nhs rotherham ccg governing body – september 2015 chief
TRANSCRIPT

Page 1 of 2
NHS Rotherham CCG Governing Body – September 2015 CHIEF OFFICER’S REPORT
Lead Director: Chris Edwards Lead Officer: n/a
Job Title: CCG Chief Officer Job Title: n/a
Purpose This report informs the Governing Body about national/local developments in the past month.
Reselection of Strategic Clinical Executive (SCE) Members Following interviews held last month Dr Kitlowski & Dr Brynes have been reselected for a further 4 years. Two New Members of the Governing Body This month welcomes two new members to the Governing Body: • Dr Robin Carlisle who is the Lay Member with a lead role for overseeing Primary Care. His focus will
be strategic and impartial, providing an external view of the work of the CCG that is removed from day-to-day running of the organisation.
• Dr Jason Page who will share responsibility with other members of the Governing Body for all aspects of the Governing Body’s business. In addition Dr Page will bring a broader view of health and care issues to underpin the work of the group. In particular, he will bring to the Governing Body specific understanding of patient care/engagement in the primary care setting in Rotherham.
Each member of the Governing Body shares the responsibility as part of a team to ensure that the Group exercises its functions effectively, efficiently and economically, with good governance and in accordance with the terms of this constitution. Each brings their unique perspective, informed by their expertise and experience. I welcome both new members to the Governing Body. Yorkshire & Humber Academic Health Science Network Annual Report and Business Plan Attached are updates from the Yorkshire & Humber Academic Health Science Network, including a link to their Business Plan and Annual Report.
Appendix(1)
The future of the Academic Health Science Networks (AHSNs) Following Ed Smith’s (Deputy Chair NHS England) review with reference to Leadership Development and Improvement. The following links give details of the findings and next steps: Joint statement from the Yorkshire & Humber AHSN and Yorkshire & Humber SCN Joint statement from Dr David Black and Professor Graham Venables Introduction by Ed Smith to the Improvement and Development Leadership Review The Improvement and Development Leadership Review Update for Staff & Partners following the Improvement and Development Leadership Review Assurance Operating Manual NHS England has published the CCG Assurance Operating Manual, including details of the new special measures regime and a CCG quarterly self-certification for delegated functions. Queries can be directed to NHS England regional teams in the first instance or by emailing [email protected] CCG Assurance: Delegated Functions Self-Certification 2015/16 The CCG Assurance Framework for 2015 /16 sets out a new assurance process that takes account of the need for NHS England to have specific additional assurances from CCGs who have taken responsibility for the commissioning of primary medical care services under delegated authority (‘Delegated Functions’) or a joint commissioning arrangement with NHS England. The Governing Body are asked to agree the attached assurance document on delegated commissioning of Primary care which will be required to be submitted to NHS on a quarterly basis. The Chief Officer and Chair of the Audit Committee are asked to sign on the CCGs behalf.
Appendix(2)

Page 2 of 2
Dame Barbara Hakin, NHS England Letter to all CCGs - Assurance required NHS England has requested assurance from all CCGs that appropriate systems and processes are in place to ensure that conflicts of interest or potential conflicts of interest are declared and mitigated. Rotherham CCG has responded to the request
Appendix(3)
Amendments to The NHS Constitution It was first published in March 2012 and is due to be refreshed fully in March 2023. However the Constitution was updated in July 2015; this paper notes those changes.
Appendix(4)
Communications Update • Pulse magazine are publishing a feature on Personal Health Budgets following a Freedom of
Information request in August. A media statement, from Sue Cassin, was been provided to Pulse on behalf of NHS Rotherham CCG
• There has been significant local and regional media interest in the first anniversary of the Alexis Jay Report into Child Sexual Exploitation in Rotherham. The main focus of media interest is on the police and local authority services.
• An Emergency Centre website has been developed and will be launched to the public in early September. The web link when the site is live will be www.rotherhamemergencycentre.nhs.uk
Recommendation The Governing Body is asked to note the Chief Officer’s Report and agree the assurance document on delegated commissioning of Primary Care.

ANNUAL REPORT2014/15

Testimonials 3
Chairman’s Foreward 5
Managing Director’s Foreward 6
Strategic Overview 7
Developing the Ecosystem 8
Delivering patient and population benefits 10
Delivering efficiency and supporting enterprise 14
Our Work Revisited: Patient Falls 18
Our Work Revisited: Workplace Wellness 20
Our Work Revisited: PADs 22
Financial Report 24
Matrix of Metrics 2015 26
Registered Directors: Biographies 30
Content
Look out for factsand figuresrelating to ourImprovementAcademy

3
TestimonialsWe have been delighted with the work we have been
doing with the Yorkshire & Humber AHSN Improvement
Academy on safety huddles. The whole ward team have
really embraced the safety huddle concept. We have
reached the milestone of 30 days without a fall today,
which given the history of falls on this ward is really
significant. We don’t often get a chance to say ‘Well done!’
Dr Alan Hart-Thomas, Clinical Director,
Calderdale & Huddersfield NHS Trust
The Y&H AHSN has provided invaluable
support through provision of industry
expertise, contacts and resources. This has
enabled the comprehensive testing and roll-
out of our highly efficacious staff wellbeing
service, which simply would not have been
possible for a higher education institution, thus
benefiting both the NHS and the university.
This support is enabling the programme to
progress into a viable business proposition.
Professor Ian Maynard, PhD, C.Psychol,
F.BASES, F.AASP
Input from the Yorkshire Y&H AHSN had been
pivotal in allowing Selex to get the programme
underway by demonstrating a commitment from
the AHSN to the work that communicated the
importance of the collaboration with Selex to the
larger Selex corporate body. CFHealthHub has
the potential to empower young people with
cystic fibrosis to manage their own care and we
hope that this will improve quality as well as
duration of life at the same time as enabling
significant cost savings across CF care.
Dr Martin Wildman, MSc, PhD, MRCP
Honorary Senior Clinical Lecturer
Health Services Research, ScHARR,
University of Sheffield
.
“
“
“ “
“
“
4
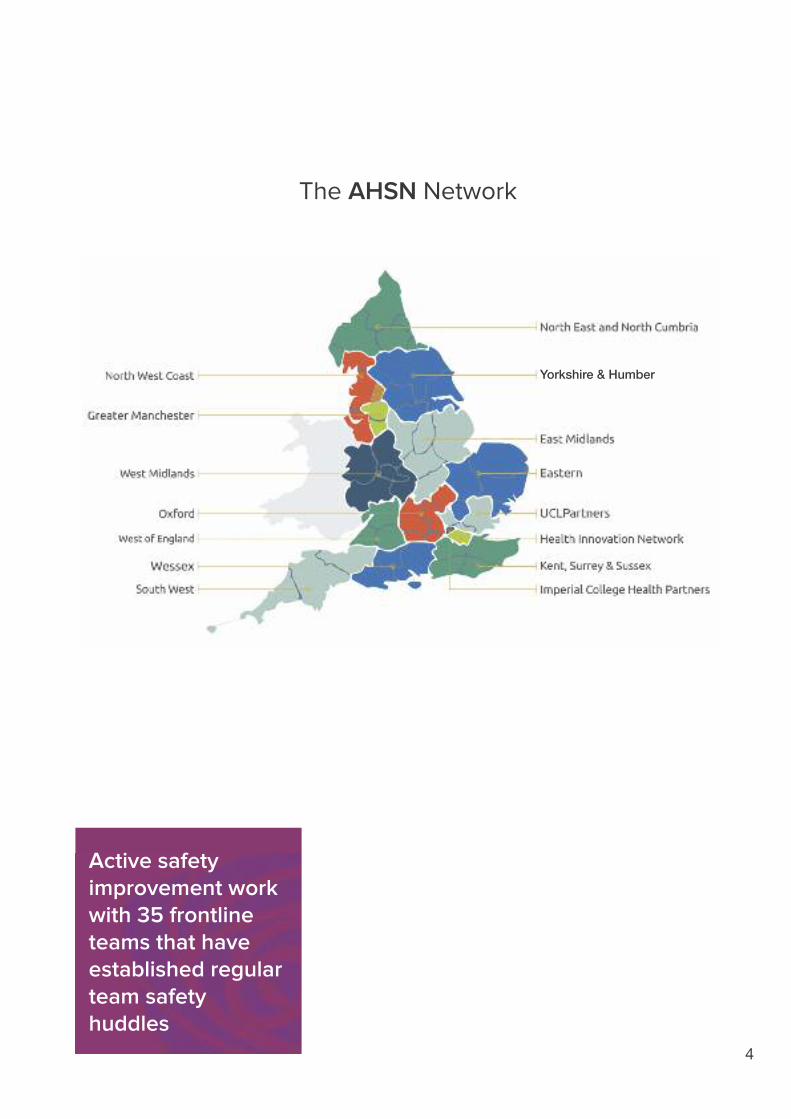
Active safetyimprovement workwith 35 frontlineteams that haveestablished regularteam safetyhuddles
Yorkshire & Humber
The AHSN Network

5
Chairman’s Foreward
At the beginning of the year leading into 2014/15 the Yorkshire & Humber
Academic Health Science Network (AHSN) was initially hosted by Sheffield
Teaching Hospitals NHS Foundation Trust, for which we are very grateful.
During the year, with the unanimous support of the interim steering group, the
AHSN became a Company Limited by Guarantee (CLG), appointed four
registered directors and established an accountable and strategic Board of
Directors, which ratified the CLG decision. The Board, having run extensive and
intensive competitions, then appointed Andrew Riley as its first Managing
Director and subsequently as its first executive directors Richard Stubbs, Dawn
Lawson and Sally-Anne Naunton. Governance and set-up of the CLG continued
at pace during 2014/15, with the subsequent appointment by the Board of
accountants, auditors and lawyers for the business.
The Managing Director has gone on to fully embed and establish the talented
senior management team that has delivered a broad and complex programme
through year one. It was pleasing to note the unqualified positive opinion of
NHS England for the quarter four and year-end quality assurance rating. The
production of the business plan for 2015/16 evolved from the lessons learned
throughout the year, and the canvassing of stakeholders through regionally held
stakeholder events, and hence reflects the support our members have told us
that they need from the AHSN to deliver their complex agendas.
The AHSN is pleased to have developed good and trusting partnerships with its
key stakeholders, in particular with the Strategic Clinical Network (SCN), with
whom integrated plans have been developed. We have also worked closely
with Medilink and Medipex who have supported our economic growth agenda,
Bradford Teaching Hospitals who host our (now) nationally recognised AHSN
Improvement Academy, and Sheffield Hallam University who are key strategic
partners in delivering the workplace wellness programme that has also been so
well received at national level.
We have been delighted to host a number of visits from key national and
international leaders and to form new and exciting relationships with
complementary organisations around the world, with the support of UKTI,
Healthcare UK, BIS and the Office of Life Sciences.
The challenge for 2015/16 is going to be maintaining and stepping up delivery of
the business plan and key objectives and evidencing the impact we are making
for patients, but based on this year I am excited and encouraged by the
prospects for the coming year.
I would like to express thanks to all our stakeholders, employees and Board
members for their support, commitment and hard work during the last year and look
forward to great outcomes this year from the work and plans which are in train.
Professor William Pope
Chairman
Y&H AHSN

6
The AHSN has, in its first year of operation, made considerable progress in
delivering its five-year objectives of contributing to the improvement in public
health, improving health service delivery and its cost-effectiveness and supporting
both regional and national economic growth. My executive director team and I
have developed our capacity and capability over the year and recruited some very
experienced leaders to deliver the exciting agenda which has been recognised by
NHS England through the quarterly review feedback we have received.
Although the AHSN is now a CLG with the benefits this brings, it remains firmly
positioned as a member organisation completely subscribing to NHS values and
with a clear focus on supporting members in improving patient outcomes and
experience.
At the outset, we identified how important achieving sustainable behaviour
change was and the need to create improvement capacity and capability locally.
We established our Improvement Academy and over 150 frontline improvement fellows embedded in member
organisations are now leading complex improvement programmes.
As an organisation working mainly through networks and across systems, developing strong partnerships with
public and private organisations has been an essential feature of the year. There is still uncertainty about the
configuration of the ‘improvement tier’ at regional level, with discussions currently taking place on the future roles
and configuration of Strategic Clinical Networks, Clinical Senates, NHS Leadership, NHSIQ and AHSNs. So we
have worked closely with the senior team at the SCN to ensure we have complementary plans that will enable
integration whatever the final decisions on future configuration might be. The key thing is not to pause
implementation and delivery.
We have had some important successes in our first year that have made a significant impact, and you will find some
of the highlights in this report, but specifically our key successes have been our workplace wellness programme,
establishing our Improvement Academy, re-launching the regional NHS CEO meetings, and working with Yorkshire
& Humber Medlink and Medipex to establish a well respected small-medium enterprise (SME) programme.
Just as important as delivery is ensuring that the work we undertake is both evidence based and its impact is
thoroughly and independently evaluated. To this end we have developed very important strategic partnerships
with both York Health Economics Consortium (YHEC) and the School of Health and Related Research (ScHARR) at
the University of Sheffield, which are supporting our evaluation programme and providing valuable health
economics advice for the start-up companies with which we are working.
We have used our NHS England core income to leverage matched funding through both membership income and
very importantly also from other external funding sources. In total, including additional funds secured by our
Improvement Academy, we generated more than £1.7 million of matched funding in the year which represents over
50% of our NHS income against a target of 20%.
Although we have achieved a lot in this, our first year of operation as a CLG, we have also learned a lot too.
Particularly ensuring that our future plans are carefully aligned to those of our members and key stakeholders such
as NHS England, UKTI, Healthcare UK, BIS and OLS. Our plan for 2015/16 reflects the many discussions and
outcomes from planning events we held across the region, and whilst it remains a broad and ambitious
programme, we are confident that it reflects the needs of our members’ as articulated to us, and that we are
building the infrastructure (in both our members organisations and in the senior central leadership) needed to
deliver it. We also realise that we need to be better at communicating what we are achieving and have recently
expanded our communications team to enable this.
In conclusion, our first full year as a CLG has been eventful, we have grown as an organisation and learned a lot. I believe
that we are now very well positioned to continue adding value and having an impact as a trusted regional organisation
helping our members lead the significant delivery and change agenda facing the NHS over the next five years.
Andrew Riley
Managing Director
Y&H AHSN
Managing Director’s Foreward

OverviewOur strategic priorities asan remain focussed onthree core objectives:
• Improving Population Health
• Improving Healthcare
• Generating Economic Growth
In October 2014, NHS England released a five-year strategy
document, The Five Year Forward View, with significant implications
for the NHS, establishing Vanguards, Test Beds and new models of
care that are being supported by AHSN.
We have aligned our 2015/16 business plan to reflect the priority
areas of the Five Year Forward View.
Throughout the year we have worked hard to ensure that we
understand local needs and priorities. We held three regional
workshops for members and our business plan for 2015/16 reflects
members’ input.
One of the strengths of the AHSN is our ability to work in
partnerships and we have engaged extensively with regional
stakeholders such as the Strategic Clinical Network, Health
Education England Leadership Academy for Yorkshire & Humber,
Public Health England, and National Institute Health Research
Clinical Research Networks.
We have also aligned our programme of work to the needs of our
members and the priorities of other national stakeholders, including
The Office of Life Science, Strategy for UK Life Sciences, UK Trade
and Investment Life Science Organisation Strategy and Healthcare
UK Strategic Business Plan.
We work closely with the Northern AHSNs and the broader AHSN
system to achieve common goals aligning education, clinical
research, informatics, innovation, training and education, and
healthcare delivery. We are working to improve patient and
population health outcomes by translating research into practice,
and developing and implementing integrated healthcare services.
The AHSN is supporting knowledge exchange to build alliances
across internal and external networks and actively share best
practice, and provide for rapid evaluating and early adoption of
new innovations. We are also working with YHEC and ScHARR
who are evaluating the impact of our work.
7

8
Developing the Ecosystem
The past 12 months have been a period of successful
transformation for the AHSN following a successful first
year in operation. Initially hosted by Sheffield Teaching
Hospitals NHS Foundation Trust we became a
Company Limited by Guarantee in February 2014. We
have four Registered Directors, legally responsible for
the lawful transaction of business and to ensure that
the CLG is a going concern. Our Interim Project Board
has been replaced with a Strategic Board that meets
every three months to discuss strategic direction and to
assure delivery of the operational plan. The Board
consists of nominated and invited directors
representing CCGs, NHS, industry, universities,
CLARHC, CLRN, LETB and SCN.
In 2013/14, our first year of existence, we launched a
series of successful programmes, with highlights
being our NHS Staff Workplace Wellness programme,
our Inpatient Falls Reduction programme and the
economic growth programme.
In 2014/15 we have continued to build upon our key
achievements of the previous year, extending
successful programmes and expanding our range of
work into other areas. We have achieved this whilst
simultaneously strengthening the foundations of the
organisation through major works including:
Member and stakeholderengagement We are developing our stakeholder engagement as a
means of describing a broader, more inclusive, and
continuous process between the AHSN and those
potentially impacted by our activities. Although the
Yorkshire & Humber region is geographically
extensive we invest in face-to-face meetings between
member CEOs and partners of the AHSN. We
regularly meet with other stakeholders and business
contacts with the aim of developing a true
understanding of the region and the people within it.
We have recently commenced a programme of
regular updates and newsletters to increase
awareness of our programmes and extend our reach
across the region.
More than 30
partner
organisations are
represented in our
Quality Improvement
Training Advisory
group

9
Expanding our core team During the past 12 months we have recruited to strengthen our delivery capacity, with significant additions to
the programme office and commercial teams. We have ensured we build our work around our expertise of
system leadership, open innovation and international engagement. We have also strengthened our corporate
team to ensure that we have the appropriate support functions to run our business successfully.
Developing the scale of work of our ImprovementAcademyOur Improvement Academy continues to deliver real step changes for our member organisations. The success
of our Inpatient Falls Reduction, Patient Flow, and mortality reduction programmes has been scaled up,
receiving grants from the Health Foundation and others and recognised as national examples of best practice.
The methods used in delivering these programmes have been extended across other areas.
Building key partnerships underpinning our workAs a network it is important that the AHSN builds extensive partnerships with academia, industry, research and
the health sector. These partnerships underpin our work and ensure we can deliver against our strategic
objectives. During the past 12 months we have formed significant partnerships with a number of organisations
including ScHARR, YHEC, Yorkshire & Humber SCN and Yorkshire & Humber Leadership Academy. The
Director of the SCN attended all of the AHSN planning meetings in the year and sits on the AHSN Strategic
Board. The COO from the AHSN is a member of the SCN Board, ensuring understanding and alignment of
key priorities.

Delivering patient andpopulation benefits
Urgent & Emergency Care(UEC)
BackgroundIn 2014, the AHSN commenced work on our urgent and
emergency care project. The project was initiated following
feedback from our members regarding local challenges.
Both CEOs and Chief Accountable Officers formed a consensus
that urgent & emergency care is a critical challenge.
The AHSN was asked to support a project to develop a better
understanding of UEC care demand within the region.
Why is this work important?In addition to being a project that serves the needs of our
members, the UEC care project is supportive of NHS England
and the Five Year Forward View. In the winter of 2014/15
Accident & Emergency Departments suffered from excessive
demands with most organisations falling short of the four hour
wait time target. Our work in this area will support both our local
and national stakeholders as they plan for winter 2015.
Over 800 attendees
at master classes,
workshops and
roundtables held
around Leeds, York,
Sheffield & Hull
10

Our contributionThis project commenced in November 2014 with a
conference that brought clinicians, managers,
commissioners, providers and academics to identify a
better understanding of the system and identity key
challenges.
The project uses a collective, connected and
co-ordinated ‘systems thinking’ approach with experts
in the region participating in four task and finish groups
that will develop resources to;-
• Map the UEC system surrounding pilot CCG areas to
identify flow; demand; misalignment; and system
blockages
• Identify predictors which give a window for
intervention and avoid A&E attendance via practiced
intervention
• Predict tomorrow’s Urgent Emergency Care (UEC)
demand – collect GP practice level data to support
near real-time prediction of UEC demand and
support capacity planning in the acute sector
• Promote UEC access to patient records by bringing
data together for direct patient care and use of the
Frailty Index to better understand patient flow
What’s next? During 2015/16 the AHSN will be confirming up to
three pilot sites and working with them to develop
local project objectives. One of the region’s vanguard
sites has come forward as an initial pilot site to identify
their specific system challenges and solutions. Work
has now begun to tailor the project requirements for
each pilot site area to their local needs.
The outputs from the task and finish groups together
will be brought together in order to generate and
prioritise ideas for testing followed by wider
implementation across the region.
PatientsThe King’s Fund
reported that EmergencyDepartment
attendances reached14.2 million in 2013-2014, a 12% increasefrom 2003-2004.1 2
TargetsThe four hour waittarget is 95%, but
departments struggle tomeet this. The number
of patients waitingbeyond four hours
reached its highest levelof 9% in the final quarter
of 2013/2014.2
BedsEmergency admissions
have increased by 47% over the past
15 years.3
StaffingThe College of
Emergency Medicinereported a less than
50% fill rate into highertraining for the
speciality in 2011-2012.4
11
1 Department of Health (2011) Total time spent in accident and emergency (pre-2011/12 Q2) (online)
2 NHS England (2014) A&E waiting times and activity (online)3 Emergency admissions to hospital: managing the demand. London: NAO, 20134 College of Emergency Medicine. Emergency medicine taskforce interim report. London:
CEM, 2012

12
Delivering patient andpopulation benefits
Patient Flow
BackgroundMeeting daily demand for admissions is a challenge
faced by all NHS organisations with an inpatient bed
base. Hospital trusts experience problems with
patients backing up for admission when the hospital
is ‘full’ and sick patients need to be admitted. Some
of the major reasons why this happens are related to
the ‘flow’ of patients through the hospital.
For example:
1. Most discharges happen in the afternoon or early
evening whilst admissions happen throughout the
day, resulting in patients waiting until the later part of
the day to get a bed.
2. There are a significant proportion of patients who
do not need to be in a bed. Estimates suggest that
this is generally about 30%.
Why is this work important?Patient flow is a priority for many hospitals. Rapid
access to a hospital bed is important for the safety of
sick patients. It is also true that staying longer than
necessary in hospital is not good for patients who may
risk losing confidence or their independence. In
addition, hospitals which do not have effective patient
flow may also have difficulty in meeting the national
four-hour standard for patients waiting in A&E.
Our contributionWe have worked with patient flow experts Operasee
to implement operational management tools ‘Visual
Hospital’ and ‘Plan for every patient’ in Scarborough
Hospital. Building on the learning and our
experience of Calderdale and Huddersfield NHS
Trust, who demonstrated a 30% reduction in length of
stay on medical wards, we have systematically
introduced the same tools into Scarborough Hospital.
Through our Improvement Academy we have
provided:
• Experienced project management to guide and
facilitate Scarborough Hospital in their learning
and in the implementation of patient flow tools.
• The analytical skills to evaluate both the results
and the learning from this project so that other
hospitals can take steps to address their own
patient flow issues.
Mapping a patient’s inpatient journey shows that the
majority of time is spent waiting. This project
demonstrates that when we design processes to
provide what patients need when they need it,
they’re satisfied, and length of stay reduces making
patient flow much easier for us to manage.
Whilst this is still very much work in progress early
length of stay results at Scarborough are very
encouraging and show a result in the order of 20%
reduced length of stay.
44 NHS partner
organisations
visited at top team
level

13
What’s next?The lessons from initial implementation sites will be shared through facilitated and targeted regional
Roundtable and Masterclass events, which will be opened up to interested trusts in the region. Following on
from this we will support wider and sustainable spread through a rigorous and supported Train the Trainer
approach. The exciting synergy with the Patient Safety Collaborative work programme will be fully exploited
to support the implementation and embedding of this approach, to deliver safer and more efficient care, and
to enhance the value of this work programme for member organisations.
“…. unlike previous years, we have been able to review every single patient, every two hours and targetresources appropriately to effect an increased number of discharges.”
Mandy McGale, Director of Operations, Scarborough Hospital

14
Delivering efficiency andsupporting enterprise
Open InnovationProgramme
BackgroundDelivered in partnership with Medilink Yorkshire &
Humber, 2014/15 saw the AHSN work closely with
colleagues from across the region to deliver a
unique Open Innovation programme for regional
SMEs, academics, clinicians and other leading
experts.
The programme was designed to trigger the
development of new projects and consortia
to cultivate new products and meet unmet
clinical needs.
Why is this workimportant?The Open Innovation programme has provided
opportunities for industry to create meaningful
dialogue with the healthcare system to identify
specific clinical needs. This has allowed a demand
pull for innovation to take place, rather than the
traditional supply side push. As a consequence
projects have been developed resulting in new
products, secured funding and a call from both sides
of the relationship to continue this work in 2015/16.
Our ContributionDuring the past 12 months the AHSN has hosted a
series of workshops both nationally and
internationally; highlights of just three of those
programmes are shown:
Workshop 1: Diagnosis of disease,
trauma and pathology of the
gastrointestinal system
Run in June 2014, this workshop was delivered in
partnership with the Colorectal Therapies Healthcare
Technology Cooperative. It brought together
expertise across the region including 20 academics,
12 clinicians and five companies. The outcome was
fantastic and generated 10 new collaborative projects
using innovation in biosensing, nanotechnology,
biomaterials and engineering. The workshop was a
huge success and these projects have gone on to
secure more than £100k of funding to support further
development.Our Open Innovation
Workshop has seen the
development of 24 new
innovations and
generated over £100k
of additional investment
into the region

Workshop 2: Diagnosis and treatment
of wound infection
Workshop 2 was run later in the year and brought
together eight academics, two clinicians and six
companies. This time we partnered with the
WoundTec Healthcare Technology Collaborative to
generate 14 new innovation projects. Projects from
this workshop have generated significant interest
from national partners and at the time of writing we
are awaiting the outcome of several bids that are
expected to generate significant funds to support
continued project development.
UK/China Open Innovation
In 2014, the AHSN worked in partnership with the
University of Bradford’s Health Tech Open Innovation
Team to deliver our inaugural UK/China Open
Innovation Programme. The programme was
delivered in the Chinese province of Guangzhou
during November of 2014, pairing UK SMEs from the
health and care sector with strong partners in China.
This enabled the development and successful
commercialisation (in China and the rest of the world)
of potential and existing health technologies within
the NHS, SMEs and academia. The workshop
focussed on opportunities capable of realising a
commercial return (either through sale or out-
licensing) inside four years. As part of the
programme the UK/China collaboration has secured
more than £850k of funding at the time of writing,
with more expected.
What’s next?The Open Innovation programme continues to
expand: further international partnerships have been
developed with Canada and a second workshop in
China with a focus on Point of Care Diagnostics is
being planned, with up to £2 million of ring-fenced
funding assigned by the Chinese municipal
government for the workshop.
15

16
Over 10 newinternationalcollaborationsgenerating morethan £850k ofinvestment
Delivering efficiency andsupporting enterprise
Industry Engagementand InnovationAdoption
BackgroundThe strength of our industry engagement programme
has been a key part of our success during 2014/15.
Driven by our commercial team, with a remit for
regional economic growth and wealth creation, we
have developed strategic partnerships and delivery
programmes in collaboration with SMEs and
multinational organisations. During 2014/15 we have
met and engaged with over 100 industry
organisations and supported more than half of those
with further development and support.
Why is this work important?The UK has one of the strongest and most productive
life science sectors in the world, generating an
annual turnover of over £50 billion. The sector
comprises nearly 5,000 companies, and employs an
estimated 175,000 people. The NHS benefits greatly
from the groundbreaking innovations that are created
in the sector. Our industry engagement programme
builds stronger relationships between the NHS and
industry resulting in better, more effective solutions
for our patients, as well as safeguarding and creating
life science sector jobs.
Our contributionA diverse range of projects and partnerships have
been created through our Industry Engagement and
Innovation Adoption programme. Our support
includes a variety of solutions, from providing funding
for our members, to supporting their engagement
with industry partners, to forging a network of over
150 innovation scouts, driving innovation within our
member organisations. Detailed are just two of our
many projects within this programme of activity.
Blackbox
The AHSN has developed a commercial partnership
with Yorkshire-based company Blackbox Medical
(BBM). The partnership sees both the AHSN and
BBM financially supporting CCGs to adopt BBM’s
innovative and unique data validation toolkit, which
identifies the level of patient discharge errors
occurring within a practice and the subsequent errors
in SUS episode coding and tariffs. The technology
has been proven to dramatically increase patient
safety whilst providing financial accuracy for NHS
organisations.

17
National Innovation Accelerator
We have continued to support national programmes
aimed at promoting the spread and adoption of
innovation. The NHS National Innovation Accelerator
is one of these and we are one of six AHSNs who are
supporting the programme.
The programme invites healthcare pioneers from
around the world to apply to develop and scale their
tried and tested innovations across the NHS. The
programme focusses on the conditions and cultural
change needed to enable the NHS to adopt
innovations at scale and pace, aiming to improve
outcomes and give patients more equitable access to
the latest products, services and technology.
Whats next?In 2015/16 we have a number of programmes aimed
at further developing our offerings to industry and
building lasting partnerships between the NHS and
Industry to better support patient care, improve NHS
operating efficiency and generate regional and
national growth.
Industry Engagement Portal
This project will see the development of a
comprehensive support programme for UK
businesses and NHS entrepreneurs . It will create a
single point of access to the NHS, and a pipeline of
validated innovation for frontline delivery that creates
growth for UK plc and increases quality in NHS
provision. It will allow for fast, effective engagement
across all sectors, providing information and support
on procurement advice, system education,
consultancy support, signposting, health economics
expertise and market access strategy creation.
Commercial Partnership Programme
The Yorkshire & Humber Commercial Partnership
Programme began in 2014 with engagement with
Black Box Medical. The 2015/16 period will see an
extension of this programme with a core focus on:
• Supporting regional/UK SMEs with improving
market access and increasing sales
• Identifying innovation solutions and enabling the
opportunity for NHS bodies to adopt them
• Generating a commercial return for the AHSN
• Proof of Concept

18
Our work revisited
Reducing InpatientFalls on HospitalWardsBackgroundFalls are a common and serious problem estimated to
cost the NHS more than £2.3 billion per year. 1
The human cost of falling includes distress, pain,
injury, loss of confidence, loss of independence and
mortality. Impact can also be seen on family
members and carers of people who fall.
Inpatient groups who are seen as being at most risk
of falling are:
• All patients aged 65 and older
• Patients aged 50 to 64 who are judged by a
clinician to be at higher risk of falling because of
an underlying condition.
Inpatient falls can lead to hip fractures and other
injuries, whilst even falls without harm can lead to
loss of confidence and increased length of stay.
Through our Improvement Academy, the AHSN is
working with 20 frontline teams across the region to
reduce patient falls. The work has resulted in
impressive results, including:
• Teams achieving a significant reduction in inpatient
falls evidenced by at least one step change
reduction in run charts plotting “falls per week”.
A group of four wards has reduced the combined
average number of falls per week by 60%.
• Sustained periods of time without any falls. One
ward has moved from an average of one fall per
week to repeatedly achieving 30 days between
falls and up to 60 days. .
A preliminary health economics evaluation is showing
this work as providing savings of £185k with costs of
running the programme at £39k. Work to scale this
programme is already underway. In March 2015 a
falls summit in collaboration with three other AHSNs
in the north was held. The event was attended by
over 200 delegates.
Why is this work
important?NHS England has identified the need for harm
reduction associated with falls. The Francis report
highlighted the importance of culture when
addressing the safety of patients.
Among older adults, falls are the leading cause of
both fatal and nonfatal injuries.2
1NICE Falls: Assessment and Prevention of Falls in Older
People (CG161). London: Nice 2013.
www.nice.org.uk/guidance/cg161
2Centers for Disease Control and Prevention, National Center
for Injury Prevention and Control. Web–based Injury Statistics
Query and Reporting System (WISQARS) [online]. Accessed
August 15, 2013
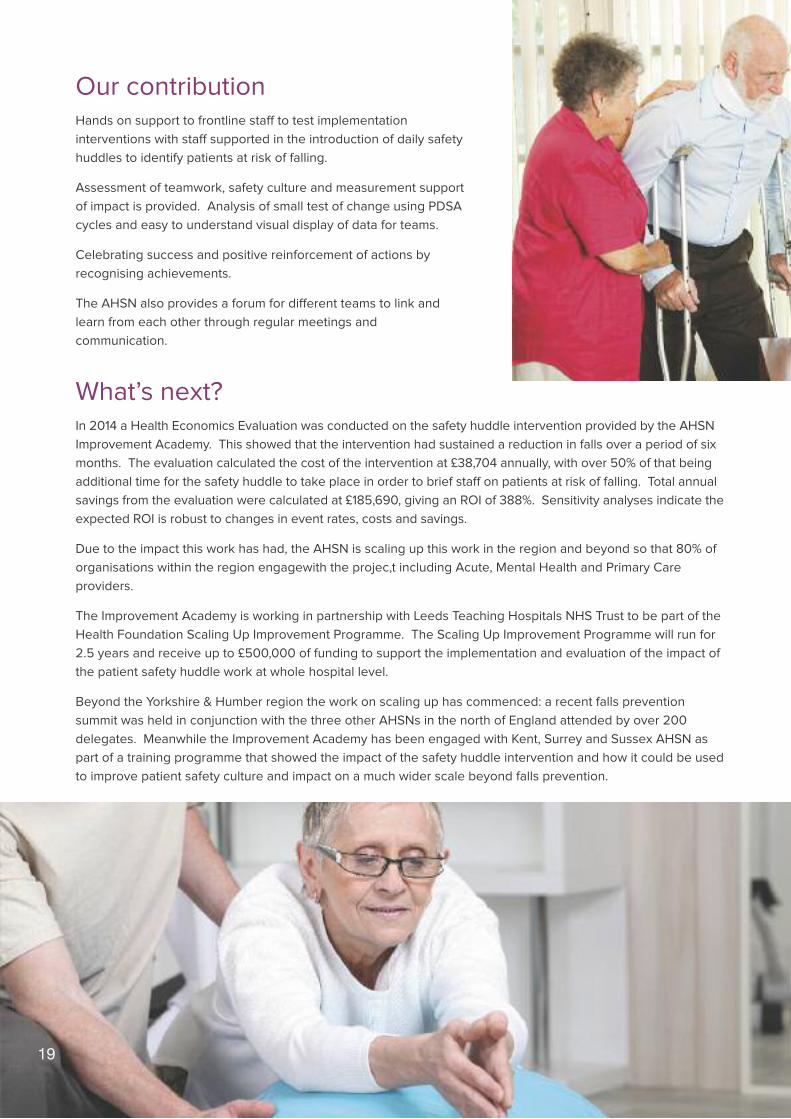
Our contributionHands on support to frontline staff to test implementation
interventions with staff supported in the introduction of daily safety
huddles to identify patients at risk of falling.
Assessment of teamwork, safety culture and measurement support
of impact is provided. Analysis of small test of change using PDSA
cycles and easy to understand visual display of data for teams.
Celebrating success and positive reinforcement of actions by
recognising achievements.
The AHSN also provides a forum for different teams to link and
learn from each other through regular meetings and
communication.
What’s next?In 2014 a Health Economics Evaluation was conducted on the safety huddle intervention provided by the AHSN
Improvement Academy. This showed that the intervention had sustained a reduction in falls over a period of six
months. The evaluation calculated the cost of the intervention at £38,704 annually, with over 50% of that being
additional time for the safety huddle to take place in order to brief staff on patients at risk of falling. Total annual
savings from the evaluation were calculated at £185,690, giving an ROI of 388%. Sensitivity analyses indicate the
expected ROI is robust to changes in event rates, costs and savings.
Due to the impact this work has had, the AHSN is scaling up this work in the region and beyond so that 80% of
organisations within the region engagewith the projec,t including Acute, Mental Health and Primary Care
providers.
The Improvement Academy is working in partnership with Leeds Teaching Hospitals NHS Trust to be part of the
Health Foundation Scaling Up Improvement Programme. The Scaling Up Improvement Programme will run for
2.5 years and receive up to £500,000 of funding to support the implementation and evaluation of the impact of
the patient safety huddle work at whole hospital level.
Beyond the Yorkshire & Humber region the work on scaling up has commenced: a recent falls prevention
summit was held in conjunction with the three other AHSNs in the north of England attended by over 200
delegates. Meanwhile the Improvement Academy has been engaged with Kent, Surrey and Sussex AHSN as
part of a training programme that showed the impact of the safety huddle intervention and how it could be used
to improve patient safety culture and impact on a much wider scale beyond falls prevention.
19

Our work revisited
Workplace Wellness BackgroundThe health and wellbeing of NHS staff is crucially
important in delivering first-class patient care, with
workplace incentives identified as a priority of 5 Year
Forward View, with a need for the NHS to set a
national example.
Poor staff health and wellbeing is estimated to cost
the UK economy around £100 billion a year. In 2009,
Boorman reported the annual cost of absence per
employee per year within the public healthcare
sector as £1,153. With 1.3 million employees, reducing
NHS staff absence by one-third could save the NHS
£500 million per year.
The AHSN partnered with Sheffield Hallam University
and the National Centre for Sport and Exercise
Medicine to develop a Workplace Wellness
programme which has now been rolled out into three
NHS Trusts: Sheffield, Bradford and Airedale.
In a study of 277 participants across the programme
the Workplace Wellness programme delivered the
following results:-
• 98% agreed that staff health and wellbeing was a
valuable workplace benefit
• 97% rated their experience of the programme as
excellent or very good
• 95% reported making changes to their health or
lifestyle
• 45% were identified as having one or more risk
factors for cardiovascular disease (CVD), of which
• 42.9% improved their health by reducing at least
one risk factor within six months of starting the
programme
• The programme has shown that for every £1 spent
on the programme, the NHS as an employer saved
£3 in costs.
Over 100
consultants and
junior doctors
trained as gold
standard mortality
case note reviewers
20

A health economics evaluation has shown that
reductions in CVD risk factors are linked to improved
productivity and patient outcomes, with a potential
ROI for the project, based on absenteeism data
estimated from the Sheffield Teaching Hospitals pilot
and the Boorman report, at between 302% and 571%.
Why is this workimportant?The Five Year Forward View set out a need “in
extending incentives for employers in England who
provide effective NICE recommended workplace
health programmes for employees. We will also
establish with NHS Employers new incentives to
ensure the NHS as an employer sets a national
example in the support it offers its own 1.3 million
staff to stay healthy, and serve as “health
ambassadors” in their local communities.”
Our contributionThe AHSN has worked in partnership with Sheffield
Hallam University and the National Centre for Sport
and Exercise Medicine to roll out the Workplace
Wellness programme across different NHS
organisations in the region.
The AHSN is now working to identify the
opportunities to scale up the project further, including
with NHS organisations beyond the Yorkshire &
Humber region, and the business opportunities
available in delivering the programme to the private
sector and other public sector bodies.
What’s next?Work is well underway in scaling this programme
throughout the Yorkshire & Humber region and
beyond. Over 60% of trusts within our region have
expressed an interest in starting the programme
within their organisations and further enquiries have
been received by NHS organisations outside of the
region.
A feasibility study is also underway investigating the
business opportunities that exist outside of our core
audience of the NHS. A number of public and private
sector organisations have approached the AHSN for
delivering this work to their organisations, with the
potential scope of engaging with over 20,000
citizens.
Sophisticated software and hardware devices are
also being developed and patented which will look to
revolutionise this workspace.21

22
Our work revisited
Location andIntelligent Mapping ofPADs in Yorkshire &Humber BackgroundThe AHSN is working with the Yorkshire Ambulance
Service (YAS), British Heart Foundation (BHF) and
NHS England to determine the location and details of
all Public Access Defibrillators (PADs) in the region.
The recent Cardiovascular Disease Outcomes
Strategy from the Department of Health (2013)
recognised the need to prioritise resuscitation from
out of hospital cardiac arrest as an area for
improvement. It is estimated that up to 75,000
OHCAs occur each year in the UK. Ambulance
services attempt resuscitation in approximately
36,000 (40%) of cases per annum. At present, only a
small number of individuals survive. There is,
however, significant variability between ambulance
services in rates of successful initial resuscitation (13-
27%) and survival to hospital discharge (2-12%)
following an OHCA. Scrutiny of international data
reveals that regions in Scandinavia and the United
States have survival rates of over 50% for some
patients who have a cardiac arrest in the community.
If survival rates were increased from the overall
national average (around 7%) to that of the best
reported (12%), it is estimated that an additional 1,000
lives could be saved each year.
Why is this workimportant?When someone has a sudden cardiac arrest (SCA),
every minute without CPR and defibrillation reduces
their chances of survival by 7-10%. More individuals
with SCA will survive to hospital discharge if
laypersons undertake cardiopulmonary resuscitation
for and employ a PAD. As a result of the
‘Defibrillators in Public Places to Initiative’, PADs were
placed in airports, railway stations and other public
places. PADs have been shown to be safe and can be
used without first aid training. The use of a
defibrillator prior to the arrival of ambulance services
has shown to approximately double rates of survival
after OHCA.
Over 200
Improvement
Fellows and
Innovation Scouts
supporting
improvements in
healthcare22

However, this is currently often dependent on
Emergency Medical Dispatchers directing bystanders
to the nearest accessible device. A recent audit
carried out by the BHF for ambulance trusts within
the UK showed that there is no standardised way of
collecting, storing, using or cleaning the data on the
location of PADs within each ambulance trust’s
catchment area. Currently there is patchy
intelligence on the number of PADs per trust, with
registered numbers ranging between 65 and 2000.
In addition to problems locating all available-to-use
PADs, information on where best to deploy the
devices is not routinely available.
Our contributionTo assist in determining the location and details of all
PADs in Yorkshire & Humber where defibrillators
should be placed in the community. The overall goal
will be to increase the use of PADs in OHCAs and
increase survival rates. The AHSN will assist in
bringing together data from across the region, using
our members, our partners and promoting
crowdsourcing campaigns to identify the location of
PADs across the region.
What’s next?Following the detailed crowdsourcing campaign to
identify the location of PADs across the Yorkshire &
Humber region cardiac arrest data will be overlaid
and cross-referenced against PAD location and
analysed to determine whether there are patterns or
hotspots that will allow the intelligent deployment of
subsequent devices. Work will then take place to
understand barriers to the use of identifiable PADs
(because current usage of existing devices is low,
even when OHCA occurs in the vicinity of the PAD).
The project will significantly increase public
awareness of resuscitation and use and location of
PADs, thus leading to:
• Increased use of PADs
• Increased rates of survival to hospital discharge
from OHCA
• Increased rates of successful initial resuscitation
• Reduction in the average time to CPR and
defibrillation
23

24
Financial Report
The 2014/15 financial year, to 31st March 2015, was
the first period the AHSN was established as a
company limited by guarantee.
The AHSN brought forward a balance of £1.218m from
2013/14. The income received for 2014/15 was
£4.853m; 70% of this income was derived from NHS
England funding of £3.375m. The remaining 30% of
income was made up of £0.92m membership fees
from 44 members and £0.558m from other sources
including RIF funding and commissioned work.
The Executive Team were appointed in May 2014,
including Dr Dawn Lawson as Chief Operating Officer,
Richard Stubbs as Commercial Director and Sally-
Anne Naunton as Director of Corporate Services,
joining the Managing Director Andrew Riley. Further
appointments were made during the course of the
period via a combination of employment and
secondment arrangements as the team was
established. At the period end the team is made up
of 11 staff and four Directors which accounts for the
£0.943m of pay expenditure for the year.
During the period, £2,771m of funds was spent on
programmes, representing financial support for a
number of partners, including the Improvement
Academy, Sheffield Hallam University, YHEC and
ScHARR.
Other non pay expenditure has been incurred during
the period of £0.309m, including the establishment of
an office in Wakefield.
During the period changes have been made to the
company’s Articles of Association to clarify the
objectives of the company as a not-for-profit
organisation. As such the only surplus subject to
corporation tax is the interest received balance of
£4,067. The company is seeking clarification from HM
Revenue & Customs regarding the tax status;
however, in the event that no further guidance is
provided the company will continue to apply this tax
treatment on a self-assessment basis.
The AHSN has an acceptable level of general
deferred income of £2.043m going into the new
financial year, which provides sufficient working
capital in order to cope with funding historically
received up to four months in arrears, and enables
the company to meet all necessary contractual
obligations. The AHSN is financially stable and
confirms that with the forecast trading position it
remains a going concern for the foreseeable future.
£1.7m additional
funding attracted
through competitive
grant applications
for improvement
work with NHS and
academic partners

25
Yorkshire & Humber Partners AHSNSummary Finance Report 2014/15 £ Actuals
Balances b/fwd from 2013/14
Balance transferred from AHSN Host 350,000
Income from NHS England 1,192,400
Less: Late costs invoiced to Y&H AHSN (323,819)
1,218,581
Income for 2014/15
Income from NHS England 3,375,682
Income from Y&H AHSN Members 919,830
Transfer from Manchester Uni Recharge 404,416
Defibrillator project 80,000
GMC Project 49,126
Inspiring Leaders Network 20,417
Interest receivable 4,067
4,853,537
Less: general deferred income (2,043,424)
Income Sub-total 4,028,694
Expenditure
Programmes expenditure 2,771,433
Pay expenditure 943,926
Non pay expenditure 309,268
Total expenditure 4,024,627
Surplus before tax 4,067
Corporation tax provision 813
Surplus for the year 3,254
N.B. Figures are unaudited at the time of production of the report
£ Actuals

26
Matrix of Metrics 2014/15
StrategicObjective
Programme Commentary
Population
Health
Move More Risk Assessment:
Olympic Games Legacy
The AHSN worked with Sheffield Hallam University to submit their successful
application for additional funding of £14m to extend the scope and remit of the
National Centre for Sport and Exercise Medicine.
Tour de France Legacy
The AHSN worked with TDF Ltd, Leeds Partners and Sheffield Hallam University to
sponsor the Yorkshire leg of the Tour de France. This included developing a "move
more" app that allowed users to ride the TDF route and measure performance.
Health & Wellbeing
programme
The AHSN worked with Sheffield Hallam University to develop the NHS wellness
programme, which was rolled out to three hospitals in Sheffield, Bradford and Airedale,
with over 300 staff recruited to the programme. The programme has been externally
evaluated, demonstrating a 3:1 ROI, significant improvement to participating
staff biometrics (95% of staff reporting lifestyle change) and additional benefits of
improved team performance and friends and family ratings.
AssociatedDiseases
Risk Assessment:
Cardiovascular
The AHSN has worked closely with the Y&H SCN and regional CCGs to develop
the atrial fibrillation programme across the region. This programme audited the use of
atrial fibrillation (AF) anticoagulation and the potential advantage of NOACs, quickly
recognising that the biggest challenge was identifying and supporting people with
undiagnosed atrial fibrillation (AF). Specifically, the programme co-created the West
Yorkshire Stroke Prevention strategy, worked jointly to transform anticoagulation
services in Leeds, and bought together pharmaceutical companies and Harrogate
CCGs to support their anticoagulation and stroke prevention work.
MSK Review was completed and decision made not to proceed with this programme.
Cancer Working with the Y&H SCN to support the Cancer Network.
Neurodegenerative
diseaseReview was completed and decision made not to proceed with this programme.
EffectiveReablementProgramme
Risk Assessment:
IA Frail Elderly
programme
The Improvement Academy (IA) established a network across the region to develop an
electronic frailty index, which is being implemented widely.
Mental Health
Programme
This programme comprises the Care Pathways and Packages Project and a
programme improving the physical health of people with severe mental illness . These
projects were scheduled to start by September 2014, but due to resource shortage
actually started in January 2015. Both projects are now sponsored by NHS Mental
Health CEOs and have associated project management teams in place, approved
project plans and are now delivering changes.
Low or no risk

27
StrategicObjective
Programme Commentary
Improving
Healthcare
Diagnostic Pathway
The AHSN is working with CCGs and providers across the region and the national
diagnostics programme to run a diagnostics programme that covers the following:
duplicated use of diagnostics, appropriate referral protocols and point of care
diagnostics to support new models of care. The AHSN is running a national
diagnostics symposium later in the year, working with 10CC and Sheffield CCG
and the NIHR DEC in Leeds.
Peptest Adoption &
Spread
Peptest is a novel diagnostic for gastro-oesophageal reflux disease (GORD) and in as
many as 50% of patients replaces gastroscopy, improving patient safety and
experience and significantly reducing costs. The AHSN supported RD Biomed’s launch
of Peptest and introduced them to several CCGs in the region. This resulted in three
large-scale pilots sponsored b the AHSN and RD Biomed. The AHSN also supported
RD Biomed in developing their evidence base and completing a health economics
assessment, which led to Peptest and complete a health economics assessment which
led to Peptest being assessed by NICE. To date RD Biomed have seen sales increase
by 85% and early assessment confirms potential large-scale savings for NHS partners.
E-Health
This programme comprises the eHRC and Qtool projects. The eHRC programme is a
partnership between Manchester University, Leeds University, TPP Ltd and the AHSN to
establish a prospective research database based on the TPP ResearchOne system. The
project has been successful in working with GPs to identify suitable cohorts of patients for
clinical trials and will be rolled out across the region by the AHSN and nationally by TPP.
The QTool project is implementing a web-based patient experience and outcome
information capture system. The information is used to feedback to staff to improve the
quality of services experienced by patients. It is currently rolled out to three pilot sites. The
AHSN also coordinated an Small Business Research Initiative competition in the telehealth
sector and delivered five roadshows across the region and has established a CEO led e-
health board for the region.
Quality & Safety Risk Assessment:
Patient Safety
Collaborative
The AHSN was awarded an NHSIQ Patient Safety Collaborative franchise during the year
and incorporated its patient safety programme into the PSC programme so please see
separate PSC summary.
NICE TA
ImplementationIncorporated into the MO programme, see below.
High Impact
Innovations
Responsive Wheelchair Services: The programme extended to all
wheelchair service providers across the region and has led to significantly improved
(63%) wheelchair access times. Collaborative work led by the AHSN has resulted
in the development of national wheelchair measures with NHS England.
IOFM: Regional audit completed, workshops to introduce IOFM benefits carried out
across the region, all trusts demonstrating increased use of IOFM.
Dementia carers: The AHSN working with the University of York produced; an
effectiveness matters review on supporting dementia carers, and a regional
conference was held in June 2014 on improving access to information for carers.
Digital First: The AHSN developed greater understanding of how to combine
electronic recording of physiological national early warning score (NEWS)
to aid clinical decision makin;, this was shared at a regional conference in
June 2014.
Medicines Optimisation
The MO programme has incorporated the AHSN’s NICE TA Implementation project.
The programme includes: Patient experience of medicines use, NOACs, safer
dispensaries, safer GP prescribing, establishing a safe prescribing community of
practice and collaborating with partners, the production of a project brief for the
development of a Centre for Medicines Optimisation Translational Research.
Low or no risk

28
Matrix of Metrics 2014/15
StrategicObjective
Programme Commentary
Improving
Healthcare
Clinical Risk Assessment:
Cystic fibrosis
The AHSN invested proof of concept funding in this project to develop a device to track
and record the use of antibiotic inhalers used by patients with CF. This is being
developed jointly with the D4D HTC.
Urgent Care
The AHSN is leading a project to develop a better understanding of urgent and
emergency care demand across the region. It is delivering in the following areas:
* Developing near real-time data analytics
* Developing algorithms to better predict routes to access services
* Understanding patient choices and experience
* Generating new models of care
Currently the AHSN is running the programme, including the steering group and four
task and finish groups, and is working with the Y&H CLAHRC and SCN to roll the
programme out and evaluate responses. A well attended regional conference
took place in November 2014.
LTC
The AHSN is running a diabetes care programme working with the SCN and some of the
regional CCGs. The objectives are to better support newly-diagnosed diabetics and work
with the SCN to reduce lower limb amputations for people with established diabetes.
Dementia
The AHSN is establishing a memory support worker programme with Leeds city
Council, West Yorkshire CCGs and NHS providers in the City. The AHSN is developing
the economic business case for the establishment of the MSW service.
Economic
Growth
SME & MNOProgrammes Risk Assessment:
The AHSN established an account management function that has been operating for just
over six months and provides comprehensive support of engagement, advice and sign
posting to SMEs and MNOs. The programme is supporting the rapid uptake and
adoption of new innovative products and technologies that support care delivery. This
has resulted in over 110 contacts with industry, successful partnerships with a number
of businesses, increased sales for partners, successful delivery of successful delivery of
a POC programme, funding four new med-tech innovations from within the region,
delivery of regional procurement clinics and workshops and continuing business assists.
InternationalOffice Risk Assessment:
The AHSN International Office provides support for regional and national SMEs, NHS
providers and HEI to generate revenue and knowledge enhancing opportunities through
import/expor, innovation collaboration and implementation of best practice. The AHSN
has run a number of open innovation workshops supporting combinatorial innovation in
the UK and internationally. This has resulted in strategic partnerships with FICCI to
support the delivery of the UK Bioconclave working closely with the Indian government,
UBI in France to identify UK distributers for game changing innovation across Europe,
and supporting UKTU and HUK to promote export opportunities for UK plc.
NHS IP Risk Assessment:
AHSN, working with Medipex Ltd, has established a network of over 100 innovation
scouts embedded in NHS organisations who have two main function: to act as
"innovation magnets" working with NHS staff to identify and scope emerging
innovations and where appropriate secure IP for the NHS, secondly to support the
development, adoption and spread of new innovation within their own NHS
organisation. Fifteen members have signed up to the Network and the programme is
now continuous professional development accredited. This coincides with a 14%
increase in NHS generated innovations across the region. The programme is being run
with our business partner 3M.
Low or no risk

29
StrategicObjective
Programme Commentary
Patient Safety
Patient Safety
CollaborativeRisk Assessment:
The AHSN established an Improvement Academy (IA) to support the system and
behavioural changes that underpin all significant change. The initial core patient safety
programme was subsumed into the PSC programme and is reported here. The IA
established a ‘Foundation for Safety’ programme, which is a team-based approach to
improving safety culture and making significant improvements in reducing patient
harm. This is scaling up the successful core programme, which not only demonstrated
significant improvements in safety but a 388% ROI evaluated by YHEC.
* The IA has established 35 multiprofessional frontline teams across 15 member
organisations to improve safety culture
* The programme has focussed on reducing falls, pressure ulcers, improving
discharge. The programme has been run in wards and departments across the region
and is demonstrating significant improvements.
* The IA has run three behavioural change workshops for 150 staff, focussed on hand
hygiene, toileting interventions, and improved drug dispensing.
* Safety culture for boards programme has been run in a number of boards and is
planned to roill out in 2015/16.
* Medicines safety collaborative (reported above).
* Mortality, and morbidity case note review has 11 acute members who all use a
standardised data collection tool. More than 50 consultants and 60 senior registrars
have been trained and are using the tool. Additional funding has been awarded to
allow the review to extend into primary care records.
* The IA has run a number of mortality conferences and master classes through the
year.
* A quality improvement training programme has been developed with Y&H Health
Education to support members develop effective QI training programmes. More than
60 training events have taken place through the year.
* The improving patient flow programme has been run in Huddersfield and
Scarborough; it is an operational tool to improve patient flow through hospitals, and
includes a component called plan for every patient. The implementation at
Scarborough started in December 2014.
Establishing aY&H GenomicsMedical Centre
(GMC)
Risk Assessment:
Following initial feedback from NHS England, the three NHS organisations involved in
the GMC (Sheffield Teaching, Sheffield Children’s and Leeds Teaching) asked the
AHSN to bring together a single proposal for Y&H. This is now underway and the plan
is to submit a second wave GMC proposal by June 2015. The AHSN has established
the programme governance, setting up and chairing the programme steering group,
establishing and chairing the operational board and the five workstream groups.
Establishmentof the
Co-creationnetwork
Risk Assessment:
Working collaboratively with Health Education Yorkshire & Humber the IA has
established a network to develop the improvement capability of staff, including an
online platform for Quality Improvement Training, supporting communities of practice
and delivering a series of round table events to address areas of common learning
need.
Low or no risk

30
Registered Directors: Biographies
Professor Pope has a wealth of experience,
leadership and expertise gained from senior roles
within industry, the NHS and academia, including at
chairman and chief executive level. He has significant
experience of working with world-leading companies
including BAE Systems, BBC, BP, Ford,
GlaxoSmithKline, Huawei and Unilever, and was CEO
of the UK’s largest integrated health, safety and
environmental business for 10 years. He has been
one of the UK’s leaders in managing and developing
environmental companies over the last 25 years, and
is a four times winner of the ‘Technology Fast 50’
awards for the fastest growing companies. He has
been awarded numerous business, environmental
excellence, bioscience and innovative biotechnology
awards and has previously been a business
innovation support person of the year..
Amongst other appointments he was previously
Chairman of the East of England Regional
Development Agency and Northamptonshire and
Milton Keynes Primary Care Trusts, and is now
Chairman of the Board at University Campus Suffolk,
Chairman of Healthwatch Northamptonshire and Vice
Chairman of East Midlands Pathology.
Other appointments and interests: Visiting Professor
at the University of the West of England; Professor of
Bioenterprise and Health at UCS; co-founder of the
Centre for Health & Wellbeing Research at the
University of Northampton; current Chairman of the
Environmental Policy Forum; a past member of the
Advisory Board of the Institute for Sustainability,
Health and Environment; and past Chairman of the
Society for the Environment and the Institution of
Environmental Sciences.
Professor Will Pope

31
Andrew has more than 15 years experience as a
Board Director in the NHS and commercial sector,
with an additional 10 years experience as an NHS
Chief Executive.
He has clinical experience with direct patient care
responsibility as a diagnostic radiographer and has
effectively engaged with patients and clinical
professionals.
He has many years experience at a national level
working in the NHS, Department of Health and UK
biopharmaceutical Industry
He brings an extensive working knowledge and
experience of operational delivery and business
strategy in the NHS and commercial sectors to the
awards evening. He also has wide-ranging business,
capital planning, programme/project management
and marketing experience in both expanding and
contracting business environments.
Andrew has an extensive track record of building
successful, cross cutting partnerships with key
stakeholder groups as well as experience managing
multi-million pound revenue budgets and capital
projects, including private finance initiatives.
Andrew Riley

32
Registered Directors: Biographies
Sir Andrew is Chief Executive of the Sheffield
Teaching Hospitals NHS Foundation Trust, one of the
largest NHS foundation trusts in England with an
annual budget in excess of £1 BN and 16,000 staff.
Sheffield Teaching Hospitals NHS Foundation Trust
has been awarded the independently assessed
‘Hospital of the Year’ three times in the last six years.
Andrew was the founding Chair of the Foundation
Trust Network (FTN) and has undertaken three spells
in the Department of Health, England – the most
recent a secondment for a year as a Director General
for developing health service providers. He is a
visiting Professor in Leadership and Development at
the Universities of Sheffield and York. He chairs the
NHS Employers Policy Board, is Deputy Chair of the
NHS Confederation, a member of the Innovation,
Health and Wealth Implementation Board, and a
member of the Shelford Group (the top 10 university
hospitals in England).
He was appointed an OBE in 2001 and knighted in
2009 for services to the NHS.
Sir Andrew Cash OBE

33
Christine Outram was appointed as Chair of The
Christie NHS Foundation Trust in October 2014. She
also joined the AHSN Board as a non-executive
director in December 2014. Chris has had a long
career in the NHS, with over 20 years' experience at
CEO level.
Leadership positions she has held include CEO of the
North Central London strategic health authority and
chief executive of NHS Leeds. At national level, in
2009 she successfully established Medical Education
England, a new Department of Health body with the
aim of developing and improving the education and
training of NHS doctors, dentists, pharmacists and
healthcare scientists. She went on to lead the
establishment of Health Education England in
2011/2012.
In 2004 Chris was appointed Director General at the
Department of Health, where she led the review of its
arm's length bodies, reducing their number from 38
to 21 and producing £0.5 billion in savings annually
for reinvestment in NHS services.
Chris continues to be passionate about working with
clinical staff and patients to deliver excellent services,
and to drive forward the quality of health research,
innovation and education.
Christine Outram

E: [email protected]: www.yhahsn.org.uk
t: @AHSN_YandH
Unit 12 Navigation Court, Calder Park, Wakefield, WF2 7BJ
A company limited by guaranteeregistered in England and Wales No 08887451
Licensed by NHS England

BUSINESS PLAN2015/16

Content
3 Foreward
4 Introduction
8 Governance
16 Yorkshire & Humber AHSN
Programme and Project Detail
72 Risks
73 Appendix

3
Professor William Pope
Chair
Andrew Riley
Managing Director
ForewardLast year, being the first fully operational
year of the Yorkshire & Humber Academic
Health Science Network (YHAHSN), we
necessarily focused on securing the
capacity and capability to deliver our
operational plan, recruiting our team,
establishing an independent base,
becoming a Company Limited by Guarantee
and engaging members. However, we did
establish nationally recognised
programmes including our Improvement
Academy, NHS Staff Workplace Wellness
programme, regional Improvement Fellows
and Innovation Scout Networks, each
having over 150 members. We also
established and delivered our Open
Innovation programme in the UK and
internationally. It is pleasing to note that our
Board of Directors and delivery teams are at
full capacity.
We have evaluated our core competencies
and how best we can apply them for the
benefits of our members and partners, and
these are set out in section 2.4. We realise
that we need to communicate and engage
more effectively with our members and
partners and are working hard to ensure we
do this.
We are a membership organisation with
governance arrangements in place to
ensure that every NHS organisation and
health community has a fair and equal input
into developing our plans for regional
benefits. We pride ourselves on being an
honest broker and a safe place for difficult
conversations, holding dear our core NHS
values of being citizen and patient focused,
whilst at the same time being more
business-like and systematic in the way we
support members, implement plans and
deliver benefits. Working with partners
during 2014/15, our Improvement Academy
secured more than £1.5m in additional
external funding, while several of our
members commissioned us to undertake
specific work on their behalf.
Our business plan has been developed with
the help and input of our members and with
the involvement of key partners. We have
reviewed their strategic objectives and,
where appropriate, reflected together how
we can best add value. Our focus is to
support the regional health economy and to
connect people, organisations and
resources to develop new solutions that
can transform the NHS, allowing it to meet
its future challenges. Our plan for 2015/16
builds on our five-year strategic objectives
and the foundations that were put in place
last year. We have aligned to the Five Year
Forward View, Office of Life Science;
Strategy for UK Life Sciences, UK Trade and
Investment Life Science Organisation
Strategy and Healthcare UK Strategic
Business Plan.
Although precise income is yet to be
finalised with NHS England, two planning
scenarios have been modelled. We will
implement the prudent plan until income
numbers are confirmed; once this
information is provided we will then re-
assess our position. This approach allows
us to continue to deliver existing
programmes and develop new ones.
We are working effectively with our
colleagues in the other 14 Academic Health
Science Networks (AHSN) to share and
spread learning, and are partnering closely
with the other three northern AHSNs to
complement work establishing the northern
innovation and research ecosystem.
As the health sector goes through a period
of change during the next few years we are
confident that the YHAHSN is well placed to
support members and partners adopt
innovation and best practices that deliver
improvements to the quality of patient care,
support system transformation and
generate economic growth.

1 INTRODUCTIONThe Yorkshire & Humber Academic Health ScienceNetwork (YHAHSN) was authorised to operate inJuly 2013, becoming a Company Limited byGuarantee (CLG) in February 2014. The CLGArticles set out the purpose of the YHAHSN:
• to create and harness strong, purposeful partnerships between
patients, health services, industry and academia in the healthcare
sector;
• to create significant improvements in the health of the population by
reducing variability and improving experiences of the healthcare
system;
• to ensure the development of new innovative products and services,
which have the potential to transform lives and become part of routine
clinical practice;
• to stimulate economic growth for the Yorkshire & Humber region,
nationally and internationally supporting inward investment projects
for health sector businesses.
Figure 1: Geographic area covered by the Yorkshire & Humber Academic Health
Science Network
1.1 LICENCE AGREEMENTThe YHAHSN was granted a licence to operate by NHS England that
focuses on delivering three strategic objectives:
• Improving Population Health
• Improving Healthcare
• Generating Economic Growth
The key objectives set out in the Five Year Forward View, published in
October 2014, along with members’ priorities, have also been reflected
in the YHAHSN’s 2015/16 business plan.
1.2 VISION“Adopting excellence, creating opportunity for healthcare innovation.”
York
Leeds
Doncaster
BradfordKingston Upon Hull
Sheffield
Huddersfield
Barnsley
Selby
SkiptonHarrogate
Malton
4

1.3 MISSION STATEMENTThe YHAHSN is a member organisation acting as an honest broker to build networks and connect people,
organisations and technology.
Using evidence to inform decision making the YHAHSN drives the adoption and spread of innovation at
pace and scale, creates change capability and leadership, and supports system redesign and improvement.
1.4 STRATEGIC OBJECTIVESThe YHAHSN has three strategic objectives:
1. Contribute to improving population
health across the Yorkshire & Humber region.
2. Support service improvement, transformation
and delivery of new models of healthcare.
3. Generate regional and national economic
growth by creating strong partnerships
between the NHS, HEIs (higher education
institutions) and business.
1.5 SUMMARY OF PROGRESS TO DATE Improving Population Health: in 2014 the YHAHSN, in partnership
with Sheffield Hallam University, supported the development of the
“Move More” and Tour de France legacy programmes.
An NHS Staff Workplace Wellness programme was established and
rolled out to three of the region’s hospitals. Evidence indicates that
there has been a 2% reduction in sickness absence for enrolled staff,
a significant improvement in key biometric indicators for participants,
an investment ratio of 3:1 and a 95% staff approval rating.
A joint programme, run with the Yorkshire & Humber Strategic Clinical
Network (SCN) and a group of regional Clinical Commissioning
Groups (CCGs), reviewed the management of atrial fibrillation (AF)
and in particular, the use of novel oral anticoagulants (NOACs).
The YHAHSN Improvement Academy (IA) initiated a frailty
programme supporting the improvement of services for frail,
elderly people.
5
Figure 1-4: Strategic Objectives

Transforming Healthcare: the YHAHSN established the IA to create
change capability and capacity in front-line clinical and managerial staff,
and provide ongoing support for all member organisations to take on
increasingly more complex transformation projects within their
organisations and across systems. This included establishing an
Improvement Fellows’ Network, which currently has more than 150
members with the capability to support the delivery of front-line
improvement projects within their own organisations from falls reduction
to a nationally recognised reduction in hospital mortality project. The IA
also delivered six high-impact innovations and established a nationally
recognised patient safety programme.
NHS IQ awarded the YHAHSN the contract for delivery of the Patient
Safety Collaborative for Yorkshire & Humber in September 2014.
RD Biomed’s Peptest innovation is now running in two large-scale pilots
where it is demonstrating the opportunity of significant patient benefit
and reduced cost while offering reconfiguration opportunities for upper
gastrointestinal gastroscopy services.
Working with the Universities of Leeds and Manchester, TPP Ltd and
EMIS Ltd, the YHAHSN has expanded a primary care research system to
prospectively identify patients suitable for participation in clinical trials,
greatly improving trial delivery.
Work commenced on a regional urgent care programme supported by
NHS member CEOs and Accountable Officers to gather workflow and
demand data from all members in order to create a data model of
urgent care flows.
Economic Growth: the YHAHSN established an SME (small and
medium sized enterprise) development programme that currently has
more than 100 members, providing proof of concept funding, access to
front-line clinicians, product development and procurement workshops,
system navigation and connection to national and international
manufacturing and distribution partners.
The YHAHSN set up a successful Innovation Scout Network, which
currently has more than 120 scouts embedded in member organisations
and acting as innovation magnets. They are responsible for identifying
potential innovation, completing initial due diligence and registering IP
(intellectual property).
We have established and run Open Innovation programmes connecting
innovators, business and finance with a focus on solving specific
problems. These have run in the region and more recently in China,
working with UK Trade and Investment (UKTI) to connect UK and
Chinese companies and academics, creating new collaborations with
the aim of attracting inward investment and, in time, lower prices for
new technology for the NHS.
6

7
We have worked closely supporting UKTI, Healthcare UK (HUK) and Office for Life Sciences (OLS) to export
NHS excellence to international markets and have established the YHAHSN International Office to work with
colleagues in the EU and internationally.
Key national documents and reference to members’
planning priorities have been considered to produce
this business plan, including:
• The AHSN licence agreement
• The NHS Outcomes framework
• The Five Year Forward View
• The OLS: Strategy for UK Life Sciences
• UKTI Life Science Organisation Strategy
• HUK Strategic Business Plan
For the purpose of the programme summary
strategic alignment is shown to the AHSN core
licence objectives and the Five Year Forward View
themes.
Three regional workshops have taken place for
member CEOs and subsequent working versions of
the business plan as it developed have been shared
and comments from members have been
incorporated.
The YHAHSN has extensively engaged with regional
stakeholders, such as the SCN, Health Education
England Leadership Academy for Yorkshire &
Humber, Public Health England and National
Institute Health Research Clinical Research
Networks, to identify their priorities.
1.6 2015/16 PLANNING PROCESS

8
2 Governance2.1 COMPANY SET UPThe YHAHSN is a Company Limited by Guarantee (CLG), registered at Companies House in the UK. It has
four Registered Directors (see Appendix) legally responsible for the lawful transaction of business and to
ensure the CLG is a financial going concern.
The Registered Directors established a Board which meets every three months to discuss strategic direction
and to assure delivery of the operational plan. The Board consists of 18 NHS CEOs and senior leaders from
HEIs and industry.
The Board has established two sub-committees, an Audit Committee and a Remuneration Committee, both
chaired by Non-Executive Directors.
Figure 2-1: Board Structure

9
2.2 ORGANISATIONAL STRUCTUREThe YHAHSN team has expanded to the proposed arrangement of 15 core central staff with additional staff
seconded for specific projects or employed by the IA. The following chart summarises the current structure:
2.2.1 Commercial Director Responsible for:
• Identifying and spreading industry-led healthcare innovation into NHS and related care pathways to
improve patient outcomes and productivity
• Facilitating regional and national economic growth through SME and MNO (multinational organisation)
engagement, support and development
• Identifying and achieving new sources of funding for the region to enable rapid growth of new healthcare
technologies and innovations
• Providing commercial expertise to NHS, industry and academic regional partners
• Establishing and running the YHAHSN International Office to attract inward investment and increase
export opportunities and partnerships in key overseas markets, for the region and the UK
Figure 2-2: Organisational Structure

2.2.2 Chief Operating Officer
Responsible for:
• Establishing and creating partnerships and networks to design and
deliver transformational programmes at scale across the region
• Leading the YHAHSN’s health community improvement and
transformation projects, such as supporting the development of new
models of care, digital health, e-health, urgent and emergency care,
diagnostic and imaging programmes
• Identifying new business opportunities, working with NHS, HEI and
commercial partners to attract funding to the region
• Managing delivery of YHAHSN programme based sub-contractors
• Leading the improvement and innovation team who provide support
for the YHAHSN and members.
2.2.3 Corporate Services Director
Responsible for:
• Operational management of the head office and satellites
• Planning
• Customer relationship management
• Contract management for all YHAHSN contracts
• Human resource management
• Quality control and health and safety
• Marketing and communications
• Financial management, including liaison with company accountants.
2.2.4 Director of the Improvement Academy
Responsible for:
• Leading delivery of the 2015/16 IA operational plan
• Leading the delivery of the Patient Safety Collaborative contract
• Establishing effective collaborative relationships with other regional
improvement bodies across England and the UK.
2.3 STRATEGIC PARTNERSHIPSAs an organisation that brings together people, organisations,
technology and finance, our preferred modus operandi is to develop
productive networks and partnerships and co-create solutions and
plans. We have developed close working relationships with regional,
national and international organisations, with local partners being
represented at the YHAHSN Board. This section focusses on some
specific partnerships where we are working jointly to plan and deliver
programmes or evaluate outcomes.
10

2.3.1 Directors of Public Health (DspH) and
Health & Wellbeing Boards
Following discussions in 2014 the DsPH identified a lead DPH to
work with the YHAHSN and identify public health priorities. The
Improving Air Quality project being run by the IA is an example of
one such collaboration. Although the Workplace Wellness project is
focused on supporting NHS staff manage their own health and
wellbeing more effectively, the longer term intention is to expand the
programme across other employers in the region and, subject to
funding, extend the programme to include communities across the
region where there is evidenced variability in life expectancy and
quality of life indicators.
2.3.2 Strategic Clinical Network Yorkshire & HumberThe YHAHSN has worked closely with the SCN in developing its
2015/16 plan, with the Director of the SCN participating in all three
planning workshops and contributing to discussions that have taken
place at the YHAHSN Board. The YHAHSN COO is also a member of
the SCN Board. The specific project that both organisations have
contributed to during the year is improving services for people with
atrial fibrillation (AF), including anticoagulation by introducing NOACs
and, in the longer term, aiming to reduce the incidence of acute
stroke. The YHAHSN and SCN are proposing to participate in the
following areas through 2015/16:
• Assistive technology and telehealth
• Management of people at risk from type 2 diabetes and for those
people who already have diabetes
• Urgent care
• Stroke and atrial fibrillation
• Dementia programmes
2.3.3 York Health Economics Consortium (YHEC)/School of
Health and Related Research (ScHARR)An important aspect of the YHAHSN’s plan for 2014/15 was the
evaluation of the benefits delivered through programmes and
projects. Contracts with the Universities of York and Sheffield allow
the YHAHSN to call on the academic rigour of the two universities in
evaluation. The partnerships support the quarterly delivery
assurance meetings scheduled with NHS England.
A further benefit of the partnerships is that they provide an
opportunity for SME partners to access health economics advice at an
affordable entry point. This provides SMEs with emerging innovations
for the health sector with access to high-quality health economics
advice in order to make informed decisions on product development
and market access.
2.3.4 Yorkshire & Humber Clinical Research Network (CRN)The Clinical Director for the CRN is a member of the YHAHSN Board
and the YHAHSN participates in the CRN Management
11

12
Board. The main focus of joint working has been in
aiming for single sign-off for multi-centre clinical
trials and in improving responsiveness to calls to
participate in commercial clinical trials, where the
YHAHSN has been working with commercial
partners and the University of Leeds to develop a
prospective primary care research system.
2.3.5 Yorkshire & Humber Leadership
Academy
The YHAHSN has been working with, and
supported financially by, the Leadership Academy
to develop the Improvement Fellows Network and
the Inspiring Leaders Network. We are planning to
extend this moving into 2015/16.
2.3.6 Health Education Yorkshire & Humber
(HEYH)
HEYH are jointly funding work to develop quality
improvement skills training for the region, and a
number of Clinical Leadership Fellows, taking a year
out of medical training on the HEYH scheme, are
working with the IA to lead change programmes.
2.3.7 CLAHRC Y&H
The CLAHRC (Collaboration for Leadership in
Applied Health Research and Care) Director is a
member of the YHAHSN Board and the YHAHSN
MD is a member of the CLAHRC Partnership Board.
Both organisations have been working to integrate
plans with the YHAHSN and CLAHRC particularly
working collaboratively in the telehealth area.
2.3.8 National Centre for Sport and Exercise
Medicine/Sheffield Hallam University (SHU)
The YHAHSN has partnered with the National
Centre for Sport and Exercise Medicine and SHU to
provide a tailored lifestyle support programme to
NHS employees. The project, commissioned by the
YHAHSN and delivered by SHU, is currently being
used at Sheffield Teaching Hospitals NHS
Foundation Trust, Bradford Teaching Hospitals NHS
Foundation Trust and Airedale NHS Foundation
Trust and encourages NHS employees to boost
fitness levels whilst improving morale and wellbeing
through individualised lifestyle checks.

13
2.4 YHAHSN CAPABILITIESOver the last year, in addition to delivering a range of specific programmes, the YHAHSN has been building
leadership and change capability and capacity in NHS member organisations, in anticipation of scaling up
the pace of change. The YHAHSN identified early last year the capabilities that it has to offer to members.
This section sets out what our value offer is to members:
2.4.1 System leadership
This role is particularly prevalent where cross
cutting, health economy wide, complex change is
being considered or where there are
provider/commissioner tensions. Our role here is
not to lead the system through change, but to bring
relevant people and organisations together, unpick
some of the often long-held views, and underpin the
decision-making process with quality-assured data,
information and evidence. We help develop diverse
solutions across the system to ensure genuine and
tangible transforming change that has the potential
for significant impact and scale.
Once we have established the project machinery,
helped define the issues and identified the key
people to resolve those issues, our role evolves to
deliver the process until the health economy feels
confident enough to take on that role itself. This a
role we are playing in the Urgent Care and GMC
(Genomics Medicines Centre) projects.
2.4.2 Developing change leaders
We have recruited, trained and are developing more
than 300 front-line leaders through our
Improvement Fellows and Innovation Scouts. With
the support of the NHS Leadership Academy we will
continue to invest in creating large-scale change
leader capacity. This brings a range of benefits
including re-engaging front-line staff and building
communities of improvement at ward, department
and system level. We are creating a cadre of leaders
that balance patient safety, outcome and
experience, and cost/value and effectiveness.
2.4.3 Collaboration
Our principle leadership role is to be able to quickly
access the CEO and Board level leaders in the HEI,
business and NHS members and bring key opinion
and knowledge leaders together to discuss
innovative solutions to complex cross cutting
problems. We have been told we are seen as an
honest broker with no vested interests, always trying
to find acceptable solutions for all parties through
careful use of data, information and evidence.
Figure 2-4: YHAHSN Capability Wheel

14
2.4.4 Creating time to think
The operational agenda for most organisations is
crowded and senior leaders tend to be focused on
the operational agenda. We create opportunities to
consider the longer view options, bring new
evidence, information and analysis to their
attention, complete due diligence of incoming
business innovation, and bring peers together to
consider new solutions.
2.4.5 Health economics
Our experience to date has shown that one of the
barriers to the development of early-stage innovation
is the lack of affordable and quick turnaround health
economics. We have developed partnerships with
two of the region’s recognised leaders in health
economic analysis, as detailed in section 2.3.3
2.4.6 Membership organisation
The YHAHSN is a membership organisation, with a
clear governance arrangement and a single
accountable board that includes CEOs and senior
leaders from the NHS, HEIs, business and other
stakeholders.
2.4.7 Research evidence
There are 12 HEIs in the region, three of which have
medical schools. It can be confusing for a small or
newly formed company to know how to access the
research capability within the region’s universities.
The YHAHSN is in the process of appointing an
Academic Director with an objective of connecting
members to the most appropriate academic contact
or unit in the region.
2.4.8 Data, intelligence and analysis
Our experience from the programmes we ran
through 2014/15 is that one of the barriers for SMEs
trying to share their innovative ideas with NHS
organisations is the lack of information or evidence
available. We have established partnerships with
some of the region’s leading ICT (information and
communications technology) companies and
university teams to support the collation of research
and evidence and to generate new information to
enhance the value of an innovation. Our
improvement programmes include measurement
and data analytical support. We also evaluate the
programmes that we run and make that information
available to members. The YHAHSN Commercial
Team carry out due diligence on commercial
organisations and their innovations to support
member engagement with minimum risk.
2.4.9 Patient and public involvement
Working with the SCN and other delivery partners,
we are developing positive public and patient
engagement. The IA involves patients or citizens in
all programmes from initial scoping through to
implementation, using research methods to identify
the most effective and appropriate engagement
methods to apply.
2.4.10 Leveraging additional resource
Although our resources are limited compared with
our members, we are developing a capability of
using our available resource, be it cash or staff, to
match fund joint projects. This is often the deciding
factor in starting a programme. We regularly submit
bids to grant-awarding bodies, the EU and
corporate boards to financially support programmes
and we have invested in commercial business
opportunities that contribute a financial return on
our investment.
2.4.11 NHS values, business discipline
The value of working together for patients is a
central tenet guiding service provision in the NHS.
Patients are central and the YHAHSN acts and
collaborates in the interests of patients. As well as
working with health service organisations,
providers, academia and business the YHAHSN
involves staff, patients, citizens and local
communities to ensure potential solutions are
tailored to local needs.
The delivery of high-quality care is dependent on
feedback; as an organisation that welcomes
feedback the YHAHSN is able to identify and drive
areas for improvement. We are focused on
delivering patient quality and safety benefits and
addressing the need to transform systems and
reduce costs, by introducing best practice and
leading edge technologies. We can quickly check
the views of our members through direct contact
and social media channels, dealing responsively
with issues or problems. We include patients or
citizens on our programme boards and invite them
to attend seminars and workshops to provide a
clear view on the matters we are addressing.

15
2.4.12 Quality and training
The YHAHSN developed the IA to support safety and quality improvement across member organisations.
A team of improvement scientists, patient safety experts and clinicians work with front-line services,
patients and the public and have delivered measurable and lasting quality and safety improvements across
the region. In 2014/15 the IA worked with members and regional experts to agree a regional Quality
Improvement Training Framework, established a network of 150 Improvement Fellows and initiated a
number of collaborative improvement programmes, including our flagship falls project and nationally
recognised hospital mortality review project.
Figure 2-4.1: YHAHSN Capability Wheel & Strategic Objectives

16
3 Yorkshire & Humber AHSN Programmeand Project Detail
The YHAHSN has 12 programmes. Each strategic objective, PopulationHealth, Improving Healthcare and Economic Growth, has four programmeseach with detailed project plans.
This section of the business plan provides more detail for each programme,including:
• Programme description
• Financial resource being allocated to the programme
• Alignment to national strategies
• Project description and outcomes
• The YHAHSN’s role
• A summary project plan and key performance indicators.
Figure 3 demonstrates how the YHAHSN will employ its strengths and capabilities to deliver 2015/16
programmes.
Figure 3: YHAHSN Capability Wheel, Strategic Objectives and Programme Detail

17
AHSN CoreLicence Objectives
Five Year Forward View Themes
Page A B C D E F G H I J K
POPULATION HEALTH
Health & Wellbeing 18 3 3 3 3 3Workplace Wellness 18
Improving Diabetes Care 20
Digital Health 22 3 3 3 3 3 3 3 3Establishing Digital Health Record Test Beds 23
Creating An E-health Ecosystem 24
Better Data 25
Enhancing Quality Of Life For People With Long Term Conditions 28 3 3 3 3 3 3 3Healthy Ageing Collaborative 29
Memory Support Workers 30
Improving Air Quality 31
Preventing People From Dying Prematurely 32 3 3 3 3 3Physical Health For Those With Serious Mental Illness 33
Mortality Reduction 34
IMPROVING HEALTHCARE
Current Systems 36 3 3 3 3 3 3 3 3 3Urgent & Emergency Care 37
Medicines Optimisation 40
Diagnostics 41
Future Systems 42 3 3 3 3 3 3 3Genomics Medicines Centre 43
Transforming Primary Care 44
Safety & Quality 46 3 3 3 3 3 3 3Patient Safety Collaborative 46
Patient Falls 48
Capacity Building For Quality Improvement 50
Efficiency & Productivity 52 3 3 3 3 3 3 3 3Patient Flow 53
Evaluating Currency Implementation For Mental Health 54
ECONOMIC GROWTH
Industry Investment 56 3 3 3 3 3 3 3 3New Source of Inward Investment 57
Investment To Accelerate Innovation 58
Industry Engagement 60 3 3 3 3 3 3 3 3Connecting Industry To Healthcare 61
Identifying & Adopting Innovation 62
Open Innovation 63 3 3 3 3 3 3 3 3 3Innovation Scouts 64
Innovation Accelerator 66
Generating Growth From Overseas Markets 68 3 3 3 3International Inward Investment 68
Exporting UK Healthcare Excellence 70
KeyA - Focus on the needs of patients and local populations: support and work in partnership with commissioners and public health bodies to identify and address unmet
medical needs, whilst promoting health equality and best practice.B - Build a culture of partnership and collaboration: promote inclusivity, partnership and collaboration to consider and address local, regional and national priorities.C - Speed up adoption of innovation into practice to improve clinical outcomes and patient experience – support the identification and more rapid spread of research
and innovation at pace and scale to improve patient care and local population health.D - Create wealth through co-development, testing, evaluation and early adoption and spread of new products and services.E - Prevention and public health.F - Providing patients with greater control and autonomy.G - Breaking down barriers to how care is provided.H - Urgent and Emergency Care redesign.I - Diverse solutions and local leadership.J - Improving the NHS' ability to undertake innovation and research.
K - Sustaining and improving a tax-funded system.
Yorkshire & Humber AHSN Strategic Alignment & Plan on a Page 2015/16

18
HEALTH AND WELLBEING
The Five Year Forward View clearly sets out theimportance of supporting citizens to make informeddecisions about their own health and wellbeingthroughout their lives. The goal is to improve quality of life and increase the life expectancy of the
population, whilst reducing their reliance on health services. The YHAHSN
Health & Wellbeing programme has two projects, Workplace Wellness and
Improving Diabetes Care.
• Currently the NHS employs more than 100,000
staff in the Yorkshire & Humber region. The
YHAHSN has a long-term goal to improve the
health and wellbeing of those staff. Initial
evaluations of the Workplace Wellness pilots have
shown that participants have achieved significant
and quantifiable improvements in their physical
and mental health, whilst staff sickness and
absence levels have reduced. The project is also
showing a return on investment ratio of 3:1.
• The Improving Diabetes Care project will improve
the support for people who might be prone to, or
who have been recently diagnosed with, type 2
diabetes. The project will allow individuals to
make choices to reduce their risk of developing
the disease in the first instance, while those who
are diagnosed will be well informed about their
disease status and supported to take
responsibility for managing their diabetes, only
accessing health services as appropriate.
POPULATION HEALTH
WORKPLACE WELLNESSWithin the Five Year Forward View, NHS England prioritises the
development and support of new workplace incentives that
promote employee health and wellbeing and contribute
to reducing inequalities in health.
The Workplace Wellness programme will
work with NHS staff to improve their health
outcomes and reduce sickness and
absence levels. The programme will
also focus on reducing operating costs for
members by reducing sickness absence costs
and costs of agency staff.

OUTCOMES • Deliver an evidence-based Workplace
Wellness programme for NHS staff
• Contribute to the ‘evidence base’ and
‘economic case’ for the role of physical activity
in achieving good workforce health
• Increase the number of NHS Trusts in the
Yorkshire & Humber region who adopt the
programme
THE ROLE OF THE YHAHSN Will be to work in partnership with SHU and The
National Centre for Sport and Exercise
Medicine. Providing a supporting role as the
Workplace Wellness programme is rolled out to
NHS organisations across the Yorkshire &
Humber region.
• The commissioning of SHU to deliver an
evidence-based Workforce Wellness
programme for NHS staff
• Agreed outcomes identified with monthly
performance monitoring in place
19

20
OUTCOMES • To allow the earlier recognition of
hypoglycaemic unawareness
• Assist people with diabetes and clinicians to
identify evidence-based strategies that will
improve self-care and avoid further episodes
impacting on urgent care demand
• Improved patient confidence in disease
management
o Fewer patients will attend A&E for
hypoglycaemic episodes
o Fewer patients will call ambulance
services to assist in hypoglycaemic
episodes
THE ROLE OF THE YHAHSN • Production of a ‘hypo toolkit’ (online; app;
paper-based)
• Pilot the implementation of the toolkit
• Develop and deliver a ‘diabetes master class’
across Yorkshire & Humber
o Raising awareness with primary care
clinicians and pharmacies and
promoting use of the toolkit at scale
• Develop an evaluation process for pilot sites
to demonstrate a reduction in severe
hypoglycaemic episodes
IMPROVING DIABETES CARE
Diabetes UK estimate that the NHS is alreadyspending approximately £10bn a year on diabetes.Almost three million people in England are alreadyliving with diabetes and another seven millionpeople are at risk of becoming diabetic. Working in partnership with the SCN and with clinical leads for
hypoglycaemia, the YHAHSN is leading an initiative to promote the
effective use of care strategies to assist people at risk of hypoglycaemia to
live longer and better lives.
POPULATION HEALTH

21

DIGITAL HEALTH
The case for e-health as a transformationalhealthcare solution receives a mixed reception.Despite numerous pilot programmes, large-scaleadoption is at best limited and current healtheconomic appraisal often describes marginal gains. One of the YHAHSN’s strategic objectives is to support healthcare
organisations access more accurate and complete health information with
a view to establishing and developing a way of pooling information from
different sources to improve clinical decision making and enable more
effective system-wide working.
We will also bring together HEIs, the NHS and business
to develop the e-health and digital economy
agenda in Yorkshire & Humber. There is
considerable strength across the region
in all sectors, with Airedale Hospital being
the only 3* EU telehealth site in England.
The YHAHSN is in a good position to
support members and partners
exploiting new technologies to
create new models of care that
transform healthcare delivery.
The YHAHSN is exploring test
bed opportunities in the e-health
sector working with the NHS England
national team and will develop an EU E-health
Ecosystem in 2015/16 to support resourcing
and implementation.
POPULATION HEALTH
22

Digital Health Record Test Beds The NHS generates millions of records containing billions of data items, and a significant proportion of
these are held in paper-based systems. This brings a number of challenges: patient records held by
many providers contain incomplete and inaccurate medical information and records are not accessible
by clinicians when patients present for diagnosis and treatment. There have been numerous reviews
which have identified that the NHS could save billions of pounds by becoming digital, and NHS England
has set two relevant targets: that patients should have access to their GP records by the end of 2015
and that the NHS should be paperless by 2018. This is a new project that is being co-developed with
the 10CC group (10 CCGs from West Yorkshire and Harrogate & Rural District) and Sheffield CCG to
build on existing work in the two economies and work undertaken last year by the YHAHSN to develop
a cloud- based digital record.
OUTCOMES • Establishing and supporting programme
boards in the two test bed communities
• A programme feasibility report for the two
health communities setting out the
opportunities, risks and potential cost of going
digital in the first instance at GP practice level
• A second feasibility report examining the
opportunity of broadening the two test beds to
include cloud-based, fully integrated medical
records
• Agreed implementation plans for the two test
beds to commence the GP digital economy
project
• At key milestones, robust evaluation of
progress, benefits delivery and health
economics impact
THE ROLE OF THE YHAHSN • To work with 10CC, Sheffield CCG and our
academic partners to develop and write the
feasibility studies for both the GP practice
level test beds and the longer term paperless
milestone in 2018
• To project manage the test beds in
partnership with 10CC and Sheffield CCG
• To set up and run programme governance
• To commission robust evaluation at regular
intervals throughout the programme
23

24
CREATING AN E-HEALTH ECOSYSTEM
We will coordinate a regional e-health Board acrossNHS provider organisations, CCGs, public healthand academia. The priorities contained within Five Year Forward View will be a key focus.
We will establish an EU e-health ecosystem programme that supports large
health economies in creating telehealth, assistive technology test beds
and spreading and adopting emerging learning. The intention is to work
with Airedale Hospital, which is EU 3* rated, and also a recently
announced Vanguard programme site and two other health systems, to
share learning from the EU e-health ecosystem programme, support the
development of plans, and evaluate delivery of benefits.
POPULATION HEALTH
OUTCOMES • To provide leadership to the region to
maximise full range of assets for implementing
e-health technologies at pace and scale
• A single EU e-health ecosystem across
Yorkshire & Humber
• Support for the Vanguard site in Airedale to
share learning across the region
• Three health communities that have
implemented agreed aspects of telehealth or
assistive living
• Robust academic evaluation of the potential
benefits of e-health to support delivery of new
models of care
THE ROLE OF THE YHAHSN • Agree and deliver a strategic plan with the e-
health Board
• To join the EU e-health ecosystem programme
on behalf of members and share their
experience
• Establishing an EU e-health ecosystem
• Arrange at least one EU e-health symposium
in the Yorkshire & Humber region during
2015/16
• To support at least two health systems
establish and roll out a good sized e-health
programme

25
BETTER DATA: RESEARCHONE ResearchOne is a health and care research database developed by TPP in partnership with the
University of Leeds. The ResearchOne database contains non-identifiable patient record information
from over four million people from more than 330 health and social care organisations. It is particularly
strong in the Yorkshire & Humber region where, for example, more than 60% of GP practices use the
TPP system.
OUTCOMES • An extensive research database made
available to researchers and academics
• Up to 15 research projects commissioned and
concluded in key areas of health and
healthcare
THE ROLE OF THE YHAHSN • To manage the contract already in place with
the University of Leeds and TPP to make the
research database available for academic
review
• To issue a call for research proposals that
would use the ResearchOne database as a
key data source
• To ensure that the research is published, peer
reviewed and that it contributes to the
innovation agenda in the region

26
BETTER DATA: QTOOL
QTool is a web-based electronic form systemdesigned to easily capture data from patients andsupply this to healthcare staff via the Internet.
The YHAHSN have funded the University of Leedsto manage the deployment of QTool questionnairesto obtain:
• anonymous feedback on care received as an in-patient
• patient identifiable data regarding previous medical history prior to
an intervention
• patient identifiable feedback on outcomes following an intervention.
POPULATION HEALTH
OUTCOMES • Improve the quality of patient-generated
data by piloting the implementation of a
web-based patient data collection tool
• If the tool evaluates positively, support the
development of a sustainable business
model for successful uptake by NHS
organisations
THE ROLE OF THE YHAHSN • Manage the contract with the University of
Leeds to ensure delivery and evaluation of
QTool and the production of patient-based
outcome measures
• To use the outputs from the QTool survey to
support members make changes to improve
service delivery, working with the IA

27

ENHANCING QUALITY OF LIFE FOR PEOPLE WITH LONG-TERM CONDITONS
Evidence indicates that as life expectancy increases,people tend to suffer from one or more long-termconditions that significantly reduce their quality oflife, requiring them to regularly access healthservices. With more effective self-management, better use of health information,
greater service delivery co-ordination and effective use of wearable
biometric and environmental telemetry, it is possible to change the way in
which people access health services. The result of this is that patients
remain in their own homes and communities rather than being admitted to
hospital. The YHAHSN will support existing regional Vanguard sites and
spread learning across the rest of the region.
The YHAHSN has three projects in this programme: The Healthy Ageing
Collaborative project will build partnerships to enable the design of the
new systems of primary and community care for older people; the Memory
Support Worker project will work with Primary Healthcare Teams and
specialist memory services to offer a ground-breaking service for people
who either have a diagnosis of dementia, or are showing signs and
symptoms that may indicate dementia; finally the Improving Air Quality
project is working with four local authorities supporting a priority of the
Directors of Public Health.
POPULATION HEALTH
28

HEALTHY AGEING COLLABORATIVE The Healthy Ageing Collaborative is building partnerships to enable the design of new systems of
primary and community care for older people with different severity grades of frailty based on an
electronic frailty index (eFI). A collaborative network of clinicians, academics, CCGs, local authorities
and industry partners has been established to implement evidence-based interventions, such as
supported self-management, and medication review protocols.
OUTCOMES • A well-tested package of care, incorporating
knowledge and skills for implementing the eFI into
routine GP care
• The creation of case studies demonstrating how the
eFI has been used to identify older people with
frailty and to more effectively manage their care
• In participating GP practices metrics will include:
improvement in numbers of frail older people
identified; improvement in number of frail older
people with evidence of a medication review;
improvement in uptake of physical activity/hearing
tests/podiatry/eye tests. These will serve as proxy
measures for primary outcome measures, which
include unplanned hospital admissions, stopping
inappropriate medications, and older people better
enabled to use supported self-management.
• The improvement case studies will be used to
inform an analysis of return on investment
THE ROLE OF THE YHAHSN • To disseminate the research evidence around
the management of frailty to general practice
staff
• Clinical utility testing of the eFI in two GP
clinical systems (SystmOne and EMIS)
• To support volunteer GP practices testing use
of the eFI to implement evidence-based
interventions, including a supported self-
management tool and implementation of a
STOPP protocol (screening tool for older
people’s potentially inappropriate
prescriptions) for medication review
• To support the testing of new ways of working
and different models of care, including the use
of clinical care coordinators and frailty
services to improve management of frailty
29

30
POPULATION HEALTH
MEMORY SUPPORT WORKERS (MSW)
Under the auspices of the Better Care Fund, LeedsCCGs, Leeds City Council and the voluntary sectorare working in partnership to implement a newMemory Support Worker Service. The MSW service is a ground-breaking development working with Primary
Healthcare Teams and specialist memory services to offer a service for
people who either have a diagnosis of dementia, or are showing signs and
symptoms that may indicate dementia. The workers will offer information,
advice, and meaningful, practical steps to connect people to opportunities
for activities and support – e.g. community-based activities, carers groups
and advocacy. The MSW service will be delivered by The Alzheimer’s
Society. The expectation is that the MSW service will deliver better
outcomes for patients and make efficiency and productivity gains for the
local health economy.
OUTCOMES • Following the delivery of the new project a
comprehensive evaluation of the impact of the
MSW service for Leeds will take place.
Pending the results of the evaluation roll-out
opportunities for MSWs beyond Leeds will be
identified.
• The economic evaluation will assess whether
the MSW service is likely to result in an overall
benefit, and what the associated costs will be.
The evaluation will demonstrate any out of
improvements in clinical care, reductions in
unnecessary hospital admissions, cost
effectiveness, return on investment and
improved patient outcomes.
THE ROLE OF THE YHAHSN Will be to work in partnership with Leeds CCGs,
Leeds and York Partnership NHS, Leeds City Council
and The Alzheimer’s Society to:
• Secure and fund expertise in health economics
from ScHARR
• Work alongside ScHARR to agree a consistent,
coordinated and coherent framework for economic
evaluation of this redesigned MSW service model
• Adopt a coordination role to project manage all
aspects of delivery of the health economics
evaluation
• Review and disseminate the findings to regional
stakeholders and the SCN

31
IMPROVING AIR QUALITYAir pollution is associated with low birth weight, ill health and an increase in the development andexacerbation of many life-limiting conditions. The YHAHSN is working with Directors of Public Health inYorkshire & Humber to improve air quality. In 2014/5 a study of best practice across all local authorities in theregion was undertaken and access provided to health economic modelling of air quality impact on health. In2015/6 the YHAHSN will build on that initial work to support four local authorities in the region through aseries of learning events to spread best practice and improve outcomes. The project will also examine therelationship between air quality and the incidence of COPD (chronic obstructive pulmonary disease).
OUTCOMES • Each of the four local authorities will
demonstrate impact in their chosen area of
evidence-based improvement using a credible
proxy measure. Example proxy measures are
percentage of fleet vehicles that are low
emission vehicles and proportion of school
children/staff using active travel to
school/work.
THE ROLE OF THE YHAHSN Will be to lead a collaborative approach with the four
local authorities to effect positive changes.
• Teams will attend a series of three learning
workshops during 2015/6, building on Learning
Event 1 which took place in December 2014
• The IA will provide one-to-one coaching support for
the teams to test changes and measure impact
• The IA will support the teams to access other major
stakeholders, including health economists
(University of York), behaviour change experts
(Universities of Leeds and Hull), and air quality
experts (Bradford District Council and Public Health
England)
• Commission a research study into the links
between air quality and COPD

PREVENTING PEOPLE FROM DYING PREMATURELY
Evidence suggests that people are dyingprematurely for avoidable reasons and the YHAHSNhas an objective to address this as part of our five-year strategy. The two priority projects in thisprogramme are:
POPULATION HEALTH
• Improving physical health for people with serious
mental illness, a project being run in collaboration
with Bradford District Care Trust.
• Reducing mortality via a thorough audit of case
notes, sharing the learning emerging from this to
better recognise and manage early signs of
deterioration, which if caught early enough could
prevent death. Shared learning about the
characteristics of good care will also improve
hospital mortality.
.
32

PHYSICAL HEALTH FOR THOSE WITH SMIPeople with diagnoses of serious mental illnesses (SMIs) such as schizophrenia and bipolar disorder die
15-20 years earlier than the general population, mainly from natural causes. The Yorkshire & Humber
NHS Mental Health Chief Executives’ Forum identified a need to reduce regional variation in both the
quality of annual healthcare checks and the number of people with SMI who receive an annual
healthcare check. Bradford District Care Trust has achieved national recognition in this area of care and
will be used as an exemplar site to guide best practice.
OUTCOMES This project supports the ambitions of the Five
Year Forward View, ensuring that:
• People with an SMI diagnosis received
improved physical healthcare
• New models of care are evaluated to establish
which produce the best experience for
patients and the best value for money
THE ROLE OF THE YHAHSN • Will be to work in partnership with the seven
NHS trusts across Yorkshire & Humber to
develop local improvement plans:
• Sharing the learning from the model of care
implemented by Bradford District Care Trust
• Support the trusts to adopt, adapt and
implement local approaches that will reduce
variation in the quality of annual health checks
and increase the numbers of people with SMI
who receive an annual health check
• We will fund health economics expertise to
review the evidence of impact for
implementing models of care that aim to
improve the physical healthcare of people
with SMI
33

34
MORTALITY REDUCTION
This is an area where the IA has already establisheda national reputation. The IA is working with trusts in the region to develop a standardised,
systematic evidence-based mortality review programme using case note
review. This project enables members to identify contributory factors to
suboptimal care. The IA supports learning and improvement within front-
line teams, sharing regional themes arising from anonymised findings.
POPULATION HEALTH
OUTCOMES • A cadre of clinical staff trained in a systematic,
structured judgement method of case note
review in hospitals across the region
• A greater understanding across healthcare
providers in Yorkshire & Humber of major
themes around safety and quality of care
arising from systematic analysis of case notes
from deceased patients
• Case study examples of organisations that
have used the information to make
improvements in care and reduce mortality
THE ROLE OF THE YHAHSN Will be to lead:
• An ongoing programme of training for
volunteer clinical reviewers, led by a leading
expert in the field
• Ongoing development of the Regional
Mortality Steering Group with representatives
from each trust forming a strong network of
clinical leads in collaborating organisations
• Master classes and events to educate, engage
and learn
• Involvement of trainees as recommended by
NHS England’s Medical Director
• Input at board level in participating
organisations
• A system for shared learning, including
learning from positive practice and good
quality care
• Strong academic input for understanding
mortality statistics, led by a leading expert in
the field
• Links to national level mortality reduction work

35

CURRENT SYSTEMS
The YHAHSN has an emerging facilitation andleadership role in system level transformation anddevelopment. We provide support as an honestbroker to resolve differences and to deliverintegrated business cases that are underpinned byrobust evidence. Through our IA and extensive networks of Improvement Fellows and
Innovation Scouts we have created improvement capability and capacity
across the region and are leading improvement throughout the region.
Within this programme the YHAHSN is working on three intensive projects:
Urgent and Emergency Care, Medicines Optimisation and Diagnostics.
IMPROVING HEALTHCARE
36

OUTCOMES • Accelerate collaboration between regional
stakeholders to identify priorities for action and
support before winter 2015
• Improve understanding of patient flow into and
through the urgent and emergency care system
• Improve understanding of the patient experience of
urgent and emergency care
• Engage with the newly announced Vanguard sites
in support of their ambitions for urgent and
emergency care
THE ROLE OF THE YHAHSN • Work collaboratively with SCNs, Urgent Care
Networks and local leaders
• Establish four task and finish groups that will
develop resources to:
o Map the UEC system surrounding pilot
CCG areas to identify flow, demand,
misalignment and system blockages
o Identify predictors that give a window for
intervention and avoid A&E attendance via
practiced intervention
o Predict tomorrow’s UEC demand – collect
GP practice level data to support near
real-time prediction of UEC demand and
support capacity planning in the acute
sector
o Promote UEC access to patient records by
bringing data together for direct patient
care and use of the Frailty index to better
understand patient flow
• Bring outputs from the task and finish groups
together in order to generate and prioritise ideas
for testing followed by wider implementation across
the region
URGENT & EMERGENCY CAREYorkshire & Humber CEOs and Chief Accountable Officers formed a consensus that urgent and
emergency care is a critical challenge. The YHAHSN has been asked to support a project to develop a
better understanding of urgent and emergency care demand in the region.
This project commenced in November 2014 with a conference that brought together clinicians,
managers, commissioners, providers and academics to identify a better understanding of the system
and identity key challenges. The project uses a collective, connected and co-ordinated ‘systems
thinking’ approach with experts in the region participating in four task and finish groups. Sheffield and
Harrogate (PACS (integrated primary and acute care systems) Vanguard) CCGs have come forward as
initial pilot sites to identify their specific system challenges and solutions. Work is now ongoing to tailor
the project requirements for each pilot site area to their local needs.
37

IMPROVING EMERGENCY DEPARTMENTS
As part of our Urgent Care work, this project issupporting Emergency Departments in memberorganisations to review and improve theiroperational processes, implementing effectivetriage systems for timely and appropriate care. The project is enabling Emergency Departments to access research
evidence and to learn from the experience of effective systems both within
the region and beyond. This project builds on work undertaken in 2014/5,
which established a strong network of Emergency Department contacts
interested in learning with and from each other. In 2015/6 the IA will
deliver support to three Emergency Departments to implement
recommendations in relation to senior doctor triage and share the learning
with other members.
IMPROVING HEALTHCARE
38

OUTCOMES • Improved speed and appropriateness of
treatment in Emergency Departments,
including improved performance on the A&E
four-hour target
• An economic evaluation will provide further
evidence of impact and cost effectiveness of
implementing triage systems.
THE ROLE OF THE YHAHSN Is to build on a regional survey of 16
participating Emergency Departments in the
Yorkshire & Humber region and collated
research evidence to:
• Support the development of a strong network
of ED contacts
• Facilitate the sharing of research evidence
across the network of ED contacts
• Support implementation of recommended
evidence-based change in up to three EDs in
the region
• Provide access to behaviour change methods,
measurement for improvement and economic
evaluation
• Support the development of impact case
studies to demonstrate results
39

40
MEDICINES OPTIMISATION
Medicines, used to best effect, benefit both patients and
the NHS but all too often medicine use is sub-optimal,
leading to lost benefit and preventable harm and waste. Medicines Optimisation (MO) brings together the concepts of patient
centred care, self-management, shared decision making and evidence-
based medicine. More could be done to shift the prevailing paradigm of
‘medicines management’ to one of ‘medicines optimisation’.
IMPROVING HEALTHCARE
OUTCOMES • Facilitate improved patient experience through
patient activation and adherence
• Improve medicines safety
• Improve patient outcomes in our exemplar
areas (frailty, stroke prevention in atrial
fibrillation, glycaemic control in diabetes,
symptom control in asthma, and physical
health of people with mental health conditions)
THE ROLE OF THE YHAHSN Will be to work in partnership with the SCN,
academia, pharmaceutical industry, commissioners
and providers to:
• Co-produce behavioural guidance for clinicians and
patients to embed MO in clinical consultations
• Increasing joint working initiatives with
pharmaceutical industry and the digital technology
sector
• Demonstrate how the use of data and health
economics can identify “positive deviance” in the
field of MO
• Use data to highlight opportunities for CCGs to
invest in MO strategies
• Establish a Yorkshire & Humber Academic and
Clinical Translational Research Community
• Build an active Community of Practice for
medication safety
• Work with community pharmacy teams to improve
the safety of dispensing
• Work with primary care and community teams to
improve medicines interventions at transitions of
care
• Work with CCGs and medicines safety officers to
increase the number and quality of medicine-
related patient safety incident reports on NRLS
(National Reporting and Learning System) and carry
out the associated root cause analysis or significant
event audit

OUTCOMES • Patients have access to world-class
diagnostics and imaging services, provided
both sustainably and effectively
• New technologies will be identified for
implementation at scale through a phased
three-year approach
• Implement new technologies to generate the
expertise of working at scale across the
region. This learning will be used to develop
additional technologies that support early
intervention and upstream care
• Position Yorkshire & Humber as the national
leader in the effective use of diagnostics and
imaging technologies
THE ROLE OF THE YHAHSN • Review the current diagnostics work,
alongside the associated evidence base
• Provide academic and health economic
support to both groups via YHEC and ScHARR
• Work with partners to plan and deliver
symposium in north of England
• Support the work with 10CC and Working
Together in relation to demand optimisation
for radiology services, looking at new models
for workforce, standardisation of protocols
and any inappropriate demand on services
• Identify existing point of care diagnostic
technologies that would support earlier
diagnosis or prevention, cash release, align
with CCG priorities and support
implementation at scale
DIAGNOSTICSMember organisations have identified diagnostics and imaging capacity and capability as a key
challenge. There are significant opportunities to work collaboratively across the region with
commissioners, providers and industry to co-create solutions to the challenges, which include:
commissioning of services; capacity and capability; variation in pathways and quality; inconsistency in
delivery and data-sharing; duplication of tests; sustainable workforce; barriers to implementation of new
innovations; and supporting behaviour change.
There is a need to improve access to, and productivity of, diagnostic services across the region. The
reason this is important is to ensure the NHS is able to meet and better manage increasing demand. A
key part of this is ensuring timely access to diagnostics services in a way that directly impacts upon
patient management to improve outcomes. There is a commitment from existing networks to engage
with this programme of work, including the 10CC and Working Together groups, NIHR DEC (National
Institute for Health Research, Diagnostic Evidence Co-operatives) and NICE (National Institute for Health
and Care Excellence). Experts from across the region have met at two steering group meetings and are
currently developing the work programme supported by three task and finish groups (North of England
Symposium Event; Demand Optimisation; Technology Implementation).
41

IMPROVING HEALTHCARE
FUTURE SYSTEMS
Healthcare needs to transform in order to manage the
demands of a growing and ageing population. Emerging technologies are having a significant impact on supporting
individual citizens to manage their own health and wellbeing and make
more informed decisions about their healthcare. The NHS needs to adopt
the latest information technologies to significantly improve service
quality and operational performance at a faster pace than has been
achieved to date. Advances in diagnostics and genomic medicine will
revolutionise the way people experience health services. Citizens are
used to easier access to services in other sectors and are demanding
change in the way they access health services; this has significant
implications for transforming primary care.
Within this programme the YHAHSN is currently engaged in two projects:
supporting the development of a Yorkshire & Humber Genomics Medical
Centre (GMC) and supporting the transformation of primary care. Working
with existing regional EU telehealth leaders and SMEs, the YHAHSN is
engaged in establishing an e-health eco-system and developing
partnerships with leading ICT businesses. Our role is to bring together
NHS members, leading edge academics and businesses to deliver
practical solutions that deliver benefits to patients in the region, with the IA
creating the change-enabled organisational culture needed for sustained
improvement.
42

OUTCOMES • Programme management infrastructure
established and functional
• Resources in place with the capacity and
capability to deliver the project to time
• Full business proposal submitted by the
deadline in July 2015
• Preparation of the project team for the
evaluation visits by NHS England
• Successful GMC operating in Yorkshire &
Humber region by December 2015
THE ROLE OF THE YHAHSN • Appoint Programme Director, set up project
governance arrangements and convene all
project working groups
• Provide all programme management functions
and support
• Lead the GMC operational group and
participate on the GMC steering board
• Write the GMC business proposal
• Coordinate and prepare the team for the NHS
England evaluation visit
GENOMICS MEDICINES CENTREThe 100,000 Genomes Project is a world-leading programme with the aim of ensuring that the UK will
be the first country to introduce this technology in its mainstream health system. The aim of the
Genomics Medicine Centre (GMC) project is to support a successful application to be designated as a
Wave 2 NHS England Genomics Medicine Centre in Yorkshire & Humber. The YHAHSN is facilitating a
collaboration between three Yorkshire-based NHS Trust organisations (Sheffield Teaching, Leeds
Teaching and Sheffield Children’s Hospitals) to submit an application to NHS England to become a GMC
delivery centre.
43

IMPROVING HEALTHCARE
TRANSFORMING PRIMARY CARE
NHS primary care is the recognised gateway to the NHS.
The majority of patients access hospital and specialist
services following referral from primary care so
transforming primary care at scale is a prerequisite to
major hospital and system change. The project will learn
from existing communities where a more integrated out of
hospital service has been wrapped around primary care. The project will be designed in partnership with the regions CCGs’ leaders
and seek to address establishing new models of integrated primary,
community and out of hospital care for health communities. It will look to
solve the problems caused by a significant proportion of the GP workforce
approaching retirement whilst the recruitment of new GPs struggles to
keep pace. Transforming primary care was identified as a priority by
members during the YHAHSN regional planning meetings.
44

OUTCOMES • Project steering groups and governance in
place to deliver long-term changes includingclinical and wider systems inclusion
• Produced and consulted on plans to establishnew models for primary and community care
• Processes in place to spread new modelsacross the region to support early adopters
• Implementation plans ready to commenceimplementation with agreed timeframes
• Involvement of the YHAHSN commercial andIA teams to support the process
• A review of emerging primary care models inthe UK and Europe
THE ROLE OF THE YHAHSN • To appoint a GP and Project Director to
support member CCGs initiate the programme
• To support local health communities as theybegin delivering changes
• Support the regional Vanguards
• To bring the IA and YHAHSN’s CommercialTeam’s expertise on change management andICT support
• Examine opportunities for additional resourceand funding to support change projects
• To bring key individuals together in projectsteering groups and teams
• To arrange workshops to scope theprogramme
• To producing PIDs and project plans andcommission programme evaluation
45

46
IMPROVING HEALTHCARE
SAFETY & QUALITY
In 2015/6 the IA will continue to be a regional focus for
quality improvement, working with partners and members
to provide access for all healthcare staff in Yorkshire &
Humber to online quality improvement training, as well as
resources to support quality improvement projects
throughout the region. The IA will work collaboratively with Health Education Yorkshire and
Humber (HEYH), Yorkshire and Humber Leadership Academy and SCNs,
and is one of the founding members of the UK Improvement Alliance.
All NHS organisations in Yorkshire & Humber have access to the support,
training and resources provided by the IA.
PATIENT SAFETY COLLABORATIVE (PSC)The PSC mobilises front-line teams to focus on areas of safety that are important to members, including
pressure ulcers, medicines safety, physical health of mental health patients, improving outcomes from
high-risk surgery and acute kidney injury. The IA will support knowledge and evidence sharing between
organisations, through facilitated networks of patient safety leads and Improvement Fellows. This
project draws on structured summaries of research evidence and provides support to our members to
become High Reliability Organisations for safety, improving care ‘bottom up from the top’. The PSC will
draw on learning from other areas of the IA portfolio, including the use of the Measurement and
Monitoring of Patient Safety framework with front-line teams and boards, and a research project to
extend the national early warning score (NEWS) to include biochemical data in a computer-assisted risk
score, and funding to scale-up team huddle and acute kidney injury interventions. This project draws on
and involves our regional network of Improvement Fellows.

47
OUTCOMES • Reduced patient harm: falls, pressure ulcers,
AKI, physical health checks, medication errors
• Improved team safety culture measured usingvalidated tool
• Increased capability for independent safetyimprovement for participating teams
THE ROLE OF THE YHAHSN • Host roundtable meetings with patient safety
leads in acute trusts, mental health trusts, andin primary and community care, setting theagenda for working together to tackle some ofthe common priority problems
• Create a TAPS (Training and Action for PatientSafety) programme focusing on safermedicines dispensing
• Use our network of Improvement Fellows andlinks to other PSCs through the YHAHSNnetwork
• Draw on resources that include access toresearch evidence, quality improvementtraining, behaviour change methodology,measurement for improvement, team cultureimprovement and training in human factors

48
IMPROVING HEALTHCARE
PATIENT FALLS
A pilot project in 2014/5 for supporting front-line teams in
Leeds Teaching Hospitals to reduce falls was positively
evaluated, showing 50% reductions in falls in engaged
ward teams, and a return on investment of 388%. For 2015/16 this programme will be offered to all members. The project is
planned to extend into community services and GP surgeries. This project
will draw on and involve our regional network of Improvement Fellows and
build on our successful Falls Summit held jointly with other northern
AHSNs. Quality improvement training is available to actively encourage
improvement across all member organisations.

OUTCOMES • Reduction in falls to levels equivalent to those
achieved in the pilots
• Improvement in team safety culture
• Capability at team level to deliverimprovement in other areas of care
THE ROLE OF THE YHAHSN • Offer light touch team level support from the
IA using a tried and tested model ofimprovement
• ‘Bottom up from the top’ delivery withexecutive support for working with front-lineclinical teams
• A pilot project will be established in eachmember organisation, to include:
o Initial meeting with member ofexecutive team of interested partnerorganisations to agree which team tostart with in their organisation
o Initial team meeting with seniorclinician and senior manager inidentified teams
o Team culture survey in each newteam
o Ongoing light touch, hands-onfacilitation with each team
o Measurement processes establishedin each team
• The initial pilot projects in each organisationwill be a basis for further spread and scale up
• All teams reporting bronze, silver, gold,platinum and diamond achievements reportedon a regional roll of honour
49

50
IMPROVING HEALTHCARE
OUTCOMES • Dedicated Quality Improvement online training
portal
• Entry-level online training accessible to allhealthcare staff in Yorkshire & Humber, free ofcharge
• Quality improvement skills training deliveredthrough core skills workshops (20-50participants)
• Specialist training that will equip organisationsto develop and maintain a sustainableimprovement culture
• A supported network of 150 ImprovementFellows in Yorkshire & Humber
• Support for the development of “communitiesof practice” through the Co-Creation Network
THE ROLE OF THE YHAHSN • Sustain strategic engagement with the QI
Training Advisory Group
• Test the online training resources withvolunteer member organisations
• Develop and deliver the face-to-face QItraining in response to identified needs
• Support a group of QI training experts througha Train the Trainer (‘gold’ level) programme
• Publicise and administer access to QI trainingproducts, both online and face-to-face
• Develop access to a range of online tools andresources
• Sustain and nourish the Improvement Fellowsnetwork
• Work with NHS Leadership Academy todevelop communities of practice through theCo-Creation Network
CAPACITY BUILDING FOR QUALITY IMPROVEMENT
The Quality Improvement (QI) training programmes help
to develop capability for improvement. In 2014/15 a
Quality Improvement Training (QIT) Advisory Group was
established from member organisations to steer the
development of a regional framework for QI training. In 2015/16 this work will continue in order to provide access for all
healthcare staff in Yorkshire & Humber to online ‘entry-level’ QI training, as
well as delivering face-to-face core skills workshops, and highly specialist
training, including a Train the Trainer programme. The Improvement
Fellows scheme supports those who are already leaders of improvement in
their own organisations.

51

IMPROVING HEALTHCARE
EFFICIENCY & PRODUCTIVITY
NHS organisations are used to making annual efficiency
targets and considerable improvements have already
been achieved. Through the Five Year Forward View the NHS has challenged itself to
achieve further significant efficiencies. This programme focuses on how
current services can be redesigned to improve quality and reduce cost.
This programme will principally be led by the IA through the Improvement
Fellows Network and is focusing on priorities identified by members. The
programme will bring organisations and technology together to take
practical steps to implement evidence-based improvements and achieve
associated patient benefits.
The projects making up this programme consist of Patient Flow and
Evaluating Currency Implementation for Mental Health: Care Pathways &
Packages Project.
52

OUTCOMES • Reduced length of stay by the equivalent
levels achieved in the pilot
• Reduced waits in Emergency Departments forpatients being admitted to hospital beds
• Improved control for staff
• A potential test bed initiative
• Evaluation of the programme
THE ROLE OF THE YHAHSN • Systematic implementation of operational
management tools designed to support betterpatient flow in hospitals
• Sharing lessons from initial implementationsites through facilitated and targeted regionalroundtable and master class events
• Support wider and sustainable spread througha Train the Trainer approach
• Ensure synergy with the Urgent Care andPatient Safety Collaborative projects in orderto exploit the implementation and embeddingof this approach
PATIENT FLOWThis project supports hospitals and community-based services to better understand and manage
patient flow. Through the introduction of operational management tools, this project aims to support
member organisations in reducing hospital length of stay (LOS) and Emergency Department (ED) waits.
One early implementation site is demonstrating a reduction in LOS of 20%, and implementation is
currently taking place at a second hospital site. The work in 2015/16 will include a roundtable discussion
with representatives from interested member organisations of the evidence and learning to date, a
master class, and further training support. We will support member organisations to demonstrate impact
on key outcome indicators, including LOS and patient waits in EDs.
53

IMPROVING HEALTHCARE
CURRENCY IMPLEMENTATION FOR MENTAL HEALTH
The Care Pathways & Packages Project (CPPP) is a
consortium of organisations in Yorkshire & Humber and the
North East who are working together to develop national
currencies and local tariffs for mental health services.
The currencies, known as ‘care clusters’, cover most mental health services
for working age adults and older people. The care clusters were mandated
for use from April 2012.
54

OUTCOMES In February 2015, the Yorkshire & Humber NHSChief Executives’ Forum for Mental HealthServices requested YHAHSN’s support for theCare Pathways & Packages Project in order to:
• Produce a health economics focused analysisof the impact upon patient, clinical andfinancial outcomes from implementing themental health clustering tool
• Improve commissioner and service providerunderstanding of implementing the costingmethodology and using mental health datamore effectively
• Achieve commissioner approval to proceedwith the CPPP programme
THE ROLE OF THE YHAHSN Work in partnership with representatives fromthe Care Pathways & Packages Project and theSCN, in order to:
• Complete a scoping exercise with mentalhealth commissioners and providers to gatherevidence, opinion and information, and reviewcurrent procedure. Review of the scopingwork completed in 2014/15.
• Discuss and agree the requirement andtimetable for delivery with a view tosupporting the production of two eLearningresources that meet the needs of the targetaudience and complement the existing suiteof resources developed for the CPPPprogramme. The e-learning resources willhave a focus on:
o Guidance for implementing thecosting and pricing methodology
o Guidance for using quality andoutcome data
• Secure health economics expertise toundertake an evaluation of implementing themental health clustering tool across twolocalities. Adopt a co-ordination role to projectmanage all aspects of delivery of the healtheconomics evaluation.
55

56
ECONOMIC GROWTH
INWARD INVESTMENT
External funding is often the key to unlocking innovation
implementation within the NHS, especially when clinical
trials necessitate the costly dual running of services or
pathways.
This programme is focused on two main goals. The first is creating and
facilitating an innovation investment funding function that de-risks
investment for both the NHS and SMEs. The second is investing in
emerging and potentially game-changing innovations that require initial
seed funding to accomplish proof of concept evidence, but that
demonstrate a future positive impact for our patients in addition to
generating returns to be reinvested into further supporting projects.
The funding function will horizon scan to identify a range of funding
options for Yorkshire & Humber companies and NHS organisations to
apply for, including, but not limited to, European and national innovation
funds (e.g. EU programmes, Innovate UK, Research Council and NIHR
initiatives), additional government assistance (especially through
engagement with Local Enterprise Partnerships), and private equity
financial investments (working with venture capital, private equity and
angel investment communities).

NEW SOURCES OF INWARD INVESTMENTMaximising the potential of available funding and investment streams is crucial to regional growth
across 2015/16. This project will continue the work of leveraging UK, European and global funding to
increase regional investment. The YHAHSN will support organisations to drive innovation into front-line
use care delivery and support access to key lines of funding inclusive of SBRI (Small Business Research
Initiative), Horizon2020, NHS Challenge Prizes and Regional Innovation Funds. Additional funding will
provide proof of concept funding and other investment opportunities to sustain innovative SME
partners, and reduce the burden on central NHS budgets.
57
OUTCOMES • Increased opportunity and access to efficientusage of UK funding opportunities
• The YHAHSN will provide supportmechanisms to access and ensure efficientusage of EU and global funding opportunities
THE ROLE OF THE YHAHSN • Establish a clear understanding of UK, EU and
global funding opportunities available
• Work closely with key stakeholders at alllevels to support organisations seeking toidentify funding opportunities, including butnot limited to: Local Enterprise Partnerships,NHS European Office and local authorities
• Develop a ‘route to funding’ pathway toprovide clear steps and advice

58
ECONOMIC GROWTH
INVESTMENT TO ACCELERATE INNOVATION
Throughout 2015/16 the YHAHSN will build upon the
regional and national growth of UK organisations and
capitalise on the economic development across the
Yorkshire & Humber region through 2014/15.
We will continue with the creation of an environment for business that
encourages them to establish and/or grow in the region, working closely
with HEI, industry and the NHS. The aim is to create public/private
partnerships and other business models that deliver value to the NHS
and industry by providing investment that supports ground breaking
innovators, SMEs and MNOs in order to provide innovation directly into
the NHS.
OUTCOMES • The provision of technical, financial and
clinical support to new innovations that willbenefit the NHS
• Identification and funding of proof of conceptprojects
• Identification of risks that act as barriers to theinnovation pathway and identification ofmitigation actions
• Generation of a financial return to theYHAHSN for future investment opportunities
THE ROLE OF THE YHAHSN • Roll out a proof of concept funding
programme, which will provide predominantlyfinancial support to innovators from public andprivate sector organisations to develop andtest new innovations
• Build and engage commercial partnershipswith public and private sector organisations tosupport the delivery of ground breakinginnovations

59

ECONOMIC GROWTH
INDUSTRY ENGAGEMENT
The UK has one of the strongest and most productive life
sciences sectors in the world, generating an annual
turnover of more than £50bn.
The sector comprises nearly 5,000 companies, and employs an estimated
175,000 people. The NHS benefits greatly from the ground-breaking
innovations that are created in the sector. Our industry engagement
programme will build stronger relationships between the NHS and industry
that will result in better, more effective solutions for our patients, as well as
safeguarding and creating life science sector jobs.
Within this programme the YHAHSN will work as market makers: opening
doors and creating a more conducive environment for relevant industries
to work more effectively with the NHS and other parts of the UK
healthcare sector. We will work with the healthcare sector to help make
the NHS a better customer to industry, supporting them to better articulate
their needs. We also work with industry to help them better understand
NHS requirements and how to access the healthcare market, moving away
from a purely transactional way of working to a partnership model.
60

OUTCOMES • Enhanced partnerships between UK industry
and the NHS
• Quicker and more widespread use ofinnovation in front-line care
• Extension of the UK’s reputation for deliveringgame changing innovation to the health andcare sector
• Support for NHS organisations in overcomingprocurement barriers
• Support for the private sector to generateincreased sales, revenue and improved jobopportunities
THE ROLE OF THE YHAHSN • Develop a single point of access (SPA) portal
to support and develop a pipeline ofinnovations for the NHS
• Establish an industry engagement pathwaythat builds relationships between UK industryand the NHS
• Provide procurement and commissioningclinic for industry partners to overcomecurrent market barriers
• Provide leadership across the region toprovide a coherent, joined up approach toSME support, inclusive of engagement withLocal Enterprise Partnerships, regionalinnovation hubs, local authority economicdepartments, Healthcare TechnologyCollaborative, and Diagnostic Evidence Co-operatives
• Delivery of Regional Open Innovationworkshops to connect HEI, industry and NHSpartners to create and develop newintellectual property, products andopportunities
CONNECTING INDUSTRY TO HEALTHCAREThe project will build a comprehensive support programme for UK businesses and NHS entrepreneurs
that creates a single point of access to the NHS. A pipeline of validated innovations for front-line
delivery will be established that creates growth for UK industry and increases quality in NHS provision.
This includes procurement advice, system education, consultancy support, signposting, health
economics expertise and market access strategy creation.partners, and reduce the burden on central
NHS budgets.
61

62
ECONOMIC GROWTH
IDENTIFYING & ADOPTING INNOVATION
Advances in technology and medicine require the NHS to
be more nimble in identifying and implementing
innovations that will allow it to deliver better care more
efficiently.
In the coming decade technological innovations such as smart phones,
wearable devices, the “Internet of things”, remote monitoring, cloud
computing and big data have the ability to create a seismic effect on
healthcare delivery. In addition medical breakthroughs such as genomics,
proteomics, personalised and stratified medicines and regenerative
medicine will also change our fundamental notion of healthcare services.
With this backdrop it is essential that the NHS becomes better at
identifying and refining the technological opportunities that will make the
biggest improvements to patient care, with a recognised pathway towards
mainstream front-line use.
This programme harnesses the creativity of the region by encouraging the
NHS to work more directly with industry and academic partners to develop
new IP and innovations that enable the rapid adoption of new technology
into the NHS front line. Open innovation is a major programme for the
YHAHSN that results in new partnerships between UK and international
organisations, developing new IP suitable for the delivery of a 21st Century
healthcare service, in addition to maximising growth opportunities for UK
industry by creating new joint ventures designed to exploit both UK and
overseas markets.

63
OUTCOMES • The delivery of an International Open
Innovation Programme in 2015/16
• The delivery of Regional Open InnovationWorkshops
THE ROLE OF THE YHAHSN • Working closely with UK industry partners and
HEIs to generate investment and growthopportunities
• Collaboration and joint delivery with expertpartners from Yorkshire & Humber, bringingtogether regional expertise and skills todevelop and explore new innovations, IP andhealthcare solutions
• Working collaboratively with the Departmentfor Business Innovation and Skills and othernational bodies to explore the potential andscope for a UK Open Innovation Programme
• Working with international partners to identifynew territories in which to deliver future OpenInnovation Programmes
OPEN INNOVATIONThe 2015/16 financial year will bring the continuation of the successful Open Innovation programme
piloted in 2014/15. The programme will support our additional objectives of connecting UK business,
the NHS and UK HEIs with potential funding sources, including venture capital and international
government investment funds, to speed up adoption and evidence generation and reduce NHS
unit costs.

ECONOMIC GROWTH
INNOVATION SCOUTS
The barriers to successful innovation across the health and
care sector are widely recognised, none more so than our
ability to sufficiently recognise and reward the innovators
within our healthcare delivery system.
The Yorkshire & Humber Innovation Scout Network has grown during
2014/15 and this next year will see the ‘scout’ network grow further. In
collaboration with delivery partners, we will support NHS staff across the
region to innovate, collaborate and develop new commercial opportunities
within and between NHS organisations. Plans for 2015/16 activity include
cross-border networking events and significant partnerships with UK
business.
64

OUTCOMES • Expansion of the Innovation Scout Network
across the region and beyond
• The identification, spread and adoption of newcommercial IP and best practice innovationacross the NHS
THE ROLE OF THE YHAHSN • Work with our key delivery partners to
strengthen the current programme forYorkshire & Humber Innovation Scouts that issuitable for cross border application also
• Work closely with, and provide leadershipacross, the four northern AHSNs to create acoherent brand and aligned objectives foreach Innovation Scout Network
• Build into the programme a series of exclusivedevelopment opportunities to reward andrecognise the efforts and impact of NHSinnovators; this will involve working closelywith industry partners, HEIs, NHSorganisations and other bodies to ensure wecreate informative and rewardingexperiences.
65

66
OUTCOMES • Supporting the identification and awarding of
the 20 Innovation Fellows
• Working with associates to deliver the NIAprogramme with reference to the followingoutcomes:
o Focusing on patients and populations
o Learning from elsewhere
o Selecting the best nationally andinternationally
o Tailored support to fellows
o Delivering through partnership
o Effective communication
THE ROLE OF THE YHAHSN • Act as co-developers of the programme and
partner with NHS England, UCL Partners, TheHealth Foundation and successful applicantsto ensure the programme is delivered to thehighest quality
• Support the application and assessmentprocess and programme delivery
• Ensure learning and development is broughtback to the Yorkshire & Humber Region,providing regular update summaries, sharingkey learning and developing informationsessions to promote and spread the identifiedbest practice
ECONOMIC GROWTH
INNOVATION ACCELERATOR
As a founder member of the National Innovation
Accelerator programme, the YHAHSN will work in
partnership with other AHSNs, the Health Foundation, NHS
England, patient groups, mentors and experts from across
the health sector to support new and emerging innovators
and maximise their impact on patient care.
“NHS Innovation Accelerator (NIA) is to help deliver on the commitment
detailed within the Five Year Forward View – creating the conditions and
cultural change necessary for proven innovations to be adopted faster and
more systematically through the NHS, and to deliver examples into
practice for demonstrable patient and population benefit.” (NHS Innovation
Accelerator: Call for Applications 2015)

67

68
ECONOMIC GROWTH
GENERATING GROWTH FROM OVERSEAS MARKETS
The Government’s Plan for Growth (2011) identified greater
inward investment and exports as a route to a more
balanced economy.
This programme supports that ambition within a healthcare context and is
focused on the twin ambitions of greater inward investment for Yorkshire &
Humber in the form of Foreign Direct Investment (FDI), and promoting our
services, innovations and expertise overseas, working in partnership with
industry and creating opportunities for healthcare and UK-based
companies to generate new revenue streams, particularly in the BRICS
(Brazil, Russia, India, China and South Africa) and MINT (Mexico, Indonesia,
Nigeria and Turkey) markets.
The NHS’s unique position as a national provider means it can lead the
world as an ‘intelligent customer’; this programme is aimed at harnessing
the collective skills and expertise of the region to promote ourselves
internationally and support the “northern powerhouse” to be the best
place in Europe to start, finance and grow a business. Success in this
programme requires close strategic alignment with our Local Enterprise
Partnerships (LEPs) as well as key government departments, particularly
Healthcare UK and the UKTI Life Sciences Organisation
INTERNATIONAL INWARD INVESTMENTIn 2015/16 the work of our International Office will be closely aligned to all our ongoing projects. There
will be a focus on creating opportunities for regional industry partners, NHS providers and key
stakeholders to generate value-enhancing engagements and inward investment opportunities. Working
in partnership with BIS (Department for Business, Innovation & Skills), Local Enterprise Partnerships and
other key regional stakeholders, the YHAHSN will showcase to international parties the strengths and
opportunities available across the UK and specifically the Yorkshire & Humber region.

69
OUTCOMES • Successful identification and marketing of the
key strengths, skills and opportunitiesavailable within the Yorkshire & Humberhealthcare sector
• Increased opportunities for the Yorkshire &Humber region to benefit from new sources ofinvestment
THE ROLE OF THE YHAHSN • Work with NHS commercial directorates to
understand the key strengths and capabilitiesof regional provider organisations. Supportthe identification of high-value opportunitiesavailable to NHS organisations.
• Work collaboratively with internationalhealthcare and trade organisations to promotethe Yorkshire & Humber region as ‘open forbusiness’. Use these relationships to translatethe wider strategic ambitions andopportunities from the international healthsector into tangible opportunities for regionalindustry partners.
• Work closely with, and provide a leadershiprole for, our four Local Enterprise Partnershipsin order to provide a coherent inwardinvestment strategy for the entire region

70
OUTCOMES • Identify, in collaboration with HUK, UKTI and
international colleagues, high-value exportopportunities for regional stakeholders
• Delivery of a successful value-enhancingstrategy for NHS organisations, exploring howthey can capitalise on expertise, IP, skills andlearning available within the NHS. Supportingincreased income to offset the reliance on tax-funded monies for core operational delivery.
THE ROLE OF THE YHAHSN • Work with NHS commercial directorates to
understand the key strengths and capabilitiesof regional provider organisations. Supportthe identification of high-value opportunitiesavailable to NHS organisations. Support thedelivery of international market accesstraining for NHS provider organisations.
• Work collaboratively with internationalhealthcare and trade organisations to promotethe Yorkshire & Humber region as ‘open forbusiness’. Use these relationships to translatethe wider strategic ambitions andopportunities from the international healthsector into tangible opportunities for regionalindustry partners.
• Work with HUK and UKTI to translateinternational healthcare need into tangibleopportunities for UK healthcare organisations
ECONOMIC GROWTH
EXPORTING UK HEALTHCARE EXCELLENCE
Working in partnership with Healthcare UK, UKTI and FCO
(Foreign & Commonwealth Office) the YHAHSN will
mobilise the UK healthcare sector to identify high-value
international opportunities that support growth, income
generation and export opportunities for industry partners,
healthcare providers and leading academic institutes from
across the region and the UK.

71

72
4 RISKS
Risks Mitigation
A constantly changing environment: The environment in which the YHAHSN isoperating is changing. Five Year Forward Viewhas set out the direction of travel and changewithin the NHS, but additional external influencessuch as the political landscape and economicclimate are harder to predict.
We have worked hard to ensure that our plans arealigned with the long-term strategy of NHSEngland and are working with members in aparallel method, improving current systems, whilstsupporting future systems and methods of care.Whilst political and economic influences cannot bepredicted, as an organisation we need to ensurewe are flexible and respond quickly to situations.Our company, board and organisational structureis set up to allow us to react quickly and withoutthe restrictions that being hosted by a third partycould impose.
Overcoming barriers to change: In order to implement improvements, areas toimprove have to be identified. For front-line staffthis could be discouraging and have negativeconsequences, one of which could be resistanceto change. Changing the culture within anorganisation, whether it be within a team or wider,is a complex and difficult issue.
The IA has already shown its ability to implementchange within small teams and at scale and has anexcellent track record. The opportunities createdby the YHAHSN through our Improvement Fellowand Innovation Scout Network create positivereinforcement and ensure change is broughtabout from within and not forced on teams. Theprojects within the plan have been aligned tomembers’ needs and requirements, which shouldhelp ensure organisational buy-in.
Lack of stakeholder engagement: There are a number of projects within the businessplan that require stakeholder engagement,whether that be from delivery partners or memberorganisations. We know financial, personnel andtime resources are stretched within the systemand that is an obstacle which must be overcomefor the success of many projects.
One of the YHAHSN’s capabilities is our ability toengage with partners and create time to think forour members. Communication with partners willneed to show that additional pressures on finance,staff and time in the short term will be for long-term gain. The use of robust evidence, casestudies, health economics and testimonials fromlive pilot sites will be key tools in overcoming thisobstacle.
Standing out from the system noise: There are many organisations that have suggestedthey have answers to problems within the NHS,from both the public and private sectors. Ensuringthat the work of the YHAHSN stands out from thesystem noise and is viewed as integral to theneeds of the regional health economy is crucial forthe plan to succeed.
Throughout the planning process the YHAHSNhas engaged with members to ensure the planmatches the region’s needs. Our role as “honestbroker” is key to ensuring that our offering is seenas different to that of others. Our ability to providehealth economics and an evidence base tosupport decision making will help ensure that ourservices are viewed as integral to the system.

73
5 APPENDIX
5.1 COMPANY INFORMATION
Yorkshire & Humber Partners Academic Health Science Network
Company Number: 08887451
Registered office address:
12 Navigation Court
Calder Park Business Park
Wakefield
West Yorkshire
WF2 7BJ
Directors registered at Companies House:
Andrew Cash
Christine Outram
William Pope
Andrew Riley

E: [email protected]: www.yhahsn.org.uk
t: @AHSN_YandH
Unit 12 Navigation Court, Calder Park, Wakefield, WF2 7BJ
A company limited by guaranteeregistered in England and Wales No 08887451
Licensed by NHS England

Excerpt from CCG assurance: delegated functions self-certification 2015/16. Publications Gateway reference: 03808
Appendix(2)
CCG Assurance Framework 2015/16 Delegated Functions - Self-certification
CCG Name or joint committee of CCGs Rotherham Quarter/year to which certification applies Q1 15/16 1. Assurance Level To support ongoing dialogue, CCGs are asked to provide a self-assessment of their level of assurance for each Delegated Function (as appropriate) . Assurance Level Change since last period Delegated commissioning Assured as good Not applicable OOH commissioning Assured as good Not applicable 2. Outcomes Briefly describe progress in last quarter towards the objectives and benefits the CCG set out in taking on delegated functions, in particular the benefits for all groups of patients <maximum 200 words> Since delegated in April 2015, the CCG has developed a GP strategy and workforce plan, consulting with patients and carers via events and PPGs and GPs via protected learning time and commissioner events. The strategy and workforce plan have been approved at the Primary Care Sub-committee. Rotherham is now working on the estates strategy with NHS property co. with focus on specific projects. 3. Governance and the management of potential conflicts of interest in
relation to primary care co-commissioning (this section should be completed by those CCGs which undertake joint commissioning with NHS England as well as those that have delegated commissioning arrangements)
Co-commissioning OOH commissioning Have any conflicts or potential conflicts of interest arisen during the last quarter?
Yes No
If so has the published register been updated?
Yes No
Is there a record in each case of how the conflict of interest has or is planned to be managed?
Yes Not applicable

Excerpt from CCG assurance: delegated functions self-certification 2015/16. Publications Gateway reference: 03808
Please provide brief details below and include details of any exceptions during the last quarter where conflicts of interest have not been appropriately managed <maximum 200 words> 4. Procurement and expiry of contracts Briefly describe any completed procurement or contract expiry activity during the last quarter in relation the Delegated Functions and how the CCG used these to improve services for patients (and if and how patients were engaged). <maximum 250 words per Delegated Function> The GP OOH contract is currently scheduled to terminate in November 2015. Rotherham CCG has taken the decision to extend the contract for a further three years with an intention to procure the service in 2018. Rotherham CCG is currently developing a new service model for urgent and emergency care based around a new-build Emergency Centre. It is currently unclear what the final service model for OOH services will look like so it would be difficult to procure a new service at this stage. Also, Care UK, our GP OOH provider, is one of the key partners involved in the development of the Emergency Centre. It would be disruptive to the Emergency Centre programme if RCCG were to go out to procurement and potentially change provider. There is a need to create a contracting environment where provider partners are totally focused on the emerging service model. Local Incentive Schemes Is the CCG offering any Local Incentive Schemes to GP practices?
Yes
Was the Local Medical Committee consulted on each new scheme?
Yes
If any of those schemes could be described as novel or contentious did the CCG seek input from any other commissioner, including NHS England, before introducing?
No
Do the offered Local Incentives Schemes include alternatives to national QOF or DES? If yes, are participating GP practices still providing national data sets?
No Choose an item.
What evidence could be submitted (if requested) to demonstrate how each scheme offered will improve outcomes, reduce inequalities and provide value for money? <maximum 250 words for each Delegated Function> The Local schemes are primarily driving appropriate activities from secondary to primary care e.g. dermatology, joint injections, phlebotomy, anti-coagulation facilitating care closer to home. Care home assignment and case management are also central to Rotherham’s strategy for improving and providing consistency in patient care.

Excerpt from CCG assurance: delegated functions self-certification 2015/16. Publications Gateway reference: 03808
5. Availability of services Briefly describe any issues raised during the last quarter impacting on availability of services to patients (include if and how patients were engaged). <maximum 250 words for each Delegated Function> Delegated
commissioning OOH commissioning
How many providers are currently identified by the CCG for review for contractual underperformance?
0 0
And of those providers, how many have been reviewed and there is action being taken to address underperformance?
N/A N/A
During the last quarter were any providers placed into special measures following CQC assessment?
No No
If yes, please provide brief details of each case and how the CCG is supporting remediation of providers in special measures <maximum 50 words per case> In the last 12 months has the CCG published benchmarked results of providers OOH performance (including Patient experience)
No
If yes, please provide link to published results: 6. Internal audit recommendations Co-commissioning OOH commissioning Has internal audit reviewed your processes for completing this self-certification since the last return?
No No
If so, what was their conclusion and recommendations for improvement? <maximum 200 words for each Delegated Function> Use this space to detail any other issues or highlight any exemplar practice supporting assurance as outstanding Rotherham has encouraged central NHS England review of Rotherham’s general practice arrangements since delegation. This commenced however has had to cease

Excerpt from CCG assurance: delegated functions self-certification 2015/16. Publications Gateway reference: 03808
due to work commitments at NHS England. Feedback had been positive in relation to the primary care sub-committee arrangements and strategic direction.

Excerpt from CCG assurance: delegated functions self-certification 2015/16. Publications Gateway reference: 03808
7. CCG declaration
I hereby confirm that the CCG has completed this self-certification accurately using the most up to date information available and the CCG has not knowingly withheld any information or misreported any content that would otherwise be relevant to NHS England assurance of the Delegated Functions undertaken by the CCG. I confirm that the primary medical services commissioning committee remains constituted in line with statutory guidance. I additionally confirm that the CCG has in place robust conflicts of interest processes which comply with the CCG’s statutory duties set out in the NHS Act 2006 (as amended by the Health and Social Care Act 2012), and the NHS England statutory guidance on managing conflicts of interest. Signed by [insert name] CCG Accountable Officer / Chair of joint committee (delete as appropriate) Name: Position: Date: Signed by [insert name] Audit Committee Chair Name: Position: Date:
Please submit this self-certification to your local NHS England team and copy to [email protected] using the email subject ‘Delegated functions self-certification.’

High quality care for all, now and for future generations
Publications Gateway Ref No. 03863
Dear Colleague As you will be aware, allegations have been made that a number of individuals in the NHS may have acted inappropriately in dealings with pharmaceutical companies. Whilst recognising that this is not solely an issue for CCGs, I am writing to seek your assurance that within your CCG:
• You have in place and operate appropriate systems and processes to ensure that conflicts of interest or potential conflicts of interest are declared and mitigated.
• You have appropriate registers in place to register any declared conflicts of interest, gifts and hospitality, and that these are kept up to date.
• You have a code of conduct (or similar code) in place for your CCG which defines required standards of behaviour for individuals working within your organisation, and those performing or authorising activities or advisory duties on your behalf, and that this has been properly communicated to all relevant personnel.
• That your code of conduct specifically covers an employee/member’s responsibility in relation to hospitality and gifts, and has regard to the Professional Standards Authority document Standards for Members of NHS Boards and Clinical Commissioning Group Governing Bodies in England, and the NHS Business Services Authority guidance Standards of Business Conduct Procedure, (HSG (93)5), as well as the Nolan principles.
• In making your arrangements and discharging your functions, you have due regard to NHS England’s published guidance on conflicts of interest.
• The arrangements you have in place ensure that the integrity of CCG decision-making processes is not affected.
• All of the above are appropriately and regularly monitored and assured by your audit committee and form part of your regular assurance.
• No individual employed by the CCG, including members of the CCG Governing body, is currently acting outwith your policies.
Whilst I know you will want to assure yourself that there are no issues which require your immediate attention, I am sure you will also want to undertake a more comprehensive review of all your systems and process.
28 July 2015
Office of the National Director:
Commissioning Operations Quarry House
Quarry Hill LEEDS LS2 7UE
CCG Accountable Officers in England

High quality care for all, now and for future generations
I would be grateful if, as Accountable Officer, you could provide your assurance on the above points after that full and comprehensive review to your local NHS England Director of Commissioning Operations, or to David Mallett (copied to Simon Weldon) for CCGs in London, by Friday 28 August 2015, in order that we can have confidence nationally that all appropriate systems and processes are in place and they are actively being utilised. I have asked for the same assurance from all CSU Managing Directors and in addition, working with other parts of the NHS, we are reviewing the current guidance and will provide an update if it would appear that is necessary.
Best wishes
Dame Barbara Hakin National Director: Commissioning Operations Copy: Moira Dumma, Director of Commissioning Operations, NHS England North, (Yorkshire & the Humber) Graham Urwin, Director of Commissioning Operations, NHS England North, Clare Duggan, Director of Commissioning Operations, NHS England North, (Cheshire & Merseyside) Tim Rideout, Director of Commissioning Operations, NHS England North, (Cumbria & the North East) Wendy Saviour, Director of Commissioning Operations, NHS England Midlands & East, (North Midlands) Andrew Pike, Director of Commissioning Operations, NHS England Midlands & East, (East) Andrew Reed, Director of Commissioning Operations, NHS England Midlands & East (West Midlands) Elliott Howard-Jones, Director of Commissioning Operations, NHS England Midlands & East (Central Midlands) Anthony Farnsworth, Director of Commissioning Operations, NHS England South (South West) Felicity Cox, Director of Commissioning Operations, NHS England South (South East), Rachel Pearce, Director of Commissioning Operations, NHS England South (South Central) Dominic Hardy, Director of Commissioning Operations, NHS England South (Wessex) Simon Weldon, Regional Chief Operating Officer, NHS England London David Mallet, Head of Reconfiguration, NHS England London Richard Barker, Regional Director, NHS England North Paul Watson, Regional Director, NHS England Midlands & East Anne Rainsberry, Regional Director, NHS England London Andrew Ridley, Regional Director, NHS England South

Conflicts of Interest – RCCG Assurance Return
Name of CCG – Rotherham CCG
Requirement Response Comment
1a There are systems & processes in place within the CCG to ensure conflicts of interest are declared and mitigated
Yes
All Employees (including GPs) and member practices submit the declaration of interest form in April each year. This is compiled and sent to Governing Body and Published on the website. Governing Body in public session receive Quarterly updates through the corporate assurance report.
1b The CCG’s systems and processes have due regard to NHS England’s guidance on conflicts of interest Yes
The COI policy was updated in January 2015 and is based on NHSE guidance. It was approved by Governing Body in February 2015
2a There is a conflict of interest, hospitality and gifts register in place Yes
Guidance for staff is in the standards of business conduct policy
2b Frequency with which the register is updated?
Quarterly updates to Governing Body
3a There is a code of conduct for employees and governing body members Yes
3b The code of conduct covers hospitality and gifts Yes
3c The code of conduct has due regard to the three national documents referenced in the Barbara Hakin letter
Yes
4 The overall arrangements (1-3) do not impact on the integrity of the CCGs decision making
Yes
Every decision making meeting records conflicts of interest and excludes conflicted members from decision making
5 These arrangements (1-3) are subject to monitoring by the Audit Committee and are reviewed as part of the CCG’s overall assurance processes.
Yes
6 All individuals employed by the CCG or on the Governing Body are currently acting within these policies and procedures
Yes
The CCG is currently reviewing how policies are being implemented to ensure best practice is followed at all times. Refresher training for all staff will be completed during August.
Name of Accountable Officer completing this template
Chris Edwards
Date 31/07/2015

Page 1 of 1
Changes to NHS Constitution The NHS constitution was first published in March 2012 and It is due to be refreshed fully in March 2023. However the Constitution was updated in July 2015; this paper notes those changes. 1.1 ‘with equal regard ‘ added in respect of mental health
1.4 ‘the patient will be’ at the heart (changed from aspire to be). Also a sentence has been added re Armed forces covenant, ensuring Veterans will not be disadvantaged Section 3a contains several additional legal rights • ‘you have the right to receive care and treatment appropriate to you, meets your needs and
reflects your preferences’. This right reflects the new fundamental standard about person-centred care, which is set out in regulation 9 of the Health and Social Care Act 2008. The purpose of the ‘person-centred care’ fundamental standard is to ensure that providers of health and adult social care services, plan and provide patient care and treatment by meeting the following criteria: be appropriate, meet their needs, and reflect their preferences.
• Waiting times are detailed in the Handbook to the Constitution, alongside the Mental Health ‘waits’ from
March 2016. It also notes the exception to waiting times for obese patients where ‘weight loss’ will improve prognosis
• You have the right to be ‘cared for in a clean safe secure and suitable environment’; And ‘to receive suitable and nutritious food and hydration to sustain good health and wellbeing’. The latter is based on the new fundamental standard about nutrition and hydration, which is set out in regulations 9, 14 and 17 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014.
• You have the right ‘to be protected from abuse and neglect and care and treatment that is degrading’. This new right is based on the fundamental standard requiring providers registered with CQC to protect people from abuse and improper treatment set out in regulation 13 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014. The standards are legal requirements that all NHS providers, must meet.
• You have the right to ‘transparent, accessible and comparable data on the quality of local health care providers and on outcomes as compared nationally’. This is likely to be addressed through NHS Choices data, Friends and Family Test data, MY NHS, and the requirement that providers display CQC quality ratings.
• You have the right ‘to be involved in planning and making decisions about your health and care with your care provider this includes ‘being given the chance to manage your own care if appropriate’.
• Also ‘you have the right to an open and transparent relationship with the organisation providing your care. You must be told about any safety incident relating to your care which has or….. could cause harm or death, etc’ This came into force for FTs and trusts last year, and is now rolled out to all providers.
Section 4b – there are no changes to the legal duties for staff, but there are additional ‘expectations’; staff should aim ‘to provide all patients with safe care and do all they can to protect patients’; ‘follow guidance, standards etc’ and ‘find alternative sources of care or assistance for patients when you are unable to provide this, including for those patients who are not receiving basic care to meet their needs’