the present studycardiac output declined, and it is likely that in this conditionthere are diastolic disturbances in the left ventricle as aresult of decreased blood flow from the right ventriclecaused by an elevation in the pulmonary arterial pressure,resulting in reduced output from the left ventricle. However,as one report indicates, endotoxins may have a suppressiveaction exerted via the central nervous system, or cytokinesinduced by endotoxins directly block the cardiac nervoussystem.30 Sosa et al. indicated endotoxins themselves mayserve to impair the contraction of cardiac muscles.31
As NO inhalation selectively dilates the pulmonaryvessels, it is more effective than any other treatment forPPHN. Furthermore, it is considered safe in cases compli-cated with systemic hypotension. However, it is a commonclinical experience that NO inhalation is not effective incases of PPHN complicated with infectious diseases such aspneumonia or sepsis. Nitric oxide inhalation, which waseffective in 60 min endotoxemia in the present study, hadeither no significant effect in lowering the pulmonary arterialpressure or else the animals fell into a fatal systemic hypo-tension in the control group with 120 min endotoxemia. Incontrast, in the L-NNA group there was a selective, signifi-cant decrease in pulmonary arterial pressure with no effecton the systemic arterial pressure. While Offner et al. havereported similar results, the present study demonstrated theeffectiveness of a combined therapy of NO inhalation andNOS inhibitors, even in neonatal animals on day 0.23,25,26
Furthermore, it was suggested that in cases of endotoxin-induced hypotension complicated with pulmonary hyper-tension, NO inhalation carries the risk of aggravating thehypotension.
According to Wu et al. and Szabo et al., hypotension inendotoxin shock is refractory to treatment and does notrespond to catecholamines or other vasopressors.21,22 In fact,refractory hypotension is the cause of death in nearly allcases of endotoxin shock in the Neonatal Intensive CareUnit. In the present study, L-NNA not only inhibited the fall of blood pressure in endotoxin-induced hypotension in neonatal animals, it even caused blood pressure to return to pre-experimental levels. Reports show that theadministration of NOS inhibitors before the administrationof endotoxins prevents shock or inhibits the decrease inblood pressure.21,23,26 There are few reports of successfultreatment after the subjects had fallen into a state of hypo-tensive shock.25 The above suggests that the use of NOSinhibitors may greatly improve the treatment of hypotensionas a result of endotoxin shock in neonates. In contrast, someEuropean studies found no effect of NOS inhibitors. Thismay have been because of the timing of the administration
NO and endotoxin-induced hypotension 347

of the NOS inhibitors in the adult human subjects in thosestudies.
Henderson et al. reported that local blood flow in organsdecreased as blood pressure rose as a result of NOSinhibitors.19 It is true that L-NNA is an endothelial NOS(eNOS) inhibitor, and that it suppresses eNOS present inblood vessel endothelium throughout the body, which mayinduce decreased blood flow as blood pressure increases.The good results in the present study may indicate that there are differences in the pathophysiology between adultsand infants, or selective differences32 between L-NNA andother NOS inhibitors (e.g. N-nitro-L-arginine methyl ester(L-NAME)), that influence the effectiveness of this treatment.
Conclusion
Using an endotoxin model in newborn piglets, a combinedtherapy of NO inhalation and a NOS inhibitor was given forendotoxin shock accompanied by pulmonary hypertension.Whereas treatment with NO inhalation alone risked inducingfurther decreases in blood pressure during hypotensive endo-toxin shock, this combined therapy improved the conditioneven to the point of bringing blood pressure back to pre-endotoxin administration levels, and was also effective againstthe simultaneously occurring pulmonary hypertension.
References
1 Peckham G, Fox W. Physiologic factors affecting pulmonaryartery pressure in infants with persistent pulmonaryhypertension. J. Pediatr. 1978; 93: 1005–10.
2 Goetzman B, Sunshine P, Johnson J et al. Neonatal hypoxiaand pulmonary vasospasms: Response to tolazoline. J. Pediatr.1976; 89: 617–21.
3 Abu-Osba Y, Galal O, Mansra K et al. Treatment of severepersistent pulmonary hypertension of the newborn withmagnesium sulfate. Arch. Dis. Child. 1992; 67: 31–5.
4 Roberts J, Polaner D, Zapol W et al. Inhaled nitric oxide inpersistent pulmonary hypertension of the newborn. Lancet1992; 340: 818–9.
5 Kinsella J, Neish S, Abman S et al. Low-dose inhalation nitricoxide in persistent pulmonary hypertension of the newborn.Lancet 1992; 340: 819–20.
6 Ehrenkranz R et al. (The Neonatal Inhaled Nitric Oxide StudyGroup). Inhaled nitric oxide in full-term and nearly full-terminfants with hypoxic respiratory failure. N. Engl. J. Med.1997; 336: 597–604.
7 Roberts J, Fineman J, Zapol W et al. (The Inhaled NitricOxide Study Group). Inhaled nitric oxide and persistentpulmonary hypertension of the newborn. N. Engl. J. Med.1997; 336: 605–10.
8 Troncy E, Collet JP, Shapiro S et al. Inhaled nitric oxide inacute respiratory distress syndrome: a pilot randomizedcontrolled study. Am. J. Respir. Crit. Care Med. 1998; 157:1483–8.
9 Habib F, Dutka D, Crossman D et al. Enhanced basal nitric
oxide production in heart failure: another failed counter-regulatory vasodilator mechanism? Lancet 1994; 344: 371–3.
10 Petros A, Lamb G, Leone A et al. Effects of a nitric oxidesynthase inhibitor in humans with septic shock. Cardiovasc.Res. 1994; 28: 34–8.
11 Rees D, Palmer R, Moncada S. Role of endothelium derivednitric oxide in the regulation of blood pressure. Proc. Natl.Acad. Sci. USA 1989; 86: 3375–8.
12 Meyer J, Trader L, Nelson S et al. Reversal of hyperdynamicresponse to continuous endotoxin administration by inhibitionof NO synthesis. J. Appl. Physiol. 1992; 73: 324–8.
13 Cobb J, Natanson C, Quezado Z et al. Differential hemo-dynamic effects of L-NMMA in endotoxemic and normaldogs. Am. J. Physiol. 1995; 268: H1634–42.
14 Avontuur J, Bruining H, Ince C. Inhibition of nitric oxidesynthesis causes myocardial ischemia in endotoxemic rats.Circ. Res. 1995; 76: 418–25.
15 Hutcheson I, Whittle B, Boughton-Smith N. Role of nitricoxide in maintaining vascular integrity in endotoxin inducedacute intestinal damage in the rat. Br. J. Pharmacol. 1990;101: 815–20.
16 Harbrecht B, Billiar T, Stadler J et al. Inhibition of nitric oxidesynthesis during endotoxemia promotes intrahepatic throm-bosis and an oxygen radical mediated hepatic injury. J. Leuko.Biol. 1992; 52: 390–5.
17 Wright C, Rees D, Moncada S. Protective and pathologicalroles of nitric oxide in endotoxin shock. Cardiovasc. Res.1992; 26: 48–52.
18 Minnard E, Shou J, Naama H et al. Inhibition of nitric oxidesynthesis is detrimental during endotoxemia. Arch. Surg. 1994;129: 142–8.
19 Henderson J, Statman R, Horovitz J et al. The effect of nitricoxide inhibition on regional hemodynamics during hyper-dynamic endotoxemia. Arch. Surg. 1994; 129: 1271–5.
20 Klabunde R, Ritger R. N-monomethyl-L-arginine (NMA)restores arterial blood pressure but reduces cardiac output in acanine model of endotoxic shock. Biochem. Biophys. Res.Commun. 1991; 178: 1135–40.
21 Wu C, Thiemermann C, Vane J. Glibenclamide-inducedinhibition of the expression of inducible nitric oxide synthasein cultured macrophages and in the anaesthetized rat. Br. J.Pharmacol. 1995; 114: 1273–81.
22 Szabo C, Mitchell J, Thiemermann C. Nitric oxide-inducedhyporeactivity to noradrenaline precedes the induction ofnitric oxide synthase in endotoxin shock. Br. J. Pharmacol.1993; 108: 786–92.
23 Offner P, Ogura H, Jordan B. Cardiopulmonary effects ofcombined nitric oxide inhibition and inhaled nitric oxide inporcin endotoxic shock. J. Trauma 1996; 41: 641–6.
24 Rojas J, Larrson L, Stahlman M et al. Pulmonary hemo-dynamic and ultrastructural changes associated with Group Bstreptococcal sepsis in adult sheep and newborn lambs.Pediatr. Res. 1983; 17: 1002–8.
25 Weitzberg E, Rudehill A, Modin A, Lundberg JM. Effect ofcombined nitric oxide inhalation and N-nitro-L-arginineinfusion in porcine endotoxin shock. Crit. Care Med. 1995;23: 909–18.
26 Klemm P, Thiemermann C, Winklmaier G, Martorana PA,Henning R. Effect of nitric oxide synthase inhibition com-bined with nitric oxide inhalation in a porcine model ofendotoxin shock. Br. J. Pharmacol. 1995; 114: 363–8.
27 Hardie E, Olson N. Prostaglandin and thromboxane levelsduring endotoxin-induced respiratory failure in pigs. Prosta-glandins Leukot. Med. 1987; 28: 255–65.
348 S Suzuki et al.

28 Demling R, Smith M, Gunther G et al. Pulmonary injury andprostaglandin production during endotoxaemia in conscioussheep. Am. J. Physiol. 1981; 240: H383–6.
29 Gibson R, Berger J, Redding G et al. Effect of nitric oxidesynthase inhibition during group B streptococcal sepsis inneonatal piglets. Pediatr. Res. 1994; 36: 776–83.
30 Koyama S. Participation of central alpha-receptors on hemo-dynamic response to E.coli endotoxin. Am. J. Physiol. 1984;247: 655–62.
31 Sosa G, Milstein J, Bennett S. Escherichia coli endotoxindepresses left ventricular contractility in neonatal lambs.Pediatr. Res. 1994; 35: 62–7.
32 Robertson F, Offner P, Ciceri D, Becker WK, Pruitt BA.Detrimental haemodynamic effects of nitric oxide synthaseinhibition in septic shock. Arch. Surg. 1994; 129: 149–56.
NO and endotoxin-induced hypotension 349