nhsn updates - stratis · pdf filenhsn updates healthcare ... summer of 2016, and the new...
TRANSCRIPT

January 21, 2016
NHSN Updates
Healthcare Associated Infection and Antimicrobial Resistance Unit

Reminder! Data for CMS Quality Reporting Programs due Soon
WHO: Acute care hospitals that participate in the CMS Hospital Inpatient Quality Reporting (IQR) Program:
WHEN: Quarter 3 (July 1 – September 30) data must be entered into NHSN by February 15, 2016
WHAT data is due:
CLABSI and CAUTI data All ICU locations, Adult and pediatric medical, surgical, and medical/surgical wards
Inpatient COLO and HYST SSI data
MRSA Bacteremia and C. difficile LabID Events (all healthcare onset and community onset) FacWideIN,ED, and 24-hour observation locations
Please note that February 15th is a federal holiday and the NHSN Help Desk will not be available.

CMS reporting requirements starting January 1, 2016
Reporting Requirements and Deadlines in NHSN per CMS Current Rules:
http://www.cdc.gov/nhsn/PDFs/CMS/CMS-Reporting-Requirements-Deadlines.pdf.
Healthcare Facility HAI Reporting Requirements to CMS via NHSN - Current and Proposed Requirements:
http://www.cdc.gov/nhsn/PDFs/CMS/CMS-Reporting-Requirements.pdf .

Patient Safety Protocols for 2016 NHSN v8.5 (January 2016)
Not as many changes this year!
Protocols have been posted to the NHSN website. The individual protocols are located on the site of the specific infection type (e.g., BSI protocol found under “Protocols” on the BSI surveillance webpage).
The major changes to the protocols are listed in the Release Notes found at: http://www.cdc.gov/nhsn/pdfs/commup/nhsn-psc-manual-revisions_2016.xlsx
These protocols should be used beginning on January 1, 2016for data collected in 2016.

Changes to the Patient Safety Component Protocol
LabID Event Reporting
Two questions were changed from “Optional” to “Required” on the LabIDEvent screen .
The questions are “Last physical overnight location of patient immediately prior to arrival into facility” and “Has the patient been discharged from another facility in the past 4 weeks?”
Note: If collection of the data is too burdensome, use of the response option “Unknown”.

Changes to the Patient Safety Component Protocol
Surgical Site Infections
ICD-10 PCS and CPT transition
ICD-9 CM procedure codes have been transitioned to ICD-10 PCS and CPT procedure codes in the NHSN application for procedures dated January 1, 2016 and going forward.
For ICD-10 PCS and CPT, the current ICD-9 CM rules for HPRO/KPRO partials and revisions have been temporarily relaxed. And, KPRO/HPRO have supplemental ICD-10 PCS codes to help clarify revisions.
Users will need to refer to the guidance for specific instructions to correctly input this data. http://www.cdc.gov/nhsn/acute-care-hospital/ssi/index.html
Changes to the Patient Safety Component Protocol
Healthcare associated infections (HAI) and Present on Admission (POA) Worksheet Generator Release Delayed
The Generator is designed to identify the:
• 7-day Infection Window Period
• Date of Event and POA or HAI determination
• 14-day Repeat Infection Timeframe (RIT)
• Secondary Bloodstream Infection Attribution Period
This has been delayed due to compliance requirements
Changes to the Patient Safety Component Protocol
UTI Defect is Fixed
In 2015, a data entry defect did not allow entry of the symptoms of urinary urgency, frequency, or dysuria when an indwelling urinary catheter was indicated to be “INPLACE”, meaning that it was in place > 2 days and present on the date of event.
Now when you select “urgency”, “frequency”, and “dysuria” a popup message warning will indicate these risk factors should only be selected if the urinary catheter was not in place at the time of the symptom. Justification – “if the catheter was removed on the date of event, it was still in place for some time, and therefore InPLACE will be selected.
Now users may select “urgency”, and/or “frequency”, and/or “dysuria”, if the catheter had been removed before the symptom occurred”.

National Risk Adjustment of HAI Data
CDC will update the risk-adjustment of HAI data using the event and denominator data reported to NHSN for 2015 –referred to as the “Re-baseline” of HAI data.
The final analyses of 2015 data will occur in the summer of 2016, and the new risk-adjustment and SIRs will be available in NHSN in December 2016/January 2017.

SIR Calculations until the re-baselining
To accommodate the CAUTI definition change until the re-baselining occurs at the end of 2016, you can customize CAUTI TAP reports using an SIR goal that closely represents or is below the current national CAUTI SIR.
The preliminary estimate of the national CAUTI SIR from the first two quarters of CY2015 is 0.55. Based on available national data, the CDC recommends using a customized SIR goal of less than or equal to 0.55 for the 2015 CAUTI TAP Reports.
2015 CAUTI Definition Changed and impacted SIRS and Rates
Details regarding the use of the re-baselined SIRs for CMS programs (e.g., Hospital Value Based Purchasing) can be found in the Final Rule, as published in the Federal Register on August 17, 2015:
http://www.gpo.gov/fdsys/pkg/FR-2015-08-17/pdf/2015-19049.pdf
2015 Patient Safety Annual Facility Survey
NHSN will release the annual patient safety facility survey in early 2016. This mandatory survey is completed by all facilities enrolled in NHSN to provide updated information on hospital characteristics and practices.
NHSN has created a short, 5-minute Quick Learn video (formerly known as NHSN Hot Topics) that provides updates regarding all of the changes made to the 2015 Patient Safety Annual Facility Survey. http://www.cdc.gov/nhsn/training/
Please remember, surveys must be completed and submitted in NHSN by March 1, 2016. Facilities that do not meet this deadline will be unable to complete monthly reporting plans.

2015 Patient Safety Annual Facility Survey
NHSN Annual Hospital Survey: Antimicrobial Stewardship Questions (Q23-34) are aligned with the CDC’s Core Elements of Hospital Antibiotic Stewardship Programs
http://www.cdc.gov/getsmart/healthcare/implementation/core-elements.html
Data from the 2014 NHSN Annual Survey showed 21.2% of hospitals in Minnesota had antibiotic stewardship programs that incorporated ALL of the core elements

7 Core Elements
1. Leadership Commitment: Dedicate necessary human, financial, and IT resources.
2. Accountability: Appoint a single leader responsible for program outcomes. Physicians have proven successful in this role
3. Drug Expertise: Appoint a single pharmacist leader to support improved prescribing.
4. Act-Take at least one prescribing improvement action
5. Track: Monitor prescribing and antibiotic resistance patterns
6. Report: Regularly Report to staff prescribing and resistance patterns and steps to improve
7. Educate: Offer education about antibiotic resistance and improving prescribing practices

2014 Patient Safety Annual Facility Survey
MN

2014 Patient Safety Annual Facility Survey
MN

Core Elements of Hospital Antibiotic Stewardship Programs
Checklist for Core Elements of Hospital Antibiotic Stewardship Programs
http://www.cdc.gov/getsmart/healthcare/implementation/checklist.html

Minnesota Performance in CMS Incentive Programs NHSN User GroupJanuary 21, 2016

Objectives• Identify current performance of Minnesota
hospitals on value-based purchasing (VBP), hospital acquired conditions (HAC) and Readmission Reduction Program
• Share resources for CMS incentive programs and Minnesota measures

Value-Based Purchasing

VBP Fact Sheet
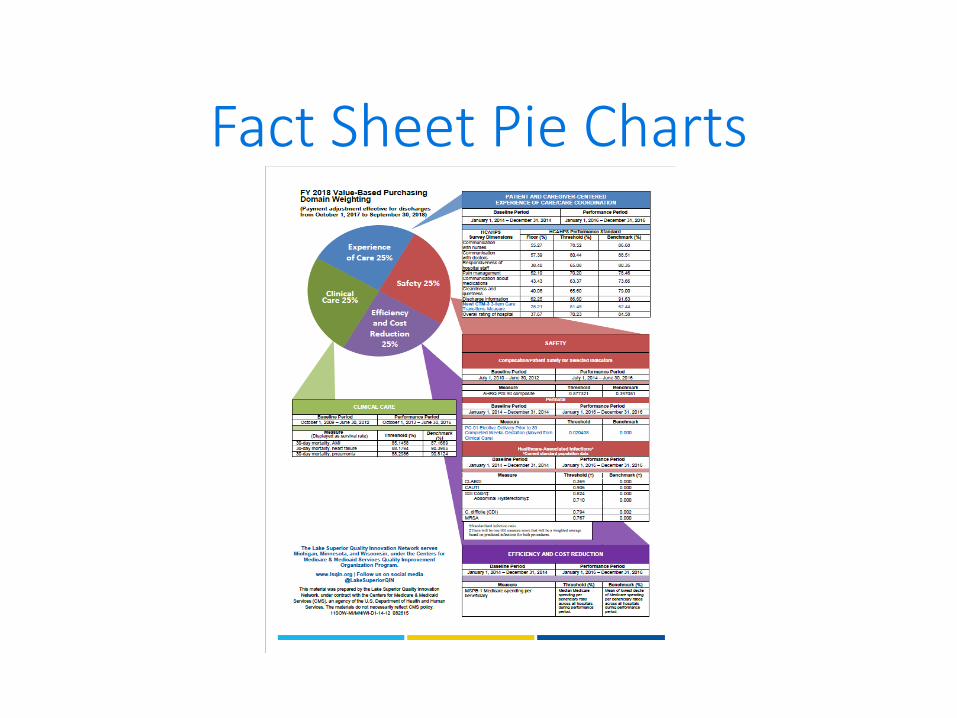
Fact Sheet Pie Charts

How to think about the years
Baseline period
Performance Period
Fiscal Year adjustment factor
2014
2016
FY2018
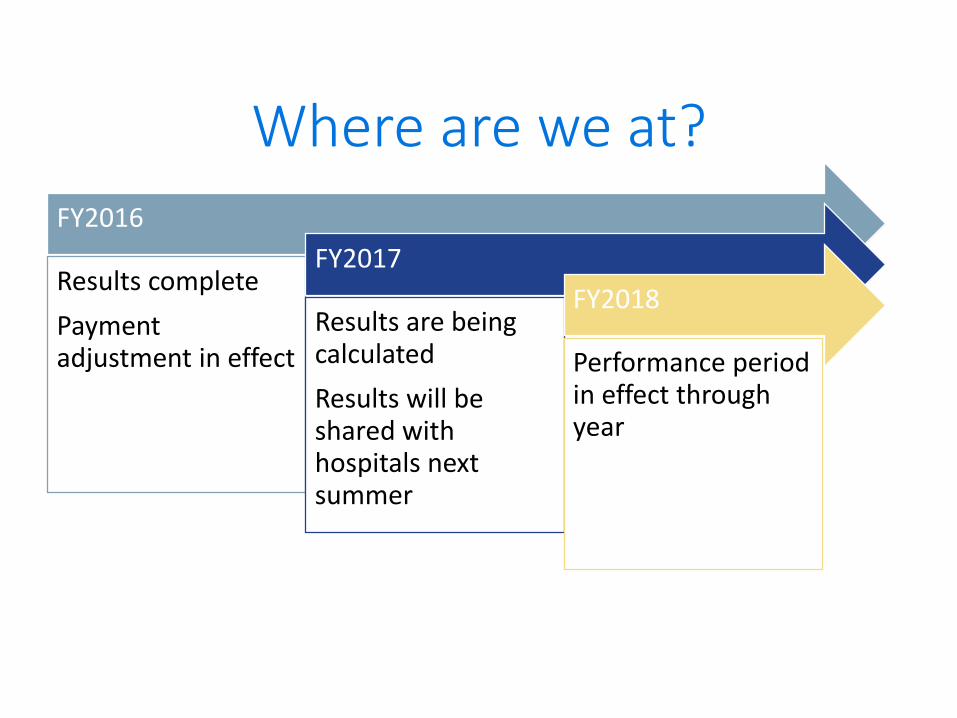
Where are we at?
FY2016
Results complete
Payment adjustment in effect
FY2017
Results are being calculated
Results will be shared with hospitals next summer
FY2018
Performance period in effect through year
VBP Facts
• Now withhold is two percento Could get some or all of it back
o Could get more than two percent back
o Could get a penalty
• Need to have enough cases to get a measure score
• If you don’t have enough cases, other measures count more
• If you don’t have enough measures in a domain, then other domains count more
• Payment adjustment impacts all Medicare billing
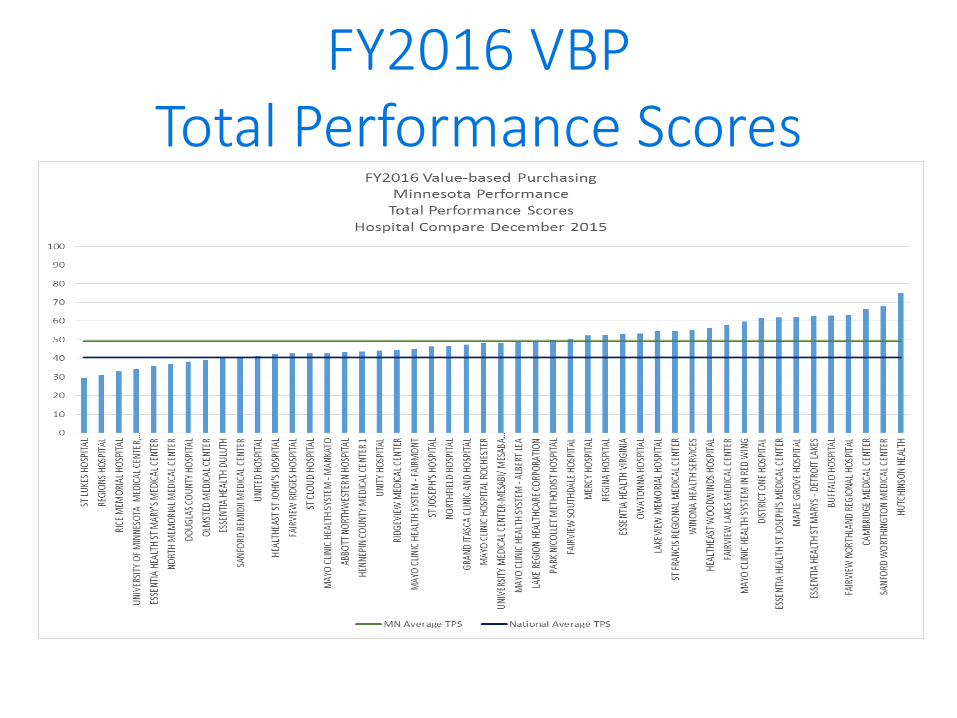
FY2016 VBP Total Performance Scores

FY2016 VBP Total Performance Scores
Range = 0 - 98.33333
FY2016 Results• Overall MN hospitals have improved every
year
• Both SSIs and CAUTI are our lowest performing measures
• Other improvement priorities are HCAHPS pain management and the new (to VBP) Care Transition Measure
• Medicare Spending per Beneficiary is also of interest to hospitals in our advisory group
• Five hospitals received a penalty
FY2018 & FY2019• HCAHPS Care Transition measure is new this
year
• Hip/Knee complications will be added in next year
• Pediatric and adult medical ward locations will be included beginning with FY2019 results

Hospital-Acquired Condition
Reduction Program
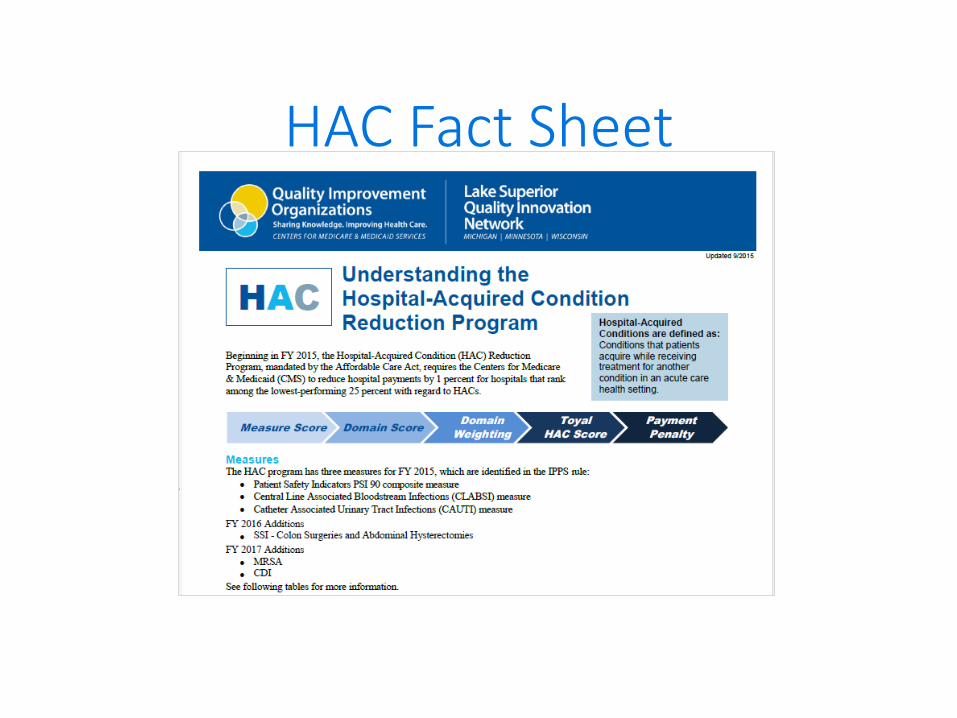
HAC Fact Sheet

HAC Facts• Similar to VBP in how it is organized
• Except there is only a penalty, no incentive payment
• Hospitals in worst quartile will receive a one percent penalty
• New standard population will be used in FY2018 results
• Pediatric and adult medical ward locations will be included beginning with FY2018 results

HAC Facts• SSI Colon and SSI Hysterectomy get one SIR
rate
• If there are not enough predicted cases to calculate a SIR, then other measures will count more
• If no measures in domain, then other domain will determine the HAC score

FY2016 HAC Program

FY2016 Results• 49 Minnesota hospitals were eligible
• Seventeen hospitals received a penalty
• CAUTI and SSI scores were the challenging measures

Readmission Reduction Program

RRP Fact Sheet

Readmission Reduction Program Facts
• Five Clinical Conditions
AMI
Heart Failure
Pneumonia
Hip/Knee
COPD
• Now up to three percent penalty
• Twelve PPS hospitals had no penalty, 40 had some penalty

Excess ReadmissionsAMI
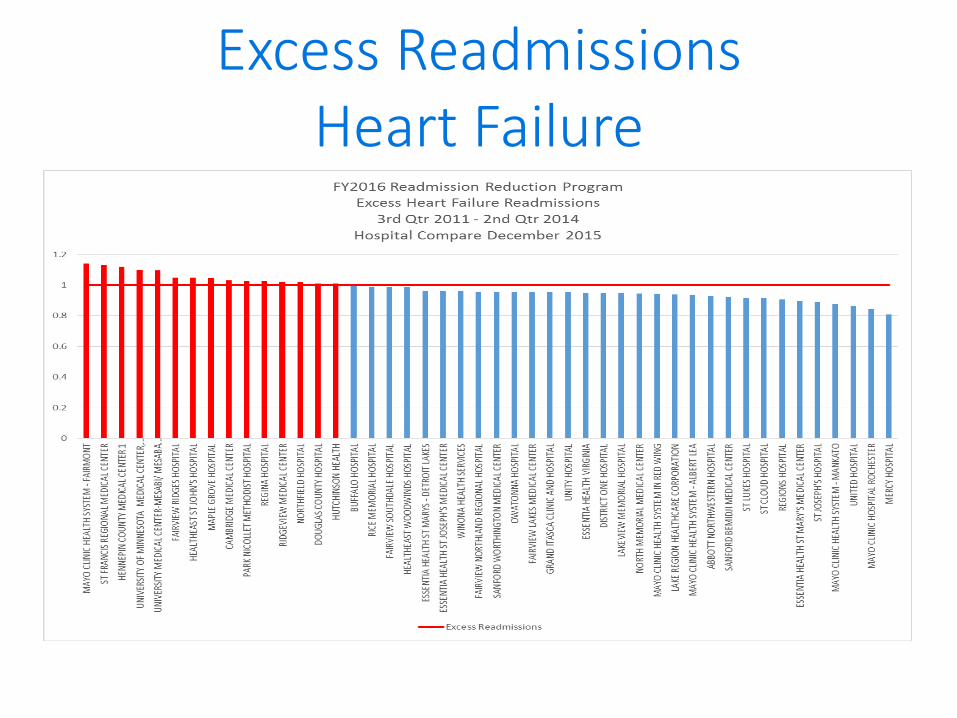
Excess ReadmissionsHeart Failure

Excess ReadmissionsPneumonia

Excess Readmissions COPD

Excess ReadmissionsHip and Knee

Statewide Quality Reporting and Measurement System
(SQRMS)
Minnesota Hospital Measures
Data Submission of VBP, RRP and HAC results
Results in summer
Final results in October
Hospital Compare in December
Required for MN in January
45
Hospital Slate of Measures
46
Additional Measures
for MN
Value- Based Purchasing
(VBP) Program
Readmission Reduction
(RRP)Program
Hospital Acquired
Condition (HAC)Program
Medicare Beneficiary
Quality Improvement
Program (MBQIP)CAH Hospitals
PPS Hospitals

Annual Measure Summary
Questions?Vicki Tang Olson, RN, MS
Program Manager
952-853-8554

This material was prepared by Lake Superior Quality
Innovation Network, under contract with the Centers for
Medicare & Medicaid Services (CMS), an agency of the
U.S. Department of Health and Human Services. The
materials do not necessarily reflect CMS policy.
11SOW-MN-D1-16-04 012016
Healthcare Personnel Influenza VaccinationNHSN Users groupJanuary 21, 2016

51
Objectives
• Understand current requirements for reporting Heathcare Personnel Influenza vaccination in critical access hospitals
• Identify resources for HCP reporting and improvement

52
Reporting Requirements

53
HCP Reporting
• For PPS hospitals, it is a requirement of the inpatient and outpatient reporting programs
• For Critical Access Hospitals (CAH), they have voluntarily signed up for the national Medicare Beneficiary Quality Improvement Program. This program has an annual cycle of September-August. This measure was added to MBQIP in September 2015
• For CAH, this measure is required for SQRMS
54
Improvement Support
“MBQIP Update and the Healthcare Personnel Influenza Reporting” conference callOctober 15, 2016
Robyn Carlson, Stratis HealthJennifer Health, Minnesota Department of HealthVicki Tang Olson, Stratis Health http://www.stratishealth.org/events/recorded.html

55
Improvement Support
SAFER Care virtual event for Critical Access Hospitals on November 18, 2015“Strategies to Improve Health Care Personnel Immunization Rates”
Denise Dunn, RN, MPHSupervisor, Vaccine Preventable Disease SectionMinnesota Department of Health

56
Improvement Support
• At November 18th webinar, also rolled out plan to have monthly data collection faxed to Stratis Health
• First submission was in December 2015 for months of October and November
• 32 CAH are participating and have received a blinded graph of comparison results
• We have just passed the deadline for the second month of data submission

57
Comparison Graphs
Six graphs• Three for percent completion for each of the three
groups• Three for percent for breakdown of immunizations
categories for each group

58
Percent Vaccinated
59
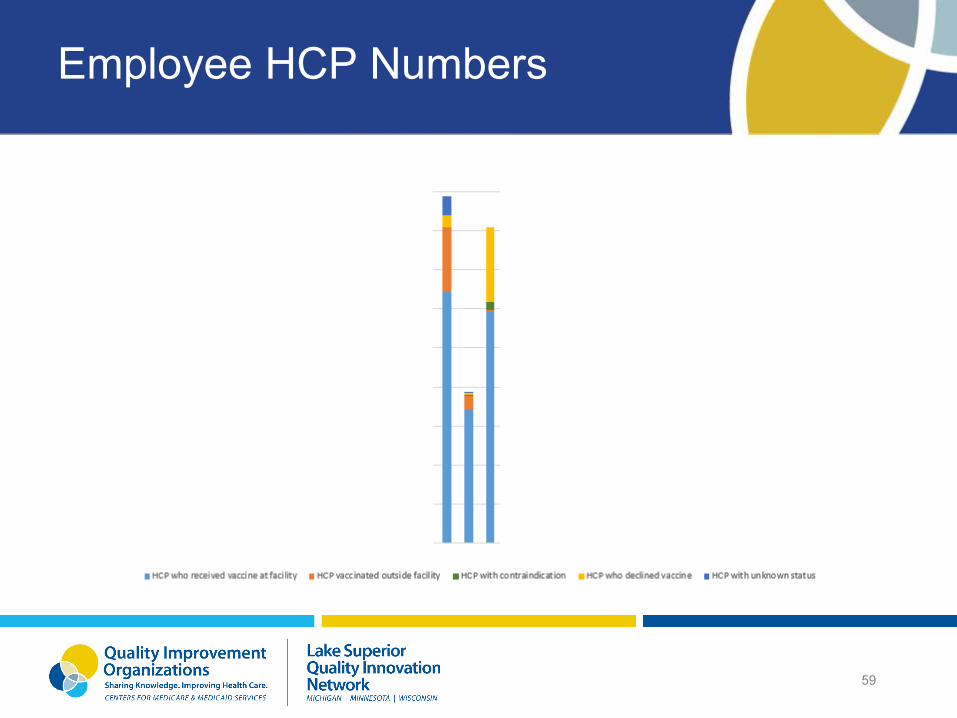
Employee HCP Numbers

60
Q & A
61
Who to Count
• What about a contract service provider such as Access RN who places PICC lines?
• Where are ED Locum Tenens included in data? • We have physician specialists that are contracted; however, they
are not paid by our facility. They bill for themselves. Would they fall under this measure?
• What about healthcare professionals that practice in a specialty clinic that is connected to the hospital, but operate under a different CCN number and are not paid by our hospital payroll? This would include physicians, RNs, med assistants, etc.

62
Who to Count
We have an attached clinic to our facility. Does that staff count in the denominator? Healthcare personnel working in inpatient or outpatient units of your critical access hospital which share the exact same CMS Certification Number (CCN) as the hospital should be included in your HCP influenza vaccination summary data reports. Assuming that this clinic does not have the same CCN as your facility and/or is not considered a unit of the hospital, you would not count individuals working in this attached clinic unless these individuals also physically work in the critical access hospital for one day or more from October 1 through March 31 and meet the definitions of one of the required denominator categories (employees, licensed independent practitioners, and adult students/trainees and volunteers).

63
Who to Count
David mentioned registering satellite clinics, but the previous speaker said not to count LIPs who work only in outpatient satellite clinics. So which is it? Healthcare personnel working in inpatient or outpatient units of your critical access hospital which share the exact same CMS Certification Number (CCN) as the hospital should be included in your HCP influenza vaccination summary data reports. As noted above, an outpatient physician clinic would not meet these criteria. Outpatient satellite physician clinics should not be included in your CAH healthcare personnel influenza vaccination summary counts unless the healthcare personnel in these clinics also physically work in the CAH for one day or more from October 1 through March 31 and meet NHSN protocol definitions for an employee, licensed independent practitioner, or adult student/trainee or volunteer.
64
Who to Count
If an off campus clinic has a different CCN and an employee only comes on hospital campus for meetings, are they still included in the numerator and denominator? If the healthcare personnel are physically present in the CAH during the reporting period of October 1 through March 31 to fulfill official work duties, then you would include these individuals in your numerator and denominator. Work-related meetings, including checking in to receive a work schedule, are considered official work duties; therefore, you would include these employees in the numerator and denominator if they physically enter an inpatient or outpatient unit of the CAH that is included in NHSN reporting for the meetings.

65
Who to Count
If we have an attached Long term care facility that is separate from our CAH, do we include those employees? You would not include the employees of the long term care facility in your CAH counts, unless these employees also physically work for one day or more in the CAH from October 1 through March 31.


This material was prepared by Lake Superior QualityInnovation Network, under contract with the Centersfor Medicare & Medicaid Services (CMS), an agency ofthe U.S. Department of Health and Human Services.The materials do not necessarily reflect CMS policy.11SOW-MN-C1-16-06 012016
2’ BSI Case Studies
Lisa Hesse MLS CIC
Case Study Coordinator

Primary (1’) BSI
Not related to an infection at another site
Secondary (2’) BSI
Associated with an infection at another site
◦ Associated infection must meet NHSN definition
◦ At least one matching organism OR blood culture used to meet criteria for infection
◦ Date of event is date of event of associated infection
◦ BSI falls within attribution period for infection [infection window + Repeat Infection Timeframe (RIT)]
◦ 2’ BSI does NOT have an RIT
Secondary BSI
2’ BSI does not have RIT
CLABSI is never 2’ BSI

Scenario 1a
On day 13 of admission, patient has positive urine culture growing >100,000 cfu/ml E coli and suprapubic tenderness
On day 18, patient has a positive blood culture growing E coli


Scenario 1a
UTI?
1’ or 2’ Blood culture?
Date of event?

SUTI 1b E coli
2’ BC E coli
X

Scenario 1b
On day 13 of admission, patient has positive urine culture growing >100,000 cfu/ml E coli and >100,000 cfu/ml C. glabrata and has suprapubic tenderness-meets SUTI criteria for E coli, candidaexcluded
On day 18, blood culture grows C glabrataand S aureus.


Scenario 1b
Is there a UTI?
Is there a BSI? 1’ or 2’?
What is reported?

X SUTI 1b E coli
X LCBI C glabrata and S aureus
Scenario 1b
Is there a UTI?
Is there a BSI? 1’ or 2’?
What is reported?
◦ SUTI, DOE day 13
◦ LCBI, C glabrata and S aureus
◦ DOE day 18

Scenario 2
Positive BC on day 8 of admit, E coli
Fever day 8-12
Positive urine culture day 11, >100,cfu/ml
E coli and >100,000cfu/ml S aureus

Scenario 2
Is there a UTI?
DOE?
Is there a BSI?
1’ or 2’?
What is reported?

X SUTI 1b E coli and S aureus, 2’ BSI E coli

Scenario 2
Is there a UTI?
DOE?
Is there a BSI?
1’ or 2’?
What is reported?
◦ SUTI 1b, E coli and S aureus, secondary BSI E coli, date of event day 8

Scenario 2 cont
BC on day 20 positive for S aureus
1’ or 2’ or not reported?


Scenario 2 cont,
2’ BSI, within attribution period (infection
window + RIT)
DOE day 8

Questions?
