new evidence in the treatment of hyperphosphatemia · hyperphosphatemia contempory issues in ......
TRANSCRIPT
New evidence in the treatment of
hyperphosphatemia
Contempory issues in management
Mario Gennaro Cozzolino
University of Milan
Italy

THE LINK BETWEEN BONE AND CARDIOVASCULAR DISEASE: THE CENTRAL ROLE OF PHOSPHATE
PP
Mortality

XPO4 Vit.D
Ca CarbonateCa Acetate
+ CalcitriolCa CarbonateCa Acetate
+ Calcitriol
Ca x PO4
Ectopic Calcifications

“….unless all of the calcium which is absorbed is laid in bonethe calcium content of the soft tissues may rise and renalfunctional deterioration increase.”

XPO4 Vit.D
Al- and Ca-freeP-binders
+ VDRAsAl- and Ca-freeP-binders
+ VDRAs(Paricalcitol)
Ca x PO4
Ectopic Calcifications
Calcimimetics
April 8th, 2010


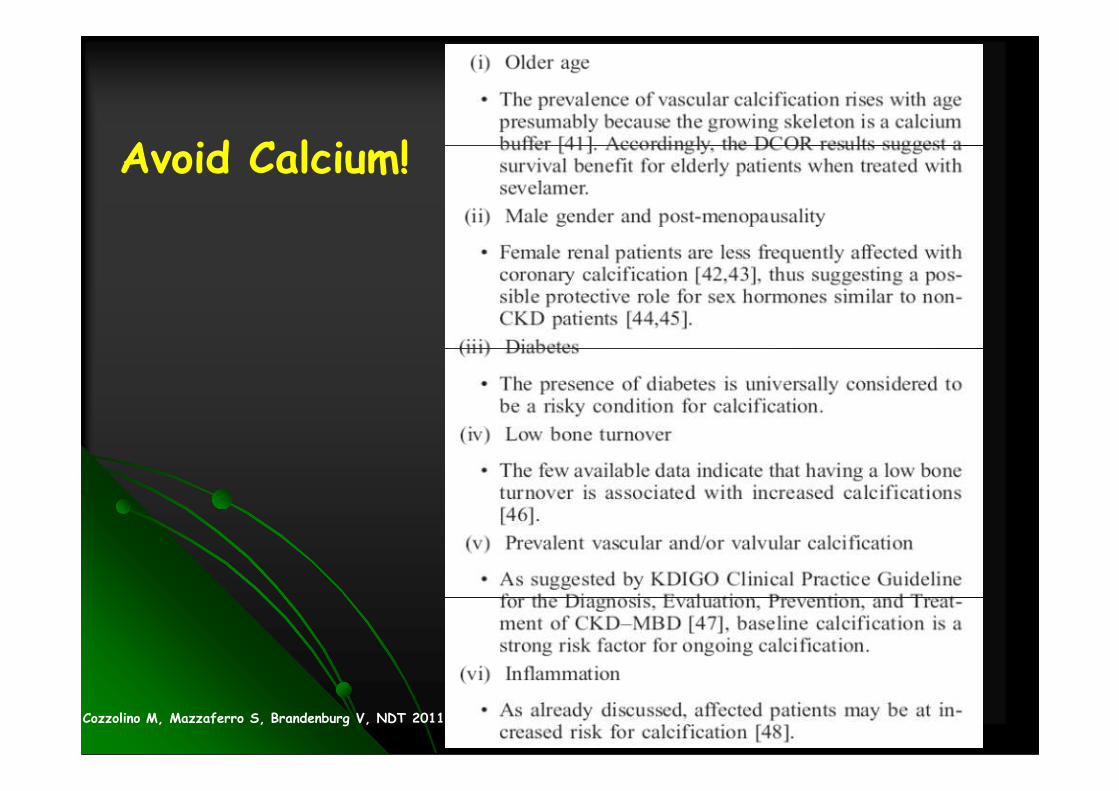
Avoid Calcium………..
� Older age
� Male Gender
� Female post-menopausality
Diabetes� Diabetes
� Low bone turnover
� Prevalent vascular/valvular calcification
� Inflammation
Cozzolino M, Mazzaferro S, Brandenburg V, NDT 2011

Optimizing the Treatment of Hyperphosphatemia in Experimental Uremia Experimental Uremia

↑↑↑↑Pi
Consequences of Hyperphosphatemiaon Parathyroid Function
↑↑↑↑ PTH Secretion
↑↑↑↑ Parathyroid Cell Growth

Pi
Silver et al, Am J Physiol Renal Physiol 2002

Regulation of PTH mRNA Stability by Lanthanum Carbonate in CKD

PiPO4
3-Na+
Pi Osf2/Cbfa-1?
Pit-1
Phosphate Regulation of Vascular SmoothPhosphate Regulation of Vascular SmoothMuscle Cell CalcificationMuscle Cell Calcification
Osteocalcin
?
Jono et al, Circul Res 2000Cozzolino et al, Kidney Int 2005Cozzolino et al, J Nephrol 2011

Effect of PFA on Ca deposition in VSMCs
Ciceri P et al. Nephrol. Dial. Transplant. 2012;27:122-127

Effect of Lanthanum on Ca deposition in VSMCs
Ciceri P et al. Biochem. Biophys. Res. Commun. (2012), in Press
Pi 5 mM LaCl 50 µµµµM LaCl 100 µµµµM

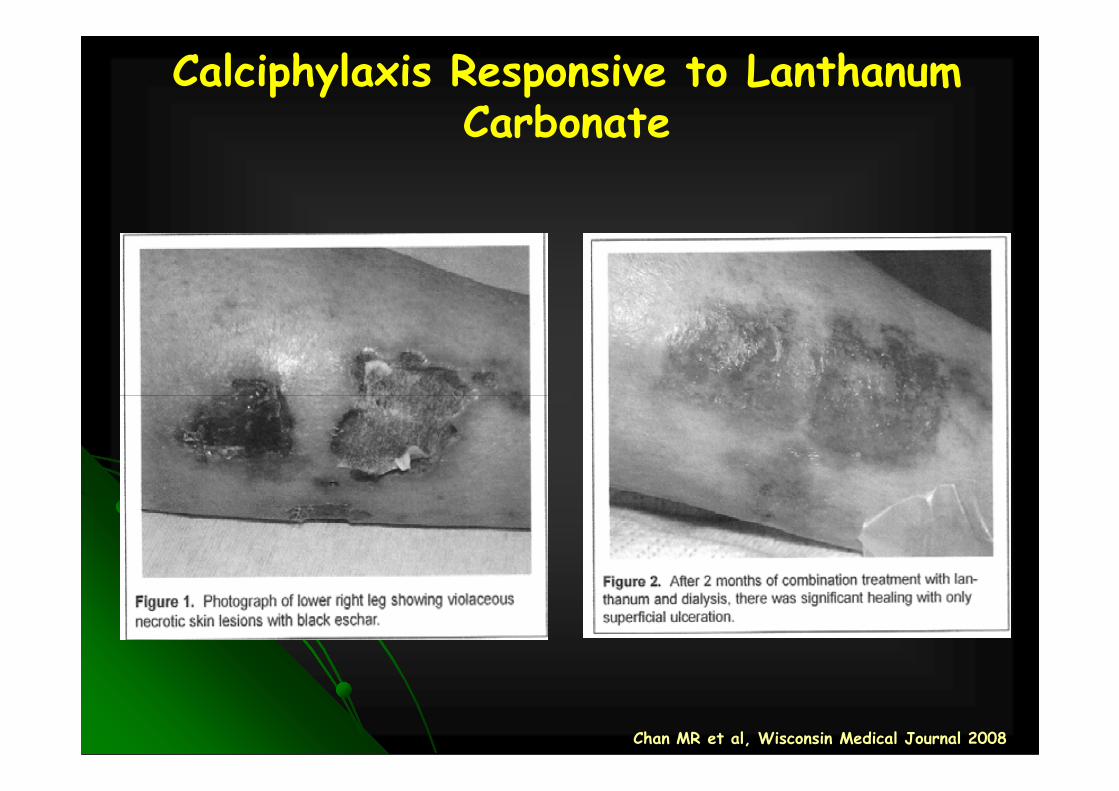
Calciphylaxis Responsive to Lanthanum Carbonate
Chan MR et al, Wisconsin Medical Journal 2008

Optimizing the Treatment of Hyperphosphatemia in CKD Hyperphosphatemia in CKD

Change in serum Pi from baseline during 8 weeks of treatment
Lanthanum carbonate reduces serum phosphate levels in CKD 3/4: Randomized multicentre trial
Weeks of treatment
0 1 2 3 4 6 8
PlaceboLanthanum
Ser
um P
i cha
nge
from
ba
selin
e (m
mol
/L)
0.0
-0.05
-0.10
Baseline: placebo 1.74 ± 0.04 mmol/L, lanthanum carbonate 1.71 ± 0.03 mmol/L. *p<0.05 between treatments, analysis of covariance (ANCOVA) model. Data are least square mean ± SE. To convert mmol to mg/dL, divide by 0.323
Lanthanum carbonate
Placebo (n)
Lanthanum carbonate (n)
34
56
32
55
31
46
32
45
30
44
28
43
28
42
Ser
um P
i cha
nge
from
ba
selin
e (m
mol
/L)
-0.15
-0.20
-0.25
-0.30
Sprague S, et al. C JASN 2009

25D and 1,25D Levels Are not Affected by Lanthanum Carbonate in CKD Patients
Objective� Evaluate the bioavailability of oral Vit D supplements in CKD 3 and 4 patients under lanthanum carbonate therapy
Methods� Randomized, double-blind, placebo-controlled, phase 2
25D
0 1 2 3 4 5 6 7 80
40
60
Mea
n (S
E)
25D
(nm
ol/L
)
Weeks of treatment
Lanthanum carbonatePlacebo
1314Lanthanum 7
Lanthanum carbonate
� Randomized, double-blind, placebo-controlled, phase 2
� Study population: subgroup of the former study who had received prior VDRAs
Conclusions� In this study, lanthanum carbonate did not interfere with the bioavailability of oral vit D supplements in patients with CKD 3-4
Finn W, et al. Nephrol Dial Transplant 2008;1(Suppl 2):59. #SP101
1,25D
13913Placebo (n)
1314Lanthanum carbonate (n)
0 1 2 3 4 5 6 7 80
60
90
Mea
n (S
E)
1,25
D (
nmol
/L)
Weeks of treatment
Placebo
121013Placebo (n)
1012Lanthanum carbonate (n)
70
80
50
15
7

Optimizing the Treatment of Hyperphosphatemia in DialysisHyperphosphatemia in Dialysis

Pro
port
ion
of p
atie
nts
cont
rolle
d (%
)
K/DOQI target serum phosphorus3.5–5.5 mg/dL1.13–1.78 mmol/L
n = 39n = 44 n = 42
n = 4850.060.070.080.0
Efficacy of Lanthanum in Patients Converting From Other Treatments
� Serum phosphorus control with LaCO3 monotherapy
41% receiving ≥2 binders
Pro
port
ion
of p
atie
nts
cont
rolle
d (%
)
n = 35
n = 8
n = 39n = 44 n = 42
0.010.020.030.040.050.0
Hutchison AJ, NDT 2009
K/DOQI, Kidney Disease Outcomes Quality Initiative LOCF, last observation carried forward

Lanthanum Carbonate vs SevelamerDifferential Effects on Renal Osteodystrophy
Ferreira A et al. JASN 2008
D’Haese Kidney International, 2003 (63)S85:S73–S78


� Clinical study conducted in CKD 5 dialysis patients
� Directly compares the efficacy of Lanthanum vs SevelamerDirectly compares the efficacy of Lanthanum vs Sevelamer� Serum phosphate reduction
� Doses commonly used in clinical practice
� Compared serum phosphate reduction in terms of:� Magnitude at end of treatment
� Magnitude at 1 week
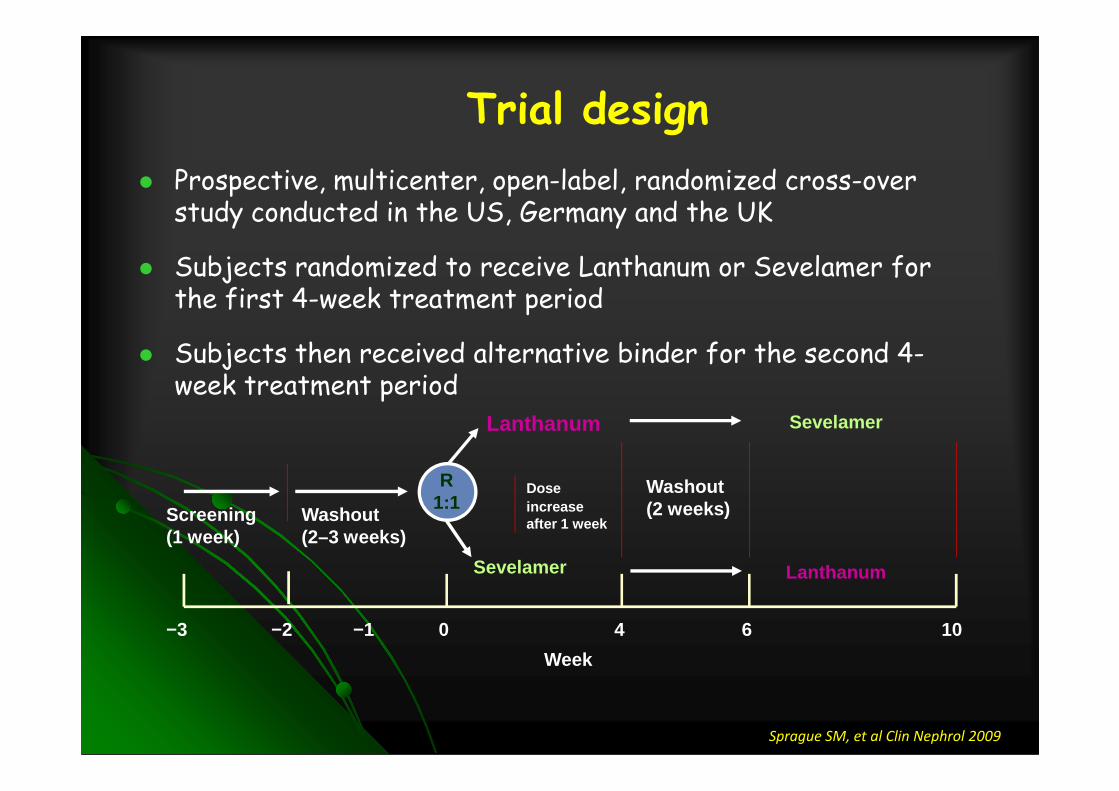
Trial design
� Prospective, multicenter, open-label, randomized cross-over study conducted in the US, Germany and the UK
� Subjects randomized to receive Lanthanum or Sevelamer for the first 4-week treatment period
� Subjects then received alternative binder for the second 4-week treatment periodweek treatment period
0−3 −1
Lanthanum
Sevelamer
4 10−2
Screening (1 week)
Washout (2–3 weeks)
Washout (2 weeks)
6
Week
R 1:1
Sevelamer
Lanthanum
Doseincrease after 1 week
Sprague SM, et al Clin Nephrol 2009

Fixed dose titration
� Subjects received predefined fixed doses for each treatment period
� Week 2 - 4 fixed dose based on that typically used in previous clinical trials1,2 and clinical practice3
Week 1 daily Week 2−4
1. Hutchison et al. Nephrol Clin Pract. 2008;110:15–23. 2. Chertow et al. Kidney Int. 2002;62:245–52 3. US DACON IMS Custom Basic Data Report, March 2006
Week 1 daily dose
Tablets/day Week 2−4 daily dose
Tablets/day
Lanthanum 2250mg 3 3000mg 3
Sevelamer 4800mg 6 6400mg 8
Sprague SM, et al Clin Nephrol 2009

Change in serum phosphate from baseline during treatment periods
-1
-0,8
-0,6
-0,4
-0,2
0
Lanthanum
Sevelamer
p=0.024
Leas
t squ
are
mea
n ch
ange
from
bas
elin
e se
rum
pho
spha
te le
vels
(m
g/dL
)
-2
-1,8
-1,6
-1,4
-1,2
Baseline Week 1 Week 2 Week 3 Week 4
p=0.438 p=0.599
p=0.028
Observed Case
Leas
t squ
are
mea
n ch
ange
from
bas
elin
e se
rum
pho
spha
te le
vels
(m
g/dL
)
Sprague SM, et al Clin Nephrol 2009

Treatment-emergent adverse events (safety populatio n)
Lanthanum Sevelamer
Any TEAE 44.7% 50.9%
Gastrointestinal Disorders 18.2% 23.3%Gastrointestinal Disorders 18.2% 23.3%
Diarrhoea 7.1% 7.4%
Nausea 8.8% 5.5%
Vomiting 5.3% 3.7%
Cardiac Disorders 4.1% 4.9%
Vascular Disorders 4.7% 3.7%
Sprague SM, et al Clin Nephrol 2009
The results from this study demonstrate interesting trends that support the suggestion from preclinical studies that
Sprague SM, et al Clin Nephrol 2009
suggestion from preclinical studies that Lanthanum Carbonate may be a more effective phosphate binder than Sevelamer Hydrochloride. These observations warrant further investigations in long-term studies.

Calcitriol + Lantanum (B)
Calcitriol
(A)Difference B-A
(95% CI) p-value
AUC0-48 (pg.h/mL) 429 318 111 (-48.9, 270) 0.171
AUC0-t (pg.h/mL) 429 318 111 (-48.9, 270) 0.171
Cmax (pg/mL) 47.0 49.7 -2.74 (-8.12, 2.63) 0.313Cmax (pg/mL) 47.0 49.7 -2.74 (-8.12, 2.63) 0.313
tmax (h) 4.00 2.00 1.27 (0.00, 2.48) 0.039
Calcitriol + Sevelamer(C)
Calcitriol(A)
Difference C-A (95% CI) p-value
AUC0-48 (pg.h/mL) 137 318 -181 (-338, -24.0) 0.024
AUC0-t (pg.h/mL) 137 318 -181 (-338, -24.0) 0.024
Cmax (pg/mL) 40.1 49.7 -9.62 (-14.9, -4.34) <0.001
tmax (h) 2.50 2.00 0.500 (-0.50, 1.46) 0.305
Pierce D, Nephrol Dial Transplant 2010

MAIN REMARKS
… Sevelamer carbonate significantly reduces serum concentrations ofexogenous calcitriol when co-administered with oral calcitriol…whereas lanthanum carbonate has no clinical relevant effects onwhereas lanthanum carbonate has no clinical relevant effects onexogenous calcitriol
… The most likely explanation for the effect of sevelamer is areduction in bioavailability through sequestering the fat-solublecalcitriol
… These findings may represent an important consideration inpatients with CKD who often require vitamin D supplementation

Avoid Calcium!
Cozzolino M, Mazzaferro S, Brandenburg V, NDT 2011

Avoid Calcium!
Cozzolino M, Mazzaferro S, Brandenburg V, NDT 2011

Avoid Calcium!
Cozzolino M, Mazzaferro S, Brandenburg V, NDT 2011

Avoid Calcium!
Cozzolino M, Mazzaferro S, Brandenburg V, NDT 2011

P
BONE-VASCULAR AXIS: THE ROLE OF PHOSPHATE
P
Mortality