neuromuscular blockade by neostigmine in anaesthetized man
TRANSCRIPT

Br.J. Anaesth. (1980), 52, 69
NEUROMUSCULAR BLOCKADE BY NEOSTIGMINEIN ANAESTHETIZED MAN
J. P. PAYNE, R. HUGHES AND S. AL AZAWI
SUMMARY
The tetanic and single twitch responses of the adductor pollicis muscle were used to study theneuromuscular effects of neostigmine in 26 patients anaesthetized with thiopentone and nitrous oxide.Neostigmine 2.5 mg i.v. given 5 min after exposure to halothane antagonized non-depolarizing neuro-muscular block, whereas a second dose given 2-5 min later depressed the peak tetanic contractionand re-established tetanic fade. In the absence of halothane the second dose of neostigmine hadless effect. Recovery of the single twitch was not impaired by the second dose. A single dose ofneostigmine 5 mg rapidly antagonized the competitive block of the tetanic response but the sub-sequent slight depression of the peak contraction and the brief reappearance of fade were lessthan after 5 mg given in two doses of 2.5 mg. In patients who were not given neuromuscular blockingdrugs, one or two injections of neostigmine 2.5 mg caused a substantial reduction in the peaktetanic contraction and severe tetanic fade which persisted for about 20 min; the single twitch wasslightly potentiated. The neostigmine block of the tetanic response could be antagonized by galla-mine and potentiated by suxamethonium. These findings indicate that neostigmine in clinical dosescan produce an acetylcholine-induced block which would be a potential hazard in anaestheticpractice.
Although the potential neuromuscular blockingproperties of neostigmine have been known for manyyears (Briscoe, 1936; Goodman and Gilman, 1956;Blaber and Bowman, 1963), no quantitative assess-ment of this effect has been described in man. In aprevious study we demonstrated that halothanepotentiated the neuromuscular block caused by non-depolarizing drugs and that it was reversed byneostigmine (Hughes and Payne, 1979). However,we also found that although the block was antagon-ized by a first dose of neostigmine, a subsequentdose of the anticholinesterase enhanced the block.
Accordingly, we decided that this interestingobservation deserved further investigation and thepresent work was undertaken to obtain a quantitativeassessment of this drug interaction in man.
METHODS
Studies were performed, after informed consent hadbeen obtained, on 26 patients about to undergoelective urological surgery. No premedication was
J. P. PAYNE, M.B., F.FJLR.C.S., D.A.; R. HUGHES,* B.SC.,M.SC., PH.D.; S. AL AZAWI, M.B., CH.B., F.F.A.R.C.S.I.,Research Department of Anaesthetics, Royal College ofSurgeons of England, London WC2 and St Peter's Hospitals,London WC2.
• Present address: Pharmacology Department, TheWellcome Research Laboratories, Langley Court, Becken-ham, Kent.
0007-0912/80/010069-08 $01.00
given and anaesthesia was induced with thiopentone300-600 mg i.v.; some patients were also givenhalothane 2-4%. Intubation of the trachea wasperformed without the use of a neuromuscularblocking agent after the larynx had been sprayed withlignocaine 4%. Where appropriate, halothane wasthen discontinued and anaesthesia maintained witha mixture of nitrous oxide 60-75% in oxygen givenby intermittent positive pressure ventilation; supple-ments of thiopentone 100-200 mg and pethidine50-150 mg were given as required. Simultaneousrecordings of tetanic and single twitch contractionsof the adductor pollicis muscles were made asdescribed previously (Sugai, Hughes and Payne,1975). Each ulnar nerve was stimulated supramaxim-ally at the wrist every 12 s with rectangular pulsesof 200 fis duration, one nerve at 50 Hz for 1 s andthe other with single pulses.
In one series of experiments halothane 2% wasadministered after i.v. neuromuscular blocking dosesof tubocurarine 0.1-0.24 mg kg"1, dimethyl tubo-curarine 0.075-0.1 mg kg"1 and gallamine 1.0-1.6 mgkg"1 when recovery of the tetanic response hadreached 50%. After 5 min when the peak height ofthe tetanic contraction was reduced and tetanic fadewas increased by halothane, neostigmine 2.5 mg wasgiven i.v. preceded by atropine 1.2 mg. Two tofive minutes later, while the administration of halo-thane continued, a second dose of neostigmine 2.5 mg
© Maanillan Journals Ltd 1980
by guest on Novem
ber 7, 2016http://bja.oxfordjournals.org/
Dow
nloaded from

was given. Groups of three patients were used foreach neuromuscular blocking drug studied.
In a second series of experiments halothane wasomitted and the first dose of neostigmine wasadministered when recovery from neuromuscularblockade had reached 50%; a second dose of neo-stigmine was administered 2 min later. Groups of twopatients were used for each neuromuscular blockingdrug studied.
Similarly, two patients received a single i.v. doseof neostigmine 5 mg, preceded by atropine 1.2 mg,one during recovery from neuromuscular paralysisby dimethyl tubocurarine 0.075 mg kg"1 and theother after gallamine 1.0 mg kg"1 when paralysis hadbeen enhanced by halothane 2%.
Finally, nine patients, who were not given neuro-muscular blocking agents, received up to three i.v.injections of neostigmine 2.5 mg preceded byatropine 1.2 mg. Four of these patients were sub-sequently given gallamine 10 mg i.v. and two patientsreceived suxamethonium 0.3 mg kg"1.
BRITISH JOURNAL OF ANAESTHESIA
RESULTS
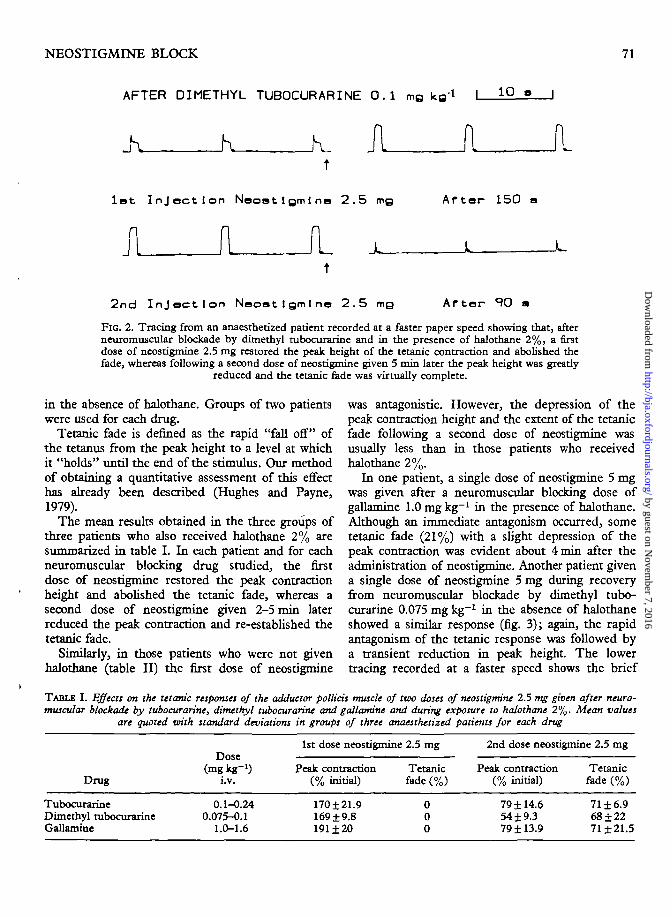
In each group of three patients simultaneous record-ings of the tetanic and twitch responses showed thatafter tubocurarine, dimethyl tubocurarine and galla-mine, administration of halothane 2% caused animmediate increase in tetanic fade with a reductionin the peak height of the tetanic contraction. Theseeffects were readily antagonized by neostigmine2.5 mg i.v., but reappeared and were often enhancedby a second dose of anticholinesterase given 2-5 minlater while the administration of halothane wascontinued (fig. 1). Recovery of the twitch responsewas unaffected by halothane; it was usually maximalwhen the first dose of neostigmine was given, andwas not impaired by the second dose. Recordingstaken at the same time, but at a faster paperspeed, show more clearly the effects on tetanic fade(fig- 2).
Similar effects with neostigmine were obtainedduring recovery from neuromuscular blockade bytubocurarine, dimethyl tubocurarine and gallamine
After Tubocurarine 0.25 mg
t tNeostigmine 2.5 mg
After D i methy 1 Tubocurar1ne 0.1 mg kg
NoostIgmlna 2.6 mg
A f ter Ga 1 1 am 1 ne 1 . 6 mg kg"1
| 5 mln |Neost igmine 2 .5 mg
FIG. 1. Tracings from three anaesthetized patients showing the increase in peak tetanic contractionwhen neostigmine 2.5 mg, preceded by atropine 1.2 mg, was given in the presence of halothane 2%after neuromuscular blockade by tubocurarine, dimethyl tubocurarine and gallamine, and thedecrease in the peak tetanic contraction following a second dose of neostigmine given 3-5 min
later.
by guest on Novem
ber 7, 2016http://bja.oxfordjournals.org/
Dow
nloaded from
NEOSTIGMINE BLOCK 71
AFTER DIMETHYL TUBOCURARINE O.I mQ kg"1 10
JL_A Alot Injection Neostigmine 2.5 mo After 150
A il L JL
2nd I n j e c t i o n Neoat1gm1 no 2 . 5 mg After SO
FIG. 2. Tracing from an anaesthetized patient recorded at a faster paper speed showing that, afterneuromuscular blockade by dimethyl tubocurarine and in the presence of halothane 2%, a firstdose of neostigmine 2.5 mg restored the peak height of the tetanic contraction and abolished thefade, whereas following a second dose of neostigmine given 5 min later the peak height was greatly
reduced and the tetanic fade was virtually complete.
in the absence of halothane. Groups of two patientswere used for each drug.
Tetanic fade is denned as the rapid "fall off" ofthe tetanus from the peak height to a level at whichit "holds" until the end of the stimulus. Our methodof obtaining a quantitative assessment of this effecthas already been described (Hughes and Payne,1979).
The mean results obtained in the three groups ofthree patients who also received halothane 2% aresummarized in table I. In each patient and for eachneuromuscular blocking drug studied, the firstdose of neostigmine restored the peak contractionheight and abolished the tetanic fade, whereas asecond dose of neostigmine given 2-5 min laterreduced the peak contraction and re-established thetetanic fade.
Similarly, in those patients who were not givenhalothane (table II) t ie first dose of neostigmine
was antagonistic. However, the depression of thepeak contraction height and the extent of the tetanicfade following a second dose of neostigmine wasusually less than in those patients who receivedhalothane 2%.
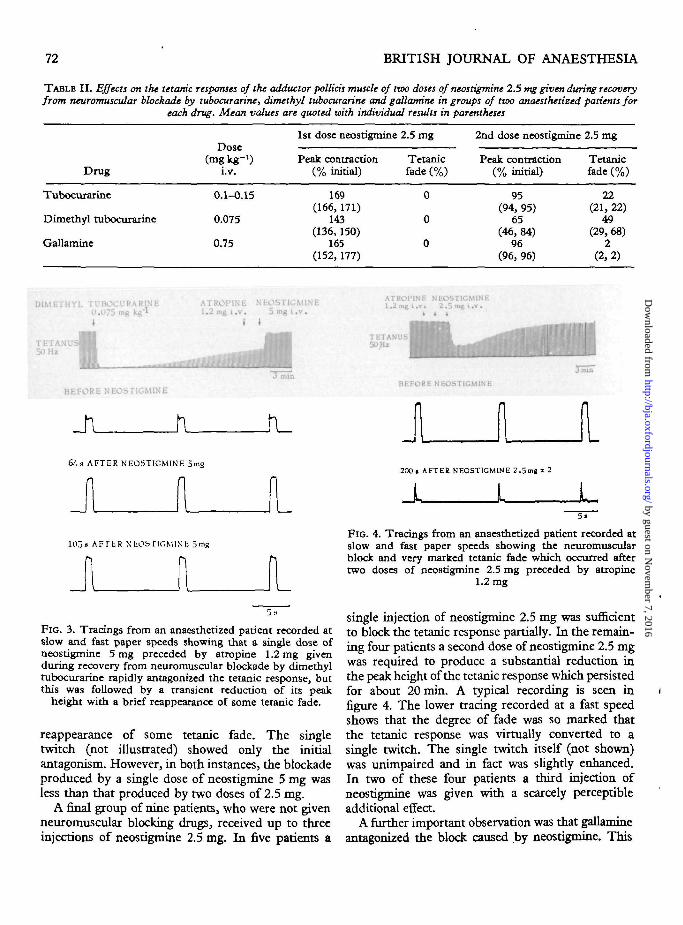
In one patient, a single dose of neostigmine 5 mgwas given after a neuromuscular blocking dose ofgallamine 1.0 mg kg"1 in the presence of halothane.Although an immediate antagonism occurred, sometetanic fade (21%) with a slight depression of thepeak contraction was evident about 4 min after theadministration of neostigmine. Another patient givena single dose of neostigmine 5 mg during recoveryfrom neuromuscular blockade by dimethyl tubo-curarine 0.075 mg kg"1 in the absence of halothaneshowed a similar response (fig. 3); again, the rapidantagonism of the tetanic response was followed bya transient reduction in peak height. The lowertracing recorded at a faster speed shows the brief
TABLE I. Effects on the tetanic responses of the adductor pollicis muscle of two doses of neostigmine 2.5 mg given after neuro-muscular blockade by tubocurarine, dimethyl tubocurarine and gallamine and during exposure to halothane 2%. Mean values
are quoted with standard deviations in groups of three anaesthetized patients for each drug
Drug
TubocurarineDimethyl tubocurarineGallamine
Dose(mg kg"1)
i.v.
0.1-0.240.075-0.1
1.0-1.6
1st dose neostigmine
Peak contraction(% initial)
170±21.9169 ±9.8191 ±20
2.5 mg
Tetanicfade (%)
000
2nd dose neostigmine 2.5 mg
Peak contraction(% initial)
79 ±14.654 ±9.379 ±13.9
Tetanicfade (%)
71 ±6.968±2271 ±21.5
by guest on Novem
ber 7, 2016http://bja.oxfordjournals.org/
Dow
nloaded from
72 BRITISH JOURNAL OF ANAESTHESIA
TABLE I I . Effects on the tetanic responses of the adductor pollicis muscle of two doses of neostigmine 2.5 mg given during recoveryfrom neuromuscular blockade by tubocurarine, dimethyl tubocurarine and gattandne in groups of two anaesthetized patients for
each drug. Mean values are quoted with individual results in parentheses
Drug
Tubocurarine
Dimethyl tubocurarine
Gallamine
(mg kg"1)i.v.
0.1-0.15
0.075
0.75
1st dose neostigmine
Peak contraction(% initial)
169(166, 171)
143(136, 150)
165(152, 177)
2.5 mg
Tetanicfade (%)
0
0
0
2nd dose neostigmine
Peak contraction(% initial)
95(94, 95)
65(46,84)
96(96, 96)
2.5 mg
Tetanicfade (%)
22(21, 22)
49(29, 68)
2(2,2)
DIMETHYL TUBOCURARINE ATROPINE NEOSTIGMINEU.O75 mg kg*' 1.2 mg i .v . 5 ing i . v .t I t
TETANU50 Hz
Plili.
BEFORE NEOSriGMLNE
Jl A
ATROIMNE NEOST1CMINE1.2mgt.v. 2 .5mgt .v .
»
TETANUS50 Hi
BEFORE NEOSTIGMINE
64s AFTER NEOSTIGMINE 5mg
1U3» AFTER NEObflCMlNb 5 mg
200« AFTEK NEOSTIGMINE 2.5mg x 2
JL L5 .
FIG. 4. Tracings from an anaesthetized patient recorded atslow and fast paper speeds showing the neuromuscularblock and very marked tetanic fade which occurred aftertwo doses of neostigmine 2.5 mg preceded by atropine
1.2 mg
FIG. 3. Tracings from an anaesthetized patient recorded atslow and fast paper speeds showing that a single dose ofneostigmine 5 mg preceded by atropine 1.2 mg givenduring recovery from neuromuscular blockade by dimethyltubocurarine rapidly antagonized the tetanic response, butthis was followed by a transient reduction of its peak
height with a brief reappearance of some tetanic fade.
reappearance of some tetanic fade. The singletwitch (not illustrated) showed only the initialantagonism. However, in both instances, the blockadeproduced by a single dose of neostigmine 5 mg wasless than that produced by two doses of 2.5 mg.
A final group of nine patients, who were not givenneuromuscular blocking drugs, received up to threeinjections of neostigmine 2.5 mg. In five patients a
single injection of neostigmine 2.5 mg was sufficientto block the tetanic response partially. In the remain-ing four patients a second dose of neostigmine 2.5 mgwas required to produce a substantial reduction inthe peak height of the tetanic response which persistedfor about 20 min. A typical recording is seen infigure 4. The lower tracing recorded at a fast speedshows that the degree of fade was so marked thatthe tetanic response was virtually converted to asingle twitch. The single twitch itself (not shown)was unimpaired and in fact was slightly enhanced.In two of these four patients a third injection ofneostigmine was given with a scarcely perceptibleadditional effect.
A further important observation was that gallamineantagonized the block caused by neostigmine. This
by guest on Novem
ber 7, 2016http://bja.oxfordjournals.org/
Dow
nloaded from

NEOSTIGMINE BLOCK 73
NEOSTIGMINE2 . 5 mg i . v .
ATROl'lNt- I I GA1.1.AM1NEI.2ms i . v . Wmt> i . v .
TETA50 Hz
I I I
SlNGLIiTWITCH
FIG. 5. Tracings from an anaesthetized patient showingneuromuscular block of the tetanic response after twodoses of neostigmine 2.5 mg, preceded by atropine 1.2 mg,and the potentiation of the single twitch. Gallamine 10 mgantagonized the neuromuscular block of the tetanic response
and reversed the potentiation of the single twitch.
NEOSTIGMINE2.5»I I.v.
ATKOPINE SUXAMLMIONIUMl . 2 m e i . v . tl.3mgkgl i .v .
i l l )
mil
FIG. 7. Recordings from an anaesthetized patient showingthat blockade of the tetanic response by two doses ofneostigmine 2.5 mg was potentiated by suxamethonium
0.3 mg kg-1; fasciculations occurred on the single twitch.
UktORE NtObflCMlNL
17Ja AL rtRNEObllCMlNIi 2.5 nig x 2
1273l AFTER CAI.LAM1NE lUmg
FIG. 6. This recording, taken simultaneously as that shownin figure 7 but at a faster paper speed, shows that thecomplete tetanic fade which occurred after the two dosesof neostigmine 2.5 mg was almost entirely abolished by
gallamine 10 mg.
effect was seen in all four patients who were given thedrug in the presence of neostigmine block (fig. 5).The first dose of neostigmine 2.5 mg produced areduction in the peak contraction of the tetanicresponse which became more marked after a furtherdose of 2.5 mg; the single twitch was potentiated.Blockade of the tetanic response was rapidly antagon-ized by gallamine 10 mg, whereas a further dose of10 mg produced a small transient depression. In
contrast, the two doses of gallamine 10 mg progres-sively reversed the initial potentiation of the singletwitch. Figure 6, recorded at faster speed, showsthat the complete tetanic fade which occurred afterthe two doses of neostigmine 2.5 mg was almostentirely abolished by gallamine 10 mg. Finally, twopatients in this group were given suxamethonium0.3 mg kg"1 after neuromuscular block had beenestablished with neostigmine. In both instances theblock of the tetanic response was potentiated bysuxamethonium (fig. 7) and in each case the sub-sequent recovery was slow. Fasciculations precededthe block on the single twitch which recovered moreslowly than normal.
DISCUSSION
These studies in anaesthetized man have substantiatedthe early work of Briscoe (1936, 1937) who showedin cats that neostigmine and physostigmine rapidlydepressed the muscle responses to high rates ofstimulation and that these muscle responses becametwitch-like in character. Furthermore, Briscoe (1938)also reported that these effects of anticholinesterasedrugs could be abolished by curare and our observa-tion that gallamine will reverse neostigmine blockconfirms her claim.
In our studies neostigmine was given to one groupof patients in whom the recovery from neuromuscularblock by non-depolarizing drugs had been reversedby exposure to halothane. In these patients paralysisof the tetanic responses of the adductor polhrismuscle was antagonized by a first dose of neostigmine2.5 mg, whereas a second dose, given a few minutes
by guest on Novem
ber 7, 2016http://bja.oxfordjournals.org/
Dow
nloaded from

74 BRITISH JOURNAL OF ANAESTHESIA
later, reduced the peak height of the tetanic contrac-tion and produced tetanic fade. The study wasrepeated without halothane when a second dose ofncostigmine was usually less effective than in thosepatients who were also receiving halothane. Thisdifference is not surprising because we have demon-strated previously that halothane itself, in thepresence of a competitive blocking agent, will depressthe peak tetanic contraction and increase tetanic fade(Hughes and Payne, 1979).
The question then arose whether or not a singledose of neostigmine 5 mg would produce a similareffect as the same amount in two doses of 2.5 mgwhen given during recovery from blockade by com-petitive agents and in the presence or absence ofhalothane. In both instances, after the immediateantagonism by neostigmine 5 mg, there was atransient reduction in the peak height of the tetaniccontraction and a brief reappearance of tetanic fade.However, these effects were substantially less thanthose produced by 5 mg given in two doses of 2.5 mg.
Since the neuromuscular paralysing action ofneostigmine in the presence of a competitive blockingagent was more marked when given in divided doses,it is possible that the tetanic response had fullyrecovered after the first dose of neostigmine 2.5 mg,so that the second dose was acting on normal un-blocked muscle. When this hypothesis was tested inpatients who were not given neuromuscular blockingdrugs, one or two doses of neostigmine 2.5 mgproduced a substantial reduction in the peak heightof the tetanic contraction which persisted for about20min. The tetanic fade was so marked that thisresponse had now virtually become a single twitch.Furthermore, we found that the neostigmine blockcould be antagonized by a small dose of gallamineand potentiated by suxamethonium, the action ofwhich was also prolonged. These findings provideevidence that neostigmine, in sufficient dosage, willproduce an acetylcholine-induced block of thetetanic response in anaesthetized man. The preservedacetylcholine will accumulate at the muscle end-plateand produce a depolarization block.
Tetanic fade produced by anticholinesterases isassociated with a marked inhibition of acetylcholines-terase (Barnes and Duff, 1953). The end-platepotentials are prolonged and during high frequencynerve stimulation they summate and block the neuro-muscular function by a persistent depolarization ofthe postsynaptic membrane. It is worth noting thatanticholinesterase drugs also have a facilitatory actionon the motor nerve terminal (Riker and Standaert,
1966) which would further increase the acetylcholineavailable at the muscle end-plate. Furthermore, itis likely that such prejunctional events would be moreevident when the motor nerve terminals are fullyactivated and when the acetylcholine reserves arefully mobilized as during tetanic stimulation. It isalso possible that an initial excessive release ofacetylcholine produced by an anticholinesterase drugwould rapidly exhaust the available transmitterwhich may in part account for the transmission failure(Blaber and Bowman, 1963). No doubt each of thesefactors contributed to our observation that neostig-mine depressed the peak tetanic contraction andcaused severe tetanic fade in anaesthetized man.
In contrast, it was intriguing that the responses ofthe single twitch were in fact potentiated by one ortwo doses of neostigmine 2.5 mg and that gallaminerestored the single twitches to their initial contractionheight This feature illustrates the genuine differencesbetween the tetanic and single twitch responses. Thepotentiation of the single twitch response by neostig-mine may be explained by the fact that anticholines-terase drugs at low frequencies of stimulationproduce a short burst of muscle action potentials(repetitive firing) so that the muscle now responds asif stimulated at a higher frequency and the twitchtension increases (Brown, Dale and Felding, 1936;Brown, 1937). The increased availability of acetyl-choline at the muscle end-plate, mainly as a resultof inhibition of acetylcholinesterase and partly as aresult of an increased release of the transmitter fromthe motor nerve terminals, would augment andprolong the end-plate potentials and lead to repeti-tive firing of the muscle fibres as described by Eccles,Katz and KufHer (1942). However, the amount ofacetylcholine available, unlike that after highfrequency tetanic stimulation, is insufficient toproduce a depolarizing neuromuscular block. Never-theless, it must be emphasized that tetanic stimulationprovides the more physiological response sincebreathing and contractions of skeletal muscles areactivated by tetanic trains of stimuli rather than bysingle pulses.
It is not immediately clear why gallamine shouldantagonize the neuromuscular blocking action ofneostigmine, but the fact that the fade in the tetanicresponse was so rapidly reversed by gallamine mightimply that the drug was competing with the excessacetylcholine for the appropriate receptors and thisinterpretation is supported, if the earlier argument isaccepted, by the restoration to control height ofthe intensified twitch response, and the enhancement
by guest on Novem
ber 7, 2016http://bja.oxfordjournals.org/
Dow
nloaded from

NEOSTIGMINE BLOCK 75
of the ncostigmine block by suxamethonium givesfurther substance to this explanation.
It may be concluded from our results that neostig-mine, in clinical doses, could be a potential hazardin anaesthetic practice. Obviously, the critical factorsare the total dose of neostigmine administered and thedegree of recovery achieved when the drug is givento reverse paralysis. Clearly, if recovery of thetetanic response has reached about 50%, then asingle 2.5-mg dose should be sufficient to provideadequate reversal. If a larger dose of neostigmine isrequired for complete antagonism of a deeper block,then a single dose of 5 mg may be preferable to twodoses of 2.5 mg.
However, when full recovery has been achieved, afurther dose of neostigmine 2.5 mg could be hazardousbecause a prolonged depolarizing block with apnoeacould ensue. Moreover, it is possible that instancesof residual curarization after apparent inadequatereversal may have been attributable to overdosagewith neostigmine.
ACKNOWLEDGEMENTS
We are indebted to Miss V. A. Bishop, S.R.N., Mr D. Knox,B.TECH. and Mr A. J. Hannan for skilled technical assistance,to our surgical and nursing colleagues for their toleranceand patience and to our volunteers without whom thisstudy would not have been possible.
REFERENCES
Barnes, J. M., and Duff, J. I. (1953). The role of cholines-terase at the myoneural junction. Br. J. Pharmacol., 8,334.
Blaber, L. C , and Bowman, W. C. (1963). Studies on therepetitive discharges evoked in motor nerve and skeletalmuscle after injection of anticholinesterase drugs. Br. J.Pharmacol., 20, 326.
Briscoe, G. (1936). Shift in optimum rate of stimulationdue to prostigmine. J. Physiol. (Land.), 88, 48P.
(1937). Optimum stimulation rates for red and whiteskeletal mammalian muscles, and shift in rates producedby the eserine group. J. Physiol. (Lond.), 90, 10P.
(1938). Changes in muscle contraction curves pro-duced by drugs of the eserine and curarine groups. J.Physiol. {Lond.), 93, 194.
Brown, G. L. (1937). Action potentials of normal mammH-lian muscle. Effects of acetylcholine and eserine. J.Physiol. {Lond.), 89, 220.
Dale, H. H., and Feldberg, W. (1936). Reactions ofnormal mammalian muscle to acetylcholine and toeserine. J . Physiol. {Lond.), 87, 394.
Ecdes, J. C , Katz, B., and Kuffer, S. W. (1942). Effect ofeserine on neuromuscular transmission, j . Neurophysxol.,4,402.
Goodman, L. S., and Gilman, A. (1956). The Pharma-cological Basis of Therapeutics, 2nd edn, p. 451. NewYork: Macmillan.
Hughes, R., and Payne, J. P. (1979). Interaction of halo-thane with non-depolarizing neuromuscular blockingdrugs in man. Br. J. Clin. Pharmacol., 7, 485.
Riker, W. F., and Standaert, F. G. (1966). The action offacilitatory drugs and acetylcholine on neuromusculartransmission. Aim. N.Y. Acad. Sd., 135, 163.
Sugai, N., Hughes, R., and Payne, J. P. (1975). Theeffect of suxamethonium alone and its interaction withgallamine on the indirectly elicited tetanic and singletwitch contractions of skeletal muscle in man duringanaesthesia. Br.J. Clin. Pharmacol., 2, 391.
BLOCAGE NEUROMUSCULAIRE APRESADMINISTRATION DE NEOSTIGMINE
CHEZ LES ANESTHESIES
RESUME
Les reactions titaniques et de contraction unique du muscleadducteur du pouce ont servi a l'etude des effets neuro-musculaires de la neostigmine sur 26 patients anesthesies al'aide de thiopentone et de protoxyde d'azote. L'administra-tion intraveineuse de 2,5 mg de neostigmine apres exposi-tion a l'halothane a ete a l'encontre du blocage neuro-musculaire non depolarisant, alors qu'une seconde doseadministree entre 2 et 5 min plus tard a deprime la con-traction tetanique de crete et retabli le "fading'' tetanique.Sans halothane, la seconde dose de neostigmine a eumoins d'effet. La recuperation a la suite de la contractionunique n'a pas ete affectee par la second dose. Une seuledose de 5 mg de neostigmine s'est rapidement opposeeau blocage competitif de la reaction tetanique, mais lalegere depression ulterieure de la contraction de Crete etla breve reapparition de "fading" ont ete moins pro-noncees qu'apres radministration de 5 mg en deux dosesde 2,5 mg. Chez les patients n'ayant pas recu d'agents deblocage neuromusculaire, une ou deux injections de 2,5 mgde neostigmine ont considerablement reduit la contractiontetanique de crfite mais cause un "fading" tetanique gravequi a dure pendant environ 20 min; la contraction uniquea ete legerement activee. Le blocage de la reaction tetaniquepar la neostigmine peut etre oppose par la gallamine etactive par le suxamethonium. Les resultants de ces etudesfont ressortir que la neostigmine administree en dosescliniques peut 6tre a l'origine d'un blocage provoque parPacetylcholine, lequel pourrait presenter un risque eventuelen anesthesie.
NEUROMUSKULARE BLOCKIERUNG DURCHNEOSTIGMXN BEI NARKOTISIERTEN
MENSCHEN
ZUSAMMENFASSUNG
Die tetanische und die Einzel-Zuckreaktionen des Adductorpollicis-Muskel wurden zum Studium der neuromuskularenEffekte von Neostigmin bei 26 mit Thiopenton undStickoxyd narkotisierten Patienten verwendet. Neosrigmin(2,5 mg) wird intravenCs nach Halothan verabreicht undhatten eine Gegenwirkung auf die nicht-depolarisierendeneuromuskulare Blockierung, wogegen eine 2-5 min spfiterverabreichte Dosis die tetanische Spitzenreaktion unter-drtickte und ein tetanisches Absinken bewirkte. Bei
by guest on Novem
ber 7, 2016http://bja.oxfordjournals.org/
Dow
nloaded from

76 BRITISH JOURNAL OF ANAESTHESIA
Abwesenheit von Halothan war die zweite Neostigmin-Dosis weniger wirksam, und Wiederherstellung derEinzelzuckung wurde dadurch nicht beeintrachtigt. EineDosis von 5 mg Neostigmin brachte eine schnelle Gegen-wirkung gegen die Blockierung der tetanischen Reaktion,abcr die folgende leichte Unterdrtickung der Spitzenkon-traktion und das kurze Wiederauftreten des tetanischenAbsinkens waren geringer als nach einer Verabreichungvon 5 mg in zwei Einzeldosen zu 2,5 mg. Bei Patienten, diekeine Drogen zur neuromuskularen Blockierung erhaltennarten, bewirkten eine oder zwei lnjektionen von Neostigmin(2,5 mg) eine wesentliche Verringerung der tetanischenSpitzenreaktion und schweres tetanisches Absinken aufetwa 20min; die Einzelzuckung war leicht verstarkt. DieNeostigmin-Blockierung der tetanischen Reaktion konntedurch Gallamin aufgehoben und durch Suxamethoniumverstarkt werden. Diese Resultate zeigen an, dass Neostigminin klinischen Doseneine durch Azetylcholin bewirkteBlockierung hervorrufen kann, die eine potentielle Gefahrin der Narkosepraxis bedeuten kann.
BLOQUEO NEUROMUSCULAR PORNEOSTIGMINA EN HOMBRE ANESTESIADO
SUMARIO
Se usaron las respuestas contraccional unica y tetanica delmusculo aductor del pulgar para estudiar los efectos
neuromusculares de la neostigmina en 26 pacientes anestesi-ados mediante tiopentona y 6xido nitroso. Con 2,5 mg i.v.de neostigmina administrados despues de la exposici6nal halotano, se antagonizo al bloqueo neuromuscular no-depolarizante, mientras que mediante una segunda dosisadministrada 2-5 min despues, se deprimi6 la contracci6ntetanica tope y se restableci6 la debilitacidn tetanica. Al nousarse halotano con la segunda do~is, esta tuvo efectosmenores. La recuperaci6n de la contracci6n \inica no fueafectada negativamente por la segunda dosis. Una dosisunica de 5 mg de neostigmina antagonize rapidamente albloqueo competitivo de la respuesta tetanica, pero laligera depresi6n consecutiva de la contracci6n tope y labreve reaparici6n de la debilitacidn fueron menos fuertesque despues de la administraci6n de 5 mg en dos dosisde 2,5 mg cada una. En los pacientes a quienes no seadministr6 substancias bloqueadoras neuromusculares, unao dos inyecciones de 2,5 mg de neostigmina causaron unareducci6n substancial de la contracci6n tetanica tope yuna debilitaci6n tetanica severa que dur6 por 20 minaproximadamente; aument6 la potencia de la contraccibnunica de manera debil. Se podia antagonizar al bloqueode la respuesta tetanica por neostigmina mediante galaminay aumentarlo con suxametonio. Estos resultados indicanque la neostigmina en dosis clinicas puede producir unbloqueo inducido por acetilcolina, lo que constituirla unriesgo potencial en la anestesia.
by guest on Novem
ber 7, 2016http://bja.oxfordjournals.org/
Dow
nloaded from