neck disorder
TRANSCRIPT

یمبسم هللا الرحمن الرح

NECK PAIN &DISORDERS IN OCCUPATIONAL
MEDICINE(VIRTUAL WORKSHOP)

CONTENTS
1-EPIDEMIOLOGY(1,4)2-PSYCHOSOCIAL FACTORS AT WORK(4)3-ANALYSIS&DESIGN OF THE JOB(1)4-JOB HAZARD ANALYSIS(JHA)(OSHA)5-FITNESS FOR WORK(4) 6-RISK(ASSESSMENT,REDUCTION,ERGONOMY)(3)
7-SCREENING(4)8-SURVIALANCE(4)

A Systematic Approach
Through Problem Oriented Research

1-EPIDEMIOLOGY 1.1WHAT ARE THE NECK AND UPPER LIMB DISORDERS?
1.3 WHAT ARE THE EXPOSURES TO BE CONSIDERED?
1.4 WHAT ARE THE EXPOSURE RESPONSERELATIONSHIPS FOR NECK AND UPPER LIMBDISORDERS?
1.5 EXPOSURE RESPONSE RELATIONSHIP ACCORDINGTO A NIOSH DOCUMENT ON MUSCULOSKELETALDISORDERS AND WORKPLACE FACTORS
1.2 WHY IS THE EPIDEMIOLOGY IMPORTANT?

?

1.1 WHAT ARE THE NECK AND UPPER LIMB DISORDERS?
1.1.1 Non-specific musculoskeletal pain
- Pain in the neck/shoulder region with or without neck stiffnessand with tenderness over the descending part of the trapezius muscle (non-specific neck/shoulder pain)-Tension neck syndrome in literature-cervical brachial pain syndrome(M53.1)in ICD-10


1.1.2 Tendinitis
-Tendinitis is inflammation of the muscle tendon, the attachmentof the muscle to the bone.-Common locations for tendinitis are the shoulder(Rotator cuff,biceps-tendinitis), the elbow as a lateral epicondylitisor to the wrist as De Quervains disease (tendinitis in the long thumb abductorand the short thumb extensor)
1.1 WHAT ARE THE NECK AND UPPER LIMB DISORDERS?


1.1.3 Nerve entrapments
1.1 WHAT ARE THE NECK AND UPPER LIMB DISORDERS?
-Nerve entrapments occur where a nerve may come under pressure or isexposed to mechanical friction(CTS-Neurogenic TOS)


1.1.4 Degenerative joint disease and osteoarthritis
-Degenerative changes in the cervical spine (spondylosis, i.e. spurs and/ordisc degeneration) are common and 80% of the population may havedegenerative changes at the age of 50 years on radiographs.
-Cervical spondylosis is related to job titles with high load on the cervical spine (Hagberg and Wegman 1987). However, the correlation between symptomsand cervical spondylosis is poor (Friedenberg and Mileer 1963; Lawrence 1969).
1.1 WHAT ARE THE NECK AND UPPER LIMB DISORDERS?


1.2WHY IS THE EPIDEMIOLOGY IMPORTANT?
1-In the general workingpopulation in Sweden, as many as one-third of women and one-quarter ofmen reported pain in the neck and shoulder that was present every day orevery other day.
2-In some surveys up to 17-20% of people complain of neck-shoulder pain and 20% of hand-wrist pain during the past 7 days.
3-The HSE estimates an incidence of work-attributed upper limb and neck complaints in the UK of 186/1000 adults/year with 4.7 million lost working days per annum.

-Conditions external to the workers, such as job demands and job requirements-Generic physical risk factors for the neck and upper limbDisorders(not only job title) are force, posture, repetition, contact stress and temperature.(intensity, duration and frequency)
1.3 WHAT ARE THE EXPOSURES TO BE CONSIDERED?

1.4 WHAT ARE THE EXPOSURE RESPONSERELATIONSHIPS FOR NECK AND UPPER LIMBDISORDERS?-1995:‘Work related musculoskeletal disorders (WMSDS): a reference book for
Prevention-Institute Recherche, Santé et Securité de Travail deQuebec (IRSST)
-1995:American Academy of Orthopedic
Surgeons was published ‘Repetitive motion disorders of the upper extremity
-1997:NIOSH published
‘Musculoskeletal disorders and workplace factors—a critical review of theepidemiological evidence for work related musculoskeletal disorders ofthe neck, upper extremity and low back.’ -The evidence was grouped into four categories: strong evidence, evidence,insufficient evidence or evidence of no effect.
-1999:‘Risk factors for work-related neck and upper limb musculoskeletal disorders’
was published by the European Agency for Health at Work

1.5 EXPOSURE RESPONSE RELATIONSHIP ACCORDINGTO A NIOSH DOCUMENT ON MUSCULOSKELETALDISORDERS AND WORKPLACE FACTORS

1.2.1 The demand-control model:Organic changes(Catabolism&Anabolism)
--High demands high psychological demands
--Increasing job strain:
-- Increasing sleep disturbance and gastrointestinal symptoms
-- Decreasing testosterone blood concentration
--Increasing blood pressure during activities at work
-2.2.1 pain perception: Chronic pain syndromes (Depression)
-- Adrenocortical axis& turnover of endorphins
--3.2.1 possibility to cope with the illness
- Lack of possibility to influence decisions at work (authority over decisions) and sick leave
2-PSYCHOLOGICAL FACTORS AT WORK

3-ANALYSIS&DESIGN OF THE JOB






5-FITNESS FOR WORK
Fitness requirements:
These include good eyesight, adequate hearing, and reasonable head/neck mobility. The
ability to look over the shoulder is important. An operator should not have a condition that
predisposes to sudden loss of conciousness.

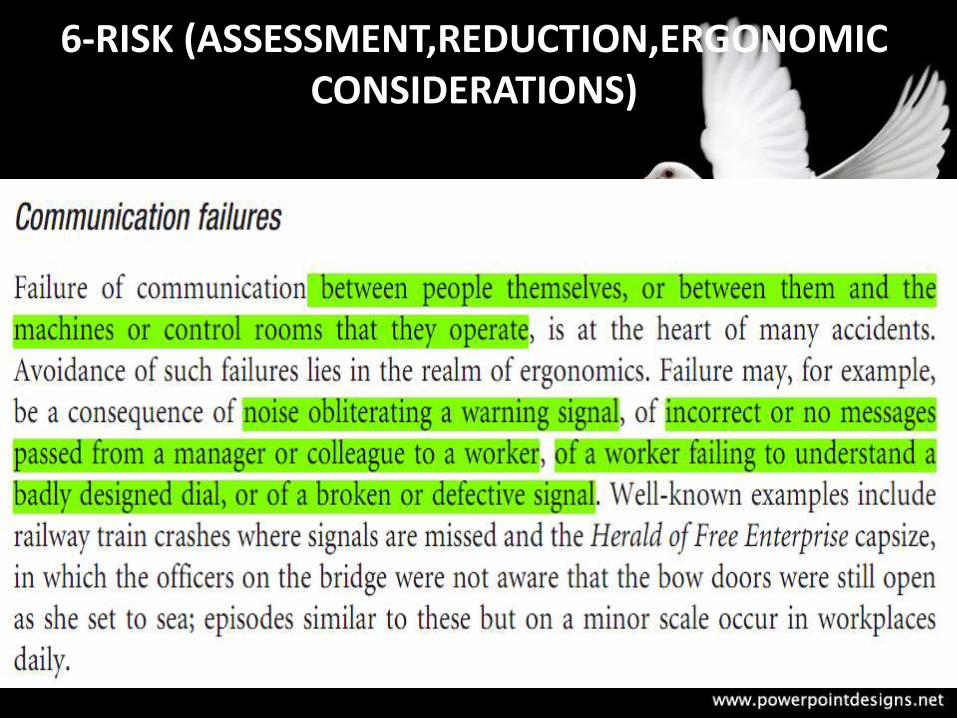
6-RISK (ASSESSMENT,REDUCTION,ERGONOMIC CONSIDERATIONS)
-Suspected Hazard
-Unsuspected Hazard:
-Gender: Almost 90 per cent of fatal and 78 per cent of other reportable industrial injuries occur in males, even though the numbers employed are roughly equal.
-Age: It might be thought that the young employee is at greater risk of industrial accidentthan the older worker, as is clearly the case with respect to traffic accidents.
When age and gender are considered together, there is a tendency for male accidentsto peak in the 25- to 34-year age group and for females this is in the 45- to 55-yeargroup. -

6-RISK (ASSESSMENT,REDUCTION,ERGONOMIC CONSIDERATIONS)

6-RISK (ASSESSMENT,REDUCTION,ERGONOMIC CONSIDERATIONS)

6-RISK (ASSESSMENT,REDUCTION,ERGONOMIC CONSIDERATIONS)
6-RISK (ASSESSMENT,REDUCTION,ERGONOMIC CONSIDERATIONS)

6-RISK (ASSESSMENT,REDUCTION,ERGONOMIC CONSIDERATIONS)
HOSTILITY
POSSIBILITY
COMPETITION

6-RISK (ASSESSMENT,REDUCTION,ERGONOMIC CONSIDERATIONS)
Physical (examples)Loading (lifting and handling)Poor postureRepetition, particularly at high speedHigh forcesIndividual differences, e.g. extremes of anthropometryPoor equipment and workplace design
Psychological (examples)Task overload/underloadMental workloadControl over workSocial supportIndividual differences (e.g. poor reaction times, mental ill health)Poor design of information, displays, controlsPoor system reliabilityHuman error
Organizational (examples)Long working hoursShift workShort deadlinesExcessive workloadPoor staffing levelsLack of worker involvement in system design
6-RISK (ASSESSMENT,REDUCTION,ERGONOMIC CONSIDERATIONS)
1.6Substitution
2.6Segregation
3.6Exhaust ventilation
4.6Dilution
5.6Personal protection
6.6Education and good housekeeping

6-RISK (ASSESSMENT,REDUCTION,ERGONOMIC CONSIDERATIONS)

7-SCREENING

7-SCREENING

7-SCREENING

7-SCREENING
7-SCREENING

7-SCREENING

8-SURVIALANCE

8-SURVIALANCE

8-SURVIALANCE
8-SURVIALANCE
GOALS OF SURVEILLANCE
-Detection of new problems
-Determine the magnitude of musculoskeletal disorders
--Track trends over time-(Surveillance evaluations may involve both the levels of occupational-exposures (hazard) and health outcome
-- Identify occupational groups, work sites to target control measures
--Describe health and risk factors to initiate ergonomic change

REFRENCES:1-Francesco V,Thomas A,Asa K.Occupational Ergonomics 2003
2-Waldermar K,William S.Marrs.Occupational Ergonomics 2003
3-Raymond A,Anthony S.Practical Occupational Medicine 2005
4-Julia S,Steven S.Oxford Handbook of Occupational Health2007