national rural health mission ministry of health and
TRANSCRIPT

5TH COMMON REVIEW MISSION
9TH -16TH NOVEMBER 2011
ASSAM
NATIONAL RURAL HEALTH MISSION
MINISTRY OF HEALTH AND FAMILY WELFARE
GOVERNMENT OF INDIA
2011
5TH COMMON REVIEW MISSION
8TH - 15TH NOVEMBER 2011
ASSAM
Dhubri
Nagaon

5th Common Review Mission-Assam 2011
2 | P a g e
TABLE OF CONTENTS
Lists of Chapters
Page No.
Abbreviations
03
Chapter I: CRM Team Members with Details
06
Chapter II: Introduction
07-13
(i) Assam: An introduction to the state 07 (ii) Public Health System in Assam 08
1. Infrastructure 08 2. Human Resource for Health 09 3. Health and Performance Indicators 11 4. Status of the PRI framework in the state 12 5. Special constraints 12
iii) Lists of facilities visited by the CRM team 13 Chapter III: Findings
14-53
(i) Changes in key aspects of health delivery system 14 1. Infrastructure Upgradation 14 2. Human Resource Health 15 3. Health Care Service Delivery- facility based –quantity and quality 17 4. Outreach Services 20 5. ASHA Program 22 6. RCH-II (Maternal Health, Child Health and Family Welfare) 23 7. Preventive & Promotive health services including Nutrition & Inter-
sectoral Convergence 30
8. Gender Issues & PCPNDT 31 9. National Disease Control Programmes 32 10. Programme Management 40 11. Procurement System 41 12. Effective Use of Information Technology 41 13. Financial Management 42 14. Decentralized local health action 45 15. Overall Outcomes 45
(ii) Progress against approved PIP of the state 50 Chapter IV: Case Studies on Success and Failure
54-55
Chapter V: Recommendations
56-62
Chapter VI: State Specific Issues
64-65

5th Common Review Mission-Assam 2011
3 | P a g e
Lists of Abbreviations:
AHS Annual Health Survey ANM Auxiliary Nurse Midwife ANC Ante-Natal Care AWTC Anganwadi Training Centres ANMTC Auxiliary Nurse Midwife Training Centre AWW Anganwadi Worker ASHA Accredited Social Health Activist API Annual Parasite Incidence ABER Annual Blood Examination Rate ARSH Adolescent Reproductive and Sexual Health AES Acute Encephalitis Syndrome AYUSH Ayurveda Yoga Unani Siddha Homeopathy BPM Block Programme Manager BHAP Block Health Action Plan BPHC Block Primary Health Center BSE Blood Slide Examined CHC Community Health Centre CRM Common Review Mission CEmOC Comprehensive Emergency Obstetric Care C-section Caesarean Section C‘NES Center for North East Studies and Policy Research DDT Dichloro-Diphenyl-Trichloroethane DMC Designated Microscopy Center DAM District Accounts Manager DHS District Health Society DRDA Department of Rural Development Agency DH District Hospital DHF Dengue Hemorrhagic Fever EAG Empowered Action Group FMR Financial Monitoring Report FRU First Referral Unit FP Family Planning GNM General Nurse Midwife GHCS General Health Care Staff GoI Government of India HR Human Resources HSC Health Sub Centre HMIS Health Management Information System IPHS Indian Public Health Standards IMR Infant Mortality Rate IUCD Intra-Uterine Contraceptive Device IDSP Integrated Disease Surveillance Programme IEC Information Education Communication IFA Iron Folic Acid ICDS Integrated Child Development Scheme IRS Indoor Residual Spraying IYCF Infant and Young Child Feeding

5th Common Review Mission-Assam 2011
4 | P a g e
IMNCI Integrated Management of Neonatal and Childhood Illnesses JSY Janani Suraksha Yojana JSSK Janani-Shishu Suraksha Karyakaram JE Japanese Encephalitis LHV Lady Health Visitor LLIN Long Lasting Insecticide Nets LSAS Life Saving Anesthetic Skills MPW Multi-Purpose Worker MMR Maternal Mortality Rate MTP Medical Termination of Pregnancy MVA Manual Vacuum Aspiration MBW New-Born Weight MU Mobile Medical Unit MDR Maternal Death Review MIS Management Information System MCTS Mother and Child Tracking System MP Malaria Parasite MPHC Mini Primary Health Center MGNREGA Mahatma Gandhi National Rural Employment Guarantee Act NLEP National Leprosy Eradication Programme NBCC New born Care Corner NPCB National Programme on Control of Blindness NLEP National Leprosy Eradication Programme NRHM National Rural Health Mission NVBDCP National Vector Borne Disease Control Programme NSSK Navjat Shishu Suraksha Karykram OPD Out-Patient Department OCP Oral Contraceptive Pill OPV Oral Polio Vaccine PIP Programme Implementation Plan PPI Pulse Polio Immunisation PHC Primary Health Centre PMU Programme Management Unit PPH Post Partum Hemorrhage PRI Panchayati Raj Institution PPP Public Private Partnership PWD Public Works Department RCH Reproductive and Child Health programme RHP Rural Health Practitioners RDK Rapid Diagnostic Kit RNTCP Revised National Tuberculosis Control Programme RI Routine Immunisation SDO Sub Division Officer SRS Sample Registration Survey SOE Statement of Expenditure SOP Standard Operating Procedure SPMO State Programme Management Officer SDH Sub Division Hospital SBA Skilled Birth Attendant

5th Common Review Mission-Assam 2011
5 | P a g e
SPR Sputum Positivity Rate SHS State Health Society SFR Slide Falciparum Rate STS Senior Treatment Supervisor STLS Senior Tuberculosis Leprosy Supervisor TOR Terms of Reference TFR Total Fertility Rate TB Tuberculosis VHND Village Health and Nutrition Day VHSC Village Health and Sanitation Committee UC Utilization Certificate UF Untied Funds

5th Common Review Mission-Assam 2011
6 | P a g e
CHAPTER I: TEAM COMPOSITION OF CRM: ASSAM
Under National Rural Health Mission (NRHM)
(8th -15th November 2011) Organized by
NRHM Ministry of Health & Family Welfare
Government of India CRM Team Composition:
Sl. No.
Name of Official Designation Contact Details
1. Dr. Rakesh Kumar Director (NCD) Ministry of Health & Family Welfare, Government of India, New Delhi-110001
2. Dr. V. K Raina
Joint Director, (NVBDCP)
Ministry of Health & Family Welfare, Government of India, New Delhi-110001
3. Dr. Partha Jyoti Gogoi Regional Director (ROHFW Regional office for Health & Family Welfare, Director General of Health Services, Guwahati, Assam
4. Dr. V. K Manchanda
Consultant (RCH) World Bank
5. Dr. Pradeep Khasnobis
CMO (IDSP)
Ministry of Health & Family Welfare, Government of India, New Delhi-110001
6. Dr. A. Raghu
Assistant Advisor, AYUSH
Ministry of Health & Family Welfare, Government of India, New Delhi-110001
7. Prof. J. K. Das
Dean of Studies
National Institute of Health & Family Welfare, Baba Ganganath Marg, Munirka, New Delhi-110067
8. Dr. K.S Jacob Professor of Psychiatry, CMC Christian Medical College, Vellore -632002 Tamil Nadu
9. Dr. Suchitra Lisam
Senior Consultant (HRH)
National Health Systems Resource Center (NHSRC), NIHFW Campus, Baba Ganganath Marg, Munirka, New Delhi-110067
10. Dr. Abhishek Gupta
Consultant (NRHM-III) Ministry of Health & Family Welfare, Government of India, New Delhi-110001
11. Dr. Bhrigu Kapuria
Consultant (UIP) World Health Organization,
12. Mr. Puneet Jain
Consultant (FMR) FMG
Ministry of Health & Family Welfare, Government of India, New Delhi-110001

5th Common Review Mission-Assam 2011
7 | P a g e
CHAPTER II: INTRODUCTION
(i) Introduction to the State: Assam
Assam is the gateway to the northeastern part of India and it is popularly called as the land of the red river and blue hills. The name "Assam" is derived from the term "Asom" which, in Sanskrit, refers to ―unequal or unrivalled‖ due to the uneven topography of the land which is full of hills, plains and rivers. The state is almost entirely isolated from the rest of the country except for a narrow corridor running through the foothills of the Himalayas that connects the state with West Bengal. It is bordered in the North and East by the Kingdom of Bhutan and Arunachal Pradesh; along the south lie Nagaland, Manipur and Mizoram. Meghalaya lies to her South-West, Bengal and Bangladesh to her West. The economy is based on agriculture and oil and produces a significant part of the total tea production of the world. Assam got statehood on 15th August 1947 and has 126 legislature seats. The capital city is Dispur and Guwahati is the largest city. The official languages are Assamese, Bodo and Karbi.
As per 2011 census, the population of Assam is 31.17 million and the population is scattered across 27 districts and 26312 villages. Assam is divided into three regions, each headed by a commissioner. Under each commissioner, there are several administrative units called Districts. The State has the highest population density among the North Eastern states, of 396.8/km2. The literacy rate is 73.13%; the male literacy rate is 78.81% and female literacy rate is 67.27%. The sex ratio (male: female) is 1000: 954.
Table I: Demographic, socio-economic and Health Profile of Assam in comparison to India figures
Sl. No. Item Assam India 1. Total population (Census 2011) (in million) 31.17 1210.19 2. Crude Birth Rate (SRS 2011) 23.6 22.5 3. Crude Death Rate (SRS 2011) 8.4 7.3 4. Total Fertility Rate (NFHS 3) 2.42 2.68 5. Infant Mortality Rate (SRS -2009) 61 53 6. Maternal Mortality Ratio (SRS 2007-2009) 390 252 7. Sex Ratio (Census 2011) 954 940 8 Population below Poverty line (%) 36.09 26.10 9. Schedule Caste population (Census 2008) (%) 6.85 166.64 10. Schedule Tribe population (Census 2008) (%) 12.41 84.33 11. Female Literacy Rate (Census 2011) (%) 67.27 65.46
The CBR and CDR of Assam are 23.6 and 8.4 as per SRS 2011 while the all India figure is 22.5 and 7.3 respectively. The state has higher IMR of 61 and MMR of 390 as compared to the all India figures of 50 and 252 while the TFR is 2.42 which are lower than all India figures of 2.68. The state has 27 districts, 56 sub-divisions/Talukas, 219 blocks and 26312 villages.
Table 2: State Profile
Sl. No. Items No. 1. Districts (RHS 2010) 27 2. Sub Division/Talukas 56 3. Blocks 219 4. Villages (RHS 2010) 26312

5th Common Review Mission-Assam 2011
8 | P a g e
(ii) Public Health System in Assam:
1. Public Health Infrastructure: As per state report 2010, the state has 4604 HSC, 856 PHC including block PHCs, 108 CHC, 25 District hospitals, 13 Sub-divisional hospitals, 4 Medical colleges, 1 Nursing college, 18 ANM training centers, 15 GNM training centers, 1 Ayurveda hospital, 1 Unani dispensary and 3 Homeopathic hospitals. The state falls short of 1396 SHC, 144 PHC and 6 medical colleges as per the below mentioned number of heath institutions compared against the population norms and IPHS 2011.
Table 3: Public Health Infrastructure in the State:
Sl. No.
Type of Health Institutions No. as in 2005 No. as in 2010
1. Health Sub-centers 4726 4604* 2. Primary Health Centers 647 856 3. Block Primary Health Centers 149 149 4. Community Health Centers 93 108 (FRU=6) 5. District and Sub divisional hospitals (SDH) 21/03 24/13 (FRU=10 6. Medical Colleges 03 04 6. B. Sc. Nursing Colleges 01 03 8. ANM Training Centers 18 18 9. GNM Training Centers 15 20 10. Ayurveda Hospitals /Dispensaries 01/380 01/380 11. Homeopathic Hospital/Dispensaries 3/75 3/75 * As per facility survey, 2010
Over the year since 2005, there has been increase in the number of HSC, PHCs, CHCs, SDH and DH across the state. The state has 4 medical colleges which are recognized by MCI and 2 more newly constructed medical colleges are in the process for starting admission from 2012.
Table 4: Infrastructure Up-gradation of facilities in Assam
Item No. functional in 2005
No. functional as in Sept’2011
No. of facilities under construction
Total No. which will be functional by March’11
District Hospital 21 24 06 ? Sub-Divisional Hospitals and other hospitals above CHC
03 13 01 ?
Community Health Centre 93 103 60 ? Block Primary Health Center 149 149 0 ? Other Health facilities above SC but below block level (may include APHC etc.)
663 789 152 ?
Health Sub-centre 4726 4604* 1292 ? * Out of 4604 HSC, 691 HSC which were located in rental buildings have been constructed under NRHM

5th Common Review Mission-Assam 2011
9 | P a g e
2. Human Resource for Health
Human Resource Policy and Planning: In the past, the state has taken up numerous initiatives and adopted strategies for ensuring the availability of skilled human resources, particularly in remote and peripheral areas of Assam. Though there is lack of a human resource policy in the state, the state has made efforts in meeting the requirements of human resources. The state has rolled out the 3-years rural health course so as to ensure that skilled manpower is available in rural areas. The state is under the process of considering the proposal for creation of a specialist cadre in 2012. The state has developed an MIS for human resource, which is used for management of human resource in areas of transfer and posting primarily. Availability & Gap Analysis of Human Resources:
Table 5: Human Resource Augmentation under NRHM at all the facilities
Category In position as in Sep’11 Requirements as per IPHS Sep’2011
Shortfall in Numbers & percentage
Regular Contractual Total
Medical Officer 2256 896 3154 3787 633 (16%) Specialist 827 87 914 1303
389 (29%)
Staff Nurse 2552 2987 5539 9854 4315 (43%) Laboratory Technician
707 584 1299 2635 1344 (51%)
Pharmacist 1110 279 1383 2447 1064 (43%) ANM 5189 4921 10110 10422 312 (3%) The state has added 896 MOs, 2987 staff nurses, 584 laboratory technicians, 279 pharmacist and 4921 ANMs on contractual basis as in September 2011. The state has shortfalls for almost all categories of staffs. Out of 3787 MOs required as per IPHS September 2011; only 3154 including both regular and contractual MOs are in position as in September 2011 which shows shortfall of 633(16%). Data reveals that the maximum shortfall is in the staff nurses and pharmacist category in the state. Mobile Medical Units are functional in all districts along with boat clinics in the PPP mode. The state conducts recruitment fairs (melas) on regular basis for appointment of large number of contractual employees under NRHM. The recruitments of medical officers and specialists from medical colleges have ensured their availability in public health facilities through enforcement of the compulsory government service bond.
Training Status of Human Resources:
Training is one of the critical areas which requires more focus since there is a huge gap in the number of training schools required for imparting training in B.Sc (Nursing), ANM and GNM courses.

5th Common Review Mission-Assam 2011
10 | P a g e
Table 6: Training institutions in the State and their Intake capacity
Training School Govt. (Sept 2011)
Govt. (added during Mission Period)
Private (Sept 2011)
Number Intake Number Intake Number Intake ANM Schools 18 775 0 0 9 375
LHV Schools 1 60 0 0 0 0
GNM Schools 20 830 5 250 19 510
MPHW Schools MPW trained at 3 Para-medical School of the State Post Basic B.Sc. (Nursing)- College
1 20 0 0 3 95
B.Sc. (Nursing) College
1 60 2 120 * 5 190
M.Sc. (Nursing)College
2 37 0 0 1 10
* Admission will start from 2012.
Table 7: Training Status of Human Resources (Cumulative achievement 2005 – 2011, Sept)
Type of Training No. & Percentage of Health Personnel Received training out of total in-position
ANMs (in position=10110)
Staff Nurses (In position=5539)
Medical Officers (In position=3154)
IUCD 3882 (38.3%) 867 (15.6%) 936 (29.6%) NSSK 225 (2.2%) 1118 (20%) 864 (27%) SBA 1359 (13.4%) 1974 (35.6%) 399 (12.6%-ToT)
IMNCI 4139 (40%) N/A 435 (13.7%-ToT) BeMOC N/A N/A 93 (2.9%) Mini Lap N/A N/A 101 (3.2%)
LSAS N/A N/A 36 (1%) CEmOC N/A N/A 24
MTP/ MVA N/A N/A 280 (8.8%)
NSV N/A N/A 166 (5.2%)
Out of 3154 MOs, majority of them i.e 936 (29%) and 864 (27%) received trainings in IUCD NSSK respectively. Only 36 (1%) were trained in LSAS. Out of the total 5539 staff nurses, 1974 (35.6%) received trainingin SBA while 4139 (40%) and 3882 (38%) of ANMs were trained in IMNCI and IUCD insertion respectively. It showed that up-gradation of skills of health personnel through capacity building initiatives needs further improvement.

5th Common Review Mission-Assam 2011
11 | P a g e
3. Health and Performance Indicators
The public health performance in Assam has been gradually improving over the years and positive trends for the three indicators i.e. IMR, MMR and TFR are very much suggestive of that. Table 8: Trends, current status and target of key health indicators for the year 2011-12
Indicator Assam Target
for 2011-12
Target for India (2011-12)
Goal (AI)
Year SRS (2001-03)
SRS (2004-06)
SRS (2007-09)
IMR
68 66 61 <40 <30 <30
MMR 301
480
333 (CES, 2009-10)
200 <100 100
TFR
2.9 2.7 2.4 (DLHS-3) 2.1 2.1 2.1
As compared to the all India figures for key heath indicators such as IMR and MMR, the state is lagging behind in almost all except for TFR. Table 9: Comparative status of key health indicators as against All India figures
Sr. No.
Indicators State All India
1. Infant Mortality Rate (SRS-2009) 61 53 2. Maternal Mortality Rate (SRS -2007-2009) 390 212 3. Total Fertility Rate (DLHS-3) 2.4 2.6 4. Institutional Deliveries (In Lakhs) (MIS) (2010-11) 4.18 168.05 5. Full immunization (In Thousands) (MIS) (since Apr 2010) 589 21317
Table 10: Trends, current status and target for 2011-12 for other key health indicators Other Key Health Indicator
Assam Target for 2011-12
Year DLHS-2 DLHS-3 2010-11
Mothers who had 3 or more ANC (%)
42.6 45.2 60.13 85
% of Institutional Delivery
26.8% 35.3% 3.13 lakhs 65%
Safe Delivery (SBA Assisted) (%)
33.2 40.9 81.07 NA

5th Common Review Mission-Assam 2011
12 | P a g e
4. Status of the PRI framework in Assam The Government of Assam enacted the Assam Panchayat Raj Act, 1994 incorporating almost all the features of the 73rd Constitutional Amendment Act, 1992. The terms of Panchayat in the state expired in October 1997. The state government had put off the Panchayat elections several times citing different reasons. The elections of the Panchayat bodies were held in December 2007 and since then the PRI bodies are active in the State.
The PRIs have been actively involved with developmental process at all the levels are involved in the planning, implementation and monitoring of the activities envisagedunder National Rural Health Mission, Sarbha Siksha Abhiyan, Public Health Engineering, Total Sanitation Campaign and Women & Social Welfare department in the state.
Under the NRHM, in each village a Village Health Sanitation (& Nutrition) Committee (VHSNC) has been formed where the elected PRI members are the Chairman of the committee and the ASHAs are the Member Secretary. 26,312 VHSNC have been formed in Assam. The ASHAs are working in close co-ordination with the VHSNC members for improving the health scenario of the village. Every year under NRHM, each VHSNC receives Rs. 10,000/- which is used for providing safe drinking water, construction of sanitary toilets, arranging emergency referral transport and organizing Village Health & Nutrition Day.
All the VHSNC members have been trained under NRHM regarding their roles and responsibilities in the years 2009-10 and 2010-11. In 2010-11 and 2011-12, on sample basis Model Village Plans havebeen prepared in each Block PHC.
5. Special Constraints
Internal issues within the state government led to delays in decision making, especially regarding certain reform measures concerning various cadres, their service conditions. This also affected the civil construction work undertakenin many health facilities. This adversely affected the upgradation of the state health system in general and the state lagged behind the other EAG states. The law and order issues heavy rains had also adversely affected the outreach and peripheral healthcare services, resulting in increased absenteeism, lack of supervision by the supervisory authorities in the state. It also affected the emergency and referral transportation as many times dug-up roads delayed the access to appropriate heath facilities.
5th Common Review Mission-Assam 2011
13 | P a g e
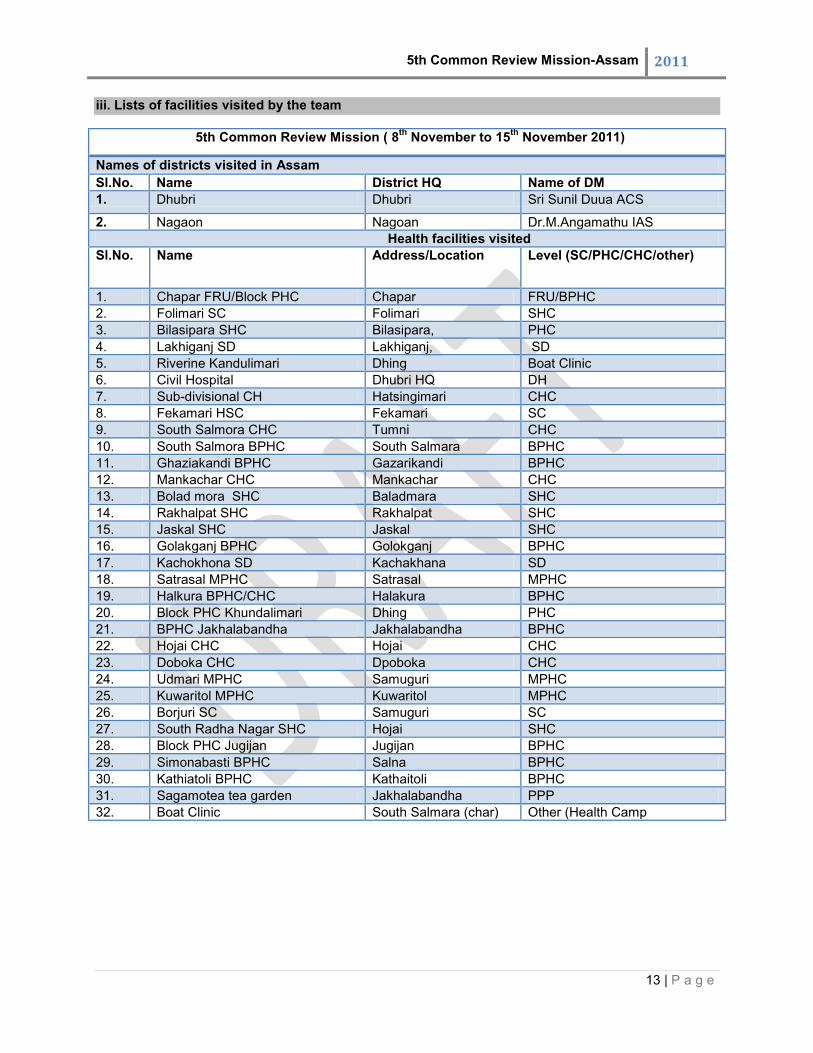
iii. Lists of facilities visited by the team
5th Common Review Mission ( 8th November to 15th November 2011)
Names of districts visited in Assam Sl.No. Name District HQ Name of DM 1. Dhubri Dhubri Sri Sunil Duua ACS
2. Nagaon Nagoan Dr.M.Angamathu IAS Health facilities visited Sl.No. Name Address/Location Level (SC/PHC/CHC/other)
1. Chapar FRU/Block PHC Chapar FRU/BPHC 2. Folimari SC Folimari SHC 3. Bilasipara SHC Bilasipara, PHC 4. Lakhiganj SD Lakhiganj, SD 5. Riverine Kandulimari Dhing Boat Clinic 6. Civil Hospital Dhubri HQ DH 7. Sub-divisional CH Hatsingimari CHC 8. Fekamari HSC Fekamari SC 9. South Salmora CHC Tumni CHC 10. South Salmora BPHC South Salmara BPHC 11. Ghaziakandi BPHC Gazarikandi BPHC 12. Mankachar CHC Mankachar CHC 13. Bolad mora SHC Baladmara SHC 14. Rakhalpat SHC Rakhalpat SHC 15. Jaskal SHC Jaskal SHC 16. Golakganj BPHC Golokganj BPHC 17. Kachokhona SD Kachakhana SD 18. Satrasal MPHC Satrasal MPHC 19. Halkura BPHC/CHC Halakura BPHC 20. Block PHC Khundalimari Dhing PHC 21. BPHC Jakhalabandha Jakhalabandha BPHC 22. Hojai CHC Hojai CHC 23. Doboka CHC Dpoboka CHC 24. Udmari MPHC Samuguri MPHC 25. Kuwaritol MPHC Kuwaritol MPHC 26. Borjuri SC Samuguri SC 27. South Radha Nagar SHC Hojai SHC 28. Block PHC Jugijan Jugijan BPHC 29. Simonabasti BPHC Salna BPHC 30. Kathiatoli BPHC Kathaitoli BPHC 31. Sagamotea tea garden Jakhalabandha PPP 32. Boat Clinic South Salmara (char) Other (Health Camp
5th Common Review Mission-Assam 2011
14 | P a g e
CHAPTER III: FINDINGS
(i) Changes in key aspects of health delivery system
The CRM team for Assam split into two teams so that one team visited the facilities in Dhubri covering both the northern and Southern region and the other team visited the facilities in Nagaon district. The team for Dhubri comprised of Dr. Rakesh Kumar, Dr. Partha Jyoti Gogoi, Dr. J.K Das, Dr. A. Raghu, Dr. Suchitra Lisam and Dr. Bhrighu Kapuria and the team for Nagaon comprised of Dr. V.K Raina, Dr. V.K Manchander, Dr. Pradeep Khasnobis, Dr. K.S Jacob, Dr. Abhishek Gupta and the financial aspects of both districts was reviewed by Mr. Puneet Jain. The team had the following observations with respect to the sixteen thematic components identified in the ToR of CRM, for the state of Assam based on the observations, on-site assessment and review of secondary data in both the districts and the state.
1. Infrastructure Upgradation
Good infrastructure is available at all facilities visited by the two sub-teams except for the newly constructed District hospital, Dhubri, which has faulty architectural design and the maintenance was found to be extremely poor. Almost 47 % of all sub-centers are located in government owned buildings but quite a few lack water and electricity connections.
The State has upgraded 494 health facilities including CHCs, PHCs and Mini PHCs for providing 24x7 services. The state has a policy of posting at least 1-2 doctors at each upgraded PHC including the AYUSH doctors. They are to be supported by at least 2 GNMs and an adequate number of ANMs.
The 24x7 facilities are required to provide normal deliveries, assisted deliveries and management of complicated deliveries services before they are referred to higher centers. While normal deliveries were being conducted at all the facilities, none of the facilities was geared up to provide other services.
Irregular power supply and lack of electric, water and internet connectivity, mostly in PHCs/CHCs and sub-centers located in remote and rural areas. Water and electricity are also not available at new delivery points were RHP has been posted, however, other basic infrastructure related to institutional deliveries were available.
o No electricity and water connection at Folimari Sub-center, Dhubri o Irregular electric supply without water connection at Satsingmari Civil
Hospital/CHC, Dhubri o Lack of separate toilets for male and female patients in most facilities in both
districts o Old sub-center buildings do not have provision for stay of ANM o There is an acute shortage of inpatient beds for MCH care in District hospital o Signages generally in place and Citizen Charter and list of drugs are displayed in
most of the facilities.
24 district hospitals are designated as FRUs and are equipped to provide comprehensive CEmOC. In addition, 38 out of 108 CHCs are stated to be operational as FRUs. The team was intimated that most of these now fulfill the 3 critical criteria of functionality.

5th Common Review Mission-Assam 2011
15 | P a g e
Nagaon District, The FRU buildings have been renovated using NRHM funds. All were functional to the
extent that caesarean sections were being done and newborn services were available with atleast 2 gynecologists and atleast one each of anesthetist and pediatrician. However, only 1 FRU at CHC, Jakhalbandha had a fully functional blood storage unit.
Dhubri District, The FRU facility has adequate infrastructure with a fully equipped operation theatre and
blood storage facility. The hospital also has a gynecologist and pediatrician but there was no anesthetist and it is not a functioning FRU. The facilities for institutional delivery at the South Samara block are in infancy stage. During FGD, it was informed that around 95% of the deliveries in that area are conducted by traditional dais at home (few assisted by ANMs from Sub-centre) and only complicated cases were referred to district hospital. The reason cited by the community was the non-availability of ANM at the sub centre when required, although nearly all sub-centers have 2 ANMs attached. ANMs informed that their duty roster is such that both of them have to be in field except for 2 days in a week. Moreover, the area being a difficult terrain, none of the ANMs prefer to stay back due to security reasons besides lack of basic facilities in most health centers making it further difficult to reside there.
2. Human Resource Planning
In overall, there is shortage of skilled human resources such as doctors (allopathic & AYUSH), specialists (pediatrician, physician, anesthetist, radiologist etc), staff nurses, MPW, laboratory technicians and pharmacists and there are there are geographical barriers making the retention of manpower further difficult. The shortfall of human resource; doctor (16%), specialist (29%), staff nurse (43%), laboratory technician (51%), pharmacist (43%) and ANM (only 2%) aggravates the problem further . The facilities visited by the teams had 2-3 doctors including the AYUSH doctor. Gynecologists were also available at some of the block PHCs in Nagaon. Each facility had 2-3 GNMs and they conduct deliveries. A number of these GNMs and some ANMs had received SBA training. In addition, in one 24x7 facility, a trained doctor in Basic emergency obstetric care was also available.
o In Dhubri district with approximately 20 lakh population, there are only 5 gynecologists, 2 surgeons, 3 pediatricians, 1 anesthetist, 1 trained anesthetist and 1 radiologist to cater the healthcare needs of the whole district. As per IPHS, in respect of existing facilities for the district; Specialists: Out of 48 total sanctioned posts for all categories in the district,
25 posts are filled up. Shortfall is 52% Staff nurse/GNM: Out of IPHS requirements for 90 staff nurses/GNM for a
200 bedded district hospital, only 47 staff nurses/GNM were in position. Shortfall is 53%.
o There are adequate numbers of Doctors (242), Staff nurses and Programme Managers in Nagaon district, 2 or more Gynecologists were posted at all the FRUs, 5 gynecologists were posted in District hospital, Nagaon
There is no specialist cadre in the state and it is under the consideration of the state government.

5th Common Review Mission-Assam 2011
16 | P a g e
The state Government is planning to start a 2-years diploma course in 2012 in Maternal Health, Paediatric Medicine, Clinical Anaesthesiology and Radiology to be imparted through five Medical Colleges of Assam under Srimanta Sankaradeva University of Health Sciences, Guwahati with a total intake of 156..
Some of the facilities are managed by AYUSH doctors since there are more AYUSH doctors available than the sanctioned posts (out of total 22 sanctioned posts; there are 52 AYUSH doctors of which 30 are contractual employees)
Lack of trained and qualified staff for hospital management and for the management of other ancillary and support services viz. medical records, central sterilization department, laundry, housekeeping, dietary and management of nursing services.
o There are no posts sanctioned for dietician in the 200 bedded district hospital of Dhubri, though there is a requirement of a dietician as per IPHS norms
There is an irrational deployment of manpower particularly para-medicals and staff nurses. Though there are 125 GNMs as against the total 78 sanctioned posts for Dhubri district, there is only 1 GNM (contractual) posted at Bilasipara Subsidiary Health Center, which runs as a emergency 24*7 PHC with 12 beds and covers nearly 1.40 lac population.
The service conditions, remunerations for doctor, nursing staff and paramedical under NRHM are at par with the state government employee.For nursing staff and paramedics, the salary under NRHM is higher than those in the private sector.
For the Dhubri district, there is only 1 ANMTC and 1 GNMTC attached to the district hospital. There is a huge backlog for trainings of ANMs in the district. No trainings for ANMs had been conducted since March 2007, though the GNM trainings are conducted every year on regular basis.
The state had initiated a 3 years course named ―Diploma in Medicine and Rural Health Care‖ (DMRHC) in 2005 as a response to the shortage of skilled human resources in remote and rural areas. As in September 2011, 19 Rural Health Practioners (RHP) were deployed in health sub-centers in remote and rural areas of Dhubri district out of total 261 RHPs in the state.
Other issues observed by the team and sub-team are as follows:
(a) Availability of Human Resources and Gap Analysis
Overall in the state, there are shortfalls in almost all categories of Human resources. The number of shortfalls for doctors (allopathic) is 633 (16%), specialist is 389 (29 %), staff nurse is 4315 (43 %), ANM is 312 (2%), LT is 1344 (51%), and pharmacist is 1064 (43%) respectively.
o Out of 168 sanctioned posts for all medical (Allopathic, Dental & AYUSH) categories, 157 posts are filled up in Dhubri district
o Excess GNM/ANM are posted as against the sanctioned posts in the Dhubri district. 125 GNMs and 466 ANMs are posted, though the total sanctioned posts are 78 and 323 respectively.
o There was no anesthetist at Chapor Block PHCof Dhubri district for the last 2 years though there was 1 post sanctioned.
5th Common Review Mission-Assam 2011
17 | P a g e
(b) Pre-service Training capacity
There was no training calendar in place for trainings of various cadre/categories of staffs.
o Out of 56 M.O in Dhubri district, only 2 were trained on Mini-Lap. o MOs, GNM/ANM need regular orientation or refresher trainings on various fields o Out of 125 GNM posted in Dhubri, 80 had received trainings on SBA till September
2011 (11 GNM trained in 2011-12 till Sep). o Out of 466 ANM posted in Dhubri, 94 had received trainings on SBA till September
2011 (only 5 ANM trained in 2011-12 till September 2011). o The trainings of ANM at ANMTC established in 1983 in Dhubri had been
discontinued since 2007
(c) Plan for Augmentation of Health Human Resources
The state is planning to respond to the shortage of specialists in the state/district, particularly gynecologist, pediatrician, anesthetist and radiologist etc with the initiation of a 2-years diploma course in Maternal Health, Paediatric Medicine, Clinical Anaesthesiology and Radiology in 2012.
The state will continue to produce more RHPs to bridge the gap in availability of skilled human resource in remote and rural areas.
AYUSH doctors are being recruited and posted at CHC/PHC as replacement of MOs
(d) Skills in Available Health Human Resources
Quality of laboratory technicians posted at remote health facilities need close attention, particularly in conducting the routine investigations for blood and urine which normally does not take place due to unavailability of stock/reagents or lack of water supply. For example, in Hitsingmiri civil hospital no routine blood and urine examination were being conducted for the reasons cited above.
The skills required through trainings on CEmOC and LSAS had not been utilized due to lack of follow-up supervision or reasons best known to administrators/officers.
3. Health Care Service Delivery- facility based –quantity and quality
The healthcare services are provided through 3699 sub-centers with 2 ANMs, 216 PHCs
with 3 staff nurses and 43 CHCs with 9 staff nurses across the state. Overall, there has been increase in the number of OPD cases and IPD admissions over
the years in the state. The number of OPD since 2005-06 has shown an increasing trend as shown in Figure 1. In 2005-06; 5,39,1318 OPD cases were registered and in 2010-11; 20,85,2677 OPD
cases were registered and upto September 2011; 12,33,7134 OPD cases were registered.

5th Common Review Mission-Assam 2011
18 | P a g e
Figure 1: The trend in OPD cases over the years
The number of IPD since 2005-06 has shown an increasing trend as shown in Figure 2 below.
In 2005-06; 2,53875 IPD cases were registered and in 2010-11; 10,27768 IPD cases were registered and upto September 2011; 5,91971 IPD cases were registered.
Figure 2: The IPD trend over the years
The maternal death audits were not being doneregularly and no measures were taken up
to find out the reasons and to take steps for improvements. In most of the cases, the cause of maternal death was mentioned as anemic failure which is a non-existent

5th Common Review Mission-Assam 2011
19 | P a g e
terminology but the real cause of death as reviewed by CRM was due to ?? hypovolumic shock due to mismanaged or untreated hemorrhage.
There are incidents of drug stock-out in periphery such as Hitsingmiri civil hospital, Mankachar CHC etc. The doctors often prescribe non-generic medicines compelling the patients to buy medicines from the market.
The basic laboratory and diagnostic services for conducting routine blood and urine tests are not available either due to lack of reagents and equipments or due to lack of water/electric supply or otherwise. The diagnostic facilities are very poor at periphery and most of them used RDK for MP even at PHC/CHC level.
There was no infection control committee in any of CHC and district hospital and there has been no orientation on Universal Safety Precautions. There was no quality assurance committee being constituted at district hospital.
In general, the Bio-medical waste management was non-functional and the concept of bio-medical waste management as regards to segregation and safe disposal of waste materials is lacking among the staffs. At most facilities reviewed, only one single color three waste baskets were placed through the guidelines on BWM is displayed.
There were common toilets for male and female patients in almost all facilities except at the district hospital. Toilets for general wards were dirty with irregular water and electric supply.
Emergency referral transport is in place and is being used for referral purposes. The incentive under JSY is paid mostly through cheque or e-transfer. Almost 50% of the
fund for ASHA and for patients under JSY could notbe encashed since the bank refused to issue cheque- books with zero balance account.
No SOP was found in the hospital. Under support services, the diet at district hospital is outsourced, however the same kind
of arrangement is not available at CHC/PHC. Signages are visible. Citizen charter and Janani Shishu Suraksha Karyakram (JSSK)
guidelines were displayed only in some facilities in Nagaon while in Dhubri, citizen charters was found everywhere)
There are proper IEC materials/posters displayed at almost all facilities visited.
Dhubri district Overall there has been a declining trend in the number of OPD and IPD in 2011-12 (April
to Sept) with 579234 and 24628 as compared to 652006 and 26455 in 2010-11 (April to Sept) for Dhubri district. The OPD and IPD figures have come down in the entire district in 2011-12 in comparison to 2009-10 and 2010-11 due to non-availability of doctors and irregular supply of medicines.
At Chapor FRU/CHC, there were 53,398 OPD, 5307 IPD cases in 2009-10 and in 2010-11 there were 55,983 OPD and 4770 IPD cases and 35228 OPD and 2661 IPD cases in 2011-12 (upto Oct‘11)
The ANC registration has gone up by 5% in 2010-11 (54589) from 2009-10 (51758) and percentage of 3 ANC check up has increase by 51% in the same year i.e 24976 in 2009-10 to 37818 in 2010-11.
At Mankachar CHC, the number of pregnant women with 3 ANC in 2010-11 was 250 and 179 in 2009-10 and for 2011-12 (upto Oct‘11) it is 153
Only 54% of the targeted pregnant women for 2011-12 (April to Sept) were registered for ANC as the percentage of pregnant women registered for ANC had gone down by 2% in the year 2011-12.

5th Common Review Mission-Assam 2011
20 | P a g e
o In Chapor FRU/CHC; out of 3332 total pregnant women targeted in 2011-12; 2014 pregnant women are registered for ANC in 2011-12. The percentage of increase over 2010-11 is 11.6%.
The number of institutional deliveries has gone up in consecutive year‘s i.e 14143 in 2008-09; 17027 in 2009-10; 18124 in 2010-11 (35%) and percentage of increase over 09-10 is 6.4%. Only District Hospital Dhubri is providing inpatient health care services. Majority of the health care services provide only OPD and inpatient services for MCH only.
o In Dhubri district hospital, the number of institutional deliveries, normal delivery and c-section has increased from 4781 in 2009-10 to 5075 in 2010-11, 3049 (2011-12 upto Oct‘11) for institutional deliveries; 3958 in 2009-10 to 4019 in 2010-11, 2397 (2011-12 upto Oct‘11) for normal delivery and 823 in 2009-10; 1056 in 2010-11 and 652 in 2011-12 (upto Oct‘11)
o At Mankachar CHC, there were 2 deliveries per day per nurse for a center covering 32,546 populations with 30 beds having 2 MBBS doctors and 4 GNM.
The percentage of fully immunized infants is 91% in 2010-11 as compared to 68% in 2009-10 though there are inter-facility variations and for BCG vaccination, it is 107% in 2010-11 as compared to 87% in 2009-10.
o In Folimari sub-center, the percentage of BCG immunization was 30% as per crude assessment for BCG scars among community children during field visit.
The patient load was found to be concentrated at 1 district hospital with very high referral rates from other peripheral facilities.
o Only c-section is performed at district hospital since there is only 1 anesthetist for the whole district.
The bed occupancy rate of the District Hospital is found to be 120% and average length of stay is 8 days
The mother and child are not staying in facilities especially in PHC/CHC level, even for 24 hours mainly due to lack of adequate facilities to stay
The uptake of family planning services is very poor in the district. o The total unmet need is 37 as per DLHS-3 which is higher than for the state (26).
Only 32% of eligible couple used any FP method in Dhubri as against 50% for the state. The percentage of female sterilization is very low (2%) as compared to 10% for the state. Only 23% used any modern method in Dhubri There were only 2 NSV conducted each in 2010-11 and 2011-12 (upto Oct‘11) and only 134 and 35 IUCD insertions for the same year period.
4. Outreach Services
Overall there are 4604 health sub-centers in Assam as in September, 2011 and 31 sub-
centers are conducting at least 3 and more deliveries in a month. 47 % of all sub-centers are located in government owned buildings but many sub-centers
lack water and electricity connections. There was no residential accommodation for ANM, who are mostly residing in another block/district.
All the sub-centers had at least 1 ANM posted; i.e out of 4592 sub-centers in the state as per facility survey conducted in 2010; all 4592 sub-centers have 1 ANM in place.

5th Common Review Mission-Assam 2011
21 | P a g e
Record keeping was found to be reasonably good but there were gaps in follow up and documentation of PNC. There was proper activity plan for ANM. OPD attendance was found to be good in sub-centers where RHP were deployed in health sub-centers
Health services provided by the boat clinic services under PPP scheme of NRHM with C‘NES is effective in geographically isolated riverine areas of the state.
There are total functional 27 MMUs in the state; 1 MMU in each district of which 23 MMU were added in 2010-11; each unit has three vehicles, each unit equipped with x-ray machine, microscope, ECG equipment, Ultrasound machine, stretchers and mobile pharmacy. They do sugar test, hemoglobin test, malaria tests in the van. These units comprise of a Mahindra Scorpio for the staff and two 709 Tata busses with inbuilt OPD, laboratory facility and other essential diagnostic accessories. A generator for power supply is also fitted in each MMU. These specially designed units are complete with two medical officers, two nurses, a lab technician, a radiographer and a pharmacist.
Since the launch of MMU in November 2007 till September 2011; 13,706 camps had been held and 20, 59,640 patients had been treated. Each MMU unit has three vehicles, each unit equipped with x-ray machine, microscope, ECG equipment, Ultrasound machine, stretchers and mobile pharmacy. They do sugar test, hemoglobin test, malaria tests in the van.
VHND – Village Health and Nutrition Days are being held as Health Day. The VHNDs are held regularly at Anganwadi centers by ANM and ASHA‘s, they organize VHND once in a month to provide services like immunization, family planning, ANC, counseling of mothers about nutrition and supplementary feeding. Apart from maternal/ child care and nutrition, they also discuss about hygiene and sanitation and about different schemes like Mamoni, Moram, Majori, Mamta kit, started by the State Government.
Dhubri district Overall there are 246 sub-centers, 1 Mobile Medical Unit (MMU) and 2 boat clinics for
Dhubri Out of 246 sub-centers, 119 sub-centers have 2 ANMs in place. All the sub-center had at
least 1 ANM and 1 MPW in place and 19 of the sub-centers have RHPs deployed where deliveries are conducted in 16 of these centers.
Record keeping was found to be reasonably good but there were gaps in follow up and documentation of PNC. There was proper activity plan for ANM. OPD attendance was found to be good in sub-centers where RHP were deployed.
o At Folimari and Fekamari sub-centers; the number of OPD is 30-40 per day on an average.
o At Folimari sub-center covering 10,400 populations, ANM conducted home deliveries- 202 as in Oct, 2011 and 2 normal deliveries were conducted in last 1 year by RHP. At Fekamari sub-center, 2 deliveries had been conducted since July 2009
o At Fekamari sub-center, 50% of essential drug lists are not available- 18 unavailable out of 37.
Out of 16128 VHND planned during 2010-11; 14498 had been organized and in 2011-12 (upto Sep‘11); out of 16980 VHND planned; 7146 had been organized i.e 42% of VHND had been achieved.
Immunization rate is 30-35% as per random survey for BCG marks among children in Folimari under Folimari sub-center. RHP kit was in demand.

5th Common Review Mission-Assam 2011
22 | P a g e
Boat Unit-I & II covers 32,000 population in char (island villages) of Dhubri- 32 target villages and boat clinics conducts health check up camps to selected islands – 5-7 trips per month – services are – ANC, immunization, malaria, PP, curative care, FP services, basic lab services, IEC etc. The two boat clinics had organized 191 camps in 2011-12 (April-Sep‘11) as compared to 89 in 2010-11 from April-Sep‘10 (114%). The number of patient undergoing health check up in 2011-12 has also increased by 116%i.e 22112 as compared to 10223 in 2010-11. The routine immunization increased by 68% i.e 2205 in 2011-12 as compared to 1305 in 2010-11 though the vitamin A supplementation had decreased by 8% from 208 in 2010-11 to 191 in 2011-12. There was 100% increase in ANC registration in 2011-12 i.e from 315 in 2010-11 to 630 in 2011-12.
The two boat clinics had organized 191 camps in 2011-12 (April-Sep‘11) as compared to 89 in 2010-11 from April-Sep‘10 (114%). The number of patient undergoing health check up in 2011-12 has also increased by 116%i.e 22112 as compared to 10223 in 2010-11. The routine immunization increased by 68% i.e 2205 in 2011-12 as compared to 1305 in 2010-11 though the vitamin A supplementation had decreased by 8% from 208 in 2010-11 to 191 in 2011-12. There was 100% increase in ANC registration in 2011-12 i.e from 315 in 2010-11 to 630 in 2011-12.
o Under Dhubri boat clinic-Unit I, there was nearly 90% of ANC are registered (863 for 2010-11) but institutional delivery is very less. The due lists for ANC is not prepared by ASHA and not shared with ANM/GNM or MO
o 50 TBA in target area- most deliveries conducted by TBA o IMR is 65% - need to analyze data on regular basis o FP service is very low- 1325 (OC/condoms only) o Helminthiasis is one of the most common illness but no focus for de-worming and
no stool tests for R/E was conducted by boat clinics. Microscope though available, was not in used.
Nagaon district MMUs are functional in the Northern part of the District. Under MMU, there has been 72% increase in the number of camps organized (93) in
2010-11 (April to Sep‘11) as compared to 54 in 2010-11 (April to Sep‘10). The number of patient treated in 2011-12 has also increased by 126% i.e. 16202 as compared to 7140 in 2010-11. There was no USG and ECG conducted in 2011-12 and the patients examined for blood test has decreased to 84 in 2011-12 from 214 in 2010-11. However, maintenance needs to be improved.
5. ASHA Program
Across the state, 29172 ASHAs were selected and 91-95% had received training for Modules
1 through 5. Training for modules 6 and 7 is yet to start. The percentage of ASHAs who have completed the 1st, 2nd, 3rd, 4th and 5th training modules were 95.5%, 94.0%, 93.0%, 93.0% and 91.6% respectively.. ASHAs are yet to be trained in the 6th and 7th module.
o All the required ASHA i.e 1725 for Dhubri district were selected and 17 had been dropped out, out of these, 1702 received trainings on 5th module
The attrition rate is low for the state (2%) and some of the reasons for drop outs, which came out through interactions, are as follows:

5th Common Review Mission-Assam 2011
23 | P a g e
o Few of them got selected as ASHA supervisor o They got selected as AWW o Some of them got selected as a member of Panchayat o Very few of them died (rare) The ASHAs seem to have social recognition in society. This seems to be supported by the relatively low attrition rate.
Over 95% of the ASHAs had received their Drug Kits. These kits were replenished regularly. Out of 1725 ASHA, 1702 received drug kits in Dhubri
ASHAs are highly motivated and converse with RCH programme and other responsibilities assigned to them except for new initiatives under disease control programmes. ASHA workers are effective in mobilizing the community for ANC registration and in ensuring institutional deliveries with varying extent across district, immunization of infants and children, family planning and, diagnosis and treatment of fever and malaria, identification of tuberculosis and leprosy, provision of contraceptive advice and services, sterilization, advise on nutrition, etc
There is an ASHA mentoring Group with three master trainers at the state level and a district ASHA nodal officer, supported by district community mobilize and assistant district community mobilize are identified at district level for overseeing the ASHA programme. As in September 2011, 2743 ASHA facilitators were recruited on contractual basis, to provide support to 10 ASHA per 1 ASHA facilitator at block level. Orientation training of ASHA facilitator and ASHA are conducted during monthly meeting. The ASHAs were supported by the health system. Their education included a twice a week radio programme broadcast by the State on All India Radio. They were provided with radios.
All ASHAs have bank accounts and they receive their incentives in the form of cheques/account transfer. The average take home amount per month per ASHA was Rs.1500/- and payment is through e-transfer to the bank account on or before 10th of every month as against the claimed amount after verifications.
The role of ASHA in imparting education, motivation and counseling (EMC), in family planning, is very limited. For example, in Dhubri district the uptake of FP services, in particular IUCD and sterilization is very low.
All ASHAs have bank accounts and they receive their incentives in the form of cheques and account transfer. The payment of incentives is regular for JSY except for RNTCP as DOTs provider, which has one year backlog (Dhubri). Almost 50% of the cheques issued to the mother were not encashed under JSY. Also at some facilities, the bank refused to issue cheque books or refused to open account on zero balance for ASHA and pregnant women.
The monitoring and supervision of ASHA, particularly in island villages is weak and drug kits are not replenished on regular basis.
The overall impression is the ASHAs are competent and proud of their work. Many of them are bright and enthusiastic and have adequate knowledge about processes and procedures. They seem to be doing a good job of their roles as links between the community and the health service.

5th Common Review Mission-Assam 2011
24 | P a g e
6. RCH-II (Maternal Health, Child Health and Family Welfare)
MATERNAL HEALTH
The MMR of the state is 390 (SRS: 2007-09). As per the AHS -2010 (reference period 2007-09), the MMR for the 23 districts of Assam varies between 342 in 4 districts to 430 in 5 districts. Nagaon has MMR of 367 as compared to 366 for Dhubri.
494 health facilities including CHCs, PHCs and Mini PHCs for providing 24x7 services have been upgraded, where atleast 1-2 doctors are posted at each upgraded PHC supported by at least 2 GNMs and adequate number of ANMs. The facilities visited by the teams had 2-3 doctors including one MO (Ayush).
None of the 24x7 facilities visited were geared to provide the other services such as assisted deliveries and management of complicated deliveries before referral to higher centers besides conducting normal deliveries.
24 district hospitals are designated as FRUs and are equipped to provide comprehensive CEmOC. In addition 38 out of 108 CHCs are stated to be operational as FRUs. The team was intimated that most of these have fulfilled the 3 critical criteria of functionality.
The state has a substantial number of male gynecologists some of whom were posted at block PHCs. In Nagaon, there are 5 gynecologists at district hospital, at least 2 at each of the 3 FRUs visited along with some them who are posted at block PHCs. On the other hand in Dhubri there are only 5 gynecologists in the whole district. There is thus a completely irrational distribution of an important resource and the state must undertake an exercise for rational placement of human resources based on needs.
The FRUs and district hospitals are required to cater to maternal emergencies requiring immediate interventions for saving lives of pregnant women with complications. A look at the indications for caesarean section revealed most of them to be elective caesareans. It was not possible to ascertain as the number of emergency obstetric cases which were being catered to by these facilities from the available records. The referral cases were found to be high in many facilities. .
Assam has the highest MMR in the country. Most of the maternal deaths occur due to complications during pregnancy, which if brought to FRUs on time and provided comprehensive emergency care could survive. It seems that most of pregnant women visit the private institutions or they die during the process of referrals or at home. In case the state wants to accelerate decline in MMR these issues need immediate attention at an appropriate technical level.
It is important to have a good system of maternal death audit/reviews in place. The state has initiated the MDR in all districts including the two districts visited by the team though it is still in a very early stage. The available records are not in not in the prescribed formats and there was hardly any follow up at community level. It may thus take considerable time to get conceptualized as to the methodology of doing or real purpose of MDR unless the state government gives more focus to the MDR and maternal death audit.
Routine drugs including Misoprostol and inj. Magnesium Sulphate and items like gloves etc were available in most labour rooms, The practice of keeping emergency drugs in treys ready for use was however not prevalent. Also the utilization of Misoprostol etc for prevention of PPH needs to be properly monitored.

5th Common Review Mission-Assam 2011
25 | P a g e
Phototherapy units and radiant warmer were found at most facilities where deliveries occur. Practices of essential newborn care immediately after birth though followed needs lot of skill up gradation of GNMs and doctors
The blood storage areas in all FRUs have received the necessary approvals of the regulatory authority even though these are functional. In one case in Nagaon, even the building has not yet been handed over.
24x7 health facilities are required to provide RTI/STI services and also MTP using at least MVA method. MTPs using MVA technique were being done at some facilities. Medical methods of termination are not much known. The team could not get any data on approval of private facilities for MTP.
The up gradation of the PHCs has led to significant increase in the number of deliveries at block PHCs and new PHCs. This has also led to a very positive response from the community about the JSY scheme in all districts. Compared to 17523 beneficiaries of the scheme in 2005-06, 391675 beneficiaries availed of the scheme in 2007-08 which is an increase of more than 20 times. The state has issued instructions for keeping PWs in hospitals for 48 hours.
Dhubri District The Team visited the only designated FRU in the district. This facility has adequate
infrastructure with a fully equipped operation theatre and blood storage facility. The hospital also has a gynecologist and pediatrician but lacks anesthetist and is not functioning as an FRU. Not a single caesarean took place in this hospital since 2007.
Facilities for institutional delivery at the South Samara block are in stages of infancy. During FGD, it was informed that ~95% of the deliveries in this area are conducted by Dias at home (few assisted by ANMs from Sub-centre) and only complicated cases were referred to district hospital. The reason cited by the community was the non-availability of ANM at the sub Centre when required although nearly all sub-centers have 2 ANMs attached to each sub-center. ANMs informed that due to their duty roster, both of them have to be in field except for 2 days in a week. Moreover, the area being a difficult terrain, none of the ANMs prefer to stay back due to security reasons.
The district hospital is the only hospital in the entire district providing full range of Comprehensive CEmOC and newborn care. It has 2 gynecologists, 2 pediatrician and 2 anesthetists and a fully functional SNCU with a capacity of 16 admissions (10 for internal patients and 6 for referrals patients). The district hospital is acutely overloaded with patients as it is the only centre in the entire district which provides facilities of Caesarean section, general surgery, emergency management and sick newborn care.
There were backlogs of JSY payments at many centers due to non-availability of cheque books. In addition, bank refusal to open zero balance accounts for the JSY beneficiaries leads to non-encashment of many issued cheques as was seen in one of the facilities where 40/72 cheques issued this year remained pending. Payments related to the Mamoni scheme (State initiative for incentivizing ANC check-up) remained pending since 2010 due to non-availability of required funds. The focus of the health providers on service under JSY is mostly on increasing numbers of institutional deliveries forgetting that the objective of the scheme is to reduce maternal mortality rate. While at some facilities SBA trained GNMs were available the quality issues and provision of basic emergency obstetric care training to doctors posted at these facilities needs immediate attention.

5th Common Review Mission-Assam 2011
26 | P a g e
Nagaon District Of the 6 designated FRUs in Nagaon district, the team visited 3. The buildings have been
renovated using NRHM funds. All were functional to the extent that caesarean sections were being done and newborn services were available. All had at least 2 gynecologists and at least one each of anesthetist and pediatrician. However, only one i.e., the FRU at CHC Jakhalbandha had a fully functional blood storage unit. This FRU was also functioning as a training centre for SBA training of GNMs and ANMs.
The district hospital at Nagaon is fully equipped for providing comprehensive EmONC and newborn care. It has 5 gynecologists, 2 pediatricians and 2 anesthetists. The hospital has a functional SNU for newborn care and also a fully functional blood bank.
The recording of causes of deaths by FRUs and district hospital in Nagaon also leaves much to be desired and terms like ‗anemic failure‘ are in common use. At FRU Hojai this issue was discussed with the gynecologist and the case records were gone into. The deaths of 2 women recorded as anemic failure were reconsidered by the gynecologist himself to ―PPH with hypovolumic shock‖ which is acceptable terminology and important from programme point of view. It would need to be stressed that at least the deaths in the institutions should be is also not as per the most probable maternal causes. In Dhubri district no maternal deaths have been recorded in any of the health facilities visited by the team except at the district hospital indicating gross underreporting of maternal deaths. It is also important that all these
The team was informed that the state has identified eclampsia as the largest contributor to maternal deaths and is taking steps to control these deaths. During the visit to Nagaon this aspect was looked into from the records at FRUs and District hospital and not many instances of abnormal attendance due to this cause were noticed. It would therefore be important that the state sets up a detailed epidemiological investigation with help of ICMR etc to find the exact situation as well as its cause before instituting specific programmes.
Labour rooms at most facilities visited were found to have upgraded physical infrastructure like tiling of floors and walls, running water supply and provision of generator/inverter connections. In some places, however, attached toilet facilities were not provided for. Infection prevention and waste management:
While colored bins were available everywhere the knowledge on use of these was lacking. Similarly different colour coded bags to collect the respective segregated wastes were available in the store but they were not in use. There is need for greater awareness and sensitivity amongst the health officers regarding the need of improving quality of care including even the basics like maintenance of general cleanliness not only in functional areas like labour rooms but also in and around health facilities.
Health care waste management and infection prevention practices and knowledge are extremely poor at all facilities with no segregation of waste, poor storage and disposal of sharps and placenta and body parts.
The systems / mechanisms for final disposal are also not there and need proper planning and orientation of facility staff.
The hub cutters available with the ANMs are being used but they have no idea on what to do after that. There is urgent need for training/orienting the ANMs as also the district staff.

5th Common Review Mission-Assam 2011
27 | P a g e
Equipment and drugs
Drug kits A& B for 2011-12 have not been received. Supplies for last year were received by sub centers in Nagaon during April 2011 and are still in use.
Essential drugs were available in the labour rooms; however antibiotics and other drugs are still being prescribed for delivery cases.
Most of the equipment required in labour rooms and during VHNDs is in place but is underutilized.
CHILD HEALTH
New Born Care
The State is in the process of establishing SNCUs at the district hospitals and Stabilization units at the FRU/CHC levels. The SNCU at Nagaon is now operational and was admitting newborns for treatment, a space for laboratory exists within the SNCU, however this is still to be equipped and made functional. General drugs were available while antibiotics which are essential aspect of a SNCU management were in very short supply. The SNCU at Dhubri district hospital is well equipped and has became functional only a week ago. All drugs supplies were adequately available at the facility.
At the FRU/CHC level we could see building coming up. The procurement of equipment will start after the building is completed. It was emphasized by the team during debriefing that procurement of equipment and training of staff should be taken up concurrently. Dhubri FRU/CHC is lagging behind in establishing the stabilization unit and currently has newborn care corners only.
All health facilities where deliveries take place have newborn care corners with adequate supplies. At a few places where SBA trained GNMs/ANMs are posted, care of healthy child at birth is being practiced. However at most places despite equipped NBCCs, health staff lacks knowledge and skills about essential newborn care. This was also true of even the district hospital which happens to be a training centre for SBAs it.
Initiation of breast feeding within an hour of birth was being practiced everywhere.
Home based newborn care through ASHA does not exist. It is important to mention that in Assam there has been no decline in neonatal mortality rate
since 2005. The early neonatal mortality (deaths in first 7 days after birth) has gone up from 25 in 2005 to 29 in 2009. Data on 96 early neonatal deaths at Nagaon Civil Hospital indicates that 45.8% deaths were due to birth asphyxia and 4 of 96 babies died of hypothermia. Such deaths should never occur at the district hospital where all facilities are available and points to the lack of attention to the problem. This should be cause of serious concern to everyone and was brought to the notice of the NRHM mission director.
Child Health Low osmolality Oral Rehydration Solution (ORS) and Cotrimoxazole tablets and Vitamin A
were available at majority of facilities visited; dispersible zinc tablets were also available at a few facilities.
At FRUs and DH there is irrational use of drugs including multiple antibiotics for management of childhood diarrhoea. This was evidenced from the examination of case

5th Common Review Mission-Assam 2011
28 | P a g e
sheets available at number facilities and discussions held with doctors including pediatricians.
Skills for managing diarrhoea and Pneumonia were uniformly poor in all categories of personnel.
The team was informed that 3 NRCs (Nutrition Rehabilitation Centers) have been established in the state. In Nagaon, however, there were no visible plans for establishing nutrition rehabilitation centers. Nutrition is an important aspect of child health and demands more attention from the state.
Integrated Management of Neonatal & Childhood Illnesses (IMNCI)
Out of total 10110 ANMs, 4139 (40%) ANMs have been trained in IMNCI in the state. IMNCI training for doctors is still to be initiated. 435 doctors have been given TOT. No
comprehensive plan on this training was shared with the team. There was adequate availability of cold chain equipments at the district, block and sub block
level cold chain points, equipments were properly installed as per guidelines with power back up at few places. There are however many blocks, especially in the riverine areas where cold chain points need to be established. The current ad-hoc practice of supplying vaccines to these large geographical areas with more than three lakh population on a day-to-day basis using boats is not sustainable especially during floods. This has directly impacted on the immunization status of children in that region, which is quite evident from the immunization cards available.
Routine immunization microplans with estimation of beneficiaries and logistics was not available at most of the facilities.
Proper Vaccine and logistics management and storing practices were witnessed at all the facilities visited by both the teams. The vaccine stock registers were up-to-date and the vaccine stocks matched on random crosscheck.
There were no standardized formats for maintaining vaccine distribution and stock registers available at facilities. State has universalized Hepatitis B vaccination under the routine immunization programme in all the districts, however birth dose of hepatitis B has not been initiated anywhere in the state. OPV zero dose coverage is poor in spite of increased institutional deliveries
District vaccination coverage data, disaggregated by block, are not very useful as it often goes way above 100 percent, apparently because denominators are provided by the State. A bottom-up approach, based on the household data generated by ASHAs and ANMs would evidently be more useful. Moreover the data collected and compiled at district level clearly indicates a disproportionately exaggerated figures pertaining to immunization wherein 91% of FI has been reported for Dhubri district.
Family Planning
Assam has a low contraceptive use rate (modern methods) of 31% compared to the national average of 47% (DLHS-3). Unmet need for family planning at 24.3% (18.5% for limiting and 5.8% for spacing). This indicates a very high demand for family planning services in the community. Total Fertility rate (TFR) of the state has come down from 2.9 in 2003 to 2.6 in2009 (SRS-2009).

5th Common Review Mission-Assam 2011
29 | P a g e
From the performance data shared with the team, it is observed that over the years there has been a steady increase in sterilizations from 17282 in 2006-2007 to 81229 in 2009-10. However in the subsequent year i.e. 2010-11 this has declined marginally to 80596. The state has not indicated the expected level of achievement (target) for any year in their report. It is, however obvious that for a population size of 3.11 crores and unmet need of 24% this coverage is very low. This also conforms to the DLHS-3 results which indicate sterilizations to contribute only 35% of contraceptive use, the remaining 65% coming from spacing methods. Of the spacing methods the largest contribution comes from oral pills which contribute 16.5 % of the use rate of 31.2 %( 52%).
Male participation in sterilization has been quite good and needs to be highlighted. However this too seems to be declining and has come down to 15.3% in 2010-11 from 17.32% in 2009-10.
A general observation of the team was a very visible lack of interest and leadership on family planning at all levels from the state to the sub centre. This could be due to a very high focus on issues related to maternal health. However it has to be realised that family planning is one of three pillars of RCH II and that for any appreciable decline in maternal mortality family planning plays a vital role.
The team found that the availability of contraceptives is quite good; however the access to services is poor. Since the fixed-day/fixed-place approach is nonexistent, only sterilization camps are relied on for providing services. The frequency of the camps is also quite infrequent. The rationale given by state and district officials is that sterilization services pick up only after the festival season in October. What is perhaps required is provision of services at the facility level on demand. It is here that providing Mini-lap sterilizations through trained medical officer at the CHCs/FRUs on fixed day/fixed place approach may be useful.
Another important issue needing attention of state is that oral pills constituted about 52% to the overall use of spacing methods. However during the visit the team did not see any evidence of this in the health facilities. With a large demand for this method it would be imperative that the state takes not of it.
IUCDs are inserted at the health facilities. However, this is done mostly by the trained ANMs even at facilities where trained doctors are available. State must take steps to ensure more participation of trained doctors at facilities.
Demand Creation: No IEC materials (pamphlets, posters, media, job aides) are available on FP or displayed at any of the facilities or in community
There is a significant increase in institutional delivery under JSY scheme. The stay of women at facilities for 48 hours is also going up. However, there is no effort by state government to promote post partum sterilization or IUCD insertion during post delivery period which is a time when the motivation as well as demand for contraception is maximum.
Summary: Services for family planning – clinical as well as community-based are very limited. This is most likely the result of lack of clarity and support from the state level on the importance of family planning as the third pillar, in addition to maternal health and child health, within RCH II. Advocacy/Policy support- Stronger advocacy and support from the state to the districts on both the central role of FP within RCH II/NRHM and the link between family planning and reductions in infant and maternal mortality. States and district are more focused on achieving reductions in IMR/MMR, often neglecting TFR.

5th Common Review Mission-Assam 2011
30 | P a g e
Routine Immunization Routine Immunization (RI) in Assam is provided as a part of the integrated package of
VHND services. Assam has shown improvement in immunization coverage during the past seven years
however the coverage is still low with only 59% children fully immunized.
Figure 3: Bar chart showing the percentage of fully immunized children as per DLHS data in Assam
As per DLHS 3, the full immunization coverage for Dhubri district is 23.2% while for Nagaon district it is 36.5%.
7. Preventive & Promotive health services- Nutrition & Inter-sectoral Convergence
Nutrition: o State initiatives: There are many state initiatives described below. o NGO support: There is evidence of some NGO involvement in school health. o Vitamin A: Vitamin A is regularly being dispensed by ANMs at sub-centres. o Iron folic acid: IFA is regularly being dispensed by ANMs at sub-centres and by
ASHAs. Some ASHAs follow up patients to encourage compliance. o Iodine deficiency: Regular survey for goitre and salt testing is being done in all
districts. There is a correlation between districts, which report low salt content and proportion of people in a district with goitre. The proportion of people with goitre has reduced over time.
o Nutrition rehabilitation: Three Nutrition Rehabilitation Centers have been established at Kharupetia, Udalguri and Gosalgaon in the current year. One more center is being planned at Chirang for this year. A total of 74 patients were admitted and 53 discharged and 30 followed up.
Linkage with ICDS: There are links between VHN Days and ICDS with supplementation of Vitamin A and IFA supplementation. There is also linkage between Sarva Shiksha Abhiyan

5th Common Review Mission-Assam 2011
31 | P a g e
and school eye check-ups. Teachers in all schools in Nagaon have been trained to identify children with refractive errors. All children are screened annually and 1690 were referred for confirmation of diagnosis. Spectacles were provided under Sarva Shiksha Abhiyan.
VHNSC and social determinants of health: Most of the VHNSC decisions and procurement is related to equipment and improvement of curative facilities at the village level. There was no evidence that the social determinants of health were being addressed. There needs to be greater coordination between the NRHM and other government departments like ICDS, MGNREGA, SSA, Total Sanitation Campaign, Social Welfare, Youth Welfare etc
AIDS: The ASHAs are aware of issues related to HIV/AIDS. However, their attempts at educating young people seem to be limited. Nevertheless, HIV/AIDS is being discussed as part of health education in high schools.
Water and Sanitation: The Nagaon district has started IEC/BCC activities related to nutrition, hygiene, water and sanitation for schools with an emphasis on institutions serving minorities. They plan a booklet and a Quiz Competition for high school students. They also plan to train one teacher per high school to be a resource person.
Yoga programme: The district has started collaboration with an NGO, VVKI North East Apex Body, a wing of The Art of Living, to teach yoga to high school students. A total of 18167 students, from 25 schools in Nagaon district, have benefited from Yoga classes. The second phase of the program plans to extend this training to 12089 students in another 25 schools. Yoga classes have also been taken for prisoners in the local prisons.
8. Gender Issues & PCPNDT
The sex ratio in Assam is 954 females per 1000 males as per Census 2011 and it has
increased over the last decade. 15.24 % of the rural population and 9.79% children of urban population are in 0-6 years age group. The male literacy rate is 78.81 % and female literacy rate is 67.27% as per provisional Census data, 2011. In 2001, literacy rate in Assam stood at 63.25 percent of which male and female were 75.23 percent and 51.85 percent literate respectively.
With an overall objective to reduce the IMR, MMR and improve on TFR, the state has come up with good female centric innovative schemes such as Majoni, Mamoni and Mamta. These female centric schemes aim to improve the sex ratio in Assam, targeting the newborn girl by safeguarding education, health and nutritional rights through Majoni scheme, providing nutritional food to pregnant women through Mamoni scheme and improving post natal care, counseling on breastfeeding, full immunization during 48 hours stay in institutions and mamta kit to newborn baby through Mamta scheme.
At many CHCs and PHCs, separate ward and separate toilets for female were not found. As per the provisions made in PC & PNDT Act and directions of Hon‘ble Supreme Court of India, the PC & PNDT Act has been fully implemented since 2004 throughout the State (in all districts).The District and Sub-District level Advisory Committee in all District (except in the District of Baksa, Chirang, Udalguri) have been constituted and are functioning normally as per PC & PNDT Act. For the District of Kamrup (Metro & Rural) there is only one District Advisory Committee. Meeting of the District level committee are being held and Quarterly reports are also being sent to Central Government regularly.
District Appropriate Authorities are functioning as per the Act. 7 Ultrasound Machines have been seized by the District authority at Kamrup and 5 in
Barpeta District during 2011

5th Common Review Mission-Assam 2011
32 | P a g e
DHS (FW) has proposed constitution and functioning of State inspection and monitoring Committee in the state.
At district level, the PC&PNDT advisory committee has been constituted and regular meetings are being held at District level under the Chairmanship of Superintendent of the Hospital
o In Dhubri, District Advisory Committee and District Appropriate Authority has been functioning in the district. They have submitted quarterly reports regularly. At present there are 8 USG Centres (Govt. and Private both) functioning in the district. The District Appropriate Authority supervises the functions of all centers regularly. Lastly the District PNDT Cell has been constituted. There is no case of seizure has been reported in the District, thus no subsequent prosecution in the court.
o In Nagaon, District PNDT Committee was constituted but the committee is not functioning properly. The submission of quarterly reports from Nagaon District is irregular since 2007. District level PNDT Cell of the district has not formed. There are 20 USG Centres in the District (including Govt. and Private). No case of prosecution being reported from Nagaon District till now.
o Functional Ultra-sound facility are available only at District Hospital
9. National Disease Control Programmes NVBDCP:
Malaria is one of the major public health problems of Assam. Out of 31.53 million population in the State approximately 10 million (31%) people are living in malaria high risk areas. All the districts are reporting malaria incidence with variable intensity. However declining trend is noticed since 2008 onwards due to Intensified Malaria Control Programme, supported by the Global Fund.
There has been a significant improvement in the implementation of NVBDCP strategy as a result of which the surveillance has considerably improved from 8.09% in 2007 to around 14% in 2011.The malaria incidence in the state has been appreciably reduced by 58% mainly due to the State as well as Central interventions and a firm state political will. The number of deaths has also been reduced from 152 in 2007 to 30 (80%) during 2011.
Table 12- Year wise Malaria statistics of the state of Assam
Year Population BSC/ BSE(total tested
No of +ve
Pf Pf% ABER SPR (TPR)
SFR API PF Death
2007 29654047 2399836 94853 65542 69.09 8.09 3.95 2.73 3.19 152
2008 30569060 2687755 83939 76350 69.3 8.62 3.18 2.28 2.74 86
2009 31274214 3021915 91413 66557 72.80 9.66 3.02 2.20 2.92 63 2010 31530334 4309287 68353 48330 70.71 13.67 1.58 1.12 2.17 36 2011( Sep) 31169272 3314867 39509 28856 73.03 - 1.19 0.87 - 30

5th Common Review Mission-Assam 2011
33 | P a g e
Figure 4: Bar chart showing the number of P.f cases and death in the year from 2006 to 2010 in Assam
NO. OF P.f. CASES AND DEATH
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
0
50
100
150
200
250
300
350
No. of P.fDeath
No. of P.f 82546 65542 76350 66567 49007
Death 304 152 86 63 36
2006 2007 2008 2009 2010
SURVEILLANCE AND COMMUNITY LOAD OF MALARIA
0
2
4
6
8
10
12
14
ABERSPR
ABER 9.35 8.09 8.62 9.66 13.33
SPR 4.59 3.95 3.18 3.02 1.68
2006 2007 2008 2009 2010

5th Common Review Mission-Assam 2011
34 | P a g e
Figure 5 Bar chart showing the surveillance and community load of Malaria in 2006 to 2010 in Assam
Figure 6: Line showing the month-wise malaria cases in the year 2009, 2010 and 2011 upto September in Assam.
While making a detailed analysis of the district data on malaria incidence for the years (2010&2011), it is heartening to note that out of 27 malaria endemic districts only two districts Lakhimpur and Dibrugarh have shown marginal increase in malaria cases during 2011 as compared to 2010.
Role of ASHAs in malaria surveillance has been undoubtedly proved in the state of Assam as is evident from the above table. During 2011 uptil 30 Sept.235541 (7.1%) fever cases have been screened contributing to 10% of case detection and treatment, a remarkable performance which is evident from the table shown below:

5th Common Review Mission-Assam 2011
35 | P a g e
Table 13: Performance of ASHAs 2010 & 2011
Year No. of ASHA trained on malaria (Total ASHA)
Total fever cases screened in the state
% of fever cases screened by ASHA
No. of RDK performed in the state
% of RDK performed by ASHA
No. of RDK +ve cases in the state
% of RDK +ve case detected & treated by ASHA
2009 22150 3021915 5.76 (174062)
503848 24.9 (125458)
18620 29.6
2010 22150 (28378)
4309287 5.7 (245629)
517104 13.09 (67688)
14923 18.13
2011 (January to Sep)
22150 (28378)
3314867 7.1 (235541)
442302 13.7 (60540)
10863 10.00
Integrated Vector Management:
Use of bed nets is an important vector control intervention in the state as the reported Insecticidal Spray operation with DDT has been observed to be poor. The community in Assam is habitual of sleeping under bed nets hence the use of bed nets has been overwhelming in the seven high malaria endemic districts of Assam.
Insecticidal Spray Operations:
Insecticidal operation is one of the main components of malaria strategy in the state of Assam. As per the national policy DDT continues to be in use in the state. Since the residual efficacy of this insecticide lasts for 10 weeks, two well covered rounds are good enough for effective control of malaria; however it has been observed that the room coverage of DDT is reported to be around 60% which is considered to be poor for a good malaria control. The reasons for poor coverage include pungent smell, lack of advance intimation to the community about spray day in their villages, lack of micro-planning at BHPCs and inadequate monitoring and supervision.
Table 14: Insecticidal Residual Spray (DDT Spray) YEAR 2010 Pop
Targeted House hold Room
Targeted Covered (%)
Targeted Covered (%)
First round 6660606 2187957 70 5003993 68
Second round 7719075 2181882 75 5024336 63
YEAR 2011
First round 5507048 1300127 75 2923794 67
Second round 5507048 1399718 79.5 3585922 73.86

5th Common Review Mission-Assam 2011
36 | P a g e
From the above table it is observed that there is hardly any improvement in the percentage of room coverage which is an important parameter to understand proper and effective spray operations as the room coverage ranges from 63 to 74% reported in the second rounds of 2010 and 2011 respectively
Prevalence of other Vector Borne Diseases.
Acute Encephalitis Syndrome (AES)/Japanese Encephalitis (JE)
AES/JE occupies an important role amongst the prevalent vector borne diseases as there has been a significant increase in the no. of AES/JE cases in the state. During 2011, 1418 and 259 AES cases & deaths were reported as against 495 &117 deaths during 2010. Similarly 511 lab. Confirmed JE cases & 114 deaths were reported during 2011 as compared to155 JE cases& 41 deaths reported during 2010.11JE endemic districts have been covered under JE vaccination so far. As the proportion of JE is more than 70% amongst adults, adult vaccination campaign has been launched on pilot basis in district Sivsagar during 2011.
Dengue/DHF
Dengue/DHF was for the first time reported from Guwahati during 2010 as 237 laboratory confirmed cases of Dengue with 2 deaths were reported from Guwahati. During 2011 no laboratory confirmed case of Dengue has been reported till October 2011
Kala-azar
Sporadic cases of Kala-azar are reported by the state. During 2010-12, Kala-azar ??cases were reported as against 7 during 2011. No death due to Kala-azar has been reported from the state so far.
Malaria situation in district Naogaon
Nagaon is one of the malaria-affected districts of Assam. Every year sporadic cases of malaria reported immediately following the flush shower of the pre monsoon period. Malaria is mostly affected in the border areas of Karbi Anglong District located in the foothill area with favorable condition for Mosquito breeding. These areas are also not easily accessible.
Moreover illiteracy, poor accessibility, poor socio- economic condition, migratory mode of living, poor health care facility, reluctance to accept medical treatment by the people of these areas have complicated the issue further .
Nagaon district
Malaria surveillance has shown significant improvement as ABER of 15.12%?? has been reported during 2011 as compared to 13.05% during 2010.Similarly reduction of 57% in total malaria cases has been reported. Proportion of Plasmodium falciparum infection has been reduced to 56.7%.Only 2 deaths have been reported due to malaria during 2011 as compared to 5 deaths reported during 2008. It is noted from the data of the district that none of the PHCs is reporting increased incidence of malaria during 2011 as compared to 2010.
DDT spray both rounds have been completed in the district with 78 & 79% room coverage in 1st and 2nd round. 28 AES and 9 Lab. confirmed cases were reported in the district during 2011.9 &
5th Common Review Mission-Assam 2011
37 | P a g e
2 deaths due to AES/JE respectively were also reported. The district has been covered with JE vaccination in campaign mode with an overall percentage of 92.6% and JE vaccination has been integrated into UIP. Dengue and Kala-azar are not reported from Nagaon.
In addition to these, the team made general and specific observations as follows:
General Observations
Overall improvement in programme implementation Malaria incidence brought down from 6888 cases and 7 deaths during 2007 to 1395 cases
and 1 death in 2010 (Reduction of 20.25%) Only 764 cases and 1 death reported till 31 october,11 from 11 BPHCs API reduced from 1.2 (2008) to 0.3 as reported during 2011 ABER has gone up from 11.2% (2008) to 13.19% during October 2011(Improved
surveillance) Proportion of Pf reduced from 1810 to 585,reduction of 32% 27.1% reduction in total positive cases during 2011 as compared to 2008. Surveillance poor
in Buragohaithan and Jugijan PHCs with ABER varying from 6.5 to 7.5% Drugs and RD kits available at all health facilities, however Primaquine (PQ) 2.5 ??and 7.5??
in short supply in most of the facilities visited. Surveillance work to be stepped up under supportive supervision in the above PHCs. No BPHC could show IRS schedule. This needs immediate correction Indiscriminate use of RDKs at all BPHCs. Stains stored in tea glasses. Staining jars with proper lids to be provided at all places. No display of revised treatment guidelines in FRUs/BPHCs JE vaccine not effectively
integrated into RI as there is no proper orientation of the staff. Some vaccine batches likely to expire on 24-11-11
Specific Observations:
Kuwaritol MPHC under Samonabasti needs immediate improvement in terms of provision of a binocular microscope as the monocular microscope in use is defective. No cases have been reported in this MPHC for last two yrs. This needs to be verified. Technician needs orientation on malaria microscopy.
Sagmootea tea estate to be immediately supplied anti-malarials as no drugs are available except 14 tablets of PQ 7.5. Orientation training on the use of RD kit to be immediately organized.
Record maintenance to be improved as old formats (Mf7) still in use in Jhakhlabandha BPHC.
Two physicians of Dist. hospital trained on case management of complicated cases. Further training has not percolated down.
Dedicated laboratory technicians working in district hospital laboratory, however laboratory needs immediate renovation and provision of minor items like staining jars and enamelled trays for processing of blood smear.
RNTCP
The performance of the State is varied. RNTCP case detections rate follows a seasonal trend in the State which can be emphasized with the table below;

5th Common Review Mission-Assam 2011
38 | P a g e
RNTCP Quarter wise monitoring format- 2011.
Table 15: Table showing the key indicators of RNTCP across the 1st, 2nd and 3rd quarter of 2011 in Assam
Indicators 1Q’11 2Q’11 3Q’11 TB suspect examination rate/lac/quarter : (National Guidelines:180/lakhs/year)
114 129 127
New Smear Positive Case Detection rate : (National Guidelines: at least 70%)
61% 77% 76%
Total Case Detection Rate 111 139 134 Treatment Success rate (NSP): (National Guidelines: 85%)
85% 83% 83%
Treatment success Rate (Re treatment case): (National Guidelines: 85%)
63% 70% 64%
Default rate in NSP : (National Guidelines: less than 5%)
8.7% 9.8% 11%
Default Rate in Re treatment cases (National Guidelines: less than 5%)
23% 16% 25%
Low referral of TB suspects for sputum examination from the PHIs which is the main reason for low cases detection in the district.
Non involvement of regular staffs in default retrieval activities and most of the retrieval activities have to be done by RNTCP contractual staffs. Dhubri district
Monitoring and supervision of the programme under Gazarikandi TB Unit has been dismal by supervisory staff at all levels.
Case detection has consistently been low in this TB unit of the district. It has been particularly been low in South Salmara and Sukchar DMC which is mainly due to a low chest symptomatic referral from the periphery.
Chest symptomatic patient (>2 weeks cough) referral from PHC/CHC to the Designated Microscopy Centre (DMC) for sputum examination has also been very low under South Salmara and Sukchar DMCs.
RNTCP is not being reviewed properly during monthly meetings in the health institutions.
Nagaon district A high default rate (9%) among Smear Positive patients which is the main reason for a low
success rate in Nagaon district. Drugs available in institution however, supervision and monitoring is very poor. Further,
ensuring the consumption of drugs under observation could not ascertain. ASHA incentive as DOTS provider pending at institutions affecting overall implementation of
programme.
NPCB: The major component of the programme i.e. School Screening Programme is not being
implemented adequately in the peripheral institutions. No records for number of spectacles distributed is available 6 out of 7 Ophthalmologists are deployed in the civil hospital.
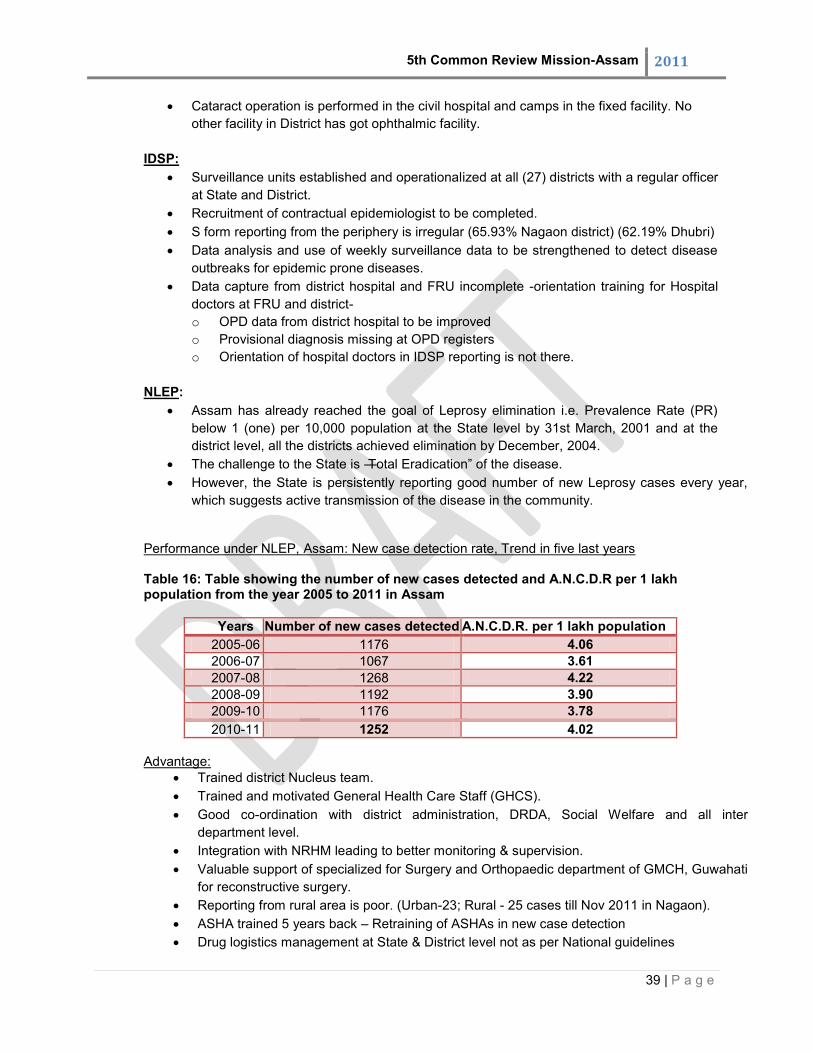
5th Common Review Mission-Assam 2011
39 | P a g e
Cataract operation is performed in the civil hospital and camps in the fixed facility. No other facility in District has got ophthalmic facility.
IDSP:
Surveillance units established and operationalized at all (27) districts with a regular officer at State and District.
Recruitment of contractual epidemiologist to be completed. S form reporting from the periphery is irregular (65.93% Nagaon district) (62.19% Dhubri) Data analysis and use of weekly surveillance data to be strengthened to detect disease
outbreaks for epidemic prone diseases. Data capture from district hospital and FRU incomplete -orientation training for Hospital
doctors at FRU and district- o OPD data from district hospital to be improved o Provisional diagnosis missing at OPD registers o Orientation of hospital doctors in IDSP reporting is not there.
NLEP:
Assam has already reached the goal of Leprosy elimination i.e. Prevalence Rate (PR) below 1 (one) per 10,000 population at the State level by 31st March, 2001 and at the district level, all the districts achieved elimination by December, 2004.
The challenge to the State is ―Total Eradication‖ of the disease. However, the State is persistently reporting good number of new Leprosy cases every year,
which suggests active transmission of the disease in the community.
Performance under NLEP, Assam: New case detection rate, Trend in five last years Table 16: Table showing the number of new cases detected and A.N.C.D.R per 1 lakh population from the year 2005 to 2011 in Assam
Years Number of new cases detected A.N.C.D.R. per 1 lakh population 2005-06 1176 4.06 2006-07 1067 3.61 2007-08 1268 4.22 2008-09 1192 3.90 2009-10 1176 3.78 2010-11 1252 4.02
Advantage:
Trained district Nucleus team. Trained and motivated General Health Care Staff (GHCS). Good co-ordination with district administration, DRDA, Social Welfare and all inter
department level. Integration with NRHM leading to better monitoring & supervision. Valuable support of specialized for Surgery and Orthopaedic department of GMCH, Guwahati
for reconstructive surgery. Reporting from rural area is poor. (Urban-23; Rural - 25 cases till Nov 2011 in Nagaon). ASHA trained 5 years back – Retraining of ASHAs in new case detection Drug logistics management at State & District level not as per National guidelines

5th Common Review Mission-Assam 2011
40 | P a g e
Constraint:
Low Female Coverage as Stigma still persist Low priority to NLEP at all levels
NBCP:
The major component of the programme i.e. School Screening Programme is being implemented adequately in the peripheral institutions.
No record for number of spectacles distributed is available. There is confusion regarding distribution of spectacles amongst school children in between Sarva Shikhsha Abhiyan and NBCP
Cataract operation is performed in the civil hospital and camps in the fixed facility. No other facility in District has got ophthalmic facility.
NIDDCP: Strength:-The strength of the National Iodine Deficiency Disorder Control Programme is that the intervention of the Iodine Deficiency Disorder is the blanket approach through, Iodized Salt, Therefore people are consuming ―Iodine‖ may be without knowing also to protect them from Iodine Deficiency Disorder. Weakness:- There are vacancy in the state level for positions such as statistician assistant, laboratory technician and attendant. Smooth fund flow is difficult as the fund release through treasury route. The monitoring is weak and it needs to be strengthened at district level.
10. Programme Management
Strong Commitment & good leadership was seen at the State level. At the state level, 111 contractual staffs in position such as Programme Managers,
consultants and other support staffs were recruited in SPMU. In DPMU, 260 contractual staffs were recruited while 1028 staffs were recruited in BPMU. Total, 1399 contractual employees were added under NRHM.
Programme Management structures at District & Block level adequate. At places the programme management unit workers are more than needed and at places
a single person is handling work out of his/her purview, for eg. Assistant Block Accounts Officer at an MPHC with 17 deliveries PM while budget for JSY handled at the main PHC whereas at one place one accounts manager is looking after accounts of entire PHCs in the area.
At the organizational level, coordination of SPMU, NRHM with directorate of Health & Family Welfare, Guwahati was uncertain.
There is acute need to look into the training of Data entry operators at block level for HMIS and MCTS.
It appears that supervision and monitoring by the PMU is weak especially in the backward, hard to reach and the riverine areas.
The Monitoring and supervision unit may also supervise the NDCPs. PMUs are placed in the Districts and Blocks. In South Salmara Block one Accounts
manager is looking after accounts of entire PHCs in the area.
5th Common Review Mission-Assam 2011
41 | P a g e
It appears that supervision and monitoring by the PMU is weak especially in South Salmara and in the riverine areas.
11. Procurement System
Centralized procurement at state level on the basis of L1 bidders Basis of need assessment for equipment etc needs improvement. Computerization of
PROMIS of logistics is only at central level. ProMIS is not installed at the regional and district drug warehouses though the training on procurement management information system for four districts is already complete in 2010-11.
No decentralization to the district and below. Some emergency drugs are procured by health facilities out of RKS fund but generally patients are asked to purchase from outside
12. Effective use of Information Technology
A web based HRD portal was developed under the Department of Health & Family Welfare, Government of Assam for optimum utilization and management of manpower resources, which is in public domain. All manpower under the Department of Health & Family Welfare, both contractual engagements under NRHM as well as regular appointment under Department of Health & Family Welfare has been captured under the system.
The HRD software developed is used for recruitment of doctors, RHP etc with an objective for ensuring transparency in recruitment process. The lists of vacancy along with merit list of candidates are published in the website and on the day of counseling, candidates are called based on merit list. During the counseling session, candidate can select their place of posting from the available list. The place of posting is displayed on the screen in the waiting hall so that candidates can see the place of posting already allotted and available for selection. As soon as the candidate selects the place of posting the same is entered in the system, the system automatically generates the appointment letter and letter of acceptance and the appointment letter is distributed on spot. The system has generated confidence among candidates through this transparent recruitment process.
Database related to transfer and posting is updated in the online portal every month and the updating is completed by27th of every month and the updated database is published in the public domain of NRHM on 29th day of every month.
An electronic complaint Redressal system has been started as an added service to 104 Health Information Help Line. Any authorized User of NRHM Directorate segregates the data and sets parameters based on the nature of the complaint and priority and then the complaint is forwarded to the concerned District/ Directorate for action.
A web GIS based planning and facility management system has been developed in which GPS data of all health facilities such as DH, SDCH, CHC, PHC and SC were collected during facility survey and plotted in GIS map. The infrastructure data, equipments, services and manpower data of the health facility collected during the facility survey is mapped with the system. Photographs of the health facility related to equipment, manpower, hospital building are also mapped with the system. One can view

5th Common Review Mission-Assam 2011
42 | P a g e
the detail information of health facility along with the photographs by clicking on the Health Institution in the map.
The HMIS web portal has been uploaded data since 2008 and facility level data uploading has started in 22 districts and remaining 5 is planned to be covered in next 2 months.
MCTS system is in a very early stage. Out of 4604 sub-centers, which are data entry points; 2125 sub-centers are reporting on MCTS portal. The rest of the health facilities have not started reporting on MCTC.
In MCTC; there was no clear cut evidence of name-based tracking of pregnant women and children. Overall MCTS is yet to be fully implemented and made functional in whole of the state.
Overall the data entry in the registers, completeness of reports and accuracy of data entered was found to be poor in the facilities visited. The main problem seems to be due to lack of proper supervision and lack of understanding about the use of data for programme management and decision making. Though the entries were made in the respective forms and registers, but there were lot of discrepancies e.g. in many of the facilities the number of 3rd dose of immunization was more than 1st dose of immunization. There were mismatch in figures and reporting that were there at the block level and facilities below.
Computer with printer and UPS has been provided to all DH, SDCH, CHC and BPHC and computer set is also provided to PHCs wherever electric connection is available and these equipments have been utilized for data entry in Tally ERP 9, HMIS and MCTS. Internet connectivity is available in all District HQ. Internet connectivity has been established in Block PHCs wherever Internet facility is available.
Overall reporting, feedback system and supervision need to be more streamlined and improved.
13. Financial Management
Followings are the observations seen during the CRM 5th visit in Assam State.
Director of Finance recently appointed on October, 2011. One State Finance Manager, Five State Accounts Manager were recruited at state level and on District level one District Accounts Manager and one District Assistant Accounts Manager were recruited.
Electronic transfer is going smoothly in the state. It was observed that tally is installed properly but not maintained by finance personnel on
regular basis, due to lack of response by Tally Solutions in some places. In most of the places Tally ERP 9 was implemented and updated regularly.
The activity plans was in place; so, funds were utilized accordingly as per plan. For Concurrent Audit and Statutory Audit time schedule is not being adhered as
prescribed in the guidelines of the same. Concurrent Audit is not being done in all the districts.
The Delegation of Financial & Administrative powers down the level is as per GoI guidelines. But, as per statement of State Finance Manager, for NDCPs, except IDD (Iodine Deficiency) all things are merged in State Health Society but still IDD Fund is transferred by the Central level to State Government of Assam.
Training has been provided to the financial personnel.

5th Common Review Mission-Assam 2011
43 | P a g e
Regular updation of HMIS was not done because there were some difference between the formats of FMR.
The financial records such as vouchers which are not kept in proper manner, they are kept in loose bunches. The supporting bills are incomplete. The MIS, SoEs are submitted sometimes in time and sometimes delayed. They did not maintain the records in an organized way. We observed that till now vouchers are not prepared and if prepared, they are incomplete. Authentication of voucher is also important.
The model accounting hand books are not yet received by some District/Sub-District because of lack of supply.
Procurement Manuals have been framed. Procurement is being made as per procurement guidelines.
The activities carried out from State Contribution is commensurate with NRHM activities. The tracking of advances is not proper. The State shows expenditure into its books of accounts and the District shows as an
advance into its books of accounts for monitoring and tracking. Diversions of funds are done temporarily but after the approval of concerned authority at
District and State Level. All Rogi Kalyan Samiti (RKS) are not registered under Societies Act 1860. The payment of Audit fees and Audit expenses incurred against interest earned on
NRHM Funds. The Income Tax related to regular deduction and timely deposit of tax sometimes in time
and sometimes within time.
Apart from these issues, some of the general observations made are as follows:
General Observations
NRHM Finance personnel need more orientation on financial procedure, working and reporting.
The bills are not in systematic order. They seem to be much unorganized. Necessary details are not recorded on the bills. Recording of supporting bills in proper way is the major part in financial procedure. Authenticity of bills is only shown if they are complete and recorded systematically.
The vouchers are not found with the supporting bills. We observed that till now vouchers are not prepared and if prepared, they are incomplete. Authentication of voucher is also important.
The formats they are used not according to the financial guidelines. Such as, Bank Reconciliation Statements, Fixed Asset Register, Advance Tracking Register, Advance ageing report, etc.
There was no Identification Marks on Fixed Asset somewhere. Fixed Asset Identification Mark must be on the Fixed Assets.
Cheque scarcity is there but if they try to coordinate with the banks, they will provide the cheques bundles. The cheques were printed by the finance personnel by the help of computer. This step may help to decrease manpower and promote efficient working.
14. Decentralized local health action

5th Common Review Mission-Assam 2011
44 | P a g e
.District level: The state receives District Health Action Plans from all districts. There was a District Health
Action Plan at Nagaon District headquarters. However, such plans should have a specific understanding of the issues and should be incisive and targeted rather than offer general improvements in all aspects of previous performance and functioning. Block level:
There was no evidence of Block Level Health Action plans. There did not seem to be any evidence of community participation in decision making or of the use of HMIS data to set new direction or to fine tune service delivery. VHSNCs:
Data was obtained from national data and from interviewing 32 ASHAs at Khandulimari Sub Centre, Dakshin Radhanagar Sub Center, Udmari Mini-PHC, Doboka CHC, Khairimari Riverine PHC, Jugijan PHC, Dhing Block PHC, Kuwaritol PHC, Hojai FRU, Jakhalabandha BPHC and FRU and a Focus Group Discussion at Khathiatoli PHC in Nagaon District and by checking records of VHN Days. Number formed: 26816 VHSNCs have been constituted. Funds: 26312 VHSNCs have operational joint accounts. Utilization: The numbers of VHND being held have shown a steady and significant
increase over the past 5 years. The funds seem to have been received regularly and have been utilized.
Panchayat linkages VHSNCs: These committees have been constituted with Panchayat members as the chair and other members of the community including teachers, etc. The funds are being regularly released and utilised. Most of ASHAs denied problems in sanctioning and procurement. Rogi Kalyan Samities: The Hojai FRU, Dhing Block PHC, Doboka CHC, Simonabasti PHC, Kuwaritol PHC, Jakalabandhu FRU and the Jugijan PHC‘s records showed a utilization of 99%, 95%, 90%, 93%, 43%, 100% and 91% of RKS funds for the year respectively. The RKS meetings were held and record of the minutes maintained. The RKS meetings at Hojai FRU were not held this year as the new committee‘s chairman is a State minister and is presumably too busy and preoccupied with more ―important‖ matters. However, this has not resulted in any delay in decision making and procurement as 99% of the funds were utilised. The Udmari Mini-PHC had not received RKS funds for the year 2010-11 and had not spent any money for 2011-12. The RKS meetings were regularly held at Udmari Mini-PHC. There were no records of RKS meetings at Kuwaritol PHC.
No money was utilised from the RKS Fund for the past 2 and half years at the Civil Hospital, Nagaon (Balance of Rs. 10, 00,100.00). The explanation given was that the expenditure for different needs was met from the User Fee Collection Fund, which has a substantial balance (Rs 32, 60,019.70). An average expenditure of over Rs 40 lakhs per year was there in the past 3 years suggesting good utilization.
District Health Societies: The Nagaon District Health Society has many activities and these are briefly mentioned: The society attempts to coordinate with the departments of Education, Social Justice,
Panchayati Raj, etc in order to provide a coordinated approach for empowerment of

5th Common Review Mission-Assam 2011
45 | P a g e
people. Meetings with Panchayati Raj Institutions were held for community sensitization, increase involvement and ownership.
The Society has provided small grants for eight NGOs to develop street theatre, plays, exhibitions etc with the aim of spreading messages related to health. Four hundred and twenty five plays were held over two years. The subjects included Anemia, Japanese Encephalitis, Malaria, antenatal care, institutional delivery, JSY, and Family Planning.
IEC/BCC activities related to nutrition, hygiene, water and sanitation for high schools is planned in collaboration with Sarva Shiksha Abhiyan. They plan more classes, a booklet and a Quiz Competition for high school children. They also plan to train one teacher per high school to be a resource person.
The Society has increased its emphasis on school programmes related to minority community as they form a significant proportion of the population. They have identified over 150 Madrasas run by religious institutions and have obtained permission for health, nutrition, hygiene, water, sanitation and education in 89 such institutions. They plan classes, a booklet and a Quiz Competition for high school children. They also plan to train one teacher per high school to be a resource person.
In collaboration with an NGO, they have started teaching Yoga to high school children (detailed above). The teaching of Yoga to prisoners in jails is currently being done in Nagaon.
In collaboration with PR department, they have educated members of different Panchayati Raj Institutions (Panchayat members, Zilla Parishad members) about Japanese Encephalitis and its prevention, vaccination, treatment, etc.
NRHM in collaboration with Tata Tea Sagmootea Tea Estate runs a primary health care centre. Provide OPD services, Inpatient care, antenatal care, institutional deliveries for 4160 workers and dependents living on the tea estate.
Community monitoring: There is no community monitoring at present but the Mission Director, who recently took
charge of the NRHM, has plans to start such endeavours across the State.
Convergence of stake holders: Interviewing members of the community showed that people had good awareness of the
NRHM and activities envisaged. They also demanded improved PHC and sub-centre facilities in their area. NRHM platforms allow for convergence with the Education department, Public Health Engineering and Panchayati Raj Institutions. There was evidence of cooperation and some collaboration between different stakeholders.
DLVMC: Such committees have not yet been notified. The Mission Director has plans to start such
endeavors across the State.
15. Mainstreaming of AYUSH
AYUSH doctors have been deployed in the rural and remote area and are providing health services and some of them even conduct deliveries also. However, they are not practising their own system of medicine and AYUSH drugs are not adequately available
None of the facilities reported availability AYUSH Pharmacists. There was no AYUSH Inpatient care reported even in District Hospitals.

5th Common Review Mission-Assam 2011
46 | P a g e
No specific IEC programme conducted on mainstreaming and strengths of AYUSH systems.
The technical monitoring of AYUSH doctors service delivery is practically not exist.
16. Overall Outcome
The state‗s main and unique innovations are in ensuring availability of skilled
professionals in rural and remote areas. It has made good efforts to retain the human resources in the peripheral areas. It has adopted a web-based MIS method for deployment of human resources across facilities in the state as per the vacancy positions.
The state could reach out to the unreached and marginalized population in riverine areas through boat clinics for providing universal primary health care services, which is commendable and has the potential to scale up and expand the coverage for better impact on health of char population.
The state has come up with good female focused innovative schemes such as Majoni, Mamoni and Mamta with an aim to improve the situation of sex ratio in Assam, targeting the newborn girl to safeguard education, health and nutritional rights through Majoni scheme and provision of nutritional food to pregnant women through Mamoni scheme and provision of post natal care, counseling on breastfeeding, full immunization during 48 hours stay in institutions and Mamta kit to newborn baby through Mamta scheme.
There has been a significant improvement in the implementation of NVBDCP strategy as a result of which the surveillance has considerably improved from 8.09% reported in 2007 to around 14% in 2011.The malaria incidence in the state has been appreciably reduced by 58% mainly due to the state as well as Central interventions and a firm state political will. The number of deaths has also been reduced from 152 reported in 2007 to 30 (80%) during 2011.
Role of ASHAs in malaria surveillance has been undoubtedly remarkable in the state of Assam. During 2011 till date 30 Sept. 235541 (7.1%) fever cases have been screened contributing to 10% of case detection and treatment which is a remarkable performance.
The state has to work seriously with respect to population stabilization. It has one of the highest IMR and MMR in the country and though the decline trend over the last five years is remarkable, it needs to adopt a more effective strategy for better outcome in coming years. An achievement of 61 in IMR and 339 in MMR, for the level of investment in the health services, is a serious problem and should be addressed through a much more active programme in home based newborn care, better facilities in the public sector for detecting high risk cases, managing referrals and better emergency obstetric management at FRUs and District Hospitals and at the same time working towards an effective and active convergence and integration within health and other social, education and relevant sectors, which are lacking and underdeveloped.
The main weakness on human resource planning is the failure to deploy the scarce skilled human resources such as specialists and trained medical doctors in facilities and areas where they are required. The learned skills of MOs as well as RHPs posted at Sub-centers are not utilized for the benefit of community either due to lack of confidence or initiations from provider‘s aspect, lack of facilities to practice the learned skill or other reasons known to them and other service providers.

5th Common Review Mission-Assam 2011
47 | P a g e
The state‘s decision to discontinue the skill upgradation training programmes for Medical officers on LSAS and CEmOC needs to be relooked into. Since this is a long term programme, the state needs to look into the immediate need for ensuring emergency obstetric care in view of their MMR which is one of the highest in the country.
Most of the VHNSC decisions and procurement is related to equipment and improvement of curative facilities at the village level. There was no evidence that the social determinants of health were being addressed. There needs to be greater coordination between the NRHM and those from other departments of the Government (e.g. ICDS, MGNREGA, Total Sanitation Campaign, Social Welfare programmes, Gender sensitization programmes)
Focus Group Discussions-I
The FDG was held on 11th November 2011 at Mitticula village, Nagaon. Most of the people living in the village belonged to scheduled casteagrarian society., It was conducted for half an hour with the village community. The team met avillage elder, who was a Ward Member. People in the village were invited to the discussion. The discussion was held in the courtyard of the house of the Ward member. The discussion was in Bengali, the local language of the people living in the village. A list of topics was introduced for discussion. The discussion was translated into English. Attempts were made to encourage all participants to express their views. Participants: The focus group was started with the following participants:

5th Common Review Mission-Assam 2011
48 | P a g e
Focus Group Discussions-II
The FDG was held on 11th November 2011 at Kathiatoli Block PHC, Nagaon. The group was mixed with village people and ASHAs hailing from the Hindu and Muslim communities and from Upper castes, other Backward classes and from Scheduled Castes. It was held for half an hour. Method: The team asked the authorities at the PHC to invite villagers and ASHAs for the focus group. The discussion was held in the PHC building. The discussion was in Assamese, the local language of the people. A list of topics for discussion was made and the issues introduced during the session. People were invited to discuss the topics. The

5th Common Review Mission-Assam 2011
49 | P a g e

5th Common Review Mission-Assam 2011
50 | P a g e
17. Overall Outcome ii). Progress against approved PIP The general trend of expenditure against the approved PIP is detained below:
Figure 7: Bar chart showing the year-wise utilization of funds as against the approved PIP in Assam
Funds released are adequate and somewhere excess utilization more than the approved PIP was there due to some circumstantial reason. The Statement showing release, expenditure and unutilized fund of Assam from FYs 2007-08 to 2011-12 (Upto 30th September, 2011) as under:-
ii). Progress against approved PIP
E. Impact of NRHM There was a general feeling that the health services in the area had improved tremendously. The free
and easy availability of medicines and access to hospitals were mentioned. F. Scope for improvement
The ASHAs wanted a regular salary as their income was variable. A male member of the group, who also happened to be the spouse of an ASHA, also supported this.
Many people voiced the opinion that the older routine of an outpatient service in the evenings, which was recently abolished, needs to be reinstated as it was very convenient for people.
Limitations of Focus Groups: The limitations of the Focus Groups were that they were not recorded on tape for verbatim transcription and detailed analysis. The larger number of people in the groups probably prevented a more detailed discussion of the issues. Conclusions of Focus Groups: Nevertheless, the overall feedback from the two Focus Group Discussions was that NRHM had made a significant impact and contribution to the lives of ordinary people. They felt that the ASHAs were a good link with the health service and that there was easy access to hospitals and free health care.

5th Common Review Mission-Assam 2011
51 | P a g e
The general trend of expenditure against the approved PIP is detained below:
Figure 7: Bar chart showing the year-wise utilization of funds as against the approved PIP in Assam
Funds released are adequate and somewhere utilization more than the approved PIP was there due to some circumstantial reason. The Statement showing release, expenditure and unutilized fund of Assam from FYs 2007-08 to 2011-12 (Upto 30th September, 2011) as under:-
Statement showing the fund released and utilized from FYs 2007-08 to 2011-12 (Upto 30th September, 2011)

5th Common Review Mission-Assam 2011
52 | P a g e
(Amount in Crore)
Year Scheme PIP Approved
Fund Released
Fund Utilized Fund Unutilized
%of fund utilization
2007-08 RCH-II 141.13 166.95 66.11 100.84 39.60 NRHM 446.83 322.31 45.28 277.03 14.05 UIP 14.19 13.65 17.1 -3.45 125.27 Total 602.15 502.91 128.49 374.42 25.55
2008-09 RCH-II 263.79 230.33 182.08 48.25 79.05 NRHM 438.41 237.12 369.43 -132.31 155.80 UIP 10.24 30.36 28.41 1.95 93.58 Total 712.44 497.81 579.92 -82.11 116.49
2009-10 RCH-II 220.45 314.65 154.62 160.03 49.14 NRHM 587.80 363.92 448.96 -85.04 123.37 UIP 15.44 23.52 19.89 3.63 84.57 Total 823.69 702.09 623.47 78.62 88.80
2010-11 RCH-II 317.39 148 241.38 -93.38 163.09 NRHM 734.12 398.23 505.06 -106.83 126.83 UIP 22.34 22.57 20.04 2.53 88.79 Total 1,073.85 568.80 766.48 -197.68 134.75
2011-12 RCH-II 315.09 0 150.49 -150.49 NA NRHM 399.93 280.49 83.58 196.91 29.80 UIP 23.73 12.95 11.87 1.08 91.66
Total 738.75 293.44 245.94 47.50 83.81
Table 16: Statement showing the fund released and utilized from FYs 2007-08 to 2011-12 (Upto 30th September, 2011)
The status on PIP approved, fund release, fund utilize and percentage of fund utilized as per approved PIP for financial year 2011-12 is shown in table below:
PIP Approved, Fund release, Fund utilized and % of Fund utilized to the PIP Approved for FY 2011-12 as below:-

5th Common Review Mission-Assam 2011
53 | P a g e
(Upto 30th September, 2011) (Rs in Crore) Year Scheme PIP Approved Fund Released Fund Utilized %of fund
utilization to PIP
Approved 1 2 3 4 5 6=5/3 1 RCH-II
316.76 -
150.49
47.51%
2 Additionalities under NRHM
373.98
280.49
83.58
22.35%
3 Routine Immunization 13.72
12.95
3.74
27.26%
4 P.P.I. 8.93
-
1.71
19.14%
5 Infrastructure Maintenance
77.42
58.07
24.51
31.66%
6 I.D.S.P. 1.93
0.93
0.25
12.93%
7 N.I.D.D.C.P. 0.42
0.32
-
0.00%
8 N.L.E.P. 1.20
-
-
0.00%
9 N.P.C.B. 10.39
-
-
0.00%
10 N.V.B.D.C.P. 38.84
-
3.65
9.40%
11 R.N.T.C.P. 7.75
5.11
0.80
10.32%
Grand Total 851.35
357.87
268.73
31.57%
Table 17: The table showing the PIP approved, fund release & utilization for FY 2011-12.
Analysis:- The above table shows that the utilization is low under NRHM Additionalities, Routine Immunization, P.P.I., Infrastructure Maintenance and IDSP. State should take necessary action for improvement of utilization of funds.
Some UCs are pending since there was no utilization of funds from the grant received. The funds will be utilized during the next year i.e., 2012. So, they will issue UC‘s in next year. For NDCPs the State is not able to give the UC of IDD because this fund is directly transferred to Government of Assam so, State Health Society in not able to give the UC. The reasons for longstanding advances are that the tracking of advances is poor which a major obstacle to achieve the desired goals. o The reason for low utilization of fund is a weak monitoring system. As per the FMR
analysis of 2nd Quarter some funds show low and high utilization of funds. o Diversions of funds are done temporarily but after the approval of Joint DHS. o The activities carried out from State Contribution are commensurate with the activities
under NRHM.

5th Common Review Mission-Assam 2011
54 | P a g e
o In some places Rogi Kalyan Samiti (RKS) are registered but some where it is not yet registered under the Societies Registration Act. The registering of Rogi Kalyan Samiti under the said Act is in process.
o There was training of Tally Accounting software and regular visits to District and block by the State Finance Personnel
o The payment of Audit fees and Audit expenses incurred against interest earned on NRHM Funds.
Statement Showing Status of Pending Utilization Certificates (UCs)
Year Scheme Sanction Letter Amount in Crore 2010-11 RCH
Flexible Pool
G.27017/18/2010-NRHM (Finance) 120.60
G.27017/18/2010-NRHM (Finance) 27.40
2009-10 RCH Flexible Pool
G27017/4/2009-NRHM (Finance)/NE/GC/5 26.62
G27017/4/2009-NRHM (Finance)/NE/EAC/3 5.62
G27017/4/2009-NRHM (Finance)/NE/GC/8 81.47 Total 261.71
Table 18: Statement Showing Status of Pending Utilization Certificates (UCs)
Achievements:-
A pilot project is going to be implemented in Kamrup District for E- banking. It is proposed to complete the rolling out E-Banking at State Health Society and Pilot District i.e. Kamrup (Rural) by January 2012.
The State is providing the Tally ERP 9 training at their State office of NRHM in Guwahati. Accounts review meetings have also been organized at district level.
Training of Tally Accounting software and regular visit to District and block.

5th Common Review Mission-Assam 2011
55 | P a g e
CHAPTER IV: CASE STUDY ON SUCCESS
Success Stories of Assam under NRHM:
NRHM has brought forth new opportunities and positive changes in the functioning of the public health system in the state. Some of the best practices and innovations are the boat clinics, MMU, ASHA radio programme and provision of mobile phones to ANM of sub-centers. The boat clinic is one of the major state innovations, which ensures delivery of primary health care services to the most inaccessible and remotest areas in the state.
Boat Clinics in Assam: “Reaching Out to the Unreached”
The unique boat clinic initiative was first launched by C-NES in 2005 with a single boat on Brahmaputra river at Dibrugarh in Upper Assam for provision of primary health care services to inhabitants of char areas, which are riverine islands created by Brahmaputra river. These riverine islands are frequently devastated by flood badly affecting the health status of these marginalized people. There are 2251
villages in these islands with a population of nearly 30 lakhs i.e. almost 10% of the population of
Assam under 52 PHCs and 132 HSC. In the year 2008; C-NES partnered with NRHM under PPP for provision of universal primary health care services to the inaccessible and remotest char areas of the state; which cannot be covered by these public health facilities. There has been rapid expansion of boat clinics and as in September 2011; there are 15 boat clinics across the state covering 13 districts of Assam. The focus of the boat clinics is routine immunization, antenatal and post natal care, general health check up, health awareness and water and sanitation. The overall objective of boat clinic is to contribute in the overall reduction of IMR, MMR and TFR of the char areas in relation with the NRHM, Government of Assam and to provide health care delivery to the outreach population in char areas under NRHM.
BOAT CLINIC UNIT-I Coverage: The total 480 char villages in Dhubri district with a population of 689909 and literacy rate of 14 are covered by boat clinics Unit-I and boat clinic Unit-II. Boat Clinic Unit-I caters to almost half of the total 480 char villages in Dhubri and coverage areas fall under the jurisdictions of total 3 PHCs, 10 SHC, 4 Development Block and 13 Gaon Panchayat. The boat clinic Unit-I cover distant char villages and conduct lengthy trips of 3-5 days with night halts at char villages. Function: Services delivered in the boat clinic are as follows:
Immunization of children in which JE vaccine campaign was also included Antenatal and post natal check up General Health check up Referral for complicated pregnancies Emergency preparedness and response in case of flood situations, relief measures etc.
Manpower: It is staffed by total 15 people with 1 district programme officer, 2 medical doctors, 3 nurses, 1 LT, 1 pharmacist, 3 community workers and 4 boat crew members. Performance: In the period from April 2011 to September 20112; total 32 char villages were covered out of 32 targeted villages with 30918 populations. Total 111 camps were conducted in this period where 10635 patients underwent general health check-up including 361 ANC, 116 PNC, 1325 eligible couples accepted oral pills and condoms and total 1355 routine immunization were completed.

5th Common Review Mission-Assam 2011
56 | P a g e
Disease Profile: In the period from April 2011 to September 2011; there were total 10635 OPD cases. Out of these, the most commonest diseases in the char villages are helminthiasis (1263- 11.8%), gastritis (1150- 10.8%), upper RTI (370- 3.4%), lower RTI (333- 3.1%), bronchitis??, fever (1447- 10.7%) and general weakness (395- 3.7%), bodyache (227- 2.1%) and common cold (226—2.1%). ASHA: There are 13 ASHA workers which cover a population of 17216 for the targeted 32 villages having population of 30918. On an average, each ASHA cover population ranging from 735 to 2400. There is a requirement of 17 additional ASHA to cover the whole population in 32 villages. Most of the ASHA are active and participate in health camps conducted by boat clinic in their respective villages.
Gaps in functioning of boat clinics: Majority of deliveries are home deliveries conducted by Traditional Birth Attendant FP services are underutilized with very low uptake for IUCD insertions and sterilization Non- tracking of pregnant women for deliveries since due lists of pregnant women for delivery is not
prepared by ASHA on regular basis Lack of coordination and supervision of ASHA and facilitators Each char village is covered only once in a month by the boat clinic
Challenges:
Difficulty in reaching these islands during flood Transporting the referred cases in the nearby institutions Dedicated manpower for boat clinic – there is high turnover of staffs, in particular doctors Follow up of the patients Low level of literacy- 14% Sustainability
Scope for Improvement:
Increase the number of ASHAs for covering all villages tTrain/orient 1 adolescent girl who is a relative of a pregnant women and tag them together for
regular follow up of pregnant women on antenatal care and other preventive health issues Devise an effective strategy which is locally relevant for reaching out to these marginalized and
underprivileged group of population with the use of audio-visual media for effective BCC etc Increase the frequency of boat clinics trips so that each village is covered more than once in a month May consider means to scale up the boat clinics so that more villages are covered

5th Common Review Mission-Assam 2011
57 | P a g e
CHAPTER V: RECOMMENDATION
1. Infrastructure Upgradation
All basic Laboratory services to be ensured at all health facilities providing inpatient care. All FRUs should be made ‗Functional‘ with blood storage facilities. At present drug
controllers approval has been issued even before the blood storage unit is constructed in FRUs. This needs to be looked by the State authorities.
Sub-centers with 2 ANMs in difficult and inaccessible areas may be upgraded for institutional delivery after training of ANMs in SBA and providing required infrastructure.
A new facility may be developed exclusively for Mother and Child Care at Dhubri Civil Hospital having capacity of 50 beds.
More number of Boats may be brought into operation in such riverine areas so that periodicity of provision of health services can be enhanced.
Water and electricity supply at the remote health facilities and sub centres should be looked up by the state government.
Sub centre construction for the rented buildings may be taken up by the state govt. in the next year PIP.
The time schedules for construction/renovation should be followed otherwise it will lead to the time and cost overrun especially for big projects.
2. Human Resource Health
Develop a comprehensive and sustainable HR policy for addressing and responding to
shortage of human resources for health in the state There is a need for rationalization of Human Resource for health. Need to look into
numbers of contract staff in particular. The specialists such as Anesthetist, Gynecologist, and Pediatricians need to be rationally deployed in facilities and areas where their service is required the most depending not just on vacancy but based on requirements and case loads and remoteness of facility.
State has discarded the multi-skilling training for LSAS and CeMOC. Since this is a long term programme, the state needs to look into the immediate need for ensuring emergency obstetric care in view of their MMR which is one of the highest in the country.
Quality of training seems to be very weak. Attention to skill impartation as part of training is a critical need requiring attention. There is a need for developing a standardized training plan and calendar for various cadre/categories of staffs with regular review of need based or training needs assessment.
Sub-centers with 2 ANMs in difficult and inaccessible areas to be upgraded for institutional delivery after training of ANMs in SBA and providing required infrastructure.
The ANM training should be conducted regularly on annual basis. Interns may be posted for one month at least in the boat clinics on rotation basis

5th Common Review Mission-Assam 2011
58 | P a g e
3. Health Care Service Delivery- facility based –quantity and quality
There is a need for constitution of a Quality Assurance Committee in district hospital and higher facilities since it was observed that quality of health service delivery is a major weakness in the district as a whole.
Orientation of health management on need for biological waste management needs immediate attention.
Supportive supervision needs to be ensured and made effective. Health officials themselves lack the capacity to effectively supervise.
All FRUs to be made ‗Functional‘ FRUs with blood storage facilities. At present drug controllers approval has been issued even for blood storage areas which are under construction in FRUs.
State has identified eclampsia as the largest contributor to maternal deaths. Since this is based on HMIS data, state needs to go in for a detailed epidemiological investigation for this and institute adequate preventive steps.
Antenatal care is weak and needs to be improved both for quantity and quality. At State level, full time nodal officers for Child Health and Maternal Health to be
identified. MDR is a very weak area at district level. The district level staff perhaps need
reorientation on the purpose of MDR
4. Outreach Services
ASHA should be adequately supported for preparing due-lists for pregnant women for ANC and conduct follow up of post natal cases with ANM. ASHA facilitator/ANM/MO should supervise her work on regular basis
There is a need to intensity the Education, motivation and counseling about Family planning and spacing methods
Strengthen the nutritional counseling and provide nutritional supplement Need to strengthen the VHSNC to incorporate ICDS component in effective manner Need to activate the village health committee in the Gram Panchayat
5. ASHA Program
A standardized state and district level monitoring plan should be developed with well
identified activities and specific targets for monitoring. The monitoring plan may be percolated at block and facility levels.
Post trainings follow up needs to be systematized, regularized and intensified A short refresher trainings, particularly about EMC on family planning, should be
conducted so that ASHA feel the need to address the gaps in family planning which is a neglected area in the state
Overall ASHA should be motivated to work for the community welfare and their community work should not be completely driven by incentives

5th Common Review Mission-Assam 2011
59 | P a g e
6. RCH-II (Maternal Health, Child Health and Family Welfare)
Rationalization of Human Resource at health facility needs attention. Facilities in some Nagaon have too many manpower and facilities in Dhubri have too few specialists like Anesthetist, Gynecologist, and Pediatricians. There is need to rationalize numbers of contractual employees also as per the actual need and requirements of these positions. Nagaon has too many and Dhubri too few contractual doctors and GNMs at health facilities.
State has discarded the multi-skilling training for anesthesia and CEmOC. While the state is looking at long term solution to meet the requirements for specialists, the state at the same time needs to look into the immediate need for ensuring emergency obstetric and newborn care in view of their high early neonatal mortality and a MMR which is highest in the country.
Quality of training seems to be very weak. Attention to skill impartation as part of training is a critical need requiring attention.
Training to health staff has to be in consonance with programme guidelines. In Nagaon WHO partograph is used while national guidelines provide a different simplified partograph. The management protocols used in labour rooms of training facilities in Nagaon also give different management of eclampsia and puerperal sepsis as compared to that given in training modules. State Institute of H&F should look into these issues before initiating training.
All FRUs to be made ‗Functional‘ FRUs with blood storage facilities. At present drug controllers approval has been issued even for blood storage areas which are under construction in FRUs.
State has identified Eclampsia as the largest contributor to maternal deaths. Since this is based on HMIS data, state needs to go in for a detailed epidemiological investigation for this and institute adequate preventive steps.
All basic Laboratory services to be ensued at all health facilities providing inpatient care. At a well functioning FRU in Nagaon gynecologists do not treat cases of ecliptic convulsion for want of liver function tests.
Sub-centers with 2 ANMs in difficult and inaccessible areas should be upgraded for institutional delivery after training of ANMs in SBA and providing required infrastructure.
Antenatal care is weak area and needs to be improved both for quantity and quality. MDR is a very weak area at district level. The district level staff perhaps need
reorientation on the purpose of MDR Quality of service delivery is a major weakness
o District QA committees need to be put into place o Orientation of health management on need for biological waste management
needs immediate attention. o Supportive supervision needs to be ensured and made effective. Health officials
themselves lack the capacity to effectively supervise. PPP exists in Nagaon tea estate hospital but protocols not in keeping with guidelines. Supportive supervision is completely lacking. The biggest gap is that the capacity of
supervisors themselves needs to be enhanced by proper orientation to RCH concepts and interventions.
5th Common Review Mission-Assam 2011
60 | P a g e
7. Preventive & Promotive health services including Nutrition & Inter-sectoral Convergence
There needs to be greater coordination between the NRHM programmes and those from other departments of the Government (e.g. ICDS, MGNREGA, Total Sanitation Campaign, Social exclusion programmes, Gender sensitization programmes)
8. Gender Issues & PCPNDT
Gender issues need to be taken into consideration in providing services at facilities and in the facilities. There should be separate toilets for male and female patients at all facilities, wherever required.
A Nodal office has to be identified at the state level to regularly monitor and for inspection of PNTC centers
District level PCPNDT committees should be formed and regular monitoring and review meetings should be held and minutes may be shared with the state level authorities.
9. National Disease Control Programmes:
NVBCP:
Immediate Measures:
Primaquine (PQ) 2.5 mg and 7.5 mg to be made available at all BPHS. Malaria record maintenance (M1 to M4) to be updated at all BPHS. Drug stock register not
maintained properly, hence necessary action to be taken for updating it and adding a column on drug expiry.
Orientation training programmes on case management in the light of recent NVBDCP guidelines to be imparted
JE vaccine of short expiry lying at BPHC to be immediately shifted to district Sindagar where adult JE vaccination project is in progress
Short term: Binocular microscope to be provided at MPHC Kuwaritol Orientation training of malaria microscopy to be provided to all technicians. Block Programme Managers of all endemic districts to be trained on some important
technical issues on malaria Staining jars with the lids to be provided in all the BPHCs
Long term:
The malaria laboratory in district hospital (Nagaon) to be renovated using funds from NRHM for infrastructure improvement.
5th Common Review Mission-Assam 2011
61 | P a g e
RNTCP: A directive needs to be issued to all MO-PHI through Joint DHS to refer all patients with
cough for >2 weeks for sputum examination. Directive to screen all contacts of sputum smear patients and register for the same is being
maintained at DMC level Screening of all high risk patients (chronic smokers, diabetes, and HIV positive elderly) as
per universal access to TB care and this is to be stressed during the monthly review meeting with DM/CMO.
Sputum collection centers to be established in the non-DMC PHI and the Char areas and transport them to the nearest Designated Microscopy centres for sputum examination.
Explore the possibilities of involving the mobile boat clinics for sputum collection and transportation to DMCs
Intensify IEC activities especially in the hard to reach areas to ensure that all ICTCs are referring any patients with 2 weeks cough for sputum examination.
A directive to be issued to all MO-PHIs to ensure that the regular staffs of the PHI are involved in default retrieval activities regularly especially MPW and MPHS.
Regular staffs of peripheral health institution like Sub- centres should also be asked to retrieve defaulting patients.
Establishing sputum collection centres in all Non DMC PHIs
Nagaon district
All STS and STLS have been asked to prepare list of all sputum positive patients every month who are supposed to come for follow up within that month and retrieve and bring back the patients who doesn‘t come for follow up within the stipulated period.
To ensure involvement of ASHAs for sputum collection from patients for follow up as well and the ASHAs should be provided with sputum cups for this purpose. ASHA incentives and should be paid in time. Retraining of ASHA should be looked at.
Dhubri district
Ensuring that RNTCP is specially reviewed in the South Bank of Dhubri district looking into the dismal performance in this TB Unit
A directive may be issued to all MO In-charge to ensure that all chest symptomatic patients (>2 weeks cough) are referred to the DMC immediately for sputum examination.
A mechanism should be in place for collection of sputum samples from TB suspects from periphery who are unable to travel to the DMC and transported to the DMC for sputum examination.
RNTCP should also be accorded priority during the monthly review meetings all activities including referral of TB suspects and review of diagnosis and treatment activities should be a part of the discussion.
Special awareness drive to be undertaken under South Salmara and Sukchar DMCs so that people instead of going to other health centers avail TB diagnosis and treatment services from their nearest DMC

5th Common Review Mission-Assam 2011
62 | P a g e
10. Programme Management
There should be a proper monitoring plan with identification of focal person for various programmes and sub-components with time-frames for monitoring.
There should be more coordination between the facilities and district level officials and more frequent field visits to be undertaken for corrective actions and advise for improvement
The PPP run facilities and programmes like school health may be monitored monthly against the performance indicators.
The co-ordination between the programme management unit and the health directorate at the state level may be strengthened.
The posting of the staff of programme management needs rationalization as per the work requirement.
Data entry operators at the block level may be oriented regularly to prevent data loss. 11. Procurement System
The basis for the need assessment for purchase of equipments for the health facilities may
be improved. Computerization (PROMIS) of logistics is only at the state level which may be extended to the
district level also. Selective decentralization of the procurement system may be done for the district and block
level as some emergency drugs are procured by health facilities via RKS funds but generally patients are asked to buy the drugs.
12. Effective Use of Information Technology
Printing option of auto generated forwarding letter along with complaint detail should be
available in the web portal for e-complaint reddressal. HMIS needs support at block level by putting in block data entry operators The uploading of HMIS data needs to be improved and completeness of uploaded should be
ensured. Proper orientation and capacity building of data and programme managers is required for use
of data for programmme management and decision making. The Block Health Action Plans seem to be non-existent and need to be systematically
planned based on local HMIS data. Mother and Child Tracking System needs to be improved and reporting on MCTC from data
entry points should be strengthen since only half of sub-centers are currently reporting on MCTS of all the total health facilities in the state.
13. Financial Management
NRHM Finance personnel need more orientation on financial procedure, working and reporting.
The physical audit of assets should be implemented and stock audit has to be done. NRHM Finance personnel need more orientation on financial procedure, working and
reporting. The bills should be in systematic order and all relevant and necessary details should be
recorded on the bills. Recording of supporting bills in proper way is the major part in financial

5th Common Review Mission-Assam 2011
63 | P a g e
procedure. Authenticity of bills is only shown if they are complete and recorded systematically.
The formats for bank reconciliation statements, fixed asset register etc should be as per the financial guidelines.
Advance Tracking Register and Advance ageing report should be prepared at all places. There should be Identification Marks on Fixed Assets Many formats were produced by the Tally ERP 9. So, the Tally Solution person may guide
the finance person to produce financial reports such as Bank Reconciliation Statement (BRS).
14. Decentralized local health action
There is a need to integrate and coordinate the many different government schemes to
improve the lives of people and to empower then and provide social justice VHSNC need to revitalize through proactive participation and involvement of PRIs in overall
development of all determinants of health. Community monitoring should be started and there is a need to actively involve community
participation in the NRHM programme across the state. The District Level Vigilance Monitoring Committees need to be notified and established. There is a need to monitor compliance of IFA medication among pregnant women as the
rates of anemia continue to be high. State should develop monitoring plan for each district with a target to cover at least 20% of
the facilities in a quarter. Visit should be prioritizing based on performance.

5th Common Review Mission-Assam 2011
64 | P a g e
CHAPTER VI: STATE SPECIFIC ISSUES
In general, the state had made various state level initiatives for increasing the accessibility and affordability of service delivery. However, the CRM team felt that the following issues are unique to the state of Assam and need to be addressed and considered with sense of urgency, calling for policy level intervention:
Human Resource Policy
The state needs to urgently implement the proposal for creation of specialist cadre and cadre review. There is a need to formulate a transfer and posting policy, to be implemented in a transparent and fair manner. The state should adopt a more rational deployment of human resources, which is need based considering the vacancy, expected case load, functionality of facilities etc. The state has discontinued the multi-skilling training for LSAS and CEmOC. While the state is looking at long term solution to meet the need for specialists, the state at the same time needs to look into the immediate need for ensuring emergency obstetric and newborn care in view of their high early neonatal mortality and MMR which is highest in the country. There is need of a restructuring of Health Directorate and initiatives should be taken to bridge the coordination gap between the Mission Directorate and Directorate. There is disconnection and lack of integration between the State Health Society and the Directorate of Health & Family Welfare. It is the need of the hour to develop a robust mechanism for integration of the State Health Mission under State Health Society into the state Health services structure for effective and successful implementation of NHRM and public health care delivery services in the long run.
Health Service Delivery
The quality of service delivery is a major weakness that the CRM team observed across facilities and districts visited. The focus should be to ensure constitution of various District Quality Assurance Committees on an urgent basis. There is need for initiation of orientation of health management and paramedical on Biological Waste Management. Supportive supervision needs to be ensured and made effective. Some of the health officials themselves lack the capacity to effectively supervise.
RCH & Child Health
The quality of RCH services in particular needs urgent improvement in the state. The state has the highest MMR in India and with the current pace and quality of implementation; the goal will not be achieved in time. The state therefore has to devise new strategies for accelerating the decline of MMR, TFR and IMR. As per HMIS data, Eclampsia is the largest contributor to maternal deaths. The state needs to go in for a detailed epidemiological investigation for identification of Eclampsia major cause of maternal death; and it requires initiating an adequate preventive steps. MDR is a very weak area at district level. The district level staff needs reorientation on the purpose of MDR. Vector borne Diseases
The AES/JE occupies an important role amongst the prevalent vector borne diseases as there has been a significant increase in the no. of AES/JE cases and death cases reported in the state.

5th Common Review Mission-Assam 2011
65 | P a g e
Financial Management
The cheques are prepared manually by Finance personnel in most of the offices. There is also scarcity of cheques which could be resolved if the state health sector coordinate with the finance sector and with their respective counterparts in health facilities and banks. The cheques were printed by the finance personnel through computer and such step may help to decrease manpower and promote efficient working.
PPP Policy
The state does not seem to have PPP policy. Although there are PPP initiatives which have been undertaken by the state, mostly in tea garden and other NGOs; there is lack of mutual understanding and close coordination, particularly in areas of implementation of guidelines and protocols.