joint meeting of nhs mansfield and ashfield ccg … · joint nhs mansfield and ashfield ccg and nhs...
TRANSCRIPT

JOINT MEETING OF NHS MANSFIELD AND ASHFIELD CCG AND NHS
NEWARK AND SHERWOOD CCG GOVERNING BODIES
TITLE: CCG Restricted and Not Funded Policies DATE OF MEETING: 8 March 2017 PAPER REF: JGB/17/55 AUTHOR: Susan Bateman
Rosa Waddingham Elaine Moss
PRESENTER: Elaine Moss
PURPOSE OF REPORT: To note the Restricted and Not Routinely Funded Policies, including the arrangements for consideration of special cases. EXECUTIVE SUMMARY: These policies replace the current East Midlands Procedures of Limited Clinical Value and Cosmetics policies. The CCG policies have been previously discussed at the Clinical and Cost Effectiveness Committee, the Clinical Executive and the February Governing Body meeting. The changes requested through these committees have been incorporated into the final policies. RECOMMENDATION:
To note to approve To agree the recommendation (see details below) REPORT: At the February Governing Body a number of elements of clarification or additional work were requested along with actions taken: A panel process was required: The special case process has been drafted and will be presented to Governing Body in April. It provides a clear process for considering funding requests where a service, intervention or treatment falls outside existing service agreements. This process will ensure that each request for individual funding is considered in a fair and transparent way, with decisions based on the best available evidence and in accordance with the CCG commissioning principles. Membership of the panel includes lay member, public health, GP, pharmacy, nurse and administrative support. Engagement with the public and practitioners is required to implement the policy: Clear messages have been developed and a FAQ leaflet is under development. Messages on the change and links to the policies have been shared with Citizens Reference Panel, Stakeholder Reference Group, providers and other commissioners. The policies and criteria have been published on the CCGs’ websites and can be found at: http://www.mansfieldandashfieldccg.nhs.uk or http://www.newarkandsherwoodccg.nhs.uk Further work will continue in light of questions and feedback. Changes to commissioning principles: These have been amended. That the policies were to be reviewed in one year: this is amended in the new policies attached. They will be reviewed annual or earlier if quality oversight or the special circumstances panel identify any unwanted, unexpected consequences.
That adverse events are to be monitored: These policies will be monitored through the Quality Team via patient, contract, and GP concerns, along with significant incidents, which along with any evidence of a significant number of panel requests for a particular procedure, will prompt a review of the policies. Enacting the policies will be undertaken swiftly through the contracting process with implementation taking place from 1 April 2017: a clear next steps plan has been developed. KEY IMPLICATIONS: FINANCIAL Both Not Routinely funded policy and policy will contribute to delivery of
the QIPP VALUE FOR MONEY All procedures included in the policy have been assessed as having no
or have limited clinical effectiveness and therefore there are best use of the finite resource for health care within Mansfield and Ashfield and Newark and Sherwood.
RISK All of the included procedures are already restricted elsewhere in England. These policies will only be effective if they are well adopted, robustly processed and audited. The special case panel and quality oversight will ensure that any unexpected consequences can be managed promptly and robustly.
LEGAL There is no indication that the restrictions proposed would generate any legal challenge given that there is a clear process for managing exceptionality and all are in force elsewhere in England.
WORKFORCE Implementation, support and, monitoring of the additional restrictions will add additional workload to the CCG team, this will be monitored as the policy is implemented. Discussion with providers on implications of additions to the policy will take place via contracting meetings.
PATIENT AND PUBLIC INVOLVEMENT
Engagement sessions conducted in September 2016 Lay members at CCG committees
CLINICAL ENGAGEMENT Clinical and Cost Effectiveness Committee, Clinical Executive COMMITTEES CONSULTED PRIOR TO GOVERNING BODY
Finance, delivery and Performance Group Clinical Cost Effectiveness Committee Clinical Executive Governing Bodies
HOW DOES THIS CONTRIBUTE TO THE OUTCOMES AND OBJECTIVES OF THE CCG:
Quality Health Financial Clinical Performance (tick as appropriate)
CONFLICTS OF INTEREST:
This is a recommended action to be agreed by the Chair at the beginning of the item. No conflict identified Conflict noted, conflicted party can participate in discussion but not decision (see below) Conflict noted, conflicted party can remain but not participate (see below) Conflicted party is excluded from discussion (see below)
This paper is not a paper for decision, however if decisions are made subsequently in the meeting, it requires noting that all GPs and the secondary care specialist are conflicted due to the potential of a direct pecuniary interest; and Mr Robinson has expressed a personal conflict
of interest.
CONFIDENTIALITY:
Is the information in this paper confidential? No Yes ANNEXES:
• Service Restriction Policy • Service Restriction Policy supporting information • Procedures not routinely funded Policy

1
Policy for Procedures Not Routinely Funded
Document purpose
This policy lists all the procedures that are not routinely funded by NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG. This policy is based on and superseded the Nottinghamshire (less Bassetlaw) Procedures of Limited Clinical Value Policy 2015 and the East Midlands Cosmetics Policy 2015.
Version Version 1.0 Final
Title Policy for Procedures Not Routinely Funded
Associated Policy
Service Restriction Policy (2017)
Nominated Lead
Chief Nurse and Director of Quality and Governance
Approval Date 16.2.17
Approving Committee
Joint NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Governing Body
Review Date This policy will be reviewed in 1 year or earlier if additions or changes
are required.
Groups/staff Consulted
Joint NHS Mansfield and Ashfield CCG and NHS Newark and
Sherwood CCG Clinical and Cost Effectiveness Committee
Joint NHS Mansfield and Ashfield CCG and NHS Newark and
Sherwood CCG Clinical Executive Committee
Joint NHS Mansfield and Ashfield CCG and NHS Newark and
Sherwood CCG Governing Body
Target audience All CCG staff
All providers All Clinicians
Circulation list CCG Websites All providers Primary Care Clinicians Associated
documents Individual Funding Requests (IFR) V2 April 2011

2
Contents
Purpose of the policy ........................................................................................................................... 7
Introduction ............................................................................................................................................ 7
Commissioning Principles ................................................................................................................... 7
Policy Exclusions .................................................................................................................................. 7
Exceptionality and Special Circumstances ...................................................................................... 8
Statement of Cosmetic Procedures ................................................................................................... 8
List of procedures covered under this policy .................................................................................... 9
Description of Procedure/Treatment ............................................................................................. 9
Abdominoplasty (Apronectomy/ Panniculectomy) ...................................................................... 9
Acupuncture for non-specific low back pain of up to 1 year duration- complimentary
therapy ............................................................................................................................................... 9
Acupuncture for all other purposes (see above) - complimentary therapy ............................. 9
Aesthetic operations on the umbilicus .......................................................................................... 9
Alternative therapies not explicitly listed in this policy ................................................................ 9
Alexander technique- complimentary therapy ............................................................................. 9
Anal rectal skin tags ......................................................................................................................... 9
Applied kinesiology-complimentary therapy ................................................................................. 9
Aromatherapy- complimentary therapy ......................................................................................... 9
Autogenic training- complimentary therapy .................................................................................. 9
Autologous Chondrocyte Implantation (ACI) - complimentary therapy .................................... 9
Ayurveda- complimentary therapy ................................................................................................. 9
Back pain - Facet joint injections ................................................................................................... 9
Benign skin lesions – cosmetic ...................................................................................................... 9
Blepharoplasty/ Brow Lift Face brow lift /Ptosis surgery -cosmetic .......................................... 9
Body Contouring – cosmetic ........................................................................................................... 9
Botulinum Toxin Treatment, lontophoresis or surgical treatments for Axillary Hyperhidrosis
............................................................................................................................................................ 9
Botulinum Toxin treatment for wrinkles frown lines or aging neck- cosmetic ......................... 9
Brachioplasty/Upper arm lift - cosmetic ........................................................................................ 9
Breast Enlargement/augmentation asymmetry surgery Female............................................... 9
Breast implant removal / reinsertion ............................................................................................ 10
Breast Reduction- cosmetic .......................................................................................................... 10

3
Breast Uplift - cosmetic ................................................................................................................. 10
Buttock Lift- cosmetic ..................................................................................................................... 10
Calf implants – cosmetic ............................................................................................................... 10
Removal of Chalazion ................................................................................................................... 10
Cheek Implants – cosmetic (except in post-trauma cases and/ or part of planned
reconstruction following surgery e.g. for cancer ........................................................................ 10
Chemical peels- cosmetic ............................................................................................................. 10
Chin implant (genioplasty, mentoplasty) - cosmetic ................................................................. 10
Chinese medicine- complimentary therapy ................................................................................ 10
Chiropractic therapy – complimentary therapy .......................................................................... 10
Cholecystectomy for asymptomatic gallstones - Where there are no symptoms,
cholecystectomy confers no benefit to patients with asymptomatic gallstones, even in
patients with one attack of uncomplicated gallstone pain. ....................................................... 10
Only funded for patients at risk of developing gallbladder carcinoma or gallstone
complications – special cases process will apply ...................................................................... 10
Circumcision for non-medical reasons- cosmetic ...................................................................... 10
Collagen implant- cosmetic (except in post-trauma cases and/ or part of planned
reconstruction following surgery e.g. for cancer ........................................................................ 10
Congenital pigmented lesions on the face (removal of) ........................................................... 10
Correction of deviated septum (see surgical treatment of snoring) ........................................ 10
Cranial banding for positional plagiocephaly- cosmetic ........................................................... 10
Dermabrasion of skin -cosmetic ................................................................................................... 11
Diagnostic investigations for Irritable Bowel Syndrome (IBS) ................................................. 11
The following tests will not be funded for confirmation of diagnosis in adults who meet the
IBS diagnostic criteria: ................................................................................................................... 11
Ultrasound ....................................................................................................................................... 11
Rigid/flexible sigmoidoscopy ........................................................................................................ 11
Colonoscopy; barium enema ........................................................................................................ 11
Thyroid function test ....................................................................................................................... 11
Faecal ova and parasite test ........................................................................................................ 11
Faecal occult blood ........................................................................................................................ 11
Hydrogen breath test ..................................................................................................................... 11
Earlobe repair-cosmetic ................................................................................................................ 11
Electrolysis - cosmetic ................................................................................................................... 11
Environmental medicine-complimentary medicine .................................................................... 11

4
Removal of Epidermoid/Pilar (Sebaceous) Cysts. .................................................................... 11
Epidural injections of non-radicular pain ..................................................................................... 11
Epidural injections of non-specific low back pain ...................................................................... 11
Excimer laser for Astugmatism and Xanthelasma .................................................................... 11
Excimer laser for corneal erosions .............................................................................................. 11
Excision of excessive skin from thigh, leg, hip, buttock, arm, forearm or other areas ........ 11
Extracorporeal shock-wave therapy for planta fasciitis ............................................................ 11
Face lifts –cosmetic (unless part of the treatment of facial nerve palsy/ congenital facial
abnormalities/treatment of specific facial skin condition e.g. cutis laxa, pseudoxanthoma
elasticum) ........................................................................................................................................ 11
Fat Grafts- cosmetic ....................................................................................................................... 12
Forearm implants – cosmetic ....................................................................................................... 12
Hair depilation (removal) for excessive hair growth (hirsutism) –cosmetic ........................... 12
Hair transplant/ Hair graft/ Hair replacement/ Intralace hair system for abnormal hair loss -
cosmetic ........................................................................................................................................... 12
Healing- complimentary therapy .................................................................................................. 12
Herbal medicine – complimentary therapy ................................................................................. 12
Hip resurfacing ................................................................................................................................ 12
Homeopathy- complimentary medicine ...................................................................................... 12
Hydrotherapy unless part of an established care package ...................................................... 12
Hymen reconstruction- cosmetic.................................................................................................. 12
Hypnosis- complimentary therapy ............................................................................................... 12
Joint revisions – including hip and knee. The commissioner will only fund revisions using
standard prosthesis ........................................................................................................................ 12
Knee - Diagnostic Arthroscopy ..................................................................................................... 12
Labial reduction/ labiaplasty ......................................................................................................... 12
Laser - general ................................................................................................................................ 12
Laser Treatment for skin conditions causing scarring including post acne and post
traumatic scarring - cosmetic ....................................................................................................... 12
Laser Treatment for facial hyperpigmentation- cosmetic ......................................................... 12
Laser treatment for myopia ........................................................................................................... 12
Laser Treatment/ therapy/ tunable dye laser for aesthetic reasons ....................................... 12
Lipoma (removal of) ....................................................................................................................... 12
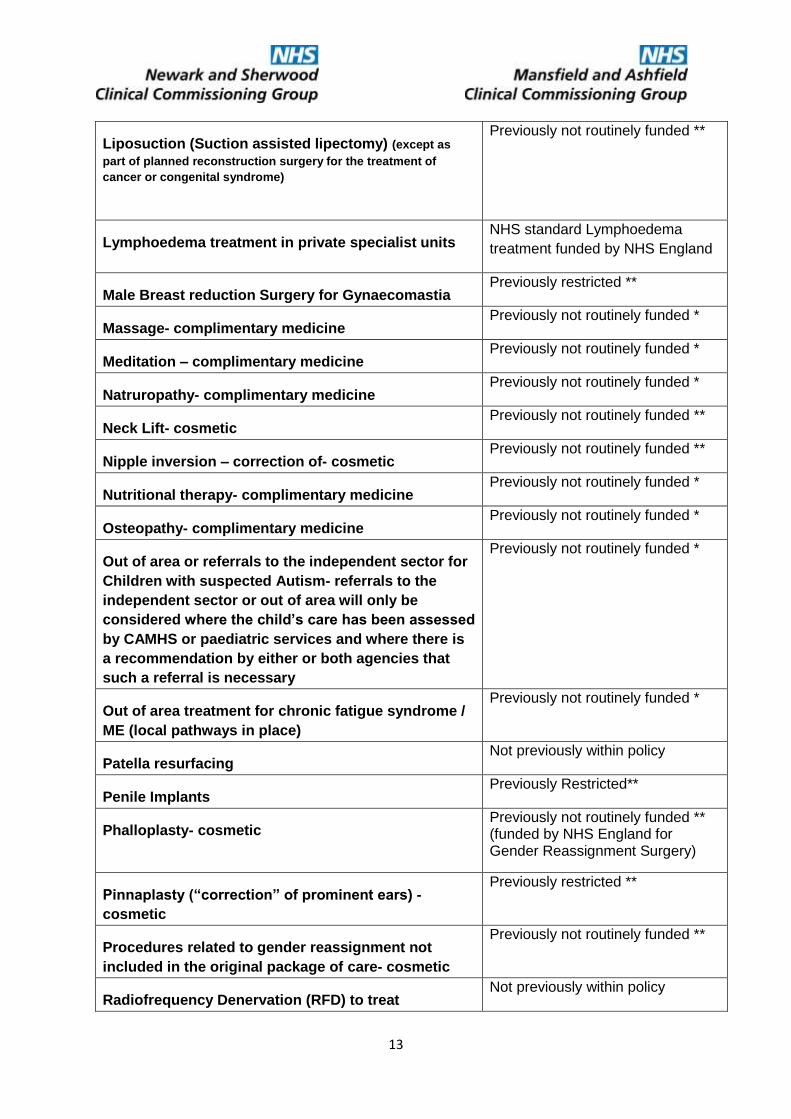
Liposuction (Suction assisted lipectomy) (except as part of planned reconstruction surgery
for the treatment of cancer or congenital syndrome) ................................................................ 13

5
Lymphoedema treatment in private specialist units .................................................................. 13
Male Breast reduction Surgery for Gynaecomastia .................................................................. 13
Massage- complimentary medicine ............................................................................................. 13
Meditation – complimentary medicine ......................................................................................... 13
Natruropathy- complimentary medicine ...................................................................................... 13
Neck Lift- cosmetic ......................................................................................................................... 13
Nipple inversion – correction of- cosmetic .................................................................................. 13
Nutritional therapy- complimentary medicine ............................................................................. 13
Osteopathy- complimentary medicine ......................................................................................... 13
Out of area or referrals to the independent sector for Children with suspected Autism-
referrals to the independent sector or out of area will only be considered where the child’s
care has been assessed by CAMHS or paediatric services and where there is a
recommendation by either or both agencies that such a referral is necessary .................... 13
Out of area treatment for chronic fatigue syndrome / ME (local pathways in place) ........... 13
Patella resurfacing ......................................................................................................................... 13
Penile Implants ............................................................................................................................... 13
Phalloplasty- cosmetic ................................................................................................................... 13
Pinnaplasty (“correction” of prominent ears) - cosmetic........................................................... 13
Procedures related to gender reassignment not included in the original package of care-
cosmetic ........................................................................................................................................... 13
Radiofrequency Denervation (RFD) to treat osteoidostemoma .............................................. 13
Reflexology – complimentary medicine ...................................................................................... 14
Reiki- complimentary medicine .................................................................................................... 14
Removal of anal/ rectal skin tags ................................................................................................. 14
Removal of excess skin following weight loss whether through surgery or natural means 14
Removal of Supernumerary Nipples (Polymastia) .................................................................... 14
Repair of chronic clefts due to avulsion of body piercing ......................................................... 14
Repair of chronic tear of lobe of external ear ............................................................................. 14
Residential pain management programmes .............................................................................. 14
Reversal of Female Sterilization .................................................................................................. 14
Reversal of Vasectomy ................................................................................................................. 14
Scar Reduction including skin grafts for scars cosmetic .......................................................... 14
Septo-Rhinoplasty or Rhinoplasty ............................................................................................... 14
Shiatsu- complimentary medicine ................................................................................................ 14

6
Submental Lipectomy (neck lift) ................................................................................................... 14
Surgery for divarication of the abdominal rectus ....................................................................... 14
Surgical procedures to correct rhinophyma "bulbous nose" or "phymatous rosacea" ........ 14
Surgical reduction of the tongue (see surgical treatment for snoring) ................................... 14
Surgical treatment for myopia or short sight .............................................................................. 14
Surgical Treatment for Snoring .................................................................................................... 14
Surgical treatment of Lipoma ....................................................................................................... 14
Surgical treatment of Myopia ........................................................................................................ 14
Tattoo removal ................................................................................................................................ 14
Therapeutic community method for treatment of borderline personality disorder ................ 14
Therapeutic use of ultrasound in hip and knee osteoarthritis .................................................. 15
Tonsillectomy as a treatment for snoring .................................................................................... 15
Toric Intraocular Lens Implant for Astigmatism ......................................................................... 15
Trigger finger (non-surgical treatment is funded by commissioners) ..................................... 15
Vaginoplasty- cosmetic ................................................................................................................. 15
X-ray (plain) of back for low back pain ........................................................................................ 15
Annex A – Individual Funding Request (IFR) policy ........................ Error! Bookmark not defined.

7
Purpose of the policy The purpose of this policy is to ensure that the Mid Nottinghamshire Clinical Commissioning Groups (the Commissioner) only fund treatment for clinically effective interventions that are then delivered to the right patients. It sets out the treatments deemed to be of insufficient priority to justify funding from the available fixed budget. This policy lists a number of procedures and services that Mansfield and Ashfield and Newark and Sherwood Clinical Commissioning Groups do not routinely fund.
If a provider undertakes one of the procedures contained within this policy commissioners will not pay unless explicit agreement has been given by the appropriate CCG.
This policy should be read in conjunction with the policy for Service Restriction Policy (2017). These two policies have been based on and include all the procedures that were part of the Procedures of Limited Clinical Value Policy (2015) or the East Midlands Cosmetic Policy (2015) which has now been superseded.
Approved prescribing of medicines falls outside the scope of this document and is covered in the guidelines and protocols produced by the Nottinghamshire Area Prescribing Committee. Further information can be obtained from the Pharmacy/Medicines Management Department or via www.nottsapc.nhs.uk.
Introduction This policy identifies procedures that the Mid Nottinghamshire CCGs do not routinely fund. These procedures have either previously been identified as not routinely funded in the Procedures of Limited Clinical Value 2015, East Midlands Cosmetics Policy 2015, or are new to Mid Nottinghamshire CCGs but have been adopted where the procedures are not routinely commissioned in a number of other CCGs
Commissioning Principles Commissioning decisions are made in accordance with the general principles set out below:
Clear evidence of clinical and cost effectiveness will be sought before NHS resources are invested in the treatment
The cost of the treatment for individual patients and others within any anticipated cohort is a relevant factor.
The extent to which the individual or patient group will gain a benefit from the treatment will be considered and balanced against the benefit which could be gained by alternative investment possibilities to meet the needs of the community
The process and policies will consider all relevant national standards, take into account all proper and authoritative guidance along with due regard to the funding available for local health services.
Policy Exclusions Patients should not be referred for or undergo the procedures listed in this policy, except in the case of:
Emergency, OR
A reasonable suspicion of cancer, OR
As part of reconstruction following treatment for cancer, traumatic injury or the correction of congenital malformation
Exceptional or Special circumstances (which will need explicit CCG

8
approval – see exceptionality and special consideration).
Exceptionality and Special Circumstances The Commissioner will consider individual cases for the funding of procedures set out in this commissioning policy where the Individual Funding Request Policy does not apply. Where the patient meets the following criteria and relevant evidence is available, clinicians may apply for individual funding related to the procedures covered by this policy.
Exceptionality
Patient is significantly different to a group of patients with the condition in question and at the same progression of the condition AND likely to gain significantly more clinical benefit than others in the group of patients with the condition in question and at the same stage of progression of the condition.
Evidence of clinical effectiveness
All other relevant commissioned therapies/treatments been tried
Anticipated clinical benefits in the individual case of the particular treatment requested are over and above all other available options
If more than one episode of treatment is required, it is clear how benefits of the procedure/treatment will be demonstrated/measured including what the intended outcomes are, what ‘stopping’ criteria would be used and how will it be measured.
Evidence of individual patient safety
Standard treatments (those available to other patients with this condition/stage of the disease) are not appropriate for this patient for clinical reasons.
Implementation and Compliance
The policy will be implemented across providers in primary and secondary care. It will be formally incorporated into contracts and will be subject to routine monitoring for compliance.
Statement of Cosmetic Procedures "Cosmetic" surgery means procedures to improve appearance. It is also known as "aesthetic" surgery. Conditions resulting from major trauma or burns, which need reconstructive surgery, will usually be funded by the NHS.
This policy lists many procedures that are judged to be cosmetic and will not normally be funded by the NHS. This policy applies to cosmetic surgery irrespective of the sub specialty of the surgeon concerned, including plastic surgery, ear nose and throat surgery, oral and maxillofacial surgery, dermatology, and other surgical specialties.

9
List of procedures covered under this policy
Description of Procedure/Treatment Status under previous East Midlands Policies
Abdominoplasty (Apronectomy/ Panniculectomy) Previously restricted *
Acupuncture for non-specific low back pain of up to
1 year duration- complimentary therapy
Previously restricted *
Acupuncture for all other purposes (see above) -
complimentary therapy
Previously not routinely funded *
Aesthetic operations on the umbilicus Not previously within policy
Alternative therapies not explicitly listed in this
policy
Previously not routinely funded *
Alexander technique- complimentary therapy Previously not routinely funded *
Anal rectal skin tags Previously not routinely funded *
Applied kinesiology-complimentary therapy Previously not routinely funded *
Aromatherapy- complimentary therapy Previously not routinely funded *
Autogenic training- complimentary therapy Previously not routinely funded *
Autologous Chondrocyte Implantation (ACI) -
complimentary therapy
Previously not routinely funded *
Ayurveda- complimentary therapy Previously not routinely funded *
Back pain - Facet joint injections Previously restricted *
Benign skin lesions – cosmetic Previously restricted **
Blepharoplasty/ Brow Lift Face brow lift /Ptosis
surgery -cosmetic
Previously restricted **
Body Contouring – cosmetic Previously not routinely funded **
Botulinum Toxin Treatment, lontophoresis or
surgical treatments for Axillary Hyperhidrosis
Previously restricted *
Botulinum Toxin treatment for wrinkles frown lines or
aging neck- cosmetic
Previously not routinely funded **
Brachioplasty/Upper arm lift - cosmetic Previously not routinely funded **
Breast Enlargement/augmentation asymmetry
surgery Female
Previously restricted **

10
Breast implant removal / reinsertion Previously restricted**
Breast Reduction- cosmetic Previously restricted**
Breast Uplift - cosmetic Previously restricted **
Buttock Lift- cosmetic Previously not routinely funded *
Calf implants – cosmetic Not previously within policy
Removal of Chalazion Not previously within policy
Cheek Implants – cosmetic (except in post-trauma
cases and/ or part of planned reconstruction
following surgery e.g. for cancer
Previously not routinely funded **
Chemical peels- cosmetic Not previously within policy
Chin implant (genioplasty, mentoplasty) - cosmetic Previously not routinely funded **
Chinese medicine- complimentary therapy Previously not routinely funded *
Chiropractic therapy – complimentary therapy Previously not routinely funded *
Cholecystectomy for asymptomatic gallstones -
Where there are no symptoms, cholecystectomy
confers no benefit to patients with asymptomatic
gallstones, even in patients with one attack of
uncomplicated gallstone pain.
Only funded for patients at risk of developing
gallbladder carcinoma or gallstone complications –
special cases process will apply
Previously not routinely funded *
Circumcision for non-medical reasons- cosmetic Previously not routinely funded **
Collagen implant- cosmetic (except in post-trauma
cases and/ or part of planned reconstruction
following surgery e.g. for cancer
Previously not routinely funded **
Congenital pigmented lesions on the face (removal
of)
Previously restricted**
Correction of deviated septum (see surgical
treatment of snoring)
Previously not routinely funded *
Cranial banding for positional plagiocephaly-
cosmetic
Previously not routinely funded **

11
Dermabrasion of skin -cosmetic Not previously within policy
Diagnostic investigations for Irritable Bowel
Syndrome (IBS)
The following tests will not be funded for
confirmation of diagnosis in adults who meet the IBS
diagnostic criteria:
Ultrasound
Rigid/flexible sigmoidoscopy
Colonoscopy; barium enema
Thyroid function test
Faecal ova and parasite test
Faecal occult blood
Hydrogen breath test
Previously not routinely funded *
Earlobe repair-cosmetic Previously not routinely funded **
Electrolysis - cosmetic Previously not routinely funded **
Environmental medicine-complimentary medicine Previously not routinely funded *
Removal of Epidermoid/Pilar (Sebaceous Cysts) with
the exception of recurrent infection and size greater
than 0.5cm diameter
Previously restricted
Epidural injections of non-radicular pain Not previously within policy
Epidural injections of non-specific low back pain Previously not routinely funded *
Excimer laser for Astugmatism and Xanthelasma Not previously within policy
Excimer laser for corneal erosions Not previously within policy
Excision of excessive skin from thigh, leg, hip,
buttock, arm, forearm or other areas
Previously not routinely funded **
Extracorporeal shock-wave therapy for planta
fasciitis
Not previously within policy
Face lifts –cosmetic (unless part of the treatment of
facial nerve palsy/ congenital facial
abnormalities/treatment of specific facial skin
condition e.g. cutis laxa, pseudoxanthoma elasticum)
Previously not routinely funded **

12
Fat Grafts- cosmetic Previously not routinely funded **
Forearm implants – cosmetic
Hair depilation (removal) for excessive hair growth
(hirsutism) –cosmetic
Previously not routinely funded **
Hair transplant/ Hair graft/ Hair replacement/ Intralace
hair system for abnormal hair loss - cosmetic
Previously not routinely funded **
Healing- complimentary therapy Previously not routinely funded *
Herbal medicine – complimentary therapy Previously not routinely funded *
Hip resurfacing Previously not routinely funded *
Homeopathy- complimentary medicine Previously not routinely funded *
Hydrotherapy unless part of an established care
package
Not previously within policy
Hymen reconstruction- cosmetic Previously not routinely funded **
Hypnosis- complimentary therapy Previously not routinely funded *
Joint revisions – including hip and knee. The
commissioner will only fund revisions using
standard prosthesis
Previously not routinely funded *
Knee - Diagnostic Arthroscopy Previously not routinely funded *
Labial reduction/ labiaplasty Previously not routinely funded **
Laser - general Previously not routinely funded **
Laser Treatment for skin conditions causing scarring
including post acne and post traumatic scarring -
cosmetic
Previously not routinely funded **
Laser Treatment for facial hyperpigmentation-
cosmetic
Previously restricted **
Laser treatment for myopia Previously not routinely funded *
Laser Treatment/ therapy/ tunable dye laser for
aesthetic reasons
Not previously within policy
Lipoma (removal of)
Previously restricted **
13
Liposuction (Suction assisted lipectomy) (except as
part of planned reconstruction surgery for the treatment of
cancer or congenital syndrome)
Previously not routinely funded **
Lymphoedema treatment in private specialist units NHS standard Lymphoedema
treatment funded by NHS England
Male Breast reduction Surgery for Gynaecomastia Previously restricted **
Massage- complimentary medicine Previously not routinely funded *
Meditation – complimentary medicine Previously not routinely funded *
Natruropathy- complimentary medicine Previously not routinely funded *
Neck Lift- cosmetic Previously not routinely funded **
Nipple inversion – correction of- cosmetic Previously not routinely funded **
Nutritional therapy- complimentary medicine Previously not routinely funded *
Osteopathy- complimentary medicine Previously not routinely funded *
Out of area or referrals to the independent sector for
Children with suspected Autism- referrals to the
independent sector or out of area will only be
considered where the child’s care has been assessed
by CAMHS or paediatric services and where there is
a recommendation by either or both agencies that
such a referral is necessary
Previously not routinely funded *
Out of area treatment for chronic fatigue syndrome /
ME (local pathways in place)
Previously not routinely funded *
Patella resurfacing Not previously within policy
Penile Implants Previously Restricted**
Phalloplasty- cosmetic Previously not routinely funded ** (funded by NHS England for Gender Reassignment Surgery)
Pinnaplasty (“correction” of prominent ears) -
cosmetic
Previously restricted **
Procedures related to gender reassignment not
included in the original package of care- cosmetic
Previously not routinely funded **
Radiofrequency Denervation (RFD) to treat Not previously within policy

14
osteoidostemoma
Reflexology – complimentary medicine Previously not routinely funded *
Reiki- complimentary medicine Previously not routinely funded *
Removal of anal/ rectal skin tags Previously not routinely funded *
Removal of excess skin following weight loss
whether through surgery or natural means
Previously not routinely funded **
Removal of Supernumerary Nipples (Polymastia) Not previously within policy
Repair of chronic clefts due to avulsion of body
piercing
Not previously within policy
Repair of chronic tear of lobe of external ear Previously not routinely funded **
Residential pain management programmes Previously not routinely funded *
Reversal of Female Sterilization Previously not routinely funded *
Reversal of Vasectomy Previously not routinely funded *
Scar Reduction including skin grafts for scars
cosmetic
Previously restricted **
Septo-Rhinoplasty or Rhinoplasty Previously restricted
Shiatsu- complimentary medicine Previously not routinely funded *
Submental Lipectomy (neck lift) Previously not routinely funded **
Surgery for divarication of the abdominal rectus Not previously within policy
Surgical procedures to correct rhinophyma "bulbous
nose" or "phymatous rosacea"
Not previously within policy
Surgical reduction of the tongue (see surgical
treatment for snoring)
Previously not routinely funded *
Surgical treatment for myopia or short sight Previously not routinely funded *
Surgical Treatment for Snoring Previously not routinely funded *
Surgical treatment of Lipoma Previously not routinely funded **
Surgical treatment of Myopia Previously not routinely funded *
Tattoo removal Previously not routinely funded **
Therapeutic community method for treatment of Previously not routinely funded *

15
borderline personality disorder
Therapeutic use of ultrasound in hip and knee
osteoarthritis
Previously not routinely funded *
Tonsillectomy as a treatment for snoring Previously not routinely funded *
Toric Intraocular Lens Implant for Astigmatism Not previously within policy
Trigger finger (non-surgical treatment is funded by
commissioners)
Previously not routinely funded *
Vaginoplasty- cosmetic Previously not routinely funded **
X-ray (plain) of back for low back pain Previously not routinely funded *
* Value-based commissioning: procedures of limited clinical value. A joint commissioning
policy of clinical commissioning groups in Nottinghamshire County (excluding Bassetlaw and Nottingham City) (2015)
** East midlands commissioning policy for cosmetic procedures (2015) Version 2
Annex B – Exceptionality and Special Circumstances Process
Please see Exceptionality and Special Circumstances section. Associated forms to be appended and published.

1
Service Restriction Policy
Document
purpose
This policy details all of procedures were there are service
restrictions in place by NHS Mansfield and Ashfield CCG and NHS
Newark and Sherwood CCG. For all the procedures and services
detailed in this policy individual prior approval must be sought.
This policy is based on and superseded the Nottinghamshire (less
Bassetlaw) Procedures of Limited Clinical Value Policy 2015 and
the East Midlands Cosmetics Policy 2015.
Version Version 1.0 Final
Title Service Restriction Policy
Associated Policy Procedures Not Routinely Funded Policy (2017)
Nominated
Lead
Director of Quality and Governance and Chief Nurse
Approval Date 16.2.17
Approving
Committee
Joint NHS Mansfield and Ashfield CCG and NHS Newark and
Sherwood CCG Governing Body
Review Date This policy will be reviewed in 1 year or earlier if additions or
changes are required.
Groups/staff
Consulted
Joint NHS Mansfield and Ashfield CCG and NHS Newark and
Sherwood CCG Clinical and Cost Effectiveness Committee
Joint NHS Mansfield and Ashfield CCG and NHS Newark and
Sherwood CCG Clinical Executive Committee
Joint NHS Mansfield and Ashfield CCG and NHS Newark and
Sherwood CCG Governing Body
Target audience All CCG staff
All providers
All Clinicians
Circulation list CCG Websites
All providers
Primary Care Clinicians
Associated
documents
Individual Funding Requests (IFR) V2 April 2011

2
Table of Contents Purpose of the policy ........................................................................................................................... 4
Introduction ............................................................................................................................................ 4
Commissioning Principles ................................................................................................................... 4
Policy Exclusions .................................................................................................................................. 5
Exceptionality and Special Consideration ........................................................................................ 5
Implementation and Compliance ....................................................................................................... 5
Schedule of procedures ...................................................................................................................... 6
Procedure ...................................................................................................................................... 6
Adenoids/Grommets .................................................................................................................... 6
Biological Mesh ............................................................................................................................. 6
Carpal Tunnel ............................................................................................................................... 6
Cataracts ....................................................................................................................................... 6
Dupuytrens Contracture .............................................................................................................. 6
Dilatation and Curettage (D&C) / Hysteroscopy Including the treatment of menorrhagia
(Heavy Menstrual Bleeding) ....................................................................................................... 6
Ganglion Cysts ............................................................................................................................. 6
Grommets ...................................................................................................................................... 6
Haemorrhoidectomy ..................................................................................................................... 6
Hallux Valgus (bunions) .............................................................................................................. 6
Hernia Repair ................................................................................................................................ 6
Hip arthroscopy ............................................................................................................................. 6
Hip replacement – elective.......................................................................................................... 6
Hysterectomy for heavy menstrual bleeding – Non Cancer .................................................. 6
Insulin Pump ................................................................................................................................. 6
Joint Injections .............................................................................................................................. 6
Knee arthroscopy ......................................................................................................................... 6
Knee washouts ............................................................................................................................. 6
Micro-suction for the removal of earwax ................................................................................... 6
Mirena Coils – insertion in secondary care .............................................................................. 6

3
MRI low back pain ........................................................................................................................ 6
Shoulder arthroscopy ................................................................................................................... 6
Sleep Studies ................................................................................................................................ 6
Snoring ENT referrals .................................................................................................................. 7
Spinal epidural injections for back pain .................................................................................... 7
Spinal Surgery for Non-Acute Lumbar Conditions including Discectomy for lumbar disc
prolapsed ....................................................................................................................................... 7
Tonsillectomy ................................................................................................................................ 7
Varicose Veins .............................................................................................................................. 7
Vasectomy – if undertaken in secondary care ......................................................................... 7
Process to be followed ........................................................................................................................ 7
Process to follow .................................................................................................................................. 9

4
Purpose of the policy The purpose of this policy is to ensure that NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG (the Commissioner) fund treatment only for clinically effective interventions delivered to the right patients. It sets out the treatments deemed to be of insufficient priority to justify funding from the available fixed budget.
This policy lists a number of procedures and services that NHS Mansfield and Ashfield and Newark and NHS Sherwood Clinical Commissioning Groups restricts funding for. Patients should only be referred for the procedures and services listed in this policy if they meet the eligibility criteria set out. The onus is on the clinician to seek prior approval from the commissioner by completing a prior approval application. The clinician must provide sufficient information to evidence how the patient meets the criteria.
If a provider undertakes one of the procedures contained within this policy without prior approval being approved commissioners will not reimburse the provider.
This policy should be read in conjunction with the Not Routinely Funded Policy (2017). These two policies have been based on and include all the procedures that were part of the Procedures of Limited Clinical Value Policy (2015) or the East Midlands Cosmetic Policy (2015) which have now been superseded.
Approved prescribing of medicines falls outside the scope of this document and is covered in the guidelines and protocols produced by the Nottinghamshire Area Prescribing Committee. Further information can be obtained from the Pharmacy/Medicines Management Department or via www.nottsapc.nhs.uk.
Introduction This policy identifies procedures that NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG will restrict the provision of through a clear set of criteria and a prior approvals process. A number of these procedures are either currently restricted through the Procedures of Limited Clinical Value 2015 and East Midlands Cosmetics Policy 2015: however there are a number of additions, which although new NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG, relate to procedures not routinely commissioned in a number of other CCGs.
In addition to these restrictions we will not routinely fund interventions in the CCGs procedures not routinely funded or as identified in the “do not do” recommendations database which is maintained by NICE.
http://www.nice.org.uk/usingguidance/donotdorecommendations/index.jsp
Commissioning Principles Commissioning decisions are made in accordance with the general principles set out below:
Clear evidence of clinical and/or cost effectiveness will be sought before NHS resources are invested in the treatment
The cost of the treatment for individual patients and others within any anticipated cohort is a relevant factor.

5
The extent to which the individual or patient group will gain a benefit from the treatment will be considered and balanced against the benefit which could be gained by alternative investment possibilities to meet the needs of the community
The process and policies will consider all relevant national standards and take into account all proper and authoritative guidance.
Policy Exclusions Patients should not be referred or undergo the procedures listed in this policy , except in the case of:
Emergency, OR
A reasonable suspicion of cancer, OR
As part of reconstruction following treatment for cancer, traumatic injury or the correction of congenital malformation
Exceptional or Special circumstances (which will need explicit CCG Approval – see exceptionality and special consideration).
Exceptionality and Special Consideration The Commissioner will consider individual cases for funding of procedures set out in this commissioning policy where the Individual Funding Request Policy does not apply. Where the patient meets the following criteria and relevant evidence is available, clinicians may apply for individual funding related to the procedures covered in this policy.
Exceptionality The patient is significantly different to a group of patients with the condition in question and at the same progression of the condition AND likely to gain significantly more clinical benefit than others in the group of patients with the condition in question and at the same stage of progression of the condition Evidence of Clinical Effectiveness
All other relevant commissioned therapies/treatments have been tried
Anticipated clinical benefits in the individual case of the particular treatment requested are over and above all other available options
If more than one episode of treatment is required, it is clear how benefits of the procedure/treatment will be demonstrated/measured, including what the intended outcomes are, what ‘stopping’ criteria would be used and how it will be measured.
Evidence of Individual Patient Safety Standard treatments (those available to other patients with this condition/stage of the disease) are not appropriate for this patient for clinical reasons.
Implementation and Compliance The policy will be implemented across providers in primary and secondary care. It will be formally incorporated into contracts and will be subject to routine monitoring for compliance.

6
Schedule of procedures
Procedure
Adenoids/Grommets
Biological Mesh
Carpal Tunnel
Cataracts
Dupuytrens Contracture
Dilatation and Curettage (D&C) / Hysteroscopy Including the treatment of
menorrhagia (Heavy Menstrual Bleeding)
Ganglion Cysts
Grommets
Haemorrhoidectomy
Hallux Valgus (bunions)
Hernia Repair
Hip arthroscopy
Hip replacement – elective
Hysterectomy for heavy menstrual bleeding – Non Cancer
Insulin Pump
Joint Injections
Knee arthroscopy
Knee washouts
Micro-suction for the removal of earwax
Mirena Coils – insertion in secondary care
MRI low back pain
Shoulder arthroscopy
Sleep Studies

7
Process to be followed
Prior Approval MUST be sought in the following scenarios
a) At the point of decision to refer for a specific procedure, which requires prior approval, the referrer will ensure that the clinical criteria are met. The referrer must then apply for pre-approval, informing the patient of the pre-approval process.
i. Please note prior approval is not required if a patient is being referred to secondary care for consultant management other than a procedure listed in this policy e.g. if referral is for diagnostic tests or investigations or treatment options
b) A consultant who wishes to undertake a procedure covered by a lower priority
treatment policy can seek approval in the same way and using the same criteria as their GP colleague. This process applies regardless of the hospital at which the patient may be treated and only applies to NHS commissioned secondary care, but is applicable in all provider settings where that care is provided. Providers should ensure that the prior approval code is recoded in the free text field in the SUS entry to ensure that the procedure is not queried.
Requesting Prior Approval
Mid Nottinghamshire CCGs Procedures Not Routinely Funded Policy 2017
Mid Nottinghamshire CCGs Service Restriction Policy 2017
Is the procedure covered by the above policies?
No – Follow best practice and peer review referral as appropriate. If unsure check with prior approval team
Yes – Assess the patient against the criteria outlined. Does the patient meet the criteria within the policy?
Snoring ENT referrals
Spinal epidural injections for back pain
Spinal Surgery for Non-Acute Lumbar Conditions including Discectomy for
lumbar disc prolapsed
Tonsillectomy
Varicose Veins
Vasectomy – if undertaken in secondary care

8
Yes – requires prior approval before referral for procedure
complete the relevant prior approval form
Please add any supporting clinical information, when using e-referral the completed form should be attached to the referral. For anything else send the completed Prior Approval form via secure nhs.net email to [email protected]
Explain process to patient so that expectations about treatment are not raised
No– if the patient does not meet the criteria in the policy, the CCG will not fund the procedure.
Please do not refer the patient for the procedure
Explain the criteria and evidence base for this policy to the patient
Prior approval Process
On receipt of the prior approvals request the CCG, or those conducting triage on their behalf, will ensure that the requests receive appropriate clinical and financial review to confirm compliance with policy and equity with other approval decisions. The CCG will have a 10 working day turnaround from date of receipt for all Primary Care requests. For the purposes of patient confidentiality we only accept e-mail requests
which should be sent to [email protected]
Primary Care
Once approval has been issued, a referral can then be sent to secondary care in the normal way. Please attach a copy of the application form with your referral letter and clearly state the prior approval reference number.
If the referral is not complete with the approved application form/approval number, the Secondary Care provider will not be able to carry out the procedure or respond to contractual challenges and can return the referral to the GP.
Procedures undertaken by primary care that are listed in either the mid Nottinghamshire Service Restriction Policy (2017) or the mid Nottinghamshire Procedures not normally funded Policy (2017) must have prior approval from the CCG.
Secondary Care
The patient can be added to the waiting list for the requested treatment only if prior approval has been received. Patients must not be listed for treatment until prior approval has been sought and approved. Providers should ensure that the prior approval code is recoded in the free text field in the SUS entry to ensure that the procedure is not queried
Prior Approval Pathways
Prior Approval Request Forms can be accessed via Mid Nottinghamshire Clinical Pathways web site: http://midnottspathways.nhs.uk/

9
Process to follow
. Is the procedure
listed in the not
routinely funded
policy?
Is the procedure
listed in the not
restricted
procedure policy?
Follow best practice and
peer review referral/
undertake procedure as
appropriate
Do not refer or undertake
If you feel there are exceptional or
special circumstances apply for CCG
consideration
Does the patient
meet the criteria
set out in the
policy?
Apply for prior
approval
No No
YES
YES
No YES

1
Service Restriction Policy Additional Information
Purpose of this document
This document is intended to be read alongside the Service Restriction Policy. This document provides detail of the criteria that clinicians must use as a basis for an application of prior approval.
Policy statement: Adenoidectomy
OPCS codes Eligibility Criteria – Prior Approval Needed
Adenoidectomy combined with grommets may be considered in children who fulfil the
criteria for grommets (see Grommet criteria) as follows:
• The child has experienced persistent hearing loss for more than a year with deficit
estimated to be more than 25 decibels;
OR
• 6 or more episodes of acute otitis media in previous 12 months (a 3 month course
of low dose daily antibiotics may be considered first);
OR
• The child has a developmental impairment (e.g. speech/ language/ cognitive/ behavioural) likely to be due to, or exacerbated by, clinically suspected hearing loss.
In a Cochrane review of grommets1, the reviewers note some improvement in outcomes
that look at adenoidectomy and grommet insertion compared to grommet insertion alone.
The other indication for adenoidectomy (usually in conjunction with tonsillectomy) is:
Sleep apnoea (usually diagnosed with by strong clinical suspicion by an ENT surgeon –
sleep studies are not likely to be a cost-effective diagnostic tool in most cases). A literature
review2
in 2005 found that, in children, including those that are obese, “adeno-
tonsillectomy was curative for 75-100%”. However, a Cochrane review3
noted that there is
no randomised trial data relating to adeno-tonsillectomy for obstructive sleep apnoea in
children and more research is needed.
In all cases, there should be evidence that the surgeon has obtained adequate informed consent, including discussing the potential risks and benefits of surgery. References
1. Cochrane Database of Systematic Reviews. Grommets (ventilation tubes) for hearing loss associated with OME in children
2. Ryan, C.F (2005). Sleep 9: An approach to treatment of obstructive sleep apnoea/hypopnoea
syndrome including upper airway surgery. Thorax (60);595-604.
3. Lim,J and McKean,M (200). Adenotonsillectomy for obstructive sleep apnoea in children. Cochrane Database of Systematic Reviews Issue 3.
Patient Information Leaflet
NHS Choices Patient Information Leaflet Adenoidectomy

2
Policy statement: Biological Mesh
OPCS codes: Eligibility Criteria – Prior Approval Needed for some
indications require IFR
Mid Nottinghamshire CCGs will consider approval and use of biological mesh in the following indication:
Hernia:
Primary ventral and inguinal hernia repair in non-infected fields
Recurrent hernias, reinforced hernia repair
Hernia prophylaxis
Hernia repair in the contaminated or potentially contaminated fields (most widely used)
Complex abdominal wall hernia repair
Breast reconstruction:
Mastectomy
Reconstructive surgery
Pelvic organ prolapse:
Pelvic organ prolapse (POP)
Laparoscopic ventral mesh rectopexy (rectal prolapse)
Other indications (will require Individual Funding Request)
Mucogingival surgery
Urethroplasty
eLAPE (Extralevator abdomino-perineal excision) reconstructive surgical technique for low rectal cancer
Closure of laparostomy
Diabetic foot ulcer repair
Onlay graft during hemicraniectomy
Sandwich bone augmentation Biological mesh is classified by:
1. Source – usually human, porcine or bovine 2. Site – dermis, small intestine submucosa, pericardium 3. Processing method – cross-linked, non-cross linked, sterilised, non-sterilised
Policy statement: Carpel Tunnel
OPCS codes: A651 Eligibility Criteria – Prior Approval Needed
Mid -Nottinghamshire CCGs commission surgery for carpal tunnel syndrome on a restricted basis. Patients with wasting of the hand muscles should be urgently referred to the acute (outside the scope of this policy).

3
Mid-Nottinghamshire CCGs commission surgery for carpal tunnel syndrome on a restricted basis. Nerve conduction studies (EMG) are NOT generally needed to confirm the diagnosis and are not routinely funded by the Mid-Nottinghamshire CCGs. Community based conservative treatment should be initiated for ALL patients with suspected Carpal Tunnel Syndrome for a period of 6 months, excluding those noted below. Conservative treatment will include the following:
Analgesia
Splinting with Futuro-type cock up splint (night time only or constant)
Steroid injection – should be administered once prior to referral for consideration of surgery
All GPs should seek access to carpal tunnel injections prior to referral to surgery. Patients with Carpal Tunnel Syndrome should be referred if any of the following criteria apply:
Severe symptoms (fewer than 5% of patients) uncontrolled by conservative measures, significantly interfering with daily activities.
Neurological deficit i.e. constant sensory blunting or weakness of thenar abduction (wasting or weakness of abductor pollicis brevis).
Unclear diagnosis or dual pathology
Rheumatoid
Recent trauma
Previous surgery
The referral must detail conservative methods tried and the length of time that each of these was carried out. Uncomplicated cases who have NOT responded to conservative management for 6 months should be referred. Rationale: Conservative treatment offers short-term benefit (1-3 months) similar to surgery and many patients’ symptoms may resolve for at least a year after conservative treatment. After corticosteroid injection, up to 50% of patients may report minor or no symptoms at one year. The benefits of conservative therapy are seen early after treatment and then decrease while the benefits of surgery take longer to be fully realised. Corticosteroid injections and nocturnal splinting are effective conservative therapies. Therefore patients would not normally be referred for carpal tunnel syndrome unless they have had a local steroid injection into the carpal tunnel together with the provision of night splints. Electro-diagnostic tests are not indicated in the diagnosis of classical carpal tunnel syndrome. These may be done where there is doubt about the diagnosis, which is uncommon. In the longer term (3-18 months), surgery is better than conservative therapy with up to 90% of patients reporting complete or much improvement at 18 months.

4
A trial of conservative therapy offers the opportunity to avoid surgery for some patients.
Patient information leaflet
NHS Choices Carpal Tunnel Treatment Information Leaflet
Policy statement: Cataracts
OPCS codes: C712 – Phacoemulsification of lens C751 – Insertion of
prosthetic replacement
for lens NEC
Eligibility Criteria – Prior Approval Needed
Background
Cataracts are a common condition of later life affecting the lens of the eye. If left untreated, they can cause a gradual loss of clarity of vision, which can have a large impact on the quality of life of many elderly people. Currently the only effective treatment is surgery. The aims of cataract surgery are to improve visual acuity and to improve the vision-related quality of the patient’s life. A best corrected VA of 6/12 or better [Snellen], 0.30 [LogMAR] in the worse eye normally allows a patient to function without significant visual difficulties. Guidance Referral of patients with cataracts to ophthalmologists should be based on the following indications;
1. The patient has sufficient cataract to account for the visual symptoms. AND
2. The patient has best corrected visual acuity of 6/12 or worse in the worst eye and the reduced visual acuity is impairing their lifestyle:
a. the patient is at significant risk of falls, and has been assessed by a falls assessment team b. the patient’s vision is affecting their ability to drive c. the patient’s vision is substantially affecting their ability to work d. The patient’s vision is substantially affecting their ability to undertake leisure activities
such as reading, watching television or recognising faces. OR
3. The patient has best corrected visual acuity of better than 6/12 in the worst eye but they are working in an occupation in which good visual acuity is essential to their ability to continue to work e.g. watchmaker, microsurgeon. OR
4. The patient has bilateral cataracts, neither of which fulfils the threshold for surgery, but which together reduce binocular vision below the DVLA standard for driving. OR
5. The patient has best corrected visual acuity of better than 6/12 in the worst eye but they are experiencing some other significant impact on their quality of life, as a result of their visual symptoms. A description of this impact must accompany the referral information. AND
6. The patient is willing to have cataract surgery:

5
a. The referring optometrist or GP has discussed the risks and benefits using an approved information leaflet (national or locally agreed) and ensured the Patient understands and is willing to undergo surgery before referring. Second eye surgery in patients with bilateral cataracts Second eye surgery will be funded if the criteria above are met again. This should be assessed not earlier than the post-operative review following surgery on the first eye. This policy does not extend to cataract removal incidental to the management of other eye conditions. For patients at significant risk of falls If a patient has been deemed at significant risk of falls by a specialist falls assessment team and visual impairment due to cataract is deemed to be a contributor to this risk by the specialist team, patients who do not meet the visual acuity criteria above will be considered on an individual patient basis. References Department of Health 2007. Commissioning toolkit for community based eye care services. NHS Executive 2000. Action on cataracts. Good practice guidance. Royal College of Ophthalmologists 2010. Cataract surgery guidelines. P Jaycock, R L Johnston, H Taylor, M Adams, D M Tole, P Galloway, C Canning, J M Sparrow and the UK EPR user group (2009). The Cataract National Dataset electronic multi-centre audit of 55 567 operations: updating benchmark standards of care in the United Kingdom and internationally. Eye 23: 38-49
Policy statement:
Dupuytrens Contracture
OPCS codes: A651 Eligibility Criteria – Prior Approval Needed
Symptoms of Dupuytrens contracture are often mild and painless and do not require treatment. Patients may be managed with observation if the contractures themselves are not functionally limiting. Commissioners will fund surgical intervention where one or more of the criteria are met:
Metacarpophalangeal (MCP) joint contracture of 30° (inability to place hand flat on table), or
Any degree of proximal interphalangeal (IP) joint contracture, or
First web contracture, or
Significant functional loss which prevents activities of daily living, e.g. washing, dressing
The Commissioner does not fund routinely fund collagenase injections (Xiapex).
The Commissioner does not routinely fund radiation therapy for early Dupuytrens Reference
1. NICE Clinical Knowledge Summary

6
2. British Society for Surgery to the Hand Evidence for Surgical Treatment Guide: Dupuytrens Disease
3. British Society for Surgery of the Hand Evidence for Surgical Treatment Process Manual (Nov 2016)
Patient Information Leaflet
NHS Choices Patient Information Leaflet Dupuytrens Contracture
Policy statement: Dilatation and Curettage (D&C) / Hysteroscopy Including
the treatment of menorrhagia (Heavy Menstrual Bleeding)
OPCS codes: Eligibility Criteria – Prior Approval Needed
Hysteroscopy will be funded in the investigation and management of heavy menstrual bleeding only when it is carried out:
As an investigation for structural and histological abnormalities where ultrasound has been used as a first line diagnostic tool and where the outcomes are inconclusive, for example to determine the exact location of a fibroid or the exact nature of the abnormality. Or
Where dilatation is required for non-hysteroscopic ablative procedures. Or
Hysteroscopy should be considered immediately prior to the ablative procedure to ensure correct placement of the device (unless pre-operative ultrasound assessment has already been undertaken). Or
Postmenopausal women who have had a pelvic scan and endometrial biopsy and who present with further bleeding 6 months later should be offered hysteroscopy to be sure no small cancer has been missed without a mandatory preliminary scan.
Dilation and Curettage will not be funded in the following circumstances:
As a diagnostic tool for heavy menstrual bleeding. Or
As a therapeutic treatment for heavy menstrual bleeding.
Reference D&C and hysteroscopy will only be used in line with NICE guidance (CG44, 2007).
Patient information leaflet NHS Choices Patient Information Leaflet D&C

7
Policy statement: Ganglion cysts
OPCS Codes T591 Excision of
ganglion of wrist T601 Re‐excision of ganglion of the wrist T592 Excision of ganglion of hand
NEC T602 Re‐excision of ganglion of hand NEC T593 Excision of ganglion of knee T603 Re‐excision of ganglion of knee T594 Excision of ganglion of foot T604
Re‐excision of ganglion of foot T598 Other specified excision of
ganglion T608 Other specified re‐excision of ganglion T599 Unspecified excision of ganglion
T609 Unspecified re‐excision of
ganglion
Eligibility Criteria – Prior Approval Needed
Treatment Treatment of ganglia will not routinely be funded by the NHS except in certain significant circumstances. Surgical excision will not be commissioned for cosmetic reasons and access to secondary care will only be considered if the following criteria are met:
Significant functional impairment (significant restriction of work/domestic/care duties);
significant pain; neurological deficit; weakness of the joint; inhibition of nail growth. AND
Awareness of frequency of spontaneous resolution, likelihood of recurrence and possible complications of excision
AND
Discuss with patients frequency of spontaneous resolution AND likelihood of recurrence AND possible complications of treatment
Policy statement:
Grommet insertion for “Glue Ear” (otitis media with effusion) and recurrent acute otitis media in children.
OPCS codes: D151 -
Myringotomy with insertion of ventilation tube through tympanic membrane
Eligibility Criteria – Prior Approval Needed
Background Definitions:
1) Acute otitis media: Acute infection of the middle ear cleft. It is usually a self-limiting condition characterised by pain and fever lasting a few days which may be followed by up to 2 weeks of discharge.
2) Recurrent acute otitis media: The discrete recurrence of individual episodes rather than the prolonged course of one episode.
3) Middle ear effusion/Otitis media with effusion/Glue ear: These terms overlap and care needs to be taken with their precise meaning in each context in which they are used.
a. A middle ear effusion simply refers to the presence of fluid in the middle ear cleft under the ear drum.

8
b. Otitis media with effusion may on occasion be used interchangeably with the term Glue ear, or may be used specifically to refer to middle ear fluid occurring after an episode of (acute) otitis media.
c. Glue ear tends to suggest the presence of fluid in the middle ear cleft which has persisted and is causing hearing loss. Transient periods of middle ear effusion commonly follow episodes of upper respiratory tract infection and episodes of acute otitis media, but in many cases there is no identifiable cause of the effusion. Most middle ear effusions resolve within 3 months and cause no noticeable effects on the child’s development so do not require specialist assessment and advice. Middle ear fluid always causes a conductive hearing loss, but the magnitude of the loss is variable. The effects of the hearing loss on an individual are even more variable and often unpredictable, ranging from negligible to a significant handicap compromising speech and language, social and behavioural development. Factors affecting the amount of handicap caused include whether the impairment is unilateral or bilateral, the amount of impairment, its duration, the age of the child, the child’s social and educational circumstances and any other handicaps the child may have. It is the global impact of the effusions on the child’s life which is the important factor in determining treatment, not the presence of effusions per se. Available treatments for hearing loss associated with glue ear includes hearing aids or grommets.
Guidance
Referral of children for an ENT opinion is advised if:
• The child has hearing loss suggestive of sensori-neural deafness (urgent referral);
• There is a reasonable suspicion of hearing loss plus a delay in speech or language development, poor educational progress, social or behavioural problems or another disability such as Down’s syndrome or cleft palate (should be seen soon);
• The child has persistent hearing loss detected on two occasions separated by 3 months or more; NICE guidelines suggest a threshold of 25 dBHL or worse in the better ear;
• The child has suffered more than 6 episodes of acute otitis media in 12 months;
• The otoscopic features are atypical and accompanied by a foul smelling discharge lasting for more than 6 weeks, suggestive of cholesteatoma (urgent referral).
Surgical criteria for grommet insertion Grommet insertion will normally only be funded in children who meet one of these criteria:
1. The child has persistent bilateral otitis media with effusion, with a hearing loss, measured on two occasions separated by 3 months, of at least 25 dBHL averaged at 0.5, 1, 2 and 4 kHz (1).
OR
2. The child has persistent bilateral otitis media with effusion, with any degree of hearing loss AND there is documented evidence of significant developmental, social or educational delay.
OR
3. The child has suffered more than 6 episodes of acute otitis media in 12 months.
OR 4. The presence of an unsafe retraction pocket in the tympanic membrane.

9
The Priorities Forum acknowledges that clause 2 represents a departure from the 2008 NICE clinical guideline “Surgical management of otitis media with effusion in children”. The Priorities Forum believes that an established developmental impairment as a result of otitis-media-related hearing loss demonstrates that:
1. A de facto period of watchful waiting has already elapsed 2. The child stands to gain far more from early intervention than from deferment of
treatment. References 1. NICE. Surgical management of otitis media with effusion in children. 2008.
Patient information Leaflet NHS Choices Patient Information Leaflet Grommets
Policy statement: Haemorrhoidectomy
OPCS Codes
Eligibility Criteria – Prior Approval Needed
Background: Haemorrhoids are a common condition affecting a third of the general population. Peak incidence of Haemorrhoids is between ages 45 to 65 years [1] [2]. Symptomatic Haemorrhoids increase in prevalence in women during pregnancy and postpartum periods, but subsequently resolve. Most Haemorrhoids can be treated in primary care with dietary advice and avoidance of straining, and do not benefit from surgical intervention [3, 4]. History alone does not provide a diagnosis of Haemorrhoids. Physical examination including digital rectal examination and proctoscopy is a minimum requirement to confirm suspected diagnosis of Haemorrhoids [4] and to exclude other anorectal pathology. All cases of Haemorrhoids should be investigated for anaemia and other red flag signs and symptoms. If positive, these cases should be referred on appropriately under the two week wait criteria [5]. Haemorrhoidscan be classified as internal or external relating to their position of origin either above or below the dentate line. Haemorrhoids are graded into 4 groups by the Goligher classification [3] defined by their degree of prolapse.
1st degree Haemorrhoids: Bleed but do not prolapse
2nd degree Haemorrhoids: Prolapse but reduce spontaneously
3rd degree Haemorrhoids: Prolapse but reduced manually
4th degree Haemorrhoids: Permanently prolapsed and irreducible
Criteria for commissioning: As a non-priority condition, haemorrhoidectomy will only be commissioned if conservative treatment has failed and one of the following three criteria is present [6]
1. Haemorrhoids are recurrent;
2. Haemorrhoids are causing persistent bleeding;
3. Haemorrhoids cannot be reduced

10
For 1st and 2nd degree Haemorrhoids where conservative management has failed, rubber band ligation would constitute the first line intervention, with stapled haemorrhoidectomy/ haemorrhoidal artery ligation only to be used if rubber band ligation has failed.
For 3rd degree Haemorrhoids where conservative management has failed, rubber band ligation or haemorrhoidectomy/ haemorrhoidal artery ligation could be used as first line interventions.
For 4th degree Haemorrhoids, haemorrhoidectomy or haemorrhoidopexy should be the first line intervention. First line treatment: For first, second, and third degree Haemorrhoids, dietary management consisting of adequate fluid and fibre intake remains the treatment of choice. In addition bulk forming laxatives, non-opioid analgesia and topical haemorrhoid preparations can be prescribed for symptomatic relief [3, 4, 7-10]. For first, second and third degree Haemorrhoids refractive to conservative management with diet, rubber band ligation remains the intervention of choice [3, 11- 14], and is more efficacious than injection sclerotherapy. Stapled haemorrhoidectomy may also be used in third degree Haemorrhoids, as the probability of recurrence is lower. [3, 11, 15] Rubber band ligation offers economic advantages as a day case procedure and patients recover quicker when used appropriately. Stapled haemorrhoidopexy was considered appropriate for people with fourth-degree Haemorrhoids for whom residual external prolapse or skin tags would not be a concern [15]. Alternate treatment for fourth degree Haemorrhoids remains traditional surgical haemorrhoidectomy [3, 10, 15]. Treatment for small thrombosed Haemorrhoids remains unchanged with ice packs, analgesia and stool softeners recommended for symptomatic relief. Symptoms usually resolve within 10-14 days. Emergency surgery to excise necrotic tissue and remove the haemorrhoid may occasionally be appropriate. Second line treatment: For Haemorrhoids refractive to rubber band ligation, stapled haemorrhoidectomy is recommended by NICE in place of traditional surgical haemorrhoidectomy [15]. Models of device evaluated in the evidence review on stapled haemorrhoidopexy were the HCS33 (PPH01 model) and CDH33 model [15]. Stapled haemorrhoidopexy was found to be as effective as conventional haemorrhoidectomy when used appropriately and offered immediate benefits in terms of postoperative pain [16]. In addition, taking into account the requirements for postoperative pain management and other support during inpatient stay and after discharge, stapled haemorrhoidopexy was thought to potentially lead to modest cost savings [15]. Current evidence on haemorrhoidal artery ligation shows that this procedure is an efficacious alternative to conventional haemorrhoidectomy or stapled haemorrhoidopexy in the short and medium term, and that there are no major safety concerns [17]. Key efficacy outcomes are less postoperative pain than other treatments, resolution of Haemorrhoids, and relief of symptoms such as bleeding, prolapse, swelling, pain, soreness and itching in the short and long term

11
[17]. This procedure may therefore be used provided that normal arrangements are in place for clinical governance, consent and audit.
References: 1. Abramowitz, L., et al., [Clinical practice guidelines for the treatment of hemorrhoid
disease]. Gastroenterol Clin Biol, 2001. 25(6-7): p. 674-702.
2. Johanson, J.F. and A. Sonnenberg, The prevalence of hemorrhoids and
chronic constipation. An epidemiologic study. Gastroenterology, 1990. 98(2): p. 380-6.
3. Lohsiriwat, V., Approach to hemorrhoids. Curr Gastroenterol Rep, 2013.15(7): p. 332.
4. Hussain, J.N., Haemorrhoids. Essentials of clinical management. Aust Fam Physician, 2001. 30(1): p. 29-35.
5. Referral Guidelines for Suspected Cancer in Adults and Children. NICE Clinical
Guidelines, No. 27.
6. England, N., Interim clinical commisioning policy: Haemorrhoidectomy.November 2013.
7. Alonso-Coello, P., et al., Laxatives for the treatment of hemorrhoids.Cochrane
Database Syst Rev, 2005(4): p. Cd004649.
8. Alonso-Coello, P., et al., Fiber for the treatment of hemorrhoids complications: a systematic review and meta-analysis. Am J Gastroenterol, 2006. 101(1): p. 181-8.
9. NICE, NHS Clinical knowledge summaries: Haemorrhoids.
10. Rakinic, J. and V.P. Poola, Hemorrhoids and fistulas: new solutions to old problems. Curr Probl Surg, 2014. 51(3): p. 98-137.
11. Peng, B.C., D.G. Jayne, and Y.H. Ho, Randomized trial of rubber band ligation vs. stapled hemorrhoidectomy for prolapsed piles. Dis Colon Rectum, 2003. 46(3): p. 291-7;
discussion 296-7.
12. Kelly, M., NICE guidance does not recommend e-cigarettes. BMJ 2014;348:g315, 2014. 348(7942).
13. Drakeford, M., Mark Drakeford: E-cigarettes 're-normalising' smoking. 2014.
14. Lu, L.Y., Y. Zhu, and Q. Sun, A retrospective analysis of short and long term efficacy of RBL for hemorrhoids. Eur Rev Med Pharmacol Sci, 2013. 17(20): p. 2827-30.
15. NICE, Stapled haemorrhoidopexy for the treatment of haemorrhoids
16. Laughlan, K., et al., Stapled haemorrhoidopexy compared to Milligan-Morgan and Ferguson haemorrhoidectomy: a systematic review. Int J Colorectal Dis, 2009. 24(3): p.
335-44.
17. NICE, Haemorrhoidal artery ligation: Technology and current evidence.
2010.

12
Policy statement:
Hallux Valgus (bunions)
OPCS codes: W79.1, W79.2,
W79.9: soft tissue operations on
joint of toe;
W 15.1, 2, 3, 4, 5, 6, 8, 9: Division of
bone of foot (osteotomy of
metatarsal, tarsal or phalanx);
W 59.1, 2, 3, 4, 5, 6, 7, 8, 9:
Fusion of joint of toe (fusion
of metatarsophalangeal,
interphalangeal joints or
revision of fusion)
Eligibility Criteria – Prior Approval Needed
Hallux valgus commonly known as bunions, can cause varying degree of pain with limitation of function and mobility as an effect of pressure from shoes over the medial prominence of the metatarsal head. Conservative management such as orthoses does not always help to recover from symptoms and improve the long-term outcome. Surgical intervention can bring significant improvements in symptoms and clinical parameters, but is not always without a risk.
Surgery for asymptomatic bunions, for primarily cosmetic reasons, should be regarded as a procedure of low clinical priority - thus these procedures will not be routinely funded by the commissioners and the concerns about the cosmetic appearance of feet should not be referred onto secondary care.
In the first instance, conservative management techniques should be employed. These techniques include:
Avoiding high heel shoes and wearing wide fitting leather shoes which stretch
Non-surgical treatments such as bunion pads, splints, insoles or shields.
Simple analgesia.
Mid Nottinghamshire CCGs will only fund surgical treatment of bunions if the patient meets the following criteria.
The patient has been reviewed by podiatry services AND
Self-care advice and analgesia has been tried and symptoms are not improving (this must be evidenced in the prior approval application) OR
Severe pain unrelieved by conservative measures OR
Recurrent infection OR
Recurrent Ulcers

13
Policy statement: Hernia Repair
OPCS codes: Eligibility Criteria – Prior Approval Needed
If emergency treatment is required e.g. strangulation is suspected then the referring clinician should refer the patient.
All patients with femoral hernias should be referred for consultation however prior approval must be sought before surgical procedure.
The surgical treatment of hernias is commissioned on a restrictive basis for patients meeting the defined criteria below. This Service Restriction Policy covers the management of;
Inguinal
Femoral
Umbilical
Ventral
Incisional hernias
Criteria for referrals/treatment as below:
Inguinal: For asymptomatic or minimally symptomatic hernias, a watchful waiting approach is advocated with informed consent.
Surgical treatment should only be offered when one of the following criteria is met:
Symptomatic i.e. symptoms are such that they interfere with work or activities of daily living
Or
The hernia is difficult or impossible to reduce Or
Inguino-scrotal hernia Or
The hernia increases in size month on month Or
The patient is currently asymptomatic but works in a heavy manual occupation (for e.g. in removal firms lifting heavy weights) and there is an increased risk of strangulation and future complications.
Femoral: All suspected femoral hernias should be referred to secondary care due to the increased risk of incarceration/strangulation
Umbilical:
Surgical treatment should only be offered when one of the following criteria is met:
pain/discomfort interfering with activities of daily living Or
increase in size month on month Or
to avoid incarceration or strangulation of bowel Or
The patient is currently asymptomatic but works in a heavy manual occupation (for

14
e.g. in removal firms lifting heavy weights) and there is an increased risk of strangulation and future complications
Incisional:
Surgical treatment should only be offered when BOTH of the following criteria are met:
Pain/discomfort interfering with activities of daily living
And Appropriate conservative management has been tried first e.g. weight reduction where appropriate Or
The patient is currently asymptomatic but works in a heavy manual occupation (for e.g. in removal firms lifting heavy weights) and there is a risk of strangulation and future complications.
This procedure is not routinely funded for asymptomatic or minimally symptomatic inguinal hernias in adults. Patients should be referred for surgical assessment if they meet one or more of the following criteria:
A history of incarceration of, or real difficulty reducing, the hernia.
An inguino-scrotal hernia.
Increase in size month to month.
Pain or discomfort significantly interfering with activities of daily living.
Work related issues e.g. of work/missed work/unable to work/on light duties due to hernia
Comorbidity which does not render the patient unfit for elective surgery currently, but which is likely to significantly increase the risks associated with future surgery
Patient Information: NHS Choices Patient Information Leaflet Hernias
References
1. Simons MP, Aufenacker T. European Hernia Society guidelines on the treatment on inguinal hernia in adult patients. Hernia 2009; 13:343-403.
2. Fitzgibbons RJ, Giobbe-Hurder A. Watchful waiting vs. Repair of Inguinal Hernia in Minimally Symptomatic Men. JAMA 2006; 295:285292
3. O’Dwyer PJ, Norrie J. Observation or Operation for Patients with an Asymptomatic Inguinal hernia. Ann Surg 2006; 244:167-173>

15
Policy statement:
Hip Arthroscopy
OPCS codes: Eligibility Criteria – Prior Approval Needed
See East Midlands Commissioning Policy Arthroscopy of the Hip (EMSCGP047V1)
separate policy
In summary, commissioners will fund for the treatment of sepsis, loose bodies and excision of radiological proven labral tears in the absence of osteoarthritis or other pathology for patients meeting the policy criteria.
The Commissioner does not routinely fund the use of hip arthroscopy for the management of Hip Impingement Syndrome or other indications
Policy statement: Hip Replacement (Elective)
OPCS Codes
W37 – Total prosthetic
replacement of hip joint
using cement.
W38 – Total replacement of
hip joint not using cement.
W39 – Other total
replacement of hip joint.
Eligibility Criteria – Prior Approval Needed
Mid Nottinghamshire CCGs commission surgery for hip replacement on a restricted basis.
Referral should be when other pre-existing medical conditions have been optimised AND conservative measures have been exhausted and failed. Mid Nottinghamshire CCGs will only fund hip joint replacement surgery if:
The patient complains of severe joint pain AND has radiological features of severe disease AND has severe functional limitation irrespective of whether conservative management has been trialled, OR
The patient complains of severe joint pain AND has radiological features of severe disease AND has minor to moderate functional limitation, despite the use of non-surgical treatments such as adequate doses of NSAID analgesia, weight control treatments and physical therapies.
The patient complains of mild to moderate joint pain AND has radiological features of severe disease AND has severe functional limitation, despite the use of non-surgical treatments such as adequate doses of NSAID analgesia, weight control treatments and physical therapies AND is assessed to be at low surgical risk.
The patient has completed a self-assessment score, e.g. the Oxford Hip Score as part of their pre-assessment provided by secondary care prior to surgery. http://www.orthopaedicscore.com/scorepages/oxford_hip_score.html
Has supporting clinical diagnostics and other assessments to support the decision to operate

16
Please refer to the classification of pain levels and functional limitations in the table below.
Evidence suggests that the following patients would be INAPPROPRIATE candidates for hip joint replacement surgery:
Where the patient complains of mild joint pain AND has minor or moderate functional limitation
Where the patient complains of moderate to severe joint pain AND has minor functional limitation AND has not previously had an adequate trial of conservative management as described above
Hip replacement: Classification of Pain Levels and Functional Limitations
Variable Definition
Pain Level
Mild
Pain interferes minimally on an intermittent basis with usual daily
activities.
Not related to rest or sleep.
Pain controlled by one or more of the following: NSAIDs with no or
tolerable side effects, aspirin/paracetamol at regular doses.
Moderate
Pain occurs daily with movement and interferes with usual daily activities.
Vigorous activities cannot be performed.
Not related to rest or sleep.
Pain controlled by one or more of the following: NSAIDs with no or
tolerable side effects, aspirin/paracetamol at regular doses
Severe
Pain is constant and interferes with most activities of daily living.
Pain at rest or interferes with sleep.
Pain not controlled, even by narcotic analgesics.
Previous non-surgical treatments
Correctly Done
NSAIDs, paracetamol, aspirin or narcotic analgesics at regular doses
during 6 months with no pain relief; weight control treatment if overweight,
physical therapies done.
Incorrectly Done
NSAIDs, paracetamol, aspirin or narcotic analgesics at inadequate doses
or less than 6 months with no pain relief; or no weight control treatment if
overweight or no physical therapies done.
Functional Limitations
Minor
Functional capacity adequate to conduct normal activities and self-care.
Walking capacity of more than one hour.
No aids needed.
Moderate
Functional capacity adequate to perform only a few or none of the normal
activities and self-care.
Walking capacity of about one half hour.
Aids such as a cane are needed.

17
Severe
Largely or wholly incapacitated.
Walking capacity of less than half hour or unable to walk or bedridden.
Aids such as a cane, a walker or a wheelchair are required.
References
Nice Guidance ta 304
Patient Information leaflet
NHS Choices Patient Information Leaflet Hip Replacement
Policy statement: Hysterectomy for heavy menstrual bleeding – Non Cancer
OPCS codes: Eligibility Criteria – Prior Approval Needed
Hysterectomy for non-cancerous heavy menstrual bleeding will only be funded by Mid Nottinghamshire CCGs within NICE guidance and when;
There has been an unsuccessful trial and appropriate clinical assessment, with a levonorgestrel-releasing intrauterine system LNG-IUS, e.g. Mirena®, unless contraindicated, for at least 12 months which has not successfully relieved symptoms or has produced unacceptable side effects. And
At least one alternative treatment has failed, is not appropriate or is contra-indicated in line with NICE guidelines.
Alternative hormonal treatment Other hormone methods (e.g. combined oral contraceptives, injected progesterons, Gn-RH analogue).
In line with NICE guidance.
NSAIDs and Tranexamic Acid. And
The following are not clinically appropriate: 1. Endometrial ablation if normal uterus or if LNG-IUS contraindicated or
if ablation is contraindicated e. g. previous multiple caesarean section 2. Uterine Artery Embolisation (for fibroids under 3cm) 3. Myomectomy (for fibroids over 3cms)
Contraindications to the levonorgestrel intrauterine system are:
Distorted or small uterine cavity (with proven ultrasound measurements; Uterocervical canal length < 5cm).
Genital malignancy.
Active trophoblastic disease.
Active pelvic inflammatory disease.
Large cavity over 10cm length.
References: 1. Brown JS, Sawaya G, Thom DH, Grady D. Hysterectomy and urinary
incontinence: a systematic review. Lancet. 2000; 356: 535-9. 2. Clarke J. Treatment of heavy menstrual bleeding. BMJ 2010; 341: 353.

18
3. Lethaby A, Shepperd S, Farquhar C, Cooke I. Endometrial resection and ablation versus hysterectomy for heavy menstrual bleeding. Cochrane Database of Systematic Reviews 1999, Issue 2. Art. No.: CD000329. DOI:10.1002/14651858.CD000329
4. National Institute for Health & Care Excellence (NICE) Heavy menstrual bleeding, Jan 2013 http://publications.nice.org.uk/heavy-menstrual-bleeding-qs47.
5. National Institute for Health and Care Excellence (NICE) Heavy Menstrual Bleeding January 2007.
Patient Information Leaflet
NHS Choices Patient Information Leaflet Heavy Periods Treatment
Policy statement: Insulin Pump
OPCS Codes
Eligibility Criteria – Prior Approval Needed
Mid Nottinghamshire CCGs will fund initiation of continuous subcutaneous insulin infusion or ‘insulin pump' therapy is recommended as a possible treatment for adults and children 12 years and over with type 1 diabetes mellitus if:
attempts to reach target haemoglobin A1c (HbA1c) levels with multiple daily injections result in the person having ‘disabling hypoglycaemia', or
HbA1c levels have remained high (8.5% or above) with multiple daily injections (including using long-acting insulin analogues if appropriate) despite the person and/or their carer carefully trying to manage their diabetes
The person has attended a CCG approved diabetes educational course for example DAFNE.
Insulin pump therapy should only be started by a trained specialist team. This team should include a doctor who specialises in insulin pump therapy, a diabetes nurse and a dietitian (someone who can give specialist advice on diet). This team should provide structured education programmes and advice on diet, lifestyle and exercise that is suitable for people using insulin pumps.
Insulin pump therapy is not recommended for people with type 2 diabetes mellitus
Reference
(NICE Technology Appraisal 151: NICE GUIDANCE TA151)
Patient information leaflet
NHS Choices Patient Information Leaflet Treatment for Type 1 Diabetes

19
Policy statement: Joint Injections
OPCS codes: TBC Criteria being revised to meet new MSK pathway
Policy statement: Knee Arthroscopy
OPCS codes: Eligibility Criteria – Prior Approval Needed
Cases for knee arthroscopy will only be funded if they meet the criteria below:
Arthroscopy of the knee can be undertaken where a competent clinical examination (or MRI scan if there is diagnostic reason) has demonstrated clear evidence of an internal joint derangement (meniscal tear, ligament rupture or loose body) and where conservative treatment has failed or where it is clear that conservative treatment will not be effective.
Knee arthroscopy can therefore be carried out for:
Removal of loose body
Meniscal repair or resection / repair of chrondral defects
Ligament reconstruction/repair (including lateral release)
Synovectomy/symptomatic plica
To assist selection of appropriate patients for unicompartmental knee replacement
Knee arthroscopy should NOT be carried out (and will not be funded) for any of the following indications:
Investigation of knee pain (MRI is a less invasive alternative for the investigation of knee pain)
Treatment of osteoarthritis including arthroscopic washout and debridement.
In line with NICE guidance CG177; this should not be offered as part of treatment for osteoarthritis unless the individual has knee osteoarthritis with a clear history of mechanical locking (not gelling, ‘giving way’)
Reference NICE guidance CG177
Patient Information leaflet NHS Choices Patient Information Leaflet arthroscopy
Policy statement: Knee Washout
OPCS codes: Eligibility Criteria – Prior Approval Needed
Funded only where patient has mechanical features of locking (not gelling, ‘giving way’ or x-ray evidence of loose bodies).
Reference
1. NICE IPG230 Arthroscopic knee washout, with or without debridement, for the treatment of osteoarthritis. Aug 2007
2. NICE guidance CG177The care and management

20
Policy statement: Microsuction for the removal of ear wax
OPCS Codes
Eligibility Criteria – Prior Approval Needed
Removal of ear wax in secondary care will not be funded; Microsuction may be performed in primary care where a patient has one of the following contraindications to ear irrigation:
The patient has previously experienced complications following this procedure in the past.
There is a history of a middle ear infection in the last six weeks.
The patient has undergone ANY form of ear surgery (apart from grommets that have extruded at least 18 months previously and the patient has been discharged from the ENT Department).
The patient has a perforation or there is a history of a mucous discharge in the last year.
The patient has a cleft palate (repaired or not).
In the presence of acute otitis externa with pain and tenderness of the pinna.
Patient Information Leaflet NHS Choices Patient Information Leaflet Ear Wax